Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 10, 2026
Who this page is for
This page is for patients with atypical trigeminal neuralgia or persistent facial pain that has not improved despite standard trigeminal neuralgia treatment.
It is especially relevant when facial pain is constant, burning, aching, pressure-like, dental-like, post-dental, postherpetic, MRI-negative, or when pain continues despite carbamazepine, oxcarbazepine, nerve blocks, Gamma Knife, rhizotomy, or microvascular decompression.
In these cases, the problem is often not simply “stronger trigeminal neuralgia.” The real cause may be an unrecognized pain generator — often a trigeminal nerve branch in the face that has been irritated by scar tissue, local inflammation, dental-related nerve injury, viral nerve damage, TMJ or muscle-related irritation, local compression, or central sensitization. These causes may not be visible on routine MRI.
Through a detailed telehealth video consultation, the pain pattern can be analyzed using facial pain anatomy, trigger mapping, and previous treatment response. Through the video screen, you will be guided step-by-step to perform specific jaw movements or gently press certain points on your face to check for hidden pain triggers. Once the active mechanism is identified, the exact source of pain can be targeted using a combination of medications outside the standard protocol for typical neuralgia. Pinpointing this exact cause allows you to be treated effectively here, or by your local doctors who previously could not identify the source. If a surgical procedure has been recommended to you, an online second opinion can help clarify whether it is truly necessary.
If you are unsure whether an online consultation can help after all previous tests and treatment, read why this consultation is different.
When patients usually seek a second opinion for atypical trigeminal neuralgia
• Facial pain persists despite carbamazepine, oxcarbazepine, gabapentin, pregabalin, or other medications
• Pain is constant, burning, aching, pressure-like, dental-like, post-dental, or postherpetic
• MRI is normal, unclear, or does not explain the exact facial pain pattern
• Pain continued after microvascular decompression, Gamma Knife, rhizotomy, nerve blocks, or dental procedures
• The diagnosis feels uncertain: typical TN, atypical trigeminal neuralgia, TMJ pain, dental pain, trigeminal neuropathy, or central sensitization
• Another procedure has been recommended, but the true pain generator has not been clearly identified
If this reflects your situation, a focused telehealth review can help clarify the pain generator, why previous treatment failed, and which treatment path is most logical now:
Request Consultation
Atypical Trigeminal Neuralgia — Quick Summary (Read This First)
- Atypical trigeminal neuralgia is a form of persistent facial pain that does not behave like classical trigeminal neuralgia. Instead of only brief electric-shock attacks with pain-free intervals, the pain may be constant, burning, aching, pressure-like, dental-like, post-dental, postherpetic, or difficult to classify.
- Facial pain treatment often fails when the diagnosis is treated as a label instead of a mechanism. Many patients are treated according to the standard protocol for typical trigeminal neuralgia, even when their pain pattern suggests a different pain generator.
- Classical trigeminal neuralgia usually involves vascular compression near the brainstem, inside the skull. In atypical trigeminal neuralgia, the active problem may instead be outside this classical root-entry-zone compression site in the skull, often in a smaller peripheral branch of the trigeminal nerve in the face.
- A normal MRI does not exclude trigeminal nerve irritation. Peripheral nerve irritation, scar tissue, local inflammation, dental-related nerve injury, muscle spasm, TMJ-related irritation, postherpetic nerve injury, or early sensitization may not appear as a clear MRI abnormality.
- Pain may continue even after microvascular decompression if vascular compression was not the true pain generator. Persistent pain after MVD may mean that another mechanism is active.
- The key step is to identify the true trigeminal pain generator. This is done by analyzing facial pain anatomy, pain distribution, triggers, previous treatment response, imaging findings, and through guided testing during the video consultation, where you will be instructed to apply gentle pressure to specific points on your face or perform certain jaw movements. This type of detailed facial pain mapping requires specialized knowledge of trigeminal anatomy that goes beyond the standard neurological assessment — which is why the pain generator is often missed in routine care. Because the diagnosis relies on pain anatomy and clinical pattern rather than imaging findings, this assessment can be performed with full precision through a video consultation.
- Several mechanisms may keep atypical facial pain active at the same time. This is why treatment often needs to address both the dominant pain generator and the factors that continue to irritate or sensitize the trigeminal nerve.
- Treatment should not simply repeat the same protocol when standard trigeminal neuralgia therapy has failed. The first step is to separate the active mechanisms and then choose a logical treatment combination based on the patient’s specific pain generator.
- Many patients improve with a targeted combination of medications rather than one drug alone. The key is not simply which medication is used, but whether the treatment matches the patient’s pain generator. Depending on the mechanism, treatment may include sodium-channel blockers, gabapentinoids, baclofen, antidepressants for neuropathic pain, topical treatments, anti-inflammatory support, sleep regulation, and other carefully selected therapies. Many of these combinations were never previously tried in these patients — not because medications do not work, but because the treatment was matched to the wrong diagnosis rather than to the actual pain generator.
- Medication often needs adjustment during the first 6–8 weeks. The first 10 days are especially important. If there is no reduction in pain during this early period, or if side effects occur, these clues help guide how the treatment plan should be adjusted and fine-tuned.
