Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

MRI Findings, Symptom Correlation, CSF Flow, Syringomyelia, and When Surgery Is Needed
Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Neurosurgeon and Pain Management Specialist
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
May 28, 2026
Who This Page Is For
This page is intended for adults with suspected or confirmed Chiari malformation and for family members
seeking a clear explanation of MRI findings, symptoms, and treatment options.
It is especially relevant when brain or cervical spine MRI shows cerebellar tonsillar descent, impaired cerebrospinal fluid (CSF) flow,
or associated findings such as syringomyelia or ventricular enlargement, but it remains unclear whether these abnormalities
truly explain the patient’s symptoms.
Readers may focus only on sections relevant to their situation.
If symptoms are borderline, MRI findings are ambiguous, or surgery has been proposed without clear expectations,
an experienced
neurosurgical second opinion
can help clarify whether Chiari malformation is the primary cause of symptoms and whether observation or surgical treatment is likely to be beneficial. Patients seek a second opinion both to confirm that surgery is truly indicated and to avoid unnecessary surgery when Chiari malformation is likely incidental or not the primary cause of symptoms.
When patients and families usually seek a second opinion for Chiari malformation
- MRI shows cerebellar tonsillar descent, but it is unclear whether Chiari malformation explains the patient’s symptoms
- Headache, neck pain, dizziness, or balance problems persist despite conservative treatment
- Symptoms overlap with occipital neuralgia, cervical spine disease, or primary headache disorders
- Neurological symptoms are present, but it is uncertain whether they are directly related to Chiari malformation
- Syringomyelia is detected on MRI, but its clinical relevance and activity are unclear
- Hydrocephalus or enlarged ventricles are reported, especially in older patients, raising questions about alternative causes such as NPH or brain atrophy
- Surgery is proposed, but the expected benefit, risks, or extent of the operation remain uncertain
In these situations, an experienced neurosurgical review can help determine whether Chiari malformation is truly responsible for symptoms, clarify the significance of associated findings, and define realistic expectations before any invasive intervention: Request a Second Opinion
Chiari Malformation in Adults — Quick Summary (Read This First)
Most readers benefit from the Quick Summary together with the sections on Pathophysiology, MRI Evaluation and CSF Flow, and Indications for Surgery. Other sections provide additional clinical detail and context.
Contents
- Who this page
- When seek second opinion
- Quick summary
- What is Chiari
- Types and stages
- Why Chiari causes symptoms
- MRI findings
- Symptoms in adults
- Diagnostic evaluation
- Observation and monitoring
- When surgery considered
- Differential diagnosis
- Surgical options overview
- Prognosis
- Chiari with hydrocephalus
- Chiari with syrinx
- Chiari with tethered cord
- Why Specialist Opinions Differ
- Key takeaway
- Request second opinion
- FAQs
- More patient information
What Is Chiari Malformation?
A Chiari malformation occurs when the lower parts (tonsils) of the cerebellum (small brain) descend through the anatomic opening at the base of the skull (foramen magnum) into the spinal canal. This displacement disrupts the flow of cerebrospinal fluid and/or puts pressure on the brainstem and upper spinal cord, as well as the lower cranial and upper spinal nerves. This mechanical compression can lead to progressive neurological symptoms.
In adults, the condition is almost exclusively Chiari malformation type I.
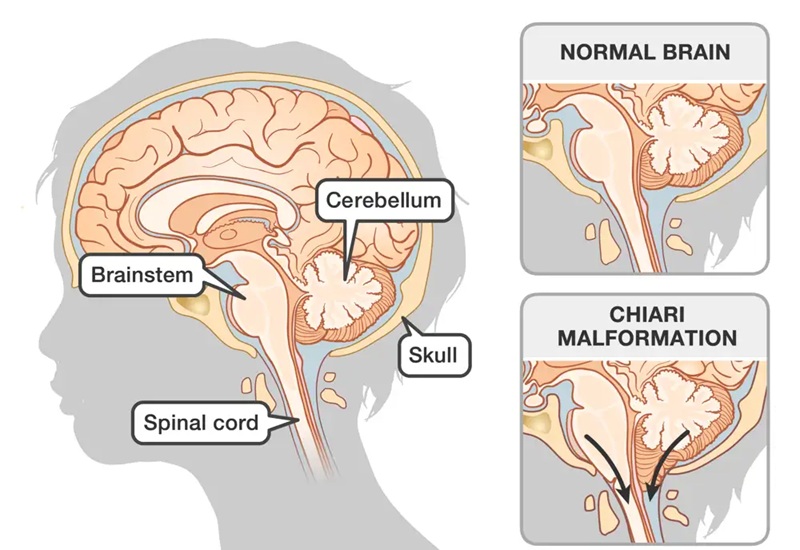
Image: Chiari malformation type 1 occurs when the lower parts (tonsils) of the cerebellum (small brain) descend through the anatomic opening at the base of the skull (foramen magnum) into the spinal canal.
Types and Stages of Chiari Malformation
Chiari 0 (Zero Stage)
- No measurable tonsillar descent
- Symptoms and/or syringomyelia are present
- Pathophysiology: impaired CSF flow at the foramen magnum
➡️ Clinically significant and often underdiagnosed.
Chiari I – The only form typically diagnosed in adults
- Cerebellar tonsillar descent ≥ 5 mm below the foramen magnum
- Usually, only this type is present in adults
- Clinical spectrum:
- Asymptomatic
- Mildly symptomatic
- Severely symptomatic
Prevalence (MRI-based studies):
- 0.5–1% in the general population
- Only a subset become symptomatic
Some specialists use the term Chiari type 1.5 to describe a more extensive form of Chiari malformation, in which the brainstem is also slightly displaced. For patients, this distinction mainly helps guide surgical planning rather than changing the overall diagnosis or treatment goals.
