Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 07, 2026
Who this page is for
This page is for patients with intercostal neuralgia — including postherpetic and non-herpetic forms — who continue to experience pain along the ribs, chest, or upper abdomen despite previous treatment.
Pain usually persists because not all factors irritating the intercostal nerve have been properly identified and treated — in many patients, nerve hypersensitivity coexists with local irritators such as muscle spasm or residual inflammation. In most cases, adequate pain control is achieved with a well-chosen combination of medications that addresses both neural and local components, sometimes supported by vitamin therapy. If pain still persists, image-guided intercostal nerve blocks or other targeted procedures may be considered.
A detailed telehealth consultation allows a comprehensive evaluation of all contributing factors and guidance on the most effective treatment combination.
Persistent intercostal pain rarely means irreversible nerve damage — most often, it reflects an incomplete identification of all pain generators. If you are unsure whether an online consultation can help after all previous tests and treatment, read why this consultation is different. The specialist who can identify the true pain generator does not necessarily need to be located in your country.
When patients usually seek a second opinion for intercostal neuralgia
- Chest or upper abdominal nerve pain persists despite medications or initial treatment
- Pain returns or keeps recurring after temporary improvement
- The pain is thought to come from the heart, lungs, or another internal organ — but tests are normal
- The diagnosis feels unclear (intercostal neuralgia vs thoracic radiculopathy, costochondritis, or post-herpetic pain)
- You are considering injections, nerve blocks, or other procedures
Intercostal Neuralgia — Quick Summary (Read This First)
- Intercostal neuralgia is nerve pain caused by irritation, inflammation, or injury of the intercostal nerves. These nerves run along the lower edge of each rib and carry sensation from the chest wall and upper abdominal wall.
- Intercostal neuralgia usually causes sharp, burning, stabbing, or belt-like pain along the ribs, chest, or upper abdomen. The pain is often one-sided and may worsen with movement, coughing, sneezing, deep breathing, or pressure along the rib.
- Intercostal neuralgia can mimic heart, lung, breast, stomach, liver, or other internal organ pain. Many patients undergo cardiac, pulmonary, abdominal, or breast testing before the nerve-related source of pain is recognized.
- Intercostal neuralgia may occur even when CT or MRI scans look normal. Local inflammation, muscle spasm, fascial irritation, rib mechanics, or small areas of nerve irritation can remain invisible on routine imaging.
- The main causes of intercostal neuralgia include postherpetic neuralgia after shingles, local muscle or fascial irritation, trauma, surgery, rib-spine dysfunction, and thoracic nerve root compression. In some patients, several causes coexist, so focusing on only one suspected source may lead to incomplete treatment.
- The diagnosis of intercostal neuralgia is mainly clinical. Diagnosis is based on pain distribution along one or more intercostal spaces, symptom triggers, local tenderness, sensory changes, exclusion of internal organ disease, and sometimes temporary relief after an intercostal nerve block.
- Intercostal neuralgia treatment should address both the sensitized nerve and local irritators around the rib pathway. Neuropathic medications, anti-inflammatory treatment, muscle relaxants, topical lidocaine or capsaicin, physical therapy, breathing exercises, and posture correction may be combined depending on the mechanism.
- Intercostal neuralgia treatment often fails when only one part of the pain mechanism is treated. Pain can persist if nerve hypersensitivity, muscle spasm, local inflammation, rib mechanics, fascial adhesions, breathing-pattern dysfunction, metabolic factors, or central sensitization are not addressed together.
- When intercostal neuralgia persists, the next step is reassessment rather than simply repeating the same medication. The goal is to identify the exact pain generator, the pathological process affecting it, and the contributing factors that continue to maintain pain over time.
- Intercostal nerve blocks can help confirm the pain source and may also reduce symptoms. Temporary pain relief after a local anesthetic block supports the diagnosis, while corticosteroid or other targeted injections may help when inflammation or focal nerve irritation is present.
- Procedures for intercostal neuralgia are considered in selected persistent or refractory cases. Intercostal nerve blocks, pulsed radiofrequency, radiofrequency ablation, or rarely DRG or spinal cord stimulation may be considered when pain is localized, severe, and resistant to optimized conservative treatment.
- Intercostal neuralgia prognosis is usually good when the true pain generator and local irritators are identified. Many non-PHN cases improve within several weeks of targeted treatment, while postherpetic intercostal neuralgia may require longer multimodal management.
- A second opinion is especially useful when intercostal neuralgia pain persists despite medication, when organ tests are normal but chest or abdominal pain continues, or when injections or procedures are being considered. A structured review can clarify whether pain comes from the intercostal nerve, postherpetic neuralgia, thoracic radiculopathy, rib-spine dysfunction, costochondritis, local muscle irritation, or another overlapping condition.
- Online consultation may still help when treatment has failed: read why this consultation is different.
AUDIO: Learn why intercostal neuralgia pain persists despite treatment.
What Is Intercostal Neuralgia?
Intercostal neuralgia is pain caused by irritation, inflammation, or injury of the intercostal nerves — the nerves running along the lower edge of each rib that carry sensation from the chest and upper abdominal wall. The pain is usually sharp, burning, or stabbing, and may follow a narrow “belt-like” line across the chest or upper abdomen.
In many cases, intercostal neuralgia develops without visible changes on CT or MRI scans. That is why local inflammation or persistent muscle spasm compressing or irritating the nerve between two ribs are often missed, leading to prolonged or recurrent pain even when imaging appears normal.

Image: Anatomy of the intercostal nerve and presentation of intercostal neuralgia. Learn more about nerve anatomy here.
Causes of Intercostal Neuralgia
Intercostal neuralgia can occur from many local or systemic conditions affecting the thoracic wall and spine, including:
- Local inflammation or muscle spasm along the course of the intercostal nerve — most often in its proximal part near the spine — can irritate or compress the nerve. Because the intercostal nerve is long and travels through several layers of muscles, fascia, and rib articulations, irritation may occur at different points along its path and still produce the same characteristic chest-wall pain. These local irritators can cause pain on their own (≈10–20%) or, more commonly, coexist with another underlying cause such as a rib–spine joint dysfunction, postherpetic neuralgia or postoperative scarring. Treatment failure often happens because attention is focused on only one suspected location (e.g., the costovertebral joint), while other structures along the nerve’s course — muscle spasm, fascial adhesions, or rib mechanics — continue to irritate the nerve. In most prolonged cases, pain persists not because the nerve cannot heal, but because the actual sites of irritation along its pathway were never identified and treated.
- Postherpetic neuralgia (PHN) after shingles (sometimes even without visible skin changes) along a thoracic dermatome — ≈45–55%.
- Minor trauma or rib fracture, even when not detected on X-ray — ≈10–15%.
- Thoracic disc herniation or foraminal stenosis compressing the nerve root — ≈5–10%.
- Post-surgical pain, especially after thoracotomy, mastectomy, or chest drain insertion — ≈20–25% (of which 5–10% remain severe and persistent beyond 6 months).
- Tumors, infections, or metabolic neuropathies (such as diabetes) — <5% (rare).
In some patients, the pain cycle is maintained long-term by both nerve hypersensitivity and secondary irritants (such as inflammation and muscle tension). For effective treatment in cases with neuropathic pain, these local irritants must be detected and treated simultaneously.
Symptoms and Pain Characteristics
Pain in intercostal neuralgia is usually unilateral and follows one or more ribs. Common features include:
- Sharp, burning, or stabbing pain along the rib, chest, and/or upper abdominal wall.
- Worsening pain with movement, coughing, sneezing, or deep breathing.
- Local tenderness and palpable muscle tightness near the spine or rib angle.
- Numbness, tingling, or hypersensitivity of the skin in the same area.
A key clinical feature is that intercostal neuralgia can often imitate internal organ pain — such as heart, lung, stomach, or liver disorders. Many patients undergo extensive testing for cardiac or abdominal diseases before realizing the pain originates from the intercostal nerves.
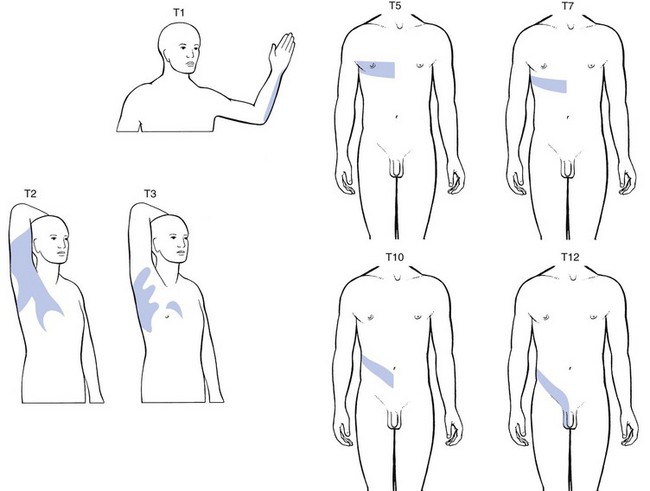
Image: The dermal presentation of pain during intercostal neuralgias (T1–T12).
Diagnosis of Intercostal Neuralgia
Diagnosis is mainly clinical and based on pain distribution, history, and tests for exclusion of visceral causes.
Important diagnostic steps include:
- Careful pain mapping along one or more intercostal spaces.
- Palpation helps identify tender trigger points near the rib or paraspinal muscles. Targeted movements during examination help determine which muscle actions increase or reduce the pain.
- Excluding internal organ causes (heart, lungs, stomach, gallbladder) through targeted tests.
- MRI or CT scans of the thoracic spine and chest wall, mainly to rule out structural lesions — minor nerve inflammation or muscle spasm often remain invisible.
- A diagnostic nerve block uses a local anesthetic to confirm the source of pain, specifically if the pain in the affected area temporarily resolves after the injection.
It is important to be examined in person or during a video consultation by a specialist who understands the pain anatomy of this region and knows how to check the many possible causes of this pain — often around 20 different nerve, muscle, disc, viral, inflammatory, or sensitization-related mechanisms.
Treatment of Intercostal Neuralgia
Treatment aims to reduce both nerve sensitivity and local irritants (such as compressions, inflammation and muscular tension) that perpetuate the pain cycle.
Conservative therapy
- Gentle stretching and breathing exercises to relieve pressure around the ribs.
- Physical therapy focused on thoracic mobility and posture.
- Heat therapy or ultrasound to relax muscle spasm.
Medication
- Neuropathic pain drugs such as gabapentin, pregabalin, or tricyclic antidepressants.
- Anti-inflammatory medications– NSAIDs or short corticosteroid courses for local inflammation.
- Topical treatments (lidocaine or capsaicin patches) for localized burning pain.
- Muscle relaxants when spasm contributes to compression.