- Nerve blocks, Botox, or image-guided procedures may help when medication alone is not enough, though this is necessary for only a minority of patients. These options are most useful when they target a clearly identified trigeminal branch, trigger zone, or local source of irritation, rather than being used simply because the diagnosis is labeled as „trigeminal neuralgia.“
- Atypical trigeminal neuralgia can still improve after months or years of pain. Long-lasting pain does not mean the condition is psychological or untreatable. It often means that the real pain generator and contributing factors have not yet been identified and treated together.
- The prognosis of atypical trigeminal neuralgia is often considered less predictable than classical trigeminal neuralgia. This is especially true when pain is constant, burning, post-dental, postherpetic, MRI-negative, or not clearly linked to vascular compression. However, poor response to standard treatment does not mean the condition is untreatable. Outcomes can be significantly better when treatment is no longer based only on the diagnosis label, but on identifying the true pain generator and the contributing factors that keep the trigeminal nerve irritated.
- A second opinion is especially useful when pain continues despite medication, MVD, Gamma Knife, rhizotomy, nerve blocks, or dental procedures. A structured review can clarify whether the pain is typical trigeminal neuralgia, atypical trigeminal neuralgia, trigeminal neuropathy, TMJ-related pain, dental-related nerve pain, postherpetic pain, or central sensitization.
- Online consultation may still help when treatment has failed: read why this consultation is different.
Why facial pain treatment fails in atypical trigeminal neuralgia
Facial pain treatment often fails because the diagnosis is treated as a label instead of a mechanism.
Many patients are told they have trigeminal neuralgia and are then treated according to the standard protocol for typical trigeminal neuralgia. This usually means carbamazepine or oxcarbazepine first, followed by consideration of microvascular decompression, Gamma Knife, rhizotomy, or repeated nerve procedures if the pain continues.
That approach can work very well in classical trigeminal neuralgia. It is much less reliable when the pain is atypical.
Atypical trigeminal neuralgia may cause constant burning, aching, pressure, tooth-like pain, jaw pain, cheek pain, pain around the eye, ear-region pain, post-dental pain, postherpetic pain, or pain that continues between attacks. In these patients, the active problem may be outside the classical root-entry-zone vascular compression site — the part of the trigeminal nerve located inside the skull, close to the brainstem, where a blood vessel typically compresses the nerve in classical trigeminal neuralgia.
The irritation may involve any peripheral branch of the trigeminal nerve in the face. Possible causes of the nerve irritation include dental-related nerve injury, scar tissue, local inflammation, viral nerve damage, muscle spasm, TMJ-related irritation, local compression, other pain-contributing factors, or central sensitization. If these mechanisms are not identified, treatment becomes incomplete.
Listen to the YouTube audio explanation on the diagnosis and treatment of refractory trigeminal neuralgia explained by the author.
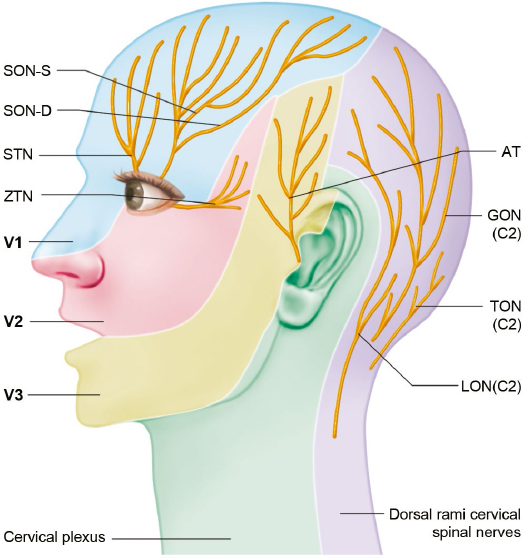
Image: Nerves that innervate skin of the head and face This image shows the main sensory nerves of the head and face. The most important facial pain pathways are the trigeminal branches: V1, V2, and V3. V1 is the ophthalmic branch and supplies the forehead, upper eyelid, eye region, and upper nose. V2 is the maxillary branch and supplies the cheek, lower eyelid, side of the nose, upper lip, upper teeth, and upper gum. V3 is the mandibular branch and supplies the lower jaw, lower teeth, lower gum, chin, part of the tongue, and part of the ear-temple region. The smaller labels show peripheral branches of these nerves. SON-S means supraorbital nerve, superficial branch. SON-D means supraorbital nerve, deep branch. STN means supratrochlear nerve. ZTN means zygomaticotemporal nerve. AT means auriculotemporal nerve. These smaller branches can become irritated locally and may produce focal forehead, temple, eye-region, cheek, jaw, or ear-temple pain even when routine MRI does not show a clear cause. Read more about the anatomy of the cranial nerves here and about when to worry about headaches here.
Why pain may continue even after microvascular decompression
Microvascular decompression is most effective when the patient has classical trigeminal neuralgia: brief electric-shock attacks, clear trigger zones, pain-free intervals, good response to carbamazepine or oxcarbazepine, and MRI evidence of vascular compression that matches the symptoms.
When facial pain is constant, burning, atypical, post-dental, postherpetic, bilateral, poorly responsive to medication, or not clearly matched by MRI, MVD becomes less predictable.
