Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
May 06, 2026
Who This Chronic Subdural Hematoma Page Is For
This chronic subdural hematoma (cSDH) resource is designed primarily for
families whose CT or MRI scan shows a subdural hematoma and who are being told that surgery, observation, or repeat imaging is being considered,
and who need to understand what this diagnosis truly means and how urgent the situation may be.
This page explains how chronic subdural hematomas form and grow, how they compress the brain, how neurosurgeons decide between monitoring, drainage, craniotomy, or embolization,
and what patients and families can realistically expect during treatment and recovery.
If you are facing uncertainty about CT or MRI findings, the timing of surgery, the risk of recurrence,
or whether newer options such as middle meningeal artery embolization should be considered,
you can request an individualized
neurosurgical second opinion
based on your specific imaging and clinical situation.
When families usually seek a neurosurgical second opinion for chronic subdural hematoma
• Symptoms are slowly worsening weeks after a minor head injury
• CT or MRI shows a subdural collection, but urgency is unclear
• Doctors disagree about surgery versus observation
• There is concern about age, blood thinners, or recurrence risk
Chronic subdural hematoma often raises difficult timing decisions, especially in older patients.
If you need a clear, individualized neurosurgical assessment of imaging and treatment options, you can request a second opinion here:
Request Second Opinion
Chronic Subdural Hematoma — Quick Summary (Read This First)
- Chronic subdural hematoma is a delayed brain bleed. It often appears weeks after a minor or forgotten head injury.
- It grows over time. A fragile membrane forms around a small collection of blood after a minor head injury and slowly leaks fluid and blood, causing the collection to expand and compress the brain.
- Symptoms may be subtle at first. Headache, confusion, weakness, or personality change can progress gradually and then worsen suddenly.
- CT scan is the main diagnostic test. It shows the size of the hematoma and how much it compresses the brain.
- Not every case needs immediate surgery. Small, non-compressive hematomas may be observed, while larger or symptomatic ones require surgical drainage.
- Most patients are treated with 1–2 small burr holes in the skull and drainage of the blood inside the hematoma. A full craniotomy (a larger opening of the skull) is rarely needed.
- The goal is to relieve brain pressure, not to remove every drop of blood. Even partial evacuation is often enough.
- Recurrence is possible. Modern options like middle meningeal artery embolization can help prevent re-accumulation.
- Use the Contents box to jump to surgery, imaging, recurrence, or prognosis sections.
Most families only need the Quick Summary + the Treatment and Prognosis sections. The rest is for deeper understanding.
Contents
- Who This Page Is For
- Quick Summary
- Definition
- Why It Forms
- How It Grows
- Typical Location
- Brain Effects
- When Symptoms Appear
- Symptoms
- Diagnosis
- Treatment
- Observation
- Surgery
- After Surgery
- When Craniotomy
- Recurrence & Embolization
- Request Consultation
- Prognosis
- Epilepsy in Chronic Subdural Hematoma (cSDH)
- FAQs
- Further Reading
Definition
A chronic subdural hematoma (cSDH) is a slowly developing collection of blood and blood-breakdown products in the subdural space, typically surrounded by vascularized membranes that may contribute to its persistence and gradual enlargement. It most commonly develops after a minor or even forgotten head injury, although it can also occur without a clearly recognized trauma.
Unlike acute bleeding, chronic subdural hematomas grow over time.

Image: Preoperative Brain CT Scan The scan shows a crescent-shaped, low-density hematoma (a subdurah collection of old blood or chronic subdural hematoma) in the right frontotemporoparietal area. This has caused compression of the lateral ventricle (squeezing of the brain’s fluid-filled chambers) and a 0.8 cm midline shift to the left.
Incidence and Age Distribution
Chronic subdural hematoma is one of the most common neurosurgical conditions in the elderly.
The reported incidence ranges from approximately 8–15 cases per 100,000 people per year in the general population, but increases significantly with age — reaching 60–80 cases per 100,000 per year in individuals over 65 years, and even higher in those over 80.
The average age of affected patients is typically between 70 and 80 years. Although chronic subdural hematoma is primarily a disease of the elderly, approximately one-third of patients are younger than 65 years. In this younger population, risk factors such as alcohol dependence, anticoagulant use, and head trauma are more frequently involved.
