Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
June 16, 2026
Who This Arachnoid Cyst Page Is For
This page is intended for patients who have been diagnosed with an arachnoid cyst on MRI or CT scan, as well as for family members seeking a clear, structured explanation of what the finding truly means.
Many people discover an arachnoid cyst incidentally while being evaluated for headaches, seizures, dizziness, or unrelated problems. You are not expected to read this page from start to finish. Instead, you may return to specific sections when new questions arise — for example, if follow-up imaging shows growth, symptoms change, or surgery is suggested.
If medical opinions differ, surgery has been proposed without clear explanation, seizures are difficult to interpret, or you are unsure whether the cyst is truly responsible for symptoms, an individualized neurosurgical second opinion can help clarify whether monitoring or intervention is the most appropriate next step.
When patients seek a second opinion for an arachnoid cyst
• Surgery has been recommended, but it is unclear whether it is truly necessary
• Different doctors provide conflicting advice (monitoring vs. operation)
• Seizures are present and it is uncertain whether the cyst is the real cause
• Follow-up MRI suggests cyst growth or increasing mass effect
• Hydrocephalus, midline shift, or neurological symptoms are mentioned without clear explanation
• There is uncertainty about the safest surgical option (endoscopic fenestration, open surgery, or cystoperitoneal shunt)
In most cases, arachnoid cysts do not require surgery — but in selected situations, careful evaluation is essential.
If your situation involves uncertainty about indication, timing, or surgical strategy, you may request an individualized neurosurgical review here:
Request Second Opinion
Arachnoid Cyst — Quick Summary (Read This First)
- An arachnoid cyst is a benign, fluid-filled cavity within the arachnoid brain membrane. It is not a tumor and does not become malignant.
- Most arachnoid cysts are congenital. They form during fetal development due to splitting of the arachnoid membrane which covers the brain. They are often discovered incidentally later in life.
- Arachnoid cysts are relatively common. They are found in approximately 1–2% of the population, and the majority remain asymptomatic throughout life.
- Only a minority (estimated 5–20%) become symptomatic, depending on cyst size and location. Most remain asymptomatic throughout life. Symptoms usually occur because of brain compression, progressive enlargement, or disturbance of cerebrospinal fluid (CSF) circulation.
- Not every symptom in a patient with a cyst is caused by the cyst. Careful clinical and radiological correlation is essential before considering surgery, particularly when the only findings are headache or epilepsy without clear evidence of mass effect, hydrocephalus, or progressive neurological deficit.
- MRI is the key diagnostic tool. A typical arachnoid cyst follows the CSF (normal brain fluid) signal on all sequences, shows no contrast enhancement, and contains no solid components.
- Surgery is not automatically required. Indications include progressive neurological deficits, documented growth, hydrocephalus, significant mass effect, or drug-resistant epilepsy clearly linked to the cyst.
- Surgical treatment depends primarily on cyst location and individual anatomy. Endoscopic fenestration is often preferred when the cyst can be safely connected to normal cerebrospinal fluid (CSF) spaces, such as the ventricular system or adjacent cisterns, allowing a minimally invasive internal opening. However, cysts with thick walls, multiloculated compartments, convexity or deep interhemispheric locations, or those lacking a safe adjacent CSF space for communication may require open microsurgical fenestration (craniotomy) to achieve a wider and more controlled opening. Cystoperitoneal shunting is generally reserved for selected cases in which fenestration is not technically feasible, has failed, or when long-term CSF diversion is necessary, particularly in the presence of persistent symptoms or associated hydrocephalus.
- Surgery aims to relieve symptoms rather than remove the cyst completely. In properly selected patients, clinical improvement occurs in most cases (approximately 70–85%), especially when symptoms are clearly caused by mass effect or hydrocephalus. The cyst often remains visible on follow-up imaging and may not significantly decrease in size.
- Long-term prognosis is generally favorable. Most patients live normal lives without intervention, and malignant transformation does not occur.
- This page is structured so you can focus on what applies to your situation. Use the Contents box to jump directly to sections on symptoms, epilepsy, treatment decisions, or follow-up.
Most readers benefit from the Quick Summary plus the sections on Does the Cyst Need Treatment?, When Is Surgery Necessary?, and Relationship Between Arachnoid Cyst and Epilepsy. The remaining sections provide deeper clinical detail.
Contents
- Who this is for
- Quick summary
- Definition
- Congenital origin
- How congenital cysts form
- Secondary cysts
- How common
- Typical locations
- Symptomatic rate
- Why symptoms occur
- Symptoms overview
- Cyst & epilepsy
- Diagnosis
- MRI findings
- CT findings
- Treatment decision
- When surgery needed
- Surgical options
- Endoscopic fenestration
- Open craniotomy
- Cystoperitoneal shunt
- When Specialist Opinion Differ
- Prognosis
- Follow-up
- Key message
- FAQs
- Second opinion
- Further reading
Most arachnoid cysts do not need surgery. The key question is not the size alone, but whether MRI findings match the patient’s symptoms. Surgery is usually considered when there is documented growth, hydrocephalus, progressive neurological deficit, significant mass effect with matching symptoms, or drug-resistant seizures clearly linked to the cyst.
What Is an Arachnoid Cyst?
Arachnoid cyst is a benign, cerebrospinal fluid (CSF)-filled cavity located within the arachnoid membrane, one of the three layers covering the brain and spinal cord.