If pain continues after MVD, several explanations are possible. The vascular contact may not have been the true pain generator. There may have been a second mechanism active at the same time. The pain may come from a peripheral trigeminal branch in the face. The nervous system may have become sensitized after long-standing pain. Dental, viral, muscular, TMJ-related, or scar-related factors may still be irritating the nerve.
For this reason, persistent pain after MVD should not automatically lead to another destructive procedure. The first step should be a structured reassessment of the pain mechanism.
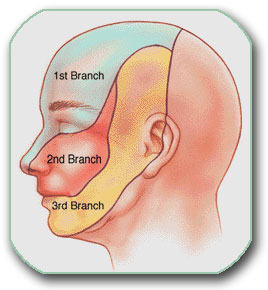
Image: Three facial regions where pain can occur, either separately or in combination
Why MRI can be normal in atypical trigeminal neuralgia
MRI is important in facial pain because it can detect tumors, multiple sclerosis, vascular compression, and other secondary causes. However, MRI cannot show every clinically important source of trigeminal nerve irritation.
Many causes of atypical trigeminal neuralgia are too small, too functional, or too peripheral to be clearly visible on routine imaging. A small irritated nerve branch in the face, scar tissue after dental work, local inflammation, muscle spasm, trigger-zone hypersensitivity, postherpetic nerve injury, or early peripheral nerve sensitization may not appear as a clear MRI abnormality.
A normal MRI does not mean that the pain is imaginary. It means that the diagnosis must rely more heavily on pain anatomy, clinical pattern, trigger analysis, response to previous treatment, and functional testing.
The most useful question is not only “what does the MRI show?” The more important question is: does the imaging explain the exact pain pattern?
How the true trigeminal pain generator is identified
The true trigeminal pain generator is identified by combining medical history, facial pain anatomy, trigger analysis, imaging review, and guided functional examination. The goal is not only to confirm the label “trigeminal neuralgia,” but to understand where and how the nerve is being irritated and why standard treatment has failed.
During the consultation, the pain pattern is analyzed in detail. It is important to determine where the facial pain starts, where it spreads, whether it feels electric, burning, aching, stabbing, pressure-like, dental-like, or deep, and whether there are pain-free intervals between attacks. The doctor also evaluates whether chewing, talking, brushing teeth, shaving, cold wind, jaw movement, pressure on certain points of the face and mouth, or neck movement changes the pain. This detailed mapping might sound deceptively simple — perhaps like a routine questionnaire you feel you have already answered, or something less advanced than an MRI scan. However, it is not. Only a specialist with deep knowledge of facial pain anatomy can use these exact clinical clues to pinpoint the hidden locations and specific processes irritating the nerve that imaging alone cannot show.
The previous history is equally important. Facial pain that began after dental treatment, facial trauma, shingles, herpes outbreaks, surgery, infection, or a previous procedure may have a different mechanism from typical trigeminal neuralgia. The response to carbamazepine, oxcarbazepine, nerve blocks, Gamma Knife, rhizotomy, or microvascular decompression also helps show whether the pain behaves like classical TN or whether another pain generator is active.
An examination of a patient with trigeminal neuralgia can be conducted in person at the clinic or during a video consultation. During a video consultation, the patient can be guided to press specific points on the face, jaw, cheek, temple, forehead, gum region, or around the eye. The patient may also be asked to perform small jaw, neck, or facial movements. If pain increases, decreases, spreads, or changes quality, this can help localize the irritated trigeminal branch or contributing structure. It is important to be examined in person or during a video consultation by a specialist who understands the pain anatomy of this region and knows how to check the many possible causes of this pain — often around 20 different nerve, muscle, joint, dental, viral, inflammatory, or sensitization-related mechanisms.
This is not a general conversation. It is an anatomical pain-mapping process. In atypical trigeminal neuralgia, this step is often more important than simply repeating MRI interpretation, because the active irritation may be located in a peripheral branch of the nerve in the face and may not be visible on standard imaging.
Why knowledge of facial pain anatomy matters
Atypical trigeminal neuralgia cannot be understood only by naming the diagnosis. The trigeminal nerve has several branches, and each branch can create a different pain pattern.
Pain around the eye, forehead, temple, upper teeth, cheek, nose, lower teeth, jaw, chin, ear region, tongue, or gum may involve different trigeminal pathways. Some pains are caused by the nerve root near the brainstem. Others are caused by peripheral branches in the face. Some are mixed with TMJ, muscle, cervical, dental, postherpetic, or central sensitization mechanisms.
If the anatomical source is not identified, treatment is often too general. A single medication may reduce nerve excitability but fail to stop ongoing local irritation. A procedure may interrupt one pathway but miss the true trigger point. Surgery may be performed for vascular contact that does not actually explain the symptoms.
Successful treatment depends on matching the treatment to the mechanism. Previous medication failure does not always mean that medication cannot help. In many persistent cases, the problem is that the right combination of mechanisms was not treated together—but it should be. In most cases, a special intervention is not needed to reduce pain.