Chiari II, III, IV
- Associated with neural tube defects and severe congenital anomalies
- Not newly diagnosed in adults
- Rarely relevant in adult neurosurgical practice
Pathophysiology – Why Does Chiari Happen and Cause Problems?
1. The Primary Mechanism (The Root Cause)
The main issue is a small posterior fossa—the area at the back of the skull is too small to comfortably hold the cerebellum.
- Crowding: Because space is limited, the brain structures become overcrowded.
- Descent: This pressure forces the lower parts of the cerebellum (tonsils) downward, pushing them out of the skull and into the spinal canal.
2. The Consequences (The Chain Reaction)
Once the cerebellum is pushed into the spinal canal, it triggers three main problems:
- Direct Compression: The displaced brain tissue physically presses against the brainstem, spinal cord, and nerves, impairing their function and causing pain
- Blocked Fluid Flow: Like a cork in a bottle, the cerebellum blocks the normal circulation of cerebrospinal fluid (CSF). This backup of fluid can lead to Hydrocephalus (increased pressure inside the head). Hydrocephalus is present in 7-10% of patients with Chiari malformation.
- Abnormal Pulsations: Because the fluid cannot flow smoothly, it creates abnormal pressure waves. Over time, this fluid can be forced into the spinal cord itself, forming a fluid-filled cyst called a Syrinx (Syringomyelia), which causes progressive nerve damage by compressing the spinal cord from inside. Syringomyelia is present in 30-70% of patients with Chiari malformation.
Putting It All Together
Symptoms of Chiari malformation may result from:
- a single dominant mechanism,
- or a combination of CSF flow disturbance, neural compression, and syrinx-related spinal cord injury.
Understanding which mechanism predominates in a given patient is essential for appropriate treatment planning and realistic expectations. For this reason, the commonly cited 5-mm threshold for tonsillar descent is only a conditional and imperfect guideline. Some patients may require surgical treatment despite less than 5 mm of tonsillar descent if cerebrospinal fluid flow is impaired or if symptoms are clearly attributable to Chiari-related mechanisms. Conversely, tonsillar descent greater than 5 mm may remain clinically insignificant and require only observation when there is no evidence of CSF flow disturbance, neural compression, or syrinx formation.

Image: Due to the descent of the tonsils into the spinal canal, the flow of cerebrospinal fluid is disrupted. As a result, a collection of fluid forms inside the spinal cord (syrinx). As this syrinx grows, it can compress the spinal cord from the inside out.
What the Doctor Sees on Your MRI
An MRI is the gold standard for diagnosing Chiari because it clearly shows the „space issues“ at the back of the head. Here is what those findings actually mean:
Key MRI Features
- Low-Sitting Cerebellum (Tonsillar Descent): The MRI shows the lower tips of the cerebellum (tonsils) dipping below the skull line. In Chiari, these tips often look pointed or „pegged“ instead of their normal rounded shape because they are being squeezed through a tight space.
- Crowded Space (Obliterated Subarachnoid Space): Normally, there is a clear „buffer zone“ of fluid around the brain. On the MRI, this space looks narrowed or completely blocked, meaning the brain tissue is packed too tightly against the bone.
- Fluid Blockage (Disturbed CSF Flow): Using a special type of MRI called a Cine MRI (which works like a movie of your fluid flow), doctors can see that the spinal fluid is „struggling“ to pass. Instead of a smooth, rhythmic flow, it looks turbulent or stops entirely at the base of the brain.
Secondary Findings (Related Conditions)
Sometimes, the MRI shows other issues caused by the Chiari malformation:
- Syringomyelia (Syrinx): A fluid-filled cyst that forms inside the spinal cord. This happens because the blocked fluid at the brain level gets „pushed“ into the cord.
- Hydrocephalus: A buildup of extra fluid inside the deep chambers (ventricles) of the brain because the exit route is blocked.
- Brainstem Distortion: Because of the lack of room, the brainstem may look slightly pushed, tilted, or „kinked“ instead of sitting straight.

Image: Sagittal MRI view showing the cerebellar tonsils (purple) descending through the foramen magnum (blue), compressing the brainstem and the upper spinal cord.
Associated Conditions and Their Frequency
| Associated condition | Approximate frequency |
|---|---|
| Syringomyelia | 30–70% |
| Hydrocephalus | 7-10% |
| Scoliosis | 20–40% |
| Basilar invagination | 5–10% |
| Tethered cord | 5–10% |
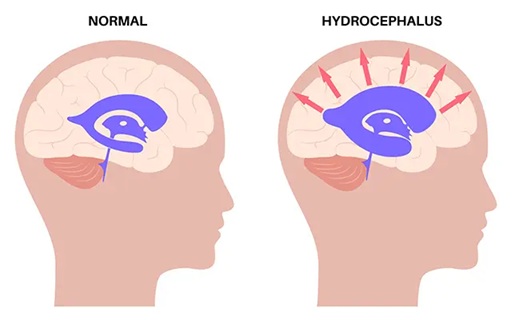
Image: On the left, normal ventricles are shown; on the right, they are enlarged due to an obstruction of cerebrospinal fluid flow, a condition known as hydrocephalus.
