Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
March 08, 2026
Who This Meralgia Paresthetica Page Is For
This page is intended for patients who have developed burning pain, numbness, or tingling on the outer side of the thigh, especially when meralgia paresthetica has been suspected or diagnosed.
If symptoms worsen with prolonged standing, walking, or pressure from clothing or belts — or if previous examinations suggest compression of the lateral femoral cutaneous nerve — understanding the possible causes, typical course of the condition, and available treatment options may help guide decisions about further evaluation and management. In complex or persistent cases, an individualized neurosurgical second opinion may help clarify the diagnosis and treatment strategy.
When patients seek a second opinion for meralgia paresthetica
• Persistent burning pain, numbness, or tingling on the outer side of the thigh
• Symptoms worsen with prolonged standing, walking, or pressure from clothing or belts
• It is unclear whether the symptoms originate from meralgia paresthetica or from lumbar spine disorders
• Conservative treatment has not improved symptoms over several months
• Persistent hypersensitivity of the skin, burning sensations, or sensitivity to touch (allodynia)
• Uncertainty whether nerve block treatment or surgical decompression should be considered
If your symptoms persist or the diagnosis and treatment options remain unclear, you may request an individualized neurosurgical review here:
Request Second Opinion
What Is Meralgia Paresthetica
Meralgia paresthetica is a condition caused by compression of the lateral femoral cutaneous nerve, a sensory nerve that supplies the skin of the outer thigh. Because this nerve carries only sensory fibers, the condition typically causes burning pain, numbness, tingling, or hypersensitivity of the skin, but it does not cause muscle weakness.
The nerve becomes irritated or compressed most often as it passes under the inguinal ligament near the front of the hip. When this happens, abnormal sensations appear in the outer thigh, sometimes suddenly, but more often gradually.
Meralgia paresthetica is most commonly seen in adults aged 30–50, occurs slightly more often in men, and is strongly associated with obesity, pregnancy, and conditions that increase abdominal pressure.
Although the symptoms can be uncomfortable and persistent, meralgia paresthetica is usually not dangerous and in many patients improves with conservative treatment.
Read more about nerve injuries and other nerve entrapments on this page: https://neurohirurgija.in.rs/en/peripheral-nerve-injury/
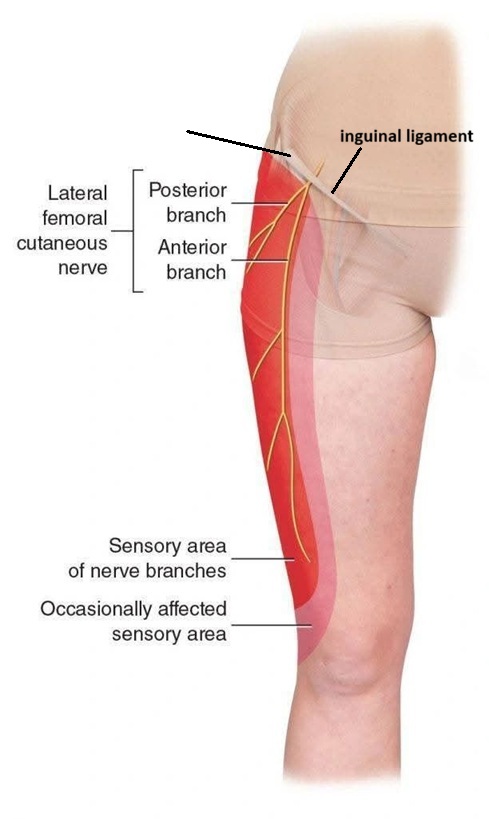
Image: Lateral femoral cutaneous nerve – its relationship with the inguinal ligament and anterior superior iliac spine, its distribution area, and the region affected by meralgia paresthetica.
Anatomy of the Lateral Femoral Cutaneous Nerve
The lateral femoral cutaneous nerve originates from the lumbar nerve roots L2 and L3 in the lower spine. It travels through the pelvis and then passes beneath or through the inguinal ligament, near the anterior superior iliac spine (ASIS), before reaching the outer thigh.
Unlike many other peripheral nerves, this nerve is purely sensory. It does not control muscles and does not affect leg strength.
