Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
June 16, 2026
Who This Lumbar Spinal Stenosis Page Is For
This page is intended for patients who have been diagnosed with lumbar spinal stenosis on MRI or CT scan, as well as for family members seeking a clear, structured explanation of what the finding truly means and why walking-related leg symptoms may occur.
Many people learn about spinal stenosis after years of gradually worsening walking limitation, leg heaviness, numbness, or pain that improves when sitting or bending forward. You are not expected to read this page from start to finish. Instead, you may return to specific sections when new questions arise — for example, when walking distance decreases, MRI findings seem alarming, injections are suggested, or surgery is recommended.
If medical opinions differ, surgery has been proposed without a clear explanation of why decompression alone or fusion is recommended, or you are unsure whether symptoms truly match imaging findings, an individualized neurosurgical second opinion can help clarify whether continued conservative care or surgical treatment is the most appropriate next step.
When patients seek a second opinion for lumbar spinal stenosis
• Surgery has been recommended, but it is unclear whether decompression alone is sufficient or fusion is necessary
• Different doctors provide conflicting advice (continue conservative treatment vs. operate now)
• Walking distance is progressively decreasing despite injections, therapy, or medication
• MRI describes “severe stenosis,” but symptoms do not clearly match the imaging findings
• Multiple levels appear narrowed, and it is unclear which level is truly responsible for symptoms
• Symptoms persist or worsen after previous lumbar decompression surgery
Not every lumbar spinal stenosis requires surgery, and not every narrowing seen on MRI is clinically dominant.
When walking limitation, neurologic findings, and imaging results do not clearly align, careful evaluation is essential.
If your situation involves uncertainty about indication, timing, or surgical strategy, you may request an individualized neurosurgical review here:
Request Second Opinion
Lumbar Spinal Stenosis — Quick Summary (Read This First)
- Lumbar spinal stenosis means narrowing of the spinal canal or nerve root corridors in the lower back. It compresses the cauda equina (a bundle of nerve roots) or individual nerve roots — not the spinal cord (which ends around L1-L2 level).
- The most common cause is spinal degeneration. Disc collapse, facet joint hypertrophy, osteophyte formation, ligamentum flavum thickening, and sometimes degenerative spondylolisthesis (instability) gradually reduce available space.
- The hallmark symptom is neurogenic claudication. Walking causes leg pain, heaviness, numbness, or weakness that improves with sitting or bending forward.
- Symptoms are posture-dependent. Extension (standing upright) narrows the canal; flexion (leaning forward) increases space and often relieves symptoms.
- Stenosis is not always “just compression.” Mechanical crowding, venous congestion, and dynamic narrowing during walking all contribute to symptoms.
- MRI is the key diagnostic tool. It shows central canal, lateral recess, and foraminal narrowing — but imaging severity must correlate with clinical findings.
- Not every severe-looking MRI requires surgery. Many patients can be managed conservatively if walking distance and neurologic function remain acceptable.
- Surgery is considered when function declines. Indications include progressive neurologic deficit, cauda equina syndrome, or severe walking limitation despite optimized conservative treatment.
- The goal of surgery is decompression, not removal of degeneration. Laminectomy or microsurgical decompression increases space for nerve roots. Fusion is reserved for proven instability.
- In properly selected patients, improvement in walking distance occurs in approximately 60–80% at one year. Back pain relief is less predictable.
- Many other conditions can mimic stenosis. Vascular disease, peripheral neuropathy, hip osteoarthritis, or cervical/thoracic pathology must be excluded before surgery.
- This page is structured so you can focus on what applies to your situation. Use the Contents box to jump directly to mechanisms, diagnosis, surgery, complications, or recovery.
Most readers benefit from the Quick Summary plus the sections on When Do You Need Surgery?, Neurogenic Claudication — Mechanisms, and Surgical Options. The remaining sections provide deeper clinical detail for patients seeking a comprehensive understanding.
Lumbar spinal stenosis with neurogenic claudication means that narrowing in the lower spinal canal compresses or crowds the cauda equina or lumbar nerve roots during standing and walking. The typical result is leg pain, heaviness, numbness, weakness, or reduced walking distance that improves when the patient sits down or bends forward. The diagnosis should not be based on MRI alone; symptoms, walking limitation, neurological findings, and the exact level of stenosis must fit together before deciding between conservative care, injections, decompression, or fusion.
Contents
- Who This Page Is For
- Quick Summary
- What Is Lumbar Spinal Stenosis?
- Lumbar Spine Anatomy
- Degenerative Components
- Why Symptoms Worsen
- Neurogenic Claudication — Mechanisms
- Clinical Patterns
- Symptoms
- Neurologic deficits
- Cauda equina syndrome
- Mimicking conditions
- MRI
- Conservative treatment
- Treatments that are often not enough
- When surgery is needed
- Who typically gets surgery
- Second opinion
- Surgical options
- Why recommendations differ
- Risks and complications
- Recovery
- Persistent symptoms
- Prognosis
- FAQs
- Additional resources
What Is Lumbar Spinal Stenosis?
Lumbar spinal stenosis means pathologic narrowing of spaces that normally allow the cauda equina and nerve roots to move freely:
- Central canal stenosis (main canal narrowing)
- Lateral recess stenosis (narrowing of the root’s “corridor” before it exits spinal canal)
- Foraminal stenosis (narrowing of the exit foramen)
Most clinically relevant stenosis is degenerative and develops gradually over years.
It most frequently affects the L4–L5 level (approximately 45–60% of cases), followed by L3–L4 (20–30%) and L5–S1 (10–20%).
In individuals over 60 years of age, imaging studies show radiological spinal canal narrowing in approximately 20–30% of the population. However, only about 8–11% develop clinically significant symptoms such as neurogenic claudication.
