Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
May 28, 2026
Who This Spinal Cord Tumors Page Is For
This page is intended for patients diagnosed with a tumor of the spinal cord (intramedullary tumor), as well as for individuals in whom MRI has revealed spinal cord enlargement, an intramedullary lesion, or an unclear finding requiring further evaluation.
Tumors of the spinal cord often progress slowly but may lead to significant neurological impairment if diagnosis or treatment is delayed. Patients are frequently faced with difficult questions regarding the timing of surgery, expected neurological recovery, the role of radiotherapy, or whether observation remains safe. Medical recommendations may differ between centers, particularly when symptoms are mild but imaging findings appear significant.
If spinal cord surgery has been proposed, neurological symptoms are progressing, or MRI findings remain difficult to interpret, an individualized neurosurgical second opinion may help clarify diagnosis, urgency of treatment, surgical risks, and the safest therapeutic strategy based on tumor type, spinal cord involvement, and overall neurological condition.
When patients seek a second opinion for spinal cord tumors
• An intramedullary spinal cord tumor or unclear lesion has been detected on MRI, but its biological nature or treatment urgency remains uncertain
• Surgery has been recommended, yet expected neurological recovery or potential risks have not been clearly explained
• Radiotherapy has been proposed, but it remains unclear whether surgical removal or decompression should be performed first
• Progressive weakness, walking instability, sensory loss, or bladder dysfunction suggest possible spinal cord involvement
• Different specialists recommend observation, surgery, or radiation therapy without clear agreement
• Neurological symptoms persist or worsen after previous spinal cord tumor treatment or surgery
Not every spinal cord tumor requires immediate surgery, but delayed treatment in the presence of spinal cord compression may lead to permanent neurological impairment.
When diagnosis, treatment timing, or surgical strategy remain uncertain, careful neurosurgical evaluation becomes essential.
If your situation involves uncertainty regarding diagnosis or treatment planning, you may request an individualized neurosurgical review here:
Request Second Opinion
Tumors of the Spinal Cord — Quick Summary (Read This First)
- Spinal cord tumors, also called intramedullary tumors, develop within the spinal cord itself; the most common types are ependymoma and astrocytoma. Even small lesions may affect movement, sensation, or bladder function because functional spinal pathways are directly involved.
- The most common spinal cord tumors are ependymomas and astrocytomas. Treatment strategy differs primarily according to tumor biology, particularly between ependymomas and astrocytomas.
- Symptoms usually develop gradually. Persistent, poorly localized back pain — frequently worse at night or at rest — is often the earliest symptom, while progressive weakness, gait disturbance, numbness, and coordination problems appear as spinal cord pathways become increasingly affected.
- Neurological deficits may remain minimal or absent for a long time despite tumor growth. Because many intramedullary tumors grow slowly, the spinal cord can temporarily adapt, allowing tumors to become large before clear symptoms appear. In such situations, treatment decisions may be complex, since neurological function may temporarily worsen after surgery even when intervention is necessary to prevent permanent spinal cord damage.
- MRI with contrast is the essential diagnostic examination. It determines tumor location, extent of spinal cord involvement, and surgical planning.
- Not all spinal cord tumors require immediate surgery. Approximately 10–20% of patients may initially undergo observation when neurological function is stable and imaging shows no progression, although many of these tumors eventually require surgical treatment during follow-up.
- Surgery is recommended when neurological deficits progress or tumor growth is documented. The goal is maximal safe removal while preserving spinal cord function.
- Temporary neurological worsening after surgery may occur. Recovery often develops gradually over weeks or months as the spinal cord recovers.
- Radiotherapy may be required after incomplete removal or in higher-grade (more aggressive) tumors. Treatment strategy depends on tumor type and neurological condition.
- Neurological outcome depends strongly on timing of treatment. Earlier intervention generally provides better functional recovery.
- The primary treatment goal is preservation of neurological independence and long-term tumor control.
Most readers benefit from reviewing this Quick Summary together with the sections on Symptoms, Diagnostic Imaging, and Surgical Treatment. Later sections provide more detailed explanations intended for patients seeking a deeper understanding before treatment decisions are made.
Contents
- Who This Spinal Cord Tumors Page Is For
- Quick Summary
- What Are Spinal Cord Tumors
- How Common Are Intramedullary Tumors
- Which Tumors Occur Inside the Spinal Cord
- Distribution Along the Spinal Cord
- Basic Anatomy Relevant for Symptoms
- How Intramedullary Tumors Develop
- Mechanisms of Spinal Cord Damage
- Tumor types: Ependymoma, Astrocytoma and Hemangioblastoma
- Association With Syringomyelia
- Symptoms Depending on Tumor Level
- Diagnostic Imaging
- Observation Versus Surgery
- Indications for Surgery
- Temporary Neurological Worsening
- Surgical Technique
- Possible Complications
- Adjuvant Treatment
- Follow-Up After Treatment
- Management of Recurrence
- Long-Term Prognosis
- Why Neurosurgical Opinions May Differ
- Request Second Opinion
- FAQs
What Are Spinal Cord Tumors
Spinal cord tumors, also called intramedullary tumors, are tumors that arise within the spinal cord itself.
The main intramedullary tumor types include ependymoma, astrocytoma, and less commonly hemangioblastoma and other rare glial tumors and metastasis.
