Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 10, 2026
Who this page is for
This page is for patients who have been diagnosed with fibromyalgia but still have one or several painful body regions that dominate the whole clinical picture — such as low back pain, neck pain, chest wall or rib pain, pelvic or bladder pain, headache, facial pain, sciatica-like pain, or joint-region pain.
Fibromyalgia can increase overall pain sensitivity, but it does not automatically explain every local pain. A patient may have fibromyalgia and still have a separate dominant pain generator, such as a facet joint, sacroiliac joint, muscle-fascial trigger point, inflamed tendon or bursa, irritated peripheral nerve, intercostal neuralgia, occipital neuralgia, trigeminal-type facial pain, or a spine-related pain source.
This page focuses on five practical questions:
- Why does pain persist despite standard fibromyalgia treatment?
- Is the most disabling pain truly caused only by fibromyalgia?
- Is there a dominant local pain generator that needs separate diagnosis?
- Can MRI or laboratory tests be normal while a treatable local source still exists?
- How should systemic fibromyalgia care and targeted local pain treatment be combined?
If you recognize this pattern, a focused online pain consultation can help clarify whether pain is mainly systemic, local, or mixed — and whether targeted treatment of the dominant local pain source may improve the overall fibromyalgia pain pattern.
If you are unsure whether an online consultation can help after all previous tests and treatment, read why this consultation is different.
When patients usually seek a second opinion for fibromyalgia pain
- Widespread or migrating pain persists despite standard fibromyalgia treatment
- Localized pain (neck, back, chest, pelvis, or limbs) dominates the symptom picture
- Imaging and lab tests are normal, yet pain remains severe
- Medications provide only partial or temporary relief
- You are unsure whether all pain truly comes from fibromyalgia or if a treatable focal source exists
If this reflects your situation, a focused telehealth review can help distinguish fibromyalgia-related sensitization from focal nerve or musculoskeletal pain — and clarify what targeted treatments may actually help: Request Consultation
Contents
- What Is Fibromyalgia?
- Who Is Affected
- Main Symptoms
- Diagnosis
- General Treatment
- Local Pain Sources: Back, Neck, Headache, etc.
- Identifying the Dominant Pain Source
- Treatment Approach for Dominant Pain
- Why This Approach Works
- Why Pain Persists in Fibromyalgia
- Prognosis and Long-Term Management
- FAQ About Pain in Fibromyalgia
- Additional Information for Patients
Many people diagnosed with fibromyalgia feel pain “everywhere,” yet in clinical reality one or a few regions usually dominate — the neck, shoulders, low back, or pelvis.
Real improvement often begins when the physician identifies what exactly hurts within a local pain syndrome — and why: whether it is a muscle in spasm, an inflamed tendon or a compressed nerve.
Effective management then requires two parallel levels of care: treatment of fibromyalgia as a systemic pain condition, and treatment of the specific causes of the dominant pain syndromes that maintain or amplify it.
What Is Fibromyalgia?
Fibromyalgia is a systemic pain-sensitivity disorder, but many patients also have dominant local pain generators that must be diagnosed and treated separately.
Definition
Fibromyalgia is a chronic pain syndrome characterized by widespread musculoskeletal pain, fatigue, and non-restorative sleep.
Fibromyalgia involves two closely interacting mechanisms.
The first is a disturbance of pain neuromodulation within the central nervous system — including the brain and spinal cord — where pain-transmitting neurons become overly sensitive (central sensitization) and the normal descending inhibitory pathways that regulate pain perception become less effective. This leads to an exaggerated pain response even to mild stimuli.
The second mechanism is a tendency of the body to develop and sustain local musculoskeletal pain sources such as low-grade inflammation, muscle spasm, or nerve irritation. This occurs because in fibromyalgia there is a predisposition of the tissues to metabolic and microcirculatory disturbances, and mild activation of inflammatory pathways in muscles, fascia, and small nerve fibers. These changes make the tissues more reactive to everyday mechanical or metabolic stress and more likely to maintain chronic pain.