The brain and spinal cord are protected by three layers called meninges: the tough outer dura mater, the delicate inner pia mater, and the middle arachnoid membrane. An arachnoid cyst occurs when this middle membrane splits or doubles over, forming a „pocket“ that traps cerebrospinal fluid (CSF). CSF is a clear, nutrient-rich liquid that usually flows freely around the brain to provide cushioning. Essentially, the cyst is a localized collection of this natural fluid contained within a duplication of the protective arachnoid tissue.
It is not a tumor.
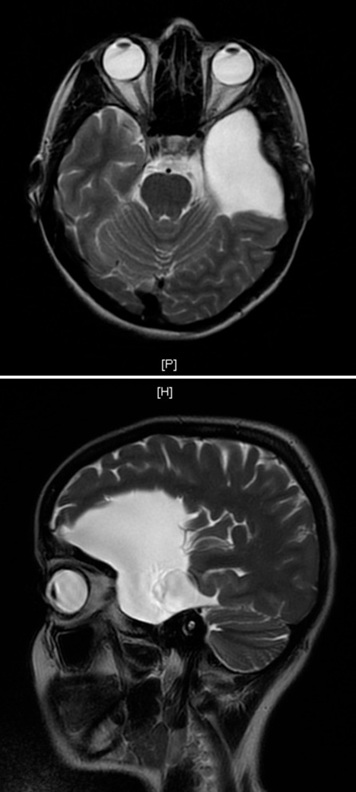
Image: MRI scan (T2-weighted scans) showing an arachnoid cyst in the temporal region (temple area). On this scan, the cyst appears as a bright white area.

Image: Arachnoid cyst CSF-filled cavity located within the arachnoid membrane, one of the three layers covering the brain and spinal cord.
Are Arachnoid Cysts Congenital?
In most cases — yes.
Approximately 80–90% are congenital (primary cysts).
How Do Arachnoid Cysts Form?
Most arachnoid cysts are present from birth (congenital). During early fetal development, the thin middle layer covering the brain (the arachnoid membrane) may not form as a perfectly smooth sheet. Instead, it can split or fold in a small area, creating a pocket. This pocket can trap normal cerebrospinal fluid (CSF) — the clear fluid that cushions and protects the brain. In some cases, fluid can enter this pocket more easily than it can leave, creating a “one-way valve” effect, which may slowly cause the cyst to enlarge over time. When the cyst forms very early in development, it may occupy space before the nearby brain tissue has fully expanded, which is why some larger temporal cysts are associated with mild underdevelopment of the adjacent brain region. Importantly, this reflects a variation in early development rather than brain damage occurring later in life.
Most of these are primary cysts, meaning they are present from birth, and they are usually detected incidentally later in life during scans for unrelated reasons.
Secondary (acquired) cysts
10–20% are acquired and may develop after:
- head trauma
- meningitis
- intracranial hemorrhage
- neurosurgical procedures
How Common Are Arachnoid Cysts?
- Found in 1–2% of the general population
- Most large imaging studies showing a slight male predominance
- Most are discovered incidentally on MRI
Where Are These Cysts Usually Found?
Arachnoid cysts can appear anywhere in the brain or spine, but they tend to favor certain „pockets.“ Here is how their location is typically distributed:
- Middle cranial fossa (temporal region) — 50–60%: This is the most common spot, located near the temples and behind the eyes. It’s the area where the “temporal pole” we mentioned earlier is located.
- Posterior fossa — 10–15%: This is the back of the head, near the base of the skull. This area houses the cerebellum, which controls balance and coordination.
- Suprasellar region — 5–10%: Located deep in the center of the brain, just above the area where the optic nerves cross and near the pituitary gland (the “master gland” for hormones).
- Convexity or interhemispheric — 5–10%: These are found on the top or outer surface of the brain, or in the deep groove that separates the left and right halves of the brain.
- Spinal — less common: These occur along the spinal cord rather than in the brain.
How Many Become Symptomatic?
Only 5–20% of arachnoid cysts become symptomatic. However, only a minority of symptomatic cases ultimately require surgical treatment.
The majority (≈80–95%) remain asymptomatic throughout life.
Why Do Symptoms Occur? (Pathophysiological Mechanisms)
Symptoms are not caused by the cyst “being there” — but by its mass effect or CSF dynamics disturbance.
While many cysts remain small and quiet, they can sometimes cause issues through these main mechanisms:
- Expansion (The Valve Effect): Fluid enters but cannot exit, causing the cyst to grow and increase local pressure.
- Compression: The cyst physically pushes against brain tissue, potentially disrupting the functions controlled by that specific area.
- CSF blockage: distorting the natural flow of brain fluid and potentially causing pressure buildup.
- Intracranial pressure: Large cysts can increase overall pressure inside the skull, leading to chronic headaches or nausea.
- Seizure trigger: In selected cases, a cyst located adjacent to the cerebral cortex may contribute to abnormal electrical activity. This is more likely when there is cortical thinning or structural distortion near the cyst.
Importantly:
Many cysts are stable and never enlarge.
Symptoms of Arachnoid Cyst
Symptoms depend entirely on location.
Common symptoms:
- Headache (most frequent)
- Seizures
- Focal neurological deficit may include limb weakness, coordination problems (ataxia), visual disturbances such as blurred or double vision, facial numbness, speech difficulties, or balance impairment. These symptoms occur when the cyst compresses specific functional areas of the brain.
- Balance disturbance (posterior fossa)
- Visual disturbances (suprasellar)
- Cognitive or behavioral changes (large temporal cysts)
- Hydrocephalus (rare but possible)
In children:
- Macrocephaly
- Developmental delay
- Irritability
Relationship Between Arachnoid Cyst and Epilepsy
This is one of the most misunderstood aspects.
Important principle:
Not every seizure in a patient with an arachnoid cyst is caused by the cyst.