Symptoms of Chiari Malformation in Adults
Common Symptoms
- Headache at the back of the head (occipital) that worsens with coughing, sneezing, or physical straining
- Neck pain
- Dizziness or vertigo
- Balance problems and gait instability (unsteadiness, tendency to veer or fall)
- Numbness or weakness of the arms, often related to associated syringomyelia
Brainstem- and Cerebellar-Related Symptoms
- Nystagmus (involuntary rhythmic eye movements), which may cause visual instability
- Double vision
- Swallowing difficulties (dysphagia)
- Hoarseness or voice changes
- Syncope or near-syncope, particularly with straining or neck movement
Symptoms Related to Syringomyelia (Syrinx)
- Dissociated Sensory Loss (The „Burn Without Pain“ Sign): A person can feel touch or pressure, but loses the ability to feel pain and temperature. In Chiari malformation with associated syringomyelia or hydromyelia, this sensory loss most often follows a cape-like distribution, affecting the neck, shoulders, upper back, and upper arms, reflecting the frequent involvement of the cervical spinal cord. Because of this dissociation, a patient may unknowingly burn or injure these areas — for example, by touching a hot stove or cup — and only notice the injury visually.
- Progressive Upper Limb Weakness: A gradual loss of strength in the arms and hands. Patients often notice this as clumsiness, such as having difficulty opening jars, buttoning a shirt, or dropping objects unexpectedly.
- Muscle Atrophy: The visible wasting away or thinning of muscles, most commonly noticed in the small muscles of the hands (between the thumb and index finger). This happens because the syrinx damages the nerves that keep these muscles healthy and active.
Diagnostic Evaluation
Primary Diagnostic Tool
- MRI of the brain and the entire spine is essential to evaluate cerebrospinal fluid dynamics, define the full extent of the syrinx, and identify associated abnormalities anywhere along the spinal axis.
How Many Millimeters of Tonsillar Descent Actually Matter?
- ≥ 5 mm: diagnostic for Chiari I
- 3–5 mm: borderline (clinical correlation required)
- < 3 mm: consider Chiari 0 if syringomyelia present
Important:
The degree of tonsillar descent alone does not determine disease severity. Clinical symptoms, cerebrospinal fluid flow disturbance, and associated conditions — such as syringomyelia, hydrocephalus, or tethered cord — are equally important. Importantly, significant CSF flow impairment may occur even with minimal tonsillar descent or, in some cases, in the absence of obvious descent on standard MRI. In such patients, abnormal CSF dynamics at the craniocervical junction can still lead to symptoms or syrinx formation, a phenomenon best demonstrated by cine (phase-contrast) MRI studies.
Additional Diagnostic Studies (When Indicated)
In selected cases, additional imaging and neurophysiological studies may be required to clarify the underlying mechanism of symptoms or guide treatment planning.
Dynamic imaging studies
Dynamic flexion–extension imaging of the cervical spine may be used to assess craniocervical or cervical instability, which can contribute to symptoms even in the absence of marked tonsillar descent. Instability may involve the occipito-atlantal or atlanto-axial junction, as well as lower cervical segments.
Cine (phase-contrast) MRI
Cine MRI evaluates cerebrospinal fluid flow dynamics at the craniocervical junction and along the spinal canal. It is particularly useful when standard MRI does not show a clear Chiari malformation but symptoms or syringomyelia suggest functional CSF flow obstruction.
Additional neurophysiological tests (as needed)
Depending on the clinical presentation, further studies may include:
- EMG/NCS to assess peripheral nerve or motor neuron involvement,
- Somatosensory evoked potentials (SSEP) to evaluate conduction pathways within the spinal cord,
- other targeted tests based on individual symptoms.
Observation and Monitoring
Approximately 60–70% of adults with Chiari I are managed conservatively.
Indications for Observation
- No symptoms even if tonsillar descent >5 mm
- Stable, mild symptoms
- No syringomyelia
- No radiological progression
Follow-up Strategy
- Periodic neurological examination
- MRI every 12–24 months
- Patient education regarding symptom progression
In adults with cerebellar tonsillar descent greater than 5 mm (Chiari malformation type I), the presence of hydrocephalus alone does not automatically indicate the need for Chiari decompression. If hydrocephalus is the only clinically relevant finding and there are no Chiari-specific symptoms, no syringomyelia, and no significant cerebrospinal fluid flow obstruction at the foramen magnum, treatment should be directed at hydrocephalus itself, most commonly with ventriculoperitoneal (VP) shunt placement, while Chiari malformation is managed conservatively with clinical and radiological follow-up.
Indications for Surgery
Before surgery, the average period of follow-up is around 3-7 years.
Surgical treatment is considered when one or more of the following are present:
- Progressive neurological deficits
- Syringomyelia
- Documented CSF flow obstruction
- Obstructive hydrocephalus related to impaired CSF circulation at the craniovertebral junction, with other symptoms of Chiari
- Severe, disabling headaches refractory to conservative therapy
The Importance of Clinical Experience and Differential Diagnosis
In both borderline and clearly expressed forms of Chiari malformation, significant clinical experience is required to determine whether a patient’s symptoms are truly caused by Chiari malformation or by other, more common conditions.
Headache, in particular, may result from occipital neuralgia, cervicogenic headache, primary headache disorders, or other pain generators, rather than from Chiari-related CSF flow disturbance. When diagnostic certainty is lacking, it is essential to first identify and treat potential alternative sources of pain, using an appropriate combination of pharmacological therapy and, when indicated, targeted local interventions such as nerve blocks or regional injections.
Similarly, the presence of neurological symptoms must be carefully evaluated to determine whether they are directly attributable to Chiari malformation or whether they arise from unrelated neurological or musculoskeletal conditions.
The same level of caution applies to associated findings:
- Syringomyelia must be assessed not only for its presence, but for its clinical relevance and symptomatic activity.
- Hydrocephalus, particularly in older patients, may have alternative etiologies, such as communicating hydrocephalus, normal pressure hydrocephalus (NPH), or ventricular enlargement secondary to cerebral atrophy, rather than being a direct consequence of Chiari malformation.