Due to population aging and widespread use of anticoagulant and antiplatelet medications, the incidence of chronic subdural hematoma continues to rise worldwide.
Why Chronic Subdural Hematomas Form
With aging or chronic alcohol use, brain atrophy increases tension on the bridging veins that run from the brain surface to the dura mater. These veins become stretched and more vulnerable to minor tears, allowing slow venous bleeding to occur even after trivial or forgotten head trauma.
Brain atrophy also enlarges the subdural space. This enlargement is crucial: it allows a relatively larger volume of blood to accumulate without immediately producing symptoms. In a younger brain with minimal extra space, a small venous bleed is more likely to be rapidly resorbed before it becomes clinically significant. In contrast, in an atrophic brain, the same amount of bleeding may persist long enough to avoid early symptoms yet remain present within the subdural space. This asymptomatic persistence is a key step in the development of a chronic subdural hematoma. When blood remains in the subdural space, it can trigger inflammatory and vascular changes. Over time, biologically active membranes form around the collection. These membranes contain fragile new blood vessels that may leak repeatedly, contributing to gradual enlargement of the hematoma.
Coagulation abnormalities — common in elderly patients, alcohol-dependent individuals, and those taking anticoagulant or antiplatelet medications — further increase both the likelihood of initial bleeding and the risk that the collection will continue to grow rather than resolve spontaneously.
This happens especially in:
- Older adults, as they often develop brain atrophy (shrinkage)
- Alcohol-dependent patients as they often develop brain atrophy too
- Patients with brain atrophy
- People with large subarachnoid spaces
- Patients taking blood thinners or antiplatelet drugs
- Patients with clotting disorders
- People with achnoid cysts
- Patients with low intracranial pressure
(for example from over-drainage of a VP shunt)
How the Hematoma Grows (Pathophysiology)
Once bleeding starts:
- A thin clot forms in the subdural space
- The clot becomes surrounded by a fibrous membrane
- That membrane produces inflammatory and angiogenic factors
- Fragile capillaries grow into the membrane
- These vessels leak fluid and blood
- The hematoma expands
- Pressure on the brain increases
This is why chronic subdural hematomas often worsen weeks after the injury, not immediately.
Typical Location
Chronic subdural hematomas usually lie over the convex surface of the brain.
They can be:
- Unilateral (most common)
- Bilateral (less common)
When bilateral, one side is usually larger and more symptomatic.
Effect on the Brain
As the hematoma enlarges, it:
- Compresses the brain – This means the pressure is squeezing healthy brain tissue, which can lead to permanent damage if not relieved.
- Shifts midline structures – This indicates that the pressure is so high it is pushing the brain out of its normal position, a sign of severe imbalance inside the skull.
- Can cause subfalcine herniation – This occurs when one part of the brain is pushed under a rigid internal membrane, potentially cutting off vital blood flow.
- In severe cases, transtentorial herniation – This is a life-threatening emergency where the brain is pushed downward toward the brainstem, risking the loss of basic functions like breathing.
This pressure — not the blood itself — causes the neurological symptoms.

Image: Brain Herniations — A large chronic subdural hematoma creates a mass effect, pushing parts of the brain into narrow spaces where they normally do not belong. In these tight areas, the pressure can compromise vital parts of the brain, including the brainstem, which controls breathing and consciousness. Among the different types of herniation, transtentorial (uncal) herniation is the most clinically significant pattern because it is the one most often associated with sudden deterioration.
When Symptoms Appear
Symptoms usually begin 10 days to several weeks or months after the injury.
Many patients do not remember the trauma.
Some patients remain asymptomatic until the hematoma becomes very large, and then deteriorate rapidly and require urgent surgery.
Symptoms
Symptoms depend on size and brain compression and may include:
- Headache
- Confusion
- Memory problems
- Personality or behavior change
- Drowsiness
- Speech difficulty
- Weakness on one side of the body
- Balance problems
- Seizures
- Reduced level of consciousness
In some cases, patients may have had some of these conditions prior to the injury, and it may take some time before a worsening of symptoms or the first new signs become noticeable.