Cysts may be:
- Incidental finding in epileptic patients
- True epileptogenic focus (rare but possible)
When is epilepsy likely cyst-related?
- Large temporal cyst
- Cortical thinning adjacent to cyst
- EEG abnormality localized to the cyst region (an electroencephalogram showing focal electrical dysfunction or „short circuits“ in the brain tissue immediately adjacent to the cyst).
- No other structural lesion on MRI
Even then, surgery does not guarantee seizure freedom.
Diagnosis
MRI: The Gold Standard
To confirm an arachnoid cyst, radiologists look for these four specific signs on your MRI:
- Matches brain fluid: The cyst looks identical to your normal brain fluid (CSF) on all types of scans.
- No contrast „glow“: It does not absorb contrast dye (no enhancement), which helps rule out tumors.
- Purely liquid: It is a hollow pocket of fluid with no solid or fleshy parts inside.
- Free movement: The fluid inside moves freely (no diffusion restriction), which distinguishes it from other types of cysts.
What a CT Scan Shows
A CT scan is often the first step in finding a cyst. Doctors look for:
- Dark pocket: The cyst appears as a dark area because fluid is less dense than brain tissue.
- Bone remodeling: In long-standing cases, the cyst can gently „reshape“ or thin the nearby skull bone. This is a sign the cyst has been there for a very long time.
- Mass effect: This is a term for the cyst „pushing“ or displacing the surrounding brain tissue due to its size.
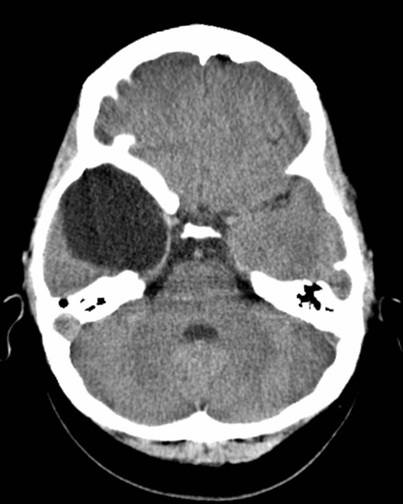
Image: CT scan of the brain showing a right temporal arachnoid cyst.
Is an Arachnoid Cyst a Cause of Symptoms?
Finding a cyst on an MRI doesn’t always mean it is the cause of your symptoms.
Doctors use the following criteria to determine whether the cyst is truly responsible for the symptoms:
- Size vs. symptoms: A large cyst might cause zero issues, while a small one in a sensitive spot might be troublesome. Doctors check if your symptoms actually match the cyst’s size. Many middle cranial fossa (temporal) cysts smaller than approximately 2–2.5 cm remain asymptomatic, but clinical relevance depends more on mass effect and anatomical relationships than on absolute size.
- Location–symptom correlation: Doctors assess whether the cyst’s anatomical location matches the neurological findings. For example, a cyst near visual pathways should explain visual symptoms, while a posterior fossa cyst may correlate with balance or coordination problems. If the symptoms do not anatomically correspond to the cyst’s position, it is less likely to be the true cause.
- Anatomical change: Doctors look at how much the cyst is „pushing“ the brain or shifting its midline. If the brain looks comfortable despite the cyst, it is usually left alone.
- Fluid build-up (hydrocephalus): It is important to see if the cyst is blocking the brain’s drainage system. If it’s causing fluid to back up, it’s more likely to need attention.
- EEG testing: For patients with seizures, an EEG helps confirm if the electrical „short circuit“ is actually coming from the cyst area or somewhere else.
- Watching over time: Often, the best move is to do nothing and simply repeat the scan in 6–12 months to ensure the cyst isn’t growing.
Important note: Only after careful clinical and radiological correlation can a cyst reasonably be considered responsible for symptoms — and even then, surgery is not always necessary.
When is Surgery Necessary?
Surgery is not the default choice for most cysts. It is typically only considered in these specific situations:
- Worsening symptoms: If there is a clear „neurological deficit“—such as new weakness, balance issues, or loss of certain functions.
- Significant pressure: When the cyst is visibly pushing the brain out of its normal position (mass effect) and causing matching symptoms. Importantly, the clinical meaning of midline shift in arachnoid cysts is not the same as in acute hemorrhage or trauma. A few millimeters of chronic shift may be well tolerated, whereas similar numbers in an acute condition can be dangerous. Surgical decisions are therefore based on symptoms and progression — not on millimeter measurements alone.
- Documented growth: If follow-up scans show the cyst is actually getting larger over time.
- Fluid back-up (hydrocephalus): If the cyst blocks the brain’s drainage system, causing dangerous pressure build-up.
- Special cases of epilepsy: Only when seizures cannot be controlled by medication and tests prove the cyst is the exact trigger.
Arachnoid Cyst and Headaches
Headache is the most commonly reported symptom in symptomatic arachnoid cysts, occurring in roughly 50–70% of cases. Having a headache alone is usually not a reason for surgery. Headaches are very common and often have causes unrelated to the cyst. Conditions such as migraine, tension-type headache, or occipital neuralgia are far more frequent explanations. A headache needs a standard headache evaluation regardless of the cyst. Unless the headache is clearly linked to increased intracranial pressure, progressive mass effect, or documented cyst enlargement, surgery is unlikely to resolve it. Ideally, this assessment is performed by a neurosurgeon familiar with both primary headache disorders and the surgical decision-making process for arachnoid cysts.
Types of Surgical Treatment
There is no single “best” operation for all arachnoid cysts.
