Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
March 08, 2026
Who This Peripheral Nerve Injury Page Is For
This page is intended for patients in whom a peripheral nerve injury has been suspected or confirmed after trauma or surgery.
If weakness, numbness, burning pain, or loss of movement has developed after an injury — or if EMG or nerve conduction studies suggest damage to a peripheral nerve — understanding the type of nerve injury, the likelihood of spontaneous recovery, and the possible role of surgery may be important for making treatment decisions. In complex situations, an individualized neurosurgical second opinion may help.
When patients seek a second opinion for peripheral nerve injury
• Weakness, numbness, or loss of movement developed after trauma, fracture, surgery, or injection
• EMG or nerve conduction studies show nerve damage and the prognosis is uncertain
• It is unclear whether the nerve may recover spontaneously or whether surgical repair should be considered
• Persistent pain, burning sensations, or hypersensitivity suggest possible neuroma or nerve irritation
• Several months have passed after the injury and recovery remains limited
• Different specialists recommend observation, rehabilitation, or surgery without clear agreement
If your situation involves uncertainty regarding the severity of nerve damage, expected recovery, or the need for surgery, you may request an individualized neurosurgical review here:
Request Second Opinion
Peripheral Nerve Injury — Quick Summary (Read This First)
- Peripheral nerve injury occurs when a nerve is damaged by trauma, compression, stretching, or surgical procedures. These nerves connect the brain and spinal cord with muscles, skin, and internal organs.
- Peripheral nerves carry motor, sensory, and autonomic signals. Motor fibers control muscle movement, sensory fibers transmit touch and pain signals, and autonomic fibers regulate blood vessels and glands.
- The severity of nerve injury depends mainly on which parts of the nerve are damaged. In mild injuries affecting only the myelin sheath (neuropraxia), recovery is usually complete. When the axon is disrupted (axonotmesis), regeneration is slower but still possible. In severe injuries where the entire internal structure of the nerve is destroyed (neurotmesis), spontaneous recovery is unlikely without surgical repair.
- Peripheral nerve injuries are most commonly caused by trauma. Frequent causes include fractures, joint dislocations, penetrating wounds, traction injuries, surgical procedures, and compression from scar tissue.
- Symptoms depend on the nerve involved and the level of injury. Typical symptoms involve initial numbness and tingling, progressing to burning pain, muscle weakness, and eventually, gradual muscle atrophy.
- Commonly affected nerves include the median, ulnar, and radial nerves in the arm, and the sciatic, femoral, tibial, and peroneal nerves in the leg. Each produces a characteristic pattern of weakness and sensory loss.
- Electrodiagnostic testing is essential for evaluating nerve injury. Electromyography (EMG) and nerve conduction studies (ENG) help determine whether axonal damage has occurred (more severe injury) and whether regeneration is taking place.
- Peripheral nerves have the ability to regenerate. After axonal injury, regenerating nerve fibers grow at an average rate of approximately 1 millimeter per day, although recovery depends on the distance to the target muscle and the preservation of the internal nerve structure.
- Many mild nerve injuries recover spontaneously. Observation, physical therapy, splints, and pain management may be sufficient when nerve continuity and regeneration are preserved.
- Surgery may be required when the nerve is completely severed or when regeneration does not occur. Surgical options include nerve repair (direct suturing), nerve grafting, neurolysis to release scar compression, or nerve transfer procedures.
- Early evaluation is important because motor recovery has a limited time window. If regenerating axons do not reach the target muscle before motor end plates degenerate (usually after about 12–18 months), functional recovery may be incomplete. In closed nerve injuries without signs of regeneration, surgical exploration is often considered after approximately 3–6 months.
- The prognosis depends on the type of injury, the distance to the target muscle, the timing of treatment, and the age of the patient. Mild injuries may recover completely, while severe injuries may leave permanent weakness or sensory deficits.
Most readers benefit from reviewing this Quick Summary together with the sections on Symptoms of Peripheral Nerve Injury, Diagnosis, Treatment, Nerve Regeneration, and Recovery and Prognosis. Later sections provide more detailed explanations intended for patients seeking a deeper understanding before important treatment decisions are made.
Contents
- Who This Page
- Quick Summary
- What Peripheral Nerves Are
- Why Internal Structure Matters
- Mechanisms of Injury
- Types of Nerve Injury
- Neuropraxia
- Axonotmesis
- Neurotmesis
- Symptoms
- Median Nerve Injury
- Ulnar Nerve Injury
- Radial Nerve Injury
- Sciatic Nerve Injury
- Peroneal Nerve Injury
- Tibial Nerve Injury
- Femoral Nerve Injury
- Pain After Nerve Injury
- Diagnosis
- Clinical Examination
- EMG and ENG
- Nerve Conduction Studies
- Electromyography
- Closed Nerve Injuries
- Why Repeated Studies Matter
- Imaging Studies
- Nerve Regeneration
- Motor vs Sensory Recovery
- Treatment
- When Is Surgery Necessary
- Conservative Treatment
- Pain Treatment After Nerve Injury
- Surgical Treatment
- New Treatments: Medications, Stem Cells and Emerging Therapies
- Recovery and Prognosis
- Injury vs Entrapment Syndromes
- Request Second Opinion
- FAQ
Peripheral nerve injuries occur when peripheral nerves are damaged by trauma, compression, stretching, or surgical procedures. Peripheral nerves carry signals between the brain, spinal cord, and the rest of the body, such as muscles and skin. When these nerves are injured, symptoms may include pain, numbness, weakness, or loss of movement in the affected area.
Understanding how a nerve is built is essential to understand why some nerve injuries recover completely while others recover poorly or not at all.
What Peripheral Nerves Are and How They Work
Peripheral nerves are bundles of nerve fibers (axons) that connect the brain and spinal cord with the rest of the body. They transmit:
- motor signals from the brain to muscles
- sensory signals from the skin and joints to the brain
- autonomic signals that regulate blood vessels, glands, and internal organs.
Each individual nerve fiber consists of a long projection called the axon, which carries electrical impulses. The axon is surrounded by a protective insulating layer called the myelin sheath, produced by Schwann cells. Groups of axons are organized into fascicles, and several fascicles together form a peripheral nerve.
The structure can be simplified as: axon → myelin sheath → fascicle → nerve.
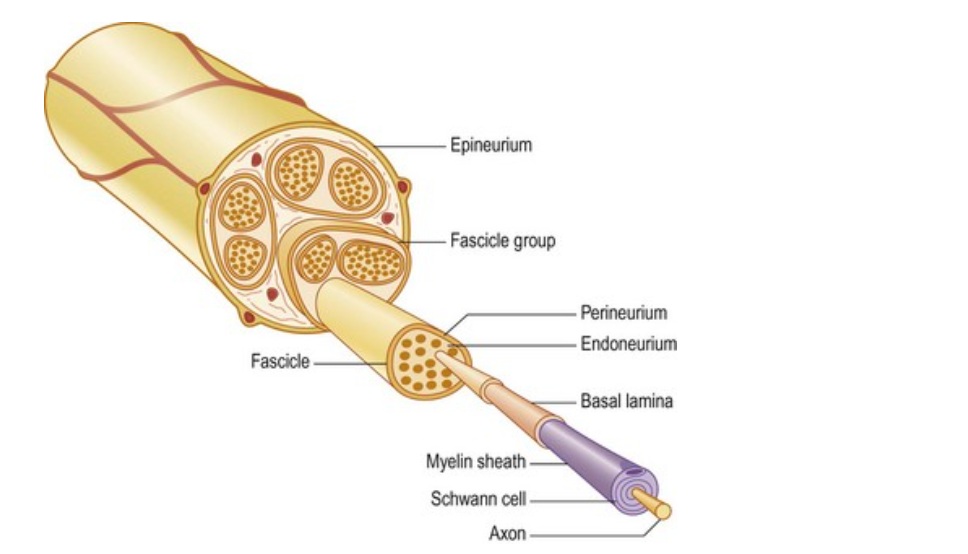
Image: Elements of the nerve
Why the Internal Structure of a Nerve Determines Recovery
The preservation of the internal structure of a nerve is the key factor that determines whether functional recovery is possible after injury.
