Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Neurosurgeon and Pain Management Specialist
Specialized Experience:
30 years of clinical expertise in cerebrovascular surgery and neurocritical care.
Last medically reviewed:
May 30, 2026
Who This SAH Page Is For
This page is designed for family members of patients who have suffered a sudden subarachnoid hemorrhage (SAH) due to a ruptured aneurysm, as well as for patients seeking to understand the real risks, ICU course, and treatment options. It explains, in plain language, why aneurysm rupture does not cause a single problem, but several parallel critical conditions that must be treated simultaneously.
Who This SAH Page Is NOT For
This page is not intended to replace emergency medical care or guide immediate treatment decisions in the first hours after aneurysm rupture. It is not designed for self-diagnosis, home management, or delaying hospital treatment. All patients with suspected or confirmed subarachnoid hemorrhage must be managed in a hospital with neurocritical care facilities.
This content is intended to support understanding and informed discussion, not to determine acute treatment decisions.
If you feel overwhelmed by complex terms such as rebleeding, vasospasm, hydrocephalus, or intracranial pressure (ICP), or if you are unsure whether the current treatment plan (clipping, coiling, or conservative care) is truly optimal, you may contact us to see how we provide an individualized neurosurgical second opinion for aneurysm rupture and SAH based on your imaging studies and ICU course.
In such complex cases, standard protocols are rarely sufficient on their own — the outcome often depends on the judgement and experience of a neurosurgeon who understands how these parallel disease processes evolve over time.
When families usually seek a neurosurgical second opinion
• The patient is not waking as expected
• Explanations from doctors feel unclear or inconsistent
• Families must decide about surgery or ICU treatment
• There are many important questions that remain unanswered
In complex or unstable SAH cases, this is a normal and responsible step.
If this reflects your situation, you can request an individualized neurosurgical review here:
Request Second Opinion
Ruptured Aneurysm & Subarachnoid Hemorrhage (SAH) — Quick Summary (Read This First)
- A ruptured brain aneurysm causes SAH (bleeding into the fluid space around the brain). This is a neuro-ICU emergency because risk evolves over days, not just hours.
- The core concept is “parallel processes.” SAH is dangerous because several critical problems unfold at the same time: brain pressure/oxygen instability, rebleeding risk, delayed vessel narrowing, CSF flow blockage, and systemic ICU complications.
- Early rebleeding is the biggest early killer until the aneurysm is secured (blocking blood flow into it). This is why ultra-early securing (coiling or clipping) is the central goal whenever feasible.
- Severity and prognosis depend on “clinical grade + the amount of blood on CT scan.” Doctors describe the clinical condition using GCS / WFNS / Hunt–Hess, while the amount and distribution of blood on CT (the Fisher grade) strongly predicts the risk of vasospasm/DCI (delayed brain damage due to reduced blood flow).
- Even after successful coiling/clipping, the danger is not over. The next critical phase is vasospasm (vessel narrowing) / delayed cerebral ischemia, usually peaking around days 3–9 (often 4–10), and it can cause stroke even when the aneurysm is perfectly secured.
- Sudden deterioration is often driven by high ICP, swelling, or hydrocephalus — and these are often treatable. Rising ICP may be caused by acute hydrocephalus, brain swelling (edema), or associated hemorrhages. Hydrocephalus often requires an EVD to drain CSF and monitor ICP.
- “Not waking up” in the first 72 hours is often not a final verdict. Deep sedation, ICP/swelling dynamics, hydrocephalus/EVD management, metabolic factors, and seizures can all delay responsiveness and cause day-to-day fluctuations.
- Use the Contents box to jump to what you need right now (e.g. ultra-early securing & rebleeding risk, vasospasm window days 4–10 and how it’s treated, ICU pattern in the First 72 Hours, hydrocephalus/EVD and rising ICP, grading scales, coiling vs. clipping, prognosis timeline).
Most families only need the Key Takeaways + the First 72 Hours and Vasospasm (Days 3–9) sections. Everything else is for deeper understanding.
Understanding Brain Aneurysm Rupture: Why the Patient’s Condition Changes and What Families Often Find Confusing
Contents
- Who This SAH Page Is For
- Quick Summary
- What Is a Brain Aneurysm?
- Aneurysm Locations
- Aneurysm Size
- Aneurysm Incidence
- Unruptured vs Ruptured
- What Is SAH?
- Key Facts
- Core Concept: Parallel Processes
- ICP Rise After SAH
- Early Rebleeding
- Rebleeding Statistics
- Vasospasm (Days 3–9)
- Vasospasm Incidence
- Why Vasospasm Matters
- Other Hemorrhages & Hydrocephalus
- Systemic Complications
- Symptoms of Rupture
- How Doctors Grade the Severity of SAH
- Diagnosis Overview
- CT Scan
- CTA Scan
- Lumbar Puncture
- DSA Angiography
- Vasospasm Diagnosis
- Request SAH Consultation
- Treatment Overview
- ICU Stabilization
- Securing the Aneurysm
- Ultra-Early Treatment Timing
- When Securing Is Delayed
- Endovascular Coiling
- Microsurgical Clipping
- Coiling vs Clipping
- Treating Vasospasm
- – Nimodipine
- – Blood Pressure Strategy
- – Vasospasm Interventions
- Treating High ICP
- ICU Care & Monitoring
- First 72 Hours
- Systemic ICU Complications
- Early Prognosis
- Recurrence After Coiling or Clipping
- Late Prognosis After Aneurysmal SAH
- SAH Telehealth Opinion
- What Families Often Ask
- SAH FAQ
- Patient Resources
What Is a Brain Aneurysm?
A brain (intracranial) aneurysm is a weak, balloon-like dilation of an artery. The condition most often occurs where arteries branch, as the vessel wall is under the most stress and is structurally weakest at those points.
These arteries are primarily located within the subarachnoid space. The subarachnoid space is the protective layer surrounding the brain, normally filled with clear, cushioning fluid (Cerebrospinal fluid or CSF). Because the major blood vessels—especially those at the base of the skull where aneurysms commonly occur—travel through this CSF-filled space, rupture releases blood directly into the fluid, causing a Subarachnoid Hemorrhage (SAH). Along with Subarachnoid Hemorrhage (SAH), bleeding can also occur into the brain(Intracerebral Hemorrhage or ICH) and the ventricle (Intraventricular Hemorrhage or IVH).