Common mechanisms behind persistent atypical facial pain
Atypical trigeminal neuralgia and persistent facial pain are often maintained by more than one mechanism at the same time. This is one of the main reasons why standard treatment may fail. A patient may have a partial vascular contact on MRI, but the active pain generator may still be in a peripheral trigeminal branch, a dental-related nerve injury, scar tissue, muscle spasm, viral nerve damage, or central sensitization.
Peripheral trigeminal branch irritation may involve the main trigeminal branches but also supraorbital, infraorbital, mental, alveolar, auriculotemporal, or other smaller branches of the trigeminal nerve. These irritations are often very small and may not be visible on routine MRI, but they can produce severe facial pain when the affected branch becomes hypersensitive.
Post-dental trigeminal nerve pain may appear after tooth extraction, root canal treatment, dental implants, local infection, prolonged jaw opening, or repeated dental procedures. In these cases, the patient may continue to feel tooth-like or gum-region pain even when the tooth itself is no longer the source of the problem.
Postherpetic or herpes-related trigeminal pain may follow shingles or recurrent herpes outbreaks, even after the skin lesions have healed. Viral injury can sensitize the trigeminal nerve or one of its branches, causing burning, hypersensitivity, electric pain, or pain triggered by light touch.
Muscle and TMJ-related irritation may amplify trigeminal pain through chewing muscles, jaw mechanics, bruxism, clenching, or referred pain. These factors may not be the only cause, but they can maintain irritation and make trigeminal nerve pain harder to control.
Scar tissue and local inflammation may irritate small nerve branches after trauma, surgery, dental procedures, infection, or chronic tissue irritation. This type of local pain generator is often missed because it may be too small to appear clearly on imaging.
Central sensitization may develop after long-standing facial pain. The nervous system becomes more reactive, and normal touch, chewing, cold wind, or mild pressure may start to feel painful. This does not mean the pain is psychological. It means that the pain system has become hypersensitive.
Mixed mechanisms are common in persistent atypical facial pain. Treating only one factor may give partial or temporary relief, but long-term improvement usually requires identifying the dominant pain generator and correcting the additional mechanisms that keep the trigeminal nerve irritated.
Contributing factors that can keep atypical trigeminal neuralgia active
In atypical trigeminal neuralgia, treatment often fails not only because the primary pain generator is missed, but also because additional pain-contributing factors are not recognized. These factors may not be the main cause of facial pain, but they can maintain trigeminal nerve irritation, increase nerve sensitivity, delay recovery, and reduce the effect of otherwise appropriate treatment.
The most important contributing factors include previous dental or facial procedures, chronic irritation of peripheral trigeminal branches, muscle tension, TMJ dysfunction, jaw clenching or bruxism, scar tissue, local inflammation, viral nerve injury, sleep disturbance, metabolic or inflammatory conditions, nutritional deficiencies, medication effects, and central sensitization. Therefore, patients must undergo a comprehensive diagnostic protocol, which is often neglected in cases of trigeminal neuralgia due to a lack of awareness regarding its importance in detecting factors that provoke and sustain facial pain.
This does not mean that every patient has all of these factors. The purpose of assessment is to identify which of them are actually active in that patient. Treating only one part of the problem — for example only increasing medication, repeating dental procedures, or focusing only on MRI findings — often gives incomplete or temporary relief.
A more effective approach is to identify the dominant trigeminal pain generator and then correct the contributing factors that keep the nerve irritated. This is why treatment usually requires a carefully selected combination of medication, dose adjustment, trigger control, sleep and metabolic correction when relevant, and sometimes targeted nerve blocks or interventional procedures.
Many patients have already tried one part of this strategy — medication, supplements, physiotherapy, dental treatment, diet changes, or injections — but not the complete mechanism-based approach. This is one of the common reasons why atypical trigeminal neuralgia becomes persistent.
Treatment when standard trigeminal neuralgia therapy has failed
When atypical trigeminal neuralgia does not improve, treatment should not simply repeat the same protocol. The first step is to separate the active mechanisms.
Once the pain generator and contributing factors are identified, treatment usually starts with a targeted combination of medications. This may include sodium-channel blockers, gabapentinoids, baclofen, antidepressants for neuropathic pain, topical treatments, anti-inflammatory support, sleep regulation, and, when clinically appropriate, medications targeting viral or inflammatory mechanisms, as well as various other therapies and procedures.
The goal is not to use many drugs randomly. The goal is to choose a logical combination that covers the mechanisms present in that patient. Many of these drugs, particularly the right combinations, were never previously given to these patients. They had been treated under standard protocols for typical trigeminal neuralgia, which are simply not effective enough here.
Medication often has to be adjusted during the first 6–8 weeks. The first 10 days are especially important because early response, side effects, sedation, dizziness, mood change, sleep quality, and pain pattern changes help guide correction of the plan.
When the correct combination is found and pain remains controlled for 6–8 weeks, the effect is often more stable. In many patients, this avoids another major procedure.
When nerve blocks, Botox, or interventional treatment may help
Interventional treatment may help when medication alone is not enough or when the doctor needs to confirm the pain generator. It must be emphasized that once the cause of the pain is identified, an appropriate combination is often sufficient to control or significantly reduce pain—as mentioned above—making surgical interventions unnecessary for the majority of patients. Patients often assume that because they have already tried medications, they now require a specific procedure, but this is simply not the case.