Each nerve fiber (axon) is surrounded by specialized support cells called Schwann cells and by a microscopic tube formed by their basal lamina. These structures create natural pathways that guide nerve fibers along the length of the nerve. You can think of these structures as microscopic tunnels that guide regenerating nerve fibers back to their destination. When a nerve is injured, the part of the axon beyond the injury site degenerates. Preservation of tunnels is crucial for recovery because regenerating axons can grow back inside these preserved pathways and follow the same route toward their original muscle or skin target.
The outcome depends on which parts of the nerve are damaged.
1. Damage to the myelin sheath only (neuropraxia)
- the axon remains intact
- nerve conduction temporarily stops
Because the axon and its guiding structures are preserved, recovery is usually rapid once the myelin sheath regenerates.
2. Damage to the axon, but the basal lamina tubes remain intact (axonotmesis)
- the axon is interrupted
- the distal part of the nerve degenerates
- the microscopic tunnels remain preserved
In this situation, a new axon can slowly grow back inside the existing tunnels and may reconnect with its original target.
Recovery is possible but takes much longer. After an initial delay of about 2-3 weeks, axons grow 1 mm/day.
3. Damage to both the axon and the basal lamina (neurotmesis)
- the axon is destroyed
- the microscopic guiding tunnels are also disrupted
Without these natural tunnels, regenerating axons lose their path. They may grow in the wrong direction, form a painful neuroma, or fail to reach their target.
The more of the nerve’s internal guiding structures are damaged, the worse the prognosis.
Mechanisms of Peripheral Nerve Injury
Peripheral nerves can be injured in several ways.
Closed trauma
Blunt trauma can cause:
- stretching of the nerve
- compression against bone
- crushing injury.
Closed trauma may occur in:
- sports injuries
- traffic accidents
- falls.
Even without visible wounds, the nerve can be damaged.
Injuries associated with fractures
Bone fractures may damage nerves through:
- direct pressure from displaced fragments
- traction or stretching during injury.
For example, fractures around the elbow or humerus may affect the radial nerve, while knee injuries may affect the peroneal nerve.
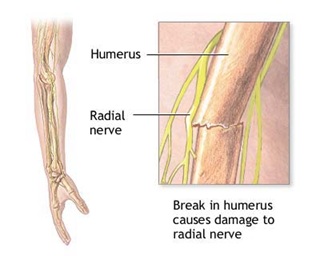
Image: A humerus fracture causes injury to the radial nerve
Sharp injuries
Penetrating trauma such as:
- cuts
- glass injuries
- knife wounds
may partially or completely sever the nerve.
Delayed compression
After trauma or surgery, nerves may become compressed by:
- scar tissue
- fibrosis
- postoperative adhesions.
In such cases, symptoms may develop weeks or months after the original injury.
Types of Nerve Injury
Peripheral nerve injuries are classically divided into three main types: neuropraxia, axonotmesis, and neurotmesis.
Neuropraxia
This is the mildest form of nerve injury.
Only the myelin sheath is damaged, while the axon remains intact.
Because the axon survives, recovery is usually complete and occurs within weeks or months.
Axonotmesis
In this injury, the axon is disrupted, but the surrounding connective tissue structures remain intact.
The axon must regenerate, which occurs slowly. However, because the connective tissue tubes guide the regenerating axon, recovery may still occur.
In closed injuries, the nerve itself may remain anatomically intact, but scar tissue can develop around the nerve during healing. This scar may compress the nerve and interfere with regeneration. In such situations, recovery may appear to stall even though the internal structure of the nerve is preserved. During surgical exploration, it may sometimes be found that the nerve is still continuous, and that simple decompression or release of the scar tissue is sufficient to restore the conditions necessary for recovery.
Neurotmesis
This is the most severe injury. Both the axon and the surrounding connective tissue structures are disrupted.
Neurotmesis most commonly occurs when a nerve is completely cut, but it can also develop after severe contusion or crush injuries that destroy the internal structure of the nerve. Without surgical repair, regeneration is unlikely.
In real injuries, these patterns often occur in combination within the same nerve. Some fibers may have only myelin damage (neuropraxia), while others may have axonal disruption (axonotmesis).
The overall recovery of the nerve therefore depends largely on how many fibers retain preserved internal structure. Injuries dominated by neuropraxia or axonotmesis usually have a much better prognosis than injuries in which a large proportion of fibers suffer neurotmesis.
In addition to the classic three-part classification, surgeons often use a more detailed grading system based on how much of the internal nerve structure remains preserved. In practice, this matters because many real injuries are mixed injuries: one part of the nerve may still have preserved pathways for regeneration, while another part may already be replaced by scar tissue. This is one of the reasons why recovery in the same nerve may be partial, uneven, or slower than expected.
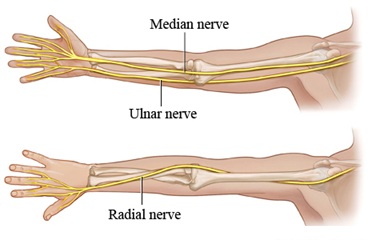
Image: Arm nerves- median, ulnar, radial nerves

Image: Leg nerves — femoral, obturator, sciatic, tibial, and peroneal nerves.
Symptoms of Peripheral Nerve Injury
The symptoms depend on which nerve is affected.
Typical symptoms include:
- numbness or loss of sensation
- tingling or burning pain
- muscle weakness
- loss of movement
- muscle atrophy over time.
Common nerves affected in the arm include the median nerve, ulnar nerve, and radial nerve. Common nerves affected in the leg include the sciatic nerve, femoral nerve, and common peroneal (fibular) nerve.
Median Nerve Injury
Injury to the median nerve most commonly occurs around the elbow or in the forearm, although the nerve can be damaged at other levels along its course. Such injuries may produce a characteristic combination of motor weakness and sensory loss.
Motor symptoms may include:
- weakness of thumb opposition
- difficulty gripping small objects
- loss of fine hand movements
- weakness of thumb flexion and abduction.
In more severe injuries, patients may develop thenar muscle atrophy, meaning wasting of the muscles that form the fleshy mound at the base of the thumb. This leads to flattening of the thumb base and weakness when pinching or gripping objects.
Sensory symptoms typically involve:
- numbness or tingling in the thumb, index finger, middle finger, and part of the ring finger
- reduced sensation on the palmar side of the hand in the radial three and a half fingers.
As the nerve begins to recover, or when neuropathic irritation develops, patients may later experience burning pain or electric sensations in these fingers.