In many patients, multiple potential contributors to symptoms may coexist, and careful analysis may reveal that none of them are primarily driven by Chiari malformation. In such cases, surgical treatment of Chiari is unlikely to provide meaningful benefit and may therefore be unnecessary. When standard imaging does not provide a clear explanation, additional studies may be indicated, but their value depends on expert interpretation in the context of the patient’s clinical presentation and other imaging findings. Complementary investigations may include cine (phase-contrast) MRI to assess cerebrospinal fluid dynamics, dynamic imaging to evaluate craniocervical or cervical instability, and other targeted tests as clinically appropriate.
Because of this complexity, neurosurgeons may reasonably differ in their opinions regarding whether surgery is appropriate and which surgical strategy, if any, should be pursued. This underscores the importance of individualized evaluation, cautious surgical decision-making, and, in selected cases, obtaining a second expert opinion.
When Tonsillar Descent Is Not Chiari Malformation
Cerebellar tonsillar descent on MRI does not always represent primary Chiari malformation. Several conditions can displace the tonsils downward and mimic Chiari I on standard imaging. Recognizing these secondary causes is essential, because treatment must be directed at the underlying condition — not at the tonsils.
- Intracranial hypotension (CSF leak) — loss of CSF due to a spinal dural tear, a CSF-venous fistula, or a post-procedural leak reduces intracranial pressure and causes the brain to shift downward. MRI may show tonsillar descent indistinguishable from primary Chiari I, often accompanied by dural enhancement, subdural collections, or pituitary enlargement. A positional headache — worse when upright, better when lying down — is a key clinical clue.
- Hydrocephalus — sustained elevation of intracranial pressure can push the tonsils downward through the foramen magnum.
- Posterior fossa mass — a tumor or other space-occupying lesion increasing pressure within the posterior fossa can mechanically displace the tonsils.
- Post-traumatic or post-surgical changes — altered CSF dynamics following spine or skull base surgery may result in acquired tonsillar descent.
An important principle: treating the primary cause may resolve tonsillar descent.
When the underlying condition is successfully treated — the CSF leak is sealed, hydrocephalus is shunted, or the mass is removed — intracranial pressure and CSF dynamics normalize. In many patients, tonsillar descent partially or fully resolves as a result, and syringomyelia, if present, may regresses without any additional intervention at the foramen magnum.
For this reason, posterior fossa decompression is not automatically indicated in patients with secondary tonsillar descent. Decompression should be considered only if, after successful treatment of the primary cause, tonsillar descent persists, syringomyelia does not regress or continues to progress, or neurological symptoms attributable to craniocervical CSF flow obstruction remain.
Surgical decompression for Chiari malformation performed before or instead of treating the true underlying cause is ineffective and potentially harmful.
Surgical Treatment – Why Are There So Many Variations?
Chiari malformation is not a single uniform disease, but a spectrum of anatomical and physiological abnormalities. Therefore, surgery must be individualized. These surgical methods are listed below according to their extensiveness. It is important to note that each subsequent, more invasive method typically implies that all the preceding steps have already been performed as part of the procedure.
Surgical Spectrum: How Is Space Created?
The goal of surgery is to relieve pressure and restore normal cerebrospinal fluid (CSF) flow at the back of the brain. This is not a single fixed operation, but a graded and individualized approach. Surgeons begin with the least extensive option and proceed further only if necessary. Most patients do not require all of the steps described below.
Suboccipital bone decompression involves removing a small portion of bone from the back of the skull to create additional space for the brain. In some patients, this step alone is sufficient to restore CSF circulation and relieve symptoms.
C1 laminectomy is performed by removing the upper part of the first cervical vertebra, further widening the passage between the brain and the spinal canal and reducing crowding at the craniovertebral junction.
Release of restrictive dural and ligamentous bands
In some patients, thickened or tight fibrous and ligamentous structures at the craniocervical junction — such as the atlanto-occipital membrane or dural bands — may contribute to cerebrospinal fluid flow restriction. Carefully releasing these structures can improve CSF dynamics without opening the dura and may be sufficient in selected cases.
Duraplasty (dural patch) involves opening the tough outer membrane covering the brain (the dura) and expanding it with a patch. This significantly improves CSF flow and is commonly combined with bone decompression when imaging shows restricted fluid circulation.
Lysis of adhesions is performed when scar tissue is present, releasing the cerebellar tonsils and surrounding neural structures so that normal movement and CSF pulsation can occur.
Restoration of the fourth ventricle outlet is performed in selected cases when the normal CSF exit pathway is obstructed. This does not involve entering brain tissue, but rather re-establishing physiological CSF flow.
Tonsillar coagulation (reduction) may be used to gently reduce the size of the cerebellar tonsils when crowding persists despite adequate decompression.
Partial or complete tonsillectomy is reserved for advanced or refractory cases. This step is not routine, but in carefully selected patients and in experienced hands it can be safe and effective. Current evidence indicates that bilateral tonsil removal does not result in permanent neurological deficits when properly indicated.
Throughout all stages, the extent of surgery is tailored to the individual patient, based on anatomy, symptoms, CSF dynamics, and associated conditions such as syringomyelia or hydrocephalus.
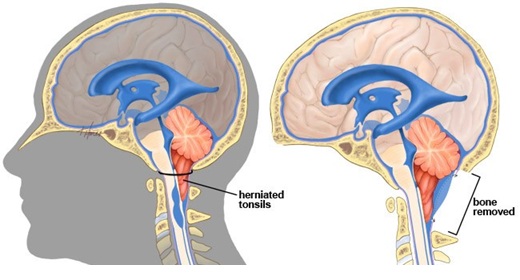
Image: On the left, the descended tonsils are visible as part of a Chiari malformation. On the right, the removal of a portion of the bone is shown, creating space for the tonsils to relieve pressure on the spinal cord. If this is not sufficient, depending on the surgeon’s assessment and preference, the procedure can be expanded to include opening and enlarging the brain’s lining (dura) with a patch, releasing the tonsils from adhesions, reducing the tonsils through coagulation (shrinking), or even removing the tonsils entirely.
