Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Zeljko Kojadinovic, MD, PhD — neurosurgeon and chronic pain specialist
Last medically reviewed: June 10, 2026
Who this page is for
This page is for patients who have persistent pain after surgery — especially pain that started or became worse after an operation and has lasted longer than the expected healing period, usually 3 months or more.
It is especially relevant after procedures such as gallbladder removal, thoracic or lung surgery, breast surgery, inguinal hernia repair, spinal surgery, hysterectomy, C-section, sternotomy, amputation, or other operations near important sensory nerves. Pain may be burning, stabbing, electric, pressure-like, radiating, or located near a scar, even when MRI, CT, ultrasound, blood tests, or organ-focused evaluations are normal.
In many patients, the real pain generator is not recurrent disease, but nerve irritation, nerve injury, scar-tissue entrapment, neuroma formation, muscle spasm, altered mechanics, or mixed nerve–musculoskeletal pain. For example, pain after gallbladder surgery may come from intercostal nerve irritation or upper abdominal wall nerves, while groin pain after hernia repair may involve ilioinguinal, iliohypogastric, or genitofemoral nerves.
This page explains how a focused pain-source assessment can help identify whether persistent postsurgical pain is nerve-related, scar-related, muscle-related, spine-referred, organ-related, or mixed — and when a targeted telehealth pain consultation may help guide the next treatment step.
When patients usually contact us for persistent pain after surgery
Patients usually contact us when pain continues after the expected healing period and repeated tests do not clearly explain the symptoms. This is common after gallbladder removal, thoracic or lung surgery, breast surgery, inguinal hernia repair, spinal surgery, C-section, hysterectomy, sternotomy, amputation, or other operations performed close to sensory nerves.
- Pain has lasted for weeks or months after surgery, especially longer than 3 months
- MRI, CT, ultrasound, blood tests, or organ-focused evaluations are normal or do not explain the pain
- Pain is burning, stabbing, electric, shooting, pressure-like, or radiating from the scar or operated region
- There is suspected nerve pain after gallbladder removal or gallbladder surgery
- Upper abdominal or right-sided pain persists after cholecystectomy, but liver, bile duct, stomach, or imaging tests are reassuring
- Pain after thoracic surgery, lung surgery, wedge resection, or sternotomy follows the rib line or worsens with breathing, coughing, movement, or pressure
- Groin, genital, lower abdominal, or inner thigh pain persists after inguinal hernia repair, C-section, hysterectomy, or pelvic surgery
- Back or leg pain persists after spine surgery despite no clear recurrent disc herniation or surgical complication
- Pain is located near a scar, becomes worse when the scar is pressed or stretched, or feels like a trapped nerve
- Different doctors give different explanations, and it is unclear whether the pain is nerve-related, scar-related, muscle-related, spine-referred, organ-related, or mixed
- Standard painkillers, antibiotics, stomach medication, anti-inflammatory treatment, or repeated reassurance have not solved the problem
- The patient wants to know whether further imaging, nerve blocks, medication changes, injections, rehabilitation, or another specialist evaluation makes sense
In these situations, a focused pain-source assessment can help determine whether persistent postsurgical pain is coming from a nerve, scar tissue, neuroma, muscle, fascia, joint, spine referral, an organ-related cause, or a mixed mechanism: Request a Postsurgical Pain Second Opinion
Contents
- Who This Page Is For
- General About Postsurgical Pain
- Specific Pain Syndromes
- Post-thoracotomy Pain Syndrome
- Post-mastectomy Pain Syndrome
- Pain After Cholecystectomy
- Pain After Hernia Repair
- Post-sternotomy Pain Syndrome
- Failed Back Surgery Syndrome
- Post-Hysterectomy/Orchiectomy Pain
- Post-cesarean Pain Syndrome
- Phantom/Neuroma Pain After Amputation
- FAQs About Postsurgical Pain
- Start Telehealth Consultation Now
- Related Topics and Resources
General About Postsurgical Pain
Many patients continue to experience pain after surgery, sometimes very similar or even identical to what they had before the operation. Examples include pain after gallbladder removal, spinal disc surgery, breast surgery, thoracic surgery, or inguinal hernia repair. Typical situations include “chronic pain after surgery,” “pain after surgery with a normal MRI,” “persistent pain after gallbladder removal,” “chest pain after thoracic surgery,” and “groin pain after hernia repair.”