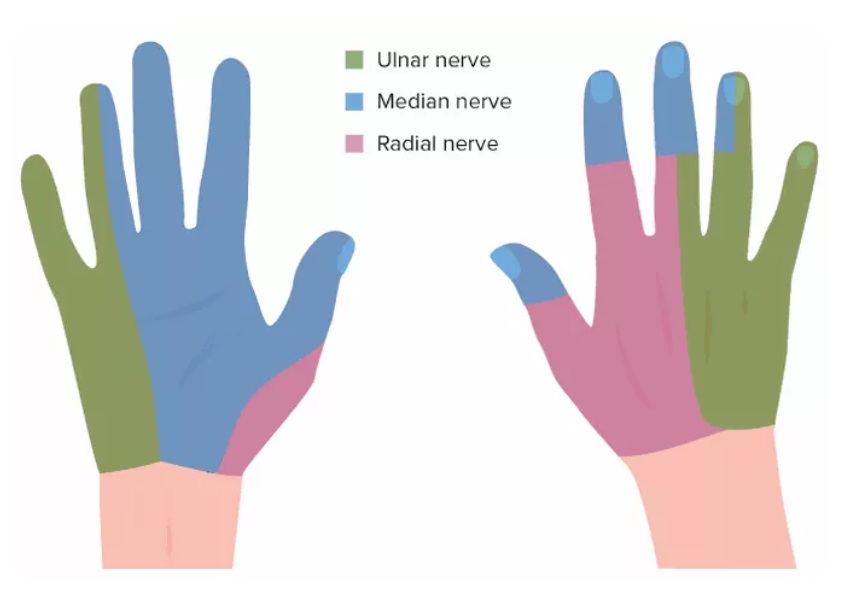
Image: Areas of the hand affected by sensory loss following median, ulnar, or radial nerve injuries.
Ulnar Nerve Injury
The ulnar nerve supplies many of the intrinsic muscles of the hand and is most commonly injured at the elbow in the cubital tunnel or at the wrist in Guyon’s canal.
Motor deficits may include:
- weakness of finger spreading (interossei muscles)
- reduced grip strength
- difficulty holding objects between the fingers
- clawing of the ring and little finger in more severe injuries.
Over time, patients may develop atrophy of the intrinsic hand muscles, especially between the metacarpal bones.
Sensory disturbances involve:
- numbness of the little finger and half of the ring finger
- reduced sensation along the ulnar side of the hand.
Radial Nerve Injury
The radial nerve mainly controls extension of the wrist and fingers and is most commonly injured in the upper arm along the humerus, especially in the part where the nerve runs close to the bone.
Motor injury commonly causes:
- weakness or inability to extend the wrist
- inability to straighten the fingers
- difficulty lifting the thumb.
The classic clinical sign is wrist drop, where the hand hangs downward because the wrist extensors are paralyzed.
Sensory symptoms usually affect:
- the back (dorsal surface) of the hand
- the skin between the thumb and index finger.
Pain is usually less prominent than in some other nerve injuries. However, later during recovery patients may develop burning or tingling sensations on the back of the hand.
Sciatic Nerve Injury
The sciatic nerve is the largest nerve in the body and supplies most of the muscles of the leg. Injuries to the sciatic nerve most commonly occur after trauma to the hip or thigh, particularly hip dislocations, pelvic fractures, penetrating injuries, or complications of hip surgery and injections in the gluteal region.
When the injury occurs lower in the thigh, the clinical picture usually reflects damage to the tibial and peroneal branches, leading to weakness of foot movements such as dorsiflexion, plantar flexion, and toe movements.
When the injury occurs higher in the buttock or upper thigh, the deficit can be more extensive and may also involve the hamstring muscles, leading to weakness of knee flexion in addition to the deficits in the leg and foot.
Because of this, the clinical presentation of sciatic nerve injury depends largely on the level at which the nerve is damaged.
Peroneal (Fibular) Nerve Injury
The peroneal nerve is particularly vulnerable around the fibular head near the knee.
Motor deficits typically include:
- weakness of ankle dorsiflexion
- inability to lift the foot when walking.
This leads to the characteristic condition known as foot drop, where the patient must lift the leg higher to avoid dragging the foot.
Weakness may also affect toe extension and foot eversion.
Sensory disturbances usually involve:
- numbness on the outer side of the lower leg
- reduced sensation on the top of the foot and toes.
Patients may also describe burning pain or tingling on the dorsum of the foot.
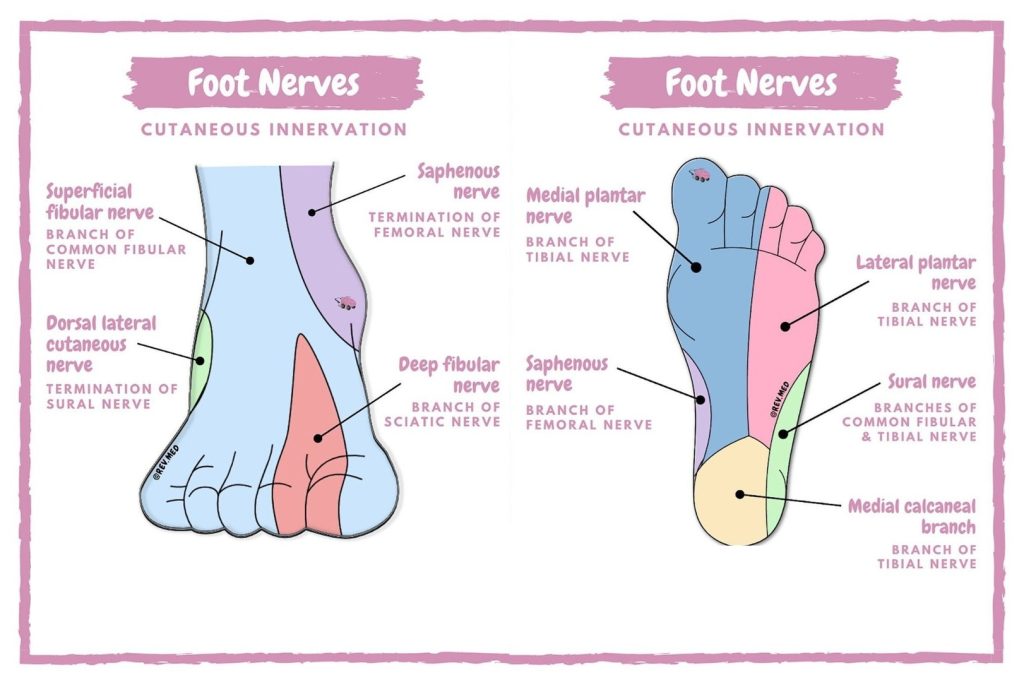
Image: Cutaneous sensory innervation of the foot.
Tibial Nerve Injury
The tibial nerve controls muscles responsible for plantar flexion of the foot and toe flexion and is most commonly injured around the knee or in the popliteal region, often in association with trauma to the posterior knee or leg.
Motor symptoms may include:
- weakness when pushing the foot downward
- difficulty standing on the toes
- weakness of toe flexion.
Severe injuries can interfere with walking and balance.
Sensory loss typically involves:
- the sole of the foot
- the heel and plantar surface of the toes.
Later during recovery, patients may experience burning or tingling sensations on the sole of the foot.
Femoral Nerve Injury
The femoral nerve is important for knee extension and hip flexion and is most commonly injured in the groin or upper thigh region, often during pelvic trauma, hip surgery, or compression in the iliopsoas area.
Motor deficits include:
- weakness when straightening the knee
- difficulty climbing stairs or rising from a seated position.
The quadriceps muscle may become visibly weak or atrophic over time.
Sensory changes usually involve:
- reduced sensation in the front of the thigh
- numbness along the inner side of the lower leg through the saphenous nerve branch.
Later during recovery, some patients may develop deep aching pain in the anterior thigh or groin region.
Pain After Nerve Injury
Pain after nerve injury is often neuropathic.
Patients may experience:
- burning pain
- electric shock sensations
- hypersensitivity to touch.
In some cases a neuroma may form. A neuroma is a painful mass of regenerating nerve fibers that develop at the end of a severed nerve. Neuroma pain can be severe and is often triggered by pressure on the injured nerve.
Diagnosis of Peripheral Nerve Injury
Diagnosis is based on a combination of:
- clinical examination
- electrophysiological studies
- imaging.
Clinical examination
The physician evaluates:
- sensory loss
- muscle strength
- reflexes.
The pattern of neurological deficit often helps determine which nerve is involved, the approximate level of the lesion, and whether the injury is partial or complete.