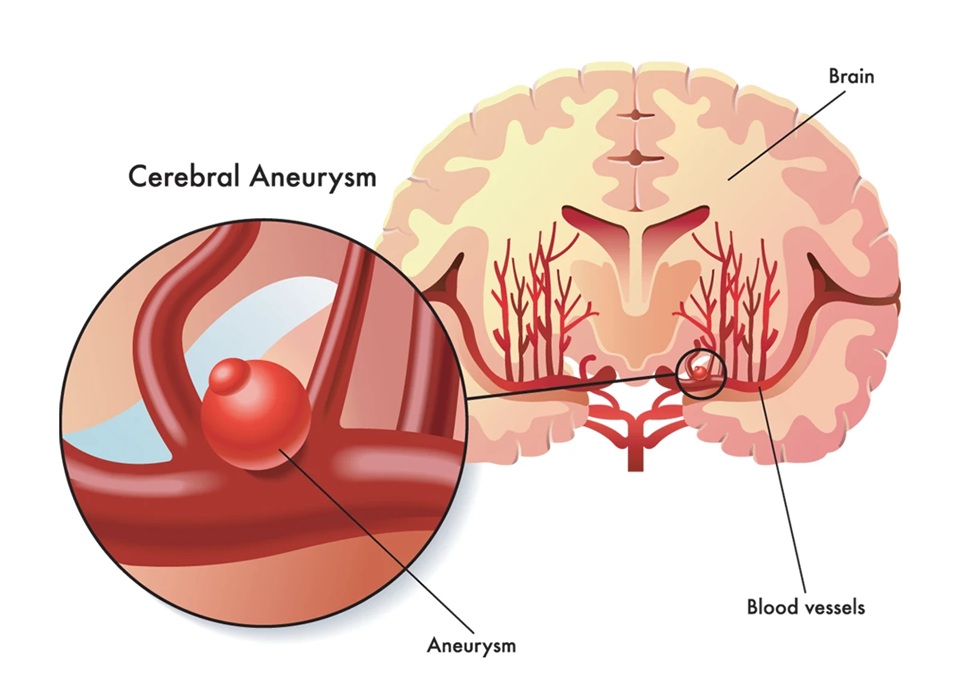
Image: Aneurysm (saccular dilation) at arterial bifurcation in the subarachnoid space at the base of the brain.
Most Common Locations of Brain Aneurysms
- Anterior communicating artery (ACom) – ~30–35%
- Posterior communicating artery (PCom) – ~25%
- Middle cerebral artery bifurcation (MCA) – ~20%
- Intracranial internal carotid artery (ICA) – ~5–7%
- Vertebrobasilar system (less common but often more severe) – ~10% total
Patients will typically encounter these artery names during their diagnosis, which is why we list them, and we show them in the image below to prevent the concept from being abstract.
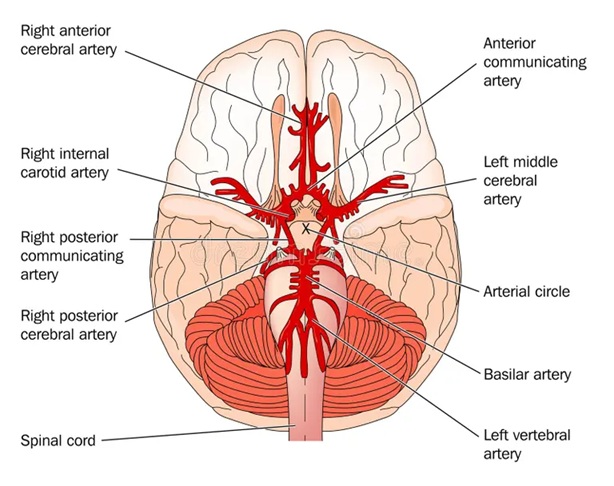
Image: Names of the arteries at the base of the brain where an aneurysm may occur. Read more about brain vascular anatomy here.
Brain Aneurysms Size Classification
- Small: <5 mm
- Medium: 5–10 mm
- Large: 10–25 mm
- Giant: >25 mm
The size and location of the aneurysm are important because larger ones rupture more frequently. Those positioned toward the back of the brain—such as vertebrobasilar aneurysms, which are fortunately rarer—also have a higher risk of rupture. Larger aneurysms are also more difficult to treat.
Incidence and Rupture Risk of Brain Aneurysm
About 2–3% of the general population has an unruptured intracranial aneurysm. The average annual risk of rupture is approximately 0.5–1%, but it increases significantly with aneurysm size and certain locations: <5 mm aneurysms rupture at 0.2–0.5% per year, while giant aneurysms exceed 10% per year. ACom, PCom, and posterior circulation aneurysms are the most rupture-prone. The worldwide incidence of aneurysmal SAH is around 6–10 cases per 100,000 people annually, with exceptionally high rates reported in Finland and Japan (up to 20–22 per 100,000).
Two Different Medical Situations with Cerebral Aneurysms
There is a major difference between:
- Unruptured aneurysm (planned, elective management)
- Ruptured aneurysm (emergency condition causing subarachnoid hemorrhage)
This page focuses entirely on ruptured aneurysms and SAH.
What Is Subarachnoid Hemorrhage (SAH)?
Subarachnoid hemorrhage is bleeding into the subarachnoid space — the area where cerebrospinal fluid circulates around the brain.
Key facts
- Around 85% of spontaneous SAH cases are caused by ruptured aneurysms.
- SAH is one of the most dangerous forms of brain bleeding.
- 30–40% of patients with SAH die despite treatment.
- 10–25% die before reaching a hospital.
- 13–20% die during the initial hospitalization
- Only about 20–30% of patients eventually return to an almost normal life (mRS 0–2), even in modern high-volume neurocritical care centers.
While general mortality rates provide context, they are not true prognostic parameters because survival and recovery after Subarachnoid Hemorrhage (SAH) critically depend on the final amount of brain damage and the severe complications that follow. Predicting the outcome relies on combining multiple factors, such as the initial neurological status (measured by clinical grading), the volume of blood in subarachnoid space on the CT scan (which predicts the risk of delayed damage), patient age, and the emergence of severe secondary complications like vasospasm, brain infarction or infection. These and other parameters appear in different combinations throughout the course of the illness. These factors do not simply add up—they amplify each other’s effects. Only an experienced neurosurgeon can accurately judge their true combined prognostic value, because their complex interaction is far more informative than relying on any generic score alone.
The danger of SAH is not only the bleeding itself — but a series of other conditions that start immediately after rupture.

Image: Different types of intracranial hemorrhage, including SAH.
The Core Concept: A Ruptured Brain Aneurysm Triggers Several Parallel Critical Processes
5 Parallel Critical Processes After SAH
1
Increased ICP
intracranial pressure
intracranial pressure
2
Early rebleeding risk
first hours–weeks
first hours–weeks
3
Vasospasm / DCI
Peak risk: Days 4–10
Peak risk: Days 4–10
4
Associated Brain Complications
ICH / IVH / Hydrocephalus
ICH / IVH / Hydrocephalus
5
Systemic ICU complications
heart, lungs, sepsis
heart, lungs, sepsis
A ruptured aneurysm does not create one medical problem.
It triggers main five different critical diseases at the same time, and each has its own treatment and prognosis.
This is why SAH is so complex and why families often feel overwhelmed.
The main five parallel processes are:
- A sudden spike in intracranial pressure (ICP)
- Risk of early rebleeding
- Vasospasm: This is a critical narrowing of the blood vessels (usually 3–9 days after the rupture) that can lead to a stroke (brain infarction).
- Associated bleedings and complications: ICH, IVH, hydrocephalus
- Systemic complications affecting heart, lungs, and electrolytes
Below is a clear explanation of each.

Image: Rupture of aneurysm with bleeding.
1. Acute Rise in Intracranial Pressure (ICP) After SAH
When the aneurysm ruptures, blood fills the subarachnoid space within seconds.
There is no space inside the skull to accommodate this volume, which causes:
- sudden headache (“thunderclap headache”)
- collapse or loss of consciousness
- nausea and vomiting
- seizures in some cases
Beyond the initial bleeding (SAH), several complications can further drive up ICP, including a secondary blood clot within the brain (intracerebral hematoma), fluid build-up (hydrocephalus), or lack of oxygen (ischemia). Beyond the initial bleeding, a ruptured brain aneurysm causes a problem in the tiny blood vessels (microcirculation) of the brain. This problem involves poor blood flow control (impaired autoregulation), swelling (inflammation), and reduced oxygen supply, which is particularly serious in massive brain bleeds (severe SAH). This damage to the small vessels significantly contributes to early brain injury, and this process can start even before traditional spasms of the main arteries (angiographic vasospasm) are detected.