Minimally Invasive Endoscopic Techniques
- Skin incision ~3 cm
- Endoscopic assistance
- Bilateral cerebellar tonsil removal
What Does “Minimally Invasive” Mean?
- Smaller skin incision?
- Or less neural tissue compromise?
Current evidence suggests:
- Removal of both cerebellar tonsils does not result in permanent neurological deficits?
- Cerebellar function is preserved
- Proper patient selection is critical
Surgical Complications
Potential complications include:
- CSF leakage
- Infection
- Bleeding
- Pseudomeningocele
- Incomplete symptom relief
Severe complications:
< 5% in experienced neurosurgical centers
Prognosis
- Symptomatic improvement: 70–85%
- Syringomyelia:
- Often regresses or resolves after adequate decompression
- Headache frequently improves first
Special Clinical Situations
Chiari Malformation with Hydrocephalus
- Chiari malformation and hydrocephalus are closely related and may influence each other. Downward displacement of the cerebellar tonsils can obstruct cerebrospinal fluid flow at the craniocervical junction and lead to secondary hydrocephalus.
- Conversely, chronic hydrocephalus with elevated intracranial pressure may result in acquired tonsillar descent, mimicking Chiari malformation. For this reason, hydrocephalus is often treated first, as correction of CSF pressure and flow may reduce tonsillar descent and improve symptoms.
- Normal pressure hydrocephalus (NPH), however, does not typically cause tonsillar descent, as intracranial pressure is not persistently elevated.
- Chiari decompression may be considered subsequently or in combination when symptoms persist or when there is clear evidence of craniocervical CSF flow obstruction despite adequate treatment of hydrocephalus.
Chiari Malformation with Syringomyelia
- Syrinx is not directly drained
- Treating the underlying CSF obstruction is the primary goal
Chiari Malformation and Tethered Cord
In some patients, Chiari malformation coexists with tethered cord syndrome. Although tethered cord typically causes symptoms predominantly in the lower extremities, its presence may contribute to abnormal tension along the spinal axis.
In carefully selected cases, surgical release of a tethered cord may be considered first, particularly when lower limb symptoms predominate and there is no clear evidence of significant cerebrospinal fluid flow obstruction at the craniocervical junction.
In a subset of patients, detethering may lead to partial improvement of Chiari-related findings, including reduction of tonsillar descent or improvement in cerebrospinal fluid dynamics. However, this effect is variable and cannot be reliably predicted, and many patients with symptomatic Chiari still require direct posterior fossa decompression.
Why Expert Opinions Differ in Chiari Malformation — Key Decision Points
In Chiari malformation, differences in expert opinion are common, not because the condition is poorly understood, but because symptoms, imaging findings, and their clinical relevance do not always align clearly. The following are the key areas where interpretations and treatment recommendations may differ.
Is Chiari really the cause of symptoms?
Although MRI may show tonsillar descent, this does not necessarily mean that Chiari malformation is responsible for the patient’s symptoms. Headache, dizziness, imbalance, or visual disturbances may originate from other conditions such as occipital neuralgia, cervical spine disorders, or vestibular dysfunction. Distinguishing the true source of symptoms is often the most important and most challenging step.
When is surgery actually necessary?
Some specialists recommend surgical decompression based primarily on MRI findings and symptom presence, while others consider this insufficient and advise observation unless symptoms clearly correlate with cerebrospinal fluid (CSF) obstruction. Because of this, patients with similar MRI findings may receive completely different recommendations regarding surgery.
How important is the degree of tonsillar descent?
The commonly used threshold (e.g., 5 mm) is not a reliable indicator of symptom severity or the need for surgery. Some patients with minimal descent have significant symptoms, while others with more pronounced descent remain asymptomatic. This leads to different interpretations of the same MRI finding.
What is the role of CSF flow studies?
Cine MRI can provide additional information about CSF dynamics, but its interpretation varies. Some clinicians consider impaired CSF flow a key factor in decision-making, while others place greater emphasis on symptoms and their progression over time.
How should associated findings be interpreted?
Findings such as syringomyelia or hydrocephalus may influence treatment decisions, but they do not always indicate that Chiari malformation is the primary cause of symptoms. In some cases, these findings require separate evaluation, and the order of treatment priorities may differ.
Because of these factors, patients may receive different recommendations regarding diagnosis, monitoring, or surgery. A structured evaluation that correlates symptoms, imaging, and functional findings is essential before making any irreversible treatment decision.
Key Takeaway
Chiari malformation in adults requires:
- Careful imaging interpretation
- Clinical correlation
- Individualized surgical decision-making
Neurosurgeon must treat the patient — not the MRI image.
Request a Neurosurgical Second Opinion — Chiari Malformation in Adults.
24-Hour Review or Priority Option (Usually Within 3 Hours)
Patients with Chiari malformation are often told that their MRI shows cerebellar tonsillar descent,
syringomyelia, or impaired cerebrospinal fluid (CSF) flow — yet it may remain unclear
whether these findings truly explain their symptoms or whether surgery is likely to help.
Headache, dizziness, neck pain, balance problems, or sensory symptoms may arise from Chiari malformation,
but they may also result from occipital neuralgia, cervical spine disorders, primary headache syndromes,
or unrelated neurological conditions.
An independent neurosurgical second opinion can help determine whether Chiari malformation is the primary cause,
whether observation is appropriate, or whether surgical treatment is reasonable — or unlikely to provide benefit.
- ✔ Send a brief message describing your main symptoms (headache pattern, balance issues, sensory changes) and what your MRI report states
- ✔ You’ll receive a reply within 24 hours explaining whether and how a neurosurgical second opinion could help in your specific Chiari case
- ✔ Time-sensitive cases: if neurological symptoms are progressing, syringomyelia is present, or surgery has been proposed with uncertainty — write PRIORITY in your first message
- ✔ Brain and cervical spine MRI (DICOM images) and available medical documentation can be reviewed once initial contact is established
- ✔ During the consultation, we discuss whether symptoms are truly Chiari-related, the significance of CSF flow obstruction or syringomyelia, and realistic expectations regarding observation versus surgery — with up to 10 days of follow-up for brief clarification questions
Consultation fees typically range from $180–250, depending on case complexity.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth second opinions in neurosurgery.
Frequently Asked Questions About Chiari Malformation in Adults
What is Chiari malformation type 1 in adults?
Chiari malformation type 1 in adults means that the cerebellar tonsils sit lower than expected at the opening between the skull and the upper spine, called the foramen magnum. It is the form of Chiari malformation most often diagnosed in adults. The MRI finding alone does not prove that symptoms are caused by Chiari. It becomes clinically important when the lowered tonsils crowd the foramen magnum, obstruct cerebrospinal fluid flow, compress neural structures, cause syringomyelia, or match a typical pattern of symptoms. Many adults with Chiari type 1 are monitored rather than operated on, especially when symptoms are mild, stable, or better explained by another condition.
What are the symptoms of Chiari malformation in adults?
Symptoms of Chiari malformation in adults may include headache at the back of the head or upper neck, especially when worsened by coughing, sneezing, straining, bending, or physical effort. Other possible symptoms include neck pain, dizziness, vertigo, balance problems, numbness or weakness in the arms, swallowing difficulty, hoarseness, double vision, nystagmus, or symptoms caused by syringomyelia. Syringomyelia may cause cape-like loss of pain and temperature sensation, hand weakness, clumsiness, or muscle wasting. However, headache, dizziness, neck pain, and sensory symptoms are common and may also come from migraine, occipital neuralgia, cervical spine disease, vestibular disorders, or other causes. Symptoms must be correlated with MRI and neurological findings.
What treatment is available for Chiari malformation in adults?
Treatment for Chiari malformation in adults depends on whether the MRI finding is actually causing symptoms. Observation with periodic neurological examination and MRI follow-up is often appropriate when symptoms are mild, stable, or not clearly Chiari-related. Conservative treatment may focus on alternative causes of headache, neck pain, dizziness, or neuralgia. Surgery is considered when Chiari malformation causes progressive neurological deficits, syringomyelia, clear cerebrospinal fluid flow obstruction, disabling Chiari-type cough or strain headache, or obstructive hydrocephalus related to craniocervical CSF blockage. The usual operation is posterior fossa decompression, but the exact technique depends on anatomy, CSF flow, syrinx status, and surgical judgment.
When is monitoring appropriate for Chiari malformation in adults?
Monitoring is appropriate for many adults with Chiari malformation when symptoms are absent, mild, stable, or not clearly caused by Chiari-related compression or CSF flow obstruction. Follow-up usually focuses on neurological examination, symptom progression, and MRI changes over time. Doctors monitor for new or worsening Chiari-type cough headache, balance problems, swallowing difficulty, arm weakness or numbness, syringomyelia, hydrocephalus, or progression of crowding at the foramen magnum. Monitoring does not mean ignoring the condition. It means avoiding unnecessary decompression surgery while watching for objective signs that Chiari malformation is becoming clinically active or that surgery may become more appropriate.
Can Chiari malformation on MRI be incidental in adults?
Yes. In adults, cerebellar tonsillar descent on MRI can be an incidental finding and may not explain the patient’s symptoms. Tonsillar descent means that the lower part of the cerebellum sits lower than usual near the opening at the base of the skull. Some adults have this MRI appearance but no neurological deficits, no syringomyelia, no hydrocephalus, and no clear obstruction of cerebrospinal fluid (CSF), the fluid surrounding the brain and spinal cord. In such cases, headache, dizziness, neck pain, or fatigue may come from more common conditions such as migraine, occipital neuralgia, cervical spine disease, vestibular disorders, or primary headache syndromes. The key question is whether symptoms, examination, MRI findings, CSF flow, and clinical course all point to Chiari as the dominant mechanism.
Does a 5 mm Chiari finding on MRI always explain symptoms?
No. The commonly cited 5 mm threshold is only a practical imaging guideline, not a reliable measure of disease severity. Some patients with more than 5 mm of cerebellar tonsillar descent have no symptoms and require only observation. Others with 3–5 mm of descent, or even Chiari 0, may have clinically important obstruction of cerebrospinal fluid flow or syringomyelia, meaning a fluid-filled cavity inside the spinal cord. The number of millimeters does not tell the whole story. Doctors must also evaluate the shape of the tonsils, crowding at the foramen magnum, whether normal CSF spaces are blocked, cine MRI flow pattern, presence of syrinx, neurological signs, and whether symptoms are typical for Chiari. Surgery should not be decided from millimeters alone.
Can a borderline Chiari or mild tonsillar ectopia cause symptoms?
Borderline Chiari or mild cerebellar tonsillar ectopia can sometimes be clinically relevant, but only in the right context. Tonsillar ectopia means that the cerebellar tonsils sit slightly lower than usual. Mild descent of 3–5 mm may be incidental, especially if the patient has no syrinx, no neurological deficit, and no clear CSF blockage. However, if the posterior fossa is crowded, CSF flow is impaired at the craniocervical junction, symptoms are typical, or a syrinx is present, borderline descent may be part of a true Chiari-related mechanism. The opposite is also true: visible descent may not matter if CSF spaces remain open, examination is normal, and symptoms fit migraine, neck pain, vestibular disease, or occipital neuralgia better. Borderline findings require correlation, not automatic reassurance and not automatic surgery.