The choice of surgical technique depends primarily on cyst location, anatomical relationships, and the presence of symptoms such as mass effect or hydrocephalus. Endoscopic fenestration is generally preferred when the cyst can be safely connected to normal cerebrospinal fluid spaces through a minimally invasive approach. Open microsurgical fenestration (craniotomy) is considered when the cyst has complex anatomy, thick walls, internal compartments, or lacks a safe nearby fluid space for endoscopic communication. Cystoperitoneal shunting is usually reserved for selected cases in which fenestration is not feasible, has failed, or when long-term cerebrospinal fluid diversion is required. The decision is individualized and based on detailed imaging analysis.
Endoscopic Fenestration: The Preferred Method in Many Cases
When it works best:
Endoscopic fenestration is most effective when the cyst is located near natural cerebrospinal fluid (CSF) spaces that allow safe internal drainage. It is commonly used for many middle cranial fossa (temporal region) cysts, as well as selected suprasellar and intraventricular cysts where a clear pathway to the ventricles or basal cisterns can be created.
When it may not be suitable:
This technique is less appropriate for cysts with thick walls, internal partitions (multiloculated cysts), or those located in areas where there is no safe adjacent CSF space to connect them to. Some convexity cysts, deep interhemispheric cysts, or anatomically complex posterior fossa cysts may require a different surgical strategy. Most commonly, these cases are treated with open microsurgical fenestration via craniotomy, which allows a wider and more controlled opening of the cyst wall, and in selected situations partial wall excision. If fenestration is not feasible or symptoms recur, cystoperitoneal shunting may be considered.
The procedure of endoscopic fenestration: Think of this as „opening a window.“ During an endoscopic fenestration, the surgeon makes a small opening in the skull and inserts a tiny camera (endoscope). They then create a small hole in the wall of the cyst, allowing the trapped fluid to finally flow out and rejoin the brain’s natural circulation system.
Why It Is Often the Best Choice:
- Minimally invasive: It is performed through a small keyhole opening rather than a large incision.
- Lower risk: Because it doesn’t involve leaving a permanent foreign object (like a tube) in the body, it has a lower long-term complication rate.
- Shorter recovery: Patients typically spend less time in the hospital and return to their daily lives much faster.
- Common first-line option for some locations: In many middle cranial fossa (temporal) cysts, as well as selected suprasellar and quadrigeminal cysts, endoscopic fenestration is often considered the preferred initial surgical approach when safe anatomical access is possible.

Image: Endoscopic fenestration of a suprasellar arachnoid cyst. The endoscope is shown navigating through the brain’s ventricles to reach the cyst at the skull base. A small opening is made in the cyst wall, allowing cerebrospinal fluid (CSF) to flow into the natural brain cisterns.
Open Craniotomy and Fenestration
The Procedure: Unlike the minimally invasive endoscopic approach, this is a traditional „open“ surgery. The surgeon removes a small piece of the skull (a bone flap in craniotomy) to gain direct access to the cyst. Under a high-powered microscope, they carefully open the cyst walls to create a permanent drainage path into the brain’s natural fluid spaces. At the end of the procedure, the bone flap is replaced and the incision is closed.
Key Characteristics:
- Direct visualization: It provides the surgeon with the most detailed, 3D view of the cyst and surrounding blood vessels and nerves.
- For complex anatomy: This method is often chosen when the cyst has thick walls or internal partitions (multiloculated structure), or when it is located in anatomically challenging regions such as the posterior fossa (the area at the back of the brain), the deep interhemispheric region (between the two brain hemispheres), or along the brain’s outer surface (convexity), where safe endoscopic access or durable communication with cerebrospinal fluid spaces may not be feasible.
- Higher surgical burden: Because it is a more significant operation, it requires a larger incision and more time in the operating room.
- Effective but Invasive: While highly successful in permanently opening the cyst, it involves a longer recovery period compared to endoscopic methods.

Image: Craniotomy showing the bone flap created to access and treat the cyst. After the procedure, the bone flap is replaced and secured, and the incision is closed.
Cysto-Peritoneal Shunt
The Procedure: This method involves placing a permanent, thin tube (catheter) into the cyst through a tiny hole in the skull. The tube runs under the skin all the way down to the abdomen (peritoneal cavity). A specialized valve is connected to the tube to regulate how much fluid leaves the brain.
Key Characteristics:
- Fluid diversion: Instead of opening the cyst into the brain’s natural spaces, it redirects the fluid to another part of the body.
- The „backup“ plan: It is typically used when fenestration (opening the cyst) has failed or when the cyst’s location makes other surgeries impossible.
- Shunt dependency: A major drawback is that the patient may become „shunt-dependent,“ meaning they rely on the tube for life to manage brain pressure.
- Long-term risks: Because it is a foreign object in the body, there is a lifelong risk of the tube getting blocked (malfunction) or becoming infected.
- Selected cases: Due to these risks, this procedure is usually reserved for specific, difficult cases where other treatments aren’t an option.
Recovery After Arachnoid Cyst Surgery
Recovery after arachnoid cyst surgery depends on the type of operation, cyst location, patient age, symptoms before surgery, and whether there were complications such as hydrocephalus, seizures, or significant mass effect.
Recovery is usually shorter after endoscopic fenestration because the approach is minimally invasive and does not leave a permanent shunt. Open craniotomy and microsurgical fenestration usually require a longer recovery period because the operation involves a larger surgical exposure. Cystoperitoneal shunting has a different recovery pattern because the patient must also be monitored for shunt malfunction, infection, overdrainage, or later revision surgery.
In many uncomplicated cases, patients gradually return to light daily activities over several weeks, but return to work, sports, driving, and full activity must be individualized. Patients with seizures may need separate epilepsy-related restrictions.