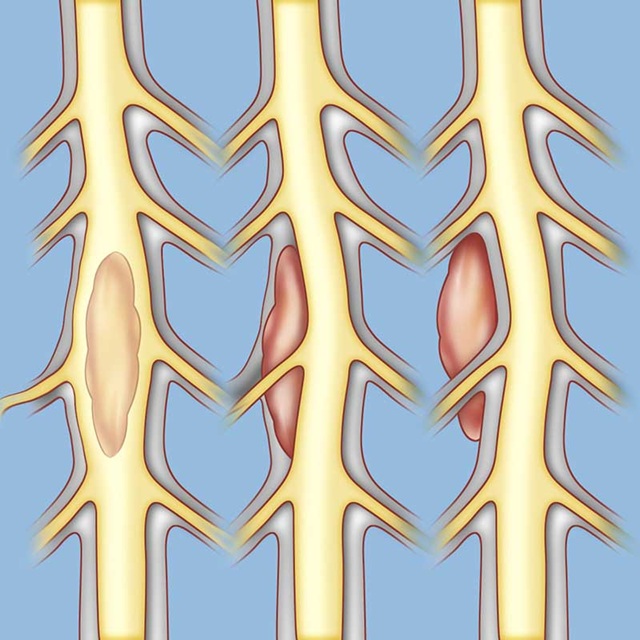
Image: Spinal tumors can be located in three different areas (from left to right): intramedullary (inside the spinal cord, e.g., ependymoma or astrocytoma), intradural-extramedullary (inside the spinal membrane but outside the cord, e.g., meningioma or schwannoma), or extradural (outside the spinal membrane, e.g., bone metastases or vertebral tumor).
How Common Are Intramedullary Tumors
Intramedullary spinal cord tumors are uncommon, representing only about 5–10% of all spinal tumors.
Among all spinal tumors:
- only 5–10% of all spinal tumors are intramedullary tumors
- about 55–65% are extradural tumors, most commonly metastatic lesions
- approximately 30–40% are intradural tumors (e.g., schwannoma, meningioma)
Although uncommon, these tumors are neurologically important because progressive damage to the spinal cord may occur even during slow tumor growth.
Which Tumors Occur Inside the Spinal Cord
The majority of intramedullary tumors include:
- ependymoma, approximately 60–70%
- astrocytoma, approximately 25–35%
- hemangioblastoma, metastasis and other rare tumors occurring less frequently
In adults, ependymoma is the dominant tumor type, while astrocytomas are relatively more frequent in pediatric patients.
Distribution Along the Spinal Cord
Intramedullary tumors may occur at any spinal level:
- cervical spinal cord — about 40–45%
- thoracic spinal cord — about 35–40%
- conus medullaris — about 15–20%
Ependymomas commonly arise near the central canal and lower spinal cord segments.
Basic Anatomy Relevant for Symptoms
The spine consists of 5 main regions: cervical, thoracic and lumbar spine, sacrum and coccyx (tailbone)
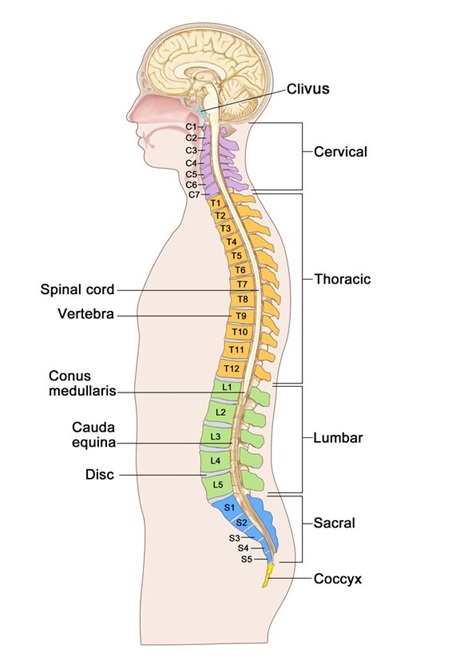
Image: Regions of the spine: cervical (neck), thoracic (mid-back), lumbar (lower back), sacral, and coccygeal (tailbone). Inside the spine is the spinal canal, which houses the spinal cord. The spinal cord ends at the level of the L1 vertebra, so the spinal canal of the lumbosacral region contains only nerve roots (either individually or as the cauda equina). Learn more on our Spine anatomy page.
From outside toward the spinal cord, anatomical layers include:
- vertebral bone
- epidural space
- dura mater
- arachnoid membrane
- cerebrospinal fluid
- spinal cord
The spinal cord contains pathways responsible for movement, sensation, coordination, and bladder and bowel control. Damage to these pathways leads to various combinations of neurological deficits. Neurological deficits therefore appear below the tumor level.

Image: The spine is composed of vertebrae stacked one on top of the other. Inside, these bones form the spinal canal, which acts as a protective tunnel. The spinal cord and the nerve roots that branch off from it pass through this canal.
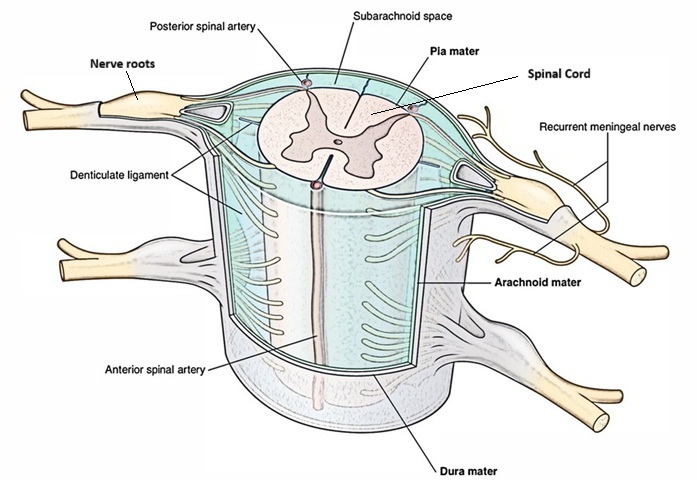
Image: The spinal cord and its nerve roots. Dura and other anatomical layers. Between the arachnoid layer and the nerve elements, clear cerebrospinal fluid (CSF) circulates.
How Intramedullary Tumors Develop
Intramedullary tumors arise from cells normally present within the spinal cord.
