Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Neurosurgeon and Pain Management Specialist
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
June 06, 2026
Who This Skull Fractures Page Is For
This skull fractures resource is designed primarily for patients and families whose CT or MRI scan shows a fracture of the skull
— or who have been told there is a fracture of the skull base — and who are being asked to decide between observation, further imaging, or neurosurgical treatment.
This page explains how different types of skull fractures form, how they may injure the brain, sinuses, nerves, or the protective membranes around the brain,
why complications such as cerebrospinal fluid (CSF) leaks or infection can occur,
and how neurosurgeons decide when monitoring is safe and when surgery is necessary.
If you are facing uncertainty about CT or MRI findings, the risk of CSF leakage, infection, facial nerve injury, or the timing and necessity of surgery,
you can request an individualized
neurosurgical second opinion
based on your specific imaging and clinical situation.
When patients usually seek a neurosurgical second opinion for skull fractures
• CT scan confirms a skull fracture and the need for surgery is unclear
• There is concern about a skull base fracture or cerebrospinal fluid (CSF) leak
• Air inside the skull (pneumocephalus) or fluid from the nose or ear is present
• The fracture is depressed, comminuted, or close to critical brain structures
• There are associated findings such as bleeding, brain contusion, or nerve injury
• Conflicting opinions exist regarding observation versus surgical treatment
Skull fractures vary widely in severity, and not all require surgery.
However, fractures involving the skull base, depressed bone fragments, persistent CSF leaks,
or associated brain injury may have important implications for infection risk, neurological outcome,
and long-term recovery.
If you need a clear, individualized neurosurgical assessment based on CT or MRI findings, you can request a telehealth second opinion here:
Request Telehealth Second Opinion
Skull Fractures — Quick Summary (Read This First)
- A skull fracture means that the bone protecting the brain has cracked or broken. It may occur alone or together with bleeding or injury inside the brain.
- Not all skull fractures are the same. Some are thin cracks (linear), while others are pushed inward (depressed) or involve the delicate bones at the base of the skull.
- The most dangerous fractures are those at the skull base. They can tear the protective lining of the brain and allow cerebrospinal fluid (CSF) to leak from the nose or ear.
- Clear fluid from the nose or ear after a head injury is a medical emergency. It may be a sign of a CSF leak and a direct pathway for infection to reach the brain.
- CT scan is the main diagnostic test. It shows the fracture and whether there is bleeding, brain swelling, or trapped air inside the skull.
- Many skull fractures heal without surgery. If there is no major bleeding, brain compression, or persistent CSF leak, careful monitoring and rest are often enough.
- Surgery is needed when the bone is pushed inward, the brain or nerves are injured, or brain fluid continues to leak. The goal is to protect the brain, prevent infection, and restore the skull.
- Even serious skull fractures can have a good outcome when they are recognized early and managed by an experienced neurosurgical team.
- Use the Contents box to jump to sections you are interested in like CSF leaks, surgery, skull base fractures, or reconstruction.
Most families only need the Quick Summary plus the sections on CSF leaks and Surgery. The rest is for deeper understanding.
Skull fractures are a type of head injury (neurotrauma). They may be isolated (no brain injury on imaging) or occur together with traumatic brain injury (TBI) such as epidural hematoma, subdural hematoma, subarachnoid hemorrhage, brain contusions, or diffuse axonal injury.
Learn more about skull anatomy on this page.
How Skull Fractures Happen
Skull fractures occur when external mechanical forces exceed the strength of the cranial bones. These forces are usually transmitted through direct impact with an object (for example the ground, a vehicle, or a blunt instrument), but may also result from rapid deceleration and energy transfer during falls or collisions. The same real-world mechanism (for example a traffic accident, a fall, or an assault) can produce different fracture patterns depending on:
- the direction and concentration of force,
- the object surface area (broad vs focal impact),
- the angle of impact,
- and patient factors (age, bone thickness, previous surgery).
A focal, high-energy impact is more likely to cause a depressed fracture, while broader forces may cause linear fractures or complex multi-fragment patterns. Skull fractures are frequently associated with epidural hematomas.
Skull fractures are primarily caused by direct contact forces, occurring when the head strikes or is struck by an object. However, in high-energy trauma, the same impact also produces inertial forces (acceleration–deceleration). These inertial forces cause the brain to move rapidly inside the skull, leading to associated injuries such as subdural hematoma, brain contusions, and diffuse axonal injury (stretching of nerve fibers). This is why severe head trauma often presents with both a broken bone (skull fracture) and damage to the brain tissue itself on imaging.
Two Major Anatomical Groups
Skull fractures are commonly divided into:
- Calvarial fractures (the “vault” — frontal, parietal, temporal squama, occipital convexity)
- Skull base fractures (anterior, middle, and posterior cranial fossa)
Both groups can occur together in the same patient.

Image: showing the calvaria (skullcap) on the left and the skull base with facial bones on the right.