Because the nerve must pass through a relatively narrow anatomical space near the inguinal ligament, it is particularly vulnerable to external pressure or stretching, which can lead to irritation and symptoms of meralgia paresthetica.
Why the Nerve Becomes Compressed
Several factors can increase pressure on the lateral femoral cutaneous nerve and lead to meralgia paresthetica. Common causes include:
- Tight belts or clothing
- Obesity
- Pregnancy
- Prolonged standing or walking
- Scar tissue after surgery in the groin or pelvic region
- Trauma near the hip
- Diabetes or metabolic conditions that make nerves more sensitive
In many patients, more than one factor may contribute to nerve irritation.
Symptoms of Meralgia Paresthetica
Symptoms typically affect only the outer (lateral) part of the thigh and may include:
- Burning pain in the outer thigh
- Tingling or “pins and needles” sensation
- Numbness of the skin
- Increased sensitivity of the skin to touch
- Symptoms often worsen during prolonged standing, walking, or hip extension, as these positions may increase tension on the lateral femoral cutaneous nerve beneath the inguinal ligament.
- Certain physical factors—such as an arched lower back (anterior pelvic tilt), a protruding abdomen, or tight hip muscles—can change how the pelvis moves. These changes often increase tension around the ligament in the groin area (the inguinal ligament), which can lead to persistent nerve irritation and ongoing pain.
Symptoms usually affect only one side of the thigh and do not extend below the knee.
Because the lateral femoral cutaneous nerve does not control muscles, leg weakness is not a typical symptom. If weakness is present, other conditions may need to be considered.
Symptoms may appear on one side of the body and can range from mild discomfort to persistent neuropathic pain.
How Meralgia Paresthetica Is Diagnosed
Diagnosis is usually based on clinical examination and the typical distribution of symptoms.
During the examination, the doctor may identify a sensitive point near the anterior superior iliac spine, where the nerve passes under the inguinal ligament. Pressure over this area can sometimes reproduce the patient’s symptoms. Certain clinical maneuvers during examination may reproduce or temporarily relieve symptoms (such as positions that increase tension on the inguinal ligament).
Additional tests may be used in selected cases:
- Nerve conduction studies to evaluate nerve function
- Ultrasound to visualize the nerve and surrounding structures
- MRI of the lumbar spine if a spinal cause of symptoms is suspected and MR neurography in selected cases
- Diagnostic nerve block
These tests are mainly used when the diagnosis is uncertain or when other conditions must be excluded.
Conditions That Can Mimic Meralgia Paresthetica
Several disorders can produce symptoms similar to meralgia paresthetica and should sometimes be considered in the differential diagnosis.
These include:
- Lumbar radiculopathy involving the L2–L3 nerve roots
- Femoral nerve neuropathy
- Hip joint disorders
- Local soft tissue conditions of the thigh
Careful clinical evaluation usually allows these conditions to be distinguished.
Conservative Treatment
Most patients improve with non-surgical treatment.
Common approaches include:
- Avoiding tight belts or clothing
- Weight reduction when appropriate
- Anti-inflammatory medications
- Medications for neuropathic pain
- Physical therapy
- Local nerve block injections
- Core strengthening exercises to improve abdominal support
- Postural correction when excessive anterior pelvic tilt contributes to tension near the inguinal ligament
In many patients, symptoms gradually decrease over weeks or months once the pressure on the nerve is reduced.
Surgical Treatment in Persistent Cases
Surgery is rarely necessary, but may be considered if symptoms are severe and persistent despite conservative treatment.
The surgical procedure usually involves decompression of the lateral femoral cutaneous nerve at the point where it passes under the inguinal ligament. Surgical decompression involves exposing the lateral femoral cutaneous nerve near the anterior superior iliac spine and releasing it from fibrous tissue or structures that compress it as it passes beneath the inguinal ligament.
In some cases the ligament or surrounding fascia is partially divided to reduce pressure on the nerve. In selected cases, a neurectomy (cutting the nerve) may be performed to relieve pain, although this results in permanent numbness in the affected skin area.
