Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist.
Specialized Experience: 30 years of clinical expertise in neurotrauma and neurocritical care.
Last medically reviewed: June 10, 2026
Who This TBI Page Is For
This comprehensive resource is built for two groups: patients dealing with lingering symptoms after traumatic brain injury, and family members seeking critical clarity on a loved one’s severe TBI diagnosis, complex ICU treatment, and uncertain recovery path. We explain the different types of lesions, the significance of the first 72 hours, and all available treatment options.
If you find the information overwhelming, or if you have doubts about the current treatment strategy, you can contact us to see how we provide an individualized
neurosurgery second opinion
for your specific case.
It is a truth acknowledged in every TBI guideline: Standard protocols and algorithms can never replace the experienced neurosurgeon’s individualized assessment.
When families usually seek a neurosurgical second opinion
• The patient is not waking as expected
• Explanations from doctors feel unclear or inconsistent
• Families must decide about surgery or ICU treatment
• There are many important questions that remain unanswered
In complex brain injuries, this is a normal and responsible step.
If this reflects your situation, you can request an individualized neurosurgical review here:
Request Second Opinion
Traumatic Brain Injuries (TBI) — Quick Summary (Read This First)
- A traumatic brain injury (TBI) occurs when an external force (traffic accidents, assaults) disrupts the brain — from mild concussion to life-threatening bleeding, swelling, and deep brain tissue injury. The most important point is that severe TBI is rarely “one problem.”
- The core concept is “combined injury + ongoing change.” The first CT often shows a combination (for example hematoma + contusions + swelling + fracture), and even if it looks “stable,” contusions and swelling can worsen over the next 48–72 hours. This is why the early ICU period is constant monitoring, not a final state.
- Severe TBI usually includes one or more specific traumatic brain lesions. These may include epidural hematoma (EDH), acute or chronic subdural hematoma (SDH), brain contusions, diffuse axonal injury (DAI), traumatic subarachnoid hemorrhage (tSAH), intracerebral hemorrhage (ICH), bleeding into the ventricles (intraventricular hemorrhage), skull fractures (linear, depressed, or skull-base), and penetrating or firearm injuries. Each lesion carries different risks, treatment priorities, and prognostic implications, which are explained in detail in the sections below and on the linked pages.
- Brain pressure and blood flow are the real targets of treatment. Rising ICP (pressure inside skull) can compress brain tissue and reduce vital blood flow, causing secondary stroke-like injury. Causes include brain swelling (edema), acute hydrocephalus (sudden buildup of cerebrospinal fluid that increases brain pressure), and hemorrhages with mass effect (brain tissue being pushed out of place).
- Surgery is about “making room,” not “fixing” the brain. Urgent neurosurgery is needed when bleeding or swelling becomes compressive (or is likely to become so). Procedures may include craniotomy (evacuating a clot) or decompression. A classic example of an urgent surgical hematoma is epidural hematoma (EDH).
- Sudden deterioration is often driven by high ICP, swelling, or hydrocephalus — and these are often treatable. Hydrocephalus may require an EVD to drain CSF and help control ICP.
- “Not waking up” in the first 72 hours is often not a final verdict. Deep sedation, evolving swelling/ICP dynamics, hydrocephalus/EVD management, seizures, and metabolic factors can delay responsiveness and cause day-to-day fluctuations. (Seizures after brain injury)
- Diffuse Axonal Injury (DAI) explains prolonged coma even when CT looks mild. It is a deep “wiring injury” from rotational forces and is best detected on MRI. Brainstem involvement is a key prognostic factor. (DAI explained)
- Severity and prognosis depend on “clinical state + imaging + evolution over time.” Clinical state is described using the GCS (Glasgow Coma Scale: a 3–15 scoring system where 3–8 indicates a severe coma) , but the trajectory also depends on how swelling behaves, how ICP is controlled, and whether ICU complications are prevented.
- Use the Contents box to jump to what you need right now (First 72 Hours, ICP & swelling, hydrocephalus/EVD, sedation vs coma, seizures, and key lesion pages such as brain contusions and EDH).
Most families only need the Key Takeaways + the First 72 Hours and ICP / swelling sections. Everything else is for deeper understanding.
Contents
- Who This TBI Page Is For
- TBI — Quick Summary (Read This First)
- What Is Traumatic Brain Injury?
- How Doctors Classify TBI
- Specific Types of Brain Injuries
- Epidural Hematoma
- Acute Subdural Hematoma
- Chronic Subdural Hematoma
- Brain Contusions
- Brain Concussion
- Skull Fractures
- Diffuse Axonal Injury
- Penetrating/Firearm Brain Injuries
- Combined Brain Injuries
- Clinical Assessment of the TBI Patient
- Diagnosis of Brain Injuries
- Treatment Options
- Emergency Neurosurgery (EDH,SDH)
- Indications for ICP Monitoring
- ICP Treatment
- Intensive Care and Monitoring
- First 72 hours after TBI
- Systemic Complications Management
- Early Prognosis in Coma
- Brain Death
- Early Prognosis – What Families Need to Understand
- Long-Term Prognosis and Recovery
- Medico-Legal Questions
- Glossary – Key Terms in Brain Injury
- Emergency Red Flags
- Frequently Asked Questions
- Request TBI Second Opinion Within 24 Hours
- Additional Resources
Traumatic brain injury (TBI) is the medical term doctors use for a brain injury caused by head trauma — such as a fall, traffic accident, assault, sports injury, or penetrating injury. Families may hear different phrases: head injury, brain injury, brain bleed, skull fracture, brain swelling, or severe TBI. This page explains how these findings fit together.
What Are Traumatic Brain Injuries?
A traumatic brain injury (TBI) occurs when an external mechanical force disrupts the brain’s structure or function. Mechanisms include direct impact, acceleration–deceleration forces, and penetrating trauma (e.g., firearm injury). Many severe cases show multiple combined lesions on CT — hematomas, contusions, and skull fractures — all of which influence prognosis. Lesions may be present on one or both sides of the brain and can involve any region — the cerebral hemispheres, deep brain structures (thalamus, hypothalamus, basal ganglia), brainstem, cerebellum, and others. Deep traumatic lesions are almost always more serious than superficial cortical injuries.
Types of primary brain lesions seen on imaging include epidural hematoma (EDH); acute and chronic subdural hematoma (SDH); traumatic subarachnoid hemorrhage (tSAH); cerebral contusions; intraparenchymal/intracerebral hematoma (ICH); diffuse axonal injury (DAI, often with microhemorrhages); intraventricular hemorrhage (IVH); and diffuse cerebral edema with mass effect/midline shift. Glossary – Key Terms in Brain Injury. For a more detailed look at brain anatomy, please visit our dedicated page.
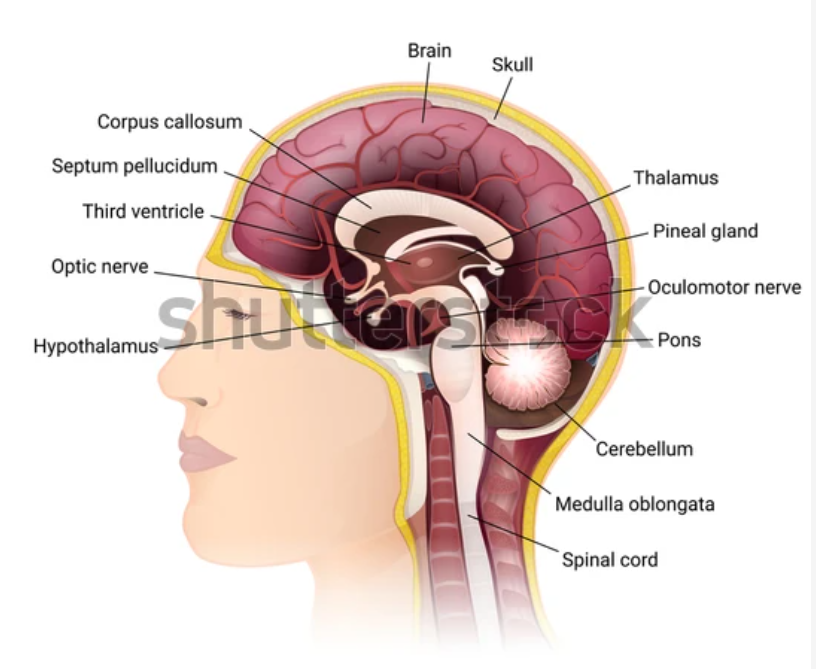
Image: Sagittal section of brain anatomy
In many patients, secondary injury occurs when a hematoma forms and exerts pressure on otherwise uninjured brain tissue (as with epidural, subdural, or intracerebral hematomas).
Understanding the exact type of brain injury helps families know what to expect — which findings are serious, which can improve, and how treatment decisions are made.
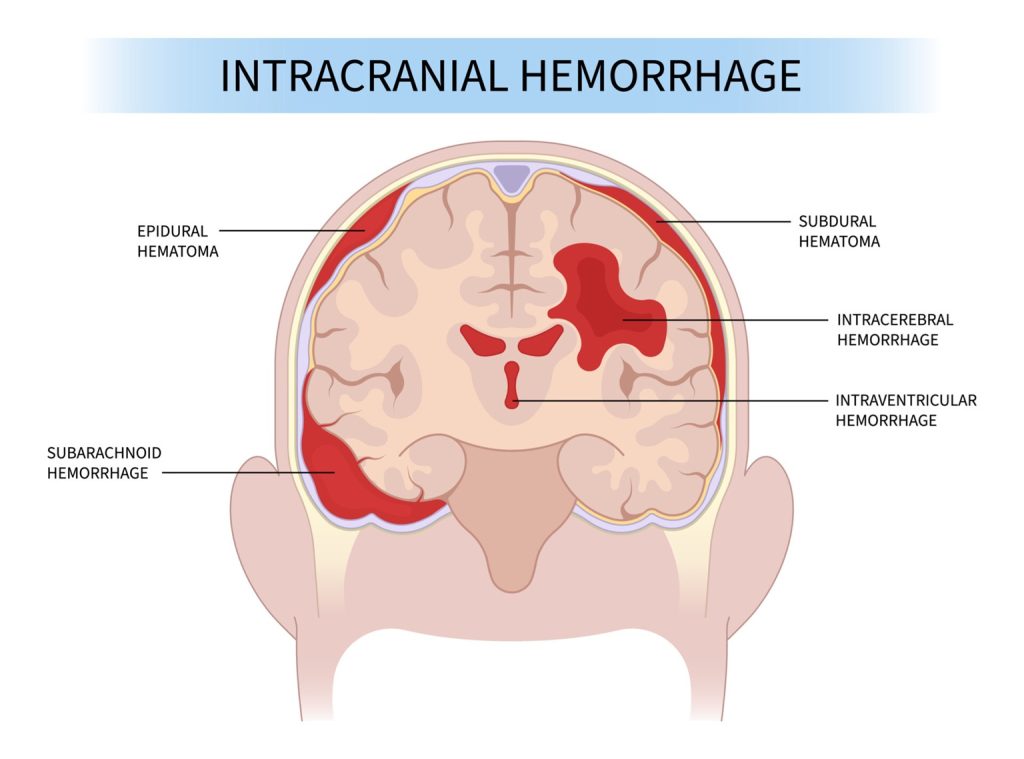
Image: Types of traumatic intracranial hematomas
Epidural Hematoma
Epidural Hematoma (EDH) most commonly results from rupture of the middle meningeal artery, which runs within the dura mater (the protective covering of the brain immediately under the skull bones) after a skull fracture. However, venous bleeding from a dural venous sinus or diploic veins (veins inside skull bones) is also possible. The blood (EDH) collects between the inner table of the skull and the dura mater. Compared with a subdural hematoma, the blood collection is typically more localized and sharply demarcated.
Epidural hematomas (EDHs) are typically caused by direct impact forces that damage the skull and the protective membrane (dura), rather than the deeper brain tissue. Consequently, patients may initially present with a relatively preserved Glasgow Coma Scale (GCS) score (meaning the patient has no or only a minor disturbance of consciousness). An isolated epidural hematoma, when treