Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Carpal Tunnel Syndrome — Median Nerve Compression
Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
August 01, 2026
Who This Carpal Tunnel Syndrome Page Is For
This page is intended for patients who have developed numbness, tingling, or weakness in the thumb, index finger, middle finger, or part of the ring finger, especially when carpal tunnel syndrome or median nerve compression at the wrist has been suspected or diagnosed.
If symptoms worsen during repetitive hand use, computer work, or at night — or if previous examinations suggest compression of the median nerve within the carpal tunnel — understanding the possible causes, typical course of the condition, and available treatment options may help guide decisions about further evaluation and management. In complex or persistent cases, an individualized neurosurgical second opinion may help clarify the diagnosis and treatment strategy.
When patients seek a second opinion for carpal tunnel syndrome
• Persistent numbness or tingling in the thumb, index, or middle fingers
• Symptoms worsen at night or during repetitive hand activities
• It is unclear whether the symptoms originate from median nerve compression at the wrist or from cervical spine disorders
• Conservative treatment such as splints or medication has not improved symptoms over several months
• Weakness of the hand or frequent dropping of objects affecting daily activities
• Uncertainty whether surgical decompression of the median nerve (carpal tunnel release) should be considered
If your symptoms persist or the diagnosis and treatment options remain unclear, you may request an individualized neurosurgical review here:
Request Second Opinion
Contents
- Who this page is for
- Definition
- Median nerve anatomy
- Who is at Risk
- Causes of compression
- Symptoms
- Diagnosis
- Similar conditions
- Operate or not
- Conservative treatment
- Surgical treatment
- Surgical complications
- Request second opinion
- Prognosis and recovery
- Symptoms after surgery
- Contributing factors for pain in CTS
- Specialist evaluation
- FAQs
What Is Carpal Tunnel Syndrome
Carpal tunnel syndrome is the most common nerve compression disorder of the hand, caused by pressure on the median nerve as it passes through the carpal tunnel at the wrist.
The median nerve passes through a narrow anatomical passage in the wrist called the carpal tunnel, which is formed by wrist bones and a strong ligament known as the transverse carpal ligament.
When the space inside the tunnel becomes narrowed or when surrounding tissues swell, pressure on the median nerve increases. This compression may lead to numbness, tingling, pain, or weakness in the hand and fingers, especially affecting the thumb, index finger, middle finger, and part of the ring finger.
Because the median nerve also controls several muscles responsible for thumb movement and grip strength, prolonged compression may eventually affect hand function.
Symptoms often develop gradually but may worsen during repetitive hand movements, prolonged wrist flexion, or nighttime sleep.
Read more about nerve injuries and other nerve entrapments on this page: https://neurohirurgija.in.rs/en/peripheral-nerve-injury/
Anatomy of the Median Nerve at the Wrist
The median nerve originates from the brachial plexus, primarily from nerve roots C5–T1. It travels down the arm and forearm before entering the wrist through the carpal tunnel, a narrow passage located at the base of the palm.
The carpal tunnel contains:
• the median nerve
• several flexor tendons that bend the fingers
Because this tunnel has limited space, any swelling of tendons, inflammation, or structural narrowing may increase pressure on the median nerve. This explains why conditions that cause tissue swelling or repetitive wrist motion can increase the risk of carpal tunnel syndrome.
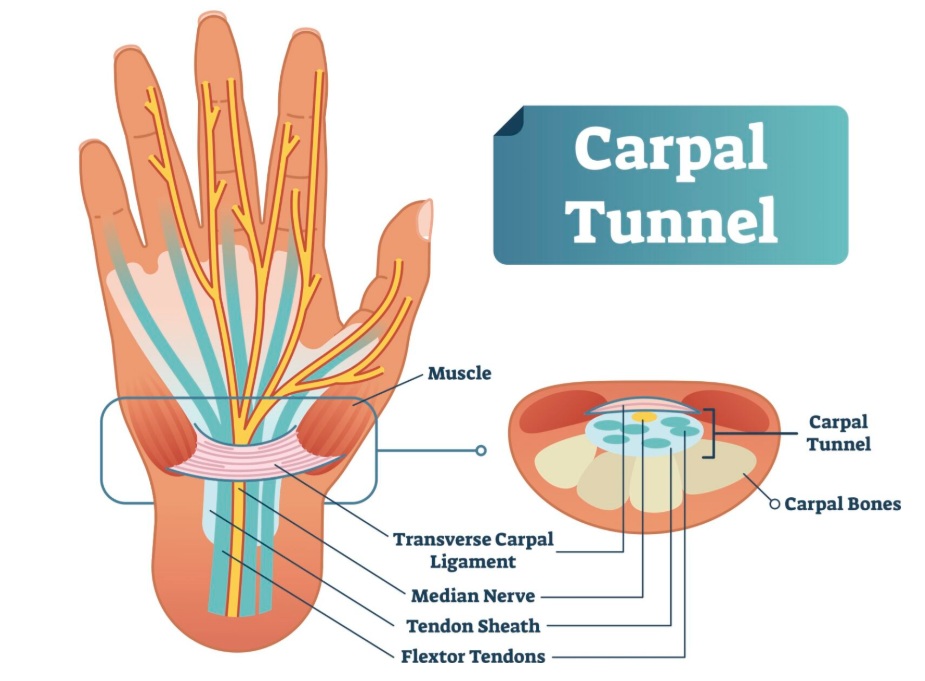
Image: Anatomy of the carpal tunnel and the relationship of the median nerve to other anatomical structures, including the transverse carpal ligament and flexor tendons.