Diagnosis
CT scan
The primary test. It shows:
- Hematoma size
- Brain compression
- Midline shift
An experienced neurosurgeon can also judge whether the hematoma is liquefied enough for minimally invasive drainage instead of craniotomy.
MRI
Helpful when CT findings are unclear or when membranes and stages of blood breakdown must be assessed.
Blood tests
Very important because many patients have:
- Clotting disorders
- Low platelets
- Blood-thinning medications
Whenever feasible, coagulation abnormalities should be corrected or optimized to a safe range before surgery in order to minimize perioperative bleeding risk.
Treatment — When to Operate and When to Observe
The key question in chronic subdural hematoma is whether surgery is needed at all, and how urgently it should be performed. In many patients, surgery is not required at all, and careful observation is the safest approach.
Conservative (Non-Surgical) Treatment
In selected patients with small hematomas and no significant neurological symptoms or brain compression, conservative management may be appropriate.
Approximately 20–30% of carefully selected chronic subdural hematomas may resolve without surgery under close monitoring.
Conservative management may include:
- Careful monitoring
- In selected cases, short courses of corticosteroids may be considered, although their role remains controversial and individualized.
- Adjustment or discontinuation of blood-thinning drugs
- In selected neurologically stable patients, middle meningeal artery (MMA) embolization may be considered as an adjunctive treatment to reduce the risk of recurrence (see detailed explanation below).
Request Chronic Subdural Hematoma Neurosurgery Consultation — CT Review, Surgery Timing, and Recurrence Risk
When a patient develops delayed or progressive symptoms from a chronic subdural hematoma, families are often faced with difficult decisions —
whether to observe, operate, repeat imaging, or consider newer options such as embolization.
An independent neurosurgical second opinion can help clarify how urgent the situation really is and what the safest next step should be.
- ✔ Send a short message describing the patient’s symptoms, CT or MRI findings, and your main concerns
- ✔ You’ll receive a reply within 24 hours explaining if and how we can help in your specific case
- ✔ Time-sensitive cases: if neurological symptoms are worsening, consultations can often be arranged within a few hours — write PRIORITY in your first message
- ✔ If available, CT scans, MRI, and hospital reports can be reviewed once initial contact is established
- ✔ During the consultation, we explain topics such as imaging findings, surgical options (burr holes vs. craniotomy), the role of embolization, and expected recovery, with up to 10 days of follow-up for brief questions.
Consultation fees typically range from $180–250, depending on imaging complexity and recurrence risk.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth second opinions in neurosurgery.
Surgery
The choice of surgical technique in chronic subdural hematoma depends on whether the hematoma is liquefied, septated, recurrent, and how fragile the patient is.
Larger or symptomatic hematomas require surgical evacuation. The key decision in chronic subdural hematoma is not only how to operate, but whether surgery is needed at all and how urgently it should be performed.
Surgery may be urgent, but in many cases surgery can be delayed briefly to stabilize clotting.
Surgical Techniques
- Burr-hole drainage (most common)
- Twist-drill drainage (less invasive option)
- Craniotomy (rarely required)
Burr-hole drainage
If the hematoma is liquefied, it can be removed using:
- One or two burr holes
- Irrigation (washing out the blood), drainage, or most commonly, a combination of both.
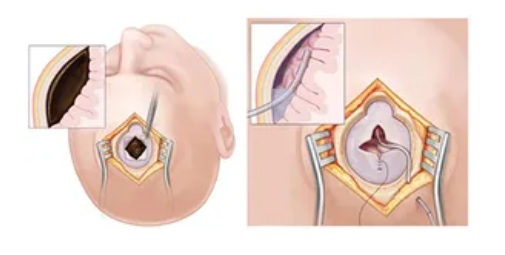
Image: Chronic Subdural Hematoma Surgery The image on the left shows a trepanation (the creation of small holes in the skull, known as burr holes) and the hematoma before evacuation and irrigation. The image on the right shows the hematoma after removal, with a drain placed in the remaining cavity, which will stay in place for 2 days.
Drains may be:
- One or two
- Passive drainage into collection bags
The operation can be done under:
- General anesthesia
- Or local anesthesia with sedation
Bilateral hematomas are usually treated on both sides, often in one session.