Calvarial (Vault) Fractures: Main Types
1) Linear fractures
A thin fracture line with no significant bone displacement. Many are treated conservatively if there is no associated intracranial bleeding and the neurological exam is stable.
2) Comminuted fractures
Multiple bone fragments. Risk increases for associated dural injury and underlying brain contusion.
3) Depressed fractures (including comminuted depressed fractures)
A segment of bone is pushed inward toward the brain. The key concerns are:
- possible dural tear,
- underlying cortical contusion,
- risk of infection if the fracture is open,
- and cosmetic deformity (especially in frontal regions).
Important clinical point: the risk of seizures is primarily related to the underlying brain injury, not simply the presence of displaced bone. Therefore, surgery does not reliably prevent post-traumatic epilepsy if a cortical injury has already occurred.
Open vs Closed Fractures
- Open (compound) fracture: scalp laceration communicates with the fracture. Infection prevention becomes a major priority.
- Closed fracture: skin intact; management depends on displacement, symptoms, and associated injuries.

Image: Types of skull fractures
Skull Base Fractures: Regions and “Classic” Clues
Skull base fractures (fractures at the very bottom of the skull where the brain sits) are described by which „floor“ or region is involved. Identifying these common patterns helps determine the risk of complications like infection or brain fluid leaks.
A) Anterior skull base (The „Front Floor“, Anterior fossa) This region is located behind the forehead and above the eyes. It involves the frontal bone and the small, delicate bones (ethmoid) that separate the brain from the nasal cavity.
Why this matters:
- A Tear in the Protective Lining (Dura): The brain is wrapped in a tough, watertight membrane called the dura. Because the bones at the base of the skull are very thin and have sharp edges, a fracture here can easily create a tear in this protective lining.
- CSF Rhinorrhea (Brain Fluid Leak): Once the dura is torn, the clear fluid that cushions the brain (cerebrospinal fluid) can leak through the crack and drip from the nose. If you see clear, watery fluid that drips like a „runny nose“ after an injury, it is a major warning sign that the brain’s sterile environment is no longer sealed. CSF leakage is particularly provoked by leaning forward while sitting or by turning the head to the side—in both cases, when the nose is positioned lower. In normal head positions, CSF typically flows down the throat, giving the patient a sensation of a salty taste.
- Sinus Involvement: Blood can collect in the sinuses (the air-filled spaces in your face), causing facial pressure and swelling shortly after the impact.
- „Raccoon Eyes“ (Periorbital Bruising): Dark, circular bruising around both eyes (not caused by a direct hit to the eyes themselves) is a classic clue that the front part of the skull base is fractured and blood is leaking into the soft tissue around the orbits.
CSF leak may not be obvious immediately. In some patients it appears after hours or days as swelling changes and the initial clot dissolves.
Fractures of the anterior skull base often involve the delicate area where olfactory nerves pass from the nose to the brain. Even if there is no severe brain injury, these tiny nerve fibers can be torn during the impact, leading to anosmia (a partial or total loss of the sense of smell). Patients often notice this change only after the initial swelling and nasal congestion subside, and in many cases, this loss of smell can be permanent.
B) Temporal Bone / Petrous pyramid (Middle Cranial Fossa)
The temporal bone is the thick part of the skull located at the side and base of the head, housing the ear structures and nerves that control facial expressions.
Fractures of this bone are serious and can be associated with:
- Hemotympanum: Blood trapped behind the eardrum (this may look like a dark or purple eardrum during an exam).
- Hearing loss or vertigo: A sudden drop in hearing or a feeling of intense dizziness/spinning.
- CSF otorrhea: Clear brain fluid (cerebrospinal fluid) leaking from the ear canal—a sign that the protective lining of the brain has been torn.
- Facial nerve palsy: Damage to the nerve that controls the face, leading to an inability to wrinkle the forehead, close the eye tightly, or smile on the injured side.
- Battle sign: Distinctive bruising that appears on the bone directly behind the ear, often showing up a few hours after the injury.
Clinical Importance: Temporal bone fractures often occur alongside intracranial bleeding (bleeding inside the skull). Medical evaluation focuses on checking the patient’s brain function (neurological status) and using CT scans to see the extent of the damage. An ENT (Ear, Nose, and Throat) specialist is usually consulted to check for long-term hearing or nerve damage.
C) Other skull base sites (sphenoid sinus, clivus, occipital condyle)
Skull base fractures can also involve the sphenoid sinus, clivus, or occipital condyle (near the C1 articulation). These may be clinically subtle and are usually diagnosed on CT.
Pneumocephalus: Air Inside The Skull
When a fracture involves a sinus or the skull base, air from the outside can sometimes enter the space around the brain. This is known as pneumocephalus.
- What it means: In most cases, small amounts of air are harmless and will be naturally reabsorbed by the body as the fracture heals. However, if a large amount of air enters and creates pressure (tension pneumocephalus), it may require medical intervention to release the trapped air.

Image: The skull base and its three fossae (anterior, middle, and posterior). Percentages indicate the frequency of fractures in each region.
