Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 10, 2026
Who this page is for
This page is for patients with trigeminal neuralgia or persistent facial pain that did not improve despite medications or previous treatments.
Some patients have typical trigeminal neuralgia with brief electric-shock attacks and pain-free intervals, while others have atypical or persistent facial pain with burning, aching, post-dental pain, viral nerve injury, peripheral nerve irritation, TMJ or muscle-related factors, or central sensitization. These situations require different treatment logic, so the first step is to determine which pain mechanism is actually active.
Pain usually persists because not all factors that irritate the trigeminal nerve have been identified — vascular compression is only one possibility. Through a detailed telehealth consultation, these contributors can be recognized, and most cases improve with a targeted combination of medications rather than a single drug. If a procedure or surgery has been recommended, an online second opinion helps confirm whether it is truly necessary and whether a less invasive option exists.
If you are unsure whether an online consultation can help after all previous tests and treatment, read why this consultation is different.
When patients usually seek a second opinion for trigeminal neuralgia
• Facial pain persists despite medications
• The diagnosis feels uncertain (TN vs atypical facial pain)
• Pain returns after temporary improvement
• You are considering procedures, injections, or surgery
If this reflects your situation, a focused telehealth review can clarify the pain generator, treatment options, and what is and is not indicated in your case:
Request Consultation
Trigeminal Neuralgia — Quick Summary (Read This First)
- Trigeminal neuralgia is a disorder of the trigeminal nerve that manifests as sudden, severe, electric-shock-like facial pain. The pain usually affects one side of the face and may appear in the jaw, teeth, cheek, around the eye, near the nose, or deep in the ear.
- Attacks are often triggered by very mild stimulation. Speaking, chewing, brushing teeth, shaving, touching the face, washing, or exposure to cold wind can provoke brief but intense pain attacks.
- The label “trigeminal neuralgia” does not always mean the same pain mechanism in every patient. Some patients have typical short electric attacks with pain-free intervals, while others have constant burning, aching, post-dental, post-traumatic, viral-related, MS-related, or treatment-resistant facial pain.
- The diagnosis of trigeminal neuralgia is primarily based on the clinical picture. MRI is used to look for associated conditions such as tumors, multiple sclerosis, or other secondary causes, and to assess whether a neurovascular contact (blood vessel compressing the nerve) is present and clinically relevant.
- MRI is important, but MRI findings must match the clinical picture. A visible blood vessel touching the trigeminal nerve does not automatically prove that it is the cause of pain, and a normal MRI does not exclude trigeminal nerve irritation elsewhere along its course.
- The most important first step in treatment is to identify the exact pain mechanism. Treatment depends on whether the pain is caused by vascular compression near the brainstem, irritation of trigeminal nerve branches in the face, dental or surgical injury, viral nerve damage, central sensitization, or overlapping contributing factors.
- Typical trigeminal neuralgia often responds well to carbamazepine or oxcarbazepine at first. If medication becomes less effective, causes side effects, or pain appears between attacks, this does not always mean that surgery is immediately required.
- Atypical or constant facial pain is harder to treat because the pain generator is often outside the classical vascular compression site. Pain may come from peripheral nerve irritation in the face, inflammation, scar tissue, post-dental injury, muscle or TMJ-related factors, herpes-related nerve injury, or sensitization of the pain system.
- Treatment failure often means that the true pain generator has not been fully identified. Standard therapy may reduce nerve excitability, but pain can persist if mechanical irritation, inflammation, local nerve injury, muscle spasm, metabolic factors, or central sensitization are not addressed together.
- Microvascular decompression surgery is most effective for classical trigeminal neuralgia with a matching vascular compression pattern. It is less predictable in continuous, burning, atypical facial pain or when MRI does not show clinically meaningful vascular compression.
- Different procedures are used for different situations in trigeminal neuralgia. Gamma Knife, percutaneous rhizotomy, nerve blocks, Botox, and neuromodulation are selected according to pain type. The choice depends on the type of pain, MRI findings, urgency of pain relief, age, medical risk, previous treatments, and whether the main goal is rapid pain control, lower numbness risk, diagnostic clarification, or long-term neuromodulation.
- Many persistent cases of trigeminal neuralgia can still improve without open surgery. When the exact irritation site and contributing factors are identified, optimized medication combinations, or sometimes targeted nerve blocks, Botox, or outpatient interventional procedures may provide meaningful pain control.
- The prognosis depends mainly on the type of trigeminal neuralgia and whether the true pain mechanism is identified. Typical trigeminal neuralgia with clinically relevant vascular compression often has a good chance of long-term relief with appropriate medication or microvascular decompression, while atypical, constant, post-dental, viral-related, or treatment-resistant facial pain usually requires a more individualized pain-control strategy.
- A second opinion is especially useful when medication no longer controls pain, when surgery, Gamma Knife, rhizotomy, or repeated dental procedures are being considered, or when the pain pattern is atypical. A structured review can clarify whether symptoms truly fit typical trigeminal neuralgia, whether MRI findings match the clinical picture, and which non-surgical or interventional options may still exist.
- Online consultation may still help when treatment has failed: read why this consultation is different.
Contents
- Typical trigeminal neuralgia
- Causes
- Who develops it
- Symptoms
- How it is diagnosed
- Treatment (medications & more)
- Surgical treatment — when and why
- Minimally invasive / non-invasive options
- Atypical trigeminal neuralgia (TN2)
- Treatment of Contributing Factors in Atypical Trigeminal Neuralgia
- Prognosis
- FAQ
- Related resources
Trigeminal neuralgia is characterized by sudden, severe, electric-shock–like facial pain that occurs when the trigeminal nerve becomes irritated or compressed. The trigeminal nerve supplies sensation to the face, oral cavity, and part of the ear.
In the early phase, the main mechanism is mechanical irritation or compression of the nerve (for example, by a blood vessel). Pain is usually triggered by light touch, speaking, chewing, or brushing teeth. Over time, repeated irritation can damage the nerve fibers and lead to neuropathic pain. The nerve becomes hypersensitive, and pain may start to appear even with minimal triggers — or without any trigger at all.
Trigeminal neuralgia can appear in several forms — typical, atypical, pre-neuralgia, post-traumatic, secondary (including MS-related), and treatment-resistant cases.
The most important first step is to determine which type is present, because treatment differs significantly between typical, atypical, and secondary trigeminal neuralgia, and each requires a different therapeutic approach.
Many patients are diagnosed simply with “trigeminal neuralgia” and are treated according to the standard protocol for typical TN, even though their pain pattern is not truly typical. If pain becomes constant, burning, post-dental, viral-related, treatment-resistant, or does not match meaningful vascular compression on MRI, the problem may not be classical trigeminal neuralgia alone. In such cases, continuing the same protocol may fail because the active pain generator has not been correctly identified.