Like other tumors in the body, intramedullary tumors develop as a result of genetic alterations (mutations) occurring in previously normal cells. Some genes become activated (proto-oncogenes transforming into oncogenes), while others become inactivated (tumor suppressor genes). Such genetic changes occur continuously in many cells. Under normal circumstances, cellular repair mechanisms and immune surveillance eliminate most abnormal cells. Occasionally, however, altered cells escape these control mechanisms and continue to proliferate, leading to tumor formation. Some tumors remain biologically slow growing, while others may acquire additional genetic alterations associated with more aggressive behavior.
The precise causes of these genetic changes are often unknown. They may occur spontaneously or rarely be associated with exposure to ionizing radiation or prior medical treatment. For most intramedullary spinal tumors, however, no single identifiable cause can be established.
Most intramedullary tumors are not inherited. Nevertheless, certain rare genetic syndromes, such as neurofibromatosis or von Hippel–Lindau disease, may increase susceptibility to tumor development. In the majority of patients, the tumor develops without a recognizable hereditary cause.
Mechanisms of Spinal Cord Damage by Intramedullary Tumor
Neurological damage develops mainly through:
- gradual compression of spinal cord or/and neural fibers
- disturbance of spinal cord blood circulation
- destruction of functional spinal pathways
- obstruction of cerebrospinal fluid flow and syringomyelia formation
Because growth can be slow, some tumors may become large before severe neurological symptoms appear.
Ependymoma, Astrocytoma and Hemangioblastoma — Biological Differences
An ependymoma usually grows centrally within the spinal cord and often forms a relatively clear border separating tumor from normal tissue. This characteristic frequently allows complete surgical removal.
According to current classifications, spinal cord ependymomas are divided into:
- WHO Grade I — myxopapillary ependymoma and subependymoma
- WHO Grade II — classic (typical) ependymoma
- WHO Grade III — anaplastic ependymoma (more aggressive and faster growing)
Most spinal ependymomas are low-grade tumors (WHO Grade I–II), representing the large majority of cases, while anaplastic (Grade III) variants are uncommon.
Ependymomas may therefore appear as:
- Myxopapillary ependymoma — typically arising in the conus medullaris or filum terminale
- Classic intramedullary ependymoma
- Anaplastic ependymoma — a rare high-grade form
An astrocytoma typically infiltrates surrounding spinal cord tissue without a clear boundary. Surgical treatment therefore prioritizes preservation of neurological function rather than radical excision.
Intramedullary astrocytomas show a broader biological spectrum:
- WHO Grade I — pilocytic astrocytoma (slow-growing, more common in children)
- WHO Grade II — diffuse astrocytoma (most common spinal astrocytoma)
- WHO Grade III–IV — high-grade or malignant astrocytomas (less frequent but associated with poorer prognosis)
Clinical series indicate that approximately 70–80% of spinal cord astrocytomas are low-grade (Grade I–II), whereas 20–30% represent higher-grade tumors, which demonstrate more aggressive behavior and limited surgical resectability.
Hemangioblastomas are rare, highly vascular tumors that may develop within the spinal cord, most commonly in adults. They are usually benign and slow growing but can cause progressive neurological symptoms due to spinal cord compression or associated fluid cavity formation (syringomyelia). Some hemangioblastomas occur sporadically, while others are associated with von Hippel–Lindau disease. Because these tumors often have a well-defined border, surgical removal is frequently effective when treatment becomes necessary. Asymptomatic tumors are frequently monitored with periodic MRI examinations, and approximately one third to one half of incidentally detected lesions may initially be managed without surgery when neurological function remains stable.
Besides the above-mentioned tumors less common tumors may also occur within the spinal cord, including gangliogliomas, primary spinal cord lymphomas, germ cell tumors, melanocytic tumors, and intramedullary metastases. In some patients, MRI appearance, tumor location, or associated systemic disease may raise suspicion for a specific diagnosis even before surgery. Importantly, not all intramedullary tumors require primary surgical removal. Certain lesions, such as lymphoma, germinoma, or metastatic tumors, may be treated primarily with radiotherapy or chemotherapy. However, in many cases the definitive diagnosis — and therefore the optimal treatment strategy — can only be established after histopathological (PH) analysis obtained during biopsy or surgical treatment.
Association With Syringomyelia
A fluid cavity inside the spinal cord, known as syringomyelia, frequently accompanies intramedullary tumors, particularly ependymomas.
This develops because tumor growth disturbs normal cerebrospinal fluid circulation inside the spinal cord.
Symptoms Depending on Tumor Level
Symptoms caused by intramedullary spinal cord tumors usually develop slowly and reflect progressive involvement of spinal cord pathways.
Diffuse back pain is often the earliest presenting symptom, but unlike extramedullary spinal tumors, this pain is typically poorly localized, non-radicular, and frequently described as deep burning or dysesthetic discomfort rather than sharp nerve-root pain. The pain commonly worsens at night or during rest, which may represent one of the earliest warning signs and often precedes clear neurological deficits. Radicular pain resembling sciatica is uncommon because the tumor arises within the spinal cord itself rather than compressing exiting nerve roots.
As tumor growth progresses, neurological symptoms become dominant, including sensory disturbance, gait instability, motor weakness, and later autonomic dysfunction below the tumor level.
Cervical spinal cord
Patients may experience:
- weakness involving arms and legs
- reduced hand coordination
- progressive walking instability
- sensory disturbance across hands and legs
- neck discomfort
- in advanced cases breathing difficulty
Thoracic spinal cord
Typical presentation includes:
- gradual difficulty walking
- stiffness of the legs
- sensory disturbance across the trunk
- balance impairment
Conus medullaris
Common symptoms include:
- impaired bladder control
- bowel dysfunction
- sexual dysfunction
- numbness in the saddle region
- leg weakness
- leg pain
Diagnostic Imaging
Spinal cord tumors are usually diagnosed with contrast-enhanced MRI of the spine, because MRI shows whether the lesion is inside the spinal cord, how far it extends, how it enhances, and whether it is more suggestive of ependymoma, astrocytoma, hemangioblastoma, inflammation, or another spinal cord disorder.
