Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 10, 2026
Who this page is for – patients with neck pain after whiplash (3+ months / chronic whiplash pain)
This page is intended for patients with neck pain after a car accident, sports injury, or fall whose imaging (X-ray, CT, or MRI) shows no fracture or dislocation, and whose symptoms persist beyond the usual healing period (4–12 weeks) despite appropriate initial care. At that stage, the real cause is often no longer simple muscle strain but facet, ligament, disc, or nerve irritation that requires targeted evaluation.
It is also relevant if you have headache, stiffness, or arm symptoms after whiplash and want to understand when MRI is useful, how recovery typically progresses, and which treatments help most.
If you would like a detailed review and next-step plan, you can request an online telehealth consultation with our specialist.
When patients usually seek a second opinion for whiplash injury and cervical sprain
- Neck pain, stiffness, or headaches persist beyond the expected recovery window
- Symptoms keep recurring after temporary improvement or flare with normal activity
- Dizziness, visual sensitivity, or “brain fog” is present and the explanation feels unclear
- MRI/CT looks normal or shows only mild degenerative findings that do not fully match the symptoms
- You are considering injections, procedures, or you need clearer guidance on next steps
If this reflects your situation, a focused telehealth review can help identify the most likely pain generators (facet joints, discs, muscles, nerve sensitization), clarify what tests or treatments are reasonable, and what is — and is not — indicated in your case: Request Consultation
Whiplash and Cervical Sprain — Quick Summary (Read This First)
- Whiplash and cervical sprain are soft-tissue neck injuries without fracture or dislocation. They usually involve muscles, ligaments, facet joint capsules, discs, or nerve irritation after sudden acceleration–deceleration, hyperextension, hyperflexion, sports injury, fall, or traffic accident.
- Most whiplash and cervical sprain injuries improve within weeks. Many patients recover with pain control, early gentle movement, posture correction, and rehabilitation, especially when there is no neurological deficit or structural instability.
- Persistent neck pain after whiplash lasting more than 3 months is no longer treated as a simple acute strain. At that stage, the key question is which structure is still generating pain — facet joint, ligament, disc, nerve root, muscle imbalance, or myofascial trigger point.
- Normal X-ray, CT, or MRI does not always explain persistent whiplash pain. Imaging may exclude fracture, dislocation, or major disc herniation, but small facet capsule injuries, ligament micro-tears, muscle dysfunction, or nerve sensitization may still maintain pain.
- Whiplash symptoms may include neck pain, stiffness, headaches, shoulder pain, dizziness, visual sensitivity, brain fog, or arm symptoms. These symptoms should be interpreted together with the injury mechanism, examination, imaging, and recovery pattern.
- Facet joints are a common pain generator after whiplash. Pain that worsens with rotation, extension, or certain neck positions may come from irritated cervical facet joints or their capsules, even when routine imaging is not dramatic.
- Whiplash can sometimes irritate a cervical disc or nerve root. Arm pain, numbness, tingling, weakness, or symptoms following a nerve-root pattern may suggest radiculopathy and may require MRI or specialist evaluation.
- Red flags after whiplash require urgent in-person medical evaluation. Progressive weakness, gait imbalance, severe neurological symptoms, bladder problems, suspected fracture, instability, or spinal cord signs should not be managed only with home treatment or telehealth.
- Long-term collar use is usually not helpful for stable whiplash injuries. A soft collar may be used briefly for comfort in selected patients, but early controlled movement and rehabilitation usually support better recovery than prolonged immobilization.
- Treatment after 3–6 months of whiplash pain must be targeted. Repeating general painkillers or generic physical therapy is often not enough if the active pain generator has not been identified and treated directly.
- A structured telehealth second opinion can help when whiplash recovery is delayed. Review of symptoms, injury mechanism, imaging, movement triggers, and pain mapping can clarify whether the likely source is a facet joint, ligament, disc, nerve root, muscle dysfunction, or mixed mechanism.
- This page is for patients with neck pain, stiffness, headache, or arm symptoms after whiplash or cervical sprain when recovery is slower than expected. It explains diagnosis, imaging, treatment, red flags, chronic pain mechanisms, and when specialist review may help.