Listen to the YouTube audio explanation on the diagnosis and treatment of refractory trigeminal neuralgia explained by the author.
Typical vs Atypical Trigeminal Neuralgia: Why the Treatment Path Differs
Trigeminal neuralgia is not one single pain mechanism. Some patients have typical trigeminal neuralgia with brief electric-shock attacks, clear trigger zones, and pain-free intervals. Others have atypical or persistent facial pain with burning, aching, post-dental pain, viral nerve injury, peripheral nerve irritation, TMJ or muscle-related factors, or central sensitization.
This distinction is important because treatments that work well for classical trigeminal neuralgia are less predictable in constant or atypical facial pain. Carbamazepine, microvascular decompression, Gamma Knife, or rhizotomy may be very effective when the pain pattern and MRI findings match classical trigeminal neuralgia. However, when pain is continuous, burning, post-traumatic, post-dental, or not supported by meaningful vascular compression on MRI, the first step is not simply choosing another procedure. The first step is identifying which trigeminal pain mechanism is actually active.
In practice, treatment decisions usually depend on four questions:
- Does the pain pattern fit typical electric-shock trigeminal neuralgia or atypical persistent facial pain?
- Does MRI show vascular compression that truly matches the clinical symptoms?
- Is the pain coming from the trigeminal nerve root, a peripheral facial branch, viral nerve injury, dental trauma, TMJ or muscle-related irritation, or central sensitization?
- Is the next step medication optimization, nerve block, Botox, Gamma Knife, rhizotomy, MVD surgery, or structured observation?
Typical trigeminal neuralgia

Image: trigeminal nerve with its three main branches across the face
Typical trigeminal neuralgia is characterized by sudden, brief, electric-shock–like attacks of severe facial pain. Each attack lasts from a few seconds up to one minute and can occur dozens or even hundreds of times per day. Between attacks, there is no pain, and the neurological examination is normal — this is one of the key diagnostic features of typical trigeminal neuralgia.
Causes of Typical Trigeminal Neuralgia (Etiology)
The most common cause of typical trigeminal neuralgia is mechanical compression of the trigeminal nerve root by a nearby artery as it exits the brainstem.
In the early stage, pain is triggered only when the nerve is stimulated — for example when speaking, chewing, brushing teeth, shaving, or touching the face.
With time, repeated compression damages the nerve fibers, making the nerve hypersensitive. A neuropathic pain component then develops, and pain may start to appear spontaneously — even without a trigger.
Who develops Typical Trigeminal Neuralgia
Typical trigeminal neuralgia most often begins after the age of 50 and is more frequent in women, and is rare in individuals under 40. The condition often has cycles: episodes of frequent attacks followed by remission lasting weeks, months, or even years.
Symptoms of Typical Trigeminal Neuralgia (Clinical Presentation)
Pain is sudden, stabbing, or electric-shock–like, usually affecting one side of the face. It may appear in the jaw, teeth, cheek, near the nose, around the eye, or deep inside the ear.
Even light stimulation — such as chewing, talking, brushing teeth, or exposure to cold wind — can trigger the attack. These highly sensitive areas on the face or in the mouth are called trigger zones.
Many patients initially assume the pain is dental in origin. They undergo fillings, root canals, or even tooth extractions — without relief, because the tooth is not the source of the pain.
Even when pain appears in different facial regions (jaw, cheek, around the eye, or in the ear), the source is the same — irritation or compression of the trigeminal nerve at the root entry zone, before it divides into individual branches.
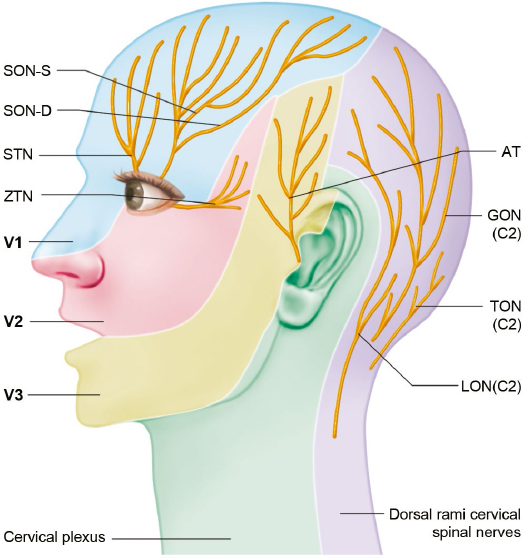
Image: Nerves that innervate skin of the head and face Read more about the anatomy of the cranial nerves here
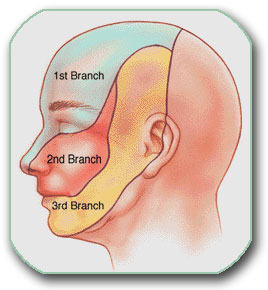
Image: Three facial regions where pain can occur, either separately or in combination
🎯 How We Diagnose Facial Pain When Others Miss the Real Cause
Most medical articles for patients focus primarily on the classical form of trigeminal neuralgia — pain caused by a blood vessel compressing the nerve inside the skull. However, many patients actually suffer from other types of facial pain — so-called atypical trigeminal neuralgia — where the irritation occurs along the course of the nerve in the face and often does not respond to standard treatments.
These irritations (for example: inflammation, muscle spasm, or scar tissue) are frequently not visible on imaging, but they can be detected through a focused conversation and functional testing during a video consultation. Before the call, the doctor reviews your medical records.
During the video consultation:
- The doctor asks targeted questions about the quality of pain and specific triggers.
- You are guided to press precise points on the face or perform small movements.
- Based on whether pain increases or decreases, the doctor locates the exact site of nerve irritation.
This approach allows an accurate diagnosis even when MRI is normal and previous treatments have failed. A focused video consultation with a specialist who understands the anatomy of pain is often more accurate than a brief in-clinic visit with a doctor who is not familiar with facial pain mechanisms.
How Typical Trigeminal Nerve Pain Is Diagnosed
In addition to examining the patient, an MRI of the brain is required to determine whether there is a pathological process causing the neuralgia. In such cases, it is referred to as secondary trigeminal neuralgia. Possible causes include tumors, multiple sclerosis, aneurysms, dental diseases, etc.
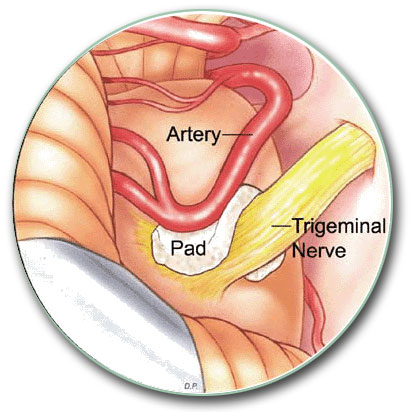
The typical cause of trigeminal neuralgia is pressure from a blood vessel on the nerve, as shown in the image. In most cases, this can be diagnosed with a brain MRI. However, the finding of vascular contact must match the clinical picture and the response to therapy to confirm that this is truly the cause and to justify surgical treatment.

Image: Arrow shows where the artery presses on the trigeminal nerve, causing pain. The nerve arises from the brainstem and ends in the Gasserian ganglion.
How Typical Trigeminal Neuralgia Is Treated – Medications and More
Treatment always begins with medication. The first-line drug is carbamazepine (Tegretol), and most patients respond well in the early phase. If carbamazepine is not effective or causes side effects, oxcarbazepine or a combination therapy with gabapentin/pregabalin or baclofen can be introduced to improve pain control with fewer adverse effects. If pain becomes more persistent or shows a neuropathic component, tricyclic antidepressants (such as amitriptyline or nortriptyline) or SNRIs (duloxetine, venlafaxine) may be added to stabilize nerve sensitivity and enhance long-term pain control. Medication initiation, monitoring of side effects, and dose titration can be performed through an online video consultation, which is especially important during the first weeks while the effective therapeutic dose is being reached.
Not all patients react the same way to medication. In the first 1–2 weeks, dosage adjustments are often required to maintain the effect. Over time, medications may become less effective, the attacks may last longer, or pain may begin to appear between attacks. Many people interpret this as “the medication has stopped working and the next step is surgery,” but this is often not true.
For patients who want to avoid surgery, or where surgery carries a higher risk due to age or comorbidities, pain can often be successfully controlled with an optimized combination of medications and outpatient interventional procedures (targeted nerve blocks, minimally invasive treatments that reduce nerve irritation). In many cases, this approach allows surgery to be avoided entirely.
Supportive therapy using appropriately selected vitamins, minerals, and supplements may help nerve recovery. The selection is not universal; it is tailored to the type of nerve irritation and laboratory findings.

Image: Interventional pain procedure used in trigeminal neuralgia treatment
Surgical treatment of typical trigeminal neuralgia: When and Why It’s Needed
This procedure involves a small opening in the skull behind the ear (craniotomy) and gently separating the blood vessel from the trigeminal nerve. A small Teflon pad is then placed between them to prevent further pulsatile compression.. It has excellent long-term results: more than 75–90% of patients achieve immediate pain relief, and about 70–80% maintain significant improvement in the long term.
MVD is the most effective treatment for classical / Type 1 trigeminal neuralgia (paroxysmal, shock-like pain).
This does not apply to more atypical trigeminal neuralgia (when the pain is continuous and characterized by burning/aching, the patient is younger than 60, and no vascular compression is seen), where surgical success rates are significantly lower.
The procedure lasts about 2 hours and is generally well tolerated, even in patients older than 70 who are in good overall condition.
Minimally invasive and non-invasive options for trigeminal neuralgia when open surgery isn’t ideal
For patients who are not candidates for open surgery or general anesthesia, a percutaneous trigeminal rhizotomy may be used—a needle procedure through the cheek to the Gasserian ganglion (the nerve cluster where trigeminal branches converge at the skull base). The main techniques are radiofrequency rhizotomy (creating a brief heat lesion), balloon compression, and, less commonly today, glycerol rhizolysis. These procedures are performed under short sedation, usually provide rapid pain relief in typical trigeminal neuralgia, and can be repeated if pain recurs. The trade-off is a higher likelihood of facial numbness; when V1 (the eye branch) is involved, the corneal (blink) reflex is carefully protected. The aim is to preferentially interrupt pain-carrying fibers while preserving normal facial sensation and motor function, but selectivity is imperfect, so some numbness or dysesthesia can still occur.
Gamma Knife radiosurgery is a non-invasive treatment option. Focused radiation is directed at the trigeminal nerve where it enters the brainstem (root entry zone), and in some centers slightly farther along the nerve (retrogasserian/cisternal segment). The goal is to reduce pain signal transmission while preserving normal facial sensation and muscle function. Despite precise targeting, some patients may still experience facial numbness.
Pain relief develops gradually — over several weeks to a few months.
Compared with percutaneous rhizotomy (balloon compression, glycerol, or radiofrequency), sensory side effects are less frequent after Gamma Knife (approximately 10–30% vs. 40–80%, depending on the technique and series). Long-term pain-free rates at around 5 years generally range from 40–60%.
Gamma Knife can be repeated if pain returns, but usually no more than 1–2 times in a lifetime due to cumulative radiation exposure. Percutaneous rhizotomy procedures can be repeated multiple times if necessary.
When choosing between Gamma Knife and percutaneous rhizotomy, a common approach is to start with Gamma Knife when a gradual onset of relief over 2–6 months is acceptable and a lower risk of permanent facial numbness is a priority. If pain is severe and uncontrolled despite medications—or if Gamma Knife does not provide adequate relief after an appropriate waiting period—percutaneous rhizotomy offers fast control (often within 24–48 hours) with a higher likelihood of numbness. The choice ultimately depends on the urgency of pain relief, comorbidities, imaging, and patient priorities regarding the risk–benefit balance of each method.
Peripheral nerve blocks are a minimally invasive option used when medications are not sufficient or when diagnostic clarification is needed. A small amount of anesthetic, sometimes combined with an anti-inflammatory medication, is injected around the trigeminal nerve branch or trigger zone to interrupt the pain cycle and confirm the source of pain. Depending on the clinical scenario, the block may target a superficial cutaneous branch (supraorbital, infraorbital, mental nerve) or a deeper segment of the trigeminal nerve (V2/V3). Deep, complex blocks include the maxillary nerve block (V2) in the pterygopalatine fossa, mandibular nerve block (V3) near the foramen ovale, or pterygopalatine ganglion block when pain radiates behind the eye or into the palate. These deeper procedures are performed under ultrasound or fluoroscopic guidance to safely navigate structures that are only millimeters wide and surrounded by major vessels and nerves. Relief is often immediate and may last from several days to several months; in many patients, one to three sessions combined with optimized medication are enough for long-term pain control.
Botulinum toxin (Botox) injections can be used as an adjunct therapy in patients who do not tolerate medications well or whose pain persists despite drug treatment. Botox is injected subcutaneously or intradermally along the painful dermatome, directly over the sensitive trigger zones or along the course of the affected trigeminal branch (most often V1, V2, or V3). By acting on the peripheral endings of sensory nerve fibers, Botox reduces the release of pain-transmitting neuropeptides, lowers nerve hypersensitivity, and decreases the frequency and intensity of pain attacks. Clinical studies and experience show that some patients feel significant improvement within 7–14 days after injection, particularly those with constant burning or aching facial pain. Botox does not damage the nerve and does not interfere with future surgical or interventional options. It can be repeated every 3–6 months if needed, and it is particularly useful in atypical trigeminal neuralgia and post-herpetic trigeminal pain.