What headache pattern is more typical for Chiari malformation?
A more typical Chiari headache is usually located at the back of the head or upper neck and is triggered or worsened by coughing, sneezing, straining, laughing, bending, or physical effort. This pattern suggests transient pressure changes at the craniocervical junction, where the skull meets the upper spine, and possible obstruction of cerebrospinal fluid flow. However, many adults with Chiari-like MRI findings have headaches that are actually migraine, tension-type headache, cervicogenic headache, or occipital neuralgia. These headaches may be frequent, severe, or disabling, but not necessarily caused by Chiari. This distinction matters because posterior fossa decompression, meaning surgery to create more space at the back of the skull, is less likely to help if the dominant pain generator is not Chiari-related CSF obstruction or neural compression.
When is cine MRI useful in suspected Chiari malformation?
Cine MRI, also called phase-contrast MRI, is a special MRI sequence that shows cerebrospinal fluid movement like a short flow movie. It can be useful when standard MRI does not fully explain whether Chiari malformation is clinically important. Cine MRI evaluates CSF flow at the foramen magnum and craniocervical junction, where the brain, skull base, and upper spine meet. This is especially helpful in borderline tonsillar descent, Chiari 0, suspected CSF flow obstruction, unclear symptoms, or when surgery is being considered but the decision is uncertain. Abnormal flow can support the idea that the tonsils are functionally obstructing CSF movement. However, cine MRI is not a stand-alone decision tool. Its value depends on expert interpretation together with symptoms, neurological examination, syringomyelia, hydrocephalus, and the rest of the MRI anatomy.
Can Chiari malformation be missed or underestimated on standard MRI?
Chiari malformation or Chiari-related CSF obstruction can sometimes be underestimated on standard MRI, especially when tonsillar descent is borderline, when symptoms suggest Chiari 0, or when the main problem is functional CSF flow obstruction rather than dramatic descent. A routine MRI report may focus on millimeters and miss important details such as crowding, peg-like tonsils, blocked CSF spaces, syringomyelia, or craniocervical junction anatomy. Syringomyelia means a fluid-filled cavity inside the spinal cord and can be a key sign that CSF flow is disturbed. Sometimes brain MRI alone is not enough; cervical and full-spine MRI may be needed to look for syrinx or associated abnormalities. Cine MRI can add information about CSF dynamics. A second review of the actual MRI images, not only the report, is often useful in unclear cases.
When does syringomyelia make Chiari surgery more likely?
Syringomyelia makes Chiari surgery more likely when the syrinx is clearly related to CSF flow obstruction at the craniocervical junction, especially if it is enlarging or causing neurological symptoms. Syringomyelia means a fluid-filled cavity inside the spinal cord. Symptoms may include cape-like loss of pain and temperature sensation over the neck, shoulders, upper back, and arms, hand weakness, clumsiness, muscle wasting, scoliosis, or progressive spinal cord signs. In Chiari-related syringomyelia, the primary goal is usually to restore CSF flow at the foramen magnum, not to drain the syrinx directly. If decompression successfully restores CSF circulation, the syrinx often regresses over time. However, a small stable syrinx must still be interpreted with symptoms, neurological examination, spinal MRI, and disease progression.
Can hydrocephalus or enlarged ventricles in adults be unrelated to Chiari malformation?
Yes. In adults with Chiari malformation, enlarged ventricles or hydrocephalus are not always caused by Chiari. Hydrocephalus means excessive cerebrospinal fluid within the brain’s ventricles. It may be obstructive and related to impaired CSF flow at the craniocervical junction, but it may also reflect communicating hydrocephalus, normal pressure hydrocephalus, or ventricular enlargement due to brain atrophy. This distinction is critical because treatment priorities may differ. If hydrocephalus is the main clinically active problem and there are no Chiari-specific symptoms, no syringomyelia, and no major foramen magnum CSF obstruction, treating hydrocephalus itself may be more appropriate than Chiari decompression. The decision requires careful review of symptoms, MRI pattern, CSF dynamics, and age-related brain changes.
Can a CSF leak or brain sagging mimic Chiari malformation?
Yes. Intracranial hypotension from a spinal CSF leak, CSF-venous fistula, or post-procedural leak can cause downward brain displacement and tonsillar descent that may look like Chiari I on MRI. This is acquired tonsillar descent, not primary Chiari malformation. A key clinical clue is positional headache that is worse when upright and improves when lying down, although not every case is classic. MRI may show diffuse dural enhancement, subdural collections, pituitary enlargement, venous engorgement, or other signs of brain sagging. Treating the leak can allow tonsillar descent and sometimes syringomyelia to improve. Performing Chiari decompression before identifying the true cause may be ineffective or harmful.
When is observation safer than Chiari decompression surgery?
Observation is often safer than Chiari decompression when symptoms are mild, stable, or not clearly attributable to Chiari-related CSF obstruction. Chiari decompression means surgery to create more space at the back of the skull and upper cervical canal so cerebrospinal fluid can move more freely. Observation is also appropriate when there is no syringomyelia, no progressive neurological deficit, no radiological progression, and no convincing flow obstruction at the foramen magnum. Many adults with Chiari I are managed conservatively with periodic neurological examination and MRI follow-up. Observation does not mean ignoring the condition. It means tracking symptoms, neurological function, syrinx status, hydrocephalus, and MRI changes over time. Surgery is more justified when there is progression, disabling Chiari-type headache, syringomyelia, brainstem or spinal cord signs, or clear evidence that Chiari is the dominant cause.