Electromyography (EMG) and Nerve Conduction Studies (ENG)
Electrodiagnostic testing is one of the most important tools for evaluating peripheral nerve injuries. It helps physicians determine whether a nerve is conducting impulses, whether axonal damage has occurred, and whether recovery is taking place over time.
Two complementary tests are usually performed together:
- nerve conduction studies (ENG)
- electromyography (EMG)
These tests examine different aspects of nerve and muscle function and together provide important information about the type, severity, and prognosis of the nerve injury.
Nerve Conduction Studies (ENG)
Nerve conduction studies evaluate how well electrical signals travel along a nerve.
During the test:
- small surface electrodes are placed on the skin
- the nerve is stimulated with a brief electrical impulse
- the response is recorded either from the nerve itself or from a muscle supplied by that nerve.
The electrical stimulation may feel like a short tapping or tingling sensation, but it is generally well tolerated.
Sensory nerve testing
For sensory nerves:
- the nerve is stimulated at one point
- the electrical response is recorded along the sensory nerve.
This allows physicians to determine:
- whether sensory fibers conduct impulses normally
- whether conduction is slowed or blocked.
Motor nerve testing
For motor nerves:
- the nerve is stimulated
- the response is recorded from the muscle supplied by that nerve.
The recorded signal reflects how many motor axons are functioning.
A reduced response suggests axonal loss or severe nerve injury.
What ENG Shows in Nerve Injury
ENG can detect several abnormalities:
- slowing of conduction, usually caused by myelin damage
- conduction block, where impulses cannot pass through a damaged segment of the nerve even though the axons may still be structurally intact
- reduced response amplitude, which indicates axonal loss.
Conduction block most often occurs when the myelin sheath is damaged, such as in compression injuries. In these cases the axon remains intact, and recovery is usually possible once the myelin regenerates.
However, when ENG shows markedly reduced response amplitude, it usually indicates significant axonal damage, which represents a more severe injury and requires a longer period of recovery.
These findings help distinguish between:
- mild injuries involving the myelin sheath
- more severe injuries involving the axon itself.
Electromyography (EMG)
Electromyography evaluates the electrical activity of muscles.
Unlike nerve conduction studies, EMG requires inserting a very thin needle electrode directly into the muscle. The needle records electrical activity produced by muscle fibers.
Most patients describe the sensation as similar to a small injection or acupuncture needle, and although it may be slightly uncomfortable, it is generally tolerable.
The physician usually examines several muscles supplied by the nerve being evaluated. EMG abnormalities usually appear about 2–3 weeks after nerve injury, when denervated muscle fibers begin to show fibrillation potentials.
What EMG Shows in Nerve Injury
EMG helps determine whether a muscle is receiving normal nerve input.
In healthy muscle:
- the muscle remains electrically quiet at rest
- electrical activity appears only during voluntary contraction.
When a nerve supplying the muscle is injured, characteristic abnormalities appear.
Early phase after nerve injury
In the first days after injury, EMG may still appear normal.
This occurs because the muscle fibers have not yet developed electrical changes.
Denervation phase
After approximately 2–3 weeks, muscles that have lost nerve supply begin to show spontaneous electrical activity at rest, including:
- fibrillation potentials
- positive sharp waves
These findings indicate denervation, meaning the muscle is no longer receiving normal signals from the nerve.
Detecting Nerve Recovery
EMG is also useful for identifying signs of regeneration.
When axons begin to regrow and reconnect with muscle fibers, EMG may show:
- reinnervation potentials
- polyphasic motor unit potentials
These findings indicate that the nerve is beginning to recover. Unlike denervation potentials, which appear spontaneously when the muscle is at rest, signs of reinnervation are usually detected during voluntary muscle contraction. If regeneration has not yet occurred, voluntary contraction produces little or no organized motor unit activity on EMG.
In summary: Repeated EMG studies over time allow physicians to determine whether regeneration is progressing and whether further treatment, including surgery or reoperation, may be necessary. In early stages, EMG typically shows denervation potentials at rest, such as fibrillation potentials and positive sharp waves. As regenerating axons begin to reconnect with muscle fibers, these denervation signals gradually decrease, while new motor unit potentials appear during voluntary contraction, often with a polyphasic shape. The appearance and increasing number of these reinnervation potentials indicate that nerve recovery is underway.
EMG is usually repeated every 2–3 months, and if no signs of recovery appear after about 3–6 months, surgical exploration may be considered.
Electrodiagnostic Testing in Closed Nerve Injuries
In closed nerve injuries (without an open wound), electrodiagnostic testing plays a key role in determining whether recovery is occurring.
Initially, physicians may observe the patient and repeat EMG or ENG after several weeks.
This approach helps determine whether:
- spontaneous recovery is occurring
- the injury is severe and unlikely to recover.
If repeated studies show no evidence of regeneration, surgical exploration may be considered.
Timing of Electrodiagnostic Testing
The timing of EMG and ENG is important.
Immediately after injury, these tests may not yet show abnormalities.
Typical timing is:
- initial evaluation several weeks after injury
- repeat studies after additional weeks or months to monitor recovery.
This allows physicians to determine whether axonal regeneration is occurring.
Why Repeated Studies Are Important
Peripheral nerve injuries evolve over time.
Electrodiagnostic studies are often repeated because they allow physicians to observe:
- whether nerve function is improving
- whether denervation is progressing
- whether regeneration has begun.
This information helps guide decisions about:
- continued observation, when there are signs of spontaneous nerve recovery
- physical therapy and rehabilitation, to preserve muscle function and prevent contractures while the nerve regenerates
- surgical treatment, when electrodiagnostic studies show severe axonal damage or no signs of regeneration over time
Imaging studies
Imaging may include:
- ultrasound
- MRI.
These methods can show:
- nerve discontinuity
- scar compression
- tumors or neuromas.
Nerve Regeneration
Peripheral nerves have the ability to regenerate. After axonal injury, the axon may regrow from the site of damage. The growth rate is approximately: 1 millimeter per day.
However, successful regeneration requires that the regenerating axon finds its original pathway. If the connective tissue tubes are intact, the axon can grow toward its original target. If these structures are destroyed, regeneration may be disorganized.
Motor vs Sensory Nerve Recovery
Motor and sensory nerves differ in their capacity for recovery. Motor nerves must reconnect with motor end plates in muscle fibers. These structures degenerate if they remain without nerve supply for too long. Motor end plates may degenerate after approximately 12–18 months of denervation.
Because of this:
- motor recovery is limited in time
- motor nerves must reconnect with motor end plates in muscle fibers
- if reinnervation occurs too late, motor end plates degenerate and the muscle may no longer respond
Sensory nerves behave differently:
- sensory recovery has a longer time window
- sensory fibers can regenerate even after longer periods without nerve supply
- partial restoration of sensation may occur months or even years after injury
Treatment of Peripheral Nerve Injury
Treatment depends on the type and severity of injury.
Diagnostic Evaluation and Surgical Decision
During diagnostic evaluation, the type of nerve injury is sometimes clear, but in many cases the exact extent of damage becomes evident only during surgery. The decision to operate is usually based on the clinical course of recovery and electrodiagnostic testing (EMG/nerve conduction studies).
Early surgery may be necessary when the nerve is completely severed. In open injuries where the nerve is visibly transected and not repaired at the time of injury, surgical repair should usually be performed as soon as possible rather than waiting for spontaneous recovery.
In closed nerve injuries, physicians may wait several months to see whether spontaneous regeneration occurs. Serial clinical examinations and EMG studies help determine whether recovery is progressing. If there are no signs of regeneration after approximately 3–6 months, surgical exploration is often considered. Even when small signs of recovery appear, careful follow-up is necessary. If recovery is minimal or does not continue to improve, surgical treatment may still be recommended. Surgery should not be delayed indefinitely when motor recovery is unlikely, because motor end plates gradually degenerate over time.
However, the final decision about the type of procedure is often made during surgery itself. If the nerve is found to be intact but compressed by scar tissue, simple decompression or neurolysis may be sufficient. If the internal structure of the nerve is severely damaged, reconstruction may be required, which can include removal of a neuroma and repair of the nerve with direct suturing or with a nerve graft.
When Is Surgery Necessary After Peripheral Nerve Injury — Wait or Operate?
In many patients, the central question is whether the nerve is still capable of recovery or whether surgical repair is required.
When the nerve remains structurally preserved, continued recovery is expected, and the focus is on monitoring progress over time rather than immediate intervention.
Surgery becomes more relevant when there are signs that recovery is not occurring as expected, particularly when function does not improve or when the injury pattern suggests loss of internal nerve continuity.
The most important factor is timing — acting too early may lead to unnecessary surgery, while waiting too long in severe injuries may reduce the chance of functional recovery, especially in motor nerves.
Because the decision depends on injury severity, functional progression, and time course, different specialists may reasonably recommend either continued observation or surgical treatment based on how these factors are interpreted in a specific case.
Conservative Treatment of Nerve Injury
Mild injuries may recover spontaneously.
Treatment may include:
- observation
- physical therapy
- splints
- pain management.
Pain Management After Nerve Injury
After a peripheral nerve injury, especially when sensory nerves are involved, pain may persist even when there is no clear indication for surgery. In these situations, the key question is not whether the nerve was injured, but what is now maintaining the pain.
In many patients, persistent pain is not caused by complete nerve disruption, but by ongoing irritation of the nerve or surrounding structures. This may include:
- local compression of the nerve
- scar-related irritation
- neuroma formation
- hypersensitivity of small nerve branches
At the same time, pain is often influenced by additional contributing factors that are not directly visible on imaging:
- mechanical stress (position, repetitive movements, posture)
- metabolic factors (inflammatory state and diet, glucose metabolism, vitamin deficiencies)
- muscle spasm and surrounding tissue tension
Because of this, treatment cannot be based only on the initial injury.
The key step is to determine:
- which nerve is responsible for the pain
- where along its course the irritation occurs
- what type of mechanism is present
Only then can treatment be properly selected.
In many cases, pain treatment includes a combination of:
- targeted pain management
- correction of contributing mechanical factors
- addressing metabolic and inflammatory influences
- and, when necessary, specific local interventions
In the context of pain management specifically, surgery is considered only when a clear structural problem — such as neuroma or nerve compression — has been identified and cannot be addressed otherwise.
Online pain consultation for pain after nerve injury in detail
How the video consultation works — step by step
See the page “Possible Reasons for Poor Pain Treatment Effectiveness of Pain After Nerve Injury” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
Surgical Treatment of Nerve Injury
Surgery may be required when:
- the nerve is severed
- regeneration does not occur
- scar tissue compresses the nerve.
Surgical options for peripheral nerve injury depend on the type of injury, the degree of nerve damage, and the time elapsed since the injury. Several different surgical techniques may be used.
- Nerve repair (direct nerve suturing)
This procedure is used when the nerve has been cleanly cut and the two ends can be brought together without tension. The surgeon aligns the two ends of the nerve and reconnects them using very fine microsurgical sutures under a microscope.
The goal is to restore the continuity of the nerve fascicles, allowing regenerating axons to grow across the repair site toward their target muscles and sensory receptors.
Direct repair usually provides the best chance of recovery, but it is only possible when the gap between the nerve ends is small. Newer techniques are sometimes used to support nerve repair in selected cases. For small nerve gaps, surgeons may use biological or synthetic nerve conduits (tubular guides) that help direct regenerating axons toward their target. Fibrin glue may also be used to stabilize the repair site or assist microsurgical suturing. - Nerve grafting
When a segment of the nerve has been lost or the gap between the nerve ends is too large, direct suturing is not possible without excessive tension. In these cases, a nerve graft is used to bridge the gap. A small segment of another nerve—often taken from the sural nerve in the leg—is transplanted to connect the two ends of the injured nerve. The graft acts as a biological guiding structure through which regenerating axons can grow.
Recovery may be slower and less predictable than with direct repair, but grafting can restore useful function in many cases. - Neurolysis
Neurolysis is performed when the nerve itself is still intact but is compressed or trapped within scar tissue or fibrotic adhesions. During surgery the surgeon carefully releases the nerve from surrounding scar tissue, allowing it to move freely and restoring normal blood supply. Neurolysis may be useful in cases where nerve recovery has been delayed because of secondary compression after trauma or surgery. - Nerve transfer procedures
When the original nerve cannot recover or when the distance to the target muscle is too long, surgeons may perform a nerve transfer. In this technique, a nearby functioning nerve or one of its branches is redirected to supply the denervated muscle. This allows reinnervation to occur more quickly because the new nerve source is located closer to the muscle.
Nerve transfers are often used in severe injuries of the brachial plexus or major peripheral nerves when conventional repair would not provide adequate recovery. In these procedures, surgeons use nearby functioning nerves as donors, such as branches of the ulnar nerve, median nerve, intercostal nerves, spinal accessory nerve, or parts of the radial nerve, and redirect them to restore critical functions like elbow flexion or shoulder movement.
The choice between these procedures depends on several factors, including the type of nerve injury, the time since the injury, the location of the lesion, and whether signs of spontaneous regeneration are present.
Even after technically successful nerve repair, full recovery cannot be guaranteed. Regenerating axons may not always reach the correct target, recovery may remain incomplete, and prolonged denervation can reduce the ability of muscles to respond even if reinnervation later occurs. For this reason, the realistic goal of surgery is often meaningful functional improvement rather than perfect restoration.
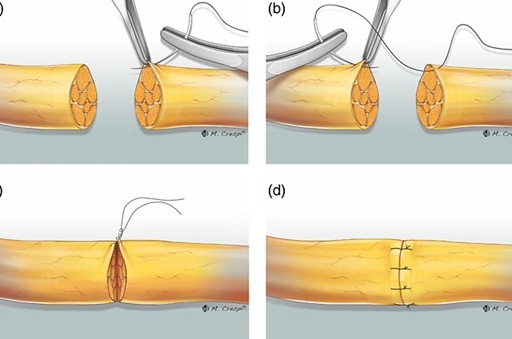
Image: Direct nerve suturing
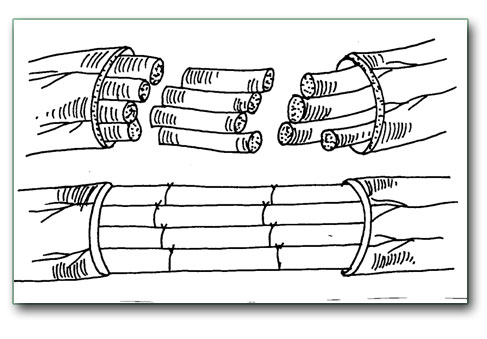
Image: Nerve repair using a nerve graft from another part of the body.
Management of Nerves That Appear Intact but Contain Internal Scarring
During surgery, the nerve may appear continuous from the outside but show a thickened segment. This thickening often represents internal scar tissue or a traumatic neuroma formed after injury.
In some cases, the nerve fibers are still present within the nerve, but they are compressed by a scar within the nerve. When this occurs, surgeons may perform internal neurolysis, carefully removing scar tissue from within the nerve in order to release the preserved fascicles and allow them to function or regenerate.
However, in other cases the thickened segment represents a neuroma in continuity, where most of the internal nerve fibers have already been destroyed and replaced by scar tissue. Although the outer covering of the nerve (epineurium) may still appear intact, detailed dissection sometimes reveals that functional fascicles are no longer present.