Neuromodulation (nerve stimulation) is reserved for rare, treatment-resistant cases where medications, blocks, and standard procedures have not provided adequate relief. A small stimulator (similar to a pacemaker) is implanted to deliver electrical impulses to the trigeminal nerve (Gasserian ganglion) or its branches. These impulses modify how the nerve transmits pain signals to the brain. Although neuromodulation is not a first-line treatment, it can be highly effective in carefully selected patients. In some centers, temporary external stimulation is performed first to evaluate response before permanent implantation is considered. In very select, treatment-resistant cases, deep brain stimulation (targeting specific regions of the thalamus) or motor cortex stimulation (placing electrodes on the surface of the brain over the motor cortex) has been investigated as a neuromodulation option. These approaches are rarely performed and remain experimental.
Peripheral neurectomy (“nerve pulling”) / thermal or chemical neurolysis of terminal trigeminal branches has a very limited role today. It may deliver short-term relief in highly selected cases (e.g., very elderly or those with major comorbidity, or a rare, well-localized peripheral trigger), but recurrence is common and there is a meaningful risk of anesthesia dolorosa (painful numbness). For these reasons it is generally avoided when other effective options (optimized medication, percutaneous rhizotomy, or Gamma Knife) are available.
These methods work best for typical (paroxysmal) TN. In patients with continuous/atypical facial pain, results are less predictable, so therapy is individualized and often begins with an optimized medication plan (dosing, combinations, sequencing). The key is to identify the exact pain generator—for example a peripheral trigger point, scar, focal nerve entrapment or a neurovascular contact—and, when appropriate, perform targeted interventions directly at that site (e.g., selective nerve blocks, trigger-point injections or very small, focused ablations).
Surgery was recommended? Request an online second opinion on MVD, radiosurgery (Gamma Knife), rhizotomy, and an optimized medication plan (dosing, combinations, sequencing) — with clear benefits, risks, and durability.
Atypical Trigeminal Neuralgia: Difference Between Typical and Atypical Trigeminal Neuralgia
Atypical trigeminal neuralgia represents a different clinical group, as the standard treatment protocol used for classical TN often fails. Consequently, these patients respond poorly to microvascular decompression (MVD) and achieve significantly lower success rates than typical TN from radiation procedures such as Gamma Knife.
In addition to the sudden, sharp paroxysmal attacks, patients often experience a persistent background pain between episodes, which is typically described as a continuous burning, aching, or throbbing sensation.
Clinical clues suggesting atypical TN include: weak or short-lived response to carbamazepine (Tegretol), younger age of onset, gradual onset instead of sudden attacks, persistent pain without pain-free intervals, pain beginning after dental procedures, pain provoked by chewing or talking, and absence of vascular compression on MRI.
In these patients, the cause is usually not a blood vessel compressing the trigeminal nerve at the brainstem, but irritation of the nerve somewhere along its course in the face. Irritants can have different locations and different types. These types include: inflammation of nearby tissues, spasms, vascular compression by facial arteries, scarring, infection, etc. The key is to locate the exact point of irritation through a detailed conversation and functional pain testing during a video consultation. Without identifying the source of irritation, treatment becomes guesswork and often fails.
Some authors use the terms trigeminal neuralgia type 1 (TN1), which mostly describes the typical paroxysmal form, and type 2 (TN2) to describe the constant pain form. The problem with this terminology is that TN2 simply groups together all cases that are not TN1, even though these patients may have completely different causes of nerve irritation. In other words, TN2 describes how the pain feels, but not why it exists. On this page, we use a more practical classification based on the actual cause of nerve irritation, because treatment depends on the mechanism, not on the label.
Viral Injury of the Trigeminal Nerve
In some patients, trigeminal pain does not come from vascular compression at the nerve root or from local irritations in the face, but from viral injury of the nerve itself. This most commonly occurs after a shingles infection affecting the trigeminal nerve (postherpetic neuralgia), or after recurrent oral herpes caused by herpes simplex virus (HSV-1). Both viruses can remain dormant in the trigeminal ganglion and, when reactivated, sensitize or inflame a single branch of the nerve—causing burning, hypersensitivity, or electric pain along a specific area of the face. In these cases, the problem is not a blood vessel pressing on the nerve but damage or inflammation of the nerve fibers, and treatment follows the principles of neuropathic pain management. During the infection, local irritative sources in the face (spasm, inflammation of local tissue) also appear. When symptoms clearly follow herpes outbreaks, antiviral suppression may also be considered.
How Atypical Trigeminal Neuralgia Is Treated When Standard Therapies Fail
When the specific process and location causing irritation of the trigeminal nerve are accurately identified, targeted treatment can be implemented. In everyday practice, however, this is often not determined precisely enough, and treatment fails as a result. In such cases, the failure is frequently blamed on the patient’s age, psychological factors, or other chronic illnesses. While these factors may contribute to the overall condition, they are not an excuse for not achieving successful treatment.
Once the type and exact location of nerve irritation are identified, an appropriate combination of medications is prescribed. The goal is to significantly reduce the pain within 10 days, even if the pain has been present for a long time. If a pain-free state can be maintained for 6 to 8 weeks, the therapeutic effect is usually long-lasting. When all contributing sources of irritation are recognized, most cases improve with a targeted combination of medications addressing every underlying mechanism, supported by vitamin and supplement therapy. These medications must be adjusted in type and dosage over a period of 6–8 weeks. Previous medication failure does not always mean that medication cannot help. In many persistent cases, the problem is that the right combination of mechanisms was not treated together—but it should be. In most cases, a special intervention is not needed to reduce pain.
This outcome can also be achieved through online consultations via messages and video calls. It is particularly important that the doctor is available during the first ten days of treatment so that medication type or dosage can be adjusted quickly if needed. Thanks to telehealth, top specialists are accessible even when the patient is not in the same city.
A physical examination is not necessary; what matters is that a specialist who understands pain anatomy conducts the consultation and asks the right questions (either in person or via video call). During the consultation, the doctor instructs the patient to perform specific jaw and neck movements or apply pressure to certain areas to provoke or relieve the pain. This has the same diagnostic value as an in-person examination. Most patients have never had such testing performed. Usually, one to three video consultations are enough to achieve long-term pain relief.
In some cases, drug therapy alone is not sufficient to treat trigeminal neuralgia, and interventional methods are required. These methods include precise injection of medication directly into the process causing nerve irritation and pain, or the use of other interventional techniques such as stimulation, heating, lesioning, or decompression.
Because pain sources are usually very small — often less than 1 cm — and located deep within the tissue surrounded by important structures, the procedure must be performed under imaging guidance. The insertion of the needle is guided by ultrasound or fluoroscopy to ensure accurate delivery of the medication.