A selective nerve block can temporarily numb a suspected trigeminal branch. If the pain improves after a precisely targeted block, this gives diagnostic information and may also help break the pain cycle.
Botulinum toxin may help some patients with persistent burning or hypersensitive trigeminal pain, especially when pain is superficial, branch-related, or associated with trigger zones.
Image-guided procedures may be considered when the pain source is small, deep, or close to important anatomical structures. These procedures should be selected according to the exact pain generator, not only according to the diagnosis name.
Gamma Knife, rhizotomy, Gasserian ganglion procedures, or repeat surgical opinions may still be appropriate in selected cases, but they should be considered only after the pain mechanism has been reassessed.

Image: Interventional pain procedure used in trigeminal neuralgia treatment
Can atypical trigeminal neuralgia improve after many years?
Yes. Long-lasting facial pain can still improve, but the treatment must be more precise than simply repeating the same medication or procedure.
When pain has been present for months or years, several mechanisms may be active at once. The nerve may be irritated locally. The brainstem and central pain pathways may become sensitized. Muscles, jaw mechanics, dental history, viral injury, sleep problems, metabolic factors, and previous treatments may all influence the pain threshold.
This does not mean the pain is psychological. It means the pain system has become more reactive and requires a structured plan.
The most important question is not how long the pain has existed. The most important question is whether the real pain generator has ever been correctly identified and treated.
When to seek a second opinion
A second opinion is useful when facial pain continues despite standard trigeminal neuralgia treatment, when the diagnosis is uncertain, or when a major procedure has been recommended.
It is especially important if:
- the pain is constant, burning, aching, pressure-like, or dental-like rather than brief electric shocks only;
- MRI is normal, unclear, or does not match the exact pain pattern;
- carbamazepine, oxcarbazepine, gabapentin, pregabalin, or other medications helped only briefly, partially, or caused limiting side effects;
- pain continued after microvascular decompression, Gamma Knife, rhizotomy, nerve blocks, or other procedures;
- repeated dental treatments, tooth extraction, root canal treatment, or implants did not solve the pain;
- doctors disagree about whether the pain is typical trigeminal neuralgia, atypical trigeminal neuralgia, TMJ pain, dental pain, trigeminal neuropathy, postherpetic pain, or central sensitization;
- another procedure has been recommended, but the true pain generator has not been clearly identified.
The purpose of a second opinion is not only to decide whether surgery is needed. The main purpose is to identify the active pain generator, understand why previous treatment failed, and choose the safest logical next step.
Prognosis of atypical trigeminal neuralgia when treatment has failed
The prognosis of atypical trigeminal neuralgia is different from the prognosis of classical trigeminal neuralgia because the pain mechanism is usually different.
In classical trigeminal neuralgia, carbamazepine or oxcarbazepine often provides strong initial pain control, commonly reported in the range of 70–90% in typical cases. However, long-term medication control is less stable, and many patients eventually need a procedure when medication loses effect or causes side effects. When classical TN is caused by MRI-confirmed vascular compression that matches the symptoms, microvascular decompression has the best long-term results, with many series reporting durable relief in approximately 70–80% of well-selected patients.
In atypical trigeminal neuralgia, the prognosis is less predictable. When pain is constant, burning, aching, post-dental, postherpetic, MRI-negative, or not clearly linked to vascular compression, response to standard medication and classical procedures is usually lower and less durable. In clinical practice and reported series, meaningful improvement with medication-based treatment is often closer to 30–50%, while stable long-term control with medication alone may be closer to 20–30% in difficult continuous-pain cases. These numbers should be understood as approximate clinical ranges, not as fixed outcomes for every patient.
The prognosis improves when treatment is based on the true pain generator rather than only on the diagnosis name. Patients usually do better when peripheral trigeminal branch irritation, post-dental nerve injury, viral nerve injury, scar tissue, local inflammation, muscle or TMJ-related factors, and central sensitization are identified separately and treated together.
Typical trigeminal neuralgia often aims for remission. Atypical trigeminal neuralgia usually aims for control. Success depends mainly on identifying the exact source of irritation and correcting the mechanisms that keep the trigeminal nerve active.
Why an Online Consultation Can Help When Atypical Trigeminal Neuralgia Pain Persists
A video consultation for atypical trigeminal neuralgia can help identify the exact source of your facial pain — one or more pain generators — as well as the factors that trigger and maintain it. This is achieved through a detailed conversation and review of your MRI scans and medical records. During the session, you are instructed to perform specific jaw, facial, or neck movements and finger-pressure tests to see what increases, reduces, or changes your pain. This helps identify which pain source is active. Many of these pain generators and sustaining factors cannot be seen on MRI.
This may sound like examinations you have already had. It is not — because what matters most is not the test itself, but who interprets it. Only a specialist with deep knowledge of pain anatomy in this region knows which questions to ask, where to instruct you to press, which movements to test, and how to confirm which pain source is active. This is not just another opinion.
You will also receive advice on which contributing factors that trigger and sustain pain should be investigated — such as hormonal factors, vitamin deficiencies, side effects of other medications, inadequate diet, metabolic disorders, physical strain during daily activities or work, and other overlooked contributors. In many patients who have already visited several specialists, these factors have still not been fully investigated.