My surgeon recommended Chiari decompression, but I am not sure — what should I consider?
Before accepting Chiari decompression, the key question is whether the symptoms are truly Chiari-related and whether surgery has a realistic chance of helping. Important factors include typical cough or strain occipital headache, progressive neurological deficits, syringomyelia, impaired CSF flow on cine MRI, hydrocephalus clearly related to craniocervical obstruction, and MRI evidence of crowding at the foramen magnum. It is also important to ask what type of decompression is planned: bone-only decompression, C1 laminectomy, duraplasty, adhesion release, tonsillar reduction, or a more extensive operation. C1 laminectomy means removing the upper arch of the first cervical vertebra to widen the canal. Duraplasty means opening and widening the dura, the tough covering of the brain, with a patch. If symptoms are mainly migraine, occipital neuralgia, cervical spine pain, vestibular disease, or unrelated neuropathy, decompression may not provide meaningful benefit.
Why are there different types of Chiari decompression surgery?
Chiari decompression is not one fixed operation because patients differ in anatomy, CSF flow obstruction, tonsillar position, adhesions, syringomyelia, and craniocervical junction crowding. Some patients may need only suboccipital bone decompression, meaning removal of a small part of bone at the back of the skull. Others also need C1 laminectomy, which removes the upper arch of the first cervical vertebra. Some require duraplasty, meaning the dura is opened and widened with a patch to improve CSF flow. In selected cases, restrictive bands or adhesions are released, the fourth ventricle outlet is restored, or tonsillar reduction is performed when crowding persists. More extensive surgery may carry higher risk but may be necessary in complex cases. The correct operation depends on the mechanism causing symptoms, not on a standard template.
Why do some patients not improve after Chiari decompression?
Some patients do not improve after Chiari decompression because Chiari was not the main cause of their symptoms, because symptoms were caused by another condition, or because neurological injury was already advanced. Headache may persist if the true source is migraine, occipital neuralgia, cervical spine disease, or central sensitization rather than CSF obstruction. Symptoms may also persist if decompression did not adequately restore CSF flow, if adhesions remain, if a syrinx does not regress, or if hydrocephalus, tethered cord, craniocervical instability, or CSF leak was not recognized. Tethered cord means abnormal fixation of the spinal cord that may create tension along the spinal axis. Improvement is most likely when the preoperative diagnosis was accurate and symptoms were directly related to Chiari mechanisms.
When is revision surgery considered after Chiari decompression?
Revision surgery after Chiari decompression is considered only when there is a clear structural or CSF-flow reason for persistent or recurrent symptoms. Possible reasons include inadequate decompression, persistent foramen magnum crowding, scarring or adhesions, blocked CSF pathways, progressive syringomyelia, or unrecognized associated conditions. A pseudomeningocele, meaning a CSF-filled pocket under the wound caused by leakage through the dura, can also be relevant in selected cases. Revision is not usually appropriate just because headache continues if the headache pattern suggests migraine, occipital neuralgia, cervical pain, or another non-Chiari cause. Before revision, MRI of the brain and spine, cine MRI, review of operative details, neurological examination, and evaluation for hydrocephalus, CSF leak, tethered cord, or craniocervical instability may be needed. The expected benefit must be realistic before another operation.
Why do neurosurgeons sometimes disagree about Chiari surgery?
Neurosurgeons may disagree about Chiari surgery because MRI findings and symptoms do not always align clearly. One surgeon may focus on tonsillar descent, crowding, headaches, or patient suffering and recommend decompression. Another may emphasize alternative causes of symptoms, absence of syringomyelia, preserved CSF flow, stable findings, or a non-Chiari headache pattern and recommend observation. There may also be different opinions about the extent of surgery: bone-only decompression, C1 laminectomy, duraplasty, adhesion release, or tonsillar reduction. These differences often reflect uncertainty in determining whether Chiari is truly the dominant mechanism. A structured second opinion helps correlate symptoms, MRI, cine MRI, syrinx status, neurological findings, and surgical risk before irreversible treatment.
When is a neurosurgical second opinion useful for Chiari malformation in adults?
A neurosurgical second opinion is useful when MRI shows Chiari malformation or tonsillar ectopia but it is unclear whether symptoms truly come from Chiari. It is especially helpful when surgery has been proposed, when headaches or dizziness may have alternative causes, when cine MRI or syringomyelia findings are difficult to interpret, when hydrocephalus or brain sagging may be involved, or when previous decompression did not help. A second opinion can review the actual MRI images, not only the report, and place symptoms, neurological signs, CSF flow, syrinx activity, and surgical options into one decision framework. The goal is to clarify whether observation, further testing, treatment of another cause, or decompression is most reasonable.
Additional Information for Patients
For those who wish to explore Chiari malformation further, we have selected four highly reliable, patient-oriented resources from leading neurosurgical and research institutions. These provide in-depth guides, support networks, and the latest research updates.
-
1. National Institute of Neurological Disorders and Stroke (NINDS)
A comprehensive fact sheet covering symptoms, causes, and ongoing NIH research.
Visit NINDS Chiari Guide -
2. Mayo Clinic – Patient Information
A clear overview of diagnosis and treatment options from one of the world’s leading medical centers.
View Mayo Clinic Overview -
3. Bobby Jones Chiari & Syringomyelia Foundation (CSF)
An organization specifically dedicated to Chiari and Syringomyelia, offering educational videos and webinars by world-renowned experts.
Explore Bobby Jones CSF Resources -
4. American Association of Neurological Surgeons (AANS)
Detailed clinical descriptions and surgical explanations provided by the leading professional organization of neurosurgeons.
Access AANS Patient Guide