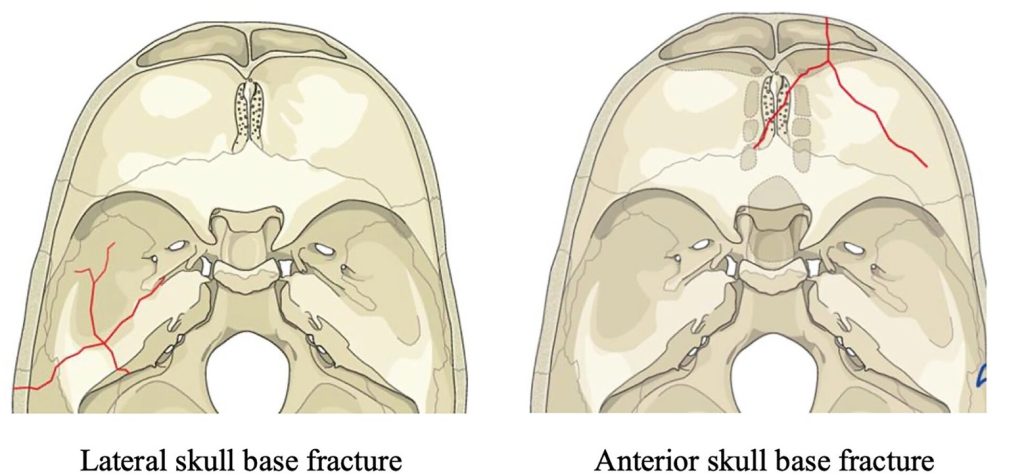
Image: The left side shows a temporal bone (petrous pyramid) fracture, which can cause otorrhagia, hearing loss, facial nerve palsy, and CSF otorrhea. The right side shows an anterior skull base fracture involving the orbit, frontal sinus, and ethmoid bone, often leading to nosebleeds, nasal CSF leak, anosmia, and raccoon eyes.
Request Skull Fracture Neurosurgery Consultation — 24-Hour Review or Priority Option (Usually Within 3 Hours)
When a CT scan shows a skull fracture — especially a fracture of the skull base, temporal bone, or frontal sinus —
families are often confronted with urgent and complex neurosurgical decisions being discussed by the treating team,
which can be difficult to interpret without specialized expertise.
An independent neurosurgical second opinion can help clarify how serious the fracture really is, whether a cerebrospinal fluid (CSF) leak is present or likely to develop,
and what the safest next step should be.
- ✔ Send a short message describing the injury, current symptoms, and what the CT or MRI report says about the skull and skull base
- ✔ You’ll receive a reply within 24 hours explaining if and how we can help in your specific situation
- ✔ Time-sensitive cases: if there is fluid leaking from the nose or ear, worsening neurological symptoms, or facial weakness, consultations can often be arranged within a few hours — write PRIORITY in your first message
- ✔ CT scans, MRI, and hospital reports can be reviewed once initial contact is established
- ✔ During the consultation, we explain fracture patterns, CSF leak risk, infection risk, the need for surgery or observation, and what recovery and reconstruction may involve, with up to 10 days of follow-up for brief questions
Consultation fees typically range from $180–250, depending on fracture complexity and imaging findings.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth second opinions in neurosurgery.
Cerebrospinal Fluid (CSF) Leak: What It Means and Why It Matters
A CSF leak indicates a communication between the intracranial compartment (subarachnoid space) and the nose/ear through a dural and bony defect.
Typical presentations:
- CSF rhinorrhea (nose) — more common with anterior skull base fractures
- CSF otorrhea (ear) — can occur with temporal bone fractures
Why it matters:
- it increases the risk of meningitis,
- and persistent leakage may require procedural or surgical repair.
How is a CSF leak confirmed?
Clear fluid coming from the nose or ear does not automatically mean that it is cerebrospinal fluid. A CSF leak cannot be confirmed by appearance alone. The fluid usually needs to be tested in a laboratory.
The most useful laboratory tests are beta-2 transferrin and beta-trace protein. Beta-2 transferrin is a highly specific marker for cerebrospinal fluid. Beta-trace protein can also support the diagnosis because it is present in much higher concentration in cerebrospinal fluid than in ordinary nasal or ear secretions.
A positive result strongly supports the diagnosis of a CSF leak. However, a negative result does not always exclude a leak, especially if the leak is intermittent, if only a very small amount of fluid was collected, or if the sample was diluted or mixed with other fluid.
Imaging is used to look for the exact place where the leak may be coming from. High-resolution CT of the skull base or temporal bone can show a small bone defect, such as tegmen dehiscence, a fracture, or an opening near the sinuses, middle ear, or mastoid air cells. MRI or MR cisternography can show whether brain covering tissue or fluid is passing through the defect.
In selected cases, CT cisternography may be needed. This is a more specialized test used when the leak site is still unclear. It can help show where cerebrospinal fluid is escaping, especially before surgical repair is considered.