Most readers benefit from reviewing the Quick Summary together with the sections on Definition of Whiplash and Distinction From Other Cervical Injuries, Diagnostic Evaluation of Cervical Sprain and Whiplash, Treatment of Cervical Sprain and Whiplash, and Why Neck Pain Persists After Whiplash. Later sections provide deeper clinical detail for patients whose neck pain, headache, stiffness, dizziness, or arm symptoms continue beyond the usual recovery period.
Contents
- Who is this page for?
- Definition of Whiplash
- Causes and Mechanisms
- Impact Biomechanics and Direction
- Specific Tissue Lesions
- Grades of Injury Severity
- Structures Commonly Affected
- Symptoms of Whiplash/Cervical Sprain
- Diagnostic Evaluation
- Differential Diagnosis
- Treatment of Whiplash/Sprain
- Prognosis and Recovery
- Long-Term Pain After Whiplash
- Key Points for Patients
- FAQs for Whiplash
- Additional Information
- Start Telehealth Consultation
Definition of Whiplash and Distinction From Other Cervical Injuries
Cervical sprain and whiplash describe soft-tissue injuries of the neck that occur when the head and cervical spine move suddenly beyond their normal range — usually during car accidents, sports injuries, or falls.
These injuries involve overstretching or tearing of the neck muscles, ligaments, and facet joint capsules, but do not include vertebral fractures or dislocations.
In some cases, however, a traumatic cervical disc herniation may occur — a soft-tissue complication of the same mechanism — producing nerve root or spinal cord compression even though the vertebrae remain intact.
In contrast, cervical spine injuries as a broader group may also include fractures, dislocations, or spinal cord damage.
Experts describe cervical sprain and whiplash as low-energy, reversible injuries on the mild end of the cervical trauma spectrum, whereas fractures and cord injuries result from high-energy mechanisms such as axial load or direct impact.
Key differences:
- Tissues involved: Sprain and whiplash affect muscles, ligaments, and capsules; fractures and dislocations involve bone and spinal alignment.
- Neurological findings: Soft-tissue injuries may cause transient nerve irritation but not spinal cord damage.
- Mechanism: Whiplash results from acceleration–deceleration or hyperflexion–extension; severe injuries stem from direct compression or high-velocity trauma.
- Imaging: Plain X-rays are often normal; MRI best shows ligament or soft-tissue injury.
Most patients who reach a specialist have already tried basic therapies; at this stage, improvement depends on identifying the dominant pain generator (facet joint, ligament, disc, nerve, or muscle imbalance).
Causes And Mechanisms of Whiplash Injury
The classic whiplash mechanism involves sudden acceleration–deceleration, typically in rear-end vehicle collisions.
Other causes include:
- Front or side vehicle collision
- Falls where the head is forced backward or sideways.
- Sports injuries with sudden neck movement or impact.
- Occupational accidents involving sudden jerking of the neck.
Biomechanics and Direction of Impact During Traffic Accidents
The classic whiplash mechanism occurs during a rear-end collision, when the body is suddenly pushed forward while the head momentarily lags behind. This produces a rapid hyperextension followed by rebound hyperflexion, creating two distinct phases of soft-tissue strain:
- Initial hyperextension — the anterior structures (anterior longitudinal ligament, longus colli, longus capitis, and sternocleidomastoid muscles) are stretched, while the posterior joints and capsules (facet and zygapophyseal joints) are compressed.
- Rebound hyperflexion — the motion reverses, stretching the posterior ligaments and muscles (nuchal ligament, interspinous and supraspinous ligaments, trapezius, semispinalis capitis), and compressing the anterior discs.
In a frontal (head-on) impact, the sequence is opposite:
- The head moves forward first, causing hyperflexion that strains the posterior soft tissues,
- followed by rebound extension, which stretches the anterior ligaments and muscles.
Thus, regardless of impact direction, both anterior and posterior structures are usually injured, because every sudden flexion is followed by an opposite rebound extension.