Who Is at Risk for Carpal Tunnel Syndrome
Carpal tunnel syndrome is the most common nerve compression disorder of the upper extremity and affects people of all ages, though it is significantly more common in women than in men. It occurs most frequently in middle-aged and older adults, although it can develop at any age.
Certain groups are at higher risk, including:
- Women, who develop carpal tunnel syndrome approximately three times more often than men
- Pregnant women, due to fluid retention and hormonal changes that increase pressure within the carpal tunnel — symptoms often resolve after delivery
- Older adults, in whom age-related changes in tendons and ligaments may narrow the tunnel over time
- Patients with diabetes, thyroid disorders, or rheumatoid arthritis, which affect nerve vulnerability and tissue inflammation
- Workers performing repetitive or forceful hand and wrist movements in occupational settings
In many patients, more than one of these factors is present simultaneously.
Why the Median Nerve Becomes Compressed
Several factors may increase pressure on the median nerve within the carpal tunnel.
Common causes include:
• Repetitive manual labor and wrist movements are proven risks (evidence fails to confirm a clear link between carpal tunnel syndrome and keyboard work alone)
• Hand-intensive occupations
• Wrist injuries or fractures
• Thickening of the transverse carpal ligament
• Ganglion cysts or other space-occupying lesions arising from the wrist joint or tendon sheaths
• Inflammatory conditions such as rheumatoid arthritis
• Pregnancy-related swelling
• Diabetes or metabolic disorders affecting nerve vulnerability
Systemic amyloidosis — carpal tunnel syndrome is sometimes an early manifestation of systemic amyloid disease, particularly in older patients. In patients undergoing carpal tunnel surgery, studies have found amyloid deposits in the tendon tissue around the median nerve in approximately 10% of cases, which in some patients leads to a diagnosis that changes their overall medical treatment. For this reason, in older patients with carpal tunnel syndrome and additional risk factors such as heart disease or unexplained weakness, further evaluation for systemic amyloidosis may be appropriate.
In many patients, multiple contributing factors are present.
Symptoms of Carpal Tunnel Syndrome
Symptoms usually affect the thumb, index finger, middle finger, and part of the ring finger.
Common symptoms include:
• Numbness or tingling in the fingers
• Burning or electric-like sensations in the hand
• Pain that may radiate toward the forearm
• Weak grip strength
• Difficulty holding objects
• Frequent dropping of items
• Symptoms that worsen at night
Carpal tunnel symptoms are often most noticeable at night. Many patients wake up with numbness, tingling, or burning sensations in the hand and fingers. Shaking or moving the hand may temporarily relieve these symptoms. In more advanced cases, muscle weakness and wasting of the thumb muscles may occur.
How Carpal Tunnel Syndrome Is Diagnosed
Diagnosis usually begins with clinical examination and evaluation of symptoms.
During examination, the doctor may identify:
• Reduced sensation in the median nerve distribution
• Weakness of thumb muscles
• Atrophy of the thenar muscles (visible thinning of the muscle at the base of the thumb) in advanced cases
• Reproduction of symptoms when tapping the nerve at the wrist (Tinel sign)
• Symptoms triggered by wrist flexion (Phalen test)
Carpal tunnel syndrome can often be diagnosed based on symptoms and physical examination alone, using a structured clinical scoring system called CTS-6. Current evidence supports this approach as an alternative to routine nerve conduction studies or ultrasound in patients with a typical clinical presentation. Additional testing is recommended when the diagnosis is uncertain or when symptoms may have another cause.
Additional tests may include:
• Nerve conduction studies (EMG) to confirm median nerve compression
• Ultrasound to visualize nerve swelling
• MRI in selected cases to evaluate surrounding structures. MRI is generally not recommended for the routine diagnosis as current evidence demonstrates limited diagnostic accuracy compared to clinical assessment and electrodiagnostic testing.
• Cervical spine imaging when symptoms may originate from the neck
In older patients with carpal tunnel syndrome undergoing surgical release, analysis of tenosynovial tissue for amyloid deposits may be considered when multiple risk factors for systemic amyloidosis are present, as carpal tunnel syndrome is sometimes an early manifestation of this condition.
These tests help confirm the diagnosis and exclude other causes.
Conditions That Can Mimic Carpal Tunnel Syndrome
Several disorders may produce symptoms similar to median nerve compression.
These include:
• Cervical radiculopathy
• Peripheral neuropathy
• Pronator syndrome (median nerve compression in the forearm)
• Ulnar nerve compression at the elbow or wrist
• Tendon disorders of the wrist
• Thoracic outlet syndrome (brachial plexus or vascular compression near the shoulder and neck region)
Careful clinical evaluation usually distinguishes these conditions.
When Is Surgery Necessary in Carpal Tunnel Syndrome — Continue Conservative Treatment or Operate?
In a substantial number of cases, the key question is whether symptoms will improve with continued conservative treatment or whether surgical decompression is needed. When symptoms are mild, intermittent, or improving, especially with splinting or activity modification, continued non-surgical treatment is usually appropriate. Surgery becomes more likely when symptoms are persistent over time, when numbness becomes constant, or when weakness or muscle wasting develops, suggesting more advanced nerve compression.
The most important factor is timing — performing surgery too early may not be necessary in milder cases, while delaying surgery in more severe or progressive compression may increase the risk of incomplete recovery.
Because this decision depends on symptom severity, duration, and clinical findings, different specialists may reasonably recommend either continued conservative treatment or surgical release based on how these factors are interpreted in an individual case.
Conservative Treatment
Many patients improve with non-surgical treatment.
Common approaches include:
- Activity modification and ergonomic adjustment
- Avoiding repetitive wrist strain
- Wrist splints, especially during sleep
- Anti-inflammatory medications
- Medications for neuropathic pain
- Physical therapy and nerve-gliding exercises
- Corticosteroid injections in selected cases — injections may provide meaningful and lasting relief when inflammation rather than fixed mechanical compression is the dominant cause of symptoms. In patients where ongoing compression is the primary mechanism, injections typically offer only short-term improvement without long-term benefit.
- Platelet-rich plasma (PRP) injection is sometimes offered as an alternative treatment, but current high-quality evidence does not support its long-term effectiveness for carpal tunnel syndrome.
When symptoms are mild or moderate, these measures often lead to gradual improvement.
Surgical Treatment in Persistent Cases
Surgery may be recommended when symptoms remain severe or progressive despite conservative treatment.
The most common surgical procedure is carpal tunnel release. During this operation, the surgeon divides the transverse carpal ligament, which increases the space within the tunnel and relieves pressure on the median nerve.
Today, carpal tunnel surgery is most often performed using one of two approaches:
–Mini-open release — a small incision of approximately 3 cm is made in the palm, limited to the area over the transverse carpal ligament and not extending across the wrist crease. This is the most widely used technique.
–Endoscopic release — the ligament is divided through one or two small portals using a camera-guided instrument, without a visible palm incision.
– Ultrasound-guided release — a newer minimally invasive technique in which the transverse carpal ligament is divided through a very small skin opening using a specially designed instrument, such as a protected microblade or hook knife, while the median nerve and surrounding structures are continuously visualized with ultrasound. Potential complications include incomplete ligament release and injury to the median nerve, its branches, or nearby blood vessels.
Current high-quality evidence shows no difference in long-term outcomes between mini-open and endoscopic carpal tunnel release. Endoscopic technique may allow a slightly faster return to work in some patients, but may also carry a somewhat higher risk of complications. The choice of technique depends on the surgeon’s training and experience, as well as individual patient factors. Both techniques aim to achieve the same goal: complete release of the transverse carpal ligament to relieve pressure on the median nerve.
This procedures aims to restore nerve function and gradually improve sensation and hand strength.
Surgical treatment is usually recommended when there is:
• Persistent numbness
• Progressive hand weakness
• Muscle wasting of the thumb muscles
• Electrodiagnostic confirmation of nerve compression
Early mobilization is generally preferred after surgery. Current evidence does not support routine immobilization through splinting or bracing after carpal tunnel release. Routine supervised physical therapy after carpal tunnel release is not supported by current evidence for most patients, although selected individuals may benefit on a case-by-case basis. For postoperative pain management NSAIDs and acetaminophen are currently recommended over opioid medications based on high-quality evidence.
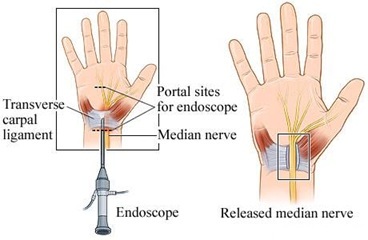
Image: Carpal tunnel release surgery aims to relieve pressure on the median nerve by cutting the ligament. This can be achieved using a traditional mini-open incision or a minimally invasive endoscopic technique.
Possible Complications and Surgical Risks
Carpal tunnel release is generally considered a safe and commonly performed procedure. However, as with any surgical intervention, certain complications may occur, although they are relatively uncommon.
These may include:
Wound healing problems (dehiscence)
In some cases, the surgical wound may heal more slowly or partially reopen, especially in patients with impaired healing capacity.
Infection
Postoperative infection is uncommon but may require additional treatment if it occurs.
Injury to sensory nerve branches
Small sensory branches in the palm may be affected during surgery, which can lead to localized numbness, tingling, or scar-related pain.
Motor branch involvement
In rare cases, the motor branch of the median nerve that supplies the thenar muscles may be affected, potentially leading to weakness of thumb movement.
Scar-related discomfort
Some patients may experience pain or sensitivity at the surgical site, especially during pressure or use of the hand.
Most of these complications are uncommon, and in many cases symptoms improve over time. It is important to distinguish these situations from more frequent causes of persistent symptoms, such as incomplete decompression, unrecognized diagnoses, or contributing factors affecting nerve recovery.
Request Carpal Tunnel Syndrome Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Persistent numbness, tingling, or weakness in the thumb, index, or middle fingers may raise several important questions:
Is this really carpal tunnel syndrome?
Could the symptoms come from the cervical spine or another nerve disorder?
Should treatment remain conservative or should surgical decompression be considered?
Why are the symptoms lasting longer than expected?
An independent neurosurgical second opinion may help clarify the cause of median nerve compression at the wrist,
confirm whether the symptoms correspond to carpal tunnel syndrome or another condition,
and determine whether conservative treatment, wrist splinting, injections, or surgical decompression
offers the best approach based on the duration of symptoms, neurological findings, and previous treatments.
- ✔ Send a brief message describing your symptoms, when they began, and whether you experience numbness, tingling, or weakness in the hand
- ✔ You will receive a reply within 24 hours explaining whether an online consultation is appropriate and which documentation is required
- ✔ Priority cases: progressive hand weakness, muscle wasting at the base of the thumb, or worsening numbness despite previous treatment — write PRIORITY in your first message
- ✔ Previous medical reports, EMG studies, cervical spine imaging, and wrist imaging can be reviewed
- ✔ During consultation we explain whether observation, splinting, physical therapy, injections, or surgical decompression may be appropriate — including expected recovery timelines and up to 10 days of follow-up clarification
Consultation fees typically range from $180–250 depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This corresponds to typical international specialist telehealth neurosurgical second-opinion services.
Prognosis and Recovery
The prognosis depends largely on how long the nerve has been compressed.
When carpal tunnel syndrome is diagnosed early, many patients improve with conservative treatment.
If compression persists for a long time, recovery may take longer.
After surgical decompression, improvement usually occurs gradually over several months as the nerve recovers.
Why Symptoms May Persist After Carpal Tunnel Surgery
In a significant number of patients, symptoms such as numbness, tingling, or pain may persist even after technically successful carpal tunnel release. This does not necessarily mean that the procedure was unsuccessful. In many cases, the operation correctly relieves pressure on the median nerve, but symptoms continue because the dominant pain mechanism has not been fully identified or additional contributing factors remain unaddressed.
Effective treatment depends on clearly defining which anatomical structure is responsible for symptoms, what pathological process is occurring within that structure, and which contributing factors are maintaining nerve sensitivity over time. When any of these elements remain unclear, improvement after surgery may be partial or delayed.
Unrecognized Alternative or Overlapping Diagnoses
In some patients, the underlying cause of symptoms may not have been fully identified before surgery. Although carpal tunnel syndrome is one of the most common causes of hand numbness and tingling, several other conditions may produce similar symptoms. These conditions are outlined in the section “Conditions That Can Mimic Carpal Tunnel Syndrome.” If one of these alternative diagnoses is present — either alone or in combination with median nerve compression — surgical decompression at the wrist may not lead to full symptom resolution.
Double Crush Syndrome and Multi-Level Nerve Involvement
In some patients, the same nerve may be affected at more than one level. For example, compression in the cervical spine combined with compression at the wrist may lead to persistent symptoms even after local decompression.
If only one site of compression is treated, symptoms may improve only partially. This is one of the most common reasons why patients report incomplete recovery despite technically adequate surgery.
Pre-existing Nerve Damage and Recovery Limitations
When nerve compression has been present for a long time, the median nerve may already be affected by chronic structural and functional changes. In such cases, even after decompression, recovery may be slow or incomplete. This is not a failure of the procedure, but rather a reflection of limited nerve recovery capacity.
Scar Tissue and Local Postoperative Factors
In some cases, scar tissue (fibrosis) may develop around the median nerve after surgery. This may contribute to ongoing irritation or reduced nerve mobility. Although less common, this may explain persistent or recurrent symptoms in selected patients.