2. Early Rebleeding — The Most Dangerous Complication
Rebleeding is the leading cause of death in the first hours and days after SAH. The bleeding from the ruptured aneurysm is initially stopped only by a fragile blood clot, or plug, which can easily detach, leading to the high frequency of re-rupture in the first weeks before the vessel wall has a chance to fully heal and stabilize.
Statistics
- Risk of rebleeding within 24 hours: 4–20%
- 25% to 30% within the first month (30 days)
- Mortality of rebleeding: 70–80%
- Nearly all survivors suffer severe disability
- Annual risk of re-rupture remains around 3% to 4% per year after the first year if the aneurysm is left untreated.
This is why securing the aneurysm (clipping or coiling) as early as possible is the central goal of treatment. Securing means permanently sealing the weakened spot to prevent blood from entering the aneurysm, either by surgical clipping (placing a metal clip across the neck) or endovascular coiling (filling the sac with platinum coils).
3. Vasospasm — The Silent Killer Between Days 3 and 9
Vasospasm is often misunderstood, especially by families.
After SAH, the blood vessels become irritated by the blood around them and start to constrict. This narrowing reduces blood flow to the brain and can cause a stroke (brain infarction).
Incidence of Vasospasm
- Vasospasm is detectable in nearly all patients, but about 30% develop clinically significant symptomatic vasospasm.
- Stroke due to vasospasm occurs in 15–30%
This process is separate from the aneurysm itself — even when the aneurysm is perfectly secured, vasospasm can still cause brain damage. The severity/massiveness of the SAH has the greatest influence on the occurrence of vasospasm. This is why the amount and distribution of blood seen on the CT scan remain among the strongest predictors of vasospasm.
Why This is so Important
It is possible to treat the aneurysm successfully — and still lose the patient to vasospasm.
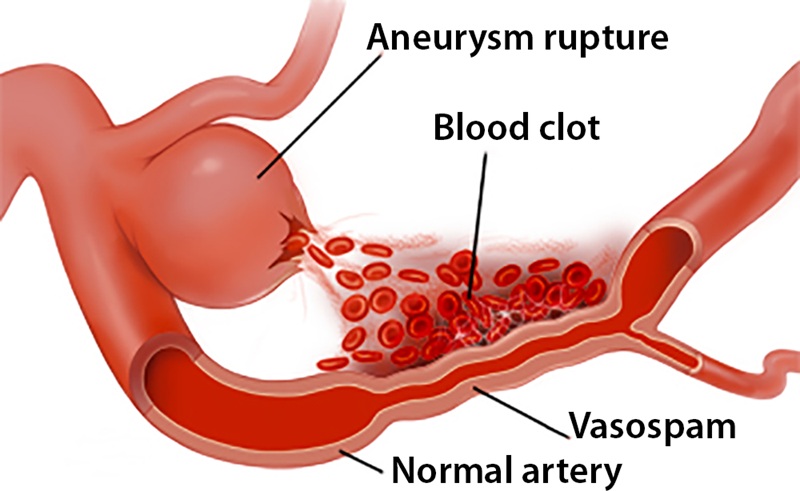
Image: Blood in SAH Causing Vasospasm and Artery Narrowing.
4. Other Hemorrhages and Complications Following SAH
Aneurysm rupture may be accompanied by:
- Intracerebral hematoma (ICH): A serious blood clot within the brain tissue itself.
- Intraventricular hemorrhage (IVH): Bleeding that fills the fluid-filled spaces (ventricles) inside the brain.
- Acute hydrocephalus: A rapid and dangerous build-up of fluid pressure inside the brain. Acute hydrocephalus develops in roughly 20% of patients with aneurysmal SAH.
Hydrocephalus often requires an External Ventricular Drain (EVD). An EVD relieves pressure and allows continuous ICP monitoring. About 15–20% of patients who recover from a ruptured brain aneurysm (SAH) later develop permanent fluid buildup in the brain (chronic hydrocephalus), requiring a permanent drainage tube (VP shunt).
5. Systemic Complications of SAH
SAH is a multi-organ disease.
After rupture, patients are vulnerable to:
- cardiac ischemia
- arrhythmias
- pulmonary edema
- fever
- electrolyte disturbances (especially hyponatremia)
- metabolic dysregulation
All of these conditions require parallel treatment in the ICU.
Symptoms of Aneurysm Rupture
Symptoms largely depend on the size of the SAH, the location of the aneurysm, and the presence of Intracerebral Hemorrhage (ICH). These are the most common symptoms:
- sudden, severe headache (“worst headache of life”). About 20% of patients report a “sentinel headache” days or weeks before the aneurysm ruptures.
- A rapid loss of consciousness is one of the most severe symptoms of SAH, often progressing from mild confusion or drowsiness to deep coma.The precise level of neurological impairment is objectively assessed using the Glasgow Coma Scale (GCS). The GCS is considered the single most critical prognostic tool for both short-term and long-term patient outcomes. A high GCS score indicates a minimal disturbance, while a low score (of 8 or less) signals severe brain dysfunction, which immediately guides urgent treatment decisions. Upon admission for aneurysmal SAH, the distribution of consciousness levels is roughly: 20–30% alert, 30–40% somnolent/confused, and 20–30% comatose.
- neck stiffness
- nausea and vomiting
- photophobia
- confusion
- seizures
- Pupil Dilatation: Often due to a direct lesion by bleeding of the oculomotor nerve, usually caused by the rupture of specific aneurysms (like the posterior communicating artery – A.comm.post) or resulting from compression by a large Intracerebral Hemorrhage (ICH), if present.
- Weakness or Paralysis of Limbs: This manifests as hemiparesis (weakness on one side of the body) and depends on the specific complications and location of the bleed.
How Doctors Grade the Severity of SAH
The table below summarizes the three main scales doctors use to describe how severe a subarachnoid hemorrhage is, so that families can understand what terms like “Hunt–Hess 3”, “WFNS 2” or “Fisher 4” really mean. Scales are here adapted for non-professionals.
How Doctors Grade the Severity of SAH
Hunt–Hess Scale (clinical severity)
| Grade I | Minimal symptoms (mild headache, no deficit) |
| Grade II | Headache and neck stiffness, no clear deficit |
| Grade III | Drowsy or confused, mild weakness |
| Grade IV | Stuporous or shallow coma, marked weakness |
| Grade V | Deep coma |
WFNS Scale (GCS + deficit)
| Grade I | GCS 15, fully awake, no deficit |
| Grade II | GCS 14–13, drowsy or mildly confused, no deficit |
| Grade III | GCS 14–13 with deficit (weakness or speech difficulty) |
| Grade IV | GCS 12–7, deeper disturbance of consciousness (from severe drowsiness to shallow coma) |
| Grade V | GCS 6–3, deep coma |
*GCS (Glasgow Coma Scale) ranges from 3 (deep coma) to 15 (fully awake).
Fisher Scale (CT – blood in the subarachnoid space)
| Grade 1 | No visible subarachnoid blood |
| Grade 2 | Thin layer of blood in the subarachnoid space |
| Grade 3 | Thick clot of blood in the subarachnoid space |
| Grade 4 | Thick subarachnoid blood plus blood in the ventricles (IVH) |
Diagnosis: CT, CTA, LP, and Angiography
CT scan
CT is indicated in any patient with sudden, severe (“thunderclap”) headache, headache lasting more than 6 hours, or headache accompanied by neck stiffness, vomiting, or any neurological deficit. The absence of neck stiffness does not exclude SAH. It is the fastest and most important initial test.