MRI demonstrates:
- precise tumor location
- if there is a clear demarcation between the tumor and the spinal cord
- spinal cord enlargement
- contrast enhancement pattern
- associated cysts or syrinx
- surrounding edema
Ependymomas usually produce central symmetric expansion of the spinal cord, while astrocytomas more commonly appear diffuse or eccentric.
Magnetic resonance imaging also plays an essential role in differential diagnosis, since not every intramedullary lesion represents a tumor. Conditions that may mimic intramedullary tumors include multiple sclerosis, neuromyelitis optica spectrum disorders, transverse myelitis, spinal cord infarction, cavernous malformations, and rare infections or granulomatous diseases. Careful analysis of lesion location, enhancement pattern, associated edema, and clinical progression helps distinguish true tumors from non-neoplastic spinal cord disorders.
Imaging of the Entire Spine and Brain
MRI of the entire spine and brain is often recommended for intramedullary spinal cord tumors to exclude multiple lesions, associated brain disease, tumor spread, or conditions that may change surgical planning.

Image: Spinal MRI shows a spinal cord tumor (ependymoma) – red arrow, which causes cysts to form within the cord both above and below the tumor (yellow arrow).
Treatment: Observation Versus Surgery
Observation may be considered for selected intramedullary spinal cord tumors when neurological function is stable, symptoms are minimal, and MRI does not show tumor growth or signs of increasing spinal cord risk.
Approximately 10–20% of patients may initially undergo monitoring with periodic MRI examinations. Observation is usually chosen when neurological function remains preserved, tumor growth appears slow, or imaging findings do not clearly indicate immediate risk of spinal cord injury. Because intramedullary tumors may enlarge gradually while neurological deficits remain mild, even relatively large tumors can occasionally be discovered before significant functional impairment develops.
However, long-term follow-up shows that many of these tumors eventually require surgical treatment as growth or neurological symptoms progress. In clinical practice, more than half of initially observed patients ultimately undergo surgery during follow-up once signs of spinal cord compromise appear.
The decision to observe rather than operate therefore reflects a balance between two risks: early surgery may temporarily worsen neurological function, while delayed treatment may allow irreversible spinal cord damage to develop.
Indications for Surgery
Surgery is recommended for an intramedullary spinal cord tumor when one or more signs suggest increasing neurological risk:
- neurological deficit progresses
- tumor enlargement is documented
- spinal cord compression threatens permanent damage
- diagnosis remains uncertain
Intramedullary tumors may become large with relatively mild symptoms because the spinal cord adapts gradually. Delayed treatment increases the risk of irreversible neurological damage. In such situations, treatment decisions may be complex, since neurological function may significantly temporarily worsen after surgery even when intervention is necessary to prevent permanent spinal cord damage.
Surgical Technique
Surgery is performed through a posterior approach with the patient positioned prone (lying on their stomach, with the incision made on the back).
Typical steps include:
- skin incision and exposure of vertebrae
- Laminectomy or Laminoplasty: The surgical approach involves either a laminectomy (the permanent removal of the vertebral arches to provide access) or a laminoplasty (the reconstruction of the spinal canal, where the removed laminae are replaced and fixed back into their original position following tumor excision to preserve spinal stability and protection).
- opening of the dura mater
- microsurgical opening of the spinal cord
- identification of tumor boundary
- maximal safe tumor removal is the main surgical principle in the treatment of intramedullary spinal cord tumors, but the achievable extent of resection depends strongly on tumor biology. In ependymomas and hemangioblastomas, a clear plane usually exists between the tumor and normal spinal cord tissue, which means that gross total resection (GTR) can often be safely achieved and is typically the preferred treatment. In contrast, most intramedullary astrocytomas grow infiltratively within the spinal cord and do not have a distinct surgical boundary. Complete removal is therefore generally possible only in selected pilocytic (WHO Grade I) astrocytomas. In diffuse astrocytomas (WHO Grade II–IV), attempts at radical resection are usually avoided because aggressive tumor removal mainly increases the risk of permanent neurological deficits without clear improvement in outcome. For this reason, surgery in astrocytomas focuses on maximal safe tumor removal while prioritizing preservation of neurological function, in accordance with current treatment guidelines.
Continuous intraoperative neurophysiological monitoring is used to protect motor and sensory pathways from surgical manipulation.