Long-term remission is often achieved when sensitized nerve, local nerve irritants and muscle causes are treated simultaneously. Very often, even in chronic cases, only an individualized combination of medications adressing all pain sources with adjustments in doses and types over 4 to 8 weeks can significantly help.
Previous medication failure does not always mean medication cannot help; in many persistent cases, the problem is that the right combination of mechanisms was not treated together. In most cases, you don’t need a special intervention to reduce pain.
Procedural treatments
- Intercostal nerve blocks with local anesthetic and corticosteroid.
- Radiofrequency ablation or pulsed RF for long-lasting relief in chronic cases.
- Targeted treatment of the underlying cause, such as spinal or rib pathology.
When postherpetic intercostal neuralgia (PHN) is present, therapy focuses on desensitizing the affected nerve and improving nerve recovery.
Before contacting us, please read our Privacy Policy and Terms of Use.
Online pain consultation in detail for intercostal neuralgia
Schematic explanation of the video consultation in intercostal neuralgia
Answers to questions about the process and success of video consultations for intercostal neuralgia
See the page “Possible Reasons for Poor Pain Treatment Effectiveness in Intercostal Neuralgia” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
When Pain Persists — Chronic Intercostal Neuralgia
Chronic intercostal neuralgia most often reflects a combination of mechanisms rather than a single ongoing cause. The initial trigger may be nerve injury or irritation, but persistent pain is usually maintained by ongoing nerve sensitization, altered signal processing along the intercostal nerve pathway, and additional mechanical or functional factors that continue to provoke the affected nerve.
A key reason for this persistence is that these mechanisms are not analyzed at three critical levels — the exact structure generating the pain, the underlying pathological process, and the contributing factors that continue to maintain it over time.
Persistent pain usually does not mean that the condition is untreatable — only that the true pain generator has not yet been fully identified, or that previous treatment has addressed only part of the underlying mechanism.
A structured reassessment of the pain mechanisms is therefore often the key step in understanding why symptoms persist and what should be targeted next.
In rare, treatment-resistant cases, interventional options such as pulsed radiofrequency (PRF) or neuromodulation (DRG or spinal cord stimulation) may be considered. These techniques are most often used for postherpetic intercostal neuralgia, but can also help in other chronic, localized intercostal neuralgias when conventional therapy and nerve blocks fail.
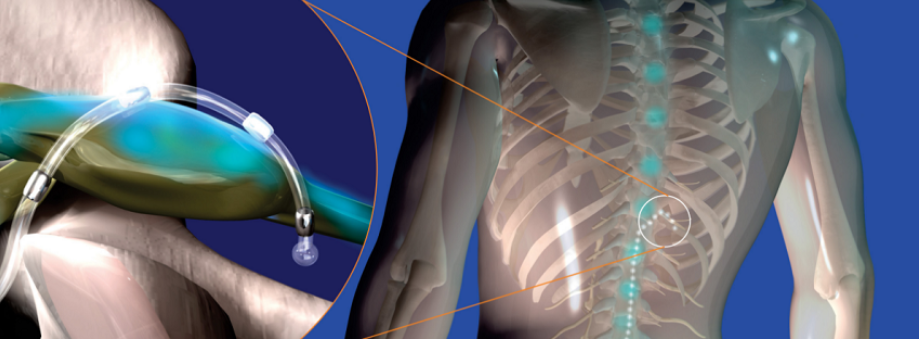
Image: A micro-lead wire for stimulation is positioned around the Dorsal Root Ganglion (DRG), which is the specific control center for the painful nerve. This wire connects to a small electrical device with a battery (the pulse generator), which is implanted under the skin, usually on the side of the abdomen or the upper trunk.
Differential Diagnosis — Intercostal Neuralgia Mimicking Internal Organ Diseases
Intercostal neuralgia frequently mimics internal organ pain such as:
- Cardiac pain (angina, myocardial ischemia)
- Pulmonary pain (pleurisy, pulmonary embolism)
- Gastrointestinal pain (gastritis, gallstones, reflux)
Recognizing the nerve-related origin prevents unnecessary procedures and ensures appropriate pain management. Most organ illnesses can be mimicked by a nerve lesion. (e.g., chest, heart, breast, abdomen, kidneys).
Treatment of Contributing Factors in Intercostal Neuralgia
Effective treatment of intercostal neuralgia always begins with identifying the primary pain generator — whether the dominant source of symptoms is intercostal nerve irritation, postherpetic nerve damage, thoracic spine pathology, or local mechanical irritation along the course of the nerve.
However, in many patients, pain persists not only because of the primary cause, but because additional contributing factors are not recognized or adequately addressed. These factors rarely act as the sole cause of pain, but they can maintain nerve irritation, increase pain sensitivity, delay recovery, and reduce the effectiveness of otherwise appropriate treatment.
For that reason, successful management requires not only identifying the dominant source of pain, but also understanding the broader mechanical, neurological, and systemic context in which the pain persists.
What contributing factors may play a role in intercostal neuralgia?
• Rib mechanics and thoracic spine dysfunction — Dysfunction of costovertebral joints, thoracic segments, or rib alignment may maintain continuous mechanical irritation of the nerve.
• Repetitive strain and sustained posture — Prolonged sitting, computer work, driving, or repetitive trunk movements can perpetuate irritation along the intercostal space.
• Breathing pattern dysfunction — Pain-related shallow breathing (splinting) increases tension in intercostal muscles, reduces rib mobility, and can perpetuate local nerve irritation — creating a cycle that maintains symptoms even when the primary cause is partially treated.