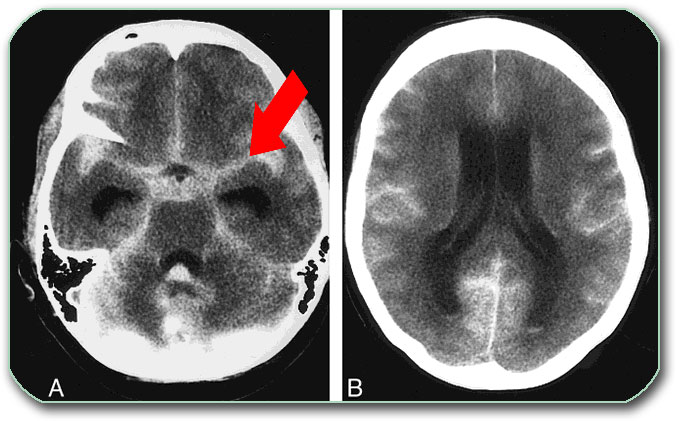
Image: Brain CT showing blood in the subarachnoid space. Fresh blood appears white (red arrow).
CTA (CT angiography)
Provides immediate visualization of the aneurysm. For urgent surgery, CTA is usually sufficient.
Lumbar puncture
Used only when CT is negative but suspicion remains.
DSA (digital subtraction angiography)
The gold standard and usually performed as part of an endovascular procedure. It offers the highest anatomical precision and allows immediate treatment during the same session if needed.
DSA is a minimally invasive imaging technique where a neuro-radiologist inserts a thin catheter, typically through a puncture in the femoral artery in the groin. The catheter is then carefully navigated through the major blood vessels of the chest and neck up to the arteries supplying the brain. Once positioned, a contrast agent is injected. This substance allows detailed X-ray images to visualize the blood flow, which clearly outlines the arteries and identifies aneurysms or other vascular pathologies.
DSA often shows multiple aneurysms in about 20% (10-30%) of cases, and while the ruptured aneurysm is always secured (coiled or clipped), the treatment for unruptured aneurysms is complex. The decision to treat an associated unruptured aneurysm, sometimes done simultaneously, is highly individualized and risk-based.

Image: DSA (angiography) showing brain arteries with the aneurysm marked by an arrow.
Recognizing and Confirming Vasospasm
The onset of vasospasm is often first suspected when the patient’s neurological condition suddenly worsens in the ICU (e.g., new confusion, focal weakness, or decline in consciousness). While clinical deterioration is key, the diagnosis is confirmed using imaging and monitoring techniques:
- Transcranial Doppler (TCD): This non-invasive ultrasound technique is performed right at the bedside in the ICU to measure the speed of blood flow in the major cerebral arteries. A significant increase in velocity strongly suggests arterial narrowing (vasospasm). Transcranial Doppler monitoring typically starts between days 3 and 5 and is performed daily until day 14.
- In deeply sedated or ventilated patients who cannot be examined neurologically, continuous EEG monitoring is recommended to detect early ischemic changes related to vasospasm.
- CT Angiography (CTA) or DSA: If TCD or clinical status indicates severe vasospasm, a CT Angiography (CTA) or Digital Subtraction Angiography (DSA). DSA is performed to visually confirm the narrowing of the vessels and assess its severity, guiding the decision to proceed with interventions like intra-arterial vasodilators or balloon angioplasty.
Request SAH / Ruptured Aneurysm Consultation — 24-Hour Review or Priority Option (Usually Within 3 Hours)
When a loved one is in the ICU with a ruptured aneurysm and subarachnoid hemorrhage (SAH), families urgently need clarity on many critical issues. An independent neurosurgical second opinion offers a clear and confident explanation of complex medical terms such as aneurysm clipping or coiling, trends in ICP, the vasospasm risk window, and the realistic expectations for recovery in the coming days.
- ✔ Send a short message describing the situation and your main questions.
- ✔ You will receive a reply within 24 hours confirming if and how we can help — including the consultation cost and the suggested time
- ✔ For high-urgency cases (like rapid deterioration, vasospasm window, rebleeding concerns), a consultation can usually be arranged within a few hours — write PRIORITY in your initial message.
- ✔ If available, please send recent medical reports following the initial reply.
- ✔ During the video consultation, you will receive a clear, structured explanation of the case and answers to all your questions
Consultation fees typically range from $180–250, depending on the complexity of your case.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Based on our medical report, reimbursement can often be obtained (if your insurance plan allows it).
This is within the usual range for specialist telehealth second opinions in neurosurgery. Families use this service to confirm the diagnosis,
review coiling vs. clipping decisions, understand vasospasm risk, and receive clear guidance during a deeply uncertain time.
Before contacting us, please read our Privacy Policy and Terms of Use.
Treatment of Ruptured Aneurysm
All patients with aneurysmal SAH are admitted to the intensive care unit (ICU) immediately after diagnosis. This is a universal standard, because the first days carry a high risk of rebleeding, hydrocephalus, vasospasm, and sudden neurological deterioration. Treatment happens on five parallel fronts, just as the disease process does.
1. Stabilization in the ICU After SAH if the Patient is Comatose
- Airway Management: This involves intubation and artificial ventilation to ensure proper breathing and oxygenation.
- Blood Pressure Control: Strict regulation using infusions and medications to maintain adequate blood flow to the brain and prevent further bleeding.
- ICP Control: Measures to control the pressure inside the skull (Intracranial Pressure) and prevent secondary brain injury.
- EVD Placement (External Ventricular Drain) if needed: A procedure for the drainage of brain ventricles to relieve excessive fluid and pressure.
2. Preventing Rebleeding (Securing the Aneurysm)
Securing aneurysm means permanently sealing the weakened spot to prevent blood from entering the aneurysm, either by surgical clipping (placing a metal clip across the neck) or endovascular coiling (filling the aneurysm sac with platinum coils). If complete coiling or clipping is not technically possible, partial treatment (“dome protection”) is acceptable, as isolating the rupture point from the circulation significantly reduces the risk of rebleeding.
Optimal Timing: Ultra-Early Intervention
The modern standard of care prioritizes ultra-early intervention for the majority of patients who are neurologically stable (Hunt and Hess Grade I–III):
- Goal: Secure the aneurysm within the first 24 hours, and certainly within 72 hours, of the initial bleed.
- Rationale: This immediately eliminates the highest risk of re-bleeding (which can be up to 30% in the first month) and allows the medical team to aggressively manage vasospasm later without the fear of elevating blood pressure.
When Intervention May Be Delayed (The „Avoidance“ Period)
Intervention is sometimes delayed, though less commonly than in the past, based on the patient’s neurological status:
- Very Poor Neurological Status (Hunt and Hess Grade IV/V): Patients who are in deep coma or have severe brain swelling (edema) are often stabilized in the ICU for a few days. Operating on a severely swollen, damaged brain can increase morbidity, so the risk must be carefully weighed against the risk of re-rupture.
- Peaking Vasospasm Window (Days 4–10): This period was historically sometimes avoided, particularly for surgical clipping, due to the peak risk of brain swelling and vasospasm. However, improvements in coiling techniques (which are less disruptive than open surgery) mean that endovascular procedure is often still performed during this window if needed.