If an interventional procedure is being considered, medication preparation is required beforehand, which can be prescribed after an in-person or online video consultation. Very often, once medication preparation begins, the need for a procedure disappears — meaning that properly selected medication therapy alone can resolve the pain.
These procedures are performed on an outpatient basis (sometimes even at home), are not painful, and pain relief is immediate. The entire process, including the examination, typically takes 1 to 1.5 hours, after which the patient can return home. For long-term effect, 1 to 3 interventional procedures are usually required, spaced a few weeks apart.
If these procedures do not achieve sufficient relief, additional methods such as Gasserian ganglion lesioning or Gamma Knife radiosurgery can be performed.
Summary: In the vast majority of patients with persistent and intense facial pain, the pain can be stopped and controlled with modern medication therapy, or — in more severe cases — with special outpatient or in-home interventional procedures. Because of their high success rate, this treatment should always be attempted before surgical procedures or stereotactic radiation (Gamma Knife).
Why Trigeminal Neuralgia Pain Persists Despite Treatment
In many patients, trigeminal neuralgia persists despite medication or procedures not because the condition is untreatable, but because the exact mechanism and location of nerve irritation have not been precisely identified. Standard therapies are often applied based on the general diagnosis, without clearly determining which anatomical structure is responsible for the pain, what pathological process is occurring within that structure, and which contributing factors are maintaining the pain — and it is precisely this failure to identify all three that leads to persistent pain despite treatment.
In many patients, pain persists even when medications such as carbamazepine or other standard therapies initially provide relief, or stop working over time.
Another common reason is that treatment addresses only one aspect of the problem. For example, medication may reduce nerve excitability, but ongoing mechanical or vascular irritation continues to trigger pain. In other cases, procedures are performed without fully understanding all contributing factors, leading to only temporary or incomplete relief.
In long-standing cases, the nervous system itself can become sensitized, meaning that even minor stimuli can provoke severe pain. This does not mean that the condition is psychological, but rather that multiple mechanisms are interacting and maintaining the pain.
For this reason, when trigeminal neuralgia does not improve, the key step is not simply repeating the same treatments, but performing a structured reassessment to identify all active pain mechanisms. Only after this analysis can treatment be adjusted in a targeted and effective way.
Treatment of Contributing Factors in Atypical Trigeminal Neuralgia
Effective treatment of atypical trigeminal neuralgia always begins with identifying the primary pain generator — whether the dominant source of symptoms is trigeminal nerve dysfunction,local irritation, post-traumatic or post-dental nerve injury, central pain processing changes, or a combination of these mechanisms.
However, in many patients, pain persists not only because of the primary cause, but because additional contributing factors are not recognized or adequately addressed. These factors rarely act as the sole cause of pain, but they can maintain nerve irritation, increase pain sensitivity, delay recovery, and reduce the effectiveness of otherwise appropriate treatment.
For that reason, successful management requires not only identifying the dominant neurological irritation but also understanding the broader mechanical, neurological, and systemic context in which the pain persists.
What contributing factors may play a role in atypical trigeminal neuralgia?
• Previous dental or surgical procedures — Tooth extractions, root canal treatments, implants, or facial surgeries may lead to nerve irritation or altered signaling, even when the procedure was technically correct.
• Chronic peripheral nerve irritation — Persistent irritation of trigeminal branches (infraorbital, mental, alveolar nerves) can maintain ongoing pain even without clear structural compression.
• Central sensitization — The nervous system becomes more sensitive over time, amplifying signals and leading to constant, burning, or diffuse pain typical for atypical trigeminal neuralgia.
• Muscle tension and myofascial factors — Increased tension in masseter, temporalis, and cervical muscles may contribute to altered pain perception and overlapping pain patterns.
• Temporomandibular joint (TMJ) dysfunction — Abnormal jaw mechanics, bruxism, or joint irritation can maintain persistent facial pain.
• Repetitive microtrauma and parafunctional habits — Teeth clenching, grinding, or repetitive jaw activity can maintain trigeminal irritation.
• Metabolic factors, pro-inflammatory diet and low-grade inflammation — Obesity, insulin resistance, chronic inflammation, and processed/high-sugar diet increase pain sensitivity and slow recovery.
• Nutritional deficiencies — Low levels of vitamin D, vitamin B12, magnesium, or iron may contribute to nerve dysfunction and impaired healing.
• Vitamin-related factors — Both deficiency and excess of vitamin B6 may contribute to burning pain, tingling, or hypersensitivity.
• Sleep disturbances and autonomic dysregulation — Poor sleep increases pain sensitivity and reduces pain tolerance.
• Stress and persistent pain-related vigilance — Stress increases central nervous system reactivity and amplifies pain perception.
• Medications and previous treatments — Long-term use of pain medications, repeated ineffective treatments, or certain drugs (such as statins in some patients, which may be associated with muscle-related symptoms) may alter pain perception or contribute to persistent symptoms without resolving the underlying mechanism.
• Other medical conditions and comorbidities — Autoimmune diseases, diabetes, thyroid disorders, and chronic inflammatory states increase nerve sensitivity and reduce treatment response.
• Psychophysical interaction (not psychological cause) — Chronic pain changes central processing of pain signals; this does not mean the pain is psychological, but that the system has become more reactive.
Why this matters in practice
In many cases, treatment fails because the primary pain generator is not correctly identified, and therapy is directed only at one part of the problem — most often a single medication alone or repeated dental procedures.
Conversely, even when the main neurological cause is recognized, failure to address contributing factors often leads to only partial or temporary improvement.
The most effective approach is a carefully selected combination of treatment that addresses both the dominant pain mechanism and all relevant contributing factors. An incomplete approach — even when it includes individually effective methods — is one of the most common reasons why atypical trigeminal neuralgia becomes persistent.
In practice, many patients try to address parts of this problem on their own — through diet changes, supplements (vitamin D, magnesium), physiotherapy, or different medications. While these approaches can be helpful, they rarely lead to lasting improvement if the primary pain mechanism is not clearly identified and treated. On the other hand, even well-targeted medical treatment may fail if all contributing factors are not recognized and corrected.
Many patients reading this recognize that they have already tried one part of this approach — but not the complete strategy. This is one of the most common reasons why atypical trigeminal neuralgia becomes chronic.
Prognosis of Trigeminal Neuralgia
Typical (Classical) Trigeminal Neuralgia
In typical TN, especially when MRI confirms vascular compression at the root entry zone of the trigeminal nerve, the prognosis is generally favorable. About 70–80% of patients experience significant pain reduction with first-line medications (carbamazepine or oxcarbazepine). However, because of side effects or decreased effectiveness over time, only about 30–40% remain well-controlled by medications alone in the long term. When pain persists or medications are poorly tolerated, interventional or surgical treatments are considered. Microvascular decompression (MVD) offers the highest long-term success rate, with approximately 70–85% of patients remaining pain-free for years. Gamma Knife radiosurgery and percutaneous rhizotomy also provide excellent short-term relief (70–90%), although durability is generally lower than with MVD. Overall, in typical TN, around one-third of patients achieve sustained relief with medications alone, while two-thirds will eventually require a procedure such as MVD, radiosurgery, or a minimally invasive percutaneous technique.