The cause may be a recurrence of the original condition, but in many cases surgery itself can trigger new musculoskeletal or nerve pain that mimics the previous illness. Even a small surgical incision, or an apparently “simple” endoscopic procedure, may be enough to irritate or injure a nearby nerve, muscle, fascial band, or ligament. This can lead to problems such as inflammation, spasm, scar tissue compression, or neuropathic changes that evolve into chronic pain.
If this is not recognized, patients are often sent for repeated imaging tests — MRI, CT, or ultrasound — or even undergo unnecessary re-operations. Yet in most cases these nerve-related or musculoskeletal causes cannot be seen on scans. Postsurgical musculoskeletal or nerve-origin pain can only be treated effectively once the exact anatomical structure responsible has been identified, as well as contributing factors causing and maintaining irritation in them.
The key first step in pain medicine is not labeling the disease, but pinpointing the specific anatomical structure (nerve, muscle, tendon, fascia, joint) that is the true pain generator. Only a specialist familiar with pain anatomy can systematically evaluate all possible causes in the operated region and confirm which one is responsible. Many patients are told that their pain cannot be explained, is untreatable, or is “psychological.” In reality, the problem usually lies in the fact that a precise diagnostic process was never carried out.
Modern imaging alone is rarely enough. What matters most is a detailed patient history combined with targeted physical tests that provoke or relieve the pain. This evaluation can be performed either in the doctor’s office or through an online consultation (telemedicine, telehealth consultation, video visit, video call, video consultation, or online second opinion).
Telemedicine plays an essential role in this process. For more than 10 years, online consultations have been successfully used in pain medicine. During a video consultation, the medical documentation is first reviewed, followed by a detailed discussion in which the doctor explores all aspects of your pain through targeted questions, movement tests, and patient-performed pressure tests. This makes it possible to identify which structure is responsible and which pathological process is involved, allowing for a more precise choice of therapy. In most cases, patients notice improvement within 10 days, and long-term resolution is expected within 6 weeks, after which treatment can be tapered. Follow-up is usually available during this period for additional questions.
If medications do not help, minimally invasive pain diagnostics may be indicated. This step-by-step method combines diagnostic and therapeutic procedures: by selectively testing and blocking one structure after another (nerve, joint, muscle, ligament) the true pain generator can be confirmed and treated at the same time.
What Makes This Consultation Different?
If you have pain after surgery and all tests show no recurrent illness, the true source of your pain may have been overlooked. When labs and imaging are normal, my approach starts by looking for a focal nerve irritation produced by the previous surgery.
During the video consultation, I review your medical documentation, ask highly targeted questions, and guide you through simple motion and pressure tests that you perform yourself. This helps locate the exact anatomical source of your pain — by reproducing or relieving it through specific actions.
This functional assessment has the same diagnostic value as an in-person physical exam. Effective treatment begins only after the true cause of pain is identified — and that starts with a conversation guided by a physician who understands pain anatomy and knows exactly what structures can generate pain in your case.
This approach can lead to improvement even in long-term, chronic pain that mimics organ disease.
In the following text, we list examples of postoperative pain syndromes.
Post-thoracotomy Pain Syndrome
Occurs after thoracic surgery. Most often involves injury or irritation of the intercostal nerves. Pain is typically burning or stabbing along the rib, sometimes mimicking cardiac or pulmonary pain.
Post-mastectomy Pain Syndrome
After breast surgery, pain is usually due to injury of the intercostobrachial nerve or small cutaneous nerves trapped in the scar. Pain radiates into the armpit and inner upper arm and is described as burning, pulsating, or electric.
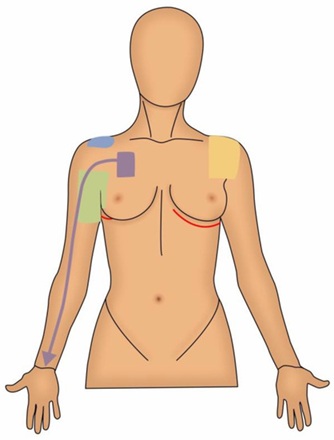
Illustration of Post-mastectomy Pain Syndrome.
Post-cholecystectomy Pain Syndrome
Pain can persist after gallbladder removal even when imaging shows no abnormalities. This often involves the intercostal nerves T7–T9 or branches of the celiac plexus. The pain is often perceived as coming from the liver or stomach but is actually neuropathic.

Illustration of Post-cholecystectomy Pain Syndrome
Pain After Inguinal Hernia Repair
Chronic groin pain is common after hernia surgery. Nerves most often involved are the ilioinguinal, iliohypogastric, and genitofemoral nerves. Pain can remain localized in the groin or radiate to the genital region or inner thigh.
Post-sternotomy Pain Syndrome
After cardiac surgery through sternotomy, pain can remain long-term. It usually involves intercostal and supraclavicular nerves or neuroma formation in the sternum. Pain may be dull or burning, often worse with breathing or arm movements.
Post-laminectomy Syndrome (Failed Back Surgery Syndrome)
After spinal surgery, a subgroup of patients develop chronic pain due to spinal nerve root irritation, scar fibrosis, or myofascial sources. Pain may be local in the back or radiating down the leg (radicular pain). See more about pain after lumbar discectomy.

Illustration of Post-laminectomy syndrome.
Post-hysterectomy and Post-orchiectomy Pain Syndromes
Chronic pelvic pain may appear after gynecological or urological surgery. Nerves involved include the pudendal, ilioinguinal, and iliohypogastric nerves. Pain is neuropathic, localized in the pelvis, groin, or genital region.
Post-cesarean Pain Syndrome
Chronic lower abdominal pain may persist after cesarean section, usually due to injury to the ilioinguinal and iliohypogastric nerves. Pain is stabbing or burning around the scar.
Post-amputation Pain Syndrome (Phantom Pain and Neuroma Pain)
After limb amputation, patients often feel pain in the missing limb. This is caused by a combination of neuroma formation at the stump and central sensitization in the nervous system. Pain can be severe and described as electric, stabbing, or pulsating.
Start Your Telehealth Consultation with a Pain Specialist
If your pain treatment has failed or you’re unsure what to do next — don’t wait. A detailed telehealth consultation can help identify the exact cause of your pain, even if previous therapies didn’t work.
- ✔ First, send a short message describing your problem
- ✔ You’ll receive a reply within 24 hours if and how we can help — including the consultation cost and a suggested time
- ✔ Only then, you can send your medical documentation
- ✔ The video consultation is followed by a written report and follow-up questions (up to 10 days)
- ✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Consultation fees typically range from $180–250, depending on the complexity of your case.
This is within the usual range for specialist telehealth consultations worldwide. Thousands of patients worldwide already use telehealth consultations for second opinions — it’s safe, accepted, and effective.
Before contacting us, please read our Privacy Policy and Terms of Use.
FAQs — Most Common Questions Patients Ask About Pain After Surgery
How long is pain normal after surgery, and when is it considered chronic postsurgical pain?
Some pain is expected after surgery, especially during the first days or weeks while tissues heal. Pain becomes more concerning when it continues beyond the usual healing period, does not steadily improve, or remains significant after 3 months. Chronic postsurgical pain is not simply “slow healing.” It may suggest that the original pain source was not fully corrected, or that the operation created a new pain generator such as nerve irritation, scar-tissue entrapment, neuroma formation, muscle spasm, fascia irritation, altered mechanics, or spine-related referral. The key question is not only how long the pain has lasted, but whether its pattern fits normal healing or a persistent anatomical pain source.
Why do I still have pain after surgery if my MRI, CT, ultrasound, or blood tests are normal?
Normal MRI, CT, ultrasound, or blood tests do not exclude nerve-related or musculoskeletal postsurgical pain. These tests are useful for detecting infection, bleeding, recurrence, organ problems, fractures, large structural lesions, or major complications. However, they often cannot show irritation of small sensory nerves, scar-related tethering, neuroma formation, muscle spasm, fascia restriction, ligament irritation, or altered movement mechanics. This is why many patients are told that “everything looks normal” even though their pain remains real and reproducible. When imaging is normal, the next step is often functional pain-source assessment: mapping pain location, triggers, radiation, scar sensitivity, movement patterns, and pressure points.
What are the main causes of persistent pain after surgery?
Persistent pain after surgery may come from several different mechanisms. The original disease may have recurred or may not have been the true pain source in the first place. Surgery can also irritate or injure nearby sensory nerves, create scar-tissue entrapment, form a painful neuroma, trigger muscle spasm, change local mechanics, or sensitize the nervous system. In some patients, pain is mixed: partly nerve-related, partly muscle-related, partly spine-referred, and partly scar-related. Treatment fails when all postsurgical pain is treated as inflammation, infection, anxiety, or recurrence. The most important step is to identify the dominant pain generator in the operated region.
Can nerve damage after surgery cause burning, stabbing, electric, or radiating pain?
Yes. Burning, stabbing, electric, shooting, tingling, numb, hypersensitive, or radiating pain often suggests a neuropathic component. This can occur when a sensory nerve is stretched, compressed, cut, trapped in scar tissue, irritated by inflammation, or forms a neuroma. The pain may start near the incision and travel along a predictable nerve path, or it may appear in a nearby region such as the ribs, groin, abdomen, pelvis, breast, inner thigh, or leg. Nerve-related pain may also be triggered by pressure on the scar, clothing contact, movement, coughing, breathing, or posture. Identifying the involved nerve is essential for targeted treatment.
Can scar tissue or a neuroma cause pain months after surgery?
Yes. Scar tissue can irritate, tether, or compress small sensory nerves near the incision. A neuroma can form when a cut or injured nerve ending becomes painful during healing. These problems may cause burning, electric, stabbing, pulling, or pressure-sensitive pain months after surgery. A typical clue is pain that starts near the scar, becomes worse when the scar is pressed or stretched, or radiates in a specific direction from the incision. Standard imaging may not show this clearly. Many cases can be treated without reoperation using medication, desensitization, local treatment, nerve blocks, injections, or targeted rehabilitation, depending on the exact pain generator.
Can nerve pain happen after gallbladder removal?
Yes. Nerve pain can occur after gallbladder removal, even when liver tests, bile duct evaluation, ultrasound, CT, or other organ-focused tests are reassuring. After cholecystectomy, persistent right upper abdominal pain may come from intercostal nerve irritation, upper abdominal wall nerves, scar sensitivity, muscle spasm, fascia irritation, or thoracic spinal referral. The pain may be burning, stabbing, band-like, pressure-like, or sensitive to movement and touch. It may feel as if it comes from the liver, stomach, or gallbladder area, even when the organ problem has already been treated. This is why pain-source mapping is important when routine tests are normal.
What causes nerve pain after gallbladder surgery or cholecystectomy?
Nerve pain after gallbladder surgery may be caused by irritation of intercostal nerves, small abdominal wall sensory branches, scar-related nerve entrapment, trocar-site sensitivity, muscle spasm, or thoracic root referral. Laparoscopic surgery uses small incisions, but even small entry points can irritate nerves, fascia, or muscles. Pain may be felt under the right ribs, near the incision, across the upper abdomen, or toward the back. If the pain changes with pressure, twisting, deep breathing, coughing, or posture, a nerve or chest-wall/abdominal-wall source becomes more likely. This does not exclude bile duct or digestive causes, but it explains why normal organ tests may not end the pain.
Can intercostal nerve pain after gallbladder surgery mimic liver, stomach, or bile duct pain?
Yes. Intercostal nerves from the lower thoracic levels supply the lower chest wall and upper abdominal wall. When these nerves are irritated after gallbladder surgery, pain can be perceived near the right upper abdomen, under the ribs, or toward the back. Patients may feel that the pain is coming from the liver, stomach, bile duct, or the area where the gallbladder used to be. A nerve source is more likely when pain is burning, stabbing, band-like, worse with movement or pressure, or reproducible at a small tender point. This pattern requires a different evaluation from repeated organ-focused testing alone.
Can phrenic nerve or vagus nerve damage explain pain after gallbladder removal?
Phrenic or vagus nerve injury is sometimes suspected by patients after gallbladder surgery, but persistent postsurgical pain is more commonly related to local abdominal wall nerves, intercostal nerve irritation, scar sensitivity, muscle spasm, or thoracic referral. The phrenic nerve can be involved in referred shoulder discomfort after laparoscopy, especially early after surgery, but long-lasting focal right upper abdominal pain usually needs a broader pain-source assessment. Vagus nerve damage is not the usual explanation for localized scar-sensitive or movement-sensitive pain. The exact pattern matters: location, radiation, relation to breathing, pressure, meals, posture, and previous test results must be reviewed together.