• Postherpetic nerve sensitization — Even after resolution of skin lesions, the nerve may remain hypersensitive, maintaining burning or stabbing pain.
• Central sensitization — The nervous system may become more reactive over time, amplifying pain signals even when the original irritation is reduced.
• Metabolic factors, pro-inflammatory diet and low-grade inflammation — Obesity, insulin resistance, chronic inflammation, and processed/high-sugar diet increase pain sensitivity and impair recovery.
• Nutritional deficiencies — Low levels of vitamin D, vitamin B12, magnesium, or iron may contribute to nerve dysfunction and slower healing.
• Vitamin-related factors — Both deficiency and excess of vitamin B6 may contribute to burning pain, tingling, or hypersensitivity.
• Sleep disturbances and pain cycle — Poor sleep increases pain perception and reduces recovery capacity.
• Stress and increased muscle tone — Stress does not cause the pain, but it increases muscle tension and nervous system reactivity, maintaining symptoms.
• Medications and previous treatments — Long-term use of pain medications, repeated ineffective treatments, or certain drugs (such as statins in some patients) may contribute to muscle-related symptoms or alter pain perception without resolving the underlying mechanism.
• Other medical conditions and comorbidities — Diabetes, autoimmune diseases, thyroid disorders, and chronic inflammatory states may increase nerve sensitivity and reduce treatment response.
• Biomechanical chain dysfunction — Dysfunction in the shoulders, thoracic spine, or even abdominal wall can redistribute load and maintain irritation along the nerve pathway.
• Physical inactivity and deconditioning — Reduced movement leads to muscle stiffness, reduced rib mobility, and increased pain sensitivity.
Why this matters in practice
In many cases, treatment fails because the primary pain generator is not correctly identified, and therapy is directed only at one part of the problem — most often medications alone or a single presumed anatomical source. Conversely, even when the main cause is recognized, failure to address contributing factors often leads to only partial or temporary improvement.
The most effective approach is a carefully selected combination of treatment that addresses both the dominant pain source and all relevant contributing factors. An incomplete approach — even when it includes individually effective methods — is one of the most common reasons why intercostal neuralgia becomes persistent or recurrent.
In practice, many patients try to address parts of this problem on their own — through stretching, posture correction, anti-inflammatory diet, supplements, or different medications. While these approaches can be helpful, they rarely lead to lasting improvement if the primary pain generator is not clearly identified and treated. On the other hand, even well-targeted medical treatment may fail if contributing factors are not recognized and corrected.
Many patients reading this recognize that they have already tried one part of this approach — but not the complete strategy. This is one of the most common reasons why intercostal neuralgia becomes chronic.
Prognosis and Long-Term Management
When the underlying nerve irritation and local nerve irritants are both treated, most patients experience sustained improvement. Persistent cases benefit from stepwise pain management combining physical therapy, medication, and minimally invasive procedures.
Most patients with non-PHN intercostal neuralgia achieve significant improvement within 6–8 weeks of targeted treatment. PHN-related cases may require longer management, but over 70% experience meaningful pain reduction with combined therapy.
Why an Online Consultation Can Help When Intercostal Neuralgia Pain Persists
A video consultation for intercostal neuralgia can help identify the exact source of your chest, rib, or upper abdominal nerve pain — one or more pain generators — as well as the factors that trigger and maintain it. This is achieved through a detailed conversation and review of your MRI scans and medical records. During the session, you are instructed to perform specific breathing, trunk, rib, or finger-pressure tests to see what increases, reduces, or changes your pain. This helps identify which pain source is active. Many of these pain generators and sustaining factors cannot be seen on MRI.
This may sound like examinations you have already had. It is not — because what matters most is not the test itself, but who interprets it. Only a specialist with deep knowledge of pain anatomy in this region knows which questions to ask, where to instruct you to press along the ribs or chest wall, which breathing or trunk movements to test, and how to confirm which pain source is active. This is not just another opinion.
When pain remains unresolved despite treatment in your country, what matters is not whether the specialist works abroad, but whether they can identify the true pain generator and the mechanisms keeping it active. Recommendations are adapted to the tests and treatments realistically available where you live, and most local doctors are willing to apply them, often leading to substantial improvement.
You will also receive advice on which additional factors that trigger and sustain pain should be investigated — such as vitamin deficiencies, side effects of other medications, inadequate diet, metabolic disorders, postherpetic nerve irritation, thoracic spine or rib-related mechanical strain, physical overload during daily activities or work, and other overlooked contributors. In many patients who have already visited several specialists, these factors have still not been fully investigated.
Once the main pain mechanism behind intercostal neuralgia symptoms is identified, treatment follows: a targeted combination of medications covering all identified mechanisms, carefully introduced and adjusted over 6–8 weeks, with regular communication during the treatment period, especially when you need it. The aim is to achieve early pain reduction during the first 10 days, then stabilize the result over the following weeks for a longer-lasting effect. When selecting medications, we take into account whether patients are older or have other health conditions, and we prescribe them in a safe combination for the shortest possible duration to avoid medication overload. All recommendations are explained during the conversation and are also given in a written medical report.
Many patients assume that because medications have already failed, a specific procedure is now needed. In most cases, this is not true — previous medications often did not cover the right combination of mechanisms, were not individualized, or were not adjusted over a sufficient period of time. In the minority of patients where medication alone is not sufficient, we recommend the exact intervention or procedure — such as a targeted intercostal nerve block or another image-guided pain procedure — chosen based on the confirmed pain generator, not assumptions.