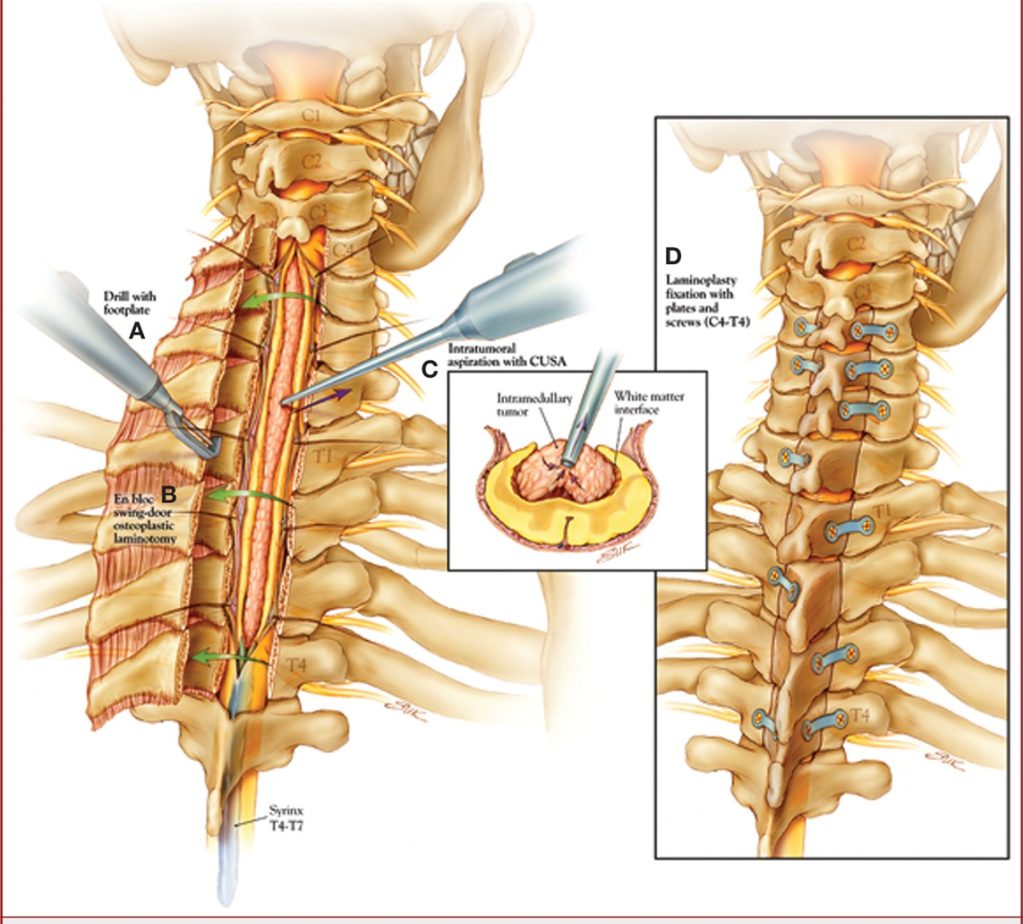
Image: The image on the left shows the removed posterior arches of the spinal canal (laminae) to access the spinal canal and spinal cord within it. The dura mater (the spinal cord’s protective envelope) is opened, followed by a midline incision of the spinal cord to reach the tumor. Whenever possible, the tumor’s margin is identified, and it is separated from the spinal cord and removed (in this case, using a specialized surgical aspirator called CUSA). The entire procedure is performed under general anesthesia with neurophysiological monitoring, which tracks the spinal cord pathways to ensure they are not damaged during manipulation. After the tumor is removed, the dura is sutured, and the laminae are re-fixed (laminoplasty, as shown in the image on the right).
Possible Complications
Local complications may include:
- Cerebrospinal fluid leakage
- Infection
- Bleeding
- Postoperative spinal instability
Neurological Worsening After Surgery
Temporary neurological worsening can occur after intramedullary spinal cord tumor surgery because the operation requires opening the spinal cord and manipulating delicate motor and sensory pathways and their blood supply. Recovery often develops gradually over weeks or months. Outcome largely depends on the spinal cord condition before surgery.
Request Spinal Cord Tumor Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Being told that an intramedullary spinal cord tumor or an unclear lesion within the spinal cord is present on MRI can raise urgent and complex questions:
Is this an ependymoma or astrocytoma? Is neurological deterioration expected?
Does the finding require early surgery, radiotherapy, or careful observation?
An independent neurosurgical second opinion may help clarify the most likely diagnosis, the urgency of treatment,
and the safest therapeutic strategy based on imaging findings, neurological status, and expected functional outcome.
- ✔ Send a brief message describing your main neurological symptoms (weakness, walking difficulty, numbness, coordination problems, bladder or bowel changes) and what your MRI report states
- ✔ You will receive a reply within 24 hours explaining whether an online consultation is appropriate and which documentation is required
- ✔ Priority cases: progressive weakness, loss of walking ability, new bladder dysfunction, or rapidly worsening neurological symptoms — write PRIORITY in your first message
- ✔ MRI images (DICOM format) and radiology reports can be reviewed after initial contact to assess tumor characteristics and surgical options
- ✔ During consultation, we explain tumor type likelihood, surgical indications, expected neurological recovery, treatment sequence, risks, and realistic next steps — including up to 10 days of follow-up clarification
Consultation fees typically range from $180–250, depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This corresponds to typical international specialist telehealth neurosurgical second-opinion services.
Adjuvant Treatment
Radiotherapy or other adjuvant treatment may be required after incomplete removal of an intramedullary spinal cord tumor, tumor progression, or higher-grade pathology, but it is not automatically needed after complete removal of a low-grade ependymoma.
1) Radiotherapy represents the most common adjuvant treatment following incomplete tumor removal or in higher-grade tumors. Treatment is usually delivered as fractionated external beam radiotherapy, while stereotactic radiotherapy may be considered in selected cases or for tumor recurrence. Chemotherapy is rarely required.
After complete removal of low-grade ependymoma, further therapy is often unnecessary.
In intramedullary astrocytomas, treatment strategy differs significantly. Because most astrocytomas infiltrate normal spinal cord tissue, subtotal (incomplete) resection is frequently performed to preserve neurological function. In low-grade (WHO Grade II) astrocytomas, postoperative management may include careful radiological follow-up rather than immediate radiotherapy, especially when neurological function is stable. Adjuvant radiotherapy is more commonly considered in cases of tumor progression, symptomatic residual tumor, or higher-grade disease.
Since intramedullary astrocytomas frequently affect children and young adults, the potential long-term consequences of radiotherapy must be carefully considered before treatment. Possible complications include permanent neurological worsening, radiation-induced myelopathy, spinal deformities such as scoliosis, impaired spinal growth, and late radiation-related tissue injury. For this reason, the indication for radiotherapy is evaluated cautiously, and all potential risks must be discussed in detail with patients and, in pediatric cases, with parents before treatment decisions are made.
2) Chemotherapy is used selectively in intramedullary astrocytomas, particularly in higher-grade tumors (WHO Grade III–IV) or in cases of tumor progression when further surgery or radiotherapy is not feasible. The most commonly used agent is temozolomide (Temodar), extrapolated from its established role in intracranial gliomas. Its benefit in spinal cord astrocytomas remains limited and variable, and treatment decisions are individualized.
Follow-Up After Treatment
MRI surveillance typically includes:
- Examination three months after surgery
- Six-month control
- Annual follow-up thereafter
Long-term monitoring remains essential.