Central sensitization often coexists with ongoing pain input from local sources in muscles, fascia, or small nerves, which are responsible for the predominant pain in certain body regions. Both mechanisms contribute to the pain and other symptoms of fibromyalgia, yet treatment is frequently focused only on the central disturbance of neuromodulation, while local pain syndromes remain underrecognized and undertreated. In practice, effective management requires addressing both — restoring normal pain modulation in the nervous system and identifying treatable local pain generators.
Who Is Affected
- Most common in women between 30 and 60 years old.
- Prevalence is estimated at 2–4% of the general population.
- Fibromyalgia often overlaps with other chronic pain syndromes such as irritable bowel syndrome, temporomandibular joint disorder, chronic pelvic pain, and tension-type headache.
- Symptoms can start or worsen after infection, emotional stress, trauma, or surgery.
Main Symptoms
- Diffuse aching or stiffness in multiple body regions lasting over 3 months.
- Fatigue, feeling unrefreshed after sleep, and morning stiffness.
- Cognitive issues (“fibro-fog”) — problems with focus and memory.
- Headache, tingling, jaw or chest wall pain, and sensitivity to pressure or temperature.
- Depression and anxiety are common in fibromyalgia, often developing as a reaction to chronic pain, poor sleep, and reduced daily functioning. However, the two conditions are distinct diagnoses and should not be reduced to one. A person with depression may experience pain or tenderness, and if fibromyalgia criteria are met, both diagnoses are made. Likewise, patients with fibromyalgia often experience low mood or anxiety, and when full diagnostic criteria for depression are present, that diagnosis is added in addition to fibromyalgia.
- Importantly, many patients have one region that hurts far more than others — which often represents a dominant pain generator such as low back pain, neck pain, interstitial cystitis/bladder pain syndrome, intercostal neuralgia, occipital headache, sciatica, and others.
Diagnosis
Fibromyalgia is diagnosed clinically — there is no single laboratory test or imaging study that confirms it. Doctors use the Widespread Pain Index (WPI) and the Symptom Severity (SS) Scale to evaluate how many body regions are painful and how intense the accompanying symptoms are. The WPI covers up to 19 possible painful areas that patients report themselves, and physicians usually ask about each of these regions to ensure that none are missed. This modern approach replaced the older method that required tenderness on 11 of 18 specific pressure points during examination. The SS Scale rates fatigue, sleep problems, and cognitive symptoms from 0 to 3 each.
A diagnosis of fibromyalgia is usually made when pain is present in at least four of five body regions (left upper, right upper, left lower, right lower, and axial), symptoms have lasted for three months or longer, and no other disorder better explains the pain pattern. Laboratory tests and imaging are performed mainly to exclude other causes such as thyroid disease, autoimmune inflammation, neuropathies, or vitamin deficiencies.
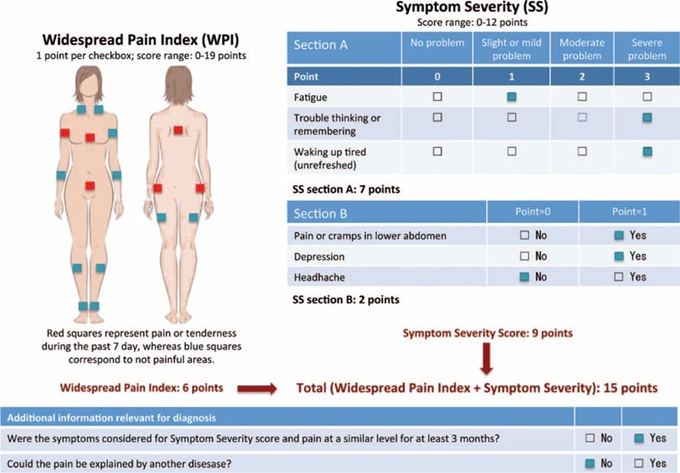
Diagram showing Widespread Pain Index (WPI) body map and Symptom Severity (SS) Scale used in the diagnosis of fibromyalgia.
General Treatment
Effective pain management depends not only on reducing peripheral irritation or central sensitization, but also on preserving the body’s natural pain-control systems — the descending neuromodulation pathways.
Just as antibiotics work best when the immune system is at least partly preserved, pain treatments are most effective when the brain’s natural inhibitory mechanisms are still functional and can be strengthened through rehabilitation, movement, and proper sleep.