Successful recovery does not always mean that the arachnoid cyst disappears on MRI. Symptoms may improve even when a residual cyst cavity remains visible, as long as cerebrospinal fluid communication has improved and mass effect or hydrocephalus has been relieved.
Prognosis of the Surgical Treatment
Surgical treatment is primarily aimed at relieving symptoms rather than removing the cyst completely. In carefully selected patients — particularly when symptoms are clearly related to mass effect or hydrocephalus — clinical improvement is reported in the majority of cases, most commonly in the range of approximately 70–85%. However, the cyst itself often remains visible on follow-up MRI and may not significantly decrease in size. A stable cyst on imaging does not mean that the surgery was unsuccessful, as long as adequate communication with normal cerebrospinal fluid pathways has been achieved and symptoms have improved.
Why Do Medical Opinions Differ in Arachnoid Cyst Treatment?
Different medical opinions are common because treatment decisions are not based on a single finding, but on the correlation between symptoms and imaging.
In many patients, the cyst is present, but it is unclear whether it is truly responsible for symptoms or just an incidental finding. This is the main reason why recommendations may differ.
Is the cyst truly responsible for symptoms?
Some specialists link symptoms such as headache or seizures to the cyst. Others consider the cyst incidental unless there is clear anatomical correlation between its location, size, and the patient’s symptoms.
When is surgery actually necessary?
There is no strict rule. Some recommend surgery based on imaging or symptoms, while others reserve it only for clear neurological deficit, growth, hydrocephalus, or strong symptom correlation.
Is epilepsy caused by the cyst?
In selected cases, the cyst may be considered a cause of seizures. However, many specialists require EEG correlation and exclusion of other causes, and even then, surgery does not guarantee seizure control.
Which surgical method is the best option?
Different surgeons may prefer different approaches. The choice depends on location, anatomy, and cyst structure, so both endoscopic and open surgery may be appropriate in different situations.
Should the cyst be monitored or treated?
Most cysts remain stable and do not require treatment. Observation is often recommended unless there is progression, new symptoms, or increasing mass effect.
Request Arachnoid Cyst Neurosurgical Second Opinion — 24-Hour Review (Priority Option Available)
Being told that you have an arachnoid cyst can raise difficult questions:
Is it dangerous? Is it causing my symptoms? Do I need surgery? Should I accept a proposed operation or continue observation?
An independent neurosurgical second opinion can help clarify whether the cyst is truly responsible for symptoms,
whether surgery is indicated, and which treatment option (endoscopic fenestration, open surgery, or shunt) is most appropriate based on MRI findings and clinical presentation.
- ✔ Send a brief message describing your diagnosis, symptoms (headache, seizures, balance issues, visual problems), and what your MRI report states
- ✔ You’ll receive a reply within 24 hours explaining whether we can help with online consultation.
- ✔ Priority cases: if there is documented cyst growth, hydrocephalus, midline shift, worsening neurological symptoms, or urgent surgical recommendation, consultations can often be arranged within a few hours — write PRIORITY in your first message
- ✔ MRI images (DICOM), radiology reports, and EEG findings (if seizures are present) can be reviewed once initial contact is established
- ✔ During the consultation, we explain whether surgery is truly indicated, expected outcomes, risks of fenestration vs shunt, and realistic follow-up strategy — with up to 10 days of follow-up for brief clarification questions
Consultation fees typically range from $180–250, depending on case complexity and imaging findings.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth neurosurgical second opinions.
Prognosis
- Most cysts remain stable and asymptomatic throughout life.
- After successful surgery, symptom improvement occurs in 70–85% when indication was correct.
- Seizure control is variable.
- Malignant transformation does not occur
Follow-Up Strategy
If asymptomatic:
- MRI at 6–12 months after diagnosis
- If stable → longer interval follow-up
- Often no further imaging needed after stability confirmed
If symptomatic or borderline:
- Closer radiological monitoring
- Clinical reassessment
Key Clinical Message
Arachnoid cyst is common, usually benign, and very often incidental.
The most important clinical question is not:
“Is the cyst present?”
But:
“Is the cyst responsible for symptoms?”
Those are two very different things.
It is not uncommon for neurosurgical opinions to differ regarding whether a cyst is truly responsible for symptoms — especially in cases of headache. Differences may also exist in decisions about surgery and the most appropriate surgical technique.
Frequently Asked Questions About Arachnoid Cysts
Is an arachnoid cyst a brain tumor?
No. An arachnoid cyst is not a brain tumor and it does not become cancer. It is a benign, fluid-filled cavity within the arachnoid membrane, one of the protective layers covering the brain and spinal cord. The fluid inside the cyst usually has the same signal as normal cerebrospinal fluid on MRI. A typical arachnoid cyst has no solid tumor component, does not enhance after contrast, and does not show diffusion restriction. This is why MRI is important: it helps confirm that the lesion behaves like a simple CSF-filled cyst rather than a tumor or another cystic abnormality. The main clinical question is therefore not whether the cyst is malignant, but whether it is causing symptoms or is simply an incidental finding.
Are arachnoid cysts dangerous?
Most arachnoid cysts are not dangerous. Many are congenital, remain stable for years, and are discovered incidentally during MRI or CT imaging performed for headaches, dizziness, seizures, trauma, or unrelated problems. In most patients, the cyst does not cause symptoms and does not require surgery. A cyst becomes clinically important when it produces clear mass effect, blocks cerebrospinal fluid circulation, causes hydrocephalus, grows on follow-up imaging, or matches progressive neurological symptoms. Location matters: a cyst near visual pathways, the posterior fossa, or important cortical areas may have different implications from a stable cyst with no pressure effect. The safest approach is not automatic surgery, but careful correlation between symptoms, neurological findings, imaging, and change over time.