Conservative measures for CSF leak (initial approach in many cases)
Common conservative steps include:
- avoiding nose blowing and straining,
- head elevation and rest,
- stool softeners may be prescribed if needed to reduce Valsalva straining (internal pressure), which helps prevent brain fluid (CSF) from leaking out due to increased pressure.
Key evidence point: Large clinical studies and modern guidelines do not recommend routine prophylactic antibiotics for basilar skull fractures, even when cerebrospinal fluid (CSF) leakage is present. However, the final decision is always made by the treating neurosurgeon, based on the individual patient’s condition, contamination risk, associated injuries, and signs of infection. Antibiotics are clearly indicated when there is clinical or laboratory evidence of infection.
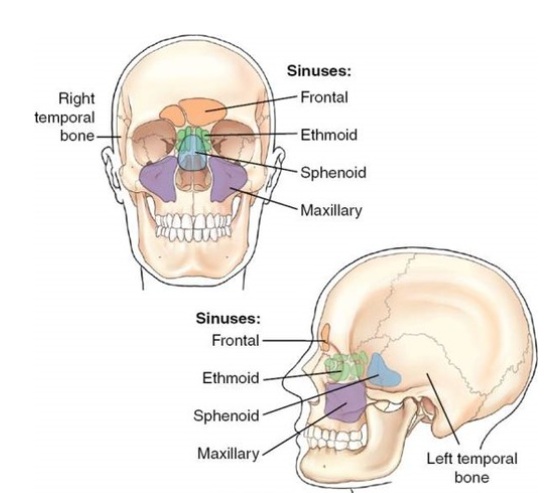
Image: Paranasal sinuses are cavities within the bones that communicate with the nose. In cases of fractures involving the frontal, ethmoid, or sphenoid sinuses, a connection can form between the CSF space and the nose, leading to CSF rhinorrhea (dripping of clear CSF from the nose, especially in provocative positions, such as leaning the head forward).
When Escalation in CSF Leak Treatment Is Considered
If the leak persists or involves a large amount of fluid, specialists may move beyond conservative treatment to more active interventions:
CSF diversion (Lumbar drainage)
In certain cases, a small, flexible tube is placed in the lower back to drain fluid away from the head. This lowers the pressure at the site of the injury, acting like a „pressure relief valve“ to allow the leak in the skull to heal without being constantly pushed open by fluid.
Traditional lumbar drainage relies on gravity, where the fluid flows into a collection bag placed at a specific height relative to the patient’s spine. This requires the patient to remain in strict bed rest, as any change in position could cause the fluid to drain too quickly or too slowly. In contrast, modern lumbar drainage systems can be regulated by a volumetric pump, which ensures a precise and constant flow of fluid regardless of the patient’s position. This allows the patient to remain mobile and walk during treatment, significantly improving comfort and reducing the risks associated with prolonged immobility.
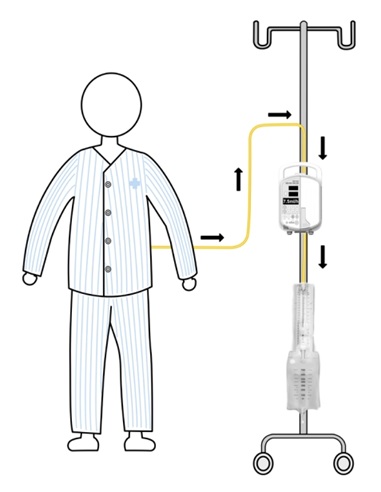
Image: Schematic drawing of pump-regulated volumetric continuous lumbar drainage. Arrows indicate the direction of cerebrospinal fluid drainage.
Definitive surgical closure
When the leak cannot close on its own, a surgical repair is required to seal the communication between the brain and the outside environment. The surgical approach is chosen based on the patient’s anatomy and specific injuries.
Before proceeding with surgery, several diagnostic tools are used to pinpoint the exact location of the leak. A high-resolution CT scan is used to map the bone and identify fractures, while MRI or MR cisternography provides a detailed view of the soft tissues and the fluid itself. In more complex cases, CT cisternography is performed, where a special contrast dye is injected into the spinal fluid to „light up“ the leak on the scan. To ensure precision during endoscopic endonasal repair, a yellow-green dye called fluorescein is often used; it makes the cerebrospinal fluid glow under a special blue light, allowing the surgeon to see the leak „live“ through the endoscope and confirm the exact spot that needs to be sealed.
Transcranial repair
This is a neurosurgical approach where the surgeon reaches the injury by creating an opening in the skull (craniotomy). This „from above“ method is used when there are other internal head injuries that require direct access to the brain, allowing the surgeon to address all issues at once.
Endoscopic endonasal repair
This is a minimally invasive technique where the surgeon uses a camera and specialized tools inserted through the nostrils. This „from below“ approach is used for isolated holes in the front part of the skull base, allowing for a precise repair through the nose without the need for external incisions or opening the skull.