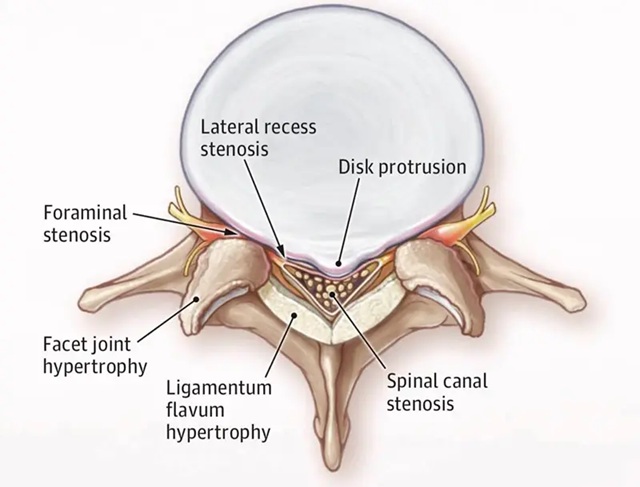
Image: Narrowed sections of the spinal canal (central canal, lateral recess) and foramina due to degenerative changes (osteophytes from the vertebral bodies anteriorly and the facets posteriorly, as well as an enlarged ligamentum flavum).
Lumbar Spine Anatomy
The lumbosacral spine consists of five lumbar vertebrae (L1–L5) and the sacrum (S1–S5), which is a single fused bone connecting the spine to the pelvis.
Between each pair of lumbar vertebrae lies an intervertebral disc, forming five lumbar motion segments (L1–L2 through L5–S1). A “segment” refers to two adjacent vertebrae together with the disc and facet joints that connect them and allow movement. (For visual clarification of the anatomical structures described here, please refer to the diagrams on this page or on the page.)
Posteriorly, each spinal segment contains:
- Facet joints, which guide motion and provide stability
- Ligamentum flavum, an elastic ligament forming part of the posterior wall of the spinal canal
- The spinal canal, which contains the cauda equina
- The lateral recess and neural foramina, where nerve roots travel and exit
Unlike the cervical spine, the lumbar spinal canal does not contain the spinal cord. The spinal cord typically ends around the L1-L2 level (conus medullaris). Below that, the canal contains the cauda equina — a bundle of lumbar and sacral nerve roots (radices), not the spinal cord. This matters because lumbar spinal stenosis compresses nerve roots (cauda equina and/or individual roots), not the spinal cord itself.

Image: Regions of the spine: cervical (neck), thoracic (mid-back), lumbar (lower back), sacral, and coccygeal (tailbone). Inside the spine is the spinal canal, which houses the spinal cord. The spinal cord ends at the level of the L1 vertebra, so the spinal canal of the lumbosacral region contains only nerve roots (either individually or as the cauda equina).
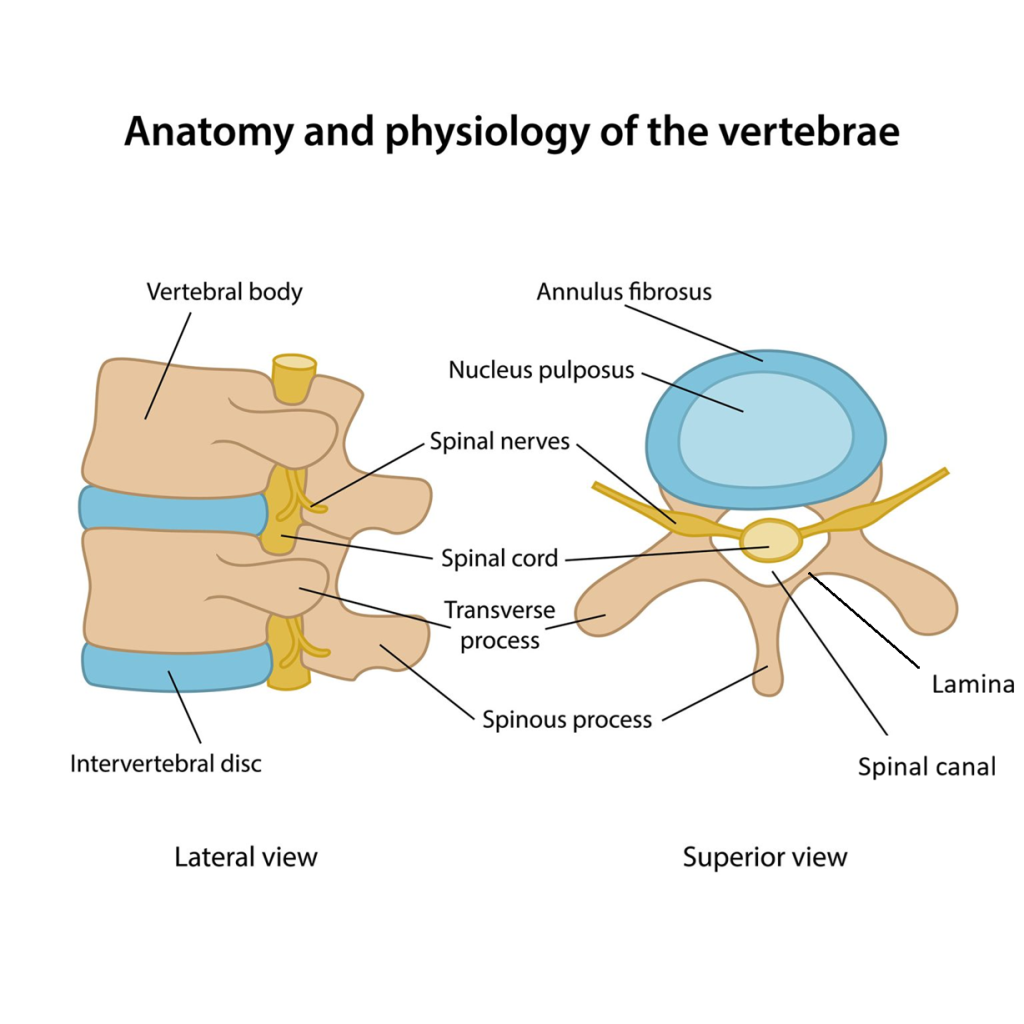
Image: Lumbar vertebrae with the anatomical elements mentioned in the text
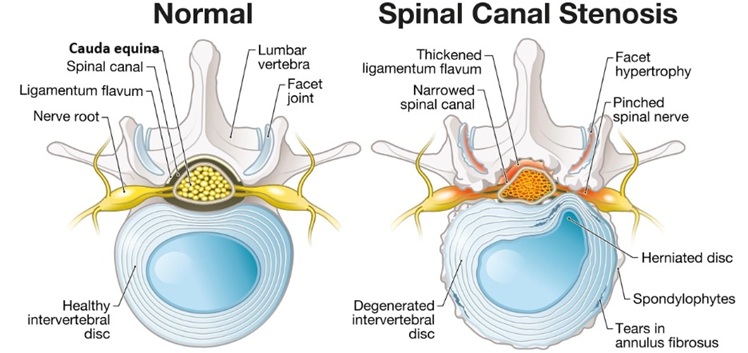
Image: The image on the left shows a normal spinal canal. The image on the right shows spinal canal stenosis caused by osteophytes originating posteriorly from the facets and anteriorly from the vertebrae, as well as hypertrophy of the ligamentum flavum. These changes lead to narrowing and pressure on the cauda equina in the central canal, and on the nerve roots within the lateral recesses and foramina.