Post-operative Care
After surgery:
- Patients usually wake up immediately if they were awake before
- They lie flat for 1–2 days
- Receive supplemental oxygen
This:
- Helps the brain re-expand – This ensures that the brain fills the space previously occupied by the hematoma, preventing fluid from collecting in the empty gap.
- Reduces recurrence – Keeping the patient flat and well-oxygenated helps stabilize the brain’s position and significantly lowers the risk of the bleeding coming back.
- Reduces pneumocephalus (air in the skull) – This helps the body naturally absorb any air trapped inside the skull during surgery, which is essential for reducing headaches and pressure.
Drains are usually removed after 2 days.
Some surgeons obtain a control CT scan; others do not if the patient is neurologically well and significant drainage has occurred.
Early CTs often still show residual fluid — this is not dangerous if the brain is decompressed.
Removing 50% of the volume is often sufficient.
Twist-Drill Drainage
Twist-drill drainage is a minimally invasive technique used in selected patients with chronic subdural hematoma.
Instead of creating a larger burr hole, the surgeon makes a very small opening in the skull using a narrow twist drill. A soft catheter is then inserted into the subdural space to allow slow drainage of the liquefied hematoma.
This procedure is typically performed under local anesthesia.
In carefully selected, neurologically stable patients — particularly very elderly or medically fragile individuals — it may be performed in a monitored hospital setting without transferring the patient to a full operating theater.
Advantages:
- Less invasive
- Can avoid general anesthesia
- Shorter procedural time
Limitations:
- Slightly higher recurrence rate compared to burr-hole drainage
- Less effective in septated or organized hematomas
For this reason, twist-drill drainage is generally reserved for selected cases rather than being the standard first-line surgical technique. Postoperative care after twist-drill drainage is generally similar to that following burr-hole surgery.
When Craniotomy Is Needed
Craniotomy is rare and reserved for:
- Septated (compartmentalized) hematomas – This means the blood is trapped in several separate „pockets“ or compartments. A simple drain cannot reach them all, so a craniotomy is necessary to open and clean each pocket directly. This is rare.
- Multiple recurrences – If the hematoma keeps coming back after being drained, a craniotomy is performed to find the underlying cause, stop any persistent slow leaks, and ensure the space is thoroughly cleared.
In those cases, the surgeon may remove the thick outer capsule to prevent further bleeding.
Recurrence and Modern Treatment
If the hematoma recurs, an effective modern option is:
Middle Meningeal Artery (MMA) Embolization
This is a modern, minimally invasive procedure used to treat chronic or recurring subdural hematomas by „cutting off“ their blood supply.
The goal: By cutting off the „fuel supply“ to the membrane, the procedure prevents the hematoma from refilling (re-accumulation) and allows the body to naturally absorb the remaining blood over time.
How it is performed: The doctor inserts a thin, flexible tube called a catheter into an artery in the groin (leg). Using real-time X-ray guidance, the catheter is carefully advanced through the vascular system all the way up to the small arteries in the head that „feed“ the hematoma membrane. Tiny particles or a special medical „glue“ are injected through the catheter to permanently block these small vessels.
Seizures and Epilepsy in Chronic Subdural Hematoma
Chronic subdural hematoma can be associated with epileptic seizures and the development of epilepsy.
The mechanism is not the hematoma itself, but prolonged cortical irritation, inflammatory membrane formation, and hemosiderin deposition on the brain surface.
Seizures may occur before diagnosis, after surgical evacuation, or weeks to months later.
In elderly patients, epileptic seizures are often subtle and may be misinterpreted as confusion or transient neurological events.
Surgical evacuation usually reduces seizure risk, but in some cases, persistent cortical changes may lead to chronic epilepsy requiring long-term management.
Prognosis
When chronic subdural hematoma is recognized and treated before severe brain compression or prolonged neurological decline, the prognosis is often good, even in elderly patients. Outcome depends mainly on preoperative neurological status, age, frailty, anticoagulant use, recurrence risk, and associated brain injury.