When Is Surgery Needed For Skull Fractures?
Not all skull fractures require surgery. In many cases, especially linear fractures without brain compression or CSF leakage, careful observation is sufficient and safe. Surgery is considered only when the fracture itself creates a risk to the brain, nerves, or infection.
Management is individualized, but common neurosurgical indications include:
Depressed skull fractures
- Open (compound) depressed fractures, especially when depressed more than the thickness of the cranium, are typically treated operatively to reduce infection risk and address dural injury/contamination.
- Closed depressed fractures may require surgery when there is:
- neurological deficit from compression,
- dural tear / CSF leak,
- significant intracranial hematoma requiring evacuation,
- major cosmetic deformity,
- or involvement of the frontal sinus/posterior table requiring specialized management.
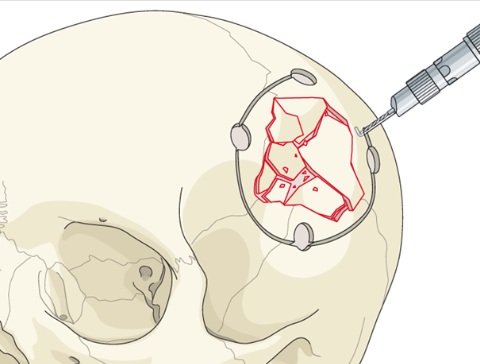
Image: Surgical repair of a depressed skull fracture. The affected bone block is removed so that fragments can be cleaned and realigned. The pieces are then fixed to each other and securely reattached to the surrounding skull.
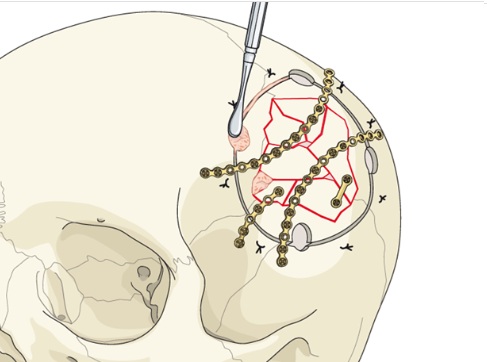
Image: Intraoperative view showing the bone fragments after they have been correctly realigned and securely fixed together.
Frontal sinus posterior table injuries
The „posterior table“ is the thin bone wall at the back of the forehead sinus that separates it from the brain. If this wall is badly shattered or leaking fluid, a procedure called cranialization may be required. In this surgery, the sinus is effectively „removed“ by taking away its back wall and stripping out the mucous membrane lining. The opening leading to the nose is then permanently sealed. This transforms the former air-filled sinus into an extension of the cranial cavity, allowing the brain to occupy the space and preventing infections from the nose from reaching the brain.
Orbital roof fracture with intracranial herniation
A special form of fronto-orbital injury is an orbital roof fracture that allows brain tissue to herniate downward (traumatic encephalocele), potentially displacing the eye (proptosis) and threatening vision. These injuries often require timely surgical repair.
Repairing Skull Defects Later (Cranioplasty)
If a part of the skull is missing after the initial injury or surgery, a reconstructive procedure called cranioplasty is performed. This is done not only for appearance but also to protect the brain and restore the correct pressure inside the skull. The timing depends on the risk of infection and the patient’s recovery.
Titanium mesh and medical-grade cement
For smaller defects, surgeons can use a strong titanium mesh that acts like a scaffold. This is often reinforced with medical-grade cement (a specialized bone substitute) to reshape the area and provide a solid, protective shield over the brain.
Patient-specific implants (3D-printed solutions)
For larger or more complex areas, custom-made implants are used. These are created using 3D-printing technology based on the patient’s actual CT scans. These „perfect fit“ implants are used for mechanically important areas or to achieve an optimal cosmetic result by restoring the natural look of the head and face.
Reconstruction after decompressive craniectomy
In cases of severe brain swelling, a part of the skull is sometimes removed to give the brain room to expand (decompressive craniectomy). To keep the bone fragment alive and sterile for later use, surgeons may surgically „store“ it in a pocket within the patient’s own abdomen. Once the swelling has gone down and the patient is stable, the bone is removed from the abdomen and returned to its original place on the head. This process is the most natural form of cranioplasty because it uses the patient’s own living bone.
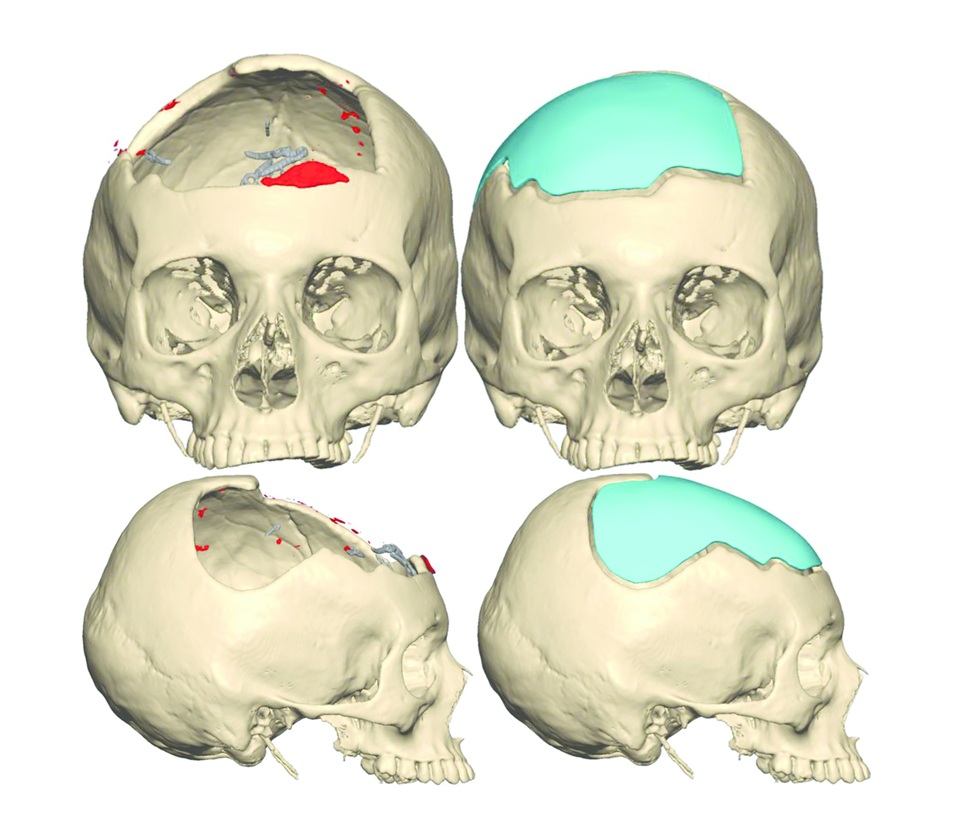
Image: Cranioplasty procedure showing the replacement of a missing skull segment using a custom-made, 3D-printed implant.
Warning Signs: When To Contact Your Doctor Immediately
If you are recovering from a skull fracture at home, you should seek immediate medical attention if you notice any of the following „red flags“:
- Sudden change in fluid leak: A sudden increase in clear fluid dripping from the nose or ear, especially when leaning forward.
- Signs of infection (Meningitis): High fever, a very stiff neck, or an intense headache that is different from the initial injury pain.
- Neurological changes: Unusual drowsiness, confusion, new weakness in arms or legs, or repeated vomiting „in a projectile fashion.“
Frequently Asked Questions About Skull Fractures
What is a skull fracture?
A skull fracture is a break or crack in one of the bones that protect the brain. It usually happens after a fall, traffic accident, assault, sports injury, or other direct head trauma. A skull fracture can be a thin linear crack, a depressed fracture where bone is pushed inward, a comminuted fracture with multiple fragments, or a skull base fracture involving the bottom of the skull. The fracture itself is important, but the main question is whether there is associated brain bleeding, brain contusion, cerebrospinal fluid leak, nerve injury, infection risk, or pressure on the brain.
What are the main types of skull fractures?
The main types of skull fractures include linear fractures, comminuted fractures, depressed fractures, open or compound fractures, calvarial or skull vault fractures, and skull base fractures. A linear fracture is a thin crack without major displacement. A comminuted fracture has several bone fragments. A depressed fracture means that bone is pushed inward toward the brain. An open fracture communicates with the scalp wound and carries a higher infection risk. Skull base fractures are especially important because they can involve the sinuses, ear structures, cranial nerves, or the dura, causing CSF leak from the nose or ear.
What is a linear skull fracture, and does it usually need surgery?
A linear skull fracture is a thin crack in the skull bone without significant displacement of the bone fragments. It is one of the most common skull fracture patterns. Many linear skull fractures do not need surgery if the neurological examination is stable, there is no major intracranial bleeding, no depressed bone, no CSF leak, and no open wound communicating with the fracture. Treatment is usually observation, pain control, head injury precautions, and follow-up when clinically needed. However, the CT scan must be reviewed carefully because a linear fracture can cross important structures, venous sinuses, the skull base, or the middle meningeal artery region.
What is a calvarial or skull vault fracture?
A calvarial fracture, also called a skull vault fracture, involves the upper rounded part of the skull that covers the brain. This includes the frontal, parietal, temporal squamous, and occipital convexity bones. Calvarial fractures may be linear, comminuted, depressed, open, or closed. Their seriousness depends on displacement, whether the fracture is open, whether the dura is torn, and whether there is underlying brain injury such as epidural hematoma, subdural hematoma, brain contusion, or pneumocephalus. Many simple nondisplaced calvarial fractures heal without surgery, while depressed or contaminated fractures may need operative repair.
What is a comminuted skull fracture?
A comminuted skull fracture means that the skull bone is broken into multiple fragments. This usually reflects a stronger or more focused impact than a simple linear fracture. A comminuted fracture can be closed, open, depressed, or associated with underlying brain contusion. The risk depends on whether bone fragments are displaced inward, whether the scalp wound communicates with the fracture, whether the dura is torn, and whether there is bleeding or compression inside the skull. A nondisplaced comminuted fracture may sometimes be observed, but a depressed, open, contaminated, or symptomatic comminuted fracture often requires neurosurgical assessment and sometimes surgery.
What is a depressed skull fracture, and when is surgery needed?
A depressed skull fracture means that part of the skull bone has been pushed inward toward the brain. Surgery is more likely when the depressed fragment compresses the brain, causes neurological symptoms, tears the dura, creates a CSF leak, is associated with an open contaminated wound, produces significant cosmetic deformity, or overlies a hematoma that needs evacuation. Open depressed fractures are especially important because they carry a higher infection risk. Not every depressed fracture automatically requires surgery, but the threshold for neurosurgical evaluation is much lower than for a simple linear fracture because the bone, dura, brain surface, and contamination risk must all be assessed.
Does every skull fracture need surgery?
No. Many skull fractures do not need surgery. A simple linear or nondisplaced calvarial fracture can often be managed with observation if the patient is neurologically stable and CT does not show significant bleeding, brain compression, depressed bone, CSF leak, or an open contaminated wound. Surgery is considered when the fracture creates a direct risk to the brain, dura, cranial nerves, sinuses, or infection control. The decision depends less on the word “fracture” and more on the fracture pattern, associated intracranial injuries, neurological examination, CSF leak, contamination, and whether the skull or brain requires mechanical repair.
When is surgery needed for a skull fracture?
Surgery for a skull fracture is usually needed when there is a depressed bone fragment pressing toward the brain, an open or contaminated fracture, a dural tear, persistent CSF leak, significant intracranial hematoma, brain compression, frontal sinus posterior table injury, orbital roof fracture with brain herniation, or major cosmetic and protective skull defect. Surgery may also be required when a skull base defect fails to seal and continues to leak cerebrospinal fluid. The operation is not performed simply because a fracture line exists. The goal is to protect the brain, prevent infection, repair the dura or skull base, remove dangerous compression, and restore skull integrity.
How is a skull fracture diagnosed on CT scan?
CT scan is the main test for diagnosing skull fractures after head trauma. Bone-window CT images show the fracture line, displacement, depression, comminution, skull base involvement, sinus injury, temporal bone fracture, pneumocephalus, and possible communication with the nose, ear, or sinuses. Brain-window CT images also show associated injuries such as epidural hematoma, subdural hematoma, traumatic subarachnoid hemorrhage, contusion, swelling, or mass effect. MRI can be useful for selected soft tissue, brain, nerve, or CSF leak questions, but CT remains the first-line imaging test for seeing the bone fracture itself.
What is a basilar skull fracture?
A basilar skull fracture is a fracture involving the base of the skull, where the brain rests above the nasal cavity, sinuses, ear structures, cranial nerves, and major blood vessels. These fractures may involve the anterior cranial fossa, middle cranial fossa, temporal bone, sphenoid sinus, clivus, occipital condyle, or posterior fossa. Basilar skull fractures are clinically important because they can tear the dura and create a pathway for cerebrospinal fluid to leak from the nose or ear. They can also cause hearing loss, vertigo, facial weakness, smell loss, pneumocephalus, meningitis risk, or cranial nerve injury.
What are the signs of a basilar skull fracture?
Signs of a basilar skull fracture may include clear fluid leaking from the nose or ear, blood behind the eardrum, hearing loss, vertigo, facial weakness, bruising behind the ear known as Battle sign, bruising around the eyes known as raccoon eyes, loss of smell, or air inside the skull on CT. Some signs appear immediately, while others develop hours or days after injury. Clear watery drainage after head trauma is especially important because it may represent a CSF leak. A basilar skull fracture can be subtle clinically, so CT imaging and careful neurological, ENT, and neurosurgical evaluation may be needed.
What does clear fluid from the nose or ear mean after a skull fracture?
Clear fluid from the nose or ear after a skull fracture may be cerebrospinal fluid, or CSF. This means that the fracture may have torn the dura and created a communication between the space around the brain and the nose, sinuses, middle ear, or mastoid air cells. A CSF leak matters because it can create a pathway for bacteria to reach the brain and meninges, increasing the risk of meningitis. Clear fluid does not prove a CSF leak by appearance alone. Laboratory testing such as beta-2 transferrin or beta-trace protein, plus high-resolution CT or MRI-based imaging, may be needed.
Can a CSF leak after skull fracture heal on its own?