Degenerative Components of Lumbar Stenosis — What Each Term Means
Lumbar stenosis is rarely caused by a single structure. It most commonly results from a combination of:
- degenerative disc collapse
- facet joint hypertrophy
- osteophyte (bone spur) formation
- thickening (hypertrophy) and infolding of the ligamentum flavum
- degenerative spondylolisthesis
Degenerative disc collapse
The intervertebral disc loses height and water content with age. When this happens, the space for the nerve roots becomes smaller and the facet joints carry more load. This contributes to both central and foraminal narrowing.
Facet joint hypertrophy
Facet joints are small posterior joints that stabilize each spinal segment. With degeneration, they enlarge due to cartilage loss and bony overgrowth. Enlarged facets can narrow the lateral recess and central canal.
Osteophyte (bone spur) formation
Osteophytes are bony outgrowths that develop as part of degenerative remodeling. They are common and often harmless. They become clinically relevant only if they reduce the space available for neural structures.
Thickening (hypertrophy) of the ligamentum flavum
The ligamentum flavum forms part of the posterior wall of the spinal canal. With aging, it becomes thicker and less elastic and may fold inward during standing or extension. This dynamic infolding is a major contributor to stenosis symptoms.
Degenerative spondylolisthesis
This refers to forward slippage of one vertebra relative to another due to facet and disc degeneration. Even mild slippage can worsen canal narrowing and introduce dynamic instability. Its presence is important because it influences whether decompression alone is sufficient or surgical stabilization may be required.
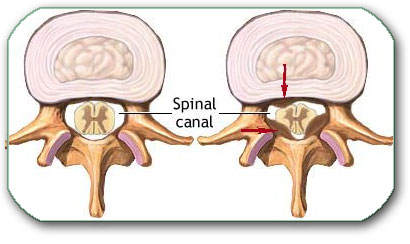
Image: The red arrows indicate osteophytes growing posteriorly from the facets and anteriorly from the vertebral bodies, leading to spinal stenosis.
Why Symptoms Worsen With Standing and Walking (Neurogenic Claudication Explained)
Lumbar spinal stenosis symptoms are posture-dependent. Standing and walking increase lumbar extension (lordosis), which narrows the available space for nerves. Sitting or bending forward does the opposite — it enlarges the canal and reduces pressure.
Symptoms during walking are not caused by “a single pinched nerve,” but by several mechanisms acting together:
• Mechanical root crowding — narrowing reduces space for the cauda equina and nerve roots, causing leg pain, heaviness, numbness, or weakness.
• Venous congestion and impaired microcirculation — narrowed spaces first impair venous outflow. During walking, nerve roots require more oxygen, and insufficient microcirculation produces exertional, ischemia-like symptoms.
• Dynamic narrowing in extension — thickened ligamentum flavum folds inward and facet joints encroach further during standing, temporarily worsening compression. This is why an MRI taken while lying down may underestimate symptom severity.
• Chronic root irritation — long-standing mechanical stress may lead to inflammatory sensitization, resulting in burning pain, persistent paresthesia, or slower recovery after delayed treatment.
Central Stenosis vs Lateral Recess vs Foraminal Stenosis — Clinical Patterns
Central canal stenosis
Typically affects multiple roots (cauda equina crowding). Symptoms are often:
- bilateral leg heaviness or pain
- numbness with walking
- “global” leg fatigue
- neurogenic claudication pattern dominates
Lateral recess stenosis
Affects the traversing root (before it exits). Often:
- unilateral or asymmetric radicular pain
- may mimic disc-related sciatica
- can coexist with central stenosis
Foraminal stenosis
Affects the exiting root. Often:
- radicular pain in a dermatomal distribution
- symptoms may worsen with standing (foraminal height decreases)
- may be prominent with disc collapse
Symptoms of Lumbar Spinal Stenosis
Common symptoms include:
- Leg pain, heaviness, numbness and/or weakness during walking
- Progressive reduction in walking distance
- Relief when sitting or bending forward
- Symptoms often bilateral, but may be asymmetric
- Low back pain may coexist but is not always dominant
- In advanced cases: balance problems and falls due to leg weakness/fatigue
Importantly, many patients do not describe sharp “electric sciatica” as their main symptom. Instead, they describe a functional walking limit.
Neurologic Deficits
Neurologic deficits may develop gradually:
- sensory loss or paresthesia
- motor weakness (often subtle early)
- reduced reflexes, sometimes symmetric
- gait deterioration
Because the lumbar spinal cord is absent, deficits reflect nerve root dysfunction (radiculopathy or multiradicular dysfunction), not myelopathy.
Cauda Equina Syndrome in Degenerative Stenosis
Although more classically linked to large disc herniation, cauda equina syndrome can occur in severe central stenosis, especially if combined with acute disc protrusion, hematoma, or other acute worsening.