During surgery, surgeons may also use intraoperative nerve stimulation or neuromonitoring to evaluate whether functional nerve fibers are still present within a damaged segment.
When this happens, the scarred segment must be removed. The nerve is then reconstructed either by direct repair (suturing the nerve ends) if there is no tension, or by interposition nerve grafts (“cable grafts”) when a gap remains between the nerve ends.
The final decision between internal neurolysis and nerve reconstruction is often made during surgery, after the surgeon evaluates the internal structure of the nerve.
When Immediate Surgery Is More Often Considered
Immediate or early surgical repair is more often considered in open injuries, penetrating wounds, or situations where the nerve has been clearly transected. In contrast, closed injuries without visible nerve discontinuity are often followed with serial clinical examinations and repeated EMG or nerve conduction studies before deciding on surgical exploration. This difference is important because some closed injuries improve spontaneously, while complete transections usually do not.
Rehabilitation After Nerve Injury or Repair
Recovery does not depend only on the nerve itself, but also on rehabilitation. Physical therapy, splinting when needed, prevention of joint stiffness, and maintenance of muscle flexibility are often important while waiting for regeneration. After surgical repair, rehabilitation also aims to protect the repair site and later help the patient retrain movement and sensation as reinnervation begins.
Request Peripheral Nerve Injury Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Being told that a peripheral nerve may be injured often raises important questions:
Will the nerve recover on its own?
How severe is the damage?
Should surgery be considered or is observation still appropriate?
What do EMG findings really mean?
An independent neurosurgical second opinion may help clarify the severity of the nerve injury,
the likelihood of spontaneous recovery, the interpretation of EMG or nerve conduction studies, and whether
observation, rehabilitation, or surgical reconstruction offers the best chance for functional recovery based on
the type of injury, time since trauma, location of the nerve lesion, and the patient’s neurological condition.
- ✔ Send a brief message describing your symptoms and the circumstances of the injury (trauma, surgery, fracture, injection, or compression)
- ✔ You will receive a reply within 24 hours explaining whether an online consultation is appropriate and which documentation is required
- ✔ Priority cases: rapidly progressing weakness, loss of movement, severe neuropathic pain, recent trauma with suspected nerve rupture, or conflicting specialist recommendations — write PRIORITY in your first message
- ✔ EMG reports, nerve conduction studies, MRI or ultrasound images, and other relevant documentation can be reviewed
- ✔ During consultation we explain whether observation, rehabilitation, neurolysis, nerve repair, grafting, or nerve transfer may be appropriate — including expected recovery timelines and up to 10 days of follow-up clarification
Consultation fees typically range from $180–250 depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This corresponds to typical international specialist telehealth neurosurgical second-opinion services.
Emerging and Experimental Therapies in Peripheral Nerve Repair
While observation and surgical repair remain the main treatment options, a number of newer approaches are being actively researched to improve nerve regeneration.
These methods aim to enhance the natural healing process at the molecular and cellular level, but most are still in experimental or early clinical phases.
Molecular and Pharmacologic Therapies
Certain biological factors play a key role in nerve regeneration. Research has focused on molecules such as neurotrophic factors (e.g., BDNF), erythropoietin (EPO), and antioxidants like N-acetylcysteine (NAC), which may support nerve survival, reduce degeneration, and improve regeneration.
However, no pharmacologic therapy is currently approved as a standard treatment for nerve repair.
Stem Cell and Cell-Based Therapies
Stem cells and Schwann cell–based therapies aim to create a more favorable environment for nerve regeneration. Various cell types are being studied, including bone marrow–derived, adipose-derived, and induced pluripotent stem cells.
Although results in experimental models are promising, these treatments remain limited by issues such as cell survival, safety, and potential tumor formation.
Gene Therapy
Gene therapy attempts to enhance nerve regeneration by delivering growth-promoting genes directly to nerve tissue. Early studies show improved axonal growth and functional recovery in experimental models, but clinical application is still limited due to safety concerns and immune responses.
Bioengineering and Nerve Conduits
Advanced materials such as nerve guidance conduits and tissue-engineered scaffolds are designed to guide nerve regeneration and improve outcomes compared to traditional repair techniques. These approaches are increasingly used in selected cases, especially for smaller nerve gaps.
Electrical Stimulation and Implantable Devices
Electrical stimulation of injured nerves has shown the ability to accelerate regeneration and improve functional recovery in both experimental and early clinical studies. However, its role in routine treatment is still evolving.
What This Means for Patients
Many of these therapies are promising, but most are not yet part of standard medical practice.
If you have been offered a “new” or “advanced” treatment, it is important to evaluate:
- whether it is evidence-based
- whether it is widely accepted
- what the realistic outcomes are
An independent second opinion can help clarify whether such treatments are appropriate in your specific case.
Recovery and Prognosis
The outcome of peripheral nerve injury depends on several important factors that influence whether regenerating nerve fibers can reach their target muscles or sensory receptors and restore function.
- Type of injury
The severity and mechanism of nerve damage strongly influence recovery.
In mild injuries where only the myelin sheath is damaged and the axon remains intact (neuropraxia), recovery is usually complete (often >90%) because nerve conduction returns once the myelin regenerates. When the axon is disrupted but the connective tissue structure of the nerve remains preserved (axonotmesis), regeneration is still possible, but it occurs slowly because new axons must grow along the preserved endoneurial tubes. The degree of recovery depends on the distance the axons must regenerate. In the most severe injuries where both the axon and the surrounding connective tissue structures are destroyed (neurotmesis), spontaneous recovery is unlikely without surgical repair because regenerating axons lose their anatomical guidance. - Distance from the muscle or sensory organ
After axonal injury, nerve fibers regenerate at an average rate of approximately 1 millimeter per day.
When the injury occurs far from the target muscle, the regenerating axons must travel a long distance before reaching the muscle fibers.
During this time the muscle may undergo progressive atrophy and degeneration of motor end plates, which reduces the chance of functional recovery.
Injuries closer to the muscle generally have better outcomes, because regenerating axons reach the muscle before irreversible degeneration occurs. - Time to treatment
Timing plays an important role, especially in motor nerve injuries.
If a nerve is completely disrupted and surgical repair is delayed too long, regenerating axons may reach the muscle only after the motor end plates have degenerated. In such cases the muscle may no longer respond even if the nerve regenerates. Early evaluation and appropriate treatment therefore increase the likelihood of meaningful recovery. - Age of the patient
Younger patients usually have better nerve regeneration and greater capacity for functional recovery.
In older individuals, axonal regeneration may be slower and muscles may be less capable of recovering after prolonged denervation. As a result, identical nerve injuries may produce better outcomes in younger patients than in elderly individuals.
Mild injuries may recover completely.
Severe injuries may lead to permanent deficits even after treatment.
Summary: Prognosis is usually better in younger patients, in injuries closer to the target muscle, and when repair can be performed without tension or with a shorter reconstruction segment. Outcomes are often worse in very proximal injuries, long graft repairs, or when treatment is delayed until after prolonged denervation.
Key Treatment Decisions After Peripheral Nerve Injury
After understanding how nerve injuries behave, most patients face a set of practical questions that determine the next step in treatment.
Should I wait for recovery or consider surgery now?
In many nerve injuries, the central question is not whether recovery is possible, but whether continued waiting still makes sense. Early after injury, observation is often appropriate because some degree of spontaneous regeneration can occur. However, if several months pass without meaningful improvement in strength or function, continued waiting may reduce the chances of successful recovery. The decision should be based on clinical progression, not just time alone.
How long is it safe to wait without losing function?