Based on our written medical report, reimbursement may often be possible if your insurance plan allows it.
Intercostal Neuralgia — Start Your Telehealth Consultation
If you have persistent intercostal neuralgia or unexplained nerve pain on the chest or abdomen that continues despite treatment, a detailed telehealth consultation can help identify all sources of pain and plan a tailored therapy covering both the neuropathic pain (sensitized nerve) and any peripheral irritators such as muscle spasm or trigger points. In many patients, pain persists because these irritators remain undetected or inadequately treated.
If the appropriate pain specialist is not available within your healthcare system, an international consultation can provide the missing expertise. Recommendations are adapted to the tests and treatments realistically available in your country, so your local doctor can use them to improve the treatment plan.
- ✔ Send a short message describing your symptoms, pain location (dermatome), and previous treatments.
- ✔ You’ll receive a reply within 24 hours explaining whether and how we can help, including consultation cost and scheduling.
- ✔ Only then, you can send your medical documentation (reports, imaging, or lab results).
- ✔ The video visit is followed by a written plan and free follow-up questions for 10 days.
- ✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Consultation fees typically range from $180–250, depending on case complexity.
Based on our medical report, reimbursement can often be obtained (if your insurance plan allows it).
This reflects the usual international range for specialist telehealth. A session helps determine whether the pain is due to
PHN alone or also to local irritators, and whether optimized medication, physical therapy/desensitization,
nerve or sympathetic blocks, or (rarely) RF/neuromodulation may be appropriate.
Questions About Intercostal Neuralgia
What is intercostal neuralgia?
Intercostal neuralgia is nerve pain caused by irritation, inflammation, compression, or injury of one or more intercostal nerves, which run between the ribs. The pain often follows a narrow band across the chest or upper abdomen and may feel burning, stabbing, sharp, or electric. Successful treatment requires more than naming the condition. The specialist must understand the anatomy of pain in this region: the intercostal nerve, ribs, thoracic spine, muscles, fascia, and nearby joints can all contribute. The key is to identify the dominant pain generator, the pathological process affecting it, and the contributing factors that keep the nerve sensitive.
What are the main causes of intercostal neuralgia?
The main causes include postherpetic neuralgia after shingles, post-surgical pain after thoracotomy or chest procedures, rib trauma, thoracic disc herniation, foraminal stenosis, local inflammation, and muscle spasm near the spine or between the ribs. In some patients, several mechanisms coexist. For example, postherpetic nerve sensitization may be worsened by rib stiffness, shallow breathing, or local trigger points. This is why a pain specialist must know which structures in the chest wall can generate pain and which contributing factors can maintain it. Treatment is most effective when it targets both the irritated nerve and the local mechanical or inflammatory factors that continue to provoke it.
Can intercostal neuralgia develop without visible findings on MRI or CT?
Yes. Intercostal neuralgia can persist even when MRI or CT does not show a clear abnormality. Imaging can rule out tumors, fractures, disc disease, or major structural lesions, but it often cannot show small local irritators such as muscle spasm, fascial adhesions, low-grade inflammation, scar-related irritation, or subtle nerve hypersensitivity. Normal imaging therefore does not mean that the pain is not real. It means that the diagnosis must rely on pain anatomy, dermatomal distribution, palpation, movement testing, and sometimes diagnostic nerve blocks. The specialist must know which structures along the rib and thoracic spine can irritate the nerve and how to test them clinically.
What does intercostal neuralgia feel like?
Intercostal neuralgia usually feels like sharp, burning, stabbing, tight, or electric pain following one or more ribs. Many patients describe a belt-like pain that wraps around one side of the chest or upper abdomen. Pain may worsen with deep breathing, coughing, sneezing, twisting, pressure on the ribs, or light touch. Some patients also feel numbness, tingling, or skin hypersensitivity in the same area. The exact pattern matters because it helps identify whether the pain comes from the intercostal nerve itself, a thoracic nerve root, local muscle spasm, rib mechanics, or postherpetic sensitization. This anatomical mapping is essential for choosing the correct treatment.
Can intercostal neuralgia cause pain in the abdomen?
Yes. Lower thoracic intercostal nerves can project pain into the upper abdominal wall, so intercostal neuralgia may feel like stomach, liver, gallbladder, or intestinal pain. This happens because the same thoracic nerves supply the rib area and parts of the abdominal wall. The pain is often one-sided, band-like, and may worsen with movement, breathing, or pressure over the rib or paraspinal region. Correct diagnosis requires knowledge of pain anatomy, because the specialist must distinguish internal organ pain from nerve-related pain coming from the chest wall. If organ tests are normal, intercostal neuralgia should be considered, especially when pain follows a clear dermatome.
Why does intercostal neuralgia pain persist despite treatment?
Intercostal neuralgia often persists because treatment addresses only one part of the problem. A medication may reduce nerve excitability, but local muscle spasm, rib dysfunction, inflammation, scar tissue, posture, breathing restriction, or central sensitization may continue to irritate the nerve. Persistent pain rarely means that nothing can be done. More often, the dominant pain generator and the maintaining factors have not been fully identified. Effective treatment requires knowledge of pain anatomy: the specialist must know all possible pain sources in that region, diagnose which structure is responsible, and exclude other contributors. Only then can medication, physical therapy, nerve blocks, or procedures be selected correctly.
Why do some patients with intercostal neuralgia improve only temporarily?
