Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
March 08, 2026
Who This Meningioma Page Is For
This page is intended for patients in whom MRI or CT has revealed a meningioma, as well as for individuals who have been advised to consider observation, surgical removal, or radiation therapy. It may be particularly helpful for patients experiencing symptoms such as headaches, seizures, visual disturbances, progressive weakness, balance problems, or other neurological changes that may be related to a tumor arising from the meninges surrounding the brain.
If surgery, stereotactic radiosurgery (such as Gamma Knife), radiotherapy, or long-term MRI monitoring has been proposed — or if specialists have offered different recommendations regarding the urgency or type of treatment — an individualized neurosurgical second opinion may help clarify the biological behavior of the tumor, expected risks of neurological deterioration, likelihood of recurrence, and the safest balance between observation, surgery, and radiation therapy based on tumor size, location, growth rate, and overall neurological status.
When patients seek a second opinion for meningioma
• MRI or CT has revealed a meningioma, but it is unclear whether observation, surgery, or radiation therapy is the most appropriate strategy
• The tumor has been discovered incidentally and different specialists recommend either monitoring with MRI or early surgical removal
• Progressive headaches, seizures, visual disturbances, weakness, or balance problems suggest that the tumor may be affecting surrounding brain structures
• Surgery has been recommended, but the expected neurological risks, likelihood of complete removal, or long-term prognosis remain unclear
• Stereotactic radiosurgery (such as Gamma Knife) or fractionated radiotherapy has been proposed, yet it is uncertain whether radiation or surgery would provide better tumor control
• Different specialists recommend observation, microsurgical removal, radiosurgery, or combined treatment without clear agreement
If your situation involves uncertainty regarding diagnosis, urgency, or treatment strategy, you may request an individualized neurosurgical review here:
Request Second Opinion
Meningioma — Quick Summary (Read This First)
- Meningioma is a tumor arising from the membranes that cover the brain and spinal cord. These membranes, called the meninges, surround and protect the central nervous system.
- Most meningiomas grow outside the brain tissue. They usually compress nearby brain structures rather than invading them directly.
- Meningiomas represent the most common primary intracranial tumor in adults. Epidemiological studies show that they account for approximately 35–41% of primary brain tumors.
- Many meningiomas grow slowly and may remain stable for years. A substantial proportion (60-80%) of meningiomas discovered incidentally on MRI do not require immediate treatment.
- Symptoms depend mainly on tumor location. Headaches, seizures, progressive weakness, visual disturbances, balance problems, or personality changes may occur when the tumor compresses specific brain regions.
- MRI with contrast is the most important diagnostic test. It allows physicians to determine meningioma size, location, surrounding edema, and the relationship of the tumor to critical brain structures.
- Not all meningiomas require immediate surgery. Many small or asymptomatic tumors are initially managed with MRI monitoring, particularly when imaging shows minimal growth and the tumor is not compressing critical structures.
- Surgery remains the main treatment for symptomatic or growing meningiomas. The goal is safe tumor removal while preserving neurological function.
- Radiation therapy (including stereotactic radiosurgery such as Gamma Knife) may control tumor growth in selected cases. It may be used for small tumors in surgically difficult locations, for residual tumor after surgery, or in selected patients when surgery carries higher risk.
- Treatment decisions depend mainly on tumor size, location, growth, symptoms, and relationship to critical structures. In most patients, the safest strategy is individualized rather than automatic.
- Prognosis depends mainly on tumor grade, location, and completeness of removal. Benign meningiomas that can be completely removed usually have an excellent long-term outcome.
- Although most meningiomas are benign, large tumors or tumors located near critical structures can still cause serious neurological problems.
Most readers benefit from reviewing this Quick Summary together with the sections on Symptoms, Diagnosis, Surgical Treatment, Radiation Therapy, and Treatment Decision-Making. Later sections provide more detailed explanations intended for patients seeking a deeper understanding before important treatment decisions are made.
Contents
- Who This Page
- Quick Summary
- Tumor Classification
- Tumor Causes
- Tumor Locations
- Multiple Tumors
- How They Affect
- Symptoms by Location
- MRI Diagnosis
- When Monitored
- Symptom Relief
- Meningioma and Epilepsy
- Surgical Treatment
- Modern Technologies
- Endoscopic Surgery
- Extent of Removal
- Radiation Therapy
- Residual Tumor Radiation
- Tumor Recurrence
- Treatment Decision Summary
- Why Opinions Differ
- Overall Prognosis
- Life-Threatening Risk
- Request Second Opinion
- FAQ
What Is a Meningioma
A meningioma is a usually slow-growing tumor that arises from the meninges and is typically attached to the dura mater—the layer covering the brain. It receives its blood supply from the meningeal arteries and grows gradually, compressing the brain and surrounding structures without infiltrating the brain tissue.
Most meningiomas arise from specialized cells located within the arachnoid layer, often referred to as arachnoid cap cells. When genetic changes occur in these cells, they may begin to multiply abnormally and gradually form a tumor. Unlike tumors that originate inside the brain tissue, meningiomas grow outside the brain, usually attached to the dura mater. As the tumor enlarges, it usually compresses the surrounding brain tissue instead of growing directly into it. Because of this growth pattern, most meningiomas remain well-defined masses that can usually be surgically separated from the brain.
Epidemiological studies show that meningiomas represent approximately 35–41% of all primary intracranial tumors in adults, making them the most common primary brain tumor. Small incidental meningiomas may be present in approximately 0.5–1% of the general population, based on autopsy and imaging studies. Most of them never cause symptoms or require treatment.
Meningiomas are also rare in children, representing less than 2% of all pediatric brain tumors. When they occur in younger patients, they are more frequently associated with genetic syndromes such as neurofibromatosis type 2 (NF2).
To learn more about other types of brain tumors, visit our Brain Tumors page.
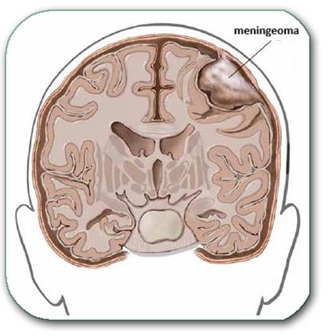
Image: A meningioma growing from the coverings of the brain (meninges, dura mater) and compressing surrounding parts of the brain, without infiltrating them.
Biological Classification of Meningiomas
The biological behavior of meningiomas is determined through histopathological analysis using the World Health Organization (WHO) classification.
Three main categories are recognized:
• WHO grade I — benign meningioma. This is the most common form, representing roughly 80–85% of meningiomas. These tumors typically grow slowly and often remain stable for long periods. When completely removed surgically, the chance of recurrence is relatively low.
• WHO grade II — atypical meningioma. Atypical meningiomas account for approximately 10–15% of of cases in surgical series of meningiomas. These tumors show increased cellular activity and a higher likelihood of recurrence after surgery. After complete tumor removal, some patients may be managed with MRI follow-up rather than immediate radiation therapy.
• WHO grade III — malignant (anaplastic) meningioma. These tumors are rare, representing roughly 1–3% of cases in surgical series of meningiomas. They grow more aggressively, recur more frequently, and usually require combined treatment with surgery and radiation therapy.
Although histological grade is important, clinical outcome also depends strongly on tumor location and the possibility of complete surgical removal.