The most effective strategy is multimodal therapy combining education, lifestyle modification, and specific symptom management:
- Patient education and reassurance — the pain is real, not psychological.
- Regular, low-impact exercise such as walking, swimming, or stretching.
- Sleep regulation and stress management — cognitive-behavioral therapy, relaxation techniques, mindfulness.
- Medications (when indicated): Medications that can help reduce pain and improve sleep include duloxetine (Cymbalta), pregabalin (Lyrica), or low-dose amitriptyline (Elavil). These are prescribed individually based on symptom profile, coexisting conditions, and tolerance.
- Physical therapy: gentle strengthening, stretching, and postural correction.
These measures reduce central sensitization, but in many patients they do not fully resolve the pain because the local pain sources remain untreated.
When dominant local pain syndromes are recognized and treated alongside general measures, most patients achieve better pain control and quality of life.
Local Pain Sources in Patients with Fibromyalgia
Although fibromyalgia is defined as “widespread pain,” it rarely feels equal in every region.
Most patients can point to one or two areas that constantly hurt more than the rest — for example, the neck, shoulders, low back, pelvic floor, or chest wall.
These regions often behave like classic localized pain syndromes involving the same mechanisms seen in other chronic pain conditions:
- Muscle spasm or myofascial trigger points leading to sustained local tenderness and referred pain, especially when they compress nearby sensory nerves.
- Low-grade inflammation in muscles, tendons, joints, or fascia that irritates sensory nerve endings or adjacent nerve branches.
- Nerve irritation or compression causing pain and, over time, structural or functional changes in the nerve that lead to neuropathic pain and heightened sensitivity.
- Fibrotic or degenerative changes in connective tissue — such as fascial thickening, peri-tendinous fibrosis, or tiny adhesions between tissue layers — can limit normal sliding and flexibility of muscles and fascia, creating constant mechanical tension that maintains local inflammation or compresses nearby nerves.
- Joint or ligament micro-instability — often resulting from loose connective tissue, repetitive strain, or poor posture — can cause abnormal traction on joint nerves, leading to reflex muscle spasm and persistent pain in surrounding structures.
- Microcirculatory and metabolic disturbances reducing oxygen supply and promoting muscle fatigue and stiffness, often amplifying the above mechanisms.
Although central sensitization is a key mechanism in fibromyalgia, peripheral nociceptive and somatic factors often contribute as well, creating a complex interaction between local and central pain processes.
How the Dominant Pain Source Is Identified in Fibromyalgia
In fibromyalgia, local pain syndrome almost never arises from a single source. Instead, several mechanisms usually overlap — including muscle tension, connective-tissue irritation, nerve hypersensitivity, and central sensitization.
The goal of evaluation is not to “find one cause,” but to determine how much each component contributes in every painful region.
1. Detailed pain history
The process starts with precise mapping of all pain areas — their onset, duration, daily fluctuation, and aggravating or relieving factors. Patients are asked about posture, repetitive activity, sleep quality, and stress triggers that may influence pain intensity.
2. Focused physical examination
Palpation identifies tense or shortened muscles, local trigger points, or zones of neuropathic sensitivity. Passive and active motion tests help reveal whether pain originates mainly from muscles, joints, or nerve structures.
3. Targeted diagnostic tests
If localized pathology is suspected, ultrasound or MRI may confirm inflammation, tendon overload, or nerve compression. Laboratory testing is used selectively to exclude systemic or rheumatologic diseases that may mimic fibromyalgia.
4. Diagnostic (test) injections when indicated
Small test injections with lidocaine — usually guided by ultrasound — can help confirm the exact pain generator, such as a peripheral nerve branch or a deep myofascial trigger zone.
5. Mechanism-based interpretation
Each painful region is analyzed to estimate the relative contribution of myofascial tension, inflammatory or overuse processes, and neuropathic or compressive mechanisms — because in most patients, several of these components coexist.
Recognizing this pattern allows therapy to target both local and central mechanisms, improving pain control and functional recovery.
Treatment prioritization: begin with the most limiting or constant pain area; combining local and general therapy gives best results.