Temporary improvement usually means that one mechanism was treated, but the full pain system was not. For example, a nerve block may calm the intercostal nerve, but if muscle spasm, rib mechanics, shallow breathing, posture, or local inflammation continue to provoke the nerve, pain may return. Medications may also help partially but fail if the dose, combination, or treatment duration is not adjusted over several weeks. The important question is not only which drug or procedure was used, but whether the anatomy of pain was correctly analyzed. The specialist must identify the primary pain generator, the process inside it, and the contributing factors that keep symptoms active.
Can muscle spasm or local inflammation maintain intercostal neuralgia pain?
Yes. Muscle spasm and low-grade inflammation are common reasons why intercostal neuralgia persists. The intercostal nerve travels through narrow anatomical spaces between ribs, muscles, fascia, and joints. If nearby muscles remain tense or inflamed, they can repeatedly irritate the nerve and keep it hypersensitive. This may happen after shingles, trauma, surgery, prolonged posture, or protective shallow breathing due to pain. These factors may not appear on standard imaging, which is why they are often missed. A specialist who understands pain anatomy must check for local tenderness, trigger points, movement-related pain, breathing-related aggravation, and other signs that the nerve is being irritated by surrounding tissues.
What contributing factors may keep intercostal neuralgia active?
Contributing factors may include rib mechanics, thoracic spine dysfunction, repetitive strain, prolonged sitting, computer work, driving, shallow breathing, postherpetic nerve sensitization, central sensitization, sleep disturbance, stress-related muscle tone, metabolic inflammation, diabetes, thyroid disease, nutritional deficiencies, and deconditioning. These factors rarely act as the only cause, but they can maintain nerve sensitivity and reduce the effect of otherwise correct treatment. This is why successful care requires a complete anatomical and functional analysis, not only a diagnosis label. The specialist must identify which factors are relevant in the individual patient, how they irritate the nerve, and which should be treated, excluded, or monitored over time.
How long can intercostal neuralgia last?
Intercostal neuralgia may last from several weeks to many months, depending on the cause and whether all pain generators are treated. Acute irritation after strain or inflammation may improve relatively quickly. Postherpetic, post-surgical, or chronic mechanically maintained pain may last much longer, especially when local irritators remain active. Long duration does not automatically mean irreversible nerve damage. It often means that the pain mechanism has not been fully mapped. When the sensitized nerve, surrounding muscle spasm, rib mechanics, inflammation, and systemic contributors are addressed together, many patients improve. The key is understanding the anatomy of pain and using a structured treatment plan rather than isolated treatments.
Can intercostal neuralgia mimic heart or lung disease?
Yes. Intercostal neuralgia can mimic angina, pleurisy, pulmonary disease, gallbladder pain, reflux, breast pain, or abdominal disorders. This happens because intercostal nerves cover the chest and upper abdominal wall, and pain from these nerves may be perceived as coming from internal organs. Cardiac, lung, or abdominal causes must be excluded when symptoms suggest them, especially with new chest pain. However, when tests are normal and the pain is one-sided, band-like, touch-sensitive, movement-related, or follows one rib level, intercostal neuralgia becomes more likely. Correct diagnosis requires knowledge of regional pain anatomy so that nerve pain is not mistaken for organ disease or treated with unnecessary procedures.
How is intercostal neuralgia diagnosed?
Intercostal neuralgia is diagnosed by combining pain mapping, medical history, clinical examination, exclusion of internal organ causes, and sometimes diagnostic nerve blocks. The doctor analyzes whether the pain follows one or more intercostal spaces, whether it is triggered by touch, movement, breathing, coughing, or pressure, and whether there are signs of postherpetic, traumatic, spinal, or muscular origin. MRI or CT may be used to rule out thoracic disc disease, tumors, fractures, or chest wall pathology, but normal imaging does not exclude nerve pain. A specialist must understand the anatomy of pain well enough to know which structures can imitate each other and which tests can confirm or exclude each mechanism.
What is the role of physical examination in intercostal neuralgia?
Physical examination helps identify whether pain comes mainly from the intercostal nerve, surrounding muscles, rib mechanics, thoracic spine, or another structure. Palpation may reveal tender trigger points near the ribs, paraspinal muscles, or costovertebral joints. Targeted movements, breathing tests, trunk rotation, and pressure over specific points can show which actions provoke or relieve pain. This matters because imaging may miss functional causes such as spasm, fascial restriction, or local irritation. A specialist familiar with pain anatomy can use examination to map the pain generator and contributing factors. Without this step, treatment may focus only on medication while the mechanical or muscular source continues to irritate the nerve.
What treatments are available for intercostal neuralgia?
Treatment may include neuropathic pain medications such as gabapentin, pregabalin, or tricyclic antidepressants; topical lidocaine or capsaicin; anti-inflammatory medication; muscle relaxants; physical therapy; breathing exercises; heat therapy; and posture or thoracic mobility work. If pain remains focal and resistant, intercostal nerve blocks, paravertebral blocks, pulsed radiofrequency, or neuromodulation may be considered. The best treatment is not the same for every patient. It depends on whether the main mechanism is postherpetic nerve sensitization, local inflammation, muscle spasm, thoracic root irritation, scar tissue, or rib mechanics. Understanding pain anatomy allows the specialist to combine treatments that address both the nerve and the factors maintaining irritation.
What medications help with intercostal neuralgia?