Genetic and Biological Causes
Most meningiomas arise from sporadic genetic mutations that occur during life rather than inherited genetic disorders. At the molecular level, tumor development usually results from two main biological mechanisms:
• inactivation of tumor suppressor genes, which normally prevent uncontrolled cell growth
• activation of oncogenic signaling pathways, which stimulate cell proliferation
The most frequently involved gene is NF2, located on chromosome 22. Loss of function of this gene disrupts normal cell growth control and allows tumor formation. Other molecular alterations identified in meningiomas include mutations involving genes such as TRAF7, AKT1, SMO, and KLF4, while additional less common alterations may involve genes such as PIK3CA or TERT.
These molecular differences partly explain why tumors in different anatomical regions may behave differently.
The only clearly established environmental risk factor is exposure to ionizing radiation, particularly during childhood.
Meningiomas occur approximately two to three times more frequently in women than in men, suggesting that hormonal influences may play a role in tumor development and growth.
Although most meningiomas arise sporadically, a small proportion occur in the context of inherited genetic syndromes. The best known example is neurofibromatosis type 2 (NF2), a hereditary condition caused by mutations of the NF2 gene on chromosome 22. Patients with NF2 frequently develop multiple meningiomas, a condition referred to as meningiomatosis, in which several tumors arise in different intracranial and spinal locations. Multiple meningiomas may also appear sporadically without a hereditary syndrome, but they are particularly characteristic of NF2. In addition, meningiomas may occur in association with other rare genetic disorders such as schwannomatosis or Cowden syndrome, although these situations are much less common. Overall, hereditary syndromes account for only a small minority of meningioma cases.
Distribution of Meningiomas by Location
Because the meninges cover the entire brain, meningiomas can develop in many different parts of the skull. Their frequency varies significantly depending on location.
The approximate distribution of intracranial meningiomas is as follows:
• Convexity meningiomas — approximately 20–25%. These arise on the outer surface of the brain beneath the skull.
• Parasagittal and falcine meningiomas — about 20–25%. These tumors grow near the superior sagittal sinus, the major venous channel of the brain.
• Sphenoid wing meningiomas — roughly 15–20%. These develop near the skull base behind the eyes.
• Olfactory groove meningiomas — about 8–10%. They arise above the nasal cavity near the olfactory nerves responsible for smell.
• Tuberculum sellae meningiomas — about 5–10%. These occur in the middle of the skull base near the optic nerves and optic chiasm.
• Posterior fossa meningiomas — approximately 7–10%.
Within this group:
• Tentorial meningiomas — about 3–6%. These arise from the tentorium cerebelli, a membrane separating the upper brain from the cerebellum.
• Cerebellopontine angle (CPA) meningiomas — approximately 2–4%. These develop in the angle between the cerebellum and the brainstem, an area that also contains several important cranial nerves related to hearing and balance.
Rare locations include:
• Cavernous sinus meningiomas. These develop in the cavernous sinus, a venous space located behind the eyes at the base of the skull, where several important cranial nerves and the internal carotid artery pass.
• Petroclival meningiomas. These arise at the junction between the petrous part of the temporal bone and the clivus, deep in the central skull base near the brainstem.
• Foramen magnum meningiomas. These occur at the foramen magnum, the large opening at the base of the skull where the brainstem transitions into the spinal cord.
The location of the tumor is extremely important because it determines both the symptoms and the complexity of surgical treatment.
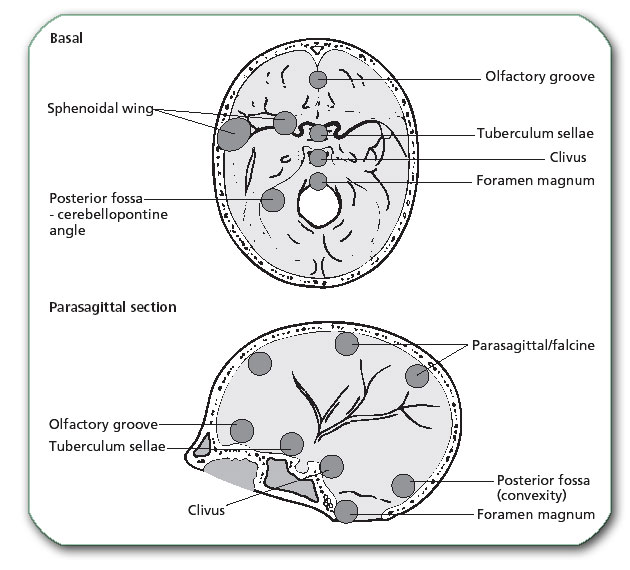
Image: Common locations of meningiomas
Multiple Meningiomas (Meningiomatosis)
Most patients develop a single meningioma, but approximately 5–10% of patients present with multiple tumors. This condition is referred to as multiple meningiomas or meningiomatosis.
Multiple meningiomas may occur sporadically, but they are particularly associated with neurofibromatosis type 2, in which patients may develop numerous tumors along the meninges.
Management of multiple meningiomas is individualized. In many cases only the symptomatic or growing tumors are treated, while the remaining lesions are monitored with periodic imaging.
How Meningiomas Grow and Affect the Brain
Meningiomas usually grow slowly over many years. Because they arise outside the brain tissue, they primarily damage the brain through compression rather than invasion.
As the tumor enlarges, it gradually presses on adjacent brain structures. This pressure interferes with normal neuronal activity and may lead to neurological deficits.
Another important mechanism is peritumoral brain edema, a form of swelling in the surrounding brain tissue caused by leakage of fluid from nearby blood vessels. This swelling increases intracranial pressure and often worsens symptoms.
Together with the tumor itself, this edema can produce a mass effect, meaning that the expanding lesion compresses and displaces normal brain structures. Because the skull is a rigid, closed cavity with very limited space for expansion, increasing pressure may force parts of the brain to shift from their normal position. In severe cases, brain tissue can be pushed through natural openings within the skull, a condition known as brain herniation. Herniation represents a dangerous stage of mass effect in which displaced brain structures may compress vital centers in the brainstem responsible for consciousness, breathing, and circulation.
Large tumors may also compress nearby arteries or veins, disrupting normal blood circulation in the brain. In certain locations, tumors may obstruct the normal circulation of cerebrospinal fluid, leading to hydrocephalus.
Even though most meningiomas do not invade brain tissue, prolonged compression may still cause permanent neurological damage if the tumor becomes very large.

Image: Brain Herniations — An extradural hematoma (the same is also for meningioma + brain swelling) creates a mass effect, pushing parts of the brain into narrow spaces where they normally do not belong. In these tight areas, the pressure can compromise vital parts of the brain, including the brainstem, which controls breathing and consciousness. Among the different types of herniation, transtentorial (uncal) herniation is the most clinically significant pattern because it is the one most often associated with sudden deterioration.
Studies following patients with untreated meningiomas have shown that a substantial proportion of tumors remain stable for long periods. Approximately 30–35% of meningiomas show no measurable growth during long-term imaging follow-up. Among tumors that do grow, the increase in size is usually slow and gradual, often measured in millimeters per year rather than rapid expansion.
Symptoms According to Tumor Location
The symptoms caused by meningiomas depend largely on their anatomical location. Headache is also a common symptom, which can either be a direct result of the meningioma or merely an incidental symptom that led to the MRI scan where the meningioma was discovered.