Yes. Some traumatic CSF leaks after skull fracture can heal on their own, especially when the leak is small, recent, and not associated with a large skull base defect or severe contamination. Conservative treatment may include head elevation, avoiding nose blowing, avoiding straining, stool softeners when needed, and close observation. However, a CSF leak should not be ignored. Persistent, recurrent, high-volume, delayed, or infection-associated leakage requires specialist evaluation. The decision depends on the leak site, fracture anatomy, duration, amount of fluid, meningitis risk, and whether imaging shows a defect that is unlikely to close spontaneously.
When does a CSF leak after skull fracture need surgery?
A CSF leak after skull fracture may need surgery when it persists despite conservative treatment, recurs after initially stopping, is high-volume, is associated with meningitis, or comes from a skull base defect that is unlikely to seal on its own. Surgery is also considered when there is a large anterior skull base, temporal bone, frontal sinus posterior table, or tegmen defect. The goal is to close the communication between the intracranial space and the nose or ear, repair the dura, prevent infection, and stop recurrent leakage. The approach may be endoscopic endonasal, transcranial, or through the temporal bone region depending on the leak location.
Can a skull fracture cause meningitis?
Yes. A skull fracture can increase the risk of meningitis when it creates a communication between the sterile intracranial space and the nose, sinuses, ear, or contaminated scalp wound. This risk is especially important with skull base fractures and persistent CSF leaks. Meningitis warning signs include fever, severe headache, neck stiffness, confusion, worsening drowsiness, light sensitivity, or new neurological symptoms. Not every skull fracture causes meningitis, and many heal without infection. The risk depends on dural tear, CSF leak duration, contamination, sinus or ear involvement, open fracture, immune status, and whether the leak is recognized and managed appropriately.
What is pneumocephalus after a skull fracture?
Pneumocephalus means air inside the skull. After a skull fracture, air can enter through the sinuses, mastoid air cells, middle ear, or an open wound if there is a pathway into the intracranial space. Small pneumocephalus is often monitored and may reabsorb over time. It becomes more concerning if it increases, causes pressure on the brain, is associated with a CSF leak, or suggests an open communication between the brain coverings and the outside environment. Tension pneumocephalus is rare but dangerous because trapped air can compress the brain and may require urgent neurosurgical treatment.
Can a skull fracture heal on its own?
Yes. Many skull fractures can heal on their own, especially simple linear or nondisplaced fractures without brain bleeding, depression, open wound, CSF leak, or neurological worsening. Bone healing takes time, and symptoms such as headache, scalp tenderness, dizziness, or fatigue may persist for a period after the trauma. Healing does not mean the injury should be ignored. The important question is whether CT shows associated bleeding, brain contusion, skull base involvement, pneumocephalus, or a fracture pattern that needs closer follow-up. Children and adults may differ in healing speed and risk profile, so management should be individualized.
How long does skull fracture recovery take in adults?
Recovery after skull fracture in adults depends on the fracture type and associated brain injury. A simple linear fracture without brain bleeding may heal over weeks to a few months, while symptoms from concussion, contusion, CSF leak, nerve injury, or surgery can take longer. Patients with skull base fractures may need follow-up for hearing, balance, smell, facial nerve function, CSF leak, or meningitis risk. Depressed or open fractures may require surgery and longer recovery. Return to work, driving, sports, or heavy physical activity should be guided by neurological recovery, imaging findings, symptoms, medications, and the treating specialist’s advice.
Can a skull fracture cause long-term problems?
A skull fracture can cause long-term problems when it is associated with brain injury, nerve injury, CSF leak, infection, hearing loss, smell loss, facial weakness, cosmetic deformity, chronic headaches, dizziness, seizures, or a persistent skull defect after surgery. Many simple fractures heal without long-term consequences, but skull base fractures and depressed or open fractures require more careful follow-up. Long-term problems often come from the associated traumatic brain injury rather than from the fracture line alone. Persistent symptoms after a skull fracture should be interpreted in the context of CT/MRI findings, neurological examination, and the original trauma mechanism.
When should a family seek a neurosurgical second opinion for a skull fracture?
A family may seek a neurosurgical second opinion when the CT report is difficult to understand, surgery is being discussed, a CSF leak is suspected, fluid is coming from the nose or ear, pneumocephalus is present, the fracture is depressed or comminuted, the skull base or temporal bone is involved, or doctors disagree about observation versus repair. A second opinion can also help when there is facial weakness, hearing loss, persistent headache, recurrent fluid leak, infection concern, or uncertainty about recovery and follow-up. The goal is to clarify the actual risk, whether surgery is necessary, and what warning signs require urgent care.
Additional Patient Resources (Skull Fracture / Head Injury)
- Cleveland Clinic — Skull Fracture (Overview, Types, Symptoms, Treatment)
- NHS (UK) — Head Injury & Concussion (Home Care + When to Seek Urgent Help)
- NHS inform (Scotland) — Severe Head Injury (Includes Skull Fracture Section)
- NICE (UK) — Head Injury Discharge Advice Cards (Printable PDF)
- Leeds Teaching Hospitals NHS — Patient Leaflet (Basal Skull Fracture / CSF Leak Mentioned) (PDF)