Emerging and Investigational Treatment Approaches in Intramedullary Tumors
A number of new treatment strategies are currently being developed for central nervous system tumors, primarily for brain tumors, but many of these approaches are increasingly being explored for intramedullary spinal cord tumors as well. These include targeted drug delivery techniques, convection-enhanced delivery (CED), focused ultrasound–assisted treatment, implantable drug-releasing systems, nanomedicine-based therapies, as well as emerging molecular and immunotherapy-based approaches aimed at improving tumor control while minimizing damage to normal nervous tissue and overcoming biological barriers such as the blood–spinal cord barrier that limit conventional therapies.
At present, most of these methods remain investigational and are available mainly within clinical trials or specialized research programs. Some techniques have shown promising early results, while others are still undergoing safety and efficacy evaluation before wider clinical adoption.
Patients who are offered participation in experimental or investigational treatment programs may consider obtaining an independent medical opinion before proceeding. This also applies to treatment methods promoted outside established academic or clinical research institutions, particularly when proposed therapies are not supported by peer-reviewed clinical evidence. If needed, treatment proposals can be reviewed independently to help assess potential benefits, risks, and realistic expectations based on current neurosurgical and neuro-oncological standards.
Management of Recurrence
Tumor recurrence may require repeat surgery, radiotherapy, or combined treatment depending on tumor biology and neurological condition. Recurrence risk differs substantially between tumor types. Intramedullary astrocytomas, particularly diffuse tumors treated with subtotal resection, demonstrate recurrence in approximately 40–50% of cases, reflecting their infiltrative growth pattern. In contrast, spinal ependymomas show significantly lower recurrence rates, reported in roughly 5–10% of patients, most commonly after incomplete tumor removal or in higher-grade variants.
Distinguishing true tumor recurrence from postoperative scar tissue or treatment-related changes may sometimes be challenging on MRI alone. Recurrent tumors typically demonstrate progressive enlargement and persistent or increasing contrast enhancement over time, whereas postoperative scarring usually remains stable or gradually decreases during follow-up examinations. For this reason, comparison with previous MRI studies and clinical evolution remains essential before additional treatment is recommended.
Long-Term Prognosis
The long-term prognosis of intramedullary spinal cord tumors is usually better for completely removable ependymomas and more variable for astrocytomas, especially when neurological function is already impaired before treatment.
Complete removal of ependymoma often provides long-term disease control, while astrocytoma outcome varies significantly according to tumor grade. Low-grade astrocytomas (WHO Grade I–II) may follow a relatively slow clinical course, whereas high-grade astrocytomas (WHO Grade III–IV) are associated with more aggressive progression and represent the group with the shortest survival, with reported average survival times of approximately 12–18 months despite treatment.
The most important predictor of recovery remains neurological status at the time of surgery. Long-term functional independence often depends more on preoperative neurological status than on tumor size alone.
Why Neurosurgical Opinions May Differ in Spinal Cord Tumors
Management of intramedullary spinal cord tumors often involves complex decision-making in which more than one medically reasonable approach may exist. Differences between neurosurgical opinions do not necessarily indicate diagnostic error, but rather reflect careful balancing between tumor control and preservation of neurological function.
Neurosurgical recommendations may differ regarding:
How MRI Findings Are Interpreted in Complex Cases
Whether imaging represents a true tumor, inflammatory disease, postoperative change, or treatment-related alteration may not always be immediately clear.
When Early Surgery Is Preferred Over Observation
Some specialists may recommend early surgery to prevent future neurological deterioration, while others may advise careful monitoring when neurological function remains stable.
How Neurological Risk Influences the Treatment Decision
Surgeons may differ in estimating the likelihood of temporary or permanent neurological worsening after tumor removal, particularly in patients with minimal symptoms despite large tumors.
How Much of the Tumor Should Be Safely Removed
In certain tumors — most commonly intramedullary astrocytomas — aggressive resection may improve long-term tumor control but substantially increase neurological risk, whereas subtotal removal is often intentionally performed to preserve spinal cord function when clear tumor boundaries are absent.
Which Surgical Strategy Is Most Appropriate
Opinions may vary regarding surgical approach, extent of bone removal, need for reconstruction, or intraoperative techniques used to minimize spinal cord injury.
When Additional (Adjuvant) Treatment Is Necessary
Recommendations may differ concerning postoperative radiotherapy, timing of radiation, or the need for additional oncological treatment depending on tumor type and histology.
How Postoperative MRI Findings Are Interpreted
Specialists may disagree whether imaging changes represent tumor recurrence, postoperative scar tissue, radiation effects, or normal healing processes.
Because spinal cord tissue has limited capacity for recovery after injury, treatment decisions frequently involve weighing competing risks rather than choosing between clearly right or wrong options. For this reason, independent neurosurgical evaluation may help patients better understand available strategies and expected outcomes.
Frequently Asked Questions About Spinal Cord Tumors
What is an intramedullary spinal cord tumor?
An intramedullary spinal cord tumor is a tumor that develops within the spinal cord itself. This makes it different from tumors that compress the spinal cord from outside, such as spinal meningiomas or schwannomas. Because intramedullary tumors arise inside functional spinal cord tissue, even a relatively small lesion may affect movement, sensation, coordination, or bladder and bowel control. These tumors often grow slowly, so symptoms may develop gradually and may remain mild for some time. However, delayed diagnosis or treatment can allow permanent spinal cord damage to occur. MRI findings, neurological symptoms, tumor type, and the rate of progression all influence whether observation, biopsy, surgery, radiotherapy, or another strategy is appropriate.
What are the most common intramedullary spinal cord tumor types?
The most common intramedullary spinal cord tumors are ependymomas and astrocytomas. Ependymomas are more frequent in adults and often arise centrally within the spinal cord, sometimes with a clearer boundary between tumor and normal tissue. Astrocytomas are relatively more frequent in children and young patients and often infiltrate spinal cord tissue without a clear surgical plane. Hemangioblastomas are less common but may occur sporadically or in association with von Hippel–Lindau disease. Rare intramedullary lesions include metastases, lymphoma, ganglioglioma, germ cell tumors, melanocytic tumors, and inflammatory or vascular conditions that may mimic tumors. Identifying the likely tumor type is important because treatment strategy and prognosis differ significantly.