Coiling vs. Clipping
Both methods are effective — the choice depends on anatomy, timing, and local expertise. A specialized cerebrovascular team at the hospital usually decides the best treatment method for the aneurysm. Endovascular coiling is currently the dominant method: it is used for approximately 70% to 80% of ruptured aneurysms and an even higher percentage of unruptured ones, often exceeding 85% in many major centers.
For patients who wish to understand the evidence guiding treatment, the decision between coiling and clipping is based on major clinical trials. The ISAT Trial showed that coiling offered better 1-year outcomes, lower early disability, and slightly lower mortality. Long-term ISAT data confirmed a survival advantage for coiling with fewer long-term cognitive effects, though clipping resulted in lower recurrence rates but a higher incidence of late epilepsy. The BRAT Trial also initially favored coiling, finding that long-term disability was similar but more deficits remained after clipping. Recent Meta-analyses (2021–2024) confirm that while coiling generally leads to fewer early complications, clipping provides a more durable mechanical closure but carries a higher risk of surgical morbidity.
Clinical interpretation:
Coiling is preferred when the patient is critically ill or when fast, minimally invasive treatment is needed. Clipping is chosen for wide-neck aneurysms, aneurysms involving branch vessels, MCA bifurcation anatomy, or when a large hematoma requires open surgery anyway.
Bottom line:
Coiling offers safer early recovery, while clipping provides the most durable closure for anatomically complex aneurysms. The ideal method is chosen individually by the cerebrovascular team.
Endovascular Options for Ruptured Aneurysm
- Coiling (first choice in many centers)– Crucially, it is performed by utilizing the same catheter and arterial access established for the diagnostic DSA (angiography) from the femoral artery in the groin. The neuro-radiologist advances soft, thin platinum coils through this catheter and precisely packs them into the aneurysm sac. Once the aneurysm is densely filled, the blood flow inside stops, causing the blood to clot and permanently seal the weakened spot, thereby preventing re-rupture—all without the need for open brain surgery.
- Stent-assisted coiling
- Balloon remodeling
- Flow Diverters are mesh stents placed across the aneurysm neck to redirect blood flow away from the sac. They work by causing slow, controlled clotting inside the aneurysm over weeks, which is why they are primarily used for unruptured aneurysms. They are rarely used in ruptured cases, but may be employed if superior options are technically impossible (or technically infeasible). They are also used for ruptures of specific aneurysm types, such as blister or fusiform aneurysms.
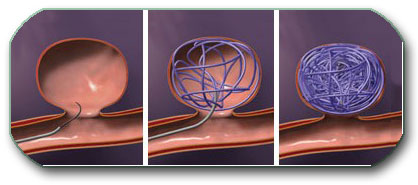
Image: Filling of the aneurysm with coils (aneurysm coiling). This is performed using the same technique as DSA (angiography), meaning without opening the skull.
Microsurgical Clipping
Surgical clipping is a procedure that includes craniotomy (opening the skull), approaching the aneurysm, and securely placing a metal clip across the neck to prevent blood from entering the aneurysm and, consequently, re-bleeding. This is considered a very complicated surgery performed by vascular neurosurgeons. Because endovascular treatment is now dominant, far fewer neurosurgeons perform high volumes of aneurysm clipping, and extensive microsurgical experience has become concentrated in only a small number of specialized centers. Patients with suspected aneurysmal SAH should ideally be transferred to high-volume centers that manage at least 30 aneurysmal SAH cases per year, as outcomes are consistently better in experienced neurovascular units.
Clipping within the first 24 hours can carry higher technical risks due to brain edema and fragile tissue, especially in patients with lower GCS scores. While early securing of the aneurysm is recommended in general, many neurosurgeons proceed more cautiously in patients with GCS <13.
Clipping is preferred when coiling is less effective:
- the aneurysm neck is wide
- artery branches originate from the aneurysm
- MCA (middle cerebral artery) aneurysms with unfavorable anatomy
- previous coiling failed or recurred
- a large hematoma must be evacuated surgically (during the same operation clipping is performed)

Image: Microsurgical clipping of ruptured aneurysm
3. Preventing and Treating Vasospasm After SAH
Nimodipine (Nimotop)
The only proven medication to reduce vasospasm-related stroke. Standard: 60 mg every 4 hours, started immediately.
Hemodynamic Management in Cerebral Vasospasm
In the treatment of vasospasm, which is often present, maintaining a high blood pressure (BP) is vital to maintain blood circulation (perfusion) through the brain by forcing blood past the narrowed arteries. However, the level of BP that can be tolerated is strictly governed by the status of the aneurysm:
- Before securing the aneurysm: Blood pressure must not be too high to avoid causing a fatal re-rupture. Therefore, maintaining optimal brain perfusion can be severely limited.
- After securing the aneurysm: Once the aneurysm is clipped or coiled, the threat of re-bleeding is eliminated, and higher blood pressure is often tolerated or deliberately induced to aggressively push blood through the constricted vessels and prevent stroke.
Interventions When Vasospasm Worsens
When vasospasm becomes severe and compromises blood flow to the brain, immediate intervention is necessary to prevent a stroke. All of these procedures are minimally invasive and are performed by a neuro-radiologist using the same approach as the diagnostic DSA (angiography)—through a catheter inserted into the femoral artery in the groin.
- Intra-arterial Vasodilators: This involves delivering specialized medications (drugs) directly through the catheter and releasing them right at the site where the artery is narrowed. The goal is for these powerful drugs to chemically relax and open up the cramped blood vessel walls to restore blood flow.
- Balloon Angioplasty: This is a mechanical treatment. If drugs don’t work, a tiny balloon catheter is carefully threaded to the narrowed section. The balloon is briefly inflated to physically stretch and widen the artery wall, providing immediate and lasting relief from the constriction.
- Emergency Endovascular Procedures: This is the general term for these urgent, catheter-based treatments (like vasodilators and angioplasty) performed to rapidly reverse the dangerous effects of severe vasospasm and save brain tissue from permanent damage.
Endovascular treatment of vasospasm is generally avoided before the ruptured aneurysm is secured, because vasodilation or mechanical manipulation can increase the risk of rebleeding. These procedures are often (40–60%) repeated several times during the vasospasm window, depending on daily neurological changes.
4. Treating High ICP After SAH
Raised intracranial pressure (ICP) is a serious complication where the pressure inside the skull dangerously compresses brain tissue, restricting blood flow and causing secondary, stroke-like damage. ICP is continuously measured using a small pressure sensor surgically placed by the neurosurgeon. In SAH, an elevated ICP is most often caused by three main factors: acute hydrocephalus (blockage of CSF drainage), an associated intracerebral hematoma, or brain edema resulting from vasospasm.
Treatment in the intensive care unit focuses on maintaining brain blood flow and reducing pressure through several key measures:
- Positioning: The patient’s head is slightly elevated to help venous drainage (improve blood flow out of the brain).
- Sedation: Sedation and pain medication reduce agitation and pain-related pressure spikes.
- Osmotherapy: Medications (such as mannitol or hypertonic saline) are used to draw excess fluid out of the brain tissue.
- Controlled Hyperventilation (via a respirator/ventilator) is a time-limited intervention used to temporarily lower dangerously high ICP by reducing blood CO2 levels, which causes the brain’s blood vessels to constrict and rapidly decreases blood volume inside the skull.
- Seizure Prevention: Antiepileptic drugs (such as levetiracetam) are often given in first 7 days to prevent seizures, which may further increase ICP.