Technical Factors Related to Surgical Outcome
In some cases, persistent symptoms may be related to technical aspects of the surgical procedure itself, even when surgery was performed according to standard principles.
One of the most important factors is incomplete decompression of the transverse carpal ligament, where residual pressure on the median nerve remains. Even a small portion of the ligament left intact may continue to compress the nerve and limit recovery. In other cases, variations in surgical technique, limited exposure, or anatomical differences may influence how effectively the nerve is released.
Although uncommon, direct irritation of the nerve, postoperative swelling, or local tissue changes may also contribute to persistent symptoms.
It is important to emphasize that these situations are less frequent than causes such as unrecognized diagnoses, multi-level nerve involvement, or contributing factors, but they should be considered when symptoms do not improve as expected.
Misinterpretation of the Dominant Pain Mechanism
In certain patients, symptoms are influenced not only by peripheral nerve compression, but also by central sensitization or altered pain processing. In these cases, the nervous system continues to amplify pain signals even after mechanical compression has been relieved. Because of this, decompression alone may not fully resolve symptoms if pain processing mechanisms remain active.
Contributing Factors That May Maintain Symptoms After Surgery
Frequently observed in patients, persistent symptoms are not caused only by the original nerve compression, but also by additional factors that maintain or amplify nerve sensitivity.
These factors rarely represent the primary cause, but they may significantly influence recovery:
Central sensitization — the nervous system remains hypersensitive and amplifies pain signals
Metabolic and systemic factors — diabetes, insulin resistance, and chronic inflammation-diet may impair nerve recovery
Nutritional factors — deficiencies in vitamin B12, vitamin D, or magnesium may affect nerve function
Mechanical factors — continued repetitive wrist use or inadequate ergonomic adaptation may maintain irritation
Sleep disturbance — poor sleep increases pain perception and reduces recovery capacity
Stress and nervous system reactivity — increased sensitivity may maintain symptoms even without ongoing compression
What Should Be Re-evaluated When Symptoms Persist
When symptoms continue after surgery, the most important step is not to repeat treatment blindly, but to reassess the underlying mechanism.
This includes confirming:
- whether the median nerve at the wrist remains the primary source of symptoms
- whether another anatomical level or condition is involved
- whether contributing factors are maintaining symptoms
In many patients, different aspects of the condition have already been treated individually. However, lasting improvement usually requires a comprehensive approach based on a clearly defined mechanism of symptoms.
Online pain consultation for pain after carpal tunnel surgery in detail
How the video consultation works — step by step
See the page “Possible Reasons for Poor Pain Treatment Effectiveness of Pain After Nerve Surgery” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
When to Seek Specialist Evaluation
Medical evaluation is recommended if:
• Numbness in the hand persists for several months
• Hand weakness develops
• Objects are frequently dropped
• Symptoms interfere with daily activities
• The diagnosis remains uncertain
Early specialist evaluation may help prevent permanent nerve damage.
Frequently Asked Questions About Carpal Tunnel Syndrome
What is carpal tunnel syndrome?
Carpal tunnel syndrome is compression of the median nerve at the wrist. The median nerve passes through a narrow passage called the carpal tunnel, together with the flexor tendons that bend the fingers. The tunnel is formed by the wrist bones and the transverse carpal ligament. When the space inside the tunnel becomes too narrow, or when the surrounding tissues swell, pressure on the median nerve increases. This can cause numbness, tingling, burning pain, and weakness in the thumb, index finger, middle finger, and part of the ring finger. Because the median nerve also controls important thumb muscles, long-standing compression may affect grip, pinching, and fine hand function.
What are the most common symptoms of carpal tunnel syndrome?
The most common symptoms of carpal tunnel syndrome are numbness, tingling, burning, or electric-like sensations in the thumb, index finger, middle finger, and part of the ring finger. Many patients notice symptoms at night and may wake up needing to shake or move the hand for relief. Pain may radiate into the forearm, especially after repetitive wrist use or prolonged wrist flexion. As median nerve compression progresses, hand strength may decrease, objects may be dropped more often, and fine tasks may become more difficult. In advanced cases, the muscles at the base of the thumb may weaken or waste, causing visible flattening and reduced thumb opposition. Persistent numbness or weakness suggests more advanced nerve involvement.
What causes median nerve compression in the carpal tunnel?
Median nerve compression in the carpal tunnel occurs when pressure rises inside the narrow wrist passage. This may happen because of repetitive or forceful hand use, swelling of flexor tendons, thickening of the transverse carpal ligament, wrist injuries or fractures, ganglion cysts, rheumatoid arthritis, pregnancy-related fluid retention, diabetes, thyroid disease, or other metabolic factors that make nerves more vulnerable. In many patients, several factors act together. Keyboard work alone is not always a proven direct cause, but hand-intensive occupations and repetitive forceful wrist movements can contribute. The important point is that the median nerve becomes compressed in a fixed anatomical space, and symptoms depend on the duration, severity, and biological vulnerability of the nerve.