Atypical (Constant Pain / Non-Classical) Trigeminal Neuralgia
The prognosis for atypical TN is different because the pain mechanism is not caused by classical vascular compression. Triggers may include peripheral irritation in the face, scarring, inflammation, infection (post-herpetic or HSV-related), or irritation of smaller nerve branches. Medication success is lower than in typical TN — only about 30–50% of patients achieve meaningful improvement with medications alone, and sustained long-term control with drugs only is achieved in roughly 20–30%. These patients usually require a targeted combination of medications and, when needed, interventional procedures that focus on the exact site of irritation (ultrasound-guided blocks, radiofrequency of peripheral branches, or botulinum therapy). Gamma Knife and Gasserian ganglion lesion are also indicated when medications and targeted nerve blocks are not successful, but long-term success rates are lower when there is no vascular compression and the pain is continuous (atypical form).
Prognosis and Long-Term Outcomes
| Trigeminal neuralgia type | Initial response to treatment | Long-term outcomes (3–10 years) | Goal of treatment |
|---|---|---|---|
| Typical TN classic electric shock attacks |
Medications: 70–80% initial response Interventions (MVD / Rhizotomy): 85–95% immediate relief Gamma Knife: 70–90% (delayed relief) |
MVD: 70–80% pain-free long-term (10 yr) Gamma Knife / Rhizotomy: 40–60% pain-free (3–5 yr) |
Complete remission |
| Atypical TN (constant pain form) burning / aching / continuous |
Medications: 30–50% response **Interventional blocks successful if the source of irritation is identified** Gamma Knife or Rhizotomy:lower initial relief (≈40–60%) |
Gamma Knife / Rhizotomy: 20–30% durable benefit MVD only if vascular compression proven |
Significant pain reduction / control |
*Typical TN aims for remission. Atypical TN aims for control. Success depends on identifying the exact source of irritation.*
Online pain consultation for trigeminal neuralgia in detail
Schematic explanation of the video consultation for trigeminal neuralgia
Answers to questions about the process and success of video consultations for trigeminal neuralgia
See the page “Possible Reasons for Poor Pain Treatment Effectiveness of Trigeminal Neuralgia” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
Treatment of complex cases of trigeminal neuralgia can be analysed by artificial intelligence (AI)
Video consultation is also known as a virtual visit, video visit, online consultation, remote consultation or telehealth appointment.
Why an Online Consultation Can Help When Trigeminal Neuralgia Pain Persists
A video consultation for trigeminal neuralgia can help identify the exact source of your facial pain — one or more pain generators — as well as the factors that trigger and maintain it. This is achieved through a detailed conversation and review of your MRI scans and medical records. During the session, you are instructed to perform specific jaw, facial, or neck movements and finger-pressure tests to see what increases, reduces, or changes your pain. This helps identify which pain source is active. Many of these pain generators and sustaining factors cannot be seen on MRI.
This may sound like examinations you have already had. It is not — because what matters most is not the test itself, but who interprets it. Only a specialist with deep knowledge of pain anatomy in this region knows which questions to ask, where to instruct you to press, which movements to test, and how to confirm which pain source is active. This is not just another opinion.
You will also receive advice on which contributing factors that trigger and sustain pain should be investigated — such as hormonal factors, vitamin deficiencies, side effects of other medications, inadequate diet, metabolic disorders, physical strain during daily activities or work, and other overlooked contributors. In many patients who have already visited several specialists, these factors have still not been fully investigated.
Once the main pain mechanism behind trigeminal neuralgia symptoms is identified, treatment follows: a targeted combination of medications covering all identified mechanisms, carefully introduced and adjusted over 6–8 weeks, with regular communication during the treatment period, especially when you need it. The aim is to achieve early pain reduction during the first 10 days, then stabilize the result over the following weeks for a longer-lasting effect. When selecting medications, we take into account whether patients are older or have other health conditions, and we prescribe them in a safe combination for the shortest possible duration to avoid medication overload. All recommendations are explained during the conversation and are also given in a written medical report.
Many patients assume that because medications have already failed, a specific procedure is now needed. In most cases, this is not true — previous medications often did not cover the right combination of mechanisms, were not individualized, or were not adjusted over a sufficient period of time. In the minority of patients where medication alone is not sufficient, we recommend the exact intervention or procedure — chosen based on the confirmed pain generator, not assumptions.
Based on our written medical report, reimbursement may often be possible if your insurance plan allows it.
Start Your Telehealth Consultation with a Pain Specialist
If your pain treatment has failed or you’re unsure what to do next — don’t wait. A detailed telehealth consultation can help identify the exact cause of your pain, even if previous therapies didn’t work.
- ✔ First, send a short message describing your problem
- ✔ You’ll receive a reply within 24 hours if and how we can help — including the consultation cost and a suggested time
- ✔ Only then, you can send your medical documentation
- ✔ The video consultation is followed by a written report and follow-up questions (up to 10 days)
Consultation fees typically range from $180–250, depending on the complexity of your case.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Based on our medical report, reimbursement can often be obtained (if your insurance plan allows it).
This is within the usual range for specialist telehealth consultations worldwide. Thousands of patients worldwide already use telehealth consultations for second opinions — it’s safe, accepted, and effective.
Before contacting us, please read our Privacy Policy and Terms of Use.
Frequently Asked Questions About Trigeminal Neuralgia
Can trigeminal neuralgia treatment fail because the pain is not typical TN?
Yes. Some patients are diagnosed with trigeminal neuralgia and treated according to the standard protocol for typical TN, even though their pain pattern is not truly typical. Classical trigeminal neuralgia usually causes brief electric-shock attacks with pain-free intervals and often responds to carbamazepine, oxcarbazepine, or carefully selected procedures when MRI and symptoms match. If pain is constant, burning, post-dental, viral-related, treatment-resistant, or not supported by meaningful vascular compression on MRI, the active mechanism may be different. In that situation, repeating the same treatment protocol may fail because peripheral nerve irritation, scar tissue, TMJ or muscle-related triggers, central sensitization, or another pain generator has not been identified. Treatment then needs a mechanism-based plan, not only a standard TN label.
Do MRI or CT scans always reveal the cause of trigeminal neuralgia?
Not always. In classical trigeminal neuralgia, MRI may show a blood vessel pressing on the trigeminal nerve near the brainstem. However, many patients with trigeminal neuralgia or persistent facial pain have normal MRI or CT scans. Imaging may not show small areas of nerve irritation in the face, inflammation, muscle spasm, scar tissue, dental-related nerve trauma, postherpetic nerve injury, or peripheral branch irritation. A normal scan does not mean the pain is not real. It means that the cause must also be searched for through symptoms, triggers, pain distribution, medication response, and functional testing.