If high ICP is due to hydrocephalus (common in SAH), the placement of an EVD (External Ventricular Drain) to continuously drain CSF is often one of the first required surgical interventions. Hydrocephalus-related ICP crises are among the most common reasons for sudden deterioration in SAH, and families should understand that this complication is both frequent and treatable. Read more about the anatomy of brain ventricles.
5. Intensive Care and Monitoring (ICU): Stabilizing Vitals and Preventing Secondary Brain Damage
ICU care for SAH involves the continuous management of homeostasis (maintaining the body’s stable internal environment). This includes managing oxygenation, blood pressure, sedation, ventilation (breathing support), and fluid and electrolyte balance (managing water and essential body salts and other important molecules in blood). The primary goal is to prevent secondary brain damage, particularly vasospasm (delayed cerebral ischemia, damage caused by restricted blood flow or lack of oxygen), and other systemic complications.
Expected ICU Pattern in the First 72 Hours
The first 72 hours after Subarachnoid Hemorrhage are often the most unpredictable. During this period, the medical team focuses on stabilizing vital functions, securing the ruptured aneurysm, controlling intracranial pressure (ICP), adjusting sedation, and preventing early vasospasm.
It is common for patients with severe SAH to remain unresponsive or minimally responsive even after aneurysm securing (clipping or coiling) or initial treatment — this does not automatically indicate deterioration. Typical day-to-day changes include fluctuations in eye-opening, breathing patterns, limb movements, and ICP trends, which are often influenced by heavy sedation and brain swelling rather than permanent damage. Families should know that meaningful neurological changes usually appear gradually, and some findings that look concerning (such as lack of eye-opening) can still be part of a normal early trajectory.
Families often feel overwhelmed during the first days after an SAH—not knowing whether slow awakening, fluctuating movements, or continued ventilation are normal. These questions are extremely common, and many early signs can look alarming even when the patient is following a typical recovery pattern. Clear, individualized explanations often bring the reassurance and direction families need during this uncertain time. We aim to provide that clarity on this page — and, when needed, through an online neurosurgical consultation.
Preventing Late Fatalities: Management of Systemic Complications
Many late fatalities result from systemic complications: pneumonia, sepsis, multiorgan failure, pulmonary embolism, gastrointestinal (GI) bleeding, renal/hepatic dysfunction, pressure sores, and constipation. Vigilant prevention, early diagnosis, and prompt treatment are essential. Addressing systemic complications such as sepsis, pneumonia, and organ failure is paramount. These conditions significantly increase the risk of secondary ischemic brain injury (in combination with vasospasm) and are major contributors to late fatalities. Systemic complications are a major cause of late mortality after SAH, and they often determine whether the patient stabilizes enough to recover neurologically.
Early Prognosis and Recovery Timeline After SAH
Families often expect rapid improvement, but SAH recovery is slow and unpredictable. Families should not expect daily improvement; instead, the trajectory is usually measured in weeks, not days.
Typical sequence:
- first 1–3 days: stabilization, preventing rebleeding
- days 3–9: vasospasm danger zone
- second and third week: gradual neurological improvement
- weeks to months: rehabilitation and long-term recovery
Definitive prognosis usually becomes clearer after 7–14 days.
In the most severe cases, particularly when massive subarachnoid hemorrhage leads to global brain injury, irreversible brainstem failure may occur. This is the key clinical criterion used to diagnose brain death. A clear explanation of what brain death means and how it is clinically confirmed is provided here.
Recurrence After Coiling or Clipping — What Families Should Know
Securing the aneurysm (coiling or clipping) is designed to permanently eliminate the risk of re-rupture.
However, a small percentage of patients can develop recurrence, and this depends on the type of treatment and the anatomy of the aneurysm.
Coiled Aneurysms — Small Risk of Re-Opening Over Time
Endovascular coiling fills the aneurysm sac with soft platinum coils.
With time, in 5–20% of cases, a part of the aneurysm may:
- re-open (recanalize)
- partially fill with blood again
- or continue to grow at the neck
This is more common when:
- the aneurysm has a wide neck,
- the aneurysm was large or giant,
- the packing density of coils was lower (common in large sacs),
- or when there is higher blood-flow pressure at the aneurysm site.
Most recurrences are small and do NOT require new treatment, but some may need additional coiling or stent-assisted coiling.
Clipped Aneurysms — Very Low Recurrence, But Not Zero
Microsurgical clipping is a durable method: the clip closes the neck and usually eliminates recurrence. However:
- if the clip does not completely close the neck (residual neck),
- or if the aneurysm wall continues to weaken at the edge of the clip,
then a tiny remnant may grow (very rare). Long-term recurrence after clipping is estimated at 1–3%.
How Recurrence Is Monitored Long-Term
Monitoring depends on the treatment type. Modern centers follow a standard schedule:
After Coiling (most important):
- First control: CTA or MRA at 6 months (Follow-up of coiled aneurysms is usually performed with contrast-enhanced MRA, although digital subtraction angiography (DSA) remains the gold standard when precise assessment is required.)
- Second control: CTA/MRA at 12 months
- Long-term: every 2–3 years if previous scans were stable
If a stent or flow-diverter was used, MRI quality may vary, and sometimes DSA is still required.
After Clipping:
- First control: CTA or MRA at 1 year
- If completely closed and stable:
→ further imaging every 5 years, or sooner if symptoms appear
When DSA Is Needed
Digital subtraction angiography (DSA) is still the most precise method and is recommended when:
- CTA/MRA shows unclear filling
- symptoms suggest possible recurrence
- retreatment is being considered
Important Takeaway for Families
Aneurysm treatment is highly effective, but follow-up imaging is essential, especially after coiling. If follow-up is skipped, a small recurrent aneurysm may grow silently for years before causing a problem. This is why CTA/MRA follow-up must be strictly respected.
Late Prognosis After Aneurysmal SAH
Late prognosis after aneurysmal SAH varies widely. Even patients who appear to recover well early can experience long-term difficulties. The most common persistent symptoms include fatigue, headaches, problems with memory, concentration, processing speed, and executive functions. Emotional and behavioral changes are also frequent — anxiety, depression, irritability, mood swings, sleep disturbances, and reduced tolerance to stress.
Focal neurological deficits may remain depending on the area of brain injury, such as weakness, speech or language problems, imbalance, or visual field defects. These often improve gradually over months, but recovery is rarely linear and can fluctuate.
Structured rehabilitation is essential for long-term recovery. Physical therapy helps restore strength, coordination, and mobility. Occupational therapy improves daily functioning and independence. Cognitive rehabilitation targets attention, memory, and higher-order thinking skills. Many patients also benefit from psychological or psychiatric support for anxiety, depression, emotional adjustment, and coping with stress intolerance after SAH.
With a stable rehabilitation plan and regular follow-up, many patients achieve significant improvement over time, even if some residual symptoms persist. Long-term recovery after SAH is best understood as a gradual, multidimensional process involving physical, cognitive, and emotional healing.
Online Second Opinion & Telehealth for SAH
Families often face the most difficult questions in the first hours after an SAH diagnosis:
- Is securing the aneurysm (coiling or clipping) the right intervention for this patient’s current neurological condition?
- Is one intervention (coiling vs. clipping) definitively safer for this specific aneurysm anatomy?
- Is the current timing of the intervention appropriate given the high risk of re-rupture?
- What is the realistic trajectory in the ICU over the next days, especially regarding the risk of vasospasm?