Key symptoms include:
- new urinary retention or incontinence
- saddle anesthesia
- rapidly progressive bilateral leg weakness
This requires urgent evaluation and decompression.
Conditions That Mimic Lumbar Stenosis (And Must Be Considered)
Several conditions can produce similar walking limitation or leg symptoms:
- Peripheral arterial disease (vascular claudication): Leg pain results from reduced blood circulation. It typically begins after walking a predictable distance, improves quickly with simple rest (without the need to bend forward), and does not usually occur while standing still. It may also be associated with cold feet, skin changes, or weak peripheral pulses.
- Peripheral neuropathy (diabetic or other): Numbness and burning are usually constant, affect both feet in a “sock-like” pattern, and are not clearly related to walking or body position.
- Hip osteoarthritis: Pain is mainly felt in the groin or hip joint, gets worse when moving or rotating the hip, and is reproduced when the hip is examined by a doctor.
- Severe bilateral foraminal disc herniation: Pain follows a specific nerve path down the leg, may start suddenly, and is often sharper and more localized than the heavy, walking-related symptoms of spinal stenosis.
- Cervical or thoracic pathology (myelopathy): Symptoms may include problems with hand coordination, stiffness, balance difficulty, or exaggerated reflexes, which indicate spinal cord involvement — something that does not occur in lumbar spinal stenosis.
- The presence of Tarlov cysts can sometimes contribute to the symptoms.
In unclear cases, the differential diagnosis is critical before surgery.
Diagnosis of Lumbar Spinal Stenosis
MRI
MRI is the gold standard. It visualizes:
- central canal diameter and crowding of cauda equina
- lateral recess narrowing
- foraminal narrowing
- facet hypertrophy and synovial cysts
- ligamentum flavum thickening
- disc collapse and degenerative changes
- presence of spondylolisthesis and secondary changes
A key limitation is that MRI is usually performed supine (while lying down), so dynamic stenosis may be underestimated. When MRI findings are complex or multilevel, selecting the truly symptomatic level is critical.
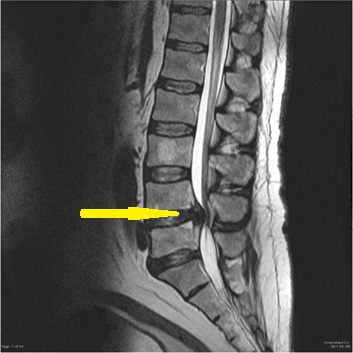
Image: MRI scan of the lumbar spine, where the yellow arrow indicates spinal stenosis at the L4-L5 level.
Key Terms on an MRI Report That Cause Misunderstanding
Radiology terms can sound alarming, but many are descriptive rather than decisive “surgical labels.” The most common confusing terms are:
- Mild / moderate / severe stenosis: a descriptive grading, not an automatic indication for surgery. Symptoms and function matter more than the label.
- Central vs lateral recess vs foraminal stenosis: different locations of narrowing, which influences symptoms and surgical planning.
- Multilevel stenosis: multiple levels may look narrow, but only one (or two) may be clinically dominant.
- Compression vs contact: contact of a root is not the same as clinically meaningful compression.
- Degenerative changes: common with age; not all are pain generators.
CT
CT is useful for detailed bony anatomy, osteophytes, facet arthrosis, and surgical planning.
In patients who cannot undergo MRI — for example due to pacemakers, certain metallic implants, or severe claustrophobia — CT may be sufficient to establish the diagnosis of spinal canal narrowing, particularly when combined with clinical findings.
In selected cases, CT myelography can provide additional information about neural compression.
Dynamic X-rays (flexion–extension)
These are important when instability is suspected, especially with degenerative spondylolisthesis. They help identify abnormal translation/angulation that may influence the decision for fusion.
EMG/EMNG
Rarely required, but may help when:
- symptoms and MRI do not correlate
- peripheral neuropathy is suspected
- there is diagnostic ambiguity about root involvement
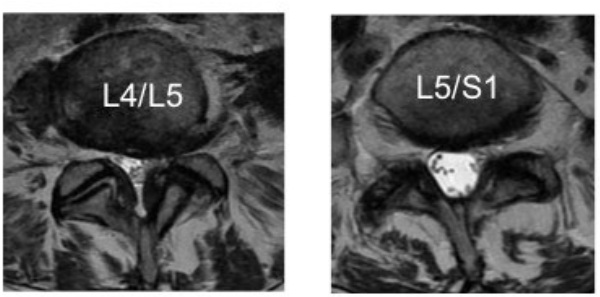
Image: Axial MRI scan of the lumbosacral spine. On the left, a stenotic spinal canal with a compressed cauda equina is visible; on the right, a level with normal spinal canal width and a normal cauda equina is shown as a bright area.
Online pain consultation for low back pain in detail
Schematic explanation of the video consultation for low back pain
Answers to questions about the process and success of video consultations for low back pain
Conservative (Non-Surgical) Treatment
Many patients can be managed without surgery, especially if neurologic deficits are absent (weakness and severe sensory problems) and function is acceptable.
Medical treatment may include:
- NSAIDs and analgesics
- neuropathic pain medications when indicated
- careful short-term use of other agents depending on comorbidities
Physical therapy for spinal stenosis typically emphasizes strategies that functionally increase space for the nerves during daily activities:
- Flexion-based positioning: Learning to maintain a slight forward lean while standing or walking. This „flexion-friendly“ posture reduces lumbar extension and keeps the spinal canal as open as possible.
- Pelvic Tilt Training (Reducing Lordosis): Learning to perform a posterior pelvic tilt (tucking the tailbone under). This movement actively flattens the lower back curve (lordosis), which mechanically opens the spinal canal and reduces the „folding“ of ligaments that causes nerve pressure.
- Core stabilization: Strengthening the deep trunk muscles to support the spine. This helps you maintain a stable posture without excessive „arching“ of the back, which would otherwise narrow the canal.
- Controlled walking programs: Gradual exposure to walking, often using intervals (walking until mild symptoms start, then resting in a flexed position/sitting). This builds endurance without over-compressing the nerves.