Can pain after lung surgery, wedge resection, or thoracotomy have a nerve origin?
Yes. Pain after lung surgery, wedge resection, thoracoscopy, or thoracotomy often has a nerve component because intercostal nerves run along the ribs and can be stretched, compressed, irritated, or injured during chest surgery. Pain may follow the rib line, wrap around the chest, or feel burning, stabbing, electric, tight, or hypersensitive. It may worsen with deep breathing, coughing, trunk rotation, arm movement, or pressure between the ribs. This can mimic heart or lung pain even when postoperative imaging is reassuring. Treatment depends on identifying whether the dominant source is intercostal neuralgia, rib/chest-wall pain, scar entrapment, muscle spasm, or mixed pain.
What is post-thoracotomy pain syndrome?
Post-thoracotomy pain syndrome is persistent pain after surgery through the chest wall. It may occur after open thoracotomy, thoracoscopy, lung surgery, rib surgery, or other procedures near the intercostal nerves. The pain is often burning, stabbing, tight, or band-like and may follow the rib line from the back toward the front of the chest. The most common mechanism is irritation or injury of the intercostal nerves, but scar sensitivity, rib mechanics, muscle spasm, and thoracic spinal referral may also contribute. Because breathing and rib movement can provoke symptoms, patients may fear heart or lung disease even when those causes have been excluded.
What is post-mastectomy pain syndrome and intercostobrachial neuralgia?
Post-mastectomy pain syndrome is chronic pain after breast surgery, lymph node surgery, or procedures near the armpit and chest wall. A common contributor is intercostobrachial neuralgia, caused by irritation or injury of the intercostobrachial nerve. Pain may be felt in the breast area, armpit, inner upper arm, chest wall, or scar region. It may be burning, electric, numb, hypersensitive, or painful to clothing and touch. This pain is different from simple wound healing and may persist even after cancer treatment is complete and imaging is reassuring. Mapping the pain distribution helps distinguish nerve pain from shoulder, chest wall, lymphatic, or spine-related causes.
Why can groin, genital, or inner thigh pain persist after inguinal hernia repair?
Groin, genital, or inner thigh pain after inguinal hernia repair may persist when ilioinguinal, iliohypogastric, or genitofemoral nerves are irritated, compressed, trapped in scar tissue, affected by mesh, or sensitized after surgery. The pain may remain in the groin or radiate toward the testicle, labia, pubic area, lower abdomen, or inner thigh. It may be burning, stabbing, pulling, electric, or worse with standing, walking, bending, hip movement, coughing, or pressure near the scar. Normal ultrasound or CT may not show the nerve source. Treatment depends on identifying the involved nerve and whether pain is neuropathic, scar-related, mechanical, or mixed.
Can C-section, hysterectomy, or pelvic surgery cause chronic nerve pain?
Yes. C-section, hysterectomy, pelvic surgery, and lower abdominal operations can irritate ilioinguinal, iliohypogastric, genitofemoral, pudendal, or other pelvic sensory nerves. Pain may appear near the scar, lower abdomen, groin, pelvis, genital region, or inner thigh. It may feel burning, stabbing, pulling, electric, or pressure-like and may worsen with sitting, standing, abdominal movement, intercourse, bowel activity, clothing pressure, or scar stretching. Because pelvic organs may appear normal, patients are sometimes told that nothing is wrong. A pain-source assessment looks beyond organs and evaluates nerves, scar mechanics, pelvic floor muscles, spine referral, and mixed mechanisms.
Can pain after spine surgery continue even if there is no recurrent disc herniation?
Yes. Pain after spine surgery can continue even when MRI does not show recurrent disc herniation or a clear surgical complication. Possible sources include nerve root irritation, epidural scar sensitivity, facet joint pain, sacroiliac joint pain, myofascial pain, altered movement mechanics, peripheral nerve entrapment, or central sensitization. In some patients, the original pain generator was not fully identified before surgery, so pain persists even after technically successful decompression. The important question is whether current pain is the same as before surgery or has a new pattern. Treatment depends on identifying the active generator now, not only reviewing the operation result.
Can post-sternotomy pain after heart surgery come from nerves or the chest wall?