Less Common Interventions
In selected cases with persistent pain, additional procedures such as radiofrequency ablation of the nerve (using controlled heat to reduce pain signals from the nerve, usually temporary) or surgical neurectomy (nerve section) may be considered. These approaches aim to reduce pain signals but may result in permanent numbness in the affected area and are usually reserved for carefully selected patients.
Request Meralgia Paresthetica Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Persistent burning pain, numbness, or hypersensitivity of the outer thigh may raise several important questions:
Is this really meralgia paresthetica?
Could the symptoms come from the spine or another nerve problem?
Should treatment remain conservative or should nerve decompression be considered?
Why are the symptoms lasting longer than expected?
An independent neurosurgical second opinion may help clarify the cause of lateral femoral cutaneous nerve irritation,
confirm whether the symptoms correspond to meralgia paresthetica or another condition,
and determine whether conservative treatment, nerve block therapy, or surgical decompression
offers the best approach based on the duration of symptoms, neurological findings, and previous treatments.
- ✔ Send a brief message describing your symptoms, when they began, and whether they are triggered by standing, walking, or clothing pressure
- ✔ You will receive a reply within 24 hours explaining whether an online consultation is appropriate and which documentation is required
- ✔ Priority cases: severe persistent burning pain, rapidly worsening sensory symptoms, or unclear diagnosis despite previous medical evaluation — write PRIORITY in your first message
- ✔ Previous medical reports, imaging studies of the lumbar spine or pelvis, EMG results, and other documentation can be reviewed
- ✔ During consultation we explain whether observation, physical therapy, nerve block treatment, or surgical decompression may be appropriate — including expected recovery timelines and up to 10 days of follow-up clarification
Consultation fees typically range from $180–250 depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This corresponds to typical international specialist telehealth neurosurgical second-opinion services.
Why Symptoms May Persist in Meralgia Paresthetica Despite Treatment
This is a common question among patients who continue to experience burning pain, numbness, or hypersensitivity of the outer thigh despite medication, physiotherapy, or lifestyle adjustments.
In many cases, treatment does not fail because the methods themselves are ineffective, but because the source of nerve irritation is not fully relieved. External pressure from clothing, body weight, or prolonged standing may continue to affect the lateral femoral cutaneous nerve even when treatment has been started.
Even when the primary cause is partially addressed, symptoms may persist if mechanical factors such as posture, pelvic tilt, or repetitive strain continue to place tension on the nerve as it passes under the inguinal ligament.
Because of this, persistent symptoms do not always indicate a more serious condition, but rather that contributing factors have not been fully identified or corrected, which may require adjustment of treatment strategy or further evaluation.
Prognosis and Recovery
The prognosis of meralgia paresthetica is generally very good.
Many patients experience gradual improvement with conservative treatment. In some cases symptoms may resolve spontaneously once the cause of nerve compression is removed.
Persistent neuropathic pain is less common but can occur in a small number of patients.
In some patients, particularly when nerve compression has been present for a prolonged period, residual sensory disturbances such as reduced sensation (hypoesthesia) or increased sensitivity of the skin to touch (allodynia) may persist in the outer thigh even after the pain has improved.
When to Seek Specialist Evaluation
Medical evaluation is recommended if:
- Symptoms persist for several months
- Pain significantly interferes with daily activities
- There is uncertainty about the diagnosis
- Symptoms extend beyond the typical area of the outer thigh
A specialist evaluation can help confirm the diagnosis and determine the most appropriate treatment.
Online pain consultation for persistent pain in Meralgia Paresthetica
How the video consultation works — step by step
See the page “Possible Reasons for Poor Pain Treatment Effectiveness of Pain in Meralgia Paresthetica” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
Frequently Asked Questions About Meralgia Paresthetica
What is meralgia paresthetica?
Meralgia paresthetica is irritation or compression of the lateral femoral cutaneous nerve, a sensory nerve that supplies the skin of the outer thigh. The nerve usually becomes compressed as it passes near the front of the hip, under or through the inguinal ligament close to the anterior superior iliac spine. Because this nerve carries sensory fibers only, meralgia paresthetica causes burning pain, numbness, tingling, or hypersensitivity of the outer thigh, but it does not cause true muscle weakness. Symptoms may develop gradually or appear after pressure from belts, tight clothing, obesity, pregnancy, prolonged standing, walking, trauma, or surgery near the groin or pelvis.
What are the most common symptoms of meralgia paresthetica?
The most common symptoms of meralgia paresthetica are burning pain, tingling, pins-and-needles sensation, numbness, or increased skin sensitivity on the outer side of the thigh. Symptoms usually affect one side and typically do not extend below the knee. Many patients notice worsening during prolonged standing, walking, hip extension, pressure from tight belts or clothing, or positions that increase tension near the inguinal ligament. The skin may become sensitive to touch, sometimes causing discomfort from clothing or light pressure. Because the lateral femoral cutaneous nerve is purely sensory, leg weakness is not typical. If weakness, loss of reflexes, or pain extending below the knee is present, another diagnosis should be considered.
What causes meralgia paresthetica?
Meralgia paresthetica is caused by irritation or compression of the lateral femoral cutaneous nerve, most often near the inguinal ligament at the front of the hip. Common contributing factors include tight belts or clothing, obesity, pregnancy, prolonged standing or walking, trauma near the hip, scar tissue after groin or pelvic surgery, and diabetes or metabolic conditions that make nerves more sensitive. Posture and pelvic mechanics can also matter. An anterior pelvic tilt, protruding abdomen, tight hip muscles, or increased tension around the inguinal ligament may keep the nerve irritated. In many patients, more than one factor contributes, so treatment must address both direct pressure on the nerve and the mechanical or metabolic factors that maintain irritation.
Is meralgia paresthetica dangerous?
Meralgia paresthetica is usually not dangerous because it affects a sensory nerve and does not damage the muscles of the leg. It can, however, be very uncomfortable and persistent. Burning pain, numbness, allodynia, or hypersensitivity of the outer thigh may interfere with walking, standing, sleep, clothing tolerance, and daily activities. The condition is also important because symptoms that look like meralgia paresthetica can sometimes come from other disorders, such as lumbar radiculopathy involving L2–L3, femoral nerve neuropathy, hip joint disease, or local soft-tissue conditions. If symptoms are typical and there is no weakness, prognosis is usually good. If weakness, spreading pain, or atypical symptoms appear, further evaluation is needed.
Can meralgia paresthetica go away on its own?
Yes. Meralgia paresthetica can go away on its own, especially when the cause of nerve irritation is temporary and can be removed. Symptoms may gradually improve after avoiding tight belts or clothing, reducing pressure over the groin and hip region, correcting provocative posture, modifying walking or standing habits, or improving abdominal and pelvic mechanics. Pregnancy-related meralgia paresthetica may improve after delivery as pressure and fluid retention decrease. Conservative treatment may also include weight reduction when appropriate, anti-inflammatory medication, neuropathic pain medication, physical therapy, core strengthening, postural correction, and local nerve blocks. Improvement often occurs over weeks or months. Persistent severe burning pain, hypersensitivity, or unclear diagnosis may require specialist reassessment.
How is meralgia paresthetica diagnosed?
Meralgia paresthetica is usually diagnosed from the clinical pattern: burning pain, numbness, tingling, or hypersensitivity limited to the outer thigh, without true leg weakness. During examination, pressure near the anterior superior iliac spine, where the lateral femoral cutaneous nerve passes under the inguinal ligament, may reproduce symptoms. Certain positions may worsen or relieve pain by changing tension around the inguinal ligament. Additional tests are used when the diagnosis is uncertain or when another condition must be excluded. These may include nerve conduction studies, ultrasound, MRI of the lumbar spine, MR neurography in selected cases, or diagnostic nerve block. The main goal is to confirm the nerve source and exclude lumbar, hip, or femoral nerve disorders.
What treatments are available for meralgia paresthetica?
Treatment for meralgia paresthetica usually begins by reducing irritation of the lateral femoral cutaneous nerve. Conservative measures include avoiding tight belts or clothing, reducing pressure around the groin and hip, weight reduction when appropriate, anti-inflammatory medication, neuropathic pain medication, physical therapy, local nerve block injections, core strengthening, and postural correction. If anterior pelvic tilt, protruding abdomen, or tight hip muscles increase tension near the inguinal ligament, therapy should address those factors. Most patients improve without surgery. If symptoms are severe, persistent, and clearly related to nerve compression despite conservative treatment, surgical decompression may be considered. Less common options include radiofrequency ablation or neurectomy in carefully selected patients with refractory pain.
When is surgery considered for meralgia paresthetica?
Surgery for meralgia paresthetica is rarely necessary, but it may be considered when symptoms are severe, persistent, and disabling despite adequate conservative treatment. The usual operation is decompression of the lateral femoral cutaneous nerve near the anterior superior iliac spine, where it passes under or through the inguinal ligament. The surgeon releases fibrous tissue, fascia, or ligament-related compression to reduce pressure on the nerve. In selected cases, neurectomy may be performed to reduce pain signals, but this causes permanent numbness in the affected skin area. Surgery is considered only after confirming that symptoms truly come from the lateral femoral cutaneous nerve and not from lumbar radiculopathy, hip disease, or another condition.
Can meralgia paresthetica leave permanent numbness?
Meralgia paresthetica can leave residual numbness or altered sensation in some patients, especially when nerve irritation has been present for a long time. Because the lateral femoral cutaneous nerve is sensory only, permanent symptoms usually involve reduced sensation, hypersensitivity, burning, or allodynia in the outer thigh rather than weakness. Many patients improve after removing pressure on the nerve, but recovery can be slow if the nerve has been chronically irritated. Surgical decompression may help selected patients, but it cannot always guarantee complete sensory recovery. Neurectomy, when used for refractory pain, intentionally cuts the nerve and usually produces permanent numbness in the affected skin area. This is why treatment choice must balance pain relief against sensory consequences.
Can I obtain an online consultation for persistent thigh nerve pain?
Yes. An online consultation can help when persistent burning pain, numbness, tingling, or hypersensitivity of the outer thigh raises the possibility of meralgia paresthetica. The consultation can review symptom distribution, triggers such as standing, walking, hip extension, belt or clothing pressure, previous lumbar spine or pelvic imaging, EMG results, nerve blocks, and previous treatments. The goal is to clarify whether symptoms fit lateral femoral cutaneous nerve compression, lumbar radiculopathy, femoral nerve neuropathy, hip disease, or another condition. It can also help decide whether continued conservative treatment, physical therapy, diagnostic nerve block, radiofrequency treatment, or surgical decompression should be discussed. Severe persistent pain or unclear diagnosis is a reasonable reason for specialist review.
Why does meralgia paresthetica cause burning pain but not leg weakness?
Meralgia paresthetica causes burning pain but not leg weakness because the lateral femoral cutaneous nerve is a purely sensory nerve. It supplies sensation to the skin of the outer thigh, but it does not control muscles. When this nerve is irritated or compressed near the inguinal ligament, abnormal sensory signals may produce burning, tingling, numbness, pins-and-needles sensations, or hypersensitivity to touch. However, walking strength, knee extension, hip flexion, and muscle power should remain normal. If a patient has true weakness, loss of reflexes, or pain extending below the knee, another condition should be considered, such as lumbar L2–L3 radiculopathy, femoral nerve neuropathy, spinal stenosis, hip pathology, or another neurological disorder.
Can meralgia paresthetica be confused with lumbar radiculopathy or hip disease?
Yes. Meralgia paresthetica can be confused with lumbar radiculopathy involving the L2–L3 nerve roots, femoral nerve neuropathy, hip joint disorders, or local soft-tissue conditions of the thigh. The distinction is important because treatment is different. Meralgia paresthetica usually causes sensory symptoms limited to the outer thigh and does not produce muscle weakness. Lumbar radiculopathy may include back pain, radiating pain, reflex changes, or weakness depending on the nerve root involved. Femoral neuropathy may affect knee extension or sensation in a different distribution. Hip disorders may cause groin pain, mechanical pain, or reduced hip motion. Clinical examination, lumbar MRI, ultrasound, nerve studies, or diagnostic nerve block may be used when the diagnosis is uncertain.
Why do standing, walking, or hip extension worsen meralgia paresthetica?
Standing, walking, or hip extension can worsen meralgia paresthetica because these positions may increase tension on the lateral femoral cutaneous nerve as it passes under or through the inguinal ligament. The nerve runs close to the anterior superior iliac spine at the front of the hip. When the hip extends or the pelvis tilts forward, tension around the inguinal ligament can increase. A protruding abdomen, anterior pelvic tilt, tight hip muscles, or prolonged upright posture may further increase mechanical stress on the nerve. This is why some patients feel better when sitting or changing posture, but worse during walking or standing. Effective treatment often requires reducing both direct pressure and the mechanical factors that keep the nerve irritated.
How do obesity, pregnancy, belts, or tight clothing contribute to meralgia paresthetica?
Obesity, pregnancy, belts, and tight clothing can contribute to meralgia paresthetica by increasing pressure near the inguinal ligament, where the lateral femoral cutaneous nerve enters the thigh. A larger abdomen can change pelvic posture and increase tension around the front of the hip. Pregnancy may add both mechanical pressure and fluid-related tissue swelling. Tight belts, waistbands, work equipment, or compressive clothing can directly press over the nerve pathway. These factors do not always act alone, but they can keep the nerve irritated even when medication or physical therapy has started. Reducing external compression, improving posture, strengthening abdominal support, and addressing weight or pregnancy-related pressure when appropriate can help the nerve recover over time.
Can posture, anterior pelvic tilt, or tight hip muscles keep meralgia paresthetica persistent?
Yes. Posture, anterior pelvic tilt, and tight hip muscles can keep meralgia paresthetica persistent by increasing tension around the inguinal ligament and front of the hip. The lateral femoral cutaneous nerve must pass through a narrow region near this ligament before reaching the outer thigh. If pelvic mechanics repeatedly stretch or compress this area, symptoms may continue even when medication is used. A protruding abdomen, arched lower back, tight hip flexors, or altered walking mechanics can maintain nerve irritation. This does not mean posture is the only cause, but it may be an important contributing factor. Physical therapy, core strengthening, postural correction, and reducing provocative positions can be useful when these mechanics are part of the problem.
What is the role of a diagnostic nerve block in meralgia paresthetica?
A diagnostic nerve block can help confirm meralgia paresthetica when symptoms suggest lateral femoral cutaneous nerve irritation but the diagnosis remains uncertain. Local anesthetic is injected around the nerve, usually near the region where it passes close to the inguinal ligament. If the patient’s typical burning pain, numbness, or hypersensitivity improves temporarily after the block, this supports the nerve as the pain source. A block may also provide therapeutic relief, especially when local inflammation or irritation contributes to symptoms. However, a nerve block is not a permanent solution in every case. If symptoms return, the doctor must decide whether conservative measures, repeated injections, radiofrequency procedures, or surgery are appropriate based on the mechanism and severity.
Can radiofrequency ablation or neurectomy help persistent meralgia paresthetica?
Radiofrequency ablation or neurectomy may help selected patients with persistent meralgia paresthetica when conservative treatment, medication, physical therapy, and nerve blocks do not provide adequate relief. Radiofrequency ablation uses controlled heat to reduce pain signals from the lateral femoral cutaneous nerve, but its effect may be temporary. Neurectomy means cutting the nerve to reduce pain transmission. This may relieve severe refractory pain, but it causes permanent numbness in the skin area supplied by the nerve. These procedures are not first-line treatments. They are considered only when the diagnosis is clear, symptoms are disabling, and the patient understands the trade-off between pain relief and sensory loss. Surgical decompression is usually considered before destructive procedures in appropriate cases.
Why can meralgia paresthetica persist despite treatment?
Meralgia paresthetica can persist despite treatment when the source of lateral femoral cutaneous nerve irritation has not been fully relieved. Medication may reduce neuropathic pain, but external pressure from tight clothing, belts, body weight, standing, walking, or hip extension may continue to irritate the nerve. Symptoms may also persist if posture, anterior pelvic tilt, tight hip muscles, or repetitive mechanical stress continue to increase tension under the inguinal ligament. In some patients, metabolic factors such as diabetes or nerve sensitivity may make recovery slower. Persistent symptoms do not always mean a dangerous condition, but they suggest that the dominant mechanism and contributing factors should be reassessed. Treatment often needs adjustment rather than repetition of the same approach.