There is no single safe time window that applies to all patients. In general, the first 3–6 months are critical for observing signs of recovery. Beyond this period, especially if there is no clinical or electrophysiological improvement, the risk increases that muscles may no longer respond even if the nerve is later repaired. This is why some specialists recommend earlier surgical evaluation, while others prefer longer observation depending on the case.
Does persistent pain mean the nerve is recovering or getting worse?
Pain after nerve injury is not a reliable sign of recovery. In some situations, it may accompany regeneration, but more often it reflects abnormal nerve signaling, neuroma formation, or hypersensitivity. Persistent or worsening pain without functional improvement may suggest that recovery is not progressing as expected and should prompt reconsideration of the treatment approach.
If EMG shows no improvement, does that mean surgery is necessary?
Electromyography (EMG) is an important tool, but it must be interpreted in context. Lack of reinnervation on EMG after several months can indicate poor spontaneous recovery, but it is not an automatic indication for surgery. The decision depends on how EMG findings correlate with clinical examination, the type of injury, and the expected benefit of surgical treatment in that specific situation.
Can a nerve that looks intact still require surgery?
Yes. A nerve may appear anatomically continuous while still being functionally impaired due to internal structural damage. In such cases, recovery may not occur despite the absence of a visible transection. This is one of the reasons why different specialists may recommend observation or surgery based on how they interpret the same findings.
Is it too late for surgery after several months?
Timing is important but not absolute. Earlier intervention often provides better outcomes, but surgery may still be beneficial even after several months in selected cases. The decision depends on the degree of muscle atrophy, residual function, and the realistic potential for recovery. In some situations, delayed surgery may still improve function or reduce pain, while in others it may no longer provide meaningful benefit.
Peripheral Nerve Injury vs Entrapment Syndromes
Peripheral nerve injuries differ from entrapment syndromes, in which the nerve is gradually compressed by surrounding structures.
Common entrapment syndromes include:
- carpal tunnel syndrome
- cubital tunnel syndrome
- Guyon canal syndrome
- peroneal nerve compression
- meralgia paresthetica
- thoracic outlet syndrome.
These conditions form a related group of disorders affecting peripheral nerves.
Frequently Asked Questions About Peripheral Nerve Injury
What is a peripheral nerve injury?
A peripheral nerve injury occurs when a nerve outside the brain and spinal cord is damaged by trauma, compression, stretching, surgery, injection, fracture, scar tissue, or another mechanical cause. Peripheral nerves carry motor signals to muscles, sensory signals from skin and joints, and autonomic signals that regulate blood vessels and glands. When a nerve is injured, symptoms may include numbness, tingling, burning pain, weakness, loss of movement, or muscle wasting. The severity depends on which parts of the nerve are damaged: the myelin sheath, the axon, or the internal guiding structures that allow regeneration. This is why some nerve injuries recover completely, while others require surgery or leave permanent deficits.
What are the most common causes of peripheral nerve injury?
The most common causes of peripheral nerve injury are trauma, fractures, dislocations, penetrating wounds, stretching injuries, surgical procedures, injections, and delayed compression from scar tissue. Closed trauma may stretch, compress, or crush the nerve even when there is no open wound. Fractures can injure nerves directly through displaced bone fragments or indirectly through traction during the injury. Sharp injuries from glass, knives, or cuts may partially or completely sever the nerve. After trauma or surgery, nerves can later become trapped in fibrosis, adhesions, or scar tissue, causing delayed symptoms. The mechanism matters because a nerve that is only compressed may recover spontaneously, while a severed or internally destroyed nerve usually needs surgical repair or reconstruction.
Can a peripheral nerve injury recover on its own?
A peripheral nerve injury can recover on its own when the internal structure of the nerve remains preserved. In neuropraxia, only the myelin sheath is damaged while the axon stays intact, so recovery is usually complete within weeks or months. In axonotmesis, the axon is disrupted but the microscopic guiding tubes remain intact; recovery is possible, but it is slower because axons must regenerate toward the target muscle or skin. Spontaneous recovery is unlikely in neurotmesis, where the axon and internal guiding structures are destroyed. Closed injuries are often observed with repeated clinical examination and EMG testing, but lack of regeneration after several months may indicate that surgery should be considered.
How fast do peripheral nerves regenerate after peripheral nerve injury?
After axonal peripheral nerve injury, regenerating nerve fibers usually grow at an average rate of about 1 millimeter per day, after an initial delay of roughly 2–3 weeks. This rate is only an approximate guide because recovery depends on the type of injury, distance to the target muscle or skin, age of the patient, blood supply, scar tissue, and whether the internal nerve pathways remain preserved. Injuries closer to the target muscle generally recover better because the regenerating axons have less distance to travel. Very proximal injuries have a worse prognosis because the muscle may lose its motor end plates before the nerve reaches it. This is why timing is critical in motor nerve recovery.
What symptoms suggest a peripheral nerve injury?
Symptoms of peripheral nerve injury depend on which nerve is affected and where the injury occurs. Sensory symptoms may include numbness, loss of sensation, tingling, burning pain, electric shock sensations, or hypersensitivity to touch. Motor symptoms may include weakness, loss of movement, poor grip, foot drop, wrist drop, difficulty climbing stairs, inability to stand on toes, or loss of fine hand function. Over time, muscles supplied by the injured nerve may become visibly smaller or atrophic. Pain may be neuropathic, especially when sensory fibers are damaged or a neuroma forms. The pattern of weakness and sensory loss often helps identify the injured nerve and the approximate level of damage.
Which nerves are most commonly injured in peripheral nerve injury?
Common peripheral nerves injured in the arm include the median, ulnar, and radial nerves. Median nerve injury may affect thumb opposition, grip, fine hand movements, and sensation in the thumb, index, middle, and part of the ring finger. Ulnar nerve injury may cause weakness of finger spreading, reduced grip, clawing of the ring and little fingers, and numbness on the ulnar side of the hand. Radial nerve injury may cause wrist drop and difficulty extending the fingers or thumb. In the leg, commonly injured nerves include the sciatic, peroneal, tibial, and femoral nerves. These may cause foot drop, weakness of plantar flexion, knee extension weakness, sensory loss, and walking difficulty.
How is peripheral nerve injury diagnosed?
Peripheral nerve injury is diagnosed by combining clinical examination, electrodiagnostic studies, and imaging. Clinical examination evaluates the pattern of sensory loss, muscle strength, reflexes, pain distribution, and whether the deficit corresponds to a specific nerve. EMG and nerve conduction studies help determine whether the nerve is conducting impulses, whether axonal damage has occurred, and whether regeneration is appearing over time. Ultrasound and MRI may show nerve discontinuity, scar compression, swelling, neuroma, tumors, or surrounding structural causes. Diagnosis is not based on one test alone. The most important step is to connect symptoms, examination, EMG/ENG findings, imaging, and the mechanism of injury into one coherent explanation.
When is EMG performed after a peripheral nerve injury?
EMG is usually most informative after enough time has passed for denervation changes to appear in the muscles. In the first days after peripheral nerve injury, EMG may still look normal because muscle fibers have not yet developed electrical signs of denervation. After approximately 2–3 weeks, denervated muscles may show fibrillation potentials and positive sharp waves. Repeated EMG and nerve conduction studies are often performed every 2–3 months to monitor whether reinnervation is beginning. New motor unit potentials during voluntary contraction suggest regeneration. If repeated studies show no meaningful recovery after about 3–6 months, especially in a motor nerve injury, surgical exploration may be considered rather than continued observation alone.
What is the difference between neuropraxia, axonotmesis and neurotmesis in peripheral nerve injury?