Once the main pain mechanism behind atypical trigeminal neuralgia symptoms is identified, treatment follows: a targeted combination of medications covering all identified mechanisms, carefully introduced and adjusted over 6–8 weeks, with regular communication during the treatment period, especially when you need it. The aim is to achieve early pain reduction during the first 10 days, then stabilize the result over the following weeks for a longer-lasting effect. When selecting medications, we take into account whether patients are older or have other health conditions, and we prescribe them in a safe combination for the shortest possible duration to avoid medication overload. All recommendations are explained during the conversation and are also given in a written medical report.
Many patients assume that because medications have already failed, a specific procedure is now needed. In most cases, this is not true — previous medications often did not cover the right combination of mechanisms, were not individualized, or were not adjusted over a sufficient period of time. In the minority of patients where medication alone is not sufficient, we recommend the exact intervention or procedure — chosen based on the confirmed pain generator, not assumptions.
Based on our written medical report, reimbursement may often be possible if your insurance plan allows it.
Start Your Telehealth Consultation for Atypical Trigeminal Neuralgia
If your facial pain treatment has failed, if the diagnosis is uncertain, or if pain continued after medication, nerve blocks, Gamma Knife, rhizotomy, dental procedures, or microvascular decompression — a focused telehealth consultation can help identify the true pain generator and the most logical next step.
- ✔ First, send a short message describing your facial pain, diagnosis, previous treatments, and MRI findings
- ✔ You’ll receive a reply within 24 hours if and how we can help — including the consultation cost and a suggested time
- ✔ Only then, you can send your medical documentation you have, like MRI/CT reports, dental reports, medication history, and previous procedure details
- ✔ The video consultation focuses on pain-pattern analysis, facial pain anatomy, trigger mapping, and previous treatment response
- ✔ The consultation is followed by a written report and follow-up questions for treatment adjustment when needed
- ✔ Secure payment via PayPal invoice, credit card, or bank transfer
Consultation fees typically range from $180–250, depending on the complexity of your case.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Based on our medical report, reimbursement can often be obtained if your insurance plan allows it.
This is within the usual range for specialist telehealth consultations worldwide. Many patients use telehealth consultations for second opinions when trigeminal neuralgia treatment has failed, when MRI findings are unclear, or when another procedure has been recommended.
Online pain consultation for atypical trigeminal neuralgia in detail
Schematic explanation of the video consultation for atypical trigeminal neuralgia
See the page “Possible Reasons for Poor Pain Treatment Effectiveness of Atypical Trigeminal Neuralgia” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
Treatment of complex cases of trigeminal neuralgia can be analysed by artificial intelligence (AI)
Can trigeminal neuralgia treatment fail because the pain is actually atypical trigeminal neuralgia?
Yes. Treatment can fail when facial pain is treated as typical trigeminal neuralgia, but the pain pattern is actually atypical. Typical trigeminal neuralgia usually causes brief electric-shock attacks with pain-free intervals and may be linked to vascular compression near the brainstem. Atypical trigeminal neuralgia may be constant, burning, aching, dental-like, post-dental, postherpetic, MRI-negative, or only partially responsive to medication. In these cases, the active pain generator may be outside the classical vascular compression site. Treatment must therefore identify the real mechanism, not only repeat the standard trigeminal neuralgia protocol.
Why does facial pain continue despite carbamazepine or oxcarbazepine?
Carbamazepine and oxcarbazepine can reduce nerve excitability, and they often work well in classical trigeminal neuralgia. However, facial pain may continue if the main problem is not only nerve hyperexcitability. Atypical trigeminal neuralgia may involve peripheral trigeminal branch irritation, dental-related nerve injury, scar tissue, inflammation, viral nerve damage, muscle spasm, TMJ-related irritation, local compression, or central sensitization. In that situation, medication may help only partially or temporarily. The next step is not simply increasing the dose, but identifying which mechanisms are keeping the trigeminal nerve irritated.
Why can atypical trigeminal neuralgia have a normal MRI?
A normal MRI does not exclude atypical trigeminal neuralgia or trigeminal nerve irritation. MRI is useful for detecting tumors, multiple sclerosis, vascular compression, and other structural causes, but many clinically important irritations are too small, too peripheral, or too functional to appear clearly on routine imaging. Small irritated nerve branches in the face, scar tissue after dental work, local inflammation, muscle spasm, trigger-zone hypersensitivity, postherpetic nerve injury, or early peripheral nerve sensitization may not produce a visible MRI abnormality. In these cases, pain anatomy, triggers, history, and functional testing become very important.
Can facial pain persist after microvascular decompression if it was not typical trigeminal neuralgia?
Yes. Microvascular decompression is most effective when the patient has classical trigeminal neuralgia with brief electric-shock attacks, pain-free intervals, clear trigger zones, and MRI evidence of vascular compression that matches the symptoms. If the pain is constant, burning, post-dental, postherpetic, bilateral, poorly responsive to medication, or not clearly matched by MRI, MVD is less predictable. Pain after MVD may mean that vascular compression was not the true pain generator, or that another mechanism was active at the same time. Peripheral nerve irritation, dental injury, viral nerve damage, TMJ-related pain, scar tissue, or central sensitization may still require treatment.