Red Flags — When to Seek In-Person Medical Evaluation for Chronic Subdural Hematoma
Patients and family members should seek urgent in-person medical evaluation with brain imaging (CT or MRI) if a person with known or suspected chronic subdural hematoma develops sudden or worsening confusion, increasing drowsiness, new weakness or speech difficulty, severe or rapidly worsening headache, seizures, repeated vomiting, or a sudden neurological decline after a period of apparent stability. These signs may indicate dangerous brain compression and require immediate hospital assessment.
Frequently Asked Questions About Chronic Subdural Hematoma
What is a chronic subdural hematoma?
A chronic subdural hematoma is a slowly growing collection of old blood between the brain and the dura, the firm covering around the brain. It often develops weeks after a minor or forgotten head injury. At first, the bleeding may be small and cause no symptoms. Over time, a membrane can form around the collection and slowly leak fluid or blood, allowing the hematoma to enlarge. The main danger is not the blood itself, but the pressure it creates on the brain. When the collection becomes large enough, it can compress brain tissue, shift midline structures, and cause headache, confusion, weakness, speech problems, drowsiness, or sudden neurological deterioration.
Why can chronic subdural hematoma appear weeks after a mild head injury?
In chronic subdural hematoma, the first bleeding is often very small. The patient may feel well, and the injury may seem insignificant or even be forgotten. The problem develops later because old blood can remain in the subdural space instead of being fully absorbed. Over time, inflammatory membranes form around the collection. These membranes contain fragile new blood vessels that may leak repeatedly. Because of this, the hematoma can slowly enlarge days or weeks after the original injury. This delayed growth explains why an older person may appear stable after a fall, but later develop confusion, headache, weakness, imbalance, or drowsiness.
Can a person have chronic subdural hematoma without remembering a head injury?
Yes. Many patients with chronic subdural hematoma do not remember a clear head injury. This is especially common in older adults, where even a mild bump, a small fall, or sudden head movement can stretch fragile bridging veins. Brain atrophy creates more space between the brain and skull, so a small bleed may not cause immediate symptoms. Because there is more room for the blood collection to grow, the patient may feel normal for days or weeks. The first noticeable signs may be headache, memory problems, confusion, gait instability, speech difficulty, or weakness, even though the original trauma seemed minor or was never recognized.
Why are elderly patients at higher risk for chronic subdural hematoma?
Elderly patients are at higher risk because the brain gradually shrinks with age, creating a larger subdural space inside the skull. This stretches the bridging veins that run between the brain surface and the dura, making them more vulnerable to tearing after minor trauma. The enlarged space also allows blood to collect without causing immediate symptoms, so the hematoma can grow silently. Blood thinners, antiplatelet drugs, clotting disorders, alcohol dependence, and previous brain atrophy further increase the risk. This is why chronic subdural hematoma is one of the most common neurosurgical conditions in older adults and why new confusion or weakness after a fall should not be ignored.
What symptoms should raise suspicion of a chronic subdural hematoma?
Chronic subdural hematoma should be suspected when symptoms appear gradually after a fall, minor head injury, or even without a remembered trauma. Warning signs include new or worsening headache, confusion, memory problems, personality change, drowsiness, speech difficulty, weakness on one side of the body, imbalance, seizures, or reduced alertness. In elderly patients, the condition can sometimes look like dementia, stroke, depression, or general decline. The key point is progression. If an older person becomes slower, more confused, weaker, sleepier, or less steady over days or weeks, brain imaging with CT or MRI is usually needed to rule out chronic subdural hematoma.
Why do some patients with chronic subdural hematoma suddenly get worse?
Some patients with chronic subdural hematoma worsen suddenly because the brain can compensate only up to a point. At first, the hematoma may enlarge slowly while symptoms remain mild, especially in older patients with brain atrophy and more intracranial reserve space. Once that reserve is exhausted, even a small additional increase in volume can produce a much larger effect on brain compression. Midline shift may increase, blood flow can be impaired, and the patient may rapidly become drowsy, confused, weak, or unable to speak normally. This sudden decline does not always mean the condition was missed; it reflects the delayed and progressive nature of chronic subdural hematoma.
Is CT scan enough to diagnose chronic subdural hematoma?
