Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
January 28, 2026
Who This Glioblastoma (GBM) Page Is For
This page is intended for patients diagnosed with glioblastoma (GBM), as well as for family members and caregivers who are seeking a clear, structured explanation of the disease and its treatment options.
Readers are not expected to read this page from start to finish. Instead, you may return to different sections as the disease progresses — when treatment decisions arise, MRI findings become unclear, or new questions appear at later stages.
If recommendations differ, surgery is described as high risk or not indicated, post-treatment MRI findings are ambiguous (tumor recurrence vs. radiation necrosis), or you are unsure what surgery can realistically achieve in your specific situation, an individualized neurosurgical second opinion can help clarify options and outline a realistic strategic path forward.
When patients and families seek a second opinion for glioblastoma (GBM)
• The diagnosis feels overwhelming or difficult to understand
• Surgery is described as high risk or not recommended
• It is unclear why surgery, biopsy, or only radiochemotherapy is proposed
• MRI findings after treatment raise questions about recurrence or radiation necrosis
• Prognosis and further treatment options are not clearly explained
• An independent, expert evaluation is needed regarding clinical trials or emerging treatment alternatives to ensure they are scientifically sound and safe for the patient
In glioblastoma care, seeking an independent expert opinion is a common and responsible step.
If this reflects your situation, you may request an individualized neurosurgical review here:
Request Second Opinion
Glioblastoma (GBM) — Quick Summary (Read This First)
- Glioblastoma (GBM) is the most aggressive primary malignant brain tumor in adults. It grows diffusely, meaning tumor cells spread microscopically into surrounding brain tissue beyond what is visible on MRI.
- GBM is classified as CNS WHO grade 4. The most common form is IDH-wildtype glioblastoma, which behaves aggressively and usually appears suddenly rather than evolving slowly over years.
- Once the diagnosis of glioblastoma (GBM) is confirmed, surgery alone can almost never cure the disease. Even when all visible tumor is removed, microscopic tumor cells remain infiltrating the surrounding brain tissue. Surgery is therefore aimed at reducing tumor burden, relieving intracranial pressure, and preserving neurological function, while additional treatments are required to address residual disease.
- MRI with contrast is the key diagnostic test. The enhancing “core” seen on MRI represents only part of the tumor; invisible infiltrative cells extend beyond it like a fog.
- Standard treatment combines surgery (when feasible), radiotherapy, and chemotherapy with Temozolomide. Radiation is typically delivered as 60 Gy over 6 weeks, with chemotherapy given during and after radiation.
- Not all patients are candidates for surgery. Decisions depend on tumor location, neurological function, and the Karnofsky Performance Status (KPS), which reflects the patient’s ability to care for themselves.
- Recurrence is common. New MRI changes after treatment may represent tumor recurrence or radiation injury (radiation necrosis), which can be difficult to distinguish.
- Overall prognosis is limited. Median survival is approximately 12–15 months, but outcomes vary depending on age, functional status, extent of resection, and molecular markers such as MGMT promoter methylation.
- This page is structured so you can read only what matters to you. Use the Contents box to jump to sections on diagnosis, surgery, radiotherapy, recurrence, or prognosis.
Most readers benefit from the Quick Summary plus the sections on Treatment, Why Surgery Is Sometimes Not Recommended, and Prognosis. The remaining sections provide deeper understanding.
Contents
- Who this is for
- Quick summary
- How GBM develops
- Infiltrative growth
- Brain damage
- Clinical presentation
- Karnofsky scale
- MRI diagnosis
- Differential Diagnosis
- Treatment overview
- Symptomatic-Treatment
- Palliative Treatment
- Surgery
- When surgery not done
- Surgical technologies
- Histopathology & genetics
- Radiation & chemo
- Recurrence
- Radiation necrosis
- Surgery vs Biopsy vs Conservative Treatment
- Prognosis
- Experimental therapies
- Alternative Treatments
- FAQs
- Second opinion
Glioblastoma (GBM) is one of the most aggressive malignant brain tumors in adults and represents the most common primary brain cancer in adulthood.
Glioblastoma belongs to a broader group of brain tumors called gliomas. The term glioma refers to tumors that arise from glial cells — the supportive cells of the brain that normally protect, nourish, and stabilize neurons (nerve cells). When these glial cells become malignant, they can grow uncontrollably and infiltrate normal brain tissue.
From a clinical perspective, glioblastoma is classified as a diffuse glioma. For patients, “diffuse” means that the tumor does not grow as a clearly defined mass with sharp borders. Instead, it spreads through the brain like a network, sending microscopic extensions into surrounding healthy tissue. This infiltrative growth pattern makes it extremely difficult to determine where the tumor ends and normal brain tissue begins.
More than 90–95% of tumors classified today as glioblastoma arise as so-called “primary” tumors, meaning they appear suddenly, without evidence of progression from a previously known lower-grade brain tumor. These tumors are defined as glioblastoma, IDH-wildtype (IDH gene not mutated) and are, by definition, WHO (World Health Organization) classification, grade 4, the highest malignancy grade in the World Health Organization classification. In this setting, the absence of an IDH mutation allows the tumor to follow a highly aggressive biological program, characterized by rapid growth and early infiltration of surrounding brain tissue.
Only a small minority — approximately 5% — of tumors previously labeled as glioblastoma were found to carry an IDH gene mutation.
These tumors usually develop through progression from a lower-grade astrocytoma and were historically referred to as secondary glioblastomas. In modern classification, they are recognized as a distinct disease entity and are now classified as astrocytoma, IDH-mutant, grade 4. This represents a rare exception in oncology, where a genetic mutation actually works in the patient’s favor. While most cancer-related mutations increase aggressiveness, the IDH mutation alters tumor metabolism in a way that slows biological behavior and is associated with a more favorable prognosis compared with IDH-wildtype glioblastoma — despite still being a grade 4 tumor.
Glioblastoma most often affects older adults, with a median age at diagnosis of approximately 65 years and the highest incidence between 60 and 75 years. It is uncommon before the age of 40 and rare in childhood. The disease occurs more frequently in men than in women, with a male-to-female ratio of approximately 1.3–1.6 : 1.
Today, the diagnosis of glioblastoma is no longer based solely on microscopic appearance. It is an integrated diagnosis that combines histological features with selected molecular markers.
Although modern research has identified numerous genetic alterations that reflect the biological diversity of glioblastoma — including changes involving genes such as EGFR, TERT, PTEN, TP53, PDGFRA, and ATRX — most of these findings are not yet directly actionable in routine diagnosis, treatment selection, or prognosis. At present, only a limited number of molecular markers have proven clinical relevance (IDH, MGMT), while many others help define tumor subtypes and remain the subject of ongoing research.
How Glioblastoma Develops: Genetic Mutations And Cellular Malignant Autonomy
Glioblastoma (GBM) develops as a consequence of acquired (somatic) genetic mutations that disrupt the normal regulatory mechanisms of cell growth and division. As these mutations accumulate, tumor cells progressively lose normal regulatory control and begin to behave increasingly autonomously from the surrounding neural tissue.
The greater the number and impact of these alterations, the more independent the malignant cells become in their growth, survival, and invasion of the brain.
Two principal groups of genes are involved in this process.
Proto-oncogenes normally regulate controlled cell proliferation. When these genes mutate into oncogenes, they become permanently activated, driving continuous cell division (uncontrolled replication) and increasing cellular autonomy (the ability of cancer cells to ignore the body’s natural signals to stop growing). Functionally, this resembles a ‘gas pedal’ that is stuck in the pressed position, forcing the tumor to grow relentlessly. A common misconception is that only some people carry proto-oncogenes. In reality, we all have them; they are essential for healthy cell growth. However, the risk of glioblastoma arises when these genes suffer accidental damage over time. While the genes themselves are universal, some individuals may have a higher tendency for these mutations to ‘stick’ due to variations in their body’s natural DNA repair mechanisms. In glioblastoma, these mutations are almost always sporadic—meaning they occur by chance during a person’s lifetime rather than being inherited from parents.
Tumor suppressor genes act as physiological brakes that prevent uncontrolled proliferation. When these genes are mutated and inactivated, the cell loses its intrinsic growth inhibition.
The combination of permanently activated growth signals (activated oncogenes) and loss of inhibitory control (deactivated tumor suppressor genes) allows tumor cells to proliferate independently of normal tissue regulation. These mutations can occur spontaneously as ‘copying errors’ when the normal cell replicates its genetic code (DNA) during division—a process that becomes more frequent with age—or as a result of exposure to external mutagenic factors.
In glioblastoma, as in cancer biology more broadly, this model represents a useful simplified framework for understanding tumor development. In reality, glioblastoma involves a wide range of additional genetic and molecular alterations — including changes affecting cell death, DNA repair, metabolism, and immune evasion — and not all involved genes fit neatly into a single functional category. This reflects the true biological complexity of the tumor.
Such genetic alterations occur continuously in the human body, and most abnormal cells are eliminated by immune surveillance (the body’s natural defense system). Tumor formation occurs when mutated cells escape immune control and accumulate additional genetic changes. In glioblastoma, this process often leads directly to a de novo malignant tumor, meaning that GBM is frequently malignant from the outset rather than evolving from a detectable benign precursor.
When we say glioblastoma is rarely inherited, we are referring to extremely uncommon genetic syndromes (such as Li-Fraumeni or Turcot syndrome) that affect less than 1% of all cases. For the vast majority of patients—over 99%—there is no hereditary link, and their family members are not at an increased risk compared to the general population.
Influence of External Factors on the Origin of Glioblastoma (GBM)
The influence of external factors on why a glioblastoma starts is still being intensively studied, but it is important to distinguish proven risks from common myths. Current scientific knowledge indicates, as for other brain tumors, the following:
Ionizing Radiation: Exposure to high-dose radiation (such as previous radiation therapy to the head for other conditions) is the only well-established environmental risk factor for developing glioblastoma. It is important to note that this refers to medical or industrial grade radiation, not the low-level radiation we encounter in daily life.
Infections and Inflammation: Researchers are investigating whether certain viruses (like Cytomegalovirus) or long-term inflammatory processes „prime“ the brain’s environment for tumor growth. While these factors are being closely watched, the evidence is not yet strong enough to label them as direct causes of GBM.
Chemicals and Occupation: Long-term exposure to certain industrial chemicals continues to be monitored. However, in the vast majority of patients, no specific occupational exposure can be identified as a direct trigger for glioblastoma.
Common Myths vs. Reality: Patients frequently ask about stress, head injuries (trauma), overwork, or the use of mobile phones. At present, there is no consistent scientific evidence that these factors directly cause glioblastoma. Specifically, large-scale international studies have not found a definitive link between cell phone radiofrequency waves and GBM. These tumors are primarily driven by the internal genetic „glitches“ mentioned earlier, rather than personal lifestyle choices or daily habits.
| Factor | Risk Level | Scientific Status |
| Ionizing Radiation | Proven Risk | High-dose medical or industrial radiation is the only well-established environmental cause. |
| Somatic Genetic Mutations | Primary Cause | Almost always sporadic (chance „copying errors“). Less than 1% are linked to rare inherited syndromes. |
| Age | Contributing Factor | Risk increases with age as natural DNA repair mechanisms become less efficient. |
| Viruses & Inflammation | Under Study | Investigated as factors that might „prime“ the brain environment, but no direct causal link yet. |
| Industrial Chemicals | Inconclusive | Some links to rubber manufacturing or pesticides are monitored, but rarely identified as a direct „trigger.“ |
| Mobile Phones | No Link | Extensive international studies have found no definitive link to radiofrequency waves. |
| Stress & Head Trauma | No Link | No consistent scientific evidence that these factors cause glioblastoma. |
Infiltrative Growth Pattern Of Glioblastoma
The defining biological feature of glioblastoma is its diffuse infiltrative growth pattern. This means that tumor cells extend microscopically into surrounding brain tissue well beyond the radiologically visible lesion (the main mass that doctors can see on an MRI scan). To put it simply, while the MRI shows the „core“ of the tumor, there are thousands of invisible, microscopic cancer cells spreading out like a fog into the „healthy“ parts of the brain.
This behavior contrasts sharply with tumors such as typical meningiomas, schwannomas, or many pituitary adenomas. Those tumors primarily grow by compressing adjacent brain structures—they act like a growing balloon that pushes the brain aside but stays contained within a relatively clear boundary. Because glioblastoma actually infiltrates (intermingles with) functional brain tissue, no true surgical cleavage plane exists. In other words, there is no „clean line“ where the tumor ends and the healthy brain begins.
This infiltrative nature explains why complete eradication by surgery alone is not possible and why multimodal treatment—using a combination of radiation and chemotherapy to „clean“ the surrounding areas—is absolutely required.
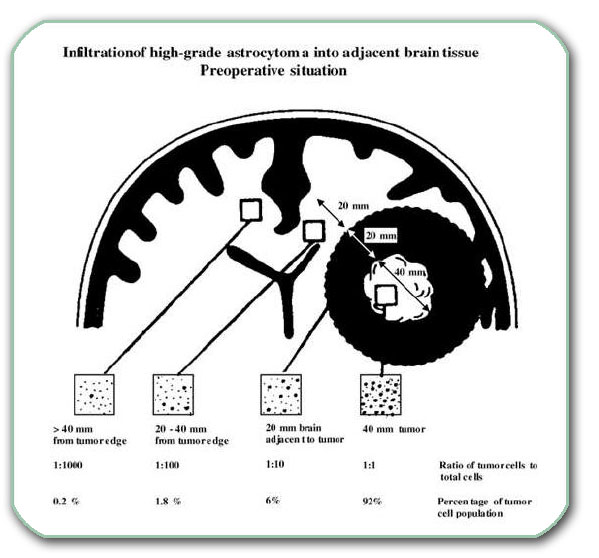
Image: A cross-section of the two cerebral hemispheres. In one hemisphere there is a large GBM (approximately 4 centimeters in diameter). Tumor cells have already penetrated into the wider surrounding area (even into the opposite hemisphere) by infiltration.
Mechanisms Of Brain Damage In Glioblastoma
There are several ways in which glioblastoma disrupts function and damages healthy brain tissue:
- Tumor Infiltration Of Functional Brain Tissue : Glioblastoma damages the brain by infiltrating cortical and subcortical regions responsible for motor control, language, vision, cognition, and behavior. Unlike other tumors that only push the brain aside, GBM pushes the brain and grows through it, weaving between healthy neurons. This progressive disruption of neural networks leads to focal neurological deficits—specific losses of function, such as weakness in an arm or difficulty finding words—that directly reflect which „neighborhood“ of the brain the tumor is invading.
- Peritumoral Edema And Increased Intracranial Pressure: A major contributor to symptoms is extensive peritumoral edema, or brain swelling. The tumor triggers a disruption of the blood–brain barrier (the brain’s protective shield in the walls of blood vessels), causing it to become „leaky.“ This allows fluid to seep into surrounding tissue, resulting in increased pressure within the rigid skull. This pressure often explains why a patient might decline rapidly, and why corticosteroid therapy (like Dexamethasone) can produce a „miracle“ temporary improvement by quickly draining that excess fluid.
- Mass Effect, Herniation Risk, And Secondary Complications: As tumor volume and swelling increase, a mass effect develops—meaning the tumor takes up so much space that it begins to physically shift the brain from its normal position. This can lead to midline shift (pushing the brain to one side) or ventricular compression, which blocks the natural flow of brain fluid and causes hydrocephalus (fluid buildup). In severe cases, this pressure can lead to herniation, where the brain is pushed toward the spinal canal, which is a life-threatening emergency. Additionally, because the tumor’s blood vessels are fragile, a hemorrhage (bleeding inside the tumor) can occur, suddenly worsening the patient’s condition.
Clinical Presentation Of Glioblastoma
There are three primary groups of symptoms associated with glioblastoma, which often develop rapidly over a few weeks:
Headache, Seizures, And Focal Neurological Deficits
Common symptoms include a progressive headache—typically worse in the morning—associated with nausea or vomiting. New-onset seizures in an adult are a major warning sign. Crucially, focal neurologic deficits depend entirely on the tumor’s location: for example, a tumor in the motor cortex causes hemiparesis (weakness on one side of the body), one in the temporal or frontal lobe leads to speech disturbances (aphasia), while a tumor in the occipital lobe results in visual field defects or vision loss. Gait impairment (unsteadiness) often occurs if the tumor affects balance centers or deep pathways.
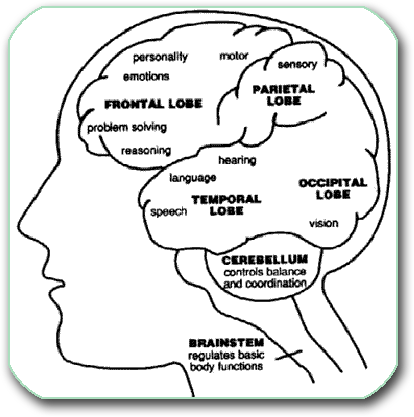
Image: Functional centers in the brain cortex. Explanations regarding the anatomy of various brain regions can be found on this page.
Cognitive And Behavioral Changes
Glioblastoma frequently causes cognitive decline, personality changes, apathy (a sudden lack of interest), and impaired executive function. Because these symptoms can mimic depression or “burnout,” they are often underestimated early on. These changes occur when the tumor disrupts the complex networks in the frontal or temporal lobes that manage behavior and social interaction.
Rapid Neurological Deterioration And Red Flags
Due to the aggressive nature of GBM, symptoms can escalate quickly. Warning signs requiring emergency evaluation include increasing somnolence (extreme sleepiness or inability to wake up), persistent vomiting, or a sudden decline in consciousness. These red flags usually indicate dangerously raised intracranial pressure or mass effect, where the tumor and surrounding swelling are physically shifting the brain, risking permanent damage or herniation.
Functional Status In Glioblastoma
Functional Status and the Karnofsky Performance Scale (KPS)
In patients with glioblastoma and other high-grade malignant brain tumors, symptoms alone are not sufficient to assess disease severity or to guide treatment decisions. Equally important is the patient’s functional status — how the tumor affects daily activity, independence, and overall physical condition.
One of the most widely used tools in neuro-oncology for this purpose is the Karnofsky Performance Status (KPS). In glioblastoma, KPS plays a central role because it directly influences:
- assessment of overall disease severity and biological impact
- indications for surgical treatment and neurological operability
- eligibility for radiation therapy and chemotherapy
- tolerance of aggressive multimodal treatment protocols
- interpretation of treatment response and prognosis
In glioblastoma, a lower Karnofsky score often reflects both tumor aggressiveness and the extent of functional brain involvement. For this reason, KPS is a key parameter in balancing surgical radicality with preservation of neurological function and quality of life.
| Karnofsky Score | Functional Meaning |
|---|---|
| 90–100 | Normal activity or only minor symptoms |
| 70–80 | Independent, but unable to carry out normal work |
| 50–60 | Requires assistance and frequent medical care |
| < 50 | Severe disability, limited self-care |
It is important to note that the Karnofsky score does not define tumor malignancy by itself. Rather, it reflects the functional consequences of the disease. Crucially, the improvement of the KPS after administering Dexamethasone plays a significant role in surgical decision-making. A positive response to steroids often indicates a higher functional reserve, suggesting that the patient may better tolerate and benefit from surgical intervention. Therefore, the score is interpreted together with imaging findings, pathohistological analysis, and molecular markers to guide individualized treatment decisions in glioblastoma.
MRI Diagnosis Of Glioblastoma: Seeing Beyond the Surface
Magnetic resonance imaging (MRI) of the brain, performed both with and without contrast, is the most critical diagnostic tool when glioblastoma is suspected. It is the diagnostic cornerstone because it allows for a precise „map“ of the tumor and its impact on the surrounding brain.
The Contrast-Enhancing „Core“ and the Invisible Roots
On a T1-weighted MRI (a specific type of scan sequence), glioblastoma typically appears as a „heterogeneously contrast-enhancing lesion.“ In simpler terms, when a special dye (contrast) is injected into the blood, the tumor „lights up“ brightly, but in an uneven or patchy way.
- Central Necrosis: Often, the center of the tumor is dark because the cancer is growing so fast it has outstripped its own blood supply, causing the middle to die (necrosis).