How can the true cause of trigeminal neuralgia pain be identified if MRI is normal?
When MRI does not clearly show the cause of trigeminal neuralgia, the most important step is to analyze how the pain behaves. The doctor must determine where the pain starts, where it spreads, what triggers it, whether it feels like electric shocks or burning pain, and how it responded to previous medication. Guided pressure over specific facial points, jaw movement, chewing muscles, trigger zones, and sensory testing can help identify which trigeminal branch or local pain generator is involved. In many difficult cases, treatment fails because the exact structure irritating the trigeminal nerve has not been found.
Why does trigeminal neuralgia pain persist despite treatment?
Trigeminal neuralgia pain often persists because treatment is aimed at the name of the diagnosis rather than the exact cause that continues to irritate the trigeminal nerve. Medication may reduce nerve excitability, but pain can continue if there is ongoing vascular compression, peripheral branch irritation, dental-related nerve trauma, postherpetic nerve injury, muscle spasm, scar tissue, local inflammation, or central sensitization. In other patients, the pain pattern changes over time and the original plan is no longer sufficient. Persistent pain does not automatically mean that surgery is needed. It means that the pain generator must be identified more precisely.
Why does medication stop working in trigeminal neuralgia?
Medication may stop working in trigeminal neuralgia when the nerve irritation becomes stronger, when the pain changes from short attacks to more constant pain, or when the real pain generator was never fully identified. Carbamazepine or oxcarbazepine may work well at first, but later the dose may become insufficient or side effects may limit further increase. Sometimes the problem is not simple drug failure. The patient may also have peripheral trigeminal branch irritation, TMJ-related pain, post-dental nerve injury, postherpetic neuralgia, or a mixed neuropathic pain mechanism. The next step should be reassessment, not only dose escalation.
What is atypical trigeminal neuralgia and why is it harder to treat?
Atypical trigeminal neuralgia is harder to treat because it does not always look like the classic form of the disease. Instead of short electric-shock attacks with pain-free intervals, the pain may be constant, burning, aching, deep, tooth-like, or located around the jaw, cheek, eye, ear, or teeth. MRI may be normal, and standard trigeminal neuralgia medication may help only partially. In these cases, the pain may come from peripheral trigeminal branch irritation, previous dental work, shingles, scar tissue, muscle spasm, or central sensitization. Treatment must therefore be based on the real mechanism, not only on the diagnosis name.
What happens when trigeminal neuralgia becomes constant instead of electric shocks?
When trigeminal neuralgia becomes constant, burning, dull, or aching instead of short electric shocks, it may indicate atypical trigeminal neuralgia or a mixed pain mechanism. Classical trigeminal neuralgia usually causes brief attacks with pain-free intervals. Constant pain may suggest peripheral branch irritation, post-dental nerve injury, postherpetic neuralgia, central sensitization, or a chronic neuropathic component added to the original condition. This matters because treatments that work well for classical trigeminal neuralgia, especially microvascular decompression, may be less predictable when the pain is continuous and there is no clear vascular compression. Treatment must be individualized.
How do I know if facial pain is trigeminal neuralgia or a tooth or TMJ problem?
Tooth pain, TMJ pain, and trigeminal neuralgia can feel very similar. Dental pain is usually related to one tooth and worsens with biting, cold, heat, or dental pressure. TMJ pain often worsens with chewing, jaw opening, clenching, or pressure over the jaw joint and chewing muscles. Classical trigeminal neuralgia usually causes sudden electric-shock attacks triggered by light touch, brushing teeth, speaking, shaving, or cold wind. Atypical trigeminal neuralgia can be more confusing because it may feel like tooth, jaw, cheek, or ear pain. The distinction depends on pain pattern, trigger zones, dental findings, jaw mechanics, and response to nerve-directed treatment.
Can a dental procedure trigger trigeminal neuralgia or trigeminal nerve pain?
A dental procedure usually does not cause classical trigeminal neuralgia from vascular compression, but it can trigger or unmask trigeminal nerve pain. Pain may begin after tooth extraction, root canal treatment, implants, local infection, prolonged jaw opening, or trauma to a small nerve branch. This may produce post-traumatic trigeminal neuropathic pain or atypical trigeminal neuralgia-like symptoms. The patient may continue to feel tooth pain even after the tooth has been treated or removed. In such cases, repeated dental procedures may not help and can sometimes make the pain worse. The focus should shift to the involved trigeminal branch and nerve pain mechanism.
Can herpes or shingles cause trigeminal neuralgia-like pain?
Herpes viruses can cause trigeminal nerve pain, but this is usually a different mechanism from classical trigeminal neuralgia caused by vascular compression. Shingles affecting the trigeminal nerve can lead to postherpetic neuralgia, with burning, hypersensitivity, tingling, or electric pain in the forehead, eye region, cheek, or jaw. Herpes simplex virus may also irritate trigeminal pathways in selected patients, especially when symptoms follow recurrent oral or facial outbreaks. MRI may be normal because the problem is nerve injury or hypersensitivity rather than a visible mass. Treatment may include neuropathic pain medication, antiviral consideration in selected cases, and targeted pain procedures.
My MRI shows no vascular compression — what are the next steps in trigeminal neuralgia?
If MRI shows no vascular compression, trigeminal neuralgia is not automatically excluded. The next step is to decide whether the pain really fits classical trigeminal neuralgia or whether another mechanism is more likely. Possible causes include atypical trigeminal neuralgia, post-dental nerve injury, postherpetic neuralgia, TMJ-related irritation, peripheral nerve entrapment or irritation, muscle-related triggers, or central sensitization. When there is no clear neurovascular conflict, MVD surgery is usually less predictable. Treatment often focuses on medication optimization, guided pain mapping, nerve blocks, botulinum toxin, or targeted interventional procedures, depending on the pain pattern.
Can trigeminal neuralgia go away on its own?
Trigeminal neuralgia can sometimes enter spontaneous remission, meaning that attacks decrease or disappear for weeks, months, or even longer without a specific treatment change. However, this usually does not mean that the condition has been cured. In many patients, the pain returns because the underlying irritation of the trigeminal nerve is still present. Over time, attacks may become more frequent, last longer, respond less well to medication, or develop into a more constant burning or aching pain. For this reason, temporary improvement should not replace proper evaluation of the pain mechanism and the source of nerve irritation.
Can trigeminal neuralgia return after temporary relief?