Treatment Approach for Dominant Pain Source in Fibromyalgia
General fibromyalgia care — including sleep optimization, stress reduction, and aerobic conditioning — remains essential.
However, the missing step for many patients is the targeted treatment of the dominant local pain generators.
If Muscle Spasm or Myofascial Pain Dominates
- Daily stretching and breathing-based relaxation.
- Myofascial release, gentle manual therapy, or dry needling.
- Local heat therapy or short sessions of low-intensity exercise.
- Short-term muscle relaxants are sometimes prescribed for fibromyalgia at night if severe sleep-related spasm is present.
If Local Inflammation or Overuse Is Present
- Postural correction and ergonomic adjustments.
- Controlled movement: slow, eccentric muscle work and core stabilization.
- NSAIDs, topical anti-inflammatory gels, or brief courses of non-opioid analgesics.
- Ultrasound-guided injections when conservative measures fail.
If Neural Irritation or Compression Exists
- Nerve-gliding and decompression-focused stretching.
- Adjust posture and workspace to minimize neural tension.
- Consider neuropathic-pain medications if symptoms persist.
- Diagnostic or therapeutic nerve block may be used to confirm the mechanism.
The care involves both general pain-management principles for fibromyalgia and local treatment methods for specific pain syndromes such as low back pain, neck pain, interstitial cystitis / bladder pain syndrome, intercostal neuralgia, occipital headache, sciatica, and others.
Why an Online Consultation Can Help When Fibromyalgia Pain Persists in One Dominant Region
A video consultation for fibromyalgia with dominant regional pain can help identify the exact source of your most disabling pain — one or more dominant pain generators — as well as the factors that trigger and maintain it. Fibromyalgia can increase overall pain sensitivity, but it does not automatically explain every severe local pain, such as low back pain, neck pain, pelvic pain, chest wall or rib pain, headache, facial pain, sciatica-like pain, or joint-region pain. This is achieved through a detailed conversation and review of your medical records, previous treatments, imaging, and laboratory tests when available. During the session, you are instructed to perform specific posture, movement, regional pressure, nerve-sensitivity, or muscle-provocation tests to see what increases, reduces, or changes your pain. This helps identify which dominant pain source is active. Many of these pain generators and sustaining factors cannot be seen on MRI or routine laboratory tests.
This may sound like examinations you have already had. It is not — because what matters most is not the test itself, but who interprets it. Only a specialist with deep knowledge of pain anatomy and fibromyalgia-related sensitization knows which questions to ask, which painful region to analyze first, where to instruct you to press, which movements to test, and how to distinguish systemic pain sensitivity from a treatable local pain generator. This is not just another opinion.
You will also receive advice on which additional factors that trigger and sustain pain should be investigated — such as sleep disturbance, stress-related nervous system reactivity, vitamin deficiencies, side effects of other medications, inadequate diet, metabolic factors, physical inactivity, repetitive strain during daily activities or work, muscle spasm, local inflammation, nerve irritation, and other overlooked contributors. In many patients who have already visited several specialists, these factors have still not been fully investigated.
Once the dominant pain mechanism behind fibromyalgia-related symptoms is identified, treatment follows: general fibromyalgia care to reduce central sensitization and targeted treatment of the dominant local pain source, carefully introduced and adjusted over several weeks, with regular communication during the treatment period, especially when you need it. The aim is to reduce the dominant pain source first, then stabilize the result so that overall fibromyalgia-related sensitivity can also decrease. When selecting or adjusting medications, we take into account whether patients are older, sensitive to side effects, or have other health conditions, and we use a safe combination for the shortest necessary duration to avoid medication overload. All recommendations are explained during the conversation and are also given in a written medical report.
Many patients assume that because fibromyalgia treatment has only partially helped, nothing else can be done. In many cases, this is not true — previous treatment may have reduced general pain sensitivity, but did not identify or treat the dominant local pain generator that continues to drive symptoms. In the minority of patients where medication and conservative treatment are not sufficient, we recommend the exact intervention or procedure — chosen based on the confirmed pain generator, not assumptions.
Based on our written medical report, reimbursement may often be possible if your insurance plan allows it.