- The Leaky Barrier: The reason the tumor „lights up“ with contrast is that aggressive growth has broken the blood-brain barrier—the brain’s natural protective filter. This „leakiness“ helps doctors distinguish high-grade tumors (Grade 4) from slower-growing, lower-grade ones.
- The Iceberg Effect: It is crucial for patients to understand that the bright mass on the T1 MRI is only the „core.“ Microscopic tumor cells extend well beyond these visible margins into healthy-looking tissue.
Practical Aspects: What to Expect During the Scan The MRI procedure is painless and usually lasts between 15 and 45 minutes. Because the machine is a narrow tube and makes loud, rhythmic mechanical noises, it can be stressful.
- Comfort and Anxiety: For patients with claustrophobia or severe anxiety, the scan can be performed under light sedation.
- Preparation: Because contrast dye is required to see the tumor clearly, an intravenous (IV) line will be placed. Doctors will check your kidney function (via a simple blood test) beforehand to ensure your body can safely process and clear the contrast agent.
What MRI Reveals to the Surgeon An MRI provides the „intelligence“ needed for neurosurgical decision-making. It reveals the tumor’s exact location, its size, and its relationship to „real estate“ in the brain—such as centers for speech, movement, and vision. It also identifies dangerous complications like mass effect (the tumor pushing the brain out of place), hemorrhage or hydrocephalus (fluid buildup).
Note: A written radiology report is never enough for a neurosurgeon. They must inspect the images directly to plan the safest „pathway“ into the brain. To a surgeon, the MRI is not just a report; it is a 3D tactical map.
Advanced MRI Techniques: Refining the Map To make surgery as safe as possible, doctors often use „Advanced Imaging“ to avoid damaging critical functions:
- Functional MRI (fMRI): This identifies exactly where your speech and motor centers are located so the surgeon can avoid them.
- MR Tractography (DTI): This visualizes the „wiring“ (white matter tracts) of the brain. Think of it as a GPS for the brain’s internal cables, helping the surgeon navigate without causing permanent paralysis or loss of function.
- MRI Spectroscopy (MRS): This analyzes the chemical „breath“ or metabolism of the tissue, helping to tell the difference between active tumor and simple swelling or radiation damage.
- MR Angiography (MRA): This maps out the blood vessels to prevent accidental bleeding during surgery.
In some cases, a CT scan may be used to look for bone involvement or sudden bleeding, and an EEG may be used if the patient is experiencing seizures. If there is any doubt about where the cancer started, doctors may also scan the rest of the body to ensure the brain tumor isn’t a „secondary“ cancer (brain metastasis) that spread from elsewhere.
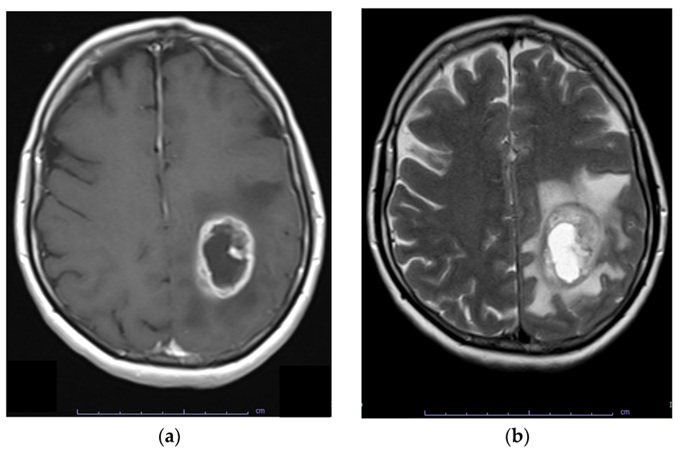
Image: (A) T1-weighted MRI with contrast showing a glioblastoma (GBM) in the left hemisphere; the tumor exhibits a bright white ring of contrast enhancement at the periphery, with a darker center due to internal necrosis. (B) T2-weighted sequence showing the same lesion with extensive surrounding peritumoral edema, which appears as a bright white (hyperintense) area. Tumor cells infiltrate even outside the shown edematous area.
Key Tumor Characteristics Influencing Surgical Strategy
- Size and Growth Pattern: We assess whether the tumor is a localized mass within a single lobe or shows a multilobar/diffuse growth pattern. If the tumor has already spread across multiple brain lobes or involves both hemispheres (crossing the midline), the surgical goal may shift from radical resection to a diagnostic biopsy or more conservative debulking.
- Location (Depth and Surroundings): Whether a tumor is superficial or deep-seated significantly impacts accessibility. Of paramount importance is the tumor’s proximity to eloquent areas—regions of the brain responsible for vital functions like speech, movement, or vision.
- Presence of Complications: The surgical plan must immediately address secondary issues such as:
- Hemorrhage: Acute bleeding within the tumor.
- Hydrocephalus: Obstruction of cerebrospinal fluid flow requiring diversion.
- Herniation: Critical brain displacement caused by extreme pressure.
Differential Diagnosis: What Else Could the MRI Show?
Because glioblastoma typically appears as a contrast-enhancing mass with a dark (necrotic) center, it can be difficult to distinguish from other lesions based on a standard MRI alone. Identifying the correct diagnosis is critical, as the treatment for a lymphoma or an abscess is fundamentally different from the treatment for glioblastoma.
The most common „imitators“ of glioblastoma include:
- Primary Central Nervous System Lymphoma: This tumor can look very similar to GBM, but it often responds dramatically to steroids. Unlike GBM, lymphoma is treated primarily with specialized chemotherapy, and surgical resection is usually avoided as it does not improve the outcome.
- Brain Metastases: These are „secondary“ cancers that have spread from other organs (like lungs or breasts). They often appear as multiple well-defined circles, whereas GBM is usually a single, more infiltrative mass.
- Brain Abscess: A localized infection can create a ring-enhancing lesion that looks almost identical to a tumor core. However, an abscess requires urgent antibiotics or drainage rather than oncological surgery.
- Tumefactive Demyelinating Lesions: In some cases of Multiple Sclerosis or related disorders, the immune system attacks the brain so aggressively that it creates a mass-like appearance on MRI that can be mistaken for a glioma.
- Subacute Ischemic Stroke: Occasionally, a healing stroke can show „luxury perfusion“ and contrast enhancement that mimics the edges of a tumor.
Why Histopathology Remains the „Gold Standard“
While advanced imaging techniques such as MR Spectroscopy, Perfusion MRI, or advanced PET studies can provide important clues — for example, suggesting high cellular turnover, altered metabolism, or increased tumor vascularity — they cannot provide absolute diagnostic certainty.
For this reason, a biopsy or surgical resection is almost always required to establish a definitive diagnosis. Tissue samples are examined under the microscope (histopathology) to identify hallmarks of malignancy, which patients often see listed in their pathology report. These may include:
- Tumor necrosis (areas of dead tumor tissue caused by rapid growth),
- Increased mitotic activity (frequent cell division),
- Microvascular proliferation / angiogenesis (abnormal new blood vessel formation),
- High cellular density and nuclear atypia (abnormal tumor cell appearance).
Immunohistochemistry is then used to confirm the tumor’s cellular origin and biological behavior. Markers such as GFAP (glial fibrillary acidic protein) help confirm glial differentiation, while additional stains (e.g., OLIG2, ATRX, p53, Ki-67 proliferation index, EMA, cytokeratins) may be used to further characterize the tumor and exclude mimicking conditions.
Modern diagnosis does not stop at microscopy. The final classification requires molecular testing, most importantly:
- IDH mutation status, which separates glioblastoma (IDH-wildtype) from biologically distinct astrocytomas,
- MGMT promoter methylation, which predicts sensitivity to Temozolomide chemotherapy and has major prognostic significance.
Only this integrated histopathological and molecular analysis can reliably distinguish glioblastoma from other entities that may appear similar on MRI — such as primary CNS lymphoma, metastases, inflammatory lesions, or treatment-related changes — and determine the most appropriate treatment strategy.
Treatment of GBM
Once a brain tumor is diagnosed, a multidisciplinary team of specialists (often referred to as a Neuro-Oncology Board) evaluates the case to determine the most effective treatment plan. The available options generally fall into three categories: symptomatic treatment, surgical intervention, and adjuvant therapy (such as radiation or chemotherapy).
The treatment strategy is based on the latest neuro-oncological clinical guidelines and the patient’s overall health.
Although this page explains glioblastoma in detail, it cannot replace individualized surgical decision-making.
After evaluation by a multidisciplinary neuro-oncology team (tumor board), the treatment decision may be one of the following:
• Surgical resection followed by radiotherapy and chemotherapy (Temozolomide), which is the most common approach when surgery is feasible
• Biopsy followed by radiotherapy and chemotherapy when safe resection is not possible or would not provide meaningful benefit
• Symptomatic (palliative) treatment only in patients with poor functional status or extensive disease where active treatment would not improve quality of life
The primary question is not whether surgery is technically possible, but what is realistically gained by surgery and whether it is truly indicated in a specific patient. This depends on a complex interaction of factors — functional status (Karnofsky score), tumor location and extent, neurological deficits, response to steroids and prior therapy, patient age, and overall clinical condition. No single factor is decisive on its own. The relative weight, quality, and combination of these factors vary from patient to patient and can be accurately interpreted only by a neurosurgeon with extensive experience in treating glioblastoma.
Even when surgery is indicated, critical decisions remain: the surgical approach, the use of intraoperative technologies, the realistic goal of resection, which surrounding brain structures are directly or indirectly at risk, and how those risks can be managed during the operation. These decisions cannot be derived from general information or MRI reports alone. They require expert interpretation based on real-world surgical experience with a large number of glioblastoma patients.
Symptomatic Treatment of Glioblastoma (GBM)
Symptomatic treatment in glioblastoma is aimed at controlling the effects of the tumor on the brain, rather than treating the tumor itself. These measures are essential at all stages of the disease and are often started immediately after diagnosis.
The most common symptoms that require treatment include brain swelling (edema), headaches, seizures (epilepsy), nausea, vomiting, confusion, and reduced level of consciousness.