• Convexity meningiomas often produce seizures because they irritate the surface of the brain. Patients may also develop progressive weakness or numbness affecting the arm and/or leg on the opposite side of the body.
• Parasagittal meningiomas (tumors located along the midline of the skull) frequently affect the brain regions responsible for opposite leg movement. Patients may gradually develop weakness or stiffness of the legs and difficulty walking.
• Sphenoid wing meningiomas may affect structures responsible for vision and eye movement. Patients may notice progressive visual loss, double vision, or sometimes bulging of one eye.
• Olfactory groove meningiomas often cause gradual loss of smell and may later (when meningioma significantly enlarges) produce personality changes due to pressure on the frontal lobes with brain edema.
• Tuberculum sellae meningiomas commonly produce progressive visual disturbances because they compress the optic nerves and optic chiasm (the junction where the optic nerves from both eyes cross).
• Tentorial meningiomas may produce dizziness, imbalance, or coordination problems due to their compression on the cerebellum.
• Cerebellopontine angle (CPA) meningiomas frequently cause hearing loss, tinnitus, or balance disturbances because they lie near the cranial nerves responsible for hearing and equilibrium.
Less common tumors may produce more specific symptoms:
• Cavernous sinus meningiomas may cause double vision and facial numbness due to involvement of cranial nerves controlling eye movement.
• Foramen magnum meningiomas may cause neck pain, progressive weakness, and walking difficulty due to compression of the upper spinal cord.
Diagnosis of Meningioma
The most important diagnostic test is MRI of the brain with contrast.
During this examination, the patient lies inside the MRI scanner while magnetic fields generate highly detailed images of the brain. A contrast agent injected through a vein highlights tumor tissue.
MRI allows physicians to determine:
• tumor size
• precise location
• relationship to cranial nerves and blood vessels
• presence of surrounding brain edema
Meningiomas typically appear as well-defined tumors located outside the brain tissue, attached to the dura, often accompanied by a characteristic imaging feature known as the dural tail.
The final diagnosis is confirmed through histopathological analysis after surgery or biopsy.
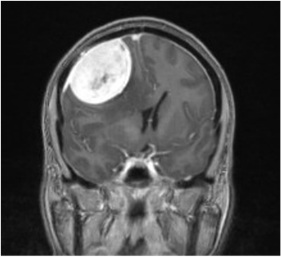
Image: Brain MRI showing a bright meningioma (image after applying contrast) in the right parietal region, causing a significant mass effect (compression) on the brain due to its size and surrounding brain edema. In the inferior extension of the tumor, there is a bright dural thickening called the ‘dural tail sign’.
However, several other conditions may produce similar MRI findings and must be considered in the differential diagnosis.
These include:
• dural metastases, which may mimic meningiomas when metastatic cancer spreads to the meninges
• hemangiopericytoma (solitary fibrous tumor), a rare dural tumor that can appear very similar radiologically but behaves more aggressively
• schwannomas, particularly in locations such as the cerebellopontine angle, where they may resemble meningiomas on imaging
• lymphoma involving the dura
Because imaging findings may overlap, the final diagnosis is often confirmed by histopathological examination of the tumor after surgical removal or biopsy.
Although MRI is the main imaging method used to diagnose meningiomas, other techniques may occasionally provide additional information. CT scans are particularly useful for evaluating changes in the skull bone, such as hyperostosis (the growth of bone in contact with meningioma) or calcification within the tumor. In selected cases, vascular imaging such as CT angiography or MR angiography may also be performed to assess the relationship of the tumor to major arteries or venous sinuses when surgical planning requires more detailed evaluation. Conventional catheter angiography (DSA) is now rarely required and is mainly performed when preoperative tumor embolization is being considered.
Monitoring Without Treatment: When Meningiomas are Only Observed
Not all meningiomas require immediate treatment.
Approximately 30–50% of newly diagnosed meningiomas are initially managed with active surveillance rather than immediate surgery. Among incidentally discovered tumors, however, observation without surgery is chosen in the majority of patients, often around 60–80%, particularly when the tumor is small and not causing symptoms.
Monitoring is usually recommended when:
- the tumor causes no neurological symptoms, especially if it is small
- imaging shows little or no growth over time
- the tumor is not compressing critical brain structures
- there is little or no surrounding brain edema
- the patient is elderly or has serious medical conditions
On imaging studies, meningiomas that are partially or extensively calcified often represent tumors with long-standing slow growth, and this finding may further support a decision for observation rather than immediate surgery. Follow-up generally involves MRI examinations every 6–12 months initially.
Symptomatic Treatment
Medications are often used to control complications caused by the tumor.
• Brain swelling (edema) is commonly treated with corticosteroids, most often dexamethasone, which reduces edema (brain swelling) in the surrounding brain tissue.
• Seizures are treated with antiepileptic medications, such as levetiracetam or other modern antiseizure drugs.
These medications stabilize the patient but do not eliminate the tumor itself.
Meningioma and Epilepsy
Seizures may sometimes be the first symptom of a meningioma, particularly when the tumor is located on the convexity of the brain or near the cerebral cortex.
However, it is important to understand that not every seizure in a patient with a meningioma is necessarily caused by the tumor. Epilepsy is relatively common in the general population, and the coexistence of a small incidental meningioma does not automatically mean that the tumor is responsible for the seizures.
For this reason, physicians must carefully evaluate whether the tumor is actually the source of epileptic activity. This assessment usually includes:
• analysis of tumor location relative to the cerebral cortex
• evaluation of peritumoral brain edema
• correlation between EEG findings and the tumor region
• consideration of other possible causes of epilepsy
When seizures are clearly related to the tumor, surgical removal of the meningioma often significantly reduces seizure frequency, and in some patients seizures may stop completely.
Antiepileptic medications are usually used to control seizures before and for some period after surgery.
Surgical Treatment of Meningiomas
Surgery remains the primary treatment for symptomatic or progressively growing meningiomas. The procedure is performed through a craniotomy, which involves temporarily removing a portion of the skull to access the tumor.
In most cases the operation proceeds through several stages:
• Skin incision and craniotomy
The scalp is opened using a carefully planned incision. Depending on the location of the tumor, the incision may be linear, curved, or horseshoe-shaped. Whenever possible, it is placed within the hairline for cosmetic reasons. In most modern neurosurgical procedures the hair does not need to be completely shaved. A small bone flap is then created to expose the dura mater covering the brain or the tumor.
• Opening of the dura
The dura mater is carefully opened to expose the tumor and the surrounding brain structures.
• Internal tumor debulking
Whenever possible, the surgeon first attempts to control or detach the tumor from its dural attachment, because meningiomas receive much of their arterial blood supply from vessels entering through the dura. Early management of this attachment reduces bleeding during the procedure. The tumor is then reduced from the inside, most often using an ultrasonic aspirator (CUSA). This internal debulking decreases tumor volume and pressure, making subsequent dissection from the surrounding brain, nerves, and blood vessels safer.
• Microsurgical dissection
The tumor is gradually separated from the surrounding brain tissue, cranial nerves, and blood vessels under high magnification (neurosurgical microscope).
• Tumor removal
The tumor is usually removed in several pieces, allowing safe separation from surrounding structures.
• Treatment of the dural attachment
Because meningiomas arise from the dura, the involved portion of the dura is usually removed together with the tumor whenever possible to reduce the risk of recurrence. When complete removal is not safe, the dural base may be coagulated. If a segment of dura must be removed, the defect is typically reconstructed using a dural graft to restore a watertight barrier around the brain. This graft may be created from the patient’s own tissue (such as periosteum elevated from the skull during the operation or muscle fascia) or from biocompatible artificial dural substitutes specifically designed for neurosurgical reconstruction.
• Removal of infiltrated bone (when present)
Some meningiomas cause thickening or infiltration of the adjacent skull bone (hyperostosis). In such cases the abnormal bone may be drilled away, and occasionally a larger bone segment must be removed and at the same surgery or later, reconstructed with cranioplasty.
• Dural reconstruction and closure
After tumor removal the dura is reconstructed using a dural graft if necessary. The bone flap is replaced (or reconstructed if bone was removed), and the scalp is closed.

Image: The image illustrates a craniotomy. Both the skin incision and the skull opening are performed within the hair-bearing area of the scalp. The dura is opened to expose the tumor or the brain as part of the surgical approach to the tumor. After the procedure, the bone flap is secured and the scalp is reconstructed, ensuring no cosmetic defect remains after healing.
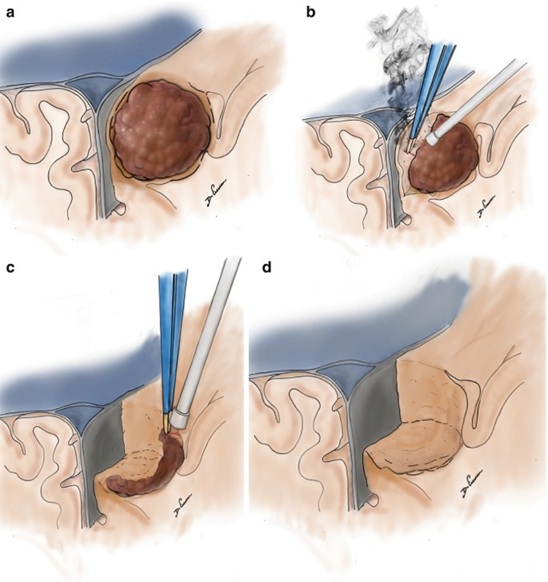
Image: Stages of surgical removal of a meningioma. After craniotomy and opening of the dura, image (a) shows the dark brown meningioma. Image (b) illustrates its separation from the brain, blood vessels, and other normal tissues, followed by its piecemeal reduction. Image (c) shows the removal of the remaining peripheral parts of the meningioma. Image (d) shows the condition after the meningioma has been completely removed.
Modern Surgical Technologies
Modern neurosurgery employs several technologies to increase precision and safety.
• Neuronavigation systems function as intraoperative GPS, allowing the surgeon to navigate within the skull with millimeter accuracy.
• Ultrasonic aspirators (CUSA) fragment and aspirate tumor tissue while preserving surrounding blood vessels and nerves.
• Intraoperative neurophysiological monitoring allows continuous monitoring of nerve function during surgery, helping avoid surgical damage to important nerves.
These technologies significantly reduce the risk of neurological injury.
In selected cases, surgeons may perform preoperative embolization before surgical removal of a meningioma. This procedure involves inserting a catheter into arteries supplying the tumor and injecting materials that reduce blood flow to the tumor in order to decrease intraoperative bleeding. Embolization is mainly considered for large, highly vascular meningiomas supplied by branches of the external carotid artery. Today it is used in a relatively small proportion of cases because the procedure itself may carry risks such as stroke, cranial nerve injury, or unintended embolization of normal vessels, and advances in modern microsurgical techniques have reduced the need for routine embolization.
Endoscopic Surgery for Skull Base Meningiomas
In addition to classical microsurgical craniotomy, some meningiomas located at the base of the skull can be removed using endoscopic techniques. These procedures access the tumor through natural anatomical corridors, most commonly through the nasal cavity, avoiding large external incisions and extensive brain retraction.
This approach is most often used for selected tumors located in the midline skull base, particularly:
• Tuberculum sellae meningiomas
• Planum sphenoidale meningiomas
• Olfactory groove meningiomas
• certain clival and anterior skull base meningiomas
In these operations the surgeon inserts a rigid endoscope through the nostrils. The endoscope contains a camera and light source that provide a high-magnification panoramic view of the surgical field.
The basic steps of endoscopic meningioma surgery usually include:
• Endonasal access through the nasal cavity
• removal of a portion of the skull base bone to expose the dura
• opening of the dura covering the tumor
• internal debulking of the tumor
• careful separation of the tumor from the optic nerves, blood vessels, and surrounding structures
• removal of the tumor in fragments
• reconstruction of the skull base defect, often using vascularized tissue flaps to prevent cerebrospinal fluid leakage
Because the surgical corridor comes from below rather than from above the brain, this approach may avoid significant brain retraction.
However, only a minority of meningiomas are suitable for endoscopic removal. Current surgical series suggest that approximately 10–15% of skull base meningiomas may be appropriate candidates for endoscopic approaches, depending on tumor size, location, and relationship to surrounding arteries and nerves.
Advantages of Endoscopic Surgery
Endoscopic skull base surgery offers several potential advantages:
• no large scalp incision and no craniotomy
• minimal or no brain retraction
• direct midline access to tumors beneath the brain
• improved visualization of deep skull base structures
These advantages can result in shorter recovery times and less manipulation of normal brain tissue in carefully selected patients.
Limitations and Risks
Despite these benefits, endoscopic surgery is not suitable for many meningiomas.
Important limitations include:
• difficulty removing large tumors extending laterally
• limited control of tumors that encase major arteries
• challenges in removing extensive dural attachment or infiltrated bone
• increased risk of cerebrospinal fluid leakage if skull base reconstruction is not adequate
For these reasons, microsurgical craniotomy remains the most common treatment for the majority of meningiomas, particularly those located on the convexity or along the brain surface.
The choice between microsurgical and endoscopic approaches depends on multiple factors, including tumor location, size, vascular relationships, and the experience of the surgical team.
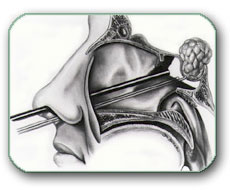
Image: Many skull base tumors, such as meningiomas, pituitary adenomas, and others, can be removed without a craniotomy using an endoscopic endonasal approach.
Extent of Tumor Removal — Simpson Classification
The completeness of tumor removal is classified using the Simpson grading system.
• Simpson Grade I — complete removal of the tumor and its dural attachment
– recurrence risk approximately 5–10% over long-term follow-up
– probability of needing another intervention ~3–5%
• Simpson Grade II — tumor removed, dural attachment coagulated
– recurrence risk approximately 10–20%
– probability of further treatment ~5–10%
• Simpson Grade III — tumor removed but dura left intact
– recurrence risk approximately 20–30%
– probability of additional treatment ~10–20%
• Simpson Grade IV — subtotal removal
– recurrence risk approximately 40–60%
– additional treatment (surgery or radiotherapy) often required in 30–50%
• Simpson Grade V — biopsy or decompression only
– tumor progression expected in most patients (>80–90%)
– further definitive treatment usually necessary
The Simpson grade strongly influences the likelihood of tumor recurrence.
Radiation Therapy for Meningiomas
Radiation therapy is used when complete surgical removal is not possible, when tumors recur, or when a small residual tumor remains after surgery. It may also be considered for small meningiomas that demonstrate clear growth during imaging follow-up, particularly when surgery carries increased risk.