Fibromyalgia Pain — Local and General
If you have fibromyalgia with one or several regions that hurt the most (neck, back, pelvis, chest, etc.), you likely need care on two levels: general fibromyalgia management and targeted treatment of dominant local pain sources. A detailed telehealth consultation helps identify the key pain generator and create a personalized, mechanism-based plan.
- ✔ Send a short message describing your main pain area and previous treatments
- ✔ Get a reply within 24 h on whether and how we can help, fee, and timing
- ✔ Send your scans and reports only if requested
- ✔ Receive a written report and follow-up Q&A (within 10 days)
- ✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Typical fee: $180 – 250 (according to case complexity)
Many patients improve once the dominant regional pain syndrome is identified and treated alongside overall fibromyalgia care.
Note: Telehealth is not a substitute for urgent in-person care. Seek emergency help for new neurological deficits, fever, chest pain, or rapid worsening.
Before contacting us, please read our Privacy Policy and Terms of Use.
Online pain consultation for regional pain in detail
Schematic explanation of the video consultation for regional pain
Answers to questions about the process and success of video consultations for regional pain
There are several common reasons for poor therapeutic outcomes in the treatment of chronic pain, which are often seen in patients with regional pain.
Artificial intelligence can also support the process by analyzing complex pain syndromes in fibromyalgia, but clinical expertise remains essential.
Why This Approach Works
Treating the dominant local pain source reduces the constant nociceptive input that fuels central sensitization.
As peripheral pain subsides, overall fibromyalgia pain often decreases as well — patients sleep better, move more easily, and need fewer medications.
In clinical studies (Affaitati 2011, Gerwin 2013, Staud 2011), this combined local + central approach consistently improves global pain ratings and function.
Why Pain Often Persists Despite Fibromyalgia Treatment
Pain often persists despite fibromyalgia treatment because treatment reduces central sensitization but does not always identify and treat the dominant local pain generator, such as low back pain, neck pain, pelvic pain, headache, chest wall pain, or nerve-related pain.
In many patients, pain does not persist because fibromyalgia treatment is incorrect, but because it remains incomplete — focused mainly on central sensitization while local pain sources are not fully identified or treated.
First, the dominant local pain generator is not clearly defined. Although fibromyalgia is characterized by widespread pain, most patients have one or a few regions that hurt significantly more than others. These areas often represent specific pain syndromes — such as muscle spasm, tendon irritation, or nerve involvement — which require targeted treatment but are frequently attributed only to “fibromyalgia.”
Second, the underlying pathological process within these local pain areas is not distinguished. Muscle tension, low-grade inflammation, mechanical overload, and nerve sensitization each require different therapeutic approaches, yet treatment is often applied without identifying which mechanism predominates in a given region.
Third, contributing factors that maintain local and central pain are frequently underestimated. These include posture, repetitive strain, poor sleep, autonomic imbalance, and metabolic or nutritional influences. Even when general fibromyalgia therapy is appropriate, these factors can continue to amplify pain signals and limit recovery.
Because of this, treatment may appear appropriate and partially helpful, yet pain remains, fluctuates, or returns — especially in the same dominant regions. More complete improvement is usually achieved only when both central sensitization and local pain generators are addressed together in a coordinated, mechanism-based approach.
Prognosis and Long-Term Management
Fibromyalgia itself does not cause tissue damage or paralysis.
Pain intensity fluctuates, but the long-term outlook is favorable when patients adopt self-management strategies and local sources of pain are treated as they arise.
Periodic reassessment prevents chronic flare-ups from becoming entrenched.
The goal is not “pain-free forever,” but a stable, active life with manageable symptoms.
FAQ About Pain in Fibromyalgia
Why does pain persist despite standard fibromyalgia treatment?
Pain in fibromyalgia often persists because treatment may reduce general pain sensitivity but still miss the dominant local pain generator. Fibromyalgia can make the nervous system more sensitive, but a patient may also have a specific painful source in the low back, neck, knee, pelvis, chest wall, or along a nerve. If that local source continues sending pain signals, the whole pain system remains irritated. In practice, improvement is often better when systemic fibromyalgia care is combined with identification and targeted treatment of the most painful local region.
Can fibromyalgia cause one body region to hurt much more than the rest?
Yes. Although fibromyalgia is defined as widespread pain, many patients have one region that clearly dominates the clinical picture. This may be the low back, neck, shoulder, knee, chest wall, pelvis, face, or one limb. Sometimes this is simply the area where fibromyalgia sensitivity is most noticeable. However, it can also mean that a separate local pain generator exists in that region. The important point is not to assume that every dominant pain is “only fibromyalgia.” The painful region should be analyzed as a possible local syndrome.
Is the most disabling pain always caused only by fibromyalgia?
No. Fibromyalgia can increase overall pain sensitivity, but it does not automatically explain every local pain. A patient may have fibromyalgia and still have a separate pain source such as a facet joint, sacroiliac joint, irritated tendon, bursa, muscle-fascial trigger point, peripheral nerve entrapment, intercostal neuralgia, occipital neuralgia, or spine-related pain. This is why the most disabling pain should be evaluated separately. If a treatable local generator is found, targeted treatment may reduce both the local pain and the overall fibromyalgia burden.
What is a dominant local pain generator in fibromyalgia?
A dominant local pain generator is the main structure or mechanism that keeps one painful region active. In fibromyalgia, the nervous system may be globally sensitive, but one area may still have a stronger local source of pain. Examples include a lumbar facet joint in low back pain, cervical muscle or joint pain in neck pain, an irritated occipital nerve in headache, a tendon or bursa in joint-region pain, or a peripheral nerve in neuralgia. Identifying this generator helps decide whether treatment should target the local structure, systemic sensitivity, or both.
Can MRI or laboratory tests be normal while a treatable local pain source still exists?
Yes. Many local pain generators in fibromyalgia are functional, inflammatory, mechanical, or nerve-related and may not be clearly visible on routine MRI or blood tests. Muscle-fascial pain, small nerve irritation, tendon overload, bursitis, sacroiliac pain, facet pain, and some peripheral nerve entrapments may produce severe symptoms even when imaging appears mild or normal. Normal tests are useful because they exclude dangerous conditions, but they do not prove that no treatable local pain source exists. Clinical mapping, examination, ultrasound assessment, and diagnostic blocks may be needed.
How is the dominant local pain source identified in fibromyalgia?
The dominant local pain source is identified by combining the patient’s history, pain map, physical examination, imaging correlation, and sometimes diagnostic injections. The first step is to define where the pain is strongest, what triggers it, what relieves it, and whether it follows a joint, muscle, nerve, or spine-related pattern. Examination then tests movement, palpation, neurological signs, and local tenderness. Imaging is interpreted only in relation to symptoms. If uncertainty remains, a small ultrasound-guided diagnostic block may help confirm whether a suspected structure is truly producing the pain.
Can treating one dominant local pain source reduce overall fibromyalgia pain?
Yes, in some patients. A dominant local pain source can continuously irritate the nervous system and increase central sensitization. When that local input is reduced, the whole pain system may become less reactive. This does not mean that fibromyalgia disappears, but sleep, movement, fatigue, and overall pain tolerance may improve. The effect is usually best when targeted local treatment is combined with general fibromyalgia care such as sleep regulation, graded activity, stress reduction, and appropriate medication. Treating the local generator is one part of a broader mechanism-based plan.
What helps low back pain in patients with fibromyalgia?
Low back pain in fibromyalgia should first be separated from generalized pain sensitivity. The doctor needs to check whether the pain comes from lumbar muscles, facet joints, sacroiliac joints, disc-related irritation, nerve roots, or myofascial trigger points. Treatment may include gentle graded movement, posture and load correction, sleep improvement, medication for central sensitivity, and targeted local treatment if a specific generator is found. In some cases, ultrasound-guided or fluoroscopy-guided diagnostic blocks help clarify the source. The goal is not only to treat fibromyalgia, but also the local low back mechanism.
Can low back pain in fibromyalgia come from a disc, facet joint, sacroiliac joint, or nerve irritation?