Is carpal tunnel syndrome dangerous?
Carpal tunnel syndrome is not usually dangerous in a life-threatening sense, but it can become functionally serious if median nerve compression is persistent or progressive. Mild intermittent symptoms may improve with splinting, activity modification, medication, or injection therapy. The concern is long-standing compression that leads to constant numbness, weakness, frequent dropping of objects, or wasting of the thenar muscles at the base of the thumb. Once motor weakness and muscle atrophy develop, recovery may be slower or incomplete even after surgery. This is why the timing of treatment matters. Surgery too early may be unnecessary in mild cases, but delaying decompression in severe cases may increase the risk of permanent nerve dysfunction.
Can carpal tunnel syndrome improve without surgery?
Yes. Carpal tunnel syndrome can improve without surgery when symptoms are mild, intermittent, recent, or clearly related to temporary swelling or activity. Conservative treatment may include wrist splints, especially during sleep, activity modification, ergonomic adjustment, avoiding repetitive wrist strain, anti-inflammatory medication, medication for neuropathic pain, physical therapy, nerve-gliding exercises, and in selected cases corticosteroid injection. Conservative treatment is more likely to help when there is no constant numbness, no progressive weakness, and no thenar muscle wasting. In pregnancy-related carpal tunnel syndrome, symptoms often improve after delivery as fluid retention decreases. Surgery becomes more likely when symptoms persist for months, worsen despite treatment, or when nerve tests and examination show significant median nerve dysfunction.
How is carpal tunnel syndrome diagnosed?
Carpal tunnel syndrome is diagnosed by combining symptoms, clinical examination, and selected tests when needed. Typical symptoms include numbness or tingling in the thumb, index, middle, and part of the ring finger, often worse at night. Examination may show reduced sensation, weakness of thumb muscles, thenar atrophy, reproduction of symptoms with tapping over the median nerve, or symptoms triggered by wrist flexion. A structured clinical scoring system such as CTS-6 may support diagnosis in typical cases. EMG and nerve conduction studies can confirm median nerve compression and grade severity. Ultrasound can show nerve swelling. MRI is not usually needed for routine diagnosis but may help when a mass, cyst, or unusual structure is suspected.
What treatments are available for carpal tunnel syndrome?
Treatment for carpal tunnel syndrome depends on severity, duration, clinical findings, and response to previous care. Mild or moderate cases often begin with conservative measures: night splints, activity modification, ergonomic changes, avoiding repetitive wrist strain, anti-inflammatory medication, neuropathic pain medication, physical therapy, nerve-gliding exercises, and corticosteroid injection in selected cases. Injection may provide meaningful relief when inflammation and swelling are important, but it may be only temporary if fixed mechanical compression is dominant. PRP is sometimes offered, but current high-quality evidence does not support long-term effectiveness. Surgery is considered when symptoms are severe, progressive, persistent despite conservative treatment, or when there is constant numbness, weakness, thenar atrophy, or electrodiagnostic confirmation of significant compression.
When is surgery recommended for carpal tunnel syndrome?
Surgery for carpal tunnel syndrome is recommended when median nerve compression is severe, progressive, or unlikely to improve with continued conservative treatment. Important signs include persistent numbness, constant sensory loss, progressive weakness, frequent dropping of objects, difficulty with thumb opposition, visible thenar muscle wasting, or significant abnormalities on EMG and nerve conduction studies. Surgery may also be considered when symptoms remain disabling after several months of splinting, medication, injections, or activity modification. The operation is called carpal tunnel release and involves dividing the transverse carpal ligament to increase space for the median nerve. Timing is important because delaying surgery in advanced compression can reduce the chance of full nerve and muscle recovery.
Can carpal tunnel syndrome cause permanent nerve damage?
Carpal tunnel syndrome can cause permanent nerve damage if compression of the median nerve is severe or prolonged. Early symptoms may be intermittent and mainly sensory, such as tingling or night numbness. Over time, pressure inside the carpal tunnel can impair nerve blood flow and conduction. Constant numbness, reduced sensation, hand weakness, and thenar muscle atrophy suggest more advanced nerve involvement. Once the muscles controlled by the median nerve have weakened or wasted, recovery may remain incomplete even after technically successful decompression. This does not mean that every patient needs early surgery, but it means that persistent or progressive symptoms should be evaluated carefully. Treatment decisions should balance the chance of spontaneous improvement against the risk of irreversible nerve dysfunction.
Can symptoms persist after carpal tunnel surgery?
Yes. Symptoms can persist after carpal tunnel surgery, and this does not always mean that the operation was unsuccessful. If the median nerve was compressed for a long time, it may already have chronic structural or functional damage, so recovery can be slow or incomplete. Symptoms may also persist when another diagnosis was present before surgery, such as cervical radiculopathy, pronator syndrome, peripheral neuropathy, ulnar nerve compression, tendon disorder, or thoracic outlet syndrome. In some cases, postoperative scar tissue, nerve irritation, incomplete decompression of the transverse carpal ligament, swelling, or altered pain processing may contribute. Persistent symptoms should lead to reassessment of the mechanism, not automatic repeat surgery.
Why do symptoms remain after carpal tunnel surgery?
Symptoms may remain after carpal tunnel surgery for several reasons. The median nerve may have been compressed long enough that recovery capacity is limited, especially if thenar weakness or atrophy was present before surgery. Another disorder may also be responsible for part of the symptoms, such as cervical radiculopathy, peripheral neuropathy, pronator syndrome, ulnar nerve compression, or thoracic outlet syndrome. Double crush syndrome can occur when the same nerve pathway is affected at more than one level. Local causes include scar tissue around the nerve, postoperative swelling, residual compression from incomplete ligament release, or direct nerve irritation. Central sensitization, diabetes, insulin resistance, chronic inflammation, nutritional deficiency, poor sleep, stress, and ongoing wrist strain may also maintain symptoms.
What should be done if symptoms persist after carpal tunnel surgery?
If symptoms persist after carpal tunnel surgery, the first step is to reassess the underlying mechanism rather than repeat treatment blindly. The doctor should determine whether the median nerve at the wrist remains the primary source, whether the transverse carpal ligament was completely released, and whether scar tissue, nerve irritation, or postoperative swelling is contributing. Other anatomical levels and conditions should be reconsidered, including cervical radiculopathy, pronator syndrome, peripheral neuropathy, ulnar nerve compression, tendon disorders, or thoracic outlet syndrome. EMG, nerve conduction studies, ultrasound, or cervical imaging may be useful depending on the case. Contributing factors such as diabetes, insulin resistance, nutritional deficiencies, inflammation, sleep disturbance, stress, and repetitive wrist strain may also need correction.
Can I obtain an online consultation for carpal tunnel syndrome?
Yes. An online consultation can help when carpal tunnel syndrome is suspected, symptoms persist, or treatment decisions remain unclear. During consultation, symptoms can be reviewed in detail, including numbness in the thumb, index, middle, or ring finger, night symptoms, hand weakness, frequent dropping of objects, and response to splints, injections, medication, or previous surgery. EMG reports, nerve conduction studies, ultrasound, MRI, cervical spine imaging, and operative notes can also be reviewed. The goal is to clarify whether symptoms truly fit median nerve compression at the wrist, whether another diagnosis may be involved, and whether continued conservative treatment or carpal tunnel release should be considered. Progressive weakness or thenar muscle wasting deserves priority specialist evaluation.
Why are carpal tunnel syndrome symptoms often worse at night?
Carpal tunnel syndrome symptoms are often worse at night because the wrist may remain flexed or bent during sleep, increasing pressure inside the carpal tunnel. Fluid shifts during the night and reduced movement may also increase swelling around the flexor tendons and median nerve. Many patients wake up with numbness, tingling, burning, or electric sensations in the thumb, index, middle, or part of the ring finger. Shaking the hand may temporarily relieve symptoms because movement changes wrist position and reduces nerve irritation. Night symptoms are clinically important because they are typical of median nerve compression. Night splints that keep the wrist in a neutral position can reduce pressure and are often used in mild or moderate cases.
Can carpal tunnel syndrome be confused with cervical radiculopathy or pronator syndrome?
Yes. Carpal tunnel syndrome can be confused with cervical radiculopathy, pronator syndrome, peripheral neuropathy, ulnar nerve compression, tendon disorders, or thoracic outlet syndrome. Cervical radiculopathy can produce arm and hand symptoms because nerve roots are affected before they become peripheral nerves. Pronator syndrome compresses the median nerve in the forearm rather than at the wrist and may mimic some median nerve symptoms. Peripheral neuropathy can cause bilateral or diffuse numbness, especially in patients with diabetes or metabolic disease. Ulnar nerve compression affects different fingers but may coexist. The distinction depends on symptom distribution, neck symptoms, provocative tests, sensory pattern, muscle weakness, EMG and nerve conduction studies, ultrasound, and sometimes cervical spine imaging.
When are EMG or nerve conduction studies needed for carpal tunnel syndrome?