Control of Brain Edema and Intracranial Pressure
Brain swelling around a glioblastoma is a major cause of neurological deterioration. To reduce edema, corticosteroids are prescribed — most commonly Dexamethasone (Dexason). These drugs rapidly decrease swelling and can lead to a dramatic, sometimes immediate, improvement in neurological symptoms. Improvement after corticosteroids reflects reduction of edema and mass effect, not a change in tumor biology.
Dexamethasone may be given intravenously or as tablets, depending on the clinical situation. Because corticosteroids can irritate the stomach and cause metabolic side effects, medications to protect the gastric lining are usually prescribed at the same time. Long-term steroid use is carefully monitored and doses are adjusted to the lowest effective level.
Seizure Control (Tumor-Related Epilepsy)
Seizures are common in patients with glioblastoma, particularly when the tumor involves the cerebral cortex. Anti-epileptic drugs (AEDs) are used to stabilize abnormal electrical activity in the brain and prevent further seizures. Once seizures occur, long-term anti-epileptic therapy is usually required. Drug choice and dosing are individualized based on seizure type, interactions with chemotherapy, and patient tolerance.
Headache, Nausea, and Other Symptoms
Headaches, nausea, and vomiting are typically related to increased intracranial pressure. These symptoms often improve with steroid therapy but may also require additional medications such as analgesics or anti-nausea drugs. Confusion, agitation, or behavioral changes may require supportive medications and careful neurological monitoring.
When Symptomatic (Palliative) Treatment Is the Main Approach
In some patients, symptomatic treatment represents the only appropriate therapeutic strategy.
This situation most often applies to patients with:
- very aggressive glioblastoma,
- severely reduced Karnofsky Performance Status (KPS), indicating major loss of independence,
- extensive brain involvement where surgery is not feasible,
- inability to tolerate radiotherapy or chemotherapy.
In these cases, aggressive oncological treatment would not improve survival or quality of life and may cause additional harm. The same approach is used in patients with advanced systemic cancer and brain involvement, where neurological symptoms are part of a widespread disease.
Goals of Symptomatic Care
When treatment is purely symptomatic, the focus is on:
- reducing brain edema and pressure,
- controlling pain and seizures,
- managing confusion, agitation, or restlessness,
- maintaining comfort and dignity,
- supporting the patient and family.
The primary goal is quality of life, not tumor control — minimizing suffering and preserving the best possible neurological function for the time that remains.
Role of Histological Confirmation in a Palliative Context
In most patients with glioblastoma, a histopathological diagnosis is obtained through surgery or biopsy.
However, in a small subset of patients with very poor functional status, extensive bilateral disease, or high procedural risk, biopsy may not be pursued if it would not change management or improve quality of life.
In such cases, treatment decisions may be based on a highly characteristic MRI appearance and clinical course, with the primary goal remaining symptom control and patient comfort.
Surgical Treatment Of Glioblastoma
Surgical treatment involves a craniotomy (the surgical opening of the skull). The surgeon then navigates through the brain tissue to access the tumor, often using neuronavigation to guide the path. Once reached, the goal is to remove as much of the tumor as safely possible—a process known as maximal safe resection. The primary goal is to maximize tumor removal while safeguarding neurological function. This balance is critical, as the preservation of a high Karnofsky Performance Status (KPS) is just as vital for the patient’s prognosis as the extent of the resection itself. A stable KPS not only ensures functional independence but also determines the patient’s eligibility for essential post-operative therapies like radiation and chemotherapy.
Goals Of Surgery In High-Grade Gliomas
Surgery in glioblastoma serves multiple purposes: maximal safe reduction of tumor burden, relief of intracranial pressure, improvement or stabilization of neurological function, and the collection of tissue for integrated histopathological and molecular diagnosis.
Maximum Safe Resection (What Guidelines Actually Support)
Greater safe tumor removal is associated with better outcomes, but there is no single universal percentage that applies to every patient. Some analyses report improved survival with increasing extent of resection above ~78%, yet the most consistent goal in modern practice is gross total resection of the contrast-enhancing tumor whenever it is safely feasible, leaving the smallest possible residual enhancing volume. Importantly, neurological safety always outweighs any numeric target, because glioblastoma is not cured by surgery alone, while a new permanent deficit can significantly reduce quality of life and limit further therapy.
In selected superficial, non-eloquent cases, some centers may attempt resection beyond the enhancing margin, but this is not a universal standard and is considered only when function can be fully protected.
Extent of resection should be verified by an early postoperative contrast-enhanced MRI, ideally within 48 hours.

Image: The image illustrates a craniotomy. Both the skin incision and the skull opening are performed within the hair-bearing area of the scalp. The dura is opened to expose the brain as part of the surgical approach to the tumor. After the procedure, the dura is closed with stitches, the bone flap is secured, and the scalp is reconstructed, ensuring no cosmetic defect remains after healing.
Modern Surgical Technologies in Glioblastoma Surgery
The goal of modern neurosurgery is to maximize tumor removal while leaving healthy brain tissue untouched. To achieve this, several advanced technologies are used to guide the surgeon in real-time.
Neuronavigation and Intraoperative Imaging
Think of neuronavigation as „GPS for the brain.“ By synchronizing the patient’s head with their MRI scans, this system allows the surgeon to see the exact position of their instruments inside the brain with sub-millimeter precision. This is especially vital for reaching deep-seated tumors or defining the irregular edges of a glioblastoma. In some centers, intraoperative MRI or Ultrasound is used to update these „maps“ during surgery as the brain shifts.

Image: Preoperative preparation for brain tumor surgery using MRI-guided neuronavigation in the operating room.
Fluorescence-Guided Surgery (5-ALA)
Glioblastoma cells often blend in with healthy brain tissue, making them hard to see under standard white light. With this technology, the patient drinks a special liquid (5-ALA) a few hours before surgery. Under a specific blue light on the surgical microscope, the tumor cells glow a bright pink/violet color. This „glow-in-the-dark“ effect helps the surgeon identify and remove hidden tumor clusters that would otherwise be invisible, significantly increasing the likelihood of a complete resection.
Intraoperative Neurophysiological Monitoring (IONM)
This acts as a continuous „early warning system“ for the brain’s function. While the patient is asleep, specialized technicians monitor electrical signals passing through the brain. If the surgeon’s instruments get too close to a vital pathway—such as the nerves controlling movement or sensation—the system provides an immediate alert. This allows the surgeon to stop or change direction before any permanent neurological damage occurs.
Awake Craniotomy in Eloquent Cortex
For tumors located in „eloquent“ areas (the centers for speech, language, or complex movement), an awake craniotomy is the safest option. Although the patient is awake for part of the procedure, they feel no pain because the brain itself has no pain receptors and local anesthesia is used for the scalp. By having the patient talk, count, or move their fingers during the resection, the surgeon can map the brain in real-time. This ensures the tumor is removed as aggressively as possible without damaging the patient’s ability to communicate or move.
Note to Patients: Not every surgery requires all of these technologies. Your neurosurgical team will select the specific tools that are most appropriate for the size and location of your tumor to ensure the safest and most effective outcome.
Read more about potential complications following craniotomy and open brain surgery on this page.
When Surgery Is Not Recommended And Biopsy Is Preferred in Glioblastoma
Surgical resection is not automatically the best option in every patient.
When microsurgical removal is judged to be high-risk due to the patient’s medical condition or tumor location in eloquent or deep brain structures, guidelines support performing a biopsy to obtain a definitive histological and molecular diagnosis. Importantly, technical resectability alone is not a sufficient indication for surgery if meaningful functional recovery cannot be expected.
In general, surgery is more often pursued when functional status is adequate to tolerate recovery and proceed with radiochemotherapy — often after medical stabilization with steroids, when improvement suggests that symptoms are driven by edema and mass effect rather than irreversible damage. However, decisions are individualized and not based on strict thresholds alone.
Surgery may do more harm than good in patients with:
• low Karnofsky Performance Status (KPS)
• tumors in eloquent cortex or deep brain regions
• extensive or diffuse tumor involvement
• significant comorbidities
• situations where resection would not improve outcome or enable further therapy
For example, in tumors with diffuse bilateral involvement or classic “butterfly” glioblastoma, where the lesion crosses the corpus callosum and spreads into both hemispheres, meaningful tumor removal is often impossible. Attempting aggressive resection in this region would risk severe and permanent neurological damage.
Similarly, lesions located in eloquent cortex, thalamus, basal ganglia, or brainstem may carry an unacceptably high risk of permanent deficit if resected.
In these situations, surgery may worsen neurological function without improving quality of life.
Instead, a stereotactic biopsy is performed to obtain tissue for definitive diagnosis and molecular analysis, which is necessary for planning and initiating adjuvant treatment (radiotherapy and chemotherapy).
A biopsy allows:
• confirmation of tumor type and grade
• identification of molecular markers
• selection of the appropriate treatment protocol
• avoidance of unnecessary or harmful resection
A biopsy is typically performed using frameless stereotaxy, allowing safe sampling of the tumor with high precision.
Importantly, biopsy is not a lesser option, but a medically appropriate step that enables timely and correct oncological treatment.
Bottom Line for Patients and Families
When doctors recommend against surgery, it is often because the patient’s ability to care for themselves is already too limited. The goal is not to remove tumor at any cost, but to avoid an operation that would take away remaining independence without real benefit.
Request Glioblastoma (GBM) Neurosurgery Consultation — 24-Hour Review or Priority Option (Usually Within 3 Hours)
When an MRI suggests glioblastoma (GBM), patients and families are often faced with urgent, high-stakes questions:
what the MRI really means, whether surgery is possible, how much can realistically be removed, and how radiotherapy and temozolomide are planned afterward. An independent, expert evaluation is needed regarding clinical trials or emerging treatment alternatives to ensure they are scientifically sound and safe for the patient.
An independent neurosurgical second opinion can help you understand the situation clearly, confirm whether the proposed plan is optimal,
and explain what outcomes are realistic based on tumor location, MRI features, neurological status, and overall functional condition.