- Avoiding prolonged extension: Minimizing activities that require standing perfectly upright or leaning backward for long periods, as these postures naturally increase canal narrowing and provoke symptoms
- Adjunctive modalities (TENS, traction, manual therapy): Electrical stimulation (such as TENS), gentle lumbar traction, and selected manual therapy techniques may provide temporary symptom relief by reducing muscle tension and improving local circulation. However, these methods do not structurally enlarge the spinal canal and should be considered supportive rather than corrective treatments.
Interventional options (selected cases):
- epidural steroid injections
- selective nerve root blocks
Unlike disc herniation, stenosis usually does not “disappear,” but symptoms can stabilize or improve, and walking tolerance can be increased with optimized therapy.
Treatments That Are Often Not Enough for Lumbar Spinal Stenosis
Many commonly promoted approaches may provide temporary relief, but they are usually insufficient when significant structural narrowing of the spinal canal is present.
Examples include:
- General back exercises without understanding posture mechanics — extension-based exercises may worsen symptoms, while flexion may help, but generic programs often ignore this distinction.
- Repeated epidural injections as a long-term strategy — injections may reduce inflammation and temporarily relieve pain, but they do not enlarge a narrowed spinal canal.
- Waiting for improvement through weight loss alone — maintaining a healthy weight supports overall spinal health, but it does not reverse ligament thickening, facet hypertrophy, or canal narrowing.
- Anti-inflammatory diets and supplements marketed as structural solutions — while systemic inflammation can influence pain sensitivity, dietary changes cannot mechanically decompress nerve roots.
- Shoe inserts and posture “correction devices” — they may improve comfort in selected individuals but do not address central canal narrowing.
- Psychological or psychiatric treatment as the primary explanation — mood disturbances often develop secondary to long-term walking limitation and chronic symptoms; they are rarely the root cause of neurogenic claudication.
- Alternative therapies heavily promoted online — massage, aromatherapy, electrical devices, and similar approaches may relax muscles but cannot resolve fixed anatomical compression.
The key issue is not whether these methods can provide temporary relief — some of them can — but whether they address the actual mechanism of nerve compression responsible for neurogenic claudication.
When Do You Need Surgery?
Absolute indications:
- Cauda equina syndrome: A surgical emergency involving severe back pain, numbness in the saddle area (the area that would touch a saddle), and sudden loss of bowel or bladder control, often accompanied by weakness in both legs.
- Progressive neurologic deficit: This refers to a measurable and worsening loss of muscle strength or sensation (such as a foot drop getting worse), indicating that the nerve is being actively damaged.
Relative indications:
- severe limitation in walking distance or daily function despite optimized conservative care
- progressive functional decline
- repeated episodes of severe leg pain and walking limitation that significantly interfere with daily life, when MRI findings clearly match the symptoms.
The main goal of surgery is to increase space for roots and improve function (especially walking distance), not necessarily to eliminate all back pain.
Who Typically Gets Surgery
- Estimated percentage of people with lumbar spinal stenosis who eventually undergo surgery:
~15 % – 30 % over the course of their condition, depending on symptom severity and failure of conservative treatment. - Typical age at surgery:
Most patients who have decompression surgery are between 60 and 75 years old.
Surgery becomes more common with advancing age because degenerative changes progress over time.
Request Lumbar Spinal Stenosis Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Being told that you have lumbar spinal stenosis can raise difficult questions:
Do I really need surgery? Is decompression enough, or is fusion necessary?
Is the MRI finding truly responsible for my walking limitation?
An independent neurosurgical second opinion can help clarify whether your symptoms match the imaging findings,
whether surgery is indicated, and which strategy (decompression alone vs. decompression with stabilization) is most appropriate based on your MRI, functional limitation, and neurologic status.
- ✔ Send a brief message describing your walking distance, leg symptoms (pain, heaviness, numbness, weakness), and what your MRI report states
- ✔ You’ll receive a reply within 24 hours explaining whether we can help with online consultation
- ✔ Priority cases: significant uncertainty about a proposed surgery, complex multilevel findings on MRI, or persistent symptoms that substantially limit daily function — write PRIORITY in your first message
- ✔ MRI images (DICOM), radiology reports, and dynamic X-rays (if available) can be reviewed once initial contact is established
- ✔ During the consultation, we explain whether surgery is truly indicated, expected improvement in walking distance, risks, alternatives, and realistic recovery expectations — with up to 10 days of follow-up for clarification questions
Consultation fees typically range from $180–250, depending on case complexity and number of levels involved.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth neurosurgical second opinions.
Surgical Options — Main Procedures (With Short Explanations)
The appropriate procedure is chosen based on the dominant pathology (central vs foraminal), number of levels, and stability.
Laminectomy (standard decompression)
Under general anesthesia, the patient lies face down (prone position). A small surgical cut (incision) is made down the center of the back over the affected area, usually measuring a few centimeters for each spinal level. The back muscles are gently separated (not cut) to reach the posterior part of the vertebra (lamina). The lamina (posterior bony arch) is partially or completely removed to enlarge the spinal canal and relieve compression of the cauda equina and/or nerve roots. Thickened ligamentum flavum is removed, and a limited medial removal of the facet may be performed if additional decompression is necessary. In most cases, patients are able to stand and walk the day after surgery, depending on their overall condition and the extent of the procedure.
Microsurgical decompression
A decompression performed under magnification (microscope) through a smaller exposure. The principle is the same as laminectomy, but with more precise tissue handling and potentially less collateral trauma.
Minimally invasive decompression
Uses tubular retractors or smaller approaches to decompress the canal/lateral recess while minimizing muscle disruption. The key issue is not the size of the incision but whether decompression is complete and matches the pathology.
Decompression with fusion (when instability exists)
Decompression is combined with stabilization (instrumented fusion) when there is proven or high-risk segmental instability — most commonly degenerative spondylolisthesis, which is present in approximately one-third of symptomatic patients.