What does it mean if trigeminal neuralgia becomes constant instead of electric-shock pain?
When trigeminal neuralgia becomes constant, burning, aching, pressure-like, or dental-like, the pain mechanism may have changed or may not have been classical trigeminal neuralgia from the beginning. Classical TN usually causes brief attacks with pain-free intervals. Constant pain suggests a more complex mechanism, such as atypical trigeminal neuralgia, post-dental trigeminal nerve pain, postherpetic neuralgia, peripheral branch irritation, muscle/TMJ contribution, or central sensitization. This distinction matters because procedures that work well for classical TN may be less predictable when pain is continuous and the true pain generator has not been identified.
How is the true pain generator found in atypical trigeminal neuralgia?
The true trigeminal pain generator is found by combining medical history, facial pain anatomy, trigger analysis, imaging review, previous treatment response, and guided functional examination. The doctor analyzes where the pain starts, where it spreads, whether it is electric, burning, aching, pressure-like, dental-like, or deep, and whether chewing, talking, brushing teeth, cold wind, jaw movement, facial pressure, or neck movement changes the pain. During consultation, the patient may be guided to press specific points on the face, jaw, cheek, temple, forehead, gum region, or around the eye. Changes in pain can help localize the irritated trigeminal branch or contributing structure.
Can a small trigeminal nerve branch in the face cause severe facial pain?
Yes. A small peripheral branch of the trigeminal nerve can cause severe facial pain when it becomes irritated or sensitized. The irritation may involve the supraorbital, infraorbital, mental, alveolar, auriculotemporal, or other smaller branches. These structures may be only a few millimeters wide and may not be visible on routine MRI. Pain may appear around the eye, forehead, cheek, teeth, gum, jaw, chin, temple, or ear-region. This is why atypical trigeminal neuralgia often requires anatomical pain mapping rather than only repeating MRI interpretation.
Can dental treatment trigger atypical trigeminal neuralgia or persistent facial pain?
Dental procedures usually do not cause classical trigeminal neuralgia from vascular compression near the brainstem, but they can trigger or unmask trigeminal nerve pain. Pain may begin after tooth extraction, root canal treatment, dental implants, local infection, prolonged jaw opening, or repeated dental procedures. The patient may continue to feel tooth-like or gum-region pain even when the tooth itself is no longer the source. In these cases, repeated dental work may not solve the problem and can sometimes worsen nerve sensitivity. The focus should shift to the involved trigeminal branch and the neuropathic pain mechanism.
Can herpes or shingles cause atypical trigeminal neuralgia-like facial pain?
Yes. Shingles and recurrent herpes outbreaks can affect trigeminal nerve pathways and produce persistent facial pain. After shingles, postherpetic trigeminal pain may cause burning, hypersensitivity, electric pain, or pain triggered by light touch. Recurrent herpes may also sensitize trigeminal pathways, especially when symptoms repeatedly affect the same facial or oral region. In these cases, the problem is not a blood vessel pressing on the nerve near the brainstem, but viral nerve injury or inflammation. Treatment follows a neuropathic pain strategy and may also consider antiviral or inflammatory factors when clinically appropriate.
Why can TMJ, muscle tension, or bruxism keep trigeminal facial pain active?
TMJ dysfunction, chewing muscle tension, bruxism, clenching, and repetitive jaw activity can amplify trigeminal facial pain. These factors may not be the only cause, but they can maintain nerve irritation, change local pain thresholds, and create overlapping pain patterns in the jaw, cheek, temple, teeth, ear-region, or face. In atypical trigeminal neuralgia, treatment may fail if the neurological pain generator is recognized but mechanical and muscular contributors are ignored. A complete assessment looks at trigeminal nerve irritation, jaw mechanics, facial muscles, previous dental history, and central sensitization together.
What contributing factors can keep atypical trigeminal neuralgia active?
Atypical trigeminal neuralgia may persist because additional pain-contributing factors are not recognized. These may include previous dental or facial procedures, chronic irritation of peripheral trigeminal branches, muscle tension, TMJ dysfunction, jaw clenching, bruxism, scar tissue, local inflammation, viral nerve injury, sleep disturbance, metabolic or inflammatory conditions, nutritional deficiencies, medication effects, and central sensitization. These factors may not be the main cause of facial pain, but they can maintain trigeminal nerve irritation and reduce the effect of otherwise appropriate treatment. The goal is to identify which factors are active in that patient and correct them together.
What treatment is used when standard trigeminal neuralgia therapy has failed?
When standard trigeminal neuralgia therapy has failed, treatment should not simply repeat the same protocol. The first step is to separate the active mechanisms. Once the pain generator and contributing factors are identified, treatment often begins with a targeted combination of medications. This may include sodium-channel blockers, gabapentinoids, baclofen, antidepressants for neuropathic pain, topical treatment, anti-inflammatory support, sleep regulation, and therapies directed at viral or inflammatory mechanisms when appropriate. The goal is not to use many drugs randomly, but to choose a logical combination that fits the patient’s pain mechanism.
Why are medications adjusted over 6–8 weeks in atypical trigeminal neuralgia?