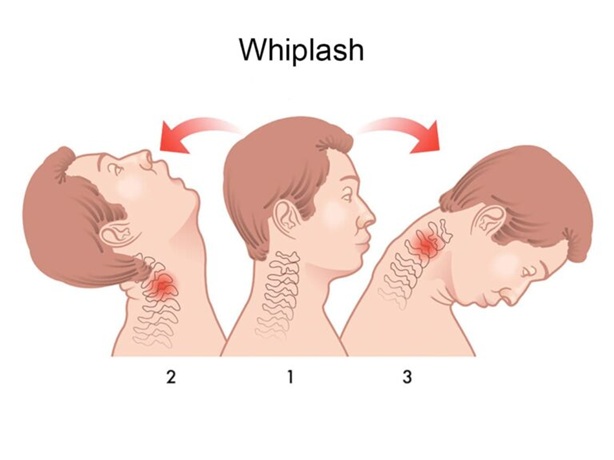
Image: Sequence of cervical motion during a vehicle collision — neutral position (center), hyperextension phase (rear impact), and hyperflexion phase (front impact).
Specific Tissue Lesions and Severity in Whiplash Injury
Whiplash and cervical sprain injuries result from rapid stretching of muscles, tendons, and ligaments that stabilize the cervical spine. The extent of tissue damage depends on the direction and magnitude of the force applied to the neck.
Grades of injury severity
- Grade I–II: Mild soft-tissue strain involving microscopic fiber disruption in muscles and tendons.
- Grade III: Partial tearing of cervical ligaments or joint capsules, often accompanied by local inflammation and muscle spasm.
- Grade IV: Severe ligament disruption with mechanical instability or neurological deficit. Such cases are not considered “whiplash injuries” but rather unstable cervical spine injuries that require urgent imaging and often surgical stabilization.
Structures commonly affected
- Muscles and tendons: Overstretching and microtears cause spasm, stiffness, and localized tenderness.
- Ligaments and joint capsules: Strain or partial rupture of the anterior/posterior longitudinal ligaments or facet joint capsules limits stability and motion.
- Facet joints: Frequently become the main source of post-traumatic neck pain
- Intervertebral discs: May show annular strain or secondary inflammation; a traumatic disc herniation can occasionally occur even without fracture, producing radiculopathy or cord compression
- Nerve roots: Transient irritation may develop from local edema or pre-existing degenerative narrowing of the foramina.
In summary:
Whiplash represents a spectrum of soft-tissue cervical injuries, from simple muscle strain to complex ligamentous or disc involvement. Most cases remain stable and recover fully with conservative treatment, but MRI is warranted if neurological deficits or signs of instability appear.
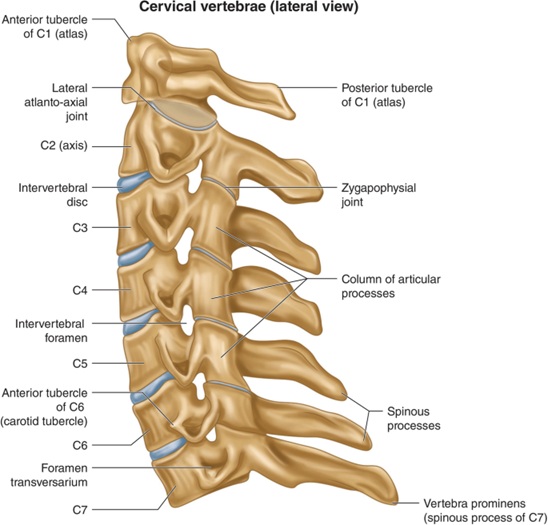
Image: Anatomy of the cervical spine. The image shows the vertebral bodies, discs between them, zygapophyseal (facet) joints, and other elements. Learn more on our Pain Anatomy page.
Symptoms of Cervical Sprain and Whiplash
Symptoms may appear immediately or within 24 hours after trauma:
- Neck pain and stiffness.
- Restricted motion, especially rotation or extension.
- Pain radiating to the shoulders or arms.
- Headache (often occipital).
- Muscle spasm or tenderness in the upper back.
- Pain or tenderness in the front of the neck (sternocleidomastoid area), especially after rear-end collisions.
- Numbness or tingling in the arms if nerve root irritation occurs.
- Fatigue, dizziness, or difficulty concentrating in some patients.
Diagnostic Evaluation of Cervical Sprain and Whiplash
Accurate diagnosis starts with:
- Clinical examination — palpation for tenderness, range-of-motion testing, and neurological assessment.
- Imaging
- X-ray: to rule out fracture or malalignment.
- CT scan: indicated when a fracture is suspected
- MRI: best for assessing soft-tissue, disc, or ligament injury, and nerve root irritation.
- Electromyography (EMG/NCV) — when neurological symptoms persist.
- Differential diagnosis — excludes cervical fracture, disc herniation, spinal cord injury, and referred shoulder pain.
Treatment of Cervical Sprain and Whiplash
Most patients recover with conservative, non-operative management:
- Pain control — NSAIDs, acetaminophen, short-term muscle relaxants, local heat, or trigger-point injections.
- Brief immobilization — a soft cervical collar may be used for a few days for comfort, but experts emphasize avoiding prolonged immobilization.
- Early mobilization — gentle neck movements as pain allows improve healing and prevent stiffness; randomized trials confirm faster recovery than rest with a collar.
- Physical therapy — stretching, posture correction, and strengthening of deep neck muscles once acute pain subsides.
- Rehabilitation — multimodal therapy (exercise + manual therapy + education) for persistent symptoms.
- Surgery — indicated only for structural instability or verified nerve/spinal cord compression.
Telehealth evaluation is appropriate for patients with stable symptoms, while emergency imaging is required if neurological deficits are present.
Start Your Telehealth Consultation for Neck Pain
Telehealth Consultation for Persistent Neck Pain After Whiplash
If your neck pain or stiffness has lasted longer than expected after a car accident or sports injury, a telehealth consultation can help identify the real pain source — whether it’s a facet joint, cervical disc, nerve root, ligament, or muscle imbalance — and create a step-by-step plan for recovery. If you are considering legal action or insurance procedures after your injury, we can also help you understand whether your symptoms and medical findings have a clear medical basis before you decide on further steps.
✔ Send a short message describing your symptoms and any imaging you have (X-ray, CT, MRI).
✔ You’ll receive a reply within 24 h confirming if we can help, consultation cost, and available time slots.
✔ After confirmation, send your medical files securely by email or WhatsApp.
✔ The video consultation includes a written report and follow-up questions within 10 days.
✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
✔ You’ll receive a reply within 24 h confirming if we can help, consultation cost, and available time slots.
✔ After confirmation, send your medical files securely by email or WhatsApp.
✔ The video consultation includes a written report and follow-up questions within 10 days.
✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Typical consultation fee: $180 – 250 USD, depending on case complexity.
Many patients worldwide now use telehealth second opinions for neck and whiplash pain — it’s safe, accepted, and often shortens recovery time.
Before contacting us, please read our Privacy Policy and Terms of Use.
Online pain consultation for neck pain in detail
Schematic explanation of the video consultation for neck pain
Answers to questions about the process and success of video consultations for neck pain
Reasons for persistent neck pain despite treatment
Artificial intelligence can also support the process by analyzing complex data, but clinical expertise remains essential.
Sometimes, the real source of pain becomes clear only after diagnostic and therapeutic interventional procedures.
Prognosis of Cervical Sprain and Whiplash
Prognosis is favorable in most cases:
- 80–90 % recover within 2–6 weeks.
- Persistent pain > 3 months occurs in a minority of patients and is usually related to unresolved soft-tissue or joint injury — most commonly facet joint irritation, ligament micro-tears, muscle imbalance, poor posture, deconditioning, untreated myofascial trigger points, or subtle disc/foraminal narrowing made symptomatic by the trauma. Persistent pain after whiplash is usually manageable once the true pain generator is identified and addressed.
- Prognosis is less favorable in patients with pre-existing degeneration, high initial pain scores, or delayed mobilization.
Differential diagnosis of Cervical Sprain and Whiplash
Important differential considerations in patients with pre-existing neck pain or degenerative changes:
- Cervical fracture or dislocation — must be excluded radiographically after trauma.