- ✔ Send a short message describing the suspected GBM diagnosis, current symptoms (weakness, speech problems, seizures, confusion, headache), and what your MRI report says
- ✔ You’ll receive a reply within 24 hours explaining if and how we can help in your specific glioblastoma situation
- ✔ Time-sensitive cases: if neurological status is worsening, there is midline shift/hydrocephalus, or doctors are urgently recommending surgery or biopsy, consultations can often be arranged within a few hours — write PRIORITY in your first message
- ✔ MRI images (DICOM) and hospital documentation can be reviewed once initial contact is established
- ✔ During the consultation, we explain operability and surgical goals (maximum safe resection vs biopsy), expected recovery, and what radiotherapy + temozolomide typically involves — with up to 10 days of follow-up for brief questions
Consultation fees typically range from $180–250, depending on case complexity and MRI findings.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth second opinions in neurosurgery.
Pathohistological And Molecular Diagnosis Of Glioblastoma
The diagnostic process begins with histopathological examination to confirm a high-grade glial tumor (WHO grade 4). Under the microscope, pathologists assess hallmark features of malignancy such as marked cellular atypia, increased mitotic activity, microvascular proliferation, and necrosis.
Immunohistochemistry is used to confirm that the tumor arises from glial cells, most commonly with markers such as GFAP (glial fibrillary acidic protein), which helps distinguish gliomas from metastases, lymphomas, or other non-glial lesions.
Final diagnosis now requires molecular analysis. Importantly, some molecular alterations involve genes that are normal and essential in healthy cells, but whose changes inside tumor cells paradoxically work in the patient’s favor.
If an IDH gene mutation is present, the tumor belongs to a biologically distinct subgroup with slower growth and a more favorable prognosis, even though it is still classified as a grade 4 tumor. In contrast, tumors that are IDH-wildtype (not mutated) follow a more aggressive biological course and are classified as glioblastoma.
The MGMT promoter status is also tested. MGMT is a normal DNA-repair gene that, when active, allows tumor cells to repair the DNA damage caused by Temozolomide chemotherapy. When the MGMT promoter is methylated (functionally inactivated), this repair mechanism is switched off. As a result, Temozolomide-induced DNA damage cannot be effectively repaired, making the chemotherapy significantly more effective.
These molecular findings are essential because they do not merely confirm the diagnosis — they explain why some glioblastomas respond better to treatment and help predict realistic benefit from standard therapy.
Adjuvant Treatment Of Glioblastoma
Radiotherapy And Temozolomide (Standard Protocol)
Radiotherapy combined with chemotherapy is the central and unavoidable part of treatment for glioblastoma, typically starting 3–6 weeks after surgical resection or biopsy. Surgery alone is never sufficient because microscopic tumor cells always remain spread throughout the surrounding brain tissue. In almost all cases, a pathohistological (PH) diagnosis is mandatory to confirm the tumor grade and molecular profile before starting these treatments. However, in rare and specific clinical situations—such as diffuse brainstem gliomas where a biopsy would be too dangerous—oncologists may proceed with radiotherapy based solely on the „typical“ appearance of the tumor on MRI scans.
How Radiotherapy Is Delivered
Radiotherapy for glioblastoma is delivered as external beam radiation, meaning the radiation comes from a machine outside the body. Treatment is carefully planned using the patient’s MRI and CT scans to create a precise three-dimensional map of the tumor and surrounding brain.
The standard total radiation dose for glioblastoma is:
- 60 Gray (Gy) delivered to the tumor region
- given in 30 fractions (sessions)
- 2 Gy per day, five days a week
- over approximately 6 weeks
Radiation is not given all at once. Dividing the dose into small daily fractions allows healthy brain tissue to recover between treatments while tumor cells—much less capable of repair—are progressively damaged.
How the Tumor Receives a Higher Dose Than the Rest of the Brain
Modern radiotherapy does not irradiate the entire brain equally. This is achieved by directing multiple radiation beams from different angles toward the same target (tumor). While each individual beam passes through a different part of the healthy brain with a low, non-destructive dose, they all converge and overlap at the tumor site. Using advanced planning techniques (3D conformal radiotherapy or intensity-modulated radiotherapy), doctors define:
- a high-dose zone focused on the tumor bed and surrounding infiltrative margin
- a lower-dose zone for adjacent brain tissue
- and strict dose limits for critical structures such as the optic nerves, brainstem, and healthy cortex
This allows the tumor area to receive the full therapeutic dose (up to 60 Gy) while minimizing radiation exposure to the rest of the brain. In practical terms, the radiation is “shaped” to the tumor, not sprayed indiscriminately. The treated margin typically extends into the surrounding infiltrative zone, historically up to 1–2 cm, but is individualized based on MRI features—particularly T2/FLAIR signal abnormalities—and proximity to critical structures.
What the Patient Experiences During Radiotherapy
Radiotherapy is not painful. Each daily session lasts only 10–20 minutes, with the actual radiation delivery taking a few minutes. The patient lies on a treatment table wearing a custom-fitted immobilization mask that keeps the head perfectly still to ensure precision.
Importantly:
- No hospital admission is required
- Patients usually go home the same day
- Most patients continue basic daily activities during treatment
Fatigue often increases gradually over the weeks of therapy, and temporary hair loss occurs in the irradiated area. Skin irritation and mild swelling may also occur, but severe acute complications are uncommon.
Concomitant Temozolomide: Why Chemotherapy Is Given During Radiation
During radiotherapy, patients receive Temozolomide (Temodar) simultaneously. This is called concomitant chemoradiotherapy.
Temozolomide is taken:
- orally, in capsule form
- daily, including weekends
- throughout the entire radiation period
Its role during radiation is not primarily to act as a standalone chemotherapy drug, but to function as a radiosensitizer—a medication that makes tumor cells more vulnerable to the effects of radiation. In simple terms, radiation damages tumor DNA, and Temozolomide prevents the cancer cells from repairing that damage.
Maintenance Temozolomide After Radiation
After completion of radiotherapy, patients typically receive maintenance Temozolomide. This involves:
- higher-dose Temozolomide
- taken for 5 consecutive days
- followed by 23 days of rest
- repeated in monthly cycles, usually for 6 cycles, sometimes longer
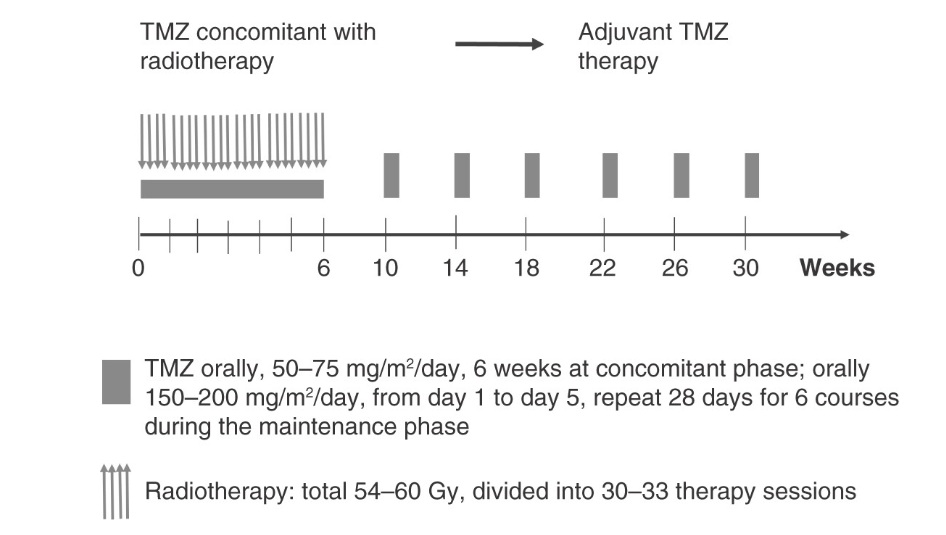
Image: Diagram of treatment courses of the Stupp regimen for patients with newly diagnosed glioblastoma multiforme.
This phase aims to suppress residual microscopic disease and delay tumor recurrence. The benefit of Temozolomide is strongly influenced by MGMT promoter methylation status, which predicts how effectively tumor cells can repair chemotherapy-induced DNA damage.
Hospitalization And Monitoring
Most patients are not hospitalized during radiotherapy or maintenance chemotherapy. Blood tests are performed regularly to monitor blood counts and liver function. Steroids may be adjusted to control brain swelling, and anti-epileptic drugs are used if seizures occur.
Hospital admission is required only if significant complications arise, such as severe neurological deterioration, infection, or uncontrolled symptoms.
Why This Combined Treatment Is Necessary
Radiotherapy and Temozolomide do not “cure” glioblastoma, but they significantly slow tumor progression, prolong survival, and help preserve neurological function. This combined approach targets:
- the visible tumor bed
- the surrounding infiltrated brain tissue
- and microscopic disease that surgery cannot reach
For this reason, radiochemotherapy is the standard of care worldwide for glioblastoma and represents the backbone of modern treatment.
Glioblastoma Recurrence And Further Treatment Options
Glioblastoma almost always comes back. This does not mean that previous treatment “failed,” but that microscopic tumor cells inevitably remain in the brain. What matters most at recurrence is how the patient is functioning, where the tumor is, and how much time has passed since the first treatment.
When Reoperation May Be Recommended
A second surgery is considered only in selected patients, when it is likely to help — not automatically.
Reoperation is most often considered when:
- The patient has a good functional status
(Karnofsky score usually ≥ 70, meaning the patient can walk and care for themselves). - The recurrent tumor is well localized and surgically accessible.
- There is clear neurological deterioration caused by mass effect (pressure) that surgery could relieve.
- A meaningful amount of tumor can be removed, not just a small fragment.
- The patient is expected to tolerate recovery and continue further treatment afterward.
In patients who are already very weak, dependent on others, or bedridden (low Karnofsky score), reoperation rarely improves quality of life and is usually avoided.
A Final Word on Reoperation: The decision to operate a second time is incredibly complex. It depends on a delicate balance of imaging trends, molecular markers, and clinical timing. Because the stakes are so high, this decision should always be made by an experienced neuro-oncological team. A multidisciplinary tumor board is essential to determine whether a second surgery will truly add quality time or merely increase the surgical burden without benefit.
Distinguishing Between Tumor Recurrence and Radiation Necrosis
After radiotherapy, MRI changes can be confusing. New or increasing contrast enhancement does not always mean tumor recurrence.