In most cases, CT scan is enough to diagnose chronic subdural hematoma. CT shows the size of the collection, its density, whether it is one-sided or bilateral, how much it compresses the brain, and whether there is midline shift. These findings are usually sufficient for deciding whether observation, repeat imaging, or surgery is needed. MRI can be useful when CT findings are unclear, when the hematoma has several compartments, when membranes need better evaluation, or when symptoms do not match the CT appearance. However, in everyday neurosurgical practice, CT is usually the first and most important test because it is fast, available, and very informative.
Does every chronic subdural hematoma require surgery?
No. Not every chronic subdural hematoma requires surgery. Small collections that do not significantly compress the brain and do not cause neurological symptoms can sometimes be monitored with repeat CT or MRI scans. Conservative treatment may also include careful clinical observation and adjustment of blood-thinning medication when appropriate. Surgery is usually recommended when the hematoma is large, causes midline shift, produces weakness, confusion, speech problems, drowsiness, seizures, or progressive symptoms. The decision is not based only on the scan, but on the combination of imaging, symptoms, age, clotting status, medication use, and how quickly the patient is changing.
Can chronic subdural hematoma be treated without surgery?
Yes, selected chronic subdural hematomas can be treated without surgery. This is usually considered when the hematoma is small, symptoms are absent or mild, and there is no significant brain compression. The patient must be monitored closely because the collection can enlarge later. Treatment may include repeat imaging, neurological observation, and correction of factors that increase bleeding risk, such as anticoagulant or antiplatelet medication when medically safe. In some stable patients, middle meningeal artery embolization may be considered to reduce the risk of growth or recurrence. However, if symptoms progress or the brain is clearly compressed, surgical drainage is usually the safer option.
What type of surgery is most commonly used in chronic subdural hematoma?
The most common operation for chronic subdural hematoma is burr-hole drainage. The surgeon makes one or two small openings in the skull, enters the subdural space, irrigates the old blood, and usually leaves a drain for one or two days. The aim is to relieve pressure on the brain and allow the brain to re-expand. The operation can often be performed under general anesthesia, and in selected fragile patients under local anesthesia with sedation. Twist-drill drainage is a less invasive option for selected cases. Craniotomy, a larger opening of the skull, is rarely needed and is usually reserved for organized, septated, or repeatedly recurrent hematomas.
Why don’t surgeons always remove all the blood in chronic subdural hematoma?
In chronic subdural hematoma, the goal of surgery is to relieve pressure on the brain, not necessarily to remove every visible drop of old blood. Even after successful drainage, early CT scans may still show residual fluid or air in the subdural space. This does not automatically mean the operation failed. If the brain is decompressed, the midline shift improves, and the patient is neurologically better, partial evacuation may be enough. Trying to remove every remnant aggressively can increase surgical risk, especially if membranes are attached to delicate brain surfaces. The body can gradually absorb remaining fluid once the dangerous pressure has been relieved.
When is craniotomy needed in chronic subdural hematoma?
Craniotomy is rarely needed in chronic subdural hematoma. Most cases are treated with burr-hole drainage because the hematoma is liquefied and can be drained through small openings. Craniotomy becomes necessary when the hematoma is organized, thick, or divided into several compartments by membranes, so a simple drain cannot empty it properly. It may also be considered after multiple recurrences, when the surgeon needs to remove a thick capsule or identify the source of persistent bleeding. Because craniotomy is a larger operation, it is reserved for selected cases where less invasive drainage is unlikely to work or has already failed.
Can chronic subdural hematoma come back after surgery?
Yes. Chronic subdural hematoma can come back after surgery, although most patients improve after the first drainage. Recurrence is more likely in elderly patients, in those with marked brain atrophy, bilateral hematomas, clotting problems, continued use of blood thinners, or persistent inflammatory membranes. A recurrent hematoma does not always mean that the first operation was poorly performed. The membrane around the hematoma can continue to leak, allowing fluid or blood to re-accumulate. Treatment may include repeat drainage, correction of bleeding risk factors, or middle meningeal artery embolization, which targets the blood supply of the membrane and may reduce further recurrence.
What is middle meningeal artery embolization for chronic subdural hematoma?