In most individuals (about 60–70%), decompression alone is sufficient. However, roughly 30–40% require additional stabilization due to instability demonstrated on flexion–extension imaging, significant facet joint removal during surgery, recurrent stenosis with segmental motion, or associated deformity such as degenerative scoliosis.
Fusion aims to prevent postoperative progression of slippage and recurrent narrowing caused by mechanical instability.
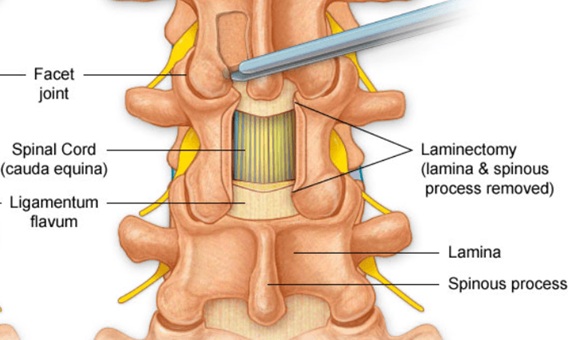
Image: Laminectomy- at the level of the spinal canal stenosis, the left and right laminae along with the spinous process have been removed from the posterior part to relieve the narrowing of the spinal canal.
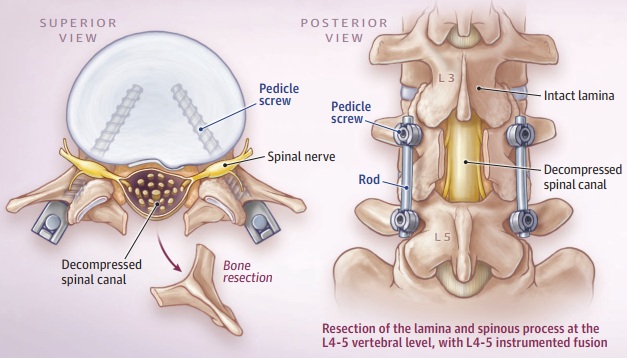
Image: Laminectomy for spinal stenosis with posterior screw and rod fixation performed due to coexisting instability (spondylolisthesis)
In selected cases, additional procedures such as interspinous spacers or disc-related surgery may be considered, but these are not standard treatments for typical degenerative central stenosis in older adults. Surgical strategy is individualized based on the primary mechanism of nerve compression.
Why Do Spinal Surgeons’ Opinions Differ?
Different centers and surgeons may recommend different operations for the same MRI label “stenosis” because the critical determinants are:
- symptoms (neurogenic claudication severity, walking distance)
- neurologic deficits
- exact stenosis location (central, lateral recess, foraminal)
- number of levels
- presence of instability (dynamic films, listhesis, facet degeneration)
- patient age, bone quality, and comorbidities
The most common reason for poor outcome is not the “wrong technique name,” but incorrect patient selection or inadequate decompression of the true symptomatic level/zone.
Potential Risks and Complications
Overall perioperative complication rate: 5 % – 15 % (varies with age and comorbidities). Even in experienced hands, risks exist:
- infection, bleeding
- dural tear and CSF leakage
- nerve root injury
- postoperative hematoma causing new deficits
- persistent symptoms if stenosis was not the main pain generator
- postoperative instability (especially if extensive facet removal is required)
- need for future surgery at the same or adjacent level
Recovery & Functional Improvement
- Significant improvement in walking distance / neurogenic claudication:
~60 % – 80 % of patients report meaningful improvement at 1 year. - Reduction in leg pain or numbness:
~60 % – 80 % report substantial relief. - Sustained long-term benefit (2–5 years):
~60 % – 75 % maintain improvement, though degeneration at adjacent levels can later contribute to new symptoms. - Hospital stay:
Many patients are discharged within 1–3 days after standard decompression. - Return to walking / daily activities:
Most patients are able to walk the next day (depending on age and baseline function).
Chronic Symptoms After Stenosis Surgery
Persistent or recurrent symptoms can occur due to:
- wrong level treated (imaging abnormality not clinically dominant)
- coexisting peripheral neuropathy or vascular disease
- coexisting causes of back and leg pain. This is the most common reason for persistent pain after surgery. Often, these conditions existed prior to the procedure but remained undiagnosed. In such cases, it is crucial to be examined by a specialist familiar with pain anatomy—someone who understands all possible causes of lumbar pain and knows how to accurately diagnose and treat them. For example, the causes of pain can stem from various anatomical structures of the back, such as facet joints, sacroiliac joints, muscles, and ligaments. Within these structures, processes like inflammation, spasms, mechanical strain, etc., can occur. All these factors are triggered and maintained by contributing factors such as prolonged sitting, metabolic disorders, and so on.
- incomplete decompression (missed lateral recess or foraminal component). If any of these three factors are left untreated, pain management will not be successful.
- scar tissue and chronic root sensitization
- progression of degeneration at adjacent segments
- instability developing over time
Read more about the possible causes, diagnosis, and treatment of lower back pain here and pain after lumbar stenosis surgery.
Prognosis and Recovery
In properly selected patients, decompression often improves:
- walking distance
- leg heaviness and pain
- neurogenic claudication tolerance
Back pain improvement is less predictable because back pain may originate from multiple degenerative pain generators (facets, discs, myofascial structures).
Recovery depends on:
- duration of symptoms before surgery
- severity of preoperative deficits
- degree of chronic root damage
- general health and rehabilitation
Frequently Asked Questions About Lumbar Spinal Stenosis
What is lumbar spinal stenosis?
Lumbar spinal stenosis means narrowing of the spinal canal or nerve root corridors in the lower back. This narrowing can compress the cauda equina or individual lumbar nerve roots. It is usually caused by degenerative changes such as disc collapse, facet joint enlargement, osteophytes, ligamentum flavum thickening, and sometimes degenerative spondylolisthesis. Lumbar stenosis does not compress the spinal cord itself, because the spinal cord usually ends around the L1–L2 level. Symptoms depend on whether the narrowing affects the central canal, lateral recess, or neural foramina. MRI findings must always be interpreted together with walking distance, leg symptoms, neurological examination, and functional limitation.