Two (Actually Three) Possibilities Exist
- True tumor recurrence
Glioblastoma eventually recurs in nearly all patients due to microscopic tumor infiltration. Recurrence most commonly appears within 6–12 months after initial treatment, but timing varies depending on tumor biology, extent of resection, and response to therapy. On MRI, recurrence typically shows progressive and sustained growth over time, often accompanied by clinical deterioration. - Pseudoprogression
A transient treatment-related effect caused by radiotherapy and Temozolomide, most commonly occurring within the first 2–3 months (sometimes up to 6 months) after treatment. It reflects inflammatory and vascular changes rather than true tumor growth and may stabilize or improve on follow-up imaging. This is why early post-treatment MRI changes should be interpreted with caution. - Radiation necrosis
A late radiation-induced injury to the brain, occurring in up to 20–30% of patients, typically months to several years after radiotherapy. It represents permanent tissue damage rather than active tumor and can closely mimic recurrence on MRI.
Why This Is Hard to Distinguish
These conditions can look very similar on MRI:
- new contrast enhancement
- surrounding swelling
- worsening symptoms
Radiation necrosis can appear months or even years after treatment and may cause significant symptoms, even though no active tumor is growing.
How Doctors Try to Tell the Difference
Doctors use a combination of:
- MRI follow-up over time (growth pattern matters)
- advanced imaging (perfusion MRI, spectroscopy, PET in some cases)
- clinical course (speed of deterioration, steroid response)
Sometimes, even with all modern imaging, the diagnosis remains uncertain.
Is Brain Radiation Necrosis Ever Operated On After GBM Treatment?
Yes — in selected cases. Distinguishing between tumor recurrence and radiation necrosis is crucial when clinical status (KPS) declines. If a mass effect is caused by radiation necrosis, surgical removal can lead to a more significant and sustained recovery of neurological function compared to a recurrence. In such cases, surgery serves as a vital ‘rescue’ intervention to restore KPS and improve the quality of life.
Surgery for radiation necrosis may be considered when:
- symptoms are severe and progressive
- steroids are ineffective or cause major side effects
- imaging cannot reliably exclude tumor recurrence
- removing the lesion would significantly reduce pressure on the brain
In these cases, surgery is done not to treat cancer, but to relieve mass effect and confirm the diagnosis.
Does the Time Since the First GBM Surgery Matter?
Yes, very much.
- Recurrence appearing very early (within a few months) usually reflects aggressive disease and is less likely to benefit from surgery.
- Recurrence appearing after 6–12 months or longer, especially in a patient who has remained functional, may be approached more actively.
A longer interval from the first surgery and radiation generally suggests a better biological behavior, even though the disease is still serious.
What About New, Small Areas of Contrast Enhancement After GBM Surgery?
Not every small new contrast-enhancing spot requires immediate surgery.
In patients with:
- good functional status
- minimal symptoms
- small or slowly growing enhancement
Doctors may choose close observation, repeat imaging, or medical treatment rather than immediate reoperation. Decisions are based on trend over time, not a single scan.
When Further Surgery Is Not Helpful in GBM Recurrence
Reoperation is usually avoided when:
- the patient’s Karnofsky score is low.
- neurological deficits are severe and fixed
- the tumor is diffuse and not removable
- the risks of surgery outweigh any realistic benefit
In these situations, treatment focuses on symptom control and quality of life, not because options are lacking, but because surgery would not change the outcome.
Non-Surgical Treatment of Recurrence: Is There More to Do?
When surgery is not an option, the focus shifts to medical management. This is not purely symptomatic; it can include active treatment to slow the disease down:
- Re-irradiation: In selected cases, a second, highly focused course of radiotherapy — such as stereotactic body radiotherapy (SBRT) or Gamma Knife — may be considered if a sufficient time interval has passed since the initial treatment. While the first radiotherapy course typically delivers around 54–60 Gy to a broader brain region, re-irradiation uses much lower additional doses, often in the range of 15–30 Gy, precisely targeted to a small recurrent lesion. Whether this is possible depends on how much radiation the surrounding brain has already received and its remaining tolerance.
- Systemic therapy: At recurrence, systemic treatment options are individualized. Re-challenge with Temozolomide is considered mainly in patients with MGMT promoter methylation, particularly if there was a meaningful initial response and a sufficient treatment-free interval. Alternative dosing schedules may be used. In other cases, treatment may shift to agents such as Bevacizumab (Avastin) targets tumor-associated angiogenesis and is highly effective at reducing peritumoral brain edema and steroid dependence, often leading to rapid symptomatic improvement, although its impact on overall survival remains limited.
- Clinical trials: Recurrence is often the point at which patients are encouraged to consider clinical trial participation, including studies of novel drugs, immunotherapies, vaccines, or experimental delivery methods. These approaches remain investigational, and potential benefit for an individual patient is uncertain.
Surgery, Biopsy, or No Operation in Glioblastoma — How Decisions Are Made
The following section provides a clear, structured overview of the key treatment decisions in glioblastoma — including when surgery, biopsy, or non-surgical management may be recommended — allowing patients and families to understand the most important decision points without revisiting the full clinical sections above.
When Surgery Is Recommended
Surgery is usually recommended when a meaningful portion of the tumor can be removed without causing major neurological damage. This is more likely when the tumor is located in non-eloquent brain regions, when there is a clear mass effect responsible for symptoms, and when the patient has a good functional status (KPS). In such situations, surgical removal can reduce intracranial pressure, improve neurological symptoms, and create better conditions for further treatment such as radiotherapy and chemotherapy.
When Biopsy Is the Better Option
In some patients, the safest and most appropriate approach is not tumor removal, but biopsy only. This is typically the case when the tumor is located in critical functional areas of the brain, when it is deep-seated, or when it shows a diffuse infiltrative pattern that cannot be safely resected. In these situations, attempting removal would carry a high risk of permanent neurological deficit. Biopsy allows for a definitive diagnosis and proper treatment planning, while avoiding unnecessary surgical harm.
When Surgery May Not Be Beneficial
There are cases in which surgery does not provide meaningful benefit. This is most often seen when the tumor is extensively infiltrating multiple brain regions, when the expected extent of resection would be minimal, or when the patient’s overall condition is significantly impaired. In such situations, treatment may focus on non-surgical therapies, symptom control, and preservation of quality of life, rather than aggressive surgical intervention.
Extent Of Surgery — How Much Should Be Removed
An important part of decision-making is not only whether surgery should be performed, but also how much of the tumor should be removed. The general principle is maximal safe resection, meaning that as much tumor as possible is removed without compromising neurological function. More aggressive surgery is beneficial only if it does not lead to significant deficits. Removing too much in critical areas may worsen functional outcome and reduce the patient’s ability to undergo further treatment.
Risks Of Surgery — What Must Be Balanced
Every surgical decision involves balancing the potential benefit of tumor removal against the risk of neurological damage. Possible complications include motor weakness, speech impairment, cognitive decline, or other deficits depending on tumor location. The level of risk is primarily determined by the relationship between the tumor and functional brain areas, as well as overall surgical accessibility.
Why Different Specialists May Recommend Different Approaches
Treatment recommendations may differ because decisions are based on how each specialist evaluates the balance between tumor resectability and functional risk. Some neurosurgeons may favor a more aggressive approach aiming for maximal tumor removal, while others prioritize preservation of neurological function and safety. These differences do not necessarily mean that one approach is incorrect, but rather reflect different interpretations of the same clinical situation.
Bottom Line For Patients And Families
At recurrence, there is no single “right” answer. Decisions depend on:
- how independent the patient is
- how the brain is affected
- whether surgery can realistically help
Reoperation is sometimes useful, sometimes harmful, and very often not the best choice. The goal remains the same throughout the disease:
to preserve function, relieve suffering, and avoid treatments that take away more than they give.
Prognostic Factors in Glioblastoma
Clinical and Radiological Prognostic Variables
Prognosis in glioblastoma is influenced by a combination of clinical and imaging-related factors. The most important include patient age, Karnofsky Performance Status (KPS), extent of safe surgical resection, tumor location, degree of infiltrative growth, and molecular profile, as well as the presence of seizures lasting more than 6 months before diagnosis. No single factor determines outcome on its own; prognosis emerges from how these variables interact in an individual patient.
Malignant Astrocytoma Score (MAS) and Its Clinical Role
The Malignant Astrocytoma Score (MAS) integrates several key prognostic elements: age, Karnofsky Performance Status, histopathological grade, and the presence of long-standing preoperative seizures (≥6 months). When interpreted together with modern molecular markers such as IDH status and MGMT promoter methylation, MAS supports a more individualized and realistic prognostic assessment rather than relying on tumor grade alone. Importantly, MAS also remains clinically useful in settings where full molecular testing (such as IDH status) is not readily available, which is still the case in many parts of the world.
Functional Survival and Quality of Life in Glioblastoma
In glioblastoma, survival must be interpreted in functional terms. Preserving neurological function, independence, and quality of life is often more meaningful than survival duration alone. Treatments are therefore judged not only by how long they extend life, but by whether they maintain mobility, communication, cognition, and self-care.
Prognosis of Glioblastoma: What the Numbers Really Mean
Glioblastoma is one of the most aggressive malignant brain tumors. Despite modern treatment, it remains incurable, and prognosis is measured in months and years rather than decades.
Overall Survival (All Patients)
Across all patients with glioblastoma:
- Median overall survival is approximately 12–15 months
(meaning half of patients live longer and half shorter) - 2-year survival: approximately 25–30%
- 5-year survival: less than 5–7%
These figures include patients of all ages, functional statuses, and tumor characteristics.
Best-Case Prognosis (Favorable Factors Present)
Outcomes are clearly better in patients with favorable prognostic factors, including:
- younger age (typically under 60–65 years)
- good functional status (Karnofsky ≥70–80)
- near-total or total resection of the contrast-enhancing tumor
- completion of full radiotherapy and Temozolomide
- MGMT promoter methylation
- longer time to recurrence
In this subgroup:
- Median survival can approach approximately 18–24 months
- 2-year survival can reach 40–50%
- 5-year survival may reach 10–15%
(still uncommon, but real)
This represents the upper boundary of what current standard therapy can achieve.