Can an intramedullary spinal cord tumor be benign?
Yes. Many intramedullary spinal cord tumors are benign or low grade, especially many ependymomas, hemangioblastomas, and some low-grade astrocytomas. However, benign does not mean unimportant. A slow-growing tumor inside the spinal cord can still damage motor, sensory, or bladder pathways by expanding within the cord, disturbing blood supply, or causing cysts and syringomyelia. Some tumors are more aggressive, especially higher-grade astrocytomas or anaplastic variants. MRI can suggest tumor behavior, but final grading often requires histopathological analysis after biopsy or surgery. Treatment decisions therefore depend not only on whether a tumor appears benign, but also on symptoms, growth, spinal cord involvement, neurological function, and realistic surgical risk.
How do ependymoma and astrocytoma differ in the spinal cord?
Spinal cord ependymoma and astrocytoma differ mainly in growth pattern and surgical strategy. Ependymomas often grow centrally and may have a relatively clear boundary between tumor and normal spinal cord tissue. For this reason, complete removal is often possible, especially in low-grade tumors, and surgery may provide long-term tumor control. Astrocytomas more often grow infiltratively through spinal cord tissue without a clear surgical plane. In these cases, aggressive removal may create a high risk of permanent neurological worsening. Surgery for astrocytoma therefore usually focuses on maximal safe removal, biopsy, decompression, and preservation of function. This distinction is one reason why the same MRI diagnosis may lead to different treatment recommendations.
What symptoms can intramedullary spinal cord tumors cause?
Intramedullary spinal cord tumors usually cause symptoms by disturbing pathways inside the spinal cord. Early symptoms may include persistent, poorly localized back or neck pain, burning or dysesthetic discomfort, numbness, tingling, stiffness, or subtle walking imbalance. Pain may be worse at night or at rest. As the tumor affects motor and sensory pathways, patients may develop weakness, spasticity, clumsiness, reduced hand coordination, gait instability, sensory level, or impaired balance. Tumors near the conus medullaris may affect bladder, bowel, sexual function, or saddle sensation. Symptoms often progress slowly, which can delay diagnosis. Progressive weakness, walking difficulty, coordination problems, or bladder dysfunction are especially important warning signs requiring careful evaluation.
Can spinal cord tumor symptoms stay mild even if the tumor is large?
Yes. Symptoms of an intramedullary spinal cord tumor can remain mild even when the tumor has become large. Many spinal cord tumors grow slowly, and the spinal cord may temporarily adapt to gradual enlargement. A patient may therefore have only mild pain, sensory disturbance, or walking imbalance despite significant MRI findings. This situation can make treatment decisions difficult. Early surgery may carry a risk of temporary neurological worsening, while delayed treatment may allow irreversible spinal cord injury. Tumor size alone is not enough to decide treatment. Neurosurgeons assess neurological function, tumor growth, spinal cord signal changes, tumor type, surgical plane, and whether the current stability is likely to remain safe.
What is the best MRI test for diagnosing intramedullary spinal cord tumors?
The most important test for diagnosing an intramedullary spinal cord tumor is contrast-enhanced MRI of the spine. MRI shows whether the lesion is located inside the spinal cord, how many spinal levels are involved, whether the spinal cord is enlarged, how the lesion enhances with contrast, and whether cysts, syringomyelia, edema, or bleeding are present. These features may suggest ependymoma, astrocytoma, hemangioblastoma, metastasis, inflammatory disease, demyelination, infarction, or another condition. MRI is also essential for surgical planning because it helps estimate whether a tumor has a clear boundary or appears infiltrative. CT is less useful for the spinal cord itself, but may help assess bone when needed.
Can MRI distinguish spinal cord tumor from inflammation or demyelinating disease?
MRI can often help distinguish an intramedullary spinal cord tumor from inflammation, demyelinating disease, spinal cord infarction, cavernous malformation, infection, or other non-tumor conditions, but it is not always definitive. Tumors often produce spinal cord enlargement, persistent contrast enhancement, cysts, syrinx formation, or progressive growth over time. Inflammatory or demyelinating lesions may have different enhancement patterns, clinical evolution, cerebrospinal fluid findings, or response to medical treatment. Sometimes repeated MRI, brain MRI, blood tests, CSF analysis, or biopsy is needed before the diagnosis becomes clear. This distinction is critical because treating inflammation as a tumor, or a tumor as inflammation, can delay the correct therapy and worsen neurological outcome.
Do intramedullary spinal cord tumors require MRI of the entire spine and brain?
MRI of the entire spine and brain is often recommended when an intramedullary spinal cord tumor is diagnosed or strongly suspected. This helps exclude multiple lesions, associated brain abnormalities, tumor spread through cerebrospinal fluid pathways, or conditions that may change the diagnosis and treatment plan. Whole-axis imaging is especially important when MRI appearance is unusual, symptoms do not fit one spinal level, hemangioblastoma or von Hippel–Lindau disease is suspected, or surgery is being planned. In some straightforward cases, the initial MRI may focus on the affected region, but complete imaging is commonly requested before definitive treatment. The goal is to avoid missing additional disease that could change prognosis, timing, or surgical strategy.
What does syringomyelia mean in a spinal cord tumor?
Syringomyelia means that a fluid-filled cavity, called a syrinx, has formed inside the spinal cord. In intramedullary spinal cord tumors, syringomyelia may develop because tumor growth disturbs normal cerebrospinal fluid flow within or around the spinal cord. It is commonly associated with ependymomas but may occur with other lesions as well. A syrinx can contribute to pain, sensory changes, weakness, or dissociated sensory loss, depending on its location and size. Its presence may help suggest that an underlying tumor is affecting spinal cord fluid dynamics. Treatment is directed primarily at the tumor or cause of obstruction, not simply at draining the syrinx. After successful tumor treatment, the syrinx may shrink over time.