What Families Most Often Ask in the ICU — And What These Signs Really Mean
Subarachnoid hemorrhage is a dynamic condition, and the patient’s status can change from day to day. Families most often need clear answers to what these changes actually mean.
Why is the patient not waking up — is this a bad sign?
Not waking up early is common and does not automatically mean permanent brain damage. It is often caused by a combination of the initial injury, high intracranial pressure (ICP), sedation, hydrocephalus, or metabolic factors. What matters is the overall trend and whether the causes are treatable.
Does every ruptured aneurysm require surgery?
In most cases, the aneurysm must be secured to prevent rebleeding. This is done by coiling or clipping, but the timing and approach depend on the patient’s condition and imaging findings.
Which procedure is better — coiling or clipping?
There is no single best option. The choice depends on aneurysm anatomy, patient status, and surgical risk. In some cases coiling is safer, in others clipping is more definitive.
Why does the condition change from day to day?
After rupture, several processes occur at the same time — vasospasm, ICP changes, hydrocephalus, and ICU complications. Because of this, recovery is not linear and fluctuations are expected.
How long does ICU treatment usually last?
The most critical period is 10–14 days, when the risk of complications is highest. Recovery varies widely depending on the severity of the injury and the occurrence of complications.
FAQ – Ruptured Aneurysm & Subarachnoid Hemorrhage (SAH)
How dangerous is aneurysmal SAH and what are the chances of survival?
Aneurysmal subarachnoid hemorrhage (SAH) is one of the most dangerous forms of brain bleeding. Some patients die before reaching the hospital, and overall mortality remains high even with modern treatment. However, population statistics cannot predict the outcome for one individual patient. Prognosis depends on the patient’s neurological condition at admission, the amount and distribution of blood on the first CT scan, whether the aneurysm rebleeds, and whether complications such as vasospasm, hydrocephalus, high intracranial pressure, infection, or systemic organ failure occur. This is why doctors combine clinical grade, CT findings, ICU evolution, and response to treatment rather than relying on one number alone.
How long can a patient remain unconscious after SAH, and does it always mean a poor outcome?
A patient with severe SAH may remain unconscious or only minimally responsive for several days, especially in the first 72 hours. This does not automatically mean that the prognosis is hopeless. Delayed awakening can be caused by the initial brain injury, deep sedation, swelling, hydrocephalus, high intracranial pressure, seizures, metabolic disturbances, or systemic ICU complications. The key question is whether the lack of response is explained by treatable factors and whether the overall trend is improving or worsening. Prognosis usually becomes clearer after sedation is reduced, ICP and hydrocephalus are controlled, and the vasospasm window is carefully monitored. In many cases, the first few days are too early for a final judgment.
What does the amount of blood on CT mean after aneurysmal SAH?
The amount and distribution of blood on the first CT scan are very important after aneurysmal SAH. Thick blood in the subarachnoid space, blood inside the ventricles, or associated bleeding inside the brain usually means a higher risk of complications. The Fisher scale is used to describe CT blood burden and helps estimate the risk of vasospasm and delayed cerebral ischemia. A patient with a relatively good neurological condition can still be at risk if the CT shows a large amount of blood. Conversely, a severe clinical presentation with less visible blood may still reflect major early brain injury. CT findings must therefore be interpreted together with the clinical grade, GCS, aneurysm anatomy, and ICU course.
Is endovascular coiling safer than microsurgical clipping for ruptured aneurysms?
Endovascular coiling is often safer in the early phase for many ruptured aneurysms because it is less invasive and can usually be performed quickly through the blood vessels, without opening the skull. This is especially important in critically ill patients or when ultra-early aneurysm securing is needed. However, clipping may be more durable and is still preferred for some aneurysms, especially wide-neck aneurysms, middle cerebral artery aneurysms, aneurysms involving important branches, or cases where a large brain hematoma must be removed surgically. There is no single best method for every patient. The safest choice depends on aneurysm anatomy, neurological condition, timing, and the experience of the treating neurovascular team.
Why is it important to secure the ruptured aneurysm early after SAH?
After an aneurysm ruptures, the bleeding may stop temporarily because a fragile clot forms at the rupture site. This clot is unstable and can detach, causing rebleeding. Rebleeding is one of the most catastrophic early complications of aneurysmal SAH and is associated with very high mortality and severe disability among survivors. For this reason, the central early goal is to secure the aneurysm, usually by coiling or clipping, as soon as it is technically and medically feasible. Once the aneurysm is secured, the risk of another rupture from that aneurysm becomes much lower, and doctors can treat other problems, especially vasospasm and blood pressure management, more safely and aggressively.
If the aneurysm is secured early and the patient looks good afterward, does that mean the danger is over?
Not necessarily. Securing the aneurysm is a crucial step because it greatly reduces the risk of rebleeding, but it does not stop all SAH-related dangers. A ruptured aneurysm triggers several parallel critical processes that continue to evolve after coiling or clipping. These include vasospasm, delayed cerebral ischemia, hydrocephalus, brain swelling, fluctuations in intracranial pressure, seizures, and systemic ICU complications affecting the lungs, heart, electrolytes, or infection risk. Some patients appear stable immediately after treatment but deteriorate several days later, especially during the vasospasm window. This is why ICU monitoring remains essential even when the aneurysm itself has been successfully secured.
What is cerebral vasospasm, and what is the vasospasm window after aneurysmal SAH?
Vasospasm is a delayed narrowing of the brain arteries after SAH. Blood in the subarachnoid space irritates the artery walls, causing them to constrict. When narrowed arteries cannot deliver enough blood to the brain, the patient may develop delayed cerebral ischemia or stroke. Vasospasm usually begins after the first few days and most often becomes clinically important between days 3 and 9, although many centers monitor carefully until about day 14. It can occur even when the aneurysm has been perfectly treated. The risk is higher when the initial CT scan shows thick or widespread subarachnoid blood, which is why daily neurological assessment, TCD monitoring, CTA, or DSA may be needed.
Can vasospasm cause stroke even after the aneurysm has been secured?
Yes. This is one of the most important points families need to understand. Coiling or clipping prevents blood from entering the ruptured aneurysm again, but vasospasm is a separate process caused by blood already present around the brain arteries. If vasospasm becomes severe, blood flow may fall below the level needed by brain tissue, causing delayed cerebral ischemia or infarction. This can happen days after the aneurysm has been successfully secured. Treatment may include nimodipine, careful blood pressure and fluid management, and in severe cases endovascular procedures such as intra-arterial vasodilators or balloon angioplasty. The goal is to prevent a secondary stroke during the critical vasospasm window.
Why is an EVD used after ruptured aneurysm and SAH?
Hydrocephalus means that cerebrospinal fluid is not circulating or draining normally, causing pressure to build up inside the brain’s ventricles. After aneurysmal SAH, this often happens because blood blocks the normal CSF pathways. Acute hydrocephalus can cause sudden worsening of consciousness, raised intracranial pressure, vomiting, pupil changes, or neurological decline. An external ventricular drain (EVD) is a temporary tube placed into the ventricles to drain CSF and monitor intracranial pressure. In many SAH patients, EVD placement is not a sign that treatment has failed; it is a common and often life-saving intervention. Some patients later need a permanent VP shunt if hydrocephalus persists after the acute phase.
What ICU complications can occur after aneurysmal SAH?