Poor Prognosis Group
In patients with:
- advanced age
- low Karnofsky score (<60)
- biopsy-only treatment
- inability to complete radiochemotherapy
- early recurrence
Expected survival is shorter:
- Median survival is often 6–9 months
- Long-term survival is exceptional
Bottom Line (Without Sugarcoating)
Glioblastoma remains a life-limiting disease.
Modern treatment extends survival and preserves function, but does not cure.
Best outcomes are seen in patients who are:
- diagnosed early
- functionally independent
- able to undergo surgery and full radiochemotherapy
This is the most honest way to discuss prognosis — with numbers, context, and clear limits.
Complementary And Supportive Treatment Considerations
Supportive therapy is essential but must not delay evidence-based treatment. Complementary approaches should be discussed with the neuro-oncology team to avoid interactions and prevent postponement of definitive therapy.
Experimental And Emerging Therapies For Glioblastoma: What Patients Should Know
Despite maximal standard treatment (surgery, radiotherapy, and Temozolomide), glioblastoma almost always progresses. For this reason, many patients and families begin to explore experimental, investigational, or non-standard treatment approaches, especially when they are told that conventional options are exhausted or unlikely to provide further benefit.
These approaches fall into several broad categories.
Clinical trials and targeted therapies.
Some patients enroll in clinical trials testing new drugs, immunotherapies, vaccines, gene-based treatments, or novel delivery systems (such as convection-enhanced delivery). Participation in a trial is a legitimate medical option, but it is important to understand that trials are designed primarily to test safety and feasibility. Benefit for an individual patient is uncertain, and most experimental agents do not ultimately prove effective.
Immunotherapy and vaccine-based approaches.
Glioblastoma has proven particularly resistant to immunotherapy compared with other cancers. While tumor vaccines, checkpoint inhibitors, and personalized immune approaches are actively studied, none have yet replaced standard therapy. Some patients choose these options because they sound biologically appealing, but expectations must remain realistic.
Tumor-treating fields and device-based therapies.
Non-invasive electrical field therapies and other device-based approaches have been introduced and are approved in some regions as adjuncts to standard treatment. Their benefit is modest and depends heavily on patient adherence, tolerance, and functional status.
Why careful evaluation matters.
The key risk of experimental or non-standard treatments is not only lack of benefit, but also loss of time, physical strength, and functional independence. In glioblastoma, preserving neurological function and quality of life is often as important as extending survival. Any experimental option should therefore be weighed against the patient’s current Karnofsky Performance Status, symptom burden, and realistic goals of care.
A balanced approach.
Exploring new or experimental options is not wrong. However, decisions should be made with a clear understanding of what is evidence-based, what is investigational, and what is speculative. Independent expert review can help distinguish between treatments that may be reasonable to consider and those that are unlikely to help or may cause harm.
This is especially important when patients are told that “nothing more can be done.” In practice, that statement may mean no further standard curative treatment — not that care, symptom control, or meaningful decision-making has ended.
Alternative, Off-Label, and Integrative Approaches
When standard treatment options reach their limits, some patients explore experimental protocols, off-label drug combinations, or integrative strategies. This is a natural response to a life-limiting diagnosis and the desire to explore every possible option.
However, in the overwhelming flood of information and „breakthrough“ claims, families often feel lost and confused. An independent second opinion provides a critical safety filter, offering a scientific analysis of these methods to ensure they are safe, evidence-based, and do not interfere with the primary treatment. This clarity allows families to make informed decisions without the burden of uncertainty.
Request an Online Second Opinion & Treatment Analysis
What These Approaches Can—and Cannot—Do
To date, no alternative or integrative approach has been proven to control glioblastoma growth or replace surgery, radiotherapy, or chemotherapy. Some strategies, including metabolic or dietary interventions, are under investigation for their potential to improve treatment tolerance or quality of life, but they should not be viewed as disease-modifying therapies.
Quality of Life, Not Tumor Control
Psychological resilience, motivation, and emotional support can improve how patients experience their illness and treatment. These factors may help maintain daily functioning and coping capacity, but they do not alter the biological aggressiveness of glioblastoma.
Off-Label and Experimental Treatments
Off-label medications or experimental protocols should only be considered within a medically supervised framework. Potential interactions with standard therapies, toxicity, and false expectations must be carefully weighed.
Open and Honest Communication Is Essential
Patients should feel safe discussing any additional or alternative approaches with their treating team. Transparency helps ensure that complementary measures do not interfere with evidence-based treatment or cause avoidable harm.
Bottom Line
Hope and dignity matter. Our responsibility is to help patients pursue hope without losing medical realism, ensuring that every decision prioritizes safety, clarity, and quality of life.
The Future Evolution of Treatment: From Mass Reduction to Precision Targeting
Current standard treatments—surgery, radiotherapy, and chemotherapy—represent the most effective tools available today for glioblastoma. Their primary goal is cytoreduction: reducing tumor burden, slowing progression, and preserving neurological function. Despite clear benefits, these approaches have inherent limitations, particularly in a disease defined by diffuse infiltration and complex molecular heterogeneity.
Toward Molecularly Defined Disease, Not a Single Diagnosis
The future of glioblastoma treatment lies in deeper biological stratification rather than a single uniform diagnosis. Advances in molecular pathology already show that glioblastoma is not one disease, but a spectrum of biologically distinct tumors with different genetic drivers, growth patterns, and treatment sensitivities.
Ongoing progress aims to move beyond histology alone toward:
- identification of key molecular alterations,
- integration of genetic, epigenetic, and metabolic profiles,
- and individualized risk–benefit assessment for each patient.
Targeted and Immune-Based Strategies: Promise and Reality
Precision targeting seeks to develop therapies directed at specific molecular alterations within tumor cells. While conceptually attractive, most targeted agents tested in glioblastoma have shown limited clinical impact so far, largely due to tumor heterogeneity, resistance mechanisms, and the blood–brain barrier.
Immunological approaches, including vaccines, checkpoint inhibitors, and cellular therapies, aim to harness the immune system against the tumor. However, glioblastoma remains a profoundly immunosuppressive disease, and meaningful clinical success with immunotherapy has not yet been achieved outside experimental settings.
What This Means for Patients Today
At present, these emerging strategies complement—but do not replace—standard treatment. They remain areas of active research rather than established clinical solutions. While progress is real, it is incremental, and no breakthrough has yet altered the fundamental prognosis of glioblastoma.
Bottom line: the future of treatment is moving toward biological precision and personalization, but current care still relies on proven multimodal therapy. Honest counseling requires balancing scientific optimism with clinical realism.gical puzzle.
Frequently Asked Questions About Glioblastoma (GBM)
What is glioblastoma (GBM)?
Glioblastoma (GBM) is the most aggressive primary malignant brain tumor in adults. It belongs to the group of diffuse gliomas, which means that tumor cells do not stay inside a clear border. Instead, they infiltrate surrounding brain tissue microscopically, beyond what can be seen on MRI. The bright contrast-enhancing mass on MRI usually represents only the visible core of the disease, while tumor cells may already extend into nearby functional brain tissue. This infiltrative pattern explains why glioblastoma is difficult to remove completely and why treatment usually requires a combination of surgery, radiotherapy, and chemotherapy rather than surgery alone.
Is glioblastoma always fatal?
Glioblastoma is currently considered incurable with standard treatments, but that does not mean treatment is useless or that every patient follows the same course. Surgery, radiotherapy, and Temozolomide can prolong survival, reduce pressure on the brain, preserve neurological function, and improve quality of life. Prognosis varies depending on age, Karnofsky Performance Status, tumor location, extent of safe resection, MGMT promoter methylation, IDH status, and how well the patient tolerates radiochemotherapy. Some patients live significantly longer than average, especially when they remain functionally independent and can complete full treatment. Honest counseling should combine realism with individualized assessment.
Can glioblastoma be completely removed by surgery?
No. Glioblastoma cannot be completely removed in the biological sense, even when the neurosurgeon removes all visible contrast-enhancing tumor on MRI. This is because GBM spreads microscopically into surrounding brain tissue, often beyond the visible tumor border. Surgery can remove the main tumor mass, reduce intracranial pressure, improve symptoms, and provide tissue for histological and molecular diagnosis. However, microscopic tumor cells remain in the brain and must be addressed with radiotherapy and chemotherapy. The surgical goal is therefore maximal safe resection: removing as much tumor as possible while protecting speech, movement, vision, cognition, and overall neurological function.
Why is surgery sometimes not recommended for GBM?
Surgery is sometimes not recommended when removal would cause more harm than benefit. This may happen if the tumor is located in deep or eloquent brain regions responsible for speech, movement, vision, or consciousness, or if the tumor is diffuse, bilateral, or crosses the corpus callosum. Surgery may also be avoided when the patient has very poor functional status, severe medical problems, or cannot tolerate further radiotherapy and chemotherapy afterward. In such cases, biopsy may be safer because it provides tissue for diagnosis and molecular testing without risking major neurological decline. The key question is not whether surgery is technically possible, but whether it meaningfully improves outcome.
What is the Karnofsky Performance Status (KPS)?
Karnofsky Performance Status (KPS) is a scale that describes how independently a patient can function in daily life. In glioblastoma, it is one of the most important practical factors in treatment planning because it reflects whether the patient can tolerate surgery, radiotherapy, chemotherapy, rehabilitation, and possible complications. A patient with KPS 70 or higher is usually independent enough to benefit from more active treatment, while very low KPS often means that aggressive therapy may reduce quality of life without providing meaningful benefit. Improvement after Dexamethasone is also important because it may show that symptoms are partly caused by swelling rather than irreversible tumor damage.
How is glioblastoma diagnosed?
Glioblastoma diagnosis usually begins with MRI of the brain with and without contrast. MRI shows the tumor location, contrast-enhancing core, surrounding edema, mass effect, relationship to functional brain areas, and possible complications such as hydrocephalus or hemorrhage. However, MRI alone cannot prove glioblastoma with certainty because lymphoma, metastasis, abscess, demyelinating disease, or subacute stroke can sometimes look similar. A definitive diagnosis usually requires biopsy or surgical resection, followed by histopathological examination and molecular testing. Modern diagnosis combines microscopic features with markers such as IDH status and MGMT promoter methylation, because these results influence prognosis and treatment planning.