Typical radiation doses for meningiomas are:
• 50–54 Gy in fractionated radiotherapy
• 12–16 Gy delivered in a single session in stereotactic radiosurgery (e.g., Gamma Knife)
Radiation therapy can effectively stop tumor growth in many patients. Modern radiation techniques provide long-term tumor control in approximately 85–95% of benign meningiomas, especially when small tumors are treated with stereotactic radiosurgery.
In modern clinical practice, approximately 10–15% of newly diagnosed meningiomas are treated primarily with radiation therapy rather than surgery. This approach is usually chosen for small tumors located in surgically difficult areas, or in situations where the patient prefers a non-surgical treatment option after discussion of the risks and benefits.
Radiosurgery is generally most suitable for tumors smaller than about 2.5–3 cm that are not causing significant compression of the brain.
However, radiation treatment is not appropriate for all meningiomas. Even relatively small tumors may be unsuitable for radiosurgery if they lie very close to structures that tolerate only limited radiation exposure.
Tumors in the following locations are often poor candidates for radiosurgery:
• tuberculum sellae and planum sphenoidale meningiomas, which lie close to the optic nerves and optic chiasm
• optic nerve sheath meningiomas
• tumors directly contacting the brainstem, such as some clival or petroclival meningiomas
• certain cavernous sinus meningiomas extending toward the optic pathways
In tumors located close to critical structures such as the optic nerves, optic chiasm, or the pituitary stalk, single-session radiosurgery may carry a higher risk of radiation injury to these structures. In such situations, fractionated radiation is often used to reduce this risk, because the total radiation dose is divided into several smaller treatments that allow surrounding tissues to recover between sessions.
Fractionated radiation may be delivered either as stereotactic treatment in 3–5 sessions (typically about 5–7 Gy per fraction, total 21–30 Gy) or as conventionally fractionated radiotherapy over several weeks (usually about 1.8–2 Gy per fraction to a total dose of approximately 50–54 Gy).
In selected patients with small tumors located near the optic pathways, radiation therapy may sometimes be used instead of surgery, particularly when the risk of surgical complications is considered high. However, in other cases surgical removal may still be the preferred option, especially when the tumor produces significant compression of the optic nerves or when decompression is required.
The final treatment decision is usually made by a multidisciplinary team, typically including a neurosurgeon, radiation oncologist, and neuroradiologist, after careful evaluation of tumor size, location, patient age, symptoms, and overall medical condition.
Planned Subtotal Resection Followed by Radiation
During surgery, the primary goal is usually complete tumor removal, including its dural attachment. However, in some cases a portion of the tumor may be firmly adherent to critical blood vessels or cranial nerves. Attempting to remove this portion could cause severe neurological injury.
In these situations the surgeon may intentionally leave a small residual tumor to protect important structures. This strategy, known as planned subtotal resection, is followed by stereotactic radiosurgery to control the remaining tumor. Modern series suggest that this combined strategy is used in approximately 10–15% of meningioma operations, particularly for tumors located near the cavernous sinus, skull base arteries, or cranial nerves.
This approach allows surgeons to balance maximal tumor control with preservation of neurological function.
Recurrence of Meningiomas
Recurrence of Meningiomas
The likelihood of recurrence depends on tumor grade and completeness of removal.
• After complete removal of benign meningiomas, recurrence occurs in approximately 5–10% of cases over 10–15 years.
• After subtotal removal, recurrence rates may reach 20–40%.
• Atypical meningiomas recur in approximately 30–40% of cases.
• Malignant meningiomas may recur in 50–80% of patients.
Because recurrence may occur many years after treatment, long-term MRI follow-up is essential.
When a meningioma recurs, treatment decisions depend on several factors:
• tumor growth rate
• tumor size
• location
• previous treatments
• patient symptoms
• histological grade
When MRI findings are uncertain, specialized PET imaging using radiotracers that bind to somatostatin receptors in the tumor may sometimes help identify recurrent meningioma, because many meningiomas show strong uptake on these scans.
Not all recurrences require immediate treatment. Some can be safely monitored, while others require additional therapy.
Observation of Small Recurrences
Small recurrent meningiomas that show minimal or no growth may initially be managed with MRI surveillance.
Observation is most commonly chosen when:
• the tumor is small
• the patient has no neurological symptoms
• imaging shows slow or stable growth
• the recurrence is located in a high-risk surgical area
Follow-up usually involves MRI every 6–12 months to monitor tumor growth.
Repeat Surgery
Surgical reoperation is considered when:
• the recurrent tumor causes neurological symptoms
• imaging shows significant tumor growth
• the tumor is accessible for safe removal
• mass effect on the brain becomes clinically important
Repeat surgery aims to remove the recurrent tumor and its dural attachment whenever possible.
However, reoperation may be more technically demanding because:
• scar tissue from the previous surgery may be present
• important blood vessels or nerves may already be displaced
• bone reconstruction may have altered anatomy
For these reasons, surgical decisions must carefully balance potential benefit and risk.
Radiation Therapy for Recurrence
Radiation therapy is frequently used for recurrent meningiomas, particularly when complete surgical removal is not feasible.
Radiation may be recommended when:
• residual tumor remains after surgery
• recurrence occurs after previous surgery
• the tumor lies in a surgically difficult skull base location
• the tumor shows atypical or malignant histology
Two main radiation approaches are used:
• fractionated radiotherapy, typically delivering 50–54 Gy
• stereotactic radiosurgery, usually delivering 12–16 Gy in a single focused treatment
Radiation therapy can effectively control tumor growth in a large proportion of patients.
Treatment Strategy by Tumor Grade
Management also depends strongly on the WHO tumor grade.
• WHO grade I meningiomas. After complete surgical removal, most patients require only periodic MRI follow-up. If the tumor recurs during follow-up, management may include continued observation, repeat surgery, or stereotactic radiosurgery, depending on the rate of growth and clinical symptoms.
• WHO grade II (atypical) meningiomas. These tumors recur more frequently. Postoperative radiotherapy is often recommended, particularly after incomplete tumor removal, although some patients may be managed with close MRI follow-up after complete resection.
• WHO grade III (malignant) meningiomas. These aggressive tumors typically require postoperative radiotherapy regardless of the completeness of surgical removal, together with close imaging follow-up.
Long-Term Monitoring
Because meningiomas may recur many years after treatment, long-term follow-up is essential.
Typical surveillance includes:
• annual MRI for several years after treatment
• longer imaging intervals if the tumor remains stable
Early detection of recurrence allows treatment before significant neurological damage develops.
Treatment Decision Summary for Meningioma
Treatment decisions for meningioma usually follow several general principles.
1. Before treatment
If the tumor is small, causes no symptoms, and does not significantly compress the brain, MRI monitoring is often the safest first step.
If the tumor causes neurological symptoms, produces significant mass effect or edema, or shows documented growth on follow-up imaging, active treatment is more often recommended.
2. Choosing the main treatment
Surgery is usually preferred when the patient is in good overall condition and the tumor can be removed with acceptable neurological risk.
Radiosurgery or fractionated radiotherapy may be considered when surgery carries higher risk, when the tumor is small and located in a surgically difficult region, or when the patient prefers radiation treatment after discussion of the available options.
3. After surgery
WHO Grade I + complete removal: MRI follow-up is usually sufficient.
WHO Grade I + residual tumor: follow-up or radiosurgery/radiotherapy may be considered depending on tumor growth and location.
WHO Grade II: postoperative radiotherapy is usually recommended after incomplete tumor removal. After complete resection, some patients may be managed with MRI follow-up or radiotherapy depending on recurrence risk.
WHO Grade III: surgery is usually followed by radiotherapy regardless of the completeness of tumor removal, together with close imaging follow-up.
This is a simplified overview. In real clinical practice, treatment decisions also depend on tumor size, location, growth rate, surrounding brain edema, proximity to the optic nerves or brainstem, patient age, and overall neurological condition.
Experimental and Targeted Therapies
Several medications have been studied for recurrent or progressive meningiomas when surgery and radiotherapy are no longer sufficient. These include bevacizumab, which targets tumor blood vessel growth, as well as drugs acting on molecular pathways such as AKT or SMO inhibitors. Somatostatin-receptor–based treatments such as octreotide and combinations including everolimus have also been investigated. However, current evidence remains limited, and surgery and radiation therapy remain the main treatments for most meningiomas. In recent years, researchers have been studying targeted drugs for selected meningiomas with specific molecular alterations such as NF2, AKT1, or SMO mutations. Some medications, including inhibitors of growth signaling pathways or anti-angiogenic drugs, are being evaluated in clinical trials. However, at present there is no established drug therapy that reliably controls most meningiomas, and surgery and radiotherapy remain the main treatments.
When Expert Opinions May Differ
In many patients diagnosed with meningioma, different specialists may recommend different treatment strategies. This situation is common in neurosurgery and does not necessarily indicate that one opinion is correct while another is wrong.
Treatment decisions for meningiomas depend on multiple clinical factors, including:
• tumor size
• tumor location
• growth rate observed on MRI
• presence of surrounding brain edema or mass effect
• patient age and overall health
• presence or absence of neurological symptoms
• relationship of the tumor to important arteries, veins, or cranial nerves
• tumor grade if histological diagnosis is already known
Because these factors interact in complex ways, reasonable specialists may arrive at different conclusions regarding the safest management strategy.
Observation vs. Early Surgery
One of the most common differences in opinion occurs when a meningioma is discovered incidentally on MRI and the patient has no symptoms. Some specialists recommend active surveillance, particularly when the tumor is small and shows no signs of growth. Others may recommend early surgery, especially if the tumor is located in an area where future growth could threaten important neurological structures. Both approaches may be appropriate depending on the individual clinical situation.
Differences in Surgical Strategy
Even when surgery is recommended, surgeons may disagree about the optimal surgical approach. In some cases a surgeon may aim for complete removal including the dural attachment, while another may prefer a more conservative removal if the tumor lies close to important blood vessels or cranial nerves. Similarly, some skull base meningiomas may be treated using microsurgical craniotomy, while others may be considered candidates for endoscopic skull base surgery.
Surgery vs. Radiation Therapy
Another area where opinions may differ involves the use of radiation therapy. Some specialists recommend surgical removal first, followed by radiation only if residual tumor remains. Others may recommend primary stereotactic radiosurgery, particularly for small tumors located in surgically complex areas such as the cavernous sinus or near the optic apparatus. Decisions between surgery and radiation therapy may also depend on tumor size, location, growth rate, proximity to critical neurological structures such as the optic nerves or brainstem, and the expected surgical risk for the individual patient.
When Tumor Location Near Critical Structures Changes the Treatment Plan
In some cases, the most important factor influencing differences in recommendations is the tumor’s relationship to critical anatomical structures.
When a meningioma is located near major venous sinuses, the optic nerves, brainstem, or cranial nerves, treatment decisions become significantly more complex. The key issue is not only whether the tumor can be removed, but whether complete removal is safe without causing permanent neurological damage.
In these situations, some specialists may recommend more conservative surgery or partial removal followed by radiation, while others may favor more aggressive resection or primary radiosurgery, depending on how they assess the balance between tumor control and neurological risk.
Why a Second Opinion Can Be Helpful
Because treatment decisions depend on many individual variables, a second neurosurgical opinion can help clarify:
• the urgency of treatment
• whether observation is safe
• whether surgery or radiation is preferable
• what degree of tumor removal is realistically achievable
• the expected neurological risks of treatment
Careful review of MRI images and clinical history often allows specialists to explain why different recommendations may exist and which option is most appropriate for a specific patient.
Request Meningioma Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Being told that an MRI has revealed a meningioma often raises difficult and sometimes conflicting questions:
Is the tumor dangerous?
Should it be monitored or removed surgically?
Is radiosurgery (such as Gamma Knife) a safer option?
What is the risk of neurological deterioration or recurrence?
An independent neurosurgical second opinion may help clarify the urgency of treatment,
expected neurological outcome, likelihood of tumor growth, and the safest balance between observation,
surgical removal, and radiation therapy based on MRI findings, tumor location, biological behavior,
and the patient’s overall neurological condition.
- ✔ Send a brief message describing your current symptoms and the key findings from your MRI or CT report
- ✔ You will receive a reply within 24 hours explaining whether an online consultation is appropriate and which documentation is required
- ✔ Priority cases: rapidly worsening neurological symptoms, newly diagnosed tumors in critical brain regions, proposed urgent surgery, or conflicting specialist recommendations — write PRIORITY in your first message
- ✔ MRI images (DICOM format), radiology reports, and relevant medical documentation can be reviewed to assess tumor size, location, surrounding brain edema, and possible treatment strategies
- ✔ During consultation, we explain whether observation, microsurgical removal, radiosurgery, or combined treatment is most appropriate — including expected neurological risks and up to 10 days of follow-up clarification
Consultation fees typically range from $180–250, depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This corresponds to typical international specialist telehealth neurosurgical second-opinion services.
How Meningioma Prognosis Depends on Location, Grade, and Extent of Removal
The prognosis of meningioma depends primarily on three major factors: the biological grade of the tumor, its anatomical location, and the extent to which it can be safely removed.
In general, WHO Grade I meningiomas have the most favorable prognosis. They usually grow slowly, and when they are completely removed together with their dural attachment, long-term tumor control is often excellent. By contrast, atypical and malignant meningiomas have a higher risk of recurrence, even after apparently complete surgery, and therefore usually require closer follow-up and often additional radiation therapy.
Tumor location is equally important. Meningiomas located on the convexity of the brain are often associated with a better surgical prognosis, because they can usually be approached more directly and separated more safely from critical neurovascular structures. In contrast, skull base meningiomas may lie in close contact with the optic nerves, the brainstem, major arteries, venous sinuses, or multiple cranial nerves, making surgery technically more demanding. In such cases, the surgeon must often choose between more radical removal and preservation of neurological function. When residual tumor remains near critical structures such as the optic nerves, optic chiasm, or the pituitary stalk, postoperative radiotherapy may sometimes be limited by the risk of radiation injury to the visual pathways. In these situations, careful MRI surveillance is often preferred, and treatment is considered only if clear tumor growth is documented.
For this reason, the extent of tumor removal strongly influences long-term outcome. The smaller the amount of residual tumor left behind, the lower the probability of recurrence. However, in modern neurosurgery, the best result does not always mean the most aggressive resection. In some patients, intentionally leaving a very small tumor remnant densely adherent to critical vessels or nerves may provide a better overall outcome than attempting complete removal at the cost of permanent neurological damage.
In practical terms, prognosis is best in patients with benign meningiomas located in surgically favorable regions and removed completely. It is generally less favorable in higher-grade tumors, skull base locations, and in cases where only subtotal removal is possible because of the risk to vital structures.
Can a Meningioma Become Life-Threatening?
Yes, a meningioma can become life-threatening, although this is not the usual course in most patients.
Most meningiomas are slow-growing tumors, and many remain stable for years without causing major neurological problems. However, if the tumor becomes large enough, it may produce severe pressure on the brain, significant surrounding edema, obstruction of cerebrospinal fluid pathways, or progressive compression of the brainstem, optic system, or major blood vessels. In such situations, the danger does not arise only from the biological nature of the tumor itself, but from its mass effect on vital brain structures.
A meningioma may therefore become life-threatening when it causes marked intracranial pressure elevation, brain herniation, hydrocephalus, severe brainstem compression, or repeated seizures with progressive neurological deterioration. This risk is higher in large tumors, tumors located in confined skull base regions, and in more aggressive histological forms such as atypical or malignant meningioma.
For this reason, even though meningiomas are often described as benign tumors, they should never be considered harmless solely on the basis of histological grade. Their real clinical significance depends on tumor size, location, rate of growth, and the effect they produce on surrounding brain structures.
Frequently Asked Questions About Meningioma
Should a meningioma be monitored or treated immediately?
Not every meningioma requires immediate treatment. Many small meningiomas, especially those discovered incidentally on MRI, can be monitored safely when they cause no neurological symptoms, show little or no growth, do not compress critical brain structures, and have little or no surrounding brain edema. Observation is often chosen in the majority of incidental meningiomas, particularly when the tumor is small and stable. Treatment becomes more likely when the tumor causes symptoms, shows documented growth, produces significant mass effect or edema, or lies near structures where future growth could threaten neurological function. The safest decision is individualized and depends on tumor size, location, growth rate, symptoms, edema, patient age, and overall neurological condition.
How do doctors decide whether a meningioma requires surgery?
Doctors decide whether a meningioma requires surgery by combining several factors rather than following one automatic rule. Surgery is usually preferred when the tumor causes neurological symptoms, produces significant mass effect, creates surrounding brain edema, shows clear growth on MRI, or can be removed with acceptable neurological risk. Tumor location is especially important because meningiomas near the optic nerves, brainstem, major arteries, venous sinuses, or cranial nerves may carry higher surgical risk. The decision also depends on patient age, general health, tumor grade if known, and whether radiation therapy could provide safer tumor control. In modern neurosurgery, the goal is not only tumor removal, but safe tumor control while preserving neurological function.
Can a meningioma be safely monitored for years without treatment?
Yes. Many meningiomas can be monitored for years without treatment, especially when they are small, asymptomatic, and not compressing critical structures. Studies of untreated meningiomas show that a substantial proportion remain stable for long periods, and some show no measurable growth during follow-up. When tumors do grow, the increase is often slow and gradual, measured in millimeters per year rather than rapid expansion. Monitoring usually involves MRI every 6–12 months initially, with longer intervals if the tumor remains stable. Observation is especially reasonable when the tumor is calcified, causes no edema, and the patient has no neurological symptoms. Treatment is reconsidered if growth, edema, symptoms, or mass effect appears.
What happens if surgery for a meningioma is delayed?
Delaying surgery for a meningioma may be safe when the tumor is small, stable, and not causing symptoms or dangerous compression. In those cases, MRI monitoring is often the safest first step. Delay becomes risky when the tumor is already producing neurological symptoms, significant mass effect, surrounding brain edema, hydrocephalus, visual compression, seizures, progressive weakness, or documented growth. Although most meningiomas grow slowly, prolonged compression can sometimes cause permanent neurological damage, especially when the tumor becomes large or lies near the optic nerves, brainstem, venous sinuses, cranial nerves, or motor areas. The key question is not simply how long the tumor has been present, but whether waiting increases the risk of irreversible deficit or more complex treatment later.
Can a small meningioma suddenly become dangerous?
A small meningioma usually does not suddenly become dangerous, especially if it is incidental, stable on MRI, and not causing edema or compression. Many small tumors remain silent for years. However, size alone does not define risk. A small meningioma may be clinically important if it is located near critical structures such as the optic nerves, optic chiasm, cavernous sinus, brainstem, cranial nerves, or cerebrospinal fluid pathways. Even limited growth in these regions can create visual problems, cranial nerve symptoms, hydrocephalus, or difficult treatment decisions. A tumor may also become more relevant if it begins to grow, causes edema, or produces seizures. Therefore, MRI location and biological behavior matter as much as diameter.
Can you die from a benign meningioma?
Yes, but this is uncommon and usually does not happen because the meningioma is “cancerous.” A benign meningioma can become life-threatening if it grows large enough to cause severe mass effect, brain swelling, hydrocephalus, brain herniation, or compression of critical structures such as the brainstem, optic pathways, major blood vessels, or cranial nerves. Most benign meningiomas grow slowly and many remain stable for years, but “benign” does not always mean harmless. The real danger depends on tumor size, location, growth rate, surrounding edema, and the effect on nearby brain structures. This is why even benign meningiomas require individualized interpretation of MRI findings and symptoms.
Does a calcified meningioma usually mean slow growth?
A calcified meningioma often suggests a long-standing and relatively slow-growing tumor, but calcification alone does not prove that the tumor is harmless or that it will never grow. Calcification is one MRI or CT feature that may support observation when the meningioma is small, asymptomatic, stable, and not causing edema or compression of critical structures. However, treatment decisions should not be based on calcification alone. Doctors also consider tumor size, location, growth on previous imaging, surrounding brain edema, mass effect, neurological symptoms, patient age, and relationship to important structures such as the optic nerves, brainstem, venous sinuses, or cranial nerves.
How does meningioma location change treatment decisions?
Location strongly changes meningioma treatment decisions because it determines symptoms, surgical difficulty, and the risk of neurological injury. Convexity meningiomas are often more accessible and may be separated more safely from critical structures. Skull base meningiomas are more complex because they may lie near the optic nerves, brainstem, major arteries, venous sinuses, pituitary stalk, or cranial nerves. Parasagittal tumors may involve the superior sagittal sinus, while cavernous sinus, petroclival, and foramen magnum meningiomas can be technically demanding. In some locations, complete removal may be unsafe, so planned subtotal removal followed by monitoring or radiation may be preferred. The best treatment is therefore based not only on tumor size, but on anatomy.
Why do some meningiomas cause symptoms while others remain silent?
Some meningiomas remain silent because they are small, grow slowly, and do not compress important brain regions, cranial nerves, blood vessels, or cerebrospinal fluid pathways. Others cause symptoms because their location makes even gradual growth clinically important. Convexity meningiomas may irritate the brain surface and cause seizures. Parasagittal tumors may affect leg movement and walking. Sphenoid wing or tuberculum sellae meningiomas may compress visual pathways. CPA meningiomas may cause hearing loss, tinnitus, or balance problems. Large tumors may also create edema and mass effect, increasing intracranial pressure and worsening symptoms. Therefore, symptoms depend less on the word “benign” and more on where the tumor grows and what it compresses.