Can an arachnoid cyst be found incidentally and not cause symptoms?
Yes. This is very common. Many arachnoid cysts are found incidentally when a brain MRI or CT scan is performed for another reason. A patient may have headaches, seizures, dizziness, or other symptoms, but the cyst may still be unrelated. This distinction is important because treating an incidental cyst will not necessarily improve symptoms caused by migraine, tension-type headache, epilepsy from another source, cervical problems, vestibular disorders, or other neurological conditions. Doctors decide whether the cyst is relevant by comparing its size, location, mass effect, hydrocephalus, EEG findings when seizures are present, neurological examination, and symptom pattern. The presence of a cyst on imaging is only the beginning of the assessment, not the final diagnosis.
Do arachnoid cysts grow over time?
Most arachnoid cysts remain stable over time and do not grow significantly. Many are present from birth and are discovered only later in life. However, a minority may enlarge, especially if fluid enters the cyst more easily than it exits, creating a valve-like mechanism. Growth is clinically important when it is documented on follow-up imaging and is associated with new or worsening symptoms, increasing mass effect, midline shift, hydrocephalus, or neurological deficits. A single MRI cannot always show whether a cyst is stable or changing. That is why follow-up imaging may be recommended after diagnosis, especially when the cyst is large, symptomatic, borderline, or discovered in a child. Stable cysts often require less frequent follow-up.
How do doctors decide whether an arachnoid cyst is really causing symptoms?
Doctors decide whether an arachnoid cyst is causing symptoms by looking for clinical and anatomical correlation. The symptoms should match the cyst’s location and the structures it affects. For example, a posterior fossa cyst may be relevant when balance or coordination symptoms are present, while a suprasellar cyst may be relevant when visual pathways or endocrine structures are affected. A cyst is more likely to be responsible when there is significant mass effect, hydrocephalus, documented growth, midline shift with matching symptoms, or a focal neurological deficit. Headache or seizures alone are not enough to prove causation. The cyst may be incidental unless symptoms, neurological findings, EEG results when relevant, and imaging all point in the same direction.
Can headaches be caused by an arachnoid cyst, or are they often unrelated?
Headaches can occur in patients with arachnoid cysts, but the cyst is not always the cause. Headache is very common in the general population, and migraine, tension-type headache, cervicogenic headache, medication overuse, sinus disease, or occipital neuralgia may explain symptoms better than an incidental cyst. An arachnoid cyst is more likely to be headache-related when there is clear mass effect, progressive enlargement, hydrocephalus, pressure-related symptoms, or a consistent anatomical relationship between the cyst and symptoms. Surgery performed for headache alone is unpredictable unless the cyst is convincingly responsible. A standard headache evaluation is still necessary. The key question is whether the headache pattern suggests increased pressure or local compression, not simply whether a cyst is present.
Can an arachnoid cyst cause seizures?
Yes, an arachnoid cyst can be associated with seizures in selected cases, but not every seizure in a patient with a cyst is caused by the cyst. Arachnoid cysts are often incidental findings in people who have epilepsy for unrelated reasons. The cyst is more likely to be relevant when it is located near the cerebral cortex, especially in the temporal region, and when there is cortical thinning, local brain distortion, no other epileptogenic lesion, and EEG abnormalities that correspond to the cyst region. When clinical, MRI, and EEG correlation is strong, meaningful seizure reduction may occur in selected patients. However, surgery does not guarantee seizure freedom, and epilepsy assessment must be individualized.
Does every arachnoid cyst require surgery?
No. Most arachnoid cysts do not require surgery. Surgery is reserved for selected cases where there is a strong reason to believe that the cyst is causing clinically meaningful problems. Indications may include progressive neurological deficit, documented cyst growth, hydrocephalus, significant mass effect with matching symptoms, or drug-resistant epilepsy clearly linked to the cyst region. Many cysts are stable, asymptomatic, and safely monitored. Headache alone is usually not enough to justify surgery unless there is evidence of raised pressure, progressive mass effect, or another convincing mechanism. The decision should be individualized. The main question is not whether the cyst exists, but whether it is responsible for symptoms and whether surgery is likely to improve them.
Is it safe to wait and monitor an arachnoid cyst without surgery?
Yes, monitoring without surgery is often the standard and safest approach when an arachnoid cyst is stable, asymptomatic, or not clearly responsible for symptoms. Observation is especially reasonable when there is no progressive neurological deficit, no hydrocephalus, no documented growth, and no convincing anatomical match between the cyst and the patient’s symptoms. Follow-up may include neurological assessment and repeat MRI, often after 6–12 months when the cyst is newly discovered or borderline. Spontaneous disappearance is uncommon, but long-term stability is very common. Monitoring becomes less appropriate if symptoms progress, imaging shows growth, mass effect increases, hydrocephalus develops, or seizures are strongly linked to the cyst region. The decision should be individualized rather than based on fear alone.
My doctor recommended surgery for my arachnoid cyst, but I am not sure it is necessary — what should I consider before deciding?
Before accepting surgery for an arachnoid cyst, the key question is whether the cyst is truly responsible for symptoms and whether surgery has a realistic chance of improving them. Important points include: whether symptoms match the cyst location, whether there is documented growth, hydrocephalus, significant mass effect, progressive neurological deficit, or drug-resistant epilepsy with EEG correlation. It is also important to understand which operation is proposed and why: endoscopic fenestration, open fenestration, or cystoperitoneal shunt. Ask what improvement is expected, what risks apply to your anatomy, and whether monitoring is a reasonable alternative. A second opinion is especially useful when surgery is recommended mainly because the cyst is large, because headaches are present, or because different doctors give conflicting advice.
My child was diagnosed with an arachnoid cyst — is it more dangerous in children than in adults?
An arachnoid cyst in a child is not automatically more dangerous than one in an adult, but it usually deserves more careful follow-up. Many pediatric arachnoid cysts are congenital and remain stable, but children are still growing, and symptoms may be harder to interpret. Warning features include increasing head size in infants, developmental delay, irritability, vomiting, balance problems, visual symptoms, seizures, hydrocephalus, documented cyst growth, or clear mass effect. In children, follow-up MRI may be recommended more readily than in stable asymptomatic adults. Surgery is not based only on the presence of the cyst. It is considered when the cyst causes pressure, hydrocephalus, progressive neurological symptoms, or strongly correlated seizures. Parents often benefit from a careful explanation before deciding between monitoring and intervention.
Does midline shift or mass effect always mean that arachnoid cyst surgery is needed?
No. Midline shift or mass effect must be interpreted in context. A few millimeters of chronic shift from a long-standing arachnoid cyst is not the same as an acute shift caused by trauma, hemorrhage, or a rapidly growing mass. The brain may adapt to a congenital cyst over many years, and some patients remain asymptomatic despite visible displacement. Surgery becomes more relevant when mass effect is progressive, associated with hydrocephalus, produces matching neurological symptoms, or increases on follow-up imaging. The number of millimeters alone should not determine treatment. Clinical course, neurological examination, cyst location, CSF flow disturbance, symptoms, and surgical risk all matter. This is one reason why neurosurgical opinions may differ.
What is the best surgical treatment for an arachnoid cyst?
There is no single best operation for every arachnoid cyst. The best surgical treatment depends on cyst location, anatomy, wall thickness, internal compartments, relationship to natural cerebrospinal fluid spaces, presence of hydrocephalus, and the reason surgery is being considered. Endoscopic fenestration is often preferred when the cyst can be safely opened into nearby CSF pathways through a minimally invasive route. Open microsurgical fenestration through craniotomy may be better for cysts with thick walls, multiloculated compartments, convexity or interhemispheric locations, or complex posterior fossa anatomy. Cystoperitoneal shunting is usually reserved for selected cases when fenestration is not feasible, has failed, or long-term CSF diversion is necessary. Surgical planning must be individualized.
What is the difference between endoscopic fenestration, open fenestration and cystoperitoneal shunt?
Endoscopic fenestration uses a small camera and a minimally invasive route to create an opening in the cyst wall so the trapped fluid can communicate with normal cerebrospinal fluid spaces. It is often preferred when safe access and a nearby CSF pathway exist. Open microsurgical fenestration uses craniotomy and microscope-guided exposure to create a wider, more controlled opening, which may be better for thick-walled, multiloculated, convexity, interhemispheric, or anatomically complex cysts. A cystoperitoneal shunt places a permanent tube from the cyst to the abdomen to drain fluid. It can be useful in selected difficult cases, but it carries long-term risks such as infection, blockage, overdrainage, subdural collections, and shunt dependency.
When is endoscopic fenestration preferred for an arachnoid cyst?
Endoscopic fenestration is preferred when the cyst is positioned near natural cerebrospinal fluid spaces and a safe internal drainage pathway can be created. It is commonly considered for many middle cranial fossa cysts, selected suprasellar cysts, intraventricular cysts, and other cysts where the endoscope can safely reach the cyst wall and open it into adjacent cisterns or ventricles. The advantages include a smaller opening, no permanent implanted shunt, and often faster recovery. However, it is not ideal for every cyst. Thick walls, multiple compartments, lack of a safe adjacent CSF space, or complex posterior fossa, convexity, or interhemispheric anatomy may make endoscopic treatment less suitable. The decision depends on detailed MRI anatomy.
When is open craniotomy and fenestration better than endoscopic surgery?
Open craniotomy and microsurgical fenestration may be better than endoscopic surgery when the cyst has complex anatomy or when a durable endoscopic opening is unlikely. This may include cysts with thick walls, internal septations, multiloculated compartments, convexity location, deep interhemispheric location, or posterior fossa anatomy where safe endoscopic communication with CSF spaces is limited. Open surgery gives the surgeon direct microscopic visualization of the cyst wall, adjacent brain, blood vessels, and nerves, allowing a wider and more controlled opening. It is more invasive and usually involves a longer recovery than endoscopy, but it may be more effective in selected anatomical situations. The choice should be based on cyst structure and surgical safety, not on a generic preference.
What are the risks of cystoperitoneal shunting?
Cystoperitoneal shunting can help selected arachnoid cysts by diverting fluid from the cyst to the abdomen, but it creates long-term dependence on an implanted device. Possible risks include shunt blockage, infection, overdrainage, underdrainage, abdominal catheter problems, cyst recurrence if the shunt fails, and the need for future revision surgery. Overdrainage may cause headaches, subdural fluid collections, or subdural hematoma because too much CSF is drained. Because a shunt is a permanent foreign body, it is generally not the first choice when a durable fenestration can be safely performed. Shunting is usually reserved for cysts where endoscopic or open fenestration is not technically feasible, has failed, or when long-term CSF diversion is required.
Can symptoms improve after arachnoid cyst surgery even if the cyst remains visible on MRI?
Yes. Surgery for an arachnoid cyst aims to relieve symptoms and improve CSF communication, not necessarily to make the cyst disappear completely. After fenestration, the cyst may remain visible on follow-up MRI and may not shrink dramatically. This does not automatically mean the operation failed. If the cyst has been opened effectively into normal CSF pathways and the patient’s symptoms improve, the surgery may be clinically successful even with a residual visible cavity. Conversely, cyst size reduction alone is not enough if symptoms persist or the original symptoms were not caused by the cyst. Follow-up interpretation should combine clinical change, neurological status, cyst size, mass effect, hydrocephalus, and evidence that CSF drainage has improved.
What size arachnoid cyst is considered large in adults?
There is no universal size chart that determines whether an arachnoid cyst is dangerous or requires surgery. A cyst may be described as large when it measures several centimeters, especially when it occupies a visible space in the middle cranial fossa, posterior fossa, suprasellar region, or along the brain convexity. However, size alone is not the most important factor. A 4–5 cm arachnoid cyst may be stable and incidental, while a smaller cyst in a critical location may cause symptoms if it blocks cerebrospinal fluid pathways or compresses important structures. Doctors interpret size together with location, mass effect, hydrocephalus, midline shift, documented growth, neurological examination, and symptom pattern. The practical question is not only “How large is it?” but “Is it causing a real clinical problem?”
What is the recovery time after arachnoid cyst brain surgery?
Recovery time after arachnoid cyst brain surgery varies depending on the surgical method and the individual case. Endoscopic fenestration usually has a shorter recovery because it is less invasive and does not require a large craniotomy. Open microsurgical fenestration generally involves a longer recovery because the surgeon needs wider exposure to safely open the cyst wall. Cystoperitoneal shunting may require recovery from the procedure itself plus long-term monitoring for shunt-related problems. Many patients gradually resume light daily activities over several weeks, but return to work, driving, sports, and heavy activity must be decided individually. Recovery also depends on whether the patient had seizures, hydrocephalus, neurological deficits, or complications. A cyst may remain visible on MRI even when surgery has successfully improved symptoms.
Can an arachnoid cyst be treated without surgery?
Yes. Most arachnoid cysts are treated without surgery because they are stable, benign, and often incidental findings. “Treatment without surgery” usually means observation, neurological follow-up, and repeat MRI when needed, rather than medication that makes the cyst disappear. Headaches, dizziness, or seizures should also be evaluated separately, because they may have causes unrelated to the cyst. Monitoring is usually appropriate when there is no hydrocephalus, no progressive neurological deficit, no documented cyst growth, and no convincing match between symptoms and cyst location. Surgery is considered only when the cyst is likely responsible for clinically important problems such as progressive mass effect, cerebrospinal fluid blockage, growth, hydrocephalus, or drug-resistant seizures clearly linked to the cyst region. The goal is to avoid unnecessary brain surgery while not missing cases that truly need intervention.
How often should MRI follow-up be done for an arachnoid cyst?
MRI follow-up depends on the patient’s age, symptoms, cyst size, location, mass effect, and whether the cyst is newly diagnosed or already known to be stable. For an asymptomatic cyst, a repeat MRI after 6–12 months is often used to confirm stability. If the cyst remains unchanged and symptoms are absent, the interval may be extended, and in some adults no frequent long-term imaging is needed. Closer follow-up is reasonable in children, large cysts, symptomatic patients, cysts near critical structures, or cases with borderline mass effect or hydrocephalus. Follow-up should not focus only on size. New symptoms, neurological changes, seizures, hydrocephalus, or documented growth matter more than a stable incidental cyst.
Why do neurosurgeons sometimes disagree about whether an arachnoid cyst should be treated?
Neurosurgeons may disagree because arachnoid cyst treatment depends on clinical judgment, not a single measurement. One surgeon may emphasize cyst size, mass effect, seizures, or headache and consider surgery. Another may consider the cyst incidental unless symptoms clearly match the cyst location, there is hydrocephalus, documented growth, focal neurological deficit, or convincing EEG correlation. Surgical method can also be debated because endoscopic fenestration, open fenestration, and cystoperitoneal shunting each have advantages and limitations depending on anatomy. These differences do not necessarily mean that one opinion is careless. They reflect uncertainty in linking symptoms to the cyst and balancing expected benefit against surgical risk. A second opinion is most useful when this correlation is unclear.
Can I receive a neurosurgical second opinion online for an arachnoid cyst?
Yes. An online neurosurgical second opinion can be useful when an arachnoid cyst has been found on MRI or CT and there is uncertainty about symptoms, monitoring, surgery, or the safest surgical method. MRI images, radiology reports, previous CT scans, EEG results when seizures are present, and specialist opinions can be reviewed together with the patient’s symptoms. The goal is to determine whether the cyst is likely incidental or clinically relevant, whether surgery is truly indicated, and whether endoscopic fenestration, open fenestration, shunting, or observation is most appropriate. Online consultation cannot replace emergency care, but it can help clarify complex decisions, especially when medical opinions differ or surgery has been proposed without a clear explanation.
Further Reading & Professional Resources
• Johns Hopkins Medicine — Arachnoid Cysts Overview
Clear explanation of symptoms, diagnosis, and when treatment may be necessary.
Read here
Clear explanation of symptoms, diagnosis, and when treatment may be necessary.
Read here
• Cleveland Clinic — Arachnoid Cyst
Patient-friendly explanation of causes, symptoms, and management options.
Read here
Patient-friendly explanation of causes, symptoms, and management options.
Read here
• National Organization for Rare Disorders (NORD)
More detailed background on congenital arachnoid cysts and clinical variability.
Read here
More detailed background on congenital arachnoid cysts and clinical variability.
Read here