Medication adjustment over 6–8 weeks is often needed because atypical trigeminal neuralgia usually has more than one active mechanism. The first 10 days are especially important because early response, side effects, sedation, dizziness, sleep quality, mood change, and changes in the pain pattern help guide correction of the plan. If the correct combination is found and pain remains controlled for 6–8 weeks, the result is often more stable. In many patients, this reduces the need for another major procedure and helps avoid repeating treatments that failed because the true pain generator was not identified.
If medication has failed for atypical trigeminal neuralgia, is an intervention necessary, or can a better medication combination still help?
An intervention is not automatically necessary just because previous medication did not help. In many patients, the earlier treatment was based on the standard protocol for classical trigeminal neuralgia, while the actual pain was maintained by a different or mixed mechanism. Medication may still help when the pain generator is reassessed and treatment is redesigned to match the specific combination of nerve irritation, post-dental or viral injury, muscle or TMJ-related factors, local inflammation, and central sensitization.
An intervention is considered when the responsible nerve branch or other pain generator has been sufficiently localized and a properly selected, adjusted, and adequately monitored medication plan has still not provided enough relief. The procedure should therefore be chosen because it targets a confirmed mechanism, not simply because one or several previous drugs were unsuccessful.
Why can destructive trigeminal procedures be less predictable or even worsen atypical facial pain?
Destructive procedures such as radiofrequency rhizotomy, balloon compression, glycerol rhizolysis, and, in a different way, Gamma Knife work by reducing pain transmission through the trigeminal nerve. This can be effective in classical trigeminal neuralgia with brief electric-shock attacks, but results are less predictable when the pain is constant, burning, aching, post-dental, postherpetic, or caused by a peripheral trigeminal branch. In these situations, the procedure may create facial numbness, dysesthesia, painful numbness, corneal sensory loss, or anesthesia dolorosa without eliminating the original pain generator.
The likelihood of individual complications is not the same for every patient. It depends on the exact pain pattern, the involved trigeminal division, existing facial numbness, previous procedures, MRI findings, and the planned technique. An experienced neurosurgeon with expertise in facial pain can usually estimate which complications are most relevant in an individual patient by reviewing these factors, although no risk can be predicted with complete certainty.
When do nerve blocks, Botox, or image-guided procedures help atypical trigeminal neuralgia?
Nerve blocks, Botox, or image-guided procedures may help when medication alone is not enough or when the doctor needs to confirm the pain generator. A selective nerve block can temporarily numb a suspected trigeminal branch. If the pain improves after a targeted block, this gives diagnostic information and may also help break the pain cycle. Botox may help some patients with persistent burning or hypersensitive trigeminal pain, especially when pain is superficial, branch-related, or associated with trigger zones. Image-guided procedures are most useful when they are directed at a clearly identified branch or local source of irritation.
Can atypical trigeminal neuralgia improve after months or years of facial pain?
Yes. Atypical trigeminal neuralgia can still improve after months or years of facial pain, but treatment has to be more precise than simply repeating the same medication or procedure. Long-lasting pain often means that several mechanisms are active at the same time: local nerve irritation, dental-related nerve injury, viral nerve injury, muscle or TMJ factors, scar tissue, sleep disturbance, metabolic factors, and central sensitization. This does not mean the pain is psychological. It means the pain system has become more reactive. Improvement is more likely when the real pain generator and contributing factors are identified and treated together.
What is the prognosis of atypical trigeminal neuralgia when treatment has failed?
The prognosis of atypical trigeminal neuralgia is less predictable than classical trigeminal neuralgia. In difficult continuous-pain cases, meaningful improvement with medication-based treatment may be closer to 30–50%, while stable long-term control with medication alone may be closer to 20–30%. These numbers are approximate clinical ranges, not fixed outcomes for every patient. The prognosis improves when treatment is based on the true pain generator rather than only on the diagnosis name. Atypical trigeminal neuralgia usually aims for stable control, significant pain reduction, and prevention of further sensitization rather than one-procedure remission.
When should I seek a second opinion for atypical trigeminal neuralgia?
A second opinion is useful when facial pain continues despite standard trigeminal neuralgia treatment, when the diagnosis is uncertain, or when another procedure has been recommended. It is especially important if pain is constant, burning, aching, pressure-like, dental-like, MRI-negative, post-dental, postherpetic, or poorly responsive to medication. It is also important when pain continued after microvascular decompression, Gamma Knife, rhizotomy, nerve blocks, or dental procedures. The purpose of a second opinion is not only to decide whether surgery is needed, but to identify the active pain generator and choose the safest logical next step.
Can an online consultation help identify the atypical trigeminal neuralgia pain generator?
Yes. An online consultation can help identify the atypical trigeminal neuralgia pain generator because the diagnosis depends heavily on pain pattern, triggers, anatomical distribution, previous treatment response, and guided functional testing. Before the consultation, MRI, CT, dental reports, operative reports, medication history, and procedure results can be reviewed. During the video call, the patient can be guided to press specific facial points or perform small jaw, neck, or facial movements. If pain changes during these tests, this can help localize the irritated trigeminal branch or contributing structure and guide a mechanism-based treatment plan.