What is lumbar spinal stenosis with neurogenic claudication?
Lumbar spinal stenosis with neurogenic claudication means that narrowing in the lower spinal canal causes walking-related leg symptoms. Patients often describe leg heaviness, pain, numbness, tingling, weakness, or fatigue that appears after standing or walking and improves when sitting or bending forward. The word “neurogenic” means that symptoms come from nerve root compression or impaired nerve root circulation, not from blocked blood vessels in the legs. Neurogenic claudication is the classic functional symptom of clinically significant lumbar stenosis. Treatment decisions are based not only on MRI severity, but also on walking distance, neurological findings, and how much daily function is limited.
Why do symptoms of lumbar spinal stenosis worsen when standing or walking?
Symptoms of lumbar spinal stenosis often worsen during standing or walking because these positions increase lumbar extension. When the lower back arches, the spinal canal and lateral recesses become narrower. The ligamentum flavum may fold inward, facet joints encroach on nerve root corridors, and already crowded nerve roots have even less space. Walking also increases the metabolic demand of nerve roots. If the narrowed canal limits venous outflow and microcirculation, patients may develop leg heaviness, pain, numbness, or weakness after a certain distance. This is why lumbar spinal stenosis is often a dynamic problem: symptoms can be much worse during upright activity than MRI appearance suggests while lying down.
Why do symptoms of lumbar spinal stenosis improve when sitting or bending forward?
Sitting or bending forward often improves symptoms of lumbar spinal stenosis because flexion increases the available space in the spinal canal. When the lower back is slightly flexed, the canal opens, the ligamentum flavum is less folded inward, and pressure on the cauda equina or nerve roots decreases. This is why many patients can walk farther while leaning on a shopping cart, using a walker, or cycling than when walking upright. This posture-dependent relief is one of the strongest clinical clues for neurogenic claudication. It does not mean the stenosis has disappeared; it means that body position temporarily reduces mechanical crowding and improves nerve root tolerance during activity.
What is neurogenic claudication in lumbar spinal stenosis?
Neurogenic claudication is a walking-related syndrome caused by compression and impaired function of lumbar nerve roots. In lumbar spinal stenosis, the narrowed canal crowds the cauda equina and nerve roots. As the patient stands or walks, symptoms appear gradually: leg heaviness, aching, numbness, weakness, burning, or a feeling that the legs may not carry the body. Symptoms often affect both legs, but they can be asymmetric. Relief usually comes with sitting, bending forward, or resting in a flexed position. Neurogenic claudication is different from vascular claudication, where leg pain is caused by poor blood circulation and usually improves simply by stopping, without needing to bend forward.
Is lumbar spinal stenosis the same as a disc herniation?
Lumbar spinal stenosis is not the same as a disc herniation, although both can compress nerve roots. A disc herniation often causes sudden or subacute sciatica, usually on one side, with sharp pain following a specific nerve distribution. Lumbar spinal stenosis is usually degenerative, develops gradually over years, and often causes walking-related leg heaviness, numbness, or bilateral symptoms. Stenosis is usually caused by several structures together: disc collapse, facet enlargement, ligamentum flavum thickening, and bony overgrowth. A disc herniation can coexist with stenosis and may suddenly worsen symptoms. Treatment depends on which problem is dominant and whether symptoms match imaging findings.
What does severe lumbar spinal stenosis on MRI mean?
Severe lumbar spinal stenosis on MRI means that the spinal canal or nerve root corridors appear markedly narrowed. The cauda equina may look crowded, compressed, or have very little surrounding cerebrospinal fluid. However, the word “severe” on MRI is not by itself an automatic indication for surgery. Some patients with severe-looking stenosis have manageable symptoms, while others with moderate stenosis have major walking limitation. The key question is whether the MRI finding matches the patient’s symptoms, walking distance, neurological examination, and functional decline. Surgery is usually considered when severe stenosis is associated with progressive limitation, neurological deficit, cauda equina symptoms, or failure of appropriate conservative treatment.
What is the difference between central canal, lateral recess, and foraminal stenosis in the lumbar spine?
Central canal stenosis means narrowing of the main spinal canal where the cauda equina nerve roots travel. It often causes bilateral leg heaviness, numbness, weakness, or neurogenic claudication during walking. Lateral recess stenosis affects the corridor where a nerve root passes before leaving the canal. It may cause more one-sided radicular pain and can mimic sciatica. Foraminal stenosis means narrowing of the exit opening where the nerve leaves the spine. It often causes pain, numbness, or weakness in a more specific nerve-root distribution and may worsen with standing. Many patients have a combination of all three, which is why precise MRI interpretation matters before choosing treatment.
Can lumbar spinal stenosis cause numbness in the feet or legs?
Lumbar spinal stenosis can cause numbness, tingling, burning, or heaviness in the legs or feet when compressed nerve roots do not function normally. In central canal stenosis, numbness may affect both legs or appear during walking as part of neurogenic claudication. In lateral recess or foraminal stenosis, symptoms may follow a more specific nerve-root pattern, such as the front of the thigh, outer leg, top of the foot, or sole. Numbness that appears after standing or walking and improves with sitting is typical for stenosis. Constant numbness may also suggest chronic root damage, peripheral neuropathy, diabetes-related nerve disease, or another condition, so clinical correlation is important.
Can lumbar spinal stenosis cause bladder problems or incontinence?
Lumbar spinal stenosis can rarely contribute to bladder problems when central canal narrowing becomes severe enough to affect the cauda equina nerve roots. The most concerning symptoms are new urinary retention, loss of bladder control, saddle numbness, rapidly worsening leg weakness, or loss of bowel control. This pattern may represent cauda equina syndrome and requires urgent medical evaluation. Most patients with ordinary lumbar stenosis do not develop true cauda equina syndrome, and bladder symptoms can also come from urologic, prostate, gynecologic, medication-related, or neurological causes. However, new bladder dysfunction together with worsening bilateral leg symptoms should never be dismissed as a routine back problem.
What are signs that lumbar spinal stenosis is getting worse?
Lumbar spinal stenosis may be getting worse when walking distance gradually decreases, leg heaviness appears sooner, numbness becomes more frequent, or weakness starts to affect balance, stairs, or daily activity. Patients may notice that they need to sit more often, lean forward more frequently, or avoid walking because symptoms appear predictably. Worsening one-sided radicular pain may suggest increasing lateral recess or foraminal compression. Red flags include progressive foot weakness, repeated falls, new saddle numbness, urinary retention, incontinence, or rapidly worsening bilateral leg symptoms. These findings require prompt medical assessment. The decision to escalate treatment depends on symptoms, function, neurological findings, and whether MRI changes match the clinical picture.
Can lumbar spinal stenosis improve without surgery?
Lumbar spinal stenosis can sometimes improve symptomatically without surgery, especially when neurological deficits are absent and walking distance remains acceptable. The anatomical narrowing usually does not disappear, but symptoms may become more manageable with posture modification, flexion-based physical therapy, activity pacing, medication, weight control, and treatment of associated pain generators. Some patients remain stable for years with conservative care. Others gradually worsen because degenerative narrowing, instability, or nerve root irritation progresses. Conservative treatment is most reasonable when symptoms are mild to moderate, there is no progressive weakness, and daily function is still acceptable. Surgery becomes more relevant when walking limitation, neurological deficit, or quality-of-life impairment becomes substantial despite appropriate non-surgical treatment.
What treatments can help lumbar spinal stenosis with neurogenic claudication?
Treatment for lumbar spinal stenosis with neurogenic claudication depends on symptom severity, walking distance, neurological findings, and MRI correlation. Conservative treatment may include analgesics, anti-inflammatory medication when appropriate, neuropathic pain medication in selected cases, flexion-based physical therapy, posture training, controlled walking programs, and activity modification. Epidural steroid injections or selective nerve root blocks may provide temporary relief in selected patients, especially when inflammation contributes to pain. These treatments do not structurally enlarge a narrowed canal, but they may improve tolerance and delay or avoid surgery in some cases. Surgical decompression is considered when symptoms remain disabling, walking distance keeps declining, or neurological deficits progress despite optimized conservative care.
Can physical therapy help lumbar spinal stenosis with neurogenic claudication?
Physical therapy can help some patients with lumbar spinal stenosis and neurogenic claudication, especially when symptoms are mild to moderate and there is no progressive neurological deficit. The most useful programs usually focus on flexion-friendly posture, pelvic tilt training, core stabilization, hip mobility, and controlled walking intervals. Patients often learn how to avoid excessive lumbar extension, which narrows the canal and worsens symptoms. Therapy does not remove bone overgrowth, ligament thickening, or fixed canal narrowing, but it can improve posture mechanics, endurance, confidence, and symptom control. If walking distance continues to decline despite appropriate therapy, or if weakness or cauda equina symptoms appear, surgical evaluation becomes more important.
When is surgery needed for lumbar spinal stenosis?
Surgery for lumbar spinal stenosis is usually considered when symptoms clearly match MRI findings and conservative treatment no longer provides acceptable function. Common reasons include severe walking limitation, progressive reduction in walking distance, disabling neurogenic claudication, persistent leg pain or numbness, and progressive neurological deficit such as worsening weakness. Emergency surgery may be needed if cauda equina syndrome develops, especially with urinary retention, saddle anesthesia, or rapidly progressive bilateral leg weakness. Surgery is not based only on the MRI word “severe.” The decision depends on the whole clinical picture: symptoms, neurological examination, functional decline, number of narrowed levels, instability, age, general health, and realistic expectations.
What is surgical decompression for lumbar spinal stenosis with neurogenic claudication?
Surgical decompression for lumbar spinal stenosis means creating more space for the cauda equina and compressed nerve roots. Depending on the anatomy, this may involve laminectomy, microsurgical decompression, removal of thickened ligamentum flavum, and limited removal of bone or enlarged facet tissue that narrows the canal, lateral recess, or foramen. The goal is not to remove all degenerative changes, but to relieve the dominant neural compression responsible for neurogenic claudication. In properly selected patients, decompression mainly improves walking distance, leg heaviness, and leg pain. Back pain may improve less predictably because it can come from multiple structures, including discs, facets, muscles, and sacroiliac joints.
Is decompression enough for lumbar spinal stenosis, or is fusion needed?
Decompression alone is enough for many patients with lumbar spinal stenosis when the spine is stable and the main problem is nerve compression. Fusion is considered when there is proven or high-risk instability, such as significant degenerative spondylolisthesis, abnormal movement on flexion-extension X-rays, recurrent stenosis with instability, deformity, or when adequate decompression would require removal of stabilizing structures. Fusion adds screws, rods, or cages to stabilize the segment, but it also increases surgical magnitude. The key question is whether instability is truly present and clinically relevant. This is why the decision between decompression alone and decompression with fusion often requires careful review of MRI, dynamic X-rays, symptoms, and surgical goals.
Why can pain persist after lumbar spinal stenosis surgery?
Pain can persist after lumbar spinal stenosis surgery for several reasons. Sometimes the compressed level was decompressed, but another pain generator remains, such as facet joint pain, sacroiliac joint pain, myofascial pain, hip disease, peripheral neuropathy, or vascular claudication. Symptoms may also persist if the wrong level was treated, decompression was incomplete, foraminal stenosis was missed, or chronic nerve root damage had already developed before surgery. Scar tissue, recurrent stenosis, adjacent segment degeneration, or postoperative instability can also contribute. Persistent pain does not always mean the operation failed, but it requires structured reassessment. The key is to determine whether the remaining pain is still nerve compression or a different pain source.
English homepage – overview of neurosurgery and pain consultation
Artificial intelligence can also support the process by analyzing complex data, but clinical expertise remains essential.
Sometimes, the real source of pain becomes clear only after diagnostic and therapeutic interventional procedures. In properly selected cases where the pain generator is confirmed and treated directly, most patients experience durable improvement.