Middle meningeal artery embolization is a minimally invasive endovascular procedure used in selected patients with chronic or recurrent subdural hematoma. A thin catheter is introduced through an artery, usually from the groin or wrist, and guided under X-ray control to the small arteries that feed the hematoma membrane. Tiny particles or liquid embolic material are then used to block these vessels. The purpose is not to drain the hematoma directly, but to reduce the membrane’s blood supply and prevent further leakage. This can help the remaining blood collection shrink over time and may lower the risk of recurrence after surgery.
Is embolization a replacement for surgery on chronic subdural hematoma?
Middle meningeal artery embolization is not always a replacement for surgery in chronic subdural hematoma. If the hematoma is large, compresses the brain, or causes significant weakness, drowsiness, speech problems, or worsening neurological symptoms, surgical drainage is usually needed first to relieve pressure quickly. Embolization may be used as an additional treatment to reduce recurrence risk after surgery, or in selected stable patients when the hematoma is not causing dangerous compression. It can also be useful when the hematoma has returned after previous drainage. The decision depends on symptoms, CT findings, age, recurrence risk, and the urgency of brain decompression.
Can chronic subdural hematoma cause seizures or epilepsy?
Yes. Chronic subdural hematoma can cause seizures in some patients. The mechanism is usually irritation of the brain surface by prolonged compression, blood-breakdown products, inflammatory membranes, or hemosiderin deposits. Seizures may occur before diagnosis, after surgical drainage, or later during recovery. In elderly patients they are not always dramatic; they may appear as brief confusion, staring, speech arrest, unusual behavior, or transient weakness. Surgical evacuation often reduces irritation and lowers the risk, but some patients may need anti-seizure medication, especially if seizures have already occurred or if there are persistent cortical changes. Any new seizure requires urgent medical evaluation.
What is the prognosis after treatment of chronic subdural hematoma?
The prognosis after treatment of chronic subdural hematoma is often good, even in elderly patients, when the condition is recognized and treated in time. Many patients improve quickly after the brain is decompressed, especially if they were awake and had reversible symptoms such as confusion, headache, imbalance, or mild weakness. Outcome is worse when treatment is delayed until severe drowsiness, major brain compression, seizures, or serious medical complications occur. Prognosis also depends on age, frailty, brain atrophy, anticoagulant use, recurrence risk, and other illnesses. The key point is that chronic subdural hematoma is often treatable, but timing and careful follow-up matter.
Why might a family need a second opinion for chronic subdural hematoma?
A second opinion can be useful when a family is unsure whether chronic subdural hematoma should be observed, drained, re-imaged, or treated with embolization. It is especially helpful when symptoms are changing, CT findings are difficult to understand, doctors disagree about timing, the patient is elderly or on blood thinners, or the hematoma has recurred after surgery. Families often need a clear explanation of how urgent the situation is, whether burr-hole drainage or craniotomy is being considered, and what recovery may realistically look like. A neurosurgical second opinion does not replace emergency care, but it can clarify decisions when the situation is complex.
Can chronic subdural hematoma be evaluated through an online neurosurgical consultation?
Yes. Chronic subdural hematoma can often be evaluated through an online neurosurgical consultation if CT or MRI images and medical reports are available. The purpose is to review the size of the hematoma, brain compression, midline shift, symptoms, age, medication use, and recurrence risk, and then explain whether observation, repeat imaging, surgery, or embolization appears reasonable. Online consultation is especially useful for second opinions and family decision-making. However, if the patient is suddenly more confused, drowsy, weak, unable to speak normally, vomiting repeatedly, or having seizures, urgent in-person hospital evaluation is required.
Learn more about neurosurgery second opinions
.
Further Reading (Patient-Friendly References)
Reliable sources for patients and families to learn more about chronic subdural hematoma.
- NHS (UK): Subdural haematoma — overview, symptoms, and treatment
- Cleveland Clinic (USA): Subdural hematoma overview (includes chronic form)
- Johns Hopkins Medicine (USA): Burr holes and subdural hematoma treatment
- PubMed: ARISE I Consensus for Chronic Subdural Hematoma (Stroke, 2024) (patient-friendly abstract)
- PubMed: MMA Embolization for Chronic Subdural Hematoma (NEJM 2025) (research summary with clinical context)