Yes. Pain after sternotomy can come from the sternum, costosternal joints, intercostal nerves, supraclavicular nerves, scar tissue, muscle spasm, or altered chest wall mechanics. The pain may be dull, burning, tight, sharp, pressure-sensitive, or worse with deep breathing, coughing, arm movement, or pressure over the sternum. Because the operation was performed for heart disease, patients often fear that any chest pain means a new cardiac problem. New or concerning chest pain still needs urgent cardiac evaluation. However, when cardiac causes are excluded and pain remains reproducible at the sternum or chest wall, a nerve–musculoskeletal source should be considered.
Is postsurgical pain neuropathic or inflammatory, and how can I tell?
Neuropathic postsurgical pain often feels burning, electric, shooting, stabbing, tingling, numb, hypersensitive, or radiating along a nerve path. It may be triggered by light touch, clothing, scar pressure, movement, coughing, breathing, or posture. Inflammatory pain is more often aching, swollen, warm, and linked to tissue irritation or healing. Many patients have a mixed pattern: nerve irritation plus muscle spasm, scar sensitivity, joint strain, or inflammation. The distinction matters because treatment is different. Anti-inflammatory medication may not help nerve pain, while neuropathic medication, nerve blocks, scar treatment, desensitization, or targeted rehabilitation may be more appropriate.
What treatments help when standard painkillers do not relieve postsurgical nerve pain?
When standard painkillers do not help postsurgical nerve pain, treatment should be guided by the suspected pain generator. Options may include neuropathic pain medication, local scar desensitization, correction of posture and movement triggers, targeted physical therapy, trigger point treatment, topical medication, diagnostic nerve blocks, therapeutic nerve blocks, peripheral nerve injections, or treatment of associated muscle and fascia irritation. If a neuroma, scar entrapment, or focal nerve source is suspected, local diagnostic procedures can help confirm the source before more invasive treatment is considered. Reoperation is usually not the first step unless there is a clear structural reason.
When are nerve blocks useful for pain after surgery?
Nerve blocks are useful when the pain pattern suggests a specific nerve or group of nerves. They can have two purposes. Diagnostically, a nerve block can test whether numbing a suspected nerve reduces the patient’s typical pain. Therapeutically, it may reduce nerve irritation and help break the pain cycle, especially when combined with medication and rehabilitation. Examples include intercostal nerve blocks after thoracic or gallbladder surgery, ilioinguinal or genitofemoral blocks after hernia or pelvic surgery, and targeted peripheral nerve blocks near scars or neuromas. A block should be chosen based on anatomy and pain mapping, not used randomly.
How can a video consultation help with persistent pain after surgery?
A video consultation can help by reviewing the operation type, pain timeline, imaging, reports, medications, scar location, pain distribution, and triggers. The patient can show where the pain starts, where it radiates, and which movements or pressure points reproduce it. Guided self-examination may include gentle scar pressure, trunk movement, breathing-related tests, hip or spine movements, and mapping of numbness or hypersensitivity. This helps determine whether pain is more likely nerve-related, scar-related, muscle-related, spine-referred, organ-related, or mixed. Video consultation does not replace urgent care, but it is useful for chronic, already investigated postsurgical pain.
When should persistent pain after surgery be evaluated urgently in person?
Persistent postsurgical pain should be evaluated urgently in person if there is fever, wound redness, swelling, pus, bleeding, new weakness, loss of bladder or bowel control, chest pain with shortness of breath, fainting, severe abdominal pain, jaundice, vomiting, calf swelling, sudden neurological symptoms, or rapidly worsening pain. Urgent evaluation is also needed if the patient feels acutely unwell or if the pain is new and severe. Telehealth is not appropriate for emergencies. It is most useful after dangerous complications have been excluded and the remaining question is why pain persists despite normal tests or unclear explanations.
Related topics about postoperative pain – Neurosurgery and Pain Treatment
Detailed explanation of online pain consultation for postsurgical pain
Step-by-step explanation of the video consultation for patients with postoperative pain
FAQ: Process and effectiveness of video consultations for postoperative pain
See the page “Possible Reasons for Poor Pain Treatment Effectiveness in Postoperative Pain ” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
Analysis of complex postoperative pain cases with artificial intelligence (AI)
A similar neuropathic pain condition is trigeminal neuralgia