Neuropraxia, axonotmesis, and neurotmesis describe different severities of peripheral nerve injury. Neuropraxia is the mildest form: the myelin sheath is damaged, but the axon remains intact, so recovery is usually complete. Axonotmesis means the axon is interrupted, but the internal guiding tubes remain preserved. The distal axon degenerates, but new fibers can grow back through these preserved pathways, so recovery is possible but slow. Neurotmesis is the most severe injury: both the axon and the internal guiding structures are destroyed. Regenerating fibers lose their pathway, may form a neuroma, or may fail to reach the target. In real injuries, these patterns may be mixed within the same nerve.
When is surgery necessary for a peripheral nerve injury?
Surgery for peripheral nerve injury is necessary when the nerve is completely severed, when regeneration is not occurring, or when the nerve is compressed by scar tissue or another structure that prevents recovery. Open penetrating injuries with visible nerve transection usually require early repair rather than waiting for spontaneous recovery. Closed injuries are often observed first because some recover spontaneously, but if clinical strength and EMG findings do not improve after several months, surgical exploration may be considered. Surgery is also considered when a neuroma, nerve discontinuity, severe internal scarring, or persistent compression is suspected. The decision depends on injury type, time since injury, neurological function, EMG/ENG findings, imaging, pain mechanism, and recovery trajectory.
When should surgery be considered if EMG shows no recovery after peripheral nerve injury?
Surgery should be considered when repeated EMG and clinical examination show no meaningful evidence of regeneration after a reasonable observation period, especially in motor nerve injuries. In many closed injuries, observation is appropriate during the first weeks or months because spontaneous regeneration may occur. However, if there is no improvement in strength, no developing reinnervation potentials on EMG, and no clinical progression after about 3–6 months, continued waiting may reduce the chance of useful recovery. The decision is not based on EMG alone. It must consider the mechanism of injury, whether the nerve may be continuous, distance to target muscles, severity of weakness, imaging findings, and the time window before motor end plates degenerate.
Can a peripheral nerve look intact but still need surgery?
Yes. A peripheral nerve can appear continuous from the outside but still fail to recover because of internal scarring, neuroma in continuity, or severe damage to the internal fascicles. In some cases, the epineurium, or outer covering of the nerve, remains intact, while the internal guiding structures are partly destroyed or compressed by scar tissue. During surgical exploration, the surgeon may find that the nerve is continuous but thickened. If functional fascicles are preserved, internal neurolysis may help release scar tissue. If the thickened segment contains mostly scar and no useful fibers, the damaged part may need to be removed and reconstructed with direct repair or nerve grafts. This decision is often made during surgery.
What types of surgery are used to repair peripheral nerve injury?
Several surgical techniques may be used to treat peripheral nerve injury, depending on the type of damage and time since injury. Direct nerve repair is used when a cleanly cut nerve can be reconnected without tension. Nerve grafting is used when a segment of nerve is missing and the gap is too large for direct suturing; the graft acts as a biological guide for regenerating axons. Neurolysis is used when the nerve remains intact but is trapped or compressed by scar tissue. Nerve transfer is used when the original nerve cannot recover in time, or the distance to the target muscle is too long. The goal is meaningful functional improvement, not always perfect restoration.
What is neurolysis in peripheral nerve injury surgery?
Neurolysis is a surgical procedure used when a peripheral nerve is still anatomically continuous but is compressed, trapped, or tethered by scar tissue or fibrotic adhesions. The surgeon carefully releases the nerve from surrounding scar tissue to restore mobility, reduce mechanical irritation, and improve blood supply. In some cases, internal neurolysis may be performed when scar tissue is present inside the nerve and preserved fascicles can still be separated and decompressed. Neurolysis is different from nerve repair or grafting because the nerve is not cut and reconstructed unless the internal structure is found to be severely destroyed. It may be useful after trauma or surgery when recovery has stalled because scar compression prevents normal regeneration or function.
What is the difference between nerve repair, nerve grafting and nerve transfer after peripheral nerve injury?
Nerve repair, nerve grafting, and nerve transfer are different ways to restore nerve function after peripheral nerve injury. Direct nerve repair reconnects two cut nerve ends when they can be brought together without tension. Nerve grafting is used when there is a gap; a segment of another nerve, often the sural nerve, bridges the distance and provides a pathway for axons. Nerve transfer uses a nearby functioning nerve branch and redirects it to a denervated muscle, allowing reinnervation to begin closer to the target. This can be useful in severe brachial plexus or major nerve injuries when conventional repair would take too long. The choice depends on gap length, injury level, time delay, and target muscle viability.
How long can muscles survive without nerve supply after peripheral nerve injury?
Muscles can survive without nerve supply only for a limited time if meaningful motor recovery is expected. After motor nerve injury, the muscle fibers and motor end plates gradually lose their ability to respond to reinnervation. Motor end plates may degenerate after about 12–18 months of denervation. If regenerating axons arrive too late, the nerve may technically grow, but the muscle may no longer respond effectively. This is why proximal nerve injuries have a worse prognosis: regenerating axons must travel a long distance at roughly 1 millimeter per day. Sensory recovery has a longer window, but motor recovery is time-sensitive. Surgical decisions must therefore balance observation against the risk of missing the motor recovery window.
Is it too late for peripheral nerve surgery after several months?
It is not automatically too late for peripheral nerve surgery after several months, but timing becomes increasingly important. In closed nerve injuries, several months of observation may be appropriate if there are clinical or EMG signs of recovery. If there is no meaningful improvement after about 3–6 months, surgical exploration is often considered. Delayed surgery may still help selected patients, especially when neurolysis can release scar compression or when reconstruction can still reach useful targets. However, the chance of motor recovery decreases as muscles remain denervated and motor end plates degenerate. The decision depends on residual function, muscle atrophy, distance to the target, EMG evidence, injury type, and realistic goals of surgery.
Can a peripheral nerve injury cause chronic pain?
Yes. Peripheral nerve injury can cause chronic neuropathic pain, especially when sensory fibers are irritated, partially damaged, trapped in scar tissue, or form a neuroma. Patients may feel burning pain, electric shocks, hypersensitivity, deep aching, or pain triggered by pressure over the injured nerve. Persistent pain is not always caused by complete nerve disruption. It may result from ongoing irritation, local compression, scar-related tethering, small nerve branch hypersensitivity, or abnormal pain processing. Mechanical stress, repetitive movement, posture, muscle spasm, inflammatory state, glucose metabolism, vitamin deficiencies, and central sensitization may also maintain symptoms. Treatment should identify which nerve is responsible, where the irritation occurs, and whether surgery or targeted pain management is appropriate.
What determines the prognosis after peripheral nerve injury?
Prognosis after peripheral nerve injury depends on injury type, preservation of internal nerve structure, distance to the target muscle or skin, timing of treatment, age, and whether regeneration is documented. Neuropraxia usually has an excellent prognosis because the axon remains intact. Axonotmesis can recover if the guiding tubes are preserved, but recovery is slow. Neurotmesis has the worst prognosis without repair because regenerating axons lose their pathway. Injuries closer to the target muscle recover better than proximal injuries because axons have less distance to grow. Younger patients generally recover better than older patients. Delayed treatment, long grafts, severe crush injury, muscle atrophy, and prolonged denervation reduce the chance of full recovery.
Can I obtain an online second opinion for peripheral nerve injury?
Yes. An online second opinion can help when a peripheral nerve injury is suspected or confirmed and there is uncertainty about severity, prognosis, EMG findings, recovery, or surgery. Medical reports, EMG and nerve conduction studies, ultrasound or MRI findings, operative notes, and the history of trauma, fracture, injection, compression, or surgery can be reviewed. The goal is to clarify whether the nerve may recover spontaneously, whether repeated EMG monitoring is enough, or whether neurolysis, direct repair, grafting, or nerve transfer should be considered. A second opinion is especially useful when several months have passed without meaningful recovery, pain is severe, weakness is progressing, or different specialists recommend different approaches. Urgent progressive deficits still require local in-person care.