When can observation be safe for an intramedullary spinal cord tumor?
Observation may be safe for selected intramedullary spinal cord tumors when neurological function is stable, symptoms are minimal, MRI does not show growth, and the lesion does not appear to threaten rapid spinal cord injury. This approach is sometimes considered for small or slow-growing lesions, incidental findings, selected hemangioblastomas, or uncertain abnormalities that require interval imaging before treatment is chosen. Observation is not the same as ignoring the tumor. It requires planned MRI surveillance and repeated neurological assessment. Surgery or biopsy becomes more important if the tumor enlarges, symptoms progress, diagnosis remains uncertain, or spinal cord function becomes threatened. The decision must balance surgical risk against the risk of delayed irreversible neurological damage.
When is surgery recommended for an intramedullary spinal cord tumor?
Surgery is recommended for an intramedullary spinal cord tumor when neurological deficits progress, tumor enlargement is documented, spinal cord function is threatened, or the diagnosis cannot be clarified safely without tissue analysis. Worsening weakness, walking instability, sensory loss, hand clumsiness, coordination problems, or bladder and bowel dysfunction are important clinical signs. MRI features also matter, including progressive spinal cord enlargement, increasing enhancement, associated cysts, or signs suggesting a surgically removable tumor such as ependymoma or hemangioblastoma. Surgery may aim for complete removal, partial removal, decompression, or biopsy depending on tumor type. The main goal is maximal safe treatment while preserving neurological independence.
Is complete removal possible for spinal cord ependymoma or astrocytoma?
Complete removal is often possible for many spinal cord ependymomas because they commonly have a more defined boundary between tumor and normal spinal cord tissue. When this plane is present, gross total resection may provide long-term control. The situation is different for many spinal cord astrocytomas. Astrocytomas often infiltrate normal spinal cord pathways and may not have a safe surgical border. In diffuse astrocytoma, forced complete removal can increase the risk of permanent weakness, sensory loss, or bladder dysfunction without clear benefit. For that reason, surgery for astrocytoma often aims at maximal safe removal, decompression, or biopsy rather than radical excision. The operative plan depends on MRI appearance, intraoperative findings, and neurophysiological monitoring.
Why can weakness worsen temporarily after spinal cord tumor surgery?
Weakness, numbness, or sensory worsening can occur temporarily after intramedullary spinal cord tumor surgery because the operation requires opening the spinal cord and working near delicate motor and sensory pathways. Even with microsurgical technique and neurophysiological monitoring, the spinal cord may react to manipulation, swelling, altered blood supply, or decompression after long-standing pressure. Temporary worsening does not always mean permanent injury. Recovery may develop gradually over weeks or months as swelling settles and pathways recover. However, the risk is higher when the spinal cord was already severely compressed, when symptoms were long-standing, when the tumor is infiltrative, or when preoperative neurological function was poor. This risk must be discussed before surgery.
Is radiotherapy used instead of or after surgery for intramedullary spinal cord tumors?
Radiotherapy may be used after surgery for some intramedullary spinal cord tumors, especially after incomplete removal, tumor progression, recurrence, or higher-grade pathology. It is not automatically needed after complete removal of a low-grade ependymoma. In astrocytomas, the decision is more complex because many are infiltrative and may be subtotally removed to protect spinal cord function. Low-grade astrocytomas may sometimes be followed with MRI, while higher-grade or progressive tumors more often require radiotherapy or oncological treatment. Radiotherapy is used cautiously because the spinal cord has limited tolerance to radiation, and late complications can be serious. In selected tumors such as lymphoma, metastasis, or germinoma, non-surgical treatment may play a primary role.
What determines long-term prognosis in intramedullary spinal cord tumors?
Long-term prognosis in intramedullary spinal cord tumors depends mainly on tumor type, tumor grade, extent of safe removal, and neurological function before treatment. Completely removable low-grade ependymomas generally have a better prognosis and may achieve long-term control after surgery. Astrocytoma prognosis is more variable because many astrocytomas infiltrate spinal cord tissue and cannot be radically removed without high neurological risk. High-grade astrocytomas have a significantly poorer outlook. The strongest functional predictor is often the patient’s neurological condition before surgery. Patients treated before severe or long-standing weakness, spasticity, sensory loss, or bladder dysfunction usually have better recovery potential than patients with advanced spinal cord damage at the time of treatment.
Can an intramedullary spinal cord tumor recur after treatment?
Yes. An intramedullary spinal cord tumor can recur after treatment, but recurrence risk depends strongly on tumor type, grade, and extent of removal. Low-grade ependymomas have a relatively low recurrence risk after complete removal, while recurrence is more likely after subtotal removal or higher-grade disease. Astrocytomas recur more often because they frequently grow infiltratively and cannot always be completely removed. MRI follow-up is essential because recurrent tumor must be distinguished from postoperative scar tissue, treatment-related changes, or radiation effects. Progressive enlargement or increasing enhancement over time is more concerning than stable postoperative change. Treatment of recurrence may involve repeat surgery, radiotherapy, chemotherapy, or observation depending on biology and neurological status.
Can I obtain an online neurosurgical second opinion for an intramedullary spinal cord tumor?
Yes. An online neurosurgical second opinion may be useful when MRI shows an intramedullary spinal cord tumor, spinal cord enlargement, ependymoma, astrocytoma, hemangioblastoma, syringomyelia, or an unclear lesion inside the spinal cord. A review can help clarify the likely diagnosis, whether observation is reasonable, whether surgery is urgent, whether biopsy or removal is appropriate, and what neurological recovery can realistically be expected. It may also help when different specialists recommend surgery, radiotherapy, or monitoring. The most useful information includes MRI images in DICOM format, radiology reports, symptom history, neurological deficits, walking ability, hand function, sensory changes, pain pattern, and bladder or bowel symptoms.