SAH is not only a bleeding event inside the brain. It is a neurocritical condition that can affect the whole body. Important brain-related complications include rebleeding, hydrocephalus, intraventricular hemorrhage, intracerebral hematoma, high intracranial pressure, seizures, vasospasm, and delayed cerebral ischemia. Systemic complications are also common and may include pneumonia, sepsis, cardiac ischemia, arrhythmias, pulmonary edema, electrolyte disturbances, fever, kidney or liver dysfunction, pulmonary embolism, and multiorgan failure. These complications can strongly influence survival and recovery. For this reason, good SAH care requires more than treating the aneurysm; it requires continuous ICU monitoring and prevention of secondary brain and systemic injury.
Why can the patient’s condition change from day to day after SAH?
Day-to-day fluctuation is common after SAH because several processes evolve at the same time. A patient may look more awake one day and less responsive the next because of sedation changes, ICP variation, hydrocephalus, fever, infection, sodium imbalance, seizures, vasospasm, or changes in ventilation and oxygenation. This does not always mean permanent deterioration, but it always requires careful interpretation. The ICU team follows neurological examination, CT findings, ICP values, EVD drainage, blood tests, TCD velocities, CTA or DSA results, and systemic complications. Families should focus less on one isolated sign and more on the overall trend: whether treatable causes are being controlled and whether brain perfusion remains protected.
When does the prognosis become clearer, and how long does recovery after SAH usually take?
Early prognosis after SAH is often uncertain. The first 72 hours are usually focused on stabilization, preventing rebleeding, securing the aneurysm, controlling intracranial pressure, and treating hydrocephalus if present. The next major danger period is the vasospasm window, usually days 3–9 and often monitored through the second week. Prognosis becomes clearer after 7–14 days, when sedation is reduced and the effect of major complications can be assessed. Recovery is usually measured in weeks and months, not days. Some patients improve slowly after a very difficult ICU course, while others develop delayed stroke, infection, or systemic complications that change the outlook. Rehabilitation may continue for months or longer.
Can SAH happen again after a ruptured aneurysm has been coiled or clipped?
Once the ruptured aneurysm has been securely clipped or coiled, the risk of bleeding again from that same aneurysm is usually very low. However, the risk is not always zero. After coiling, a small part of the aneurysm may reopen over time, especially if the aneurysm was large, wide-necked, or incompletely packed. After clipping, recurrence is rarer, but a small residual neck or remnant can occasionally grow. Some patients also have multiple aneurysms or may develop new aneurysms later, particularly if they smoke, have uncontrolled high blood pressure, or have a strong family history. Follow-up imaging with CTA, MRA, or DSA is therefore important, especially after coiling.
What if a small, unruptured aneurysm is found incidentally during SAH evaluation?
Some patients are found to have more than one aneurysm when CTA or DSA is performed after SAH. The ruptured aneurysm must be identified and secured first, because it is the immediate source of danger. A second small, unruptured aneurysm does not always require treatment during the same hospitalization. The decision depends on its size, shape, location, patient age, medical condition, rupture risk, and whether treating it would add unnecessary risk during an already critical illness. In some cases, an additional aneurysm is treated during the same session; in others, it is monitored and discussed later. This decision should be individualized by an experienced cerebrovascular team.
What long-term problems can remain after SAH, even if the patient survives?
Many SAH survivors have long-term symptoms even when they appear physically better. Common problems include fatigue, headaches, reduced concentration, memory difficulty, slower processing speed, anxiety, depression, irritability, sleep disturbance, and reduced tolerance to stress. If stroke, hydrocephalus, or brain swelling caused focal injury, patients may also have weakness, speech problems, imbalance, visual field defects, or difficulty with daily activities. Recovery is often gradual and non-linear. Physical therapy, occupational therapy, cognitive rehabilitation, and psychological support may all be needed. A patient may survive the acute hemorrhage but still require long-term follow-up because SAH affects physical, cognitive, and emotional recovery at the same time.
Are family members at higher risk of aneurysms, and should they be screened?
A family history of aneurysmal SAH can increase the risk of brain aneurysms, especially when two or more first-degree relatives, such as parents, siblings, or children, have been affected. In these higher-risk families, screening with non-invasive vascular imaging such as MRA or CTA may be considered. When only one family member has had an aneurysm, routine screening of all relatives is not always necessary, but it may still be discussed if there are additional risk factors such as smoking, uncontrolled hypertension, certain connective tissue disorders, or strong anxiety about family risk. The decision should be individualized, because screening can detect aneurysms that may never rupture but still create difficult treatment decisions.
When is it helpful to request an online neurosurgical second opinion for SAH?
A neurosurgical second opinion can be helpful when families do not understand the CT, CTA, DSA, or ICU explanations, when there is uncertainty about coiling versus clipping, when the patient is not waking as expected, or when deterioration occurs during the vasospasm window. It can also help when hydrocephalus, EVD management, high intracranial pressure, brain swelling, or unclear prognosis are causing concern. A second opinion does not replace emergency ICU treatment, but it can provide a structured explanation of what has happened, which risks are still active, and which questions families should ask the treating team. In complex SAH cases, clarity often depends on interpreting imaging, neurological status, and ICU trends together.
Can I download the SAH grading scales (Hunt–Hess, WFNS, Fisher) as an image chart adapted for non-professionals?
Yes. You can download all three grading scales — Hunt–Hess, WFNS, and Fisher — in one single image here: SAH grading chart (JPG). This chart is adapted for non-professionals and can help families understand terms used by doctors when describing the severity of aneurysmal SAH. The Hunt–Hess and WFNS scales mainly describe the patient’s clinical neurological condition, while the Fisher scale describes the amount and distribution of blood on CT. These scales are useful for orientation, but they do not replace individualized interpretation of the patient’s full ICU course.
Can I get reimbursed by my health insurance for this consultation?
Reimbursement depends on your insurance plan, country, and the type of out-of-network or telehealth coverage included in your policy. We do not bill insurance companies directly. However, when a written medical report is provided, it can usually be accompanied by a detailed invoice containing the clinical information commonly required for reimbursement claims. Some patients may be able to submit this documentation to their insurer, especially when the consultation is related to a serious neurosurgical emergency such as ruptured aneurysm and SAH. Approval is never guaranteed, so patients should check their insurance rules before assuming that reimbursement will be accepted.
Additional Resources for Patients & Families
The links below lead to reputable organizations that provide additional information about brain aneurysms and subarachnoid hemorrhage (SAH). They can help you better understand the diagnosis, treatment options, and recovery process, and may offer support resources for families.
- Mayo Clinic – Brain Aneurysm: Symptoms & Causes – clear overview of brain aneurysms, risk factors, symptoms, and when to seek emergency care.
- Brain Aneurysm Foundation – About Brain Aneurysms – patient-focused information about aneurysm types, rupture, and treatment options, plus support resources.
- NHS – Subarachnoid Haemorrhage – UK National Health Service explanation of SAH symptoms, causes, treatment, and recovery.
- Stroke Association (UK) – Haemorrhagic Stroke & SAH – information about haemorrhagic stroke, including subarachnoid haemorrhage, practical advice and support.
- Leeds Teaching Hospitals – Aneurysmal Subarachnoid Haemorrhage Booklet – detailed patient and family booklet for those admitted with aneurysmal SAH.
- Oxford University Hospitals – Subarachnoid Haemorrhage (Head2Head) – concise explanation of SAH, ICU care, and what families can expect during hospital treatment.
Related neurocritical pages
On this page, you can learn more about other neurosurgical cerebrovascular diseases.