EMG and nerve conduction studies are useful when the diagnosis of carpal tunnel syndrome is uncertain, when symptoms are atypical, when weakness or thenar atrophy is present, when surgery is being considered, or when another condition must be excluded. In typical cases, clinical assessment and scoring systems such as CTS-6 may be enough to support the diagnosis. However, electrodiagnostic testing can confirm median nerve compression at the wrist, grade severity, identify axonal damage, and help distinguish carpal tunnel syndrome from cervical radiculopathy, pronator syndrome, peripheral neuropathy, or ulnar nerve compression. Testing is also important before surgery in many patients because it helps estimate prognosis and provides a baseline if symptoms persist after treatment.
Can corticosteroid injections help carpal tunnel syndrome?
Corticosteroid injections can help carpal tunnel syndrome in selected patients, especially when inflammation or temporary swelling contributes to median nerve compression. An injection may reduce swelling around the tendons and nerve, improving numbness, tingling, and night symptoms. The effect may be meaningful and sometimes lasting in mild or moderate cases, particularly when compression is not fixed or severe. However, if the main problem is ongoing mechanical narrowing of the carpal tunnel, a thickened transverse carpal ligament, severe electrodiagnostic compression, constant numbness, or thenar weakness, injections often provide only temporary relief. Injections should not delay necessary surgery in advanced cases. Their value depends on symptom severity, duration, nerve function, and the suspected dominant mechanism.
What is the difference between mini-open and endoscopic carpal tunnel release?
Mini-open and endoscopic carpal tunnel release are two techniques used to divide the transverse carpal ligament and relieve pressure on the median nerve. Mini-open release uses a small incision in the palm, usually limited to the area over the ligament and not extending across the wrist crease. It is widely used and allows direct visualization of the ligament. Endoscopic release divides the ligament through one or two small portals using a camera-guided instrument, without a larger palm incision. High-quality evidence shows no major long-term outcome difference between the two techniques. Endoscopic surgery may allow slightly faster return to work in some patients, but may carry a somewhat higher complication risk. Surgeon experience is important.
Why can diabetes, thyroid disease, pregnancy or rheumatoid arthritis worsen carpal tunnel syndrome?
Diabetes, thyroid disease, pregnancy, and rheumatoid arthritis can worsen carpal tunnel syndrome because they increase nerve vulnerability, tissue swelling, or inflammation inside the carpal tunnel. Diabetes and metabolic disorders can make peripheral nerves more sensitive to compression and may slow recovery. Thyroid disease can be associated with soft tissue swelling. Pregnancy can cause fluid retention and hormonal changes that raise pressure in the carpal tunnel; symptoms often improve after delivery. Rheumatoid arthritis can inflame tendon sheaths and surrounding tissues, reducing available space for the median nerve. These conditions may not be the only cause, but they can amplify compression and influence treatment response. Managing systemic contributors can improve outcomes and reduce recurrence risk.
Can carpal tunnel syndrome be an early sign of systemic amyloidosis?
Yes. In some older patients, carpal tunnel syndrome can be an early manifestation of systemic amyloidosis. Amyloid deposits may accumulate in tendon tissue around the median nerve and increase pressure within the carpal tunnel. Studies in patients undergoing carpal tunnel surgery have found amyloid deposits in tenosynovial tissue in a meaningful minority of cases, and in some patients this finding changes their broader medical evaluation and treatment. This does not mean that most carpal tunnel syndrome is caused by amyloidosis. However, in older patients, especially those with bilateral carpal tunnel syndrome, heart disease, unexplained weakness, or other suggestive features, analysis of tenosynovial tissue or further systemic evaluation may be appropriate. This is a medical decision, not routine for everyone.
What is double crush syndrome in carpal tunnel syndrome?
Double crush syndrome means that the same nerve pathway is affected at more than one anatomical level. In carpal tunnel syndrome, median nerve compression at the wrist may coexist with cervical radiculopathy, brachial plexus compression, thoracic outlet syndrome, pronator syndrome, or generalized peripheral neuropathy. If only the wrist compression is treated, symptoms may improve only partially because another site continues to irritate the nerve pathway. This is one reason why some patients have persistent symptoms after technically successful carpal tunnel release. Double crush should be considered when symptoms do not match a pure median nerve distribution, when neck or shoulder symptoms are present, when EMG suggests another lesion, or when recovery after surgery is incomplete.
Why can recovery after carpal tunnel surgery take several months?
Recovery after carpal tunnel surgery can take several months because decompression relieves pressure, but the median nerve still needs time to recover. If compression was mild and recent, night symptoms and tingling may improve quickly. If compression was long-standing, nerve fibers may have structural changes, and sensory recovery may be slower. Weakness or thenar muscle wasting may recover incompletely if motor fibers were affected for too long. Postoperative scar sensitivity, swelling, local irritation, incomplete decompression, or overlapping diagnoses can also delay improvement. Systemic factors such as diabetes, inflammation, nutritional deficiencies, poor sleep, stress, and continued repetitive wrist strain may maintain symptoms. Gradual improvement is common, but lack of progress should prompt reassessment.