How do doctors know whether headaches or seizures are actually caused by the meningioma?
Doctors do not assume automatically that every headache or seizure is caused by a meningioma. The connection must be judged from tumor location, edema, cortical irritation, imaging findings, and the patient’s clinical pattern. Seizures are more likely to be related to the tumor when the meningioma lies on the convexity or near the cerebral cortex, especially if there is peritumoral edema and EEG findings match the tumor region. Headaches may be related when the tumor is large, produces mass effect, increases intracranial pressure, or causes edema. A small incidental meningioma may coexist with unrelated headaches or epilepsy. This is why careful clinical and imaging correlation is necessary before deciding that the tumor is responsible.
What does surrounding brain edema mean in meningioma and why is it important?
Surrounding brain edema means swelling in the brain tissue around the meningioma. Although most meningiomas grow outside the brain and compress rather than invade it, edema can develop because of fluid leakage from nearby blood vessels. This swelling adds to the tumor’s own mass effect and may worsen symptoms such as headache, seizures, weakness, personality changes, or raised intracranial pressure. Edema is important because the combined volume of tumor and swelling can compress and displace normal brain structures inside the closed skull. In severe cases, this may contribute to brain shift or herniation. Edema also influences treatment decisions, because a tumor that might otherwise be monitored may require active treatment if swelling becomes clinically significant.
Can a meningioma cause hydrocephalus or dangerous pressure on the brain?
Yes. A meningioma can cause dangerous pressure when it becomes large, produces significant surrounding edema, creates mass effect, or obstructs cerebrospinal fluid pathways. Because the skull is a rigid closed cavity, an expanding tumor and edema may push normal brain structures from their usual position. In severe cases, this displacement can lead to brain herniation, where vital structures such as the brainstem may be compressed. Some meningiomas, depending on location, may also obstruct normal CSF circulation and lead to hydrocephalus. This is more concerning when the tumor lies near the posterior fossa, skull base, or ventricular pathways. The danger comes not only from tumor biology, but from pressure on critical brain structures.
How is meningioma surgery performed and what does craniotomy involve?
Meningioma surgery is usually performed through a craniotomy, which means temporarily removing a portion of the skull to reach the tumor. The scalp incision is planned according to tumor location and is often placed within the hairline for cosmetic reasons. The bone flap is opened, the dura is exposed, and the dura is carefully opened to reach the tumor. The surgeon usually reduces the tumor from the inside using microsurgical techniques and often an ultrasonic aspirator, which decreases pressure and allows safer separation from the brain, nerves, and blood vessels. The dural attachment is removed or coagulated when safe, and the dura is reconstructed if needed. The bone flap and scalp are then closed.
Can a meningioma be completely removed without neurological damage?
Many meningiomas can be completely removed without neurological damage, especially when they are located in surgically favorable regions such as the convexity and are not densely attached to critical vessels, cranial nerves, venous sinuses, or brainstem structures. However, complete removal is not always the safest goal. In skull base tumors or tumors near the optic nerves, cavernous sinus, major arteries, superior sagittal sinus, or cranial nerves, aggressive removal may increase the risk of permanent neurological injury. Modern neurosurgery uses neuronavigation, microscopy, CUSA, and neurophysiological monitoring to improve safety, but anatomy remains decisive. The best result is not always the most radical resection; it is maximal safe tumor control with preserved neurological function.
What does partial meningioma removal mean and when is it intentionally planned?
Partial meningioma removal means that the surgeon intentionally leaves a small part of the tumor behind instead of removing it completely. This may be planned when the remaining tumor is firmly attached to critical arteries, veins, cranial nerves, the cavernous sinus, brainstem, or other structures where aggressive removal could cause severe neurological damage. In these situations, planned subtotal resection can be safer than radical surgery. The remaining tumor may then be monitored with MRI or treated with stereotactic radiosurgery or fractionated radiotherapy if it grows or if tumor control is needed. This approach is especially relevant for skull base meningiomas, where the balance between tumor control and preservation of neurological function is often more important than complete removal at any cost.
Is Gamma Knife or radiosurgery safer than open meningioma surgery?
Gamma Knife or stereotactic radiosurgery may be safer than open surgery in selected patients, but it is not automatically safer for every meningioma. Radiosurgery is generally most suitable for small tumors, usually below about 2.5–3 cm, especially when they are in surgically difficult areas and are not causing major brain compression. It can provide long-term tumor control in many benign meningiomas. However, radiosurgery may be unsuitable when the tumor is large, causes significant mass effect, requires decompression, or lies too close to structures that tolerate limited radiation, such as the optic nerves, optic chiasm, or brainstem. The choice depends on tumor size, location, symptoms, growth, and risk to nearby structures.
When is radiation therapy preferred over surgery for meningioma?
Radiation therapy may be preferred when surgery carries higher risk, when the tumor is small and located in a surgically difficult area, when residual tumor remains after surgery, or when a recurrent meningioma cannot be safely removed completely. It may also be considered when the patient prefers a non-surgical option after discussion of risks and benefits. Stereotactic radiosurgery is usually used for small tumors, while fractionated radiation is often chosen when the tumor is close to sensitive structures such as the optic nerves, optic chiasm, pituitary stalk, or brainstem. Radiation is not ideal when immediate decompression is needed because of mass effect, edema, hydrocephalus, or significant neurological deterioration.
What is the real risk of meningioma recurrence after surgery or radiation?
The risk of meningioma recurrence depends mainly on tumor grade and completeness of removal. After complete removal of benign meningiomas, recurrence is relatively low, approximately 5–10% over long-term follow-up. After subtotal removal, recurrence may be higher, around 20–40%. Atypical meningiomas recur more frequently, approximately 30–40%, and malignant meningiomas may recur in 50–80% of patients. Simpson grade is also important because removal of the tumor and its dural attachment lowers the chance of recurrence. Radiation therapy can control growth in many patients, especially small benign tumors, but long-term MRI follow-up remains essential because recurrence may occur many years after treatment. Not every small recurrence requires immediate treatment.
Why may different specialists recommend different meningioma treatments?
Different specialists may recommend different treatments because meningioma decisions depend on many interacting factors. One doctor may favor observation when the tumor is small, asymptomatic, and stable. Another may recommend early surgery if the tumor lies near structures where future growth could become dangerous. Surgeons may also differ in how aggressively they would attempt removal, especially near cranial nerves, blood vessels, venous sinuses, or the skull base. Radiation oncologists may favor radiosurgery for small tumors in difficult locations, while neurosurgeons may prefer surgery when decompression or tissue diagnosis is needed. These differences do not always mean that one opinion is wrong. They reflect different interpretations of tumor size, location, growth, symptoms, edema, and treatment risk.
When should patients seek a neurosurgical second opinion for meningioma?
A neurosurgical second opinion is useful when MRI or CT has revealed a meningioma but it is unclear whether observation, surgery, radiosurgery, or radiotherapy is the safest strategy. It is especially important when specialists give different recommendations, when surgery has been proposed but the risks are not clear, when Gamma Knife or radiation is suggested near critical structures, or when symptoms such as seizures, visual disturbance, weakness, balance problems, or progressive headaches may be related to the tumor. A second opinion can clarify tumor size, location, edema, growth rate, relationship to important nerves and vessels, likelihood of recurrence, and realistic treatment goals. It helps the patient understand not only what can be done, but what should be done safely.