Medications may include gabapentin, pregabalin, tricyclic antidepressants, topical lidocaine, capsaicin patches, NSAIDs, short corticosteroid courses, and muscle relaxants when spasm contributes to nerve irritation. Neuropathic medications reduce abnormal nerve signaling, while anti-inflammatory drugs and muscle relaxants address local irritators around the nerve. In many patients, long-term improvement requires a carefully selected combination rather than one drug alone. Doses often need adjustment over 4–8 weeks. Medication choice should follow the anatomy of pain: the specialist must determine whether the dominant problem is nerve sensitization, local inflammation, muscle compression, postherpetic damage, thoracic spine pathology, or a mixed mechanism.
Can intercostal neuralgia improve without surgery?
Yes. Most patients with intercostal neuralgia improve without surgery when the true pain generator and contributing factors are properly identified. Treatment usually involves medication optimization, physical therapy, desensitization, posture and breathing correction, treatment of muscle spasm or inflammation, and sometimes image-guided nerve blocks. Surgery is rarely needed because most causes are functional, inflammatory, postherpetic, post-surgical, or mechanical rather than a surgically removable lesion. The key is not simply avoiding surgery, but understanding why pain persists. A specialist must know which structures in the rib, thoracic spine, and chest wall can create or maintain pain and how to diagnose and exclude each one before choosing treatment.
How does telehealth help in diagnosing intercostal neuralgia?
Telehealth can help when the specialist uses a structured pain-anatomy approach. Before the consultation, medical reports and imaging can be reviewed. During the video visit, the doctor asks detailed questions about pain location, direction, triggers, skin sensitivity, breathing-related pain, movement-related pain, and previous treatments. The patient can be guided to press specific points near the ribs or spine and perform gentle movements to see what provokes or relieves symptoms. This can help identify whether pain is neuropathic, muscular, postherpetic, spinal, or mixed. Telehealth does not replace emergency care, but for chronic intercostal neuralgia it can guide diagnosis and treatment planning effectively.
Can intercostal neuralgia come from shingles even without a rash?
Yes. Intercostal neuralgia can result from shingles, and in some cases the virus can reactivate without visible blisters. This is called zoster sine herpete. The patient may develop burning, stabbing, band-like pain along one thoracic dermatome, often with touch sensitivity, but the skin may look normal. This can be confused with heart, lung, breast, stomach, liver, or spine disease. Diagnosis requires recognizing the dermatomal pattern and understanding that nerve pain can occur even without rash. If acute viral reactivation is suspected, testing or early antiviral treatment may be considered. Established postherpetic neuralgia requires neuropathic pain treatment and management of local irritators.
What is the difference between neuropathic and muscle-related intercostal pain?
Neuropathic intercostal pain comes from irritation, injury, or hypersensitivity of the intercostal nerve itself. It often feels burning, electric, stabbing, tingling, or touch-sensitive. Muscle-related pain comes from spasm, trigger points, strain, inflammation, or mechanical overload in the intercostal or paraspinal muscles. It may worsen with posture, movement, deep breathing, or pressure over tight muscle bands. In many patients, both mechanisms coexist: muscle spasm irritates the nerve, and the sensitized nerve increases protective muscle tension. This is why the anatomy of pain is important. The specialist must decide which structure is dominant and which secondary factors are maintaining the pain before treatment can be successful.
What is the difference between intercostal neuralgia and costochondritis?
Intercostal neuralgia and costochondritis can produce similar chest pain, but they arise from different anatomical structures and usually require different treatment. Costochondritis is pain originating from the cartilage and joints where the ribs connect to the breastbone, often producing localized tenderness and inflammation near the sternum. Intercostal neuralgia comes from irritation or sensitization of the intercostal nerve itself and typically follows a band-like path along one or more ribs. Successful diagnosis depends on understanding pain anatomy. A specialist must determine whether the dominant pain generator is the nerve, rib cartilage, surrounding muscles, thoracic spine, or a combination of factors. Without identifying the exact source and the contributing factors maintaining pain, treatment may provide only partial or temporary relief.
How is intercostal neuralgia different from pleurisy or lung-related pain?
Intercostal neuralgia and pleuritic or lung-related pain may both worsen with breathing, which is why they are sometimes confused. However, intercostal neuralgia usually follows a dermatomal or band-like pattern along one side of the chest and is often sensitive to touch, pressure, movement, or twisting. Lung and pleural pain is more commonly linked to infection, inflammation, or breathing difficulty and may be accompanied by fever, cough, or abnormal chest imaging. Correct diagnosis requires detailed knowledge of chest pain anatomy and careful exclusion of serious cardiopulmonary disease when necessary. A specialist must determine whether the pain originates from the intercostal nerve, pleura, lungs, ribs, muscles, or thoracic spine and identify any contributing factors that continue maintaining nerve sensitivity and chronic pain.
How effective are intercostal nerve blocks?
Intercostal nerve blocks can be effective when pain is clearly localized to one or more intercostal nerves. A local anesthetic, sometimes combined with corticosteroid, is injected near the painful nerve to interrupt pain signals and reduce local inflammation. Relief may be immediate and can last from hours to weeks or longer. A good response also has diagnostic value because it confirms that the targeted nerve is an important pain generator. However, blocks are not a complete strategy if other contributors remain active. For lasting improvement, the specialist must also assess muscle spasm, rib mechanics, posture, breathing restriction, postherpetic sensitization, and systemic factors that may continue maintaining pain.
What if medications and intercostal nerve blocks do not help?
If medications and nerve blocks do not help, the case should be reassessed rather than simply repeating the same treatment. The pain generator may be different from what was assumed, or several mechanisms may be active at the same time. Thoracic radiculopathy, postherpetic neuralgia, scar-related pain, costovertebral joint dysfunction, myofascial trigger points, central sensitization, or systemic contributors may need to be reconsidered. In selected refractory cases, pulsed radiofrequency, radiofrequency treatment, dorsal root ganglion stimulation, or spinal cord stimulation may be options. But escalation should follow a clear anatomical diagnosis. The specialist must know what exactly is being targeted and why previous treatments failed.
Is intercostal neuralgia dangerous?
Intercostal neuralgia itself is usually not dangerous, but chest or upper abdominal pain must be evaluated carefully because heart, lung, abdominal, or spinal conditions can produce similar symptoms. Once serious causes are excluded, intercostal neuralgia is mainly a pain and quality-of-life problem. It can still be severe, disabling, and frightening because it may mimic internal organ disease. The danger is often misdiagnosis: patients may undergo repeated tests or procedures while the nerve-related pain generator remains untreated. A specialist who understands pain anatomy can help distinguish true nerve pain from organ disease and identify local or systemic factors that keep the nerve hypersensitive.
Can exercise or stretching worsen intercostal neuralgia?
Exercise and stretching can help or worsen intercostal neuralgia depending on the pain mechanism and timing. Gentle breathing exercises, thoracic mobility work, and gradual stretching may reduce muscle tension and improve rib movement. However, forceful twisting, heavy lifting, sudden stretching, or aggressive exercises can aggravate an already irritated nerve, especially in acute phases or when rib mechanics are unstable. The key is to understand the anatomy of pain and determine whether symptoms are driven mainly by nerve sensitization, muscle spasm, inflammation, thoracic spine dysfunction, or postherpetic hypersensitivity. A tailored plan is safer than generic exercise advice, because the wrong movement can repeatedly provoke the same nerve.
If medication has failed for intercostal neuralgia, is an intervention necessary, or can a better medication combination still help?
Previous medication failure does not automatically mean that an intercostal nerve block, radiofrequency procedure, or neuromodulation is necessary. In many patients, treatment was incomplete because it addressed only nerve sensitivity while other mechanisms remained active, such as muscle spasm, local inflammation, rib or thoracic spine dysfunction, fascial irritation, postherpetic nerve injury, or central sensitization. A more carefully selected combination of neuropathic pain medication, anti-inflammatory treatment, muscle relaxation, topical therapy, physical measures, and correction of contributing factors can still provide meaningful improvement even after earlier medications were unsuccessful. An intervention is usually considered only when the pain generator has been sufficiently localized and a properly selected, adjusted, and adequately monitored conservative treatment plan has not produced enough relief.
What are the specific risks and complications of intercostal nerve blocks, radiofrequency procedures, and neuromodulation?
Intercostal nerve blocks may cause bleeding, bruising, infection, temporary numbness, transient worsening of pain, vascular puncture, intravascular injection, local-anesthetic toxicity, or injury to nearby tissues. Because the intercostal nerve lies close to the pleura and lung, pneumothorax is a specific but uncommon complication, particularly with deeper or less accurately guided injections. Pulsed radiofrequency may cause temporary neuritis, dysesthesia, numbness, pain flare, bleeding, infection, or no meaningful improvement. Thermal radiofrequency carries an additional risk of permanent sensory loss, worsened neuropathic pain, or tissue injury. Dorsal root ganglion or spinal cord stimulation may cause infection, lead migration, uncomfortable stimulation, hardware failure, loss of benefit, bleeding, and the need for reprogramming, revision, or device removal.
The likelihood of individual complications is not the same for every patient. An experienced neurosurgeon or pain-intervention specialist can usually estimate which risks are most relevant by reviewing the exact intercostal level, chest and spinal anatomy, imaging findings, previous procedures, lung disease, anticoagulant treatment, other medical conditions, and the planned technique, although no complication can be predicted with complete certainty.
When should I contact a specialist about intercostal neuralgia?
You should contact a specialist if chest, rib, or upper abdominal pain persists for more than a few weeks, keeps recurring, follows shingles, remains unexplained after heart or organ tests, or does not respond to initial medication. Specialist review is also useful when the diagnosis is unclear, when pain may be thoracic radiculopathy or costochondritis, or when nerve blocks or procedures are being considered. The goal is not only to confirm the label “intercostal neuralgia,” but to identify the exact pain generator and maintaining factors. A doctor with strong knowledge of pain anatomy can decide which causes must be excluded and which treatment combination is most likely to work.
Can I get reimbursed by my health insurance for this consultation?
Reimbursement depends on your insurance plan and whether it includes out-of-network or international specialist consultation benefits. We do not bill insurance companies directly. After the consultation, we can provide a formal medical report and a detailed invoice containing the clinical information usually needed for reimbursement claims. Many patients use this documentation when submitting a claim to their insurer, but approval is not guaranteed and should be checked with the insurance provider in advance. The consultation is paid directly by the patient. The report may then serve as supporting documentation, especially when the consultation clarifies diagnosis, treatment failure, medication strategy, or the need for targeted procedures.
Additional Information About Intercostal Neuralgia
- WebMD — What to Know About Intercostal Neuralgia
- Healthline — Intercostal Neuralgia: Symptoms, Causes, Treatment
- Cleveland Clinic — Intercostal Nerve Block (Patient Guide)
- NHS (Hull University Hospitals) — Intercostal Nerve Block for Pain Relief
- Medical News Today — Intercostal Neuralgia: Overview for Patients
Find out generally about neuralgias on this page.