Yes. A patient with fibromyalgia can still have ordinary low back pain generators, including disc-related pain, facet joint pain, sacroiliac joint pain, lumbar radiculopathy, muscle-fascial pain, or peripheral nerve irritation. Fibromyalgia may amplify the pain, but it does not exclude these local causes. MRI findings must be interpreted carefully because disc bulges or degenerative changes may be incidental, while a painful joint or nerve may be less obvious. The key is to match symptoms, examination, imaging, and response to targeted diagnostic treatment.
What helps neck pain in patients with fibromyalgia?
Neck pain in fibromyalgia often improves only when both systemic sensitivity and local cervical pain sources are addressed. Local sources may include cervical facet joints, muscle spasm, myofascial trigger points, disc irritation, posture-related overload, or nerve-root irritation. Treatment may include gentle mobility work, sleep and pillow adjustment, targeted physical therapy, medication that reduces pain sensitivity, and local treatment when a specific generator is identified. If neck pain is dominant, persistent, or radiates toward the head, shoulder, or arm, it should not be dismissed as only fibromyalgia.
Can neck pain in fibromyalgia come from cervical joints, discs, muscles, or nerve roots?
Yes. Fibromyalgia may coexist with cervical joint pain, disc-related irritation, muscle-fascial pain, occipital nerve irritation, or cervical radiculopathy. The symptoms can overlap: pain may spread to the shoulder, upper back, scalp, arm, or hand. MRI may show degenerative changes, but the visible finding is not always the true pain generator. A focused examination helps determine whether pain is mechanical, myofascial, nerve-related, or part of generalized sensitivity. This distinction matters because treatment for cervical joint or nerve pain differs from general fibromyalgia treatment.
What helps knee pain in patients with fibromyalgia?
Knee pain in fibromyalgia should be evaluated as a local pain problem, not only as part of widespread pain. The source may be the knee joint, meniscus, cartilage, patellar tendon, quadriceps tendon, pes anserine region, fat pad, bursa, nerve irritation, hip referral, or lumbar referral. Treatment depends on which generator is active. Exercise and systemic fibromyalgia care may reduce sensitivity, but persistent knee-dominant pain may require local examination, ultrasound assessment, imaging correlation, or diagnostic blocks. This is especially important before repeated injections or surgery are considered.
Can knee pain in fibromyalgia come from the joint, tendons, bursae, nerves, or referred pain?
Yes. Knee pain in a patient with fibromyalgia can come from several local or referred sources. Pain may arise from arthritis or meniscus pathology inside the knee, but also from tendons, bursae, pes anserine irritation, patellar tracking overload, peripheral nerves, hip disorders, or lumbar spine referral. Fibromyalgia may increase pain intensity, making a mild local problem feel severe. The important question is whether the knee finding truly matches the pain pattern. If not, treating only the visible MRI or X-ray change may not solve the dominant pain problem.
Can headache or occipital pain in fibromyalgia come from cervical structures or occipital nerves?
Yes. Headache in fibromyalgia may be part of generalized pain sensitivity, but occipital or back-of-head pain can also come from cervical muscles, cervical facet joints, upper cervical nerves, or occipital neuralgia. This type of pain may spread toward the scalp, temple, or behind the eye and can be worsened by neck position, pressure at the back of the head, or prolonged posture. If headache has a clear local pattern, it should be evaluated separately. Targeted treatment of cervical or occipital generators may reduce the headache burden.
Can facial pain in fibromyalgia come from trigeminal, dental, TMJ, viral, or peripheral nerve causes?
Yes. Facial pain in fibromyalgia should not automatically be attributed to fibromyalgia alone. It may come from trigeminal neuralgia, atypical facial pain, dental problems, TMJ dysfunction, post-viral nerve irritation, peripheral nerve injury, muscle-fascial pain, or central sensitization. These mechanisms require different treatment logic. The key is to analyze the pain pattern: electric shocks, burning, aching, chewing-related pain, touch sensitivity, dental triggers, or post-infection onset can point to different causes. Fibromyalgia can amplify facial pain, but the local mechanism still needs to be identified.
Can pelvic or bladder pain in fibromyalgia need separate evaluation?
Yes. Pelvic or bladder pain can coexist with fibromyalgia and still require separate evaluation. Possible mechanisms include pelvic floor muscle spasm, pudendal nerve irritation, bladder pain syndrome, interstitial cystitis, sacroiliac pain, lumbar referral, gynecological or urological causes, and central sensitization. Fibromyalgia may make pelvic pain more intense and persistent, but it does not replace a local diagnosis. If pelvic pain dominates, treatment should clarify whether the main generator is muscular, nerve-related, bladder-related, spinal, or mixed. This helps avoid repeated ineffective treatment aimed at the wrong mechanism.
Can chest wall or rib pain in fibromyalgia come from intercostal neuralgia or local muscle pain?
Yes. Chest wall or rib pain in fibromyalgia may be related to generalized tenderness, but it can also come from intercostal neuralgia, costochondral irritation, thoracic spine referral, myofascial trigger points, or local nerve irritation. Because chest pain can sometimes reflect heart, lung, or abdominal disease, urgent causes must be excluded first when symptoms are new, severe, or associated with shortness of breath, sweating, fainting, or fever. Once dangerous causes are excluded, a local pain-generator analysis can help identify whether the pain is muscular, nerve-related, joint-related, or mixed.
Can fibromyalgia mimic sciatica or nerve pain in the leg?
Fibromyalgia can produce widespread aching, burning, tingling, and sensitivity that may resemble nerve pain. However, true sciatica or lumbar radiculopathy can also occur in a patient with fibromyalgia. The difference is important. Sciatica usually follows a nerve-root pattern and may be associated with back pain, leg radiation, numbness, weakness, or reflex changes. Fibromyalgia-related leg pain is often more diffuse and variable. A focused neurological examination and careful MRI correlation help decide whether the leg pain is generalized sensitivity, local nerve irritation, lumbar radiculopathy, or a mixed condition.
When are diagnostic injections or nerve blocks useful in fibromyalgia with dominant local pain?
Diagnostic injections or nerve blocks may be useful when a patient with fibromyalgia has one dominant pain region and examination suggests a specific local generator. A small amount of local anesthetic can temporarily silence a suspected nerve, joint, bursa, tendon sheath, trigger point, or sacroiliac/facet region. If the patient’s typical pain improves during the expected anesthetic window, the source becomes more likely. These blocks are not used to “prove fibromyalgia.” They are used to identify local pain generators that may be treatable alongside systemic fibromyalgia care.
How should systemic fibromyalgia care and targeted local pain treatment be combined?
Systemic fibromyalgia care and local pain treatment should usually run together, not compete with each other. General care aims to reduce central sensitization through education, sleep improvement, graded activity, stress regulation, and carefully selected medication. Local treatment aims to reduce the strongest ongoing pain input from a specific region, such as the low back, neck, knee, pelvis, chest wall, or nerve pathway. If only systemic sensitivity is treated, the dominant local generator may continue to drive pain. If only the local source is treated, global sensitivity may still maintain symptoms.
Can an online consultation help identify the dominant pain source in fibromyalgia?
An online consultation can often help clarify whether the pain pattern is mainly systemic, local, or mixed. During review, the most painful regions, triggers, previous treatments, imaging, laboratory results, and symptom behavior are analyzed together. Video assessment can guide movement testing, pain mapping, and neurological screening, while reports and scans help check whether findings match symptoms. Online consultation cannot replace urgent in-person care or every physical examination, but it can help decide which local generator is most likely, what documentation is needed, and whether targeted treatment or second opinion is reasonable.
English homepage – overview of neurosurgery and pain consultation
Additional Information for Patients with Fibromyalgia
-
MedlinePlus — Fibromyalgia
Simple explanation of symptoms, diagnosis, and treatment options. -
NHS — Fibromyalgia
Clear, patient-friendly guide: symptoms, daily management, and when to see a doctor. -
NIH/NCCIH — Fibromyalgia (In-Depth)
Evidence summary on helpful approaches such as gentle exercise, relaxation, and acupuncture. -
U.S. Office on Women’s Health — Fibromyalgia
How fibromyalgia affects everyday life and what lifestyle changes can help. -
Arthritis Foundation — Fibromyalgia Fact Sheet (PDF)
Concise overview of key symptoms and treatment approaches for patients.