Can MRI alone prove that a brain tumor is glioblastoma?
No. MRI may strongly suggest glioblastoma, especially when doctors see irregular contrast enhancement, central necrosis, surrounding edema, and mass effect, but imaging alone cannot definitively prove the diagnosis. Other conditions such as brain metastasis, lymphoma, abscess, demyelinating lesions, or subacute stroke may sometimes mimic glioblastoma on imaging. MRI helps estimate tumor behavior, define surgical anatomy, and guide treatment planning, but final diagnosis usually requires tissue obtained through biopsy or surgical removal. Histopathological examination and molecular testing remain essential because modern glioblastoma classification depends not only on appearance under the microscope but also on markers such as IDH status and MGMT promoter methylation.
What does contrast enhancement on MRI mean in glioblastoma?
Contrast enhancement on MRI usually means that the blood–brain barrier has been disrupted. In glioblastoma, the enhancing area often represents the most aggressive visible part of the tumor, where abnormal tumor vessels allow contrast dye to leak into the tissue. The center may appear darker because of necrosis, meaning tumor tissue has died due to rapid growth outpacing its blood supply. However, the enhancing core is only part of the disease. Glioblastoma cells often extend beyond the bright rim into surrounding edema and even into areas that appear relatively normal. This is why MRI is a surgical map, but not a complete biological boundary.
How is glioblastoma surgery performed?
Glioblastoma surgery is usually performed through a craniotomy, where part of the skull is temporarily opened to reach the tumor. Modern surgery relies heavily on neuronavigation, MRI guidance, and sometimes awake mapping when the tumor lies near speech or motor areas. The neurosurgeon aims for maximal safe resection, meaning removal of as much visible tumor as possible while preserving critical neurological function. During surgery, ultrasound, fluorescence guidance, or neurophysiological monitoring may help define tumor boundaries and protect healthy brain tissue. Surgery is therefore not simply “removing a mass,” but balancing tumor reduction against the risk of permanent neurological injury. The safest strategy varies depending on tumor location and functional anatomy.
Why do different neurosurgeons sometimes recommend different operations for glioblastoma?
Different neurosurgeons may recommend different approaches because glioblastoma surgery is highly individualized and often involves balancing competing goals. One surgeon may prioritize maximal tumor removal, while another may place greater emphasis on preserving speech, movement, memory, or quality of life when the tumor lies in eloquent brain regions. Differences may also reflect experience with awake surgery, minimally invasive techniques, mapping technology, or interpretation of surgical risk. Importantly, disagreement does not necessarily mean one recommendation is wrong. It often reflects different judgments about how much tumor can be removed safely and what benefit surgery is realistically expected to provide. This is one reason why second opinions are common in glioblastoma care.
When is biopsy preferred over tumor removal in glioblastoma?
Biopsy is preferred when obtaining a diagnosis is important but major tumor removal is unlikely to improve outcome or would carry excessive neurological risk. This commonly applies to tumors located in deep structures, bilateral disease, diffuse infiltration, brainstem involvement, or lesions close to critical pathways controlling speech, movement, or consciousness. Biopsy allows tissue confirmation and molecular testing while minimizing surgical trauma. In some patients with poor Karnofsky Performance Status or severe medical illness, biopsy may also be safer because aggressive surgery could worsen neurological function without enabling meaningful further treatment. The decision is therefore not simply “operate or not,” but whether tumor removal adds realistic benefit beyond establishing diagnosis and guiding therapy.
What is the standard treatment for GBM?
Standard treatment for glioblastoma usually combines maximal safe surgery, radiotherapy, and chemotherapy with Temozolomide. When surgery is feasible, the goal is to remove as much visible tumor as safely possible while preserving neurological function. If safe removal is not possible, biopsy may be performed to confirm diagnosis and molecular profile. Radiotherapy is then typically delivered over several weeks, commonly with daily Temozolomide during treatment, followed by monthly maintenance cycles. This combined approach does not cure GBM, but it slows progression, reduces tumor burden, and helps preserve function. Treatment must be individualized based on tumor location, KPS, age, molecular markers, and overall condition.
Is hospitalization required during radiotherapy for GBM?
Hospitalization is usually not required during radiotherapy for glioblastoma. Most patients receive external beam radiation as outpatient treatment and go home the same day after each session. The treatment itself is painless and usually lasts only a short time, although planning is highly precise and based on MRI and CT images. Patients wear a custom mask to keep the head still during treatment. Fatigue, temporary hair loss in the treated area, mild skin irritation, or worsening swelling may occur, but many patients continue basic daily activities. Hospital admission is needed only if neurological deterioration, infection, uncontrolled seizures, severe swelling, or other complications develop.
What is Temozolomide and how is it taken?
Temozolomide is an oral chemotherapy drug used as part of standard glioblastoma treatment. During radiotherapy, it is usually taken daily, including weekends, because it makes tumor cells more sensitive to radiation damage. After radiation is completed, Temozolomide is often continued as maintenance therapy in monthly cycles, commonly taken for five consecutive days followed by a rest period. Blood tests are needed to monitor blood counts and liver function. The benefit of Temozolomide depends partly on MGMT promoter methylation, because tumors with methylated MGMT are less able to repair chemotherapy-induced DNA damage and often respond better to treatment.
Does MGMT promoter methylation matter in glioblastoma treatment?
Yes. MGMT promoter methylation is one of the most important molecular markers in glioblastoma because it helps predict how well the tumor may respond to Temozolomide chemotherapy. MGMT is a DNA-repair gene. When it is active, tumor cells can repair some of the DNA damage caused by chemotherapy. When the MGMT promoter is methylated, this repair mechanism is partly switched off, making Temozolomide more effective. This is generally associated with better response and longer survival. However, MGMT status is not the only factor. Age, KPS, extent of resection, tumor location, and overall treatment tolerance remain essential in prognosis.
Does glioblastoma always come back?
Glioblastoma almost always recurs because microscopic tumor cells remain in the brain even after surgery, radiotherapy, and chemotherapy. Recurrence does not mean that the first treatment was poorly done or ineffective; it reflects the infiltrative biology of the disease. The tumor may return near the original site or, less commonly, appear in a different region. What matters at recurrence is the patient’s functional status, the location and size of the recurrent tumor, the time since initial treatment, and whether further surgery, re-irradiation, Bevacizumab, clinical trials, or symptom-focused treatment could realistically help. Recurrence decisions must be individualized, not automatic.
How can doctors tell recurrence of GBM from radiation necrosis?
Distinguishing glioblastoma recurrence from radiation necrosis can be difficult because both can cause new contrast enhancement, swelling, and neurological worsening on MRI. Timing helps: pseudoprogression is more common in the first few months after radiochemotherapy, while radiation necrosis may occur months or years later. Doctors compare MRI changes over time, evaluate steroid response, and may use perfusion MRI, spectroscopy, PET imaging, or other advanced techniques. Sometimes uncertainty remains despite modern imaging. In selected cases, biopsy or surgery is needed both to relieve pressure and to confirm whether the problem is active tumor recurrence, radiation injury, or a mixture of both.
How is glioblastoma treated if the tumor comes back (recurrent GBM)?
When glioblastoma comes back, treatment depends on the patient’s functional status, MRI pattern, tumor location, previous surgery, previous radiotherapy, MGMT status, time since initial treatment, and overall goals of care. Options may include reoperation in selected patients, biopsy if the diagnosis is unclear, Bevacizumab to reduce edema and symptoms, Lomustine or other chemotherapy approaches, re-irradiation in carefully selected cases, Optune, clinical trials, or symptom-focused palliative care. There is no single standard treatment that fits every recurrent GBM case. The key question is whether further treatment can realistically preserve function, relieve symptoms, slow progression, or improve quality of life without adding excessive burden.
Can glioblastoma be operated on again?
Glioblastoma can be operated on again in selected patients, but reoperation is not automatic. It is most often considered when the patient has good functional status, the recurrence is localized and surgically accessible, there is clear mass effect causing symptoms, and a meaningful amount of tumor can be removed safely. A longer interval since the first surgery and radiotherapy usually suggests more favorable tumor biology. Reoperation is usually avoided when the patient is bedridden, severely impaired, or when the tumor is diffuse and cannot be removed meaningfully. The goal of repeat surgery is not cure, but symptom relief, diagnosis clarification, and possibly enabling further treatment.
What is the average life expectancy with glioblastoma?
Median survival for glioblastoma is often reported around 12–15 months with modern standard treatment, meaning that half of patients live longer and half live shorter than that estimate. This number should not be used as an exact prediction for an individual patient. Survival is better in patients who are younger, functionally independent, able to undergo maximal safe resection, complete radiotherapy and Temozolomide, and have favorable molecular markers such as MGMT promoter methylation. Some patients live 18–24 months or longer, while others with poor KPS, biopsy-only treatment, advanced age, or early recurrence may have much shorter survival. Prognosis must always be individualized.
Can patients receive an online neurosurgical second opinion for GBM?
Yes. A neurosurgical second opinion for glioblastoma can often be provided through telehealth if MRI scans, pathology reports, operative notes, and medical documentation are available. The goal is to clarify what the MRI shows, whether surgery, biopsy, or non-surgical management is reasonable, what the realistic surgical goal would be, and how radiotherapy, Temozolomide, recurrence, radiation necrosis, or clinical trials fit into the overall strategy. This is especially useful when surgery is described as high risk, when recommendations differ, or when families need help understanding prognosis. Urgent in-person care is still required if neurological status is rapidly worsening.
Learn more about neurosurgery second opinions
.
- MedlinePlus (NIH) — Brain Cancer (patient-friendly overview)
- National Cancer Institute (NCI) — Adult Brain Tumor Treatment (PDQ) (Patient Version)
- Cancer Research UK — Glioblastoma (overview for patients)
- Mayo Clinic — Glioblastoma (symptoms, diagnosis, treatment)
- MD Anderson Cancer Center — Glioblastoma treatment (patient-focused)
- Johns Hopkins Medicine — Glioma Center (includes glioblastoma)
- Kojadinović Z et al. – Malignant Astrocytoma Score (MAS) (PubMed)