- Cervical disc herniation — may coexist or arise after whiplash; produces radiculopathy.
- Facet joint injury or pain syndrome — common chronic sequela.
- Ligamentous instability — may appear with delayed neurological signs.
- Spinal cord injury (central cord syndrome) — hyperextension mechanism in cervical spondylosis.
- Exacerbation of cervical spondylosis or osteoarthritis — trauma may unmask prior asymptomatic disease.
- Shoulder or temporomandibular joint injury — referred pain may mimic cervical pain.
Why Neck Pain Persists After Whiplash — Why Treatment Often Fails
Chronic neck pain after whiplash usually persists because the active pain generator has not been identified — facet joint, ligament, disc, nerve root, muscle imbalance, myofascial trigger point, or mixed mechanism — even when X-ray, CT, or MRI show no fracture or major injury.
In many patients, persistent neck pain after whiplash is not due to severe injury, but because the pain has not been fully analyzed at all relevant levels. Treatment may appear appropriate, but remains incomplete if the exact structure, the underlying process, and contributing factors are not clearly identified.
Even though many cases improve in the first few weeks, when neck symptoms continue beyond 2 to 12 months, this usually indicates that one or more underlying pain generators remain active. These may include:
- Persistent inflammation or reflex spasm in cervical muscles (levator scapulae, trapezius, deep neck flexors), which can irritate adjacent nerves and reproduce the same pain pattern long after the injury.
- Small-joint (facet) capsule injury that never healed fully, keeping the segment irritated and painful during rotation or extension.
- Micro-tears in cervical ligaments that may not appear on MRI but continue to provoke stability-related pain.
- Subtle disc or foraminal narrowing made symptomatic only by trauma, often without a classic “herniation”.
- Muscle imbalance or enthesopathy in deep stabilizers that maintains asymmetric load and chronic pain.
- Deconditioning, posture changes, and altered movement patterns that convert an acute injury into a long-lasting pain cycle.
Importantly, when pain lasts longer than 3 months, treatment has to move beyond simple rest and basic painkillers. At that point, the key is a structured evaluation that identifies which exact structure is causing the pain — whether a facet joint, ligament, disc, nerve root, or a persistent muscle imbalance. In each of these structures, specific pathological processes may develop. For example, facet joints may undergo inflammatory or degenerative changes, ligaments may develop chronic micro-injury and fibrosis, discs may show internal disruption or annular tears, nerve roots may become sensitized or compressed, and muscles may develop myofascial trigger points and altered activation patterns. These processes are often driven or maintained by contributing factors such as prolonged sitting, poor posture, repetitive strain, inadequate recovery, or even systemic influences like inflammatory nutrition or metabolic factors, which can prevent proper healing and lead to persistent pain.
Once the real pain source is identified, many patients improve even if they previously “tried everything.” This is because the treatment is no longer general pain medication but a targeted combination of drugs — adjusted over 4–8 weeks — matched to the specific injured structure (facet joint, ligament, nerve, or disc). When symptoms do not improve enough with medication alone, image-guided procedures — such as facet or medial-branch blocks, trigger-point injections, or selective nerve-root blocks — can directly target the painful structure and significantly speed up recovery.
Key points for patients
- Most neck sprains and whiplash injuries heal completely without surgery.
- Early movement and proper rehabilitation are critical for full recovery.
- Persistent or progressive neurological symptoms require prompt specialist evaluation (MRI, neurosurgical review).
- Avoid long-term use of a cervical collar unless prescribed for specific instability.
FAQs for Whiplash and Cervical Sprain
What exactly is a whiplash injury?
A whiplash injury is a soft-tissue injury of the neck caused by sudden acceleration and deceleration of the head. It often happens in rear-end car accidents, but it can also occur after falls, sports injuries, or any sudden force that pushes the cervical spine beyond its normal range. Whiplash can strain muscles, ligaments, facet joint capsules, discs, and nearby nerves without causing a fracture or dislocation. This is why X-rays or CT scans may be normal even when pain is significant. The key question is which structure is now driving the pain — muscle, facet joint, ligament, disc, nerve root, or a mixed mechanism.
Is whiplash the same as a cervical sprain?
Whiplash and cervical sprain are closely related terms, but they are not always used in exactly the same way. Whiplash describes the injury mechanism: sudden back-and-forth or side-to-side movement of the head and neck. Cervical sprain describes the tissue injury: stretching or partial tearing of muscles, ligaments, tendons, or joint capsules in the cervical spine. In practice, many patients are told they have a “whiplash injury,” “neck sprain,” or “cervical sprain” after trauma without fracture. The important point is that persistent symptoms require a pain-source assessment, not only a label.
Can whiplash occur without a car accident?
Yes. Although whiplash is most often associated with car accidents, the same mechanism can happen during sports, falls, sudden slips, workplace injuries, direct impacts, amusement rides, or any event where the head and neck are suddenly forced beyond their normal range. The injury does not require a high-speed crash. Even a lower-energy mechanism can irritate cervical muscles, ligaments, facet joints, discs, or nerve roots, especially if there was pre-existing cervical degeneration or poor neck conditioning. What matters clinically is not only the cause of the trauma, but the pattern of symptoms that follows.
What are the most common symptoms of whiplash and cervical sprain?
The most common symptoms of whiplash and cervical sprain are neck pain, stiffness, reduced range of motion, muscle spasm, pain between the shoulder blades, and headache, often in the back of the head. Some patients also feel shoulder pain, arm tingling, dizziness, visual sensitivity, fatigue, concentration problems, or a sense of “brain fog.” Symptoms may appear immediately or develop over the next 24–48 hours. Persistent symptoms usually mean that one or more pain generators remain active, such as a facet joint, ligament, disc, nerve root, myofascial trigger point, or altered movement pattern.
How long does whiplash usually take to heal?
Many whiplash injuries improve within a few weeks, and a large number of patients recover within 2–6 weeks. Some cases take longer, especially when pain is more intense at the beginning, movement is avoided for too long, there is pre-existing cervical degeneration, or the injury irritates facet joints, ligaments, discs, nerve roots, or deep neck muscles. Pain that persists beyond 3 months is usually considered chronic or persistent whiplash-associated pain. At that stage, treatment should not remain limited to rest and basic painkillers. The active pain generator must be identified and treated more specifically.
Can whiplash lead to chronic neck pain?
Yes. Whiplash can lead to chronic neck pain when the injured structure does not fully recover or when the pain cycle becomes self-sustaining. Common causes include facet joint irritation, ligament micro-injury, disc annular irritation, nerve root sensitization, myofascial trigger points, muscle imbalance, poor posture, fear of movement, and deconditioning. Chronic neck pain from whiplash is not always explained by a large MRI finding. Many pain generators are functional, mechanical, or inflammatory at a small scale. Improvement is still possible, but treatment must be targeted to the structure that is actually maintaining the pain.
Why does neck pain persist after whiplash if X-ray, CT, or MRI are normal?
Normal X-ray, CT, or MRI does not exclude pain after whiplash. X-ray and CT are mainly used to rule out fracture, dislocation, or major instability. MRI can show discs, ligaments, spinal cord, and nerve roots, but it may still miss small facet capsule injuries, ligament micro-tears, muscle dysfunction, myofascial trigger points, nerve sensitization, or altered movement mechanics. In many patients, pain persists because the active generator is not visible as a dramatic structural lesion. This is why clinical pain mapping — location, triggers, movement response, tenderness, and neurological symptoms — is essential.
Can a whiplash injury cause a cervical disc herniation?
Yes, but it is not the most common outcome. Whiplash usually causes soft-tissue strain involving muscles, ligaments, facet joint capsules, and myofascial structures. In some patients, especially when there is pre-existing disc degeneration, the trauma may aggravate a disc problem or contribute to a cervical disc herniation. A disc herniation is more likely when neck pain is accompanied by arm pain, numbness, tingling, weakness, or signs of nerve root or spinal cord compression. MRI is useful when these neurological symptoms persist or progress. Not every disc bulge found after trauma is necessarily the pain source.
Can whiplash cause facet joint pain?
Yes. Facet joints are a common source of persistent neck pain after whiplash. During sudden extension, flexion, rotation, or side-bending, the small joints in the back of the cervical spine can be compressed, stretched, or irritated. Facet-related pain is often worse with neck extension, rotation, prolonged sitting, driving, or looking upward. It may refer pain to the back of the head, shoulder blade region, or upper back. MRI may not clearly show facet capsule irritation. When symptoms fit this pattern, targeted examination and sometimes diagnostic medial branch or facet-related procedures may help confirm the source.
Can whiplash cause cervical ligament injury or instability?
Whiplash can strain or partially injure cervical ligaments, especially when the neck is forced into rapid flexion, extension, or rotation. Most ligament injuries are stable and heal with conservative treatment. More serious ligament disruption or instability is less common, but it must be considered when pain is severe, there is a feeling of mechanical instability, neurological symptoms develop, or imaging suggests abnormal alignment. MRI can help assess soft tissues, while flexion-extension X-rays may be considered in selected cases after acute fracture has been excluded. Persistent pain does not automatically mean instability, but ligament-related pain should be evaluated when symptoms fit.
What imaging tests are needed after whiplash or cervical sprain?
The choice of imaging depends on the mechanism of injury, symptoms, examination, and red flags. X-ray or CT is used when fracture or dislocation must be excluded, especially after significant trauma. CT is better for bone injury. MRI is useful when there are neurological symptoms, suspected disc herniation, spinal cord signs, ligament injury, persistent severe pain, or symptoms that do not match simple muscle strain. Many patients with stable whiplash do not need repeated imaging. If previous imaging is normal but pain persists, the next step may be pain-source analysis rather than simply ordering another scan.
When should I see a doctor urgently after a whiplash injury?
Urgent medical evaluation is needed after whiplash if there is weakness, numbness spreading into the arms or legs, problems walking, loss of bladder or bowel control, severe or worsening headache, confusion, fainting, fever, severe dizziness, trouble speaking, visual loss, chest pain, or severe pain after high-energy trauma. Urgent imaging is also needed if fracture, dislocation, spinal cord injury, or unstable ligament injury is suspected. Telehealth is not appropriate for emergencies. It is most useful when dangerous injury has already been excluded and the remaining question is why pain, stiffness, headache, or arm symptoms persist.
Is a cervical collar necessary after whiplash?
A soft cervical collar may be used briefly for comfort in selected patients, especially during the first days after injury. However, prolonged immobilization is usually not helpful for uncomplicated whiplash and may worsen stiffness, fear of movement, muscle weakness, and delayed recovery. Most stable whiplash injuries recover better with early gentle movement, reassurance, gradual activity, and appropriate rehabilitation. A collar should not be used long-term unless a physician has identified a specific reason, such as instability or another condition requiring immobilization. The goal is controlled recovery, not complete avoidance of neck movement.
Which treatments help most early after whiplash?
Early treatment usually includes reassurance, short-term pain control, gentle neck movement, gradual return to activity, heat or cold depending on comfort, and avoidance of prolonged immobilization. Physical therapy may help when pain and stiffness persist, especially if it includes education, posture correction, range-of-motion exercises, deep neck muscle activation, and progressive strengthening. Treatment should be adjusted to the patient’s symptoms. If headache, dizziness, arm symptoms, severe pain, or neurological signs are present, the plan must be individualized. The most important early goal is to prevent a simple soft-tissue injury from becoming a chronic pain cycle.
When can physical therapy start after whiplash injury?
Physical therapy can often start early, once fracture, instability, or serious neurological injury has been excluded. In the first phase, therapy should be gentle and focused on pain control, safe movement, posture, breathing, and avoiding excessive guarding. Later, it can progress to range-of-motion exercises, deep neck flexor activation, shoulder blade control, strengthening, and return-to-activity training. Therapy should not be aggressive if it repeatedly worsens symptoms. If pain persists despite therapy, the question becomes whether the correct pain generator has been identified — facet joint, ligament, disc, nerve root, muscle trigger point, or mixed mechanism.
Do injections help persistent pain after whiplash?
Injections can help selected patients with persistent whiplash pain, but only when they target the correct pain generator. If pain appears to come from cervical facet joints, medial branch blocks may help confirm the source and guide further treatment. Trigger point injections may help myofascial pain. Selective nerve root blocks may be considered when radicular symptoms match nerve root irritation. Injections should not be used randomly just because pain persists. They are most useful after careful analysis of pain location, movement triggers, imaging, neurological signs, and response to previous treatment. The goal is diagnosis and targeted relief, not temporary masking alone.
Can neck crepitus after whiplash be dangerous?
Neck crepitus means clicking, cracking, grinding, or popping sounds during neck movement. After whiplash, it can come from muscle tension, facet joint irritation, altered movement mechanics, or pre-existing cervical degeneration made more noticeable by injury. Crepitus alone is not always dangerous, especially if there is no severe pain, weakness, numbness, instability, or neurological deficit. However, crepitus with persistent pain, reduced motion, dizziness, arm symptoms, or a feeling of instability should be evaluated. The important question is whether the sound is harmless joint movement or a clue to an active pain generator such as a facet joint or ligament-related problem.
Can dizziness, brain fog, or visual sensitivity happen after whiplash?
Yes. Some patients develop dizziness, concentration problems, fatigue, visual sensitivity, or a feeling of brain fog after whiplash. These symptoms may relate to pain, sleep disruption, cervical muscle tension, vestibular involvement, concussion, anxiety amplification, medication effects, or altered neck proprioception. They should not be dismissed, but they also need careful sorting because treatment differs depending on the cause. Red flags such as severe headache, fainting, neurological deficits, confusion, speech problems, or worsening symptoms require urgent in-person assessment. In stable cases, a structured review can help decide whether cervical, vestibular, neurological, or mixed mechanisms are likely.
Does age or pre-existing cervical degeneration affect whiplash recovery?
Yes. Pre-existing cervical degeneration, disc narrowing, facet arthritis, foraminal stenosis, poor posture, muscle weakness, and previous neck pain can make recovery slower or more complex. A whiplash injury may not create a new severe structural problem, but it can make a previously silent cervical condition symptomatic. This is why imaging sometimes shows “mild degenerative changes” that doctors disagree about. The question is whether those findings match the current pain pattern and neurological signs. Age or degeneration does not mean recovery is impossible. It means treatment must be more precise and adapted to the active pain generator.
What sleep positions and pillows help after whiplash?
After whiplash, the best sleeping position is usually the one that keeps the neck neutral and reduces morning stiffness. Many patients do better sleeping on the back or side with a pillow that supports the natural curve of the neck without forcing the head forward or sideways. Very high pillows can increase flexion and worsen pain, while very flat pillows may leave the neck unsupported. Stomach sleeping often aggravates symptoms because it forces rotation. If morning pain is severe, the problem may not be the pillow alone but an active facet, muscle, disc, or ligament-related pain generator that needs assessment.
My neck pain has lasted more than 3–6 months after whiplash. Can it still improve?
Yes. Neck pain that has lasted more than 3–6 months after whiplash can still improve, but the approach must change. At that stage, the problem is usually not simple acute strain. Persistent pain may be maintained by facet joint irritation, ligament micro-injury, disc-related pain, nerve root sensitization, muscle imbalance, myofascial trigger points, posture, deconditioning, or central sensitization. Improvement depends on identifying which of these mechanisms is dominant. Many patients have tried general treatment without success because the treatment was not matched to the pain source. A structured pain-source assessment can still reveal a treatable pattern.
When is an online second opinion useful after whiplash?
An online second opinion is useful after whiplash when pain, stiffness, headache, dizziness, or arm symptoms continue despite initial treatment, or when imaging is normal but symptoms remain disabling. It can also help when MRI shows mild degenerative changes and it is unclear whether they matter. During video consultation, the doctor can review the injury mechanism, reports, imaging, symptom timeline, neurological complaints, posture, movement triggers, and response to treatment. Guided self-examination can help identify whether the likely source is facet joint, ligament, disc, nerve root, muscle imbalance, myofascial pain, or a mixed mechanism.
Additional Information for Whiplash and Cervical Sprain
Additional Information About Whiplash and Cervical Sprain