Yes. Trigeminal neuralgia may return after temporary relief when the underlying irritation has not been fully controlled. Medication can calm the nerve for a time, but vascular compression, inflammation, dental-related nerve injury, scar tissue, muscle spasm, or viral nerve damage may continue to irritate it. Procedures may also give partial relief if they reduce pain transmission but do not address all active mechanisms. Over time, the nervous system may become more sensitive, so attacks become longer, more frequent, or are replaced by constant burning pain. When pain returns, the important question is not only which dose to increase, but why the pain came back.
Can trigeminal neuralgia be successfully treated after many years?
Yes. Trigeminal neuralgia can sometimes be improved even after many years, but treatment has to be more precise than simply repeating the same medication. Long-lasting pain often means that several mechanisms are active at the same time: nerve irritation, medication tolerance, peripheral branch hypersensitivity, previous dental or surgical trauma, viral nerve injury, muscle spasm, or central sensitization. If these mechanisms are not separated, treatment may give only temporary relief. A structured reassessment can show whether the next step should be medication adjustment, combination therapy, nerve blocks, interventional pain procedures, Gamma Knife, MVD surgery, or a non-surgical pain control strategy.
Do I really need surgery for trigeminal neuralgia?
Surgery is not automatically required for trigeminal neuralgia. Microvascular decompression is most appropriate when the pain is classical, shock-like, one-sided, triggered by light touch, responsive to carbamazepine or oxcarbazepine, and MRI shows vascular compression that matches the symptoms. If the pain is constant, burning, post-dental, postherpetic, bilateral, poorly responsive to medication, or not associated with clear compression, surgery may be less predictable. Many patients improve with medication optimization, combination therapy, nerve blocks, botulinum toxin, or other interventional procedures. Surgery becomes more reasonable when the mechanism is clear and non-surgical treatment is not enough.
When is MVD surgery the best treatment for trigeminal neuralgia?
Microvascular decompression, or MVD, is usually the best surgical treatment for classical trigeminal neuralgia when a blood vessel compresses the trigeminal nerve near the brainstem and the symptoms match that finding. The strongest candidates have short electric-shock attacks, clear trigger zones, pain-free intervals, one-sided pain, good early response to carbamazepine or oxcarbazepine, and MRI evidence of neurovascular conflict. MVD aims to separate the vessel from the nerve while preserving normal facial sensation. It is less predictable when pain is constant, burning, atypical, post-dental, postherpetic, or when MRI does not show relevant compression. A second opinion is useful before surgery when the mechanism is uncertain.
When does Gamma Knife work poorly in trigeminal neuralgia?
Gamma Knife tends to work less well when trigeminal neuralgia is atypical, constant, burning, poorly localized, post-dental, postherpetic, or not caused by a clear nerve-root mechanism. It is usually more effective for classical shock-like trigeminal neuralgia than for continuous facial pain. Pain relief after Gamma Knife is delayed and may take weeks or months, so it may not be ideal when rapid control is needed. Recurrence can occur, and repeat treatment is limited by radiation exposure and the risk of facial numbness. Gamma Knife can be useful in selected patients, but it should not be chosen only because medication has failed.
Can trigeminal neuralgia be controlled without surgery?
Yes. Many patients with trigeminal neuralgia can be controlled without surgery, especially when the treatment plan is based on the exact pain mechanism. Classical trigeminal neuralgia may respond to carbamazepine, oxcarbazepine, or carefully selected medication combinations. Atypical, post-dental, postherpetic, or peripheral trigeminal pain may require a different strategy, including neuropathic pain medication, baclofen, antidepressant-type pain modulators, botulinum toxin, nerve blocks, trigger-point treatment, or image-guided procedures. The key is not simply taking stronger medication, but identifying whether the pain comes from root compression, peripheral branch irritation, viral injury, central sensitization, or a mixed mechanism.
When do interventional procedures help in trigeminal neuralgia?
Interventional procedures can help trigeminal neuralgia when medication is not enough, when the diagnosis needs confirmation, or when a peripheral trigeminal branch appears to be the main pain generator. Superficial blocks may target the supraorbital, infraorbital, or mental nerve. Deeper procedures may involve the maxillary nerve, mandibular nerve, pterygopalatine ganglion, or Gasserian ganglion region. These procedures can reduce pain, confirm the involved branch, and sometimes break the pain cycle. They are especially useful in atypical trigeminal neuralgia, post-dental pain, postherpetic trigeminal pain, and cases where surgery is not clearly indicated.
Can trigeminal neuralgia still be treated after surgery or Gamma Knife has failed?
Yes. Persistent or recurrent trigeminal neuralgia after MVD surgery, Gamma Knife, rhizotomy, or another procedure does not mean that no further treatment is possible. The first step is to understand why the previous treatment failed. The original diagnosis may have been incomplete, the pain may be atypical, vascular compression may persist, or the main problem may now be nerve injury, facial numbness, anesthesia dolorosa, postherpetic pain, peripheral branch irritation, or central sensitization. Treatment after failed surgery or radiation may include medication redesign, nerve blocks, botulinum toxin, repeat imaging, selected repeat procedures, or a non-surgical pain control plan.
Can an online consultation help identify the trigeminal neuralgia pain generator?
In many chronic trigeminal neuralgia cases, an online consultation can provide useful diagnostic and treatment guidance. The doctor can review MRI or CT reports, previous treatments, medication response, dental history, and the exact pain pattern. During the consultation, the patient can be guided to test facial points, jaw movement, trigger zones, and pain distribution. This is especially useful when the main question is whether the pain is classical trigeminal neuralgia, atypical facial pain, dental-related nerve pain, postherpetic neuralgia, or another mechanism. Online consultation does not replace emergency care, but it can be helpful for second opinion and treatment planning.
When should I seek a second opinion for trigeminal neuralgia?
A second opinion is useful when trigeminal neuralgia treatment is not working, when medication side effects are limiting, when MRI findings do not clearly match the symptoms, or when MVD surgery, Gamma Knife, or rhizotomy has been recommended. It is also useful when the pain is constant, burning, dental-like, post-dental, postherpetic, or atypical, because these forms are often treated incorrectly as classical trigeminal neuralgia. A second opinion should clarify the pain type, the likely pain generator, whether the proposed procedure fits the case, and whether a non-surgical or less invasive option should be tried first.
Can a trigeminal neuralgia consultation be reimbursed by health insurance?
Reimbursement depends on your insurance plan and whether it includes out-of-network or international specialist consultation benefits. We do not bill insurance companies directly, but after the consultation we can provide a formal medical report and a detailed invoice containing the clinical information usually needed for reimbursement claims. Many patients use this documentation when submitting a claim to their insurer. Coverage is not guaranteed, so patients should check their own policy before the consultation if reimbursement is important. The consultation fee is paid directly by the patient, and the report can then be used as supporting documentation for possible reimbursement.
Related Resources on Trigeminal Neuralgia and Facial Pain
Treatment of Trigeminal Neuralgia
You can read about the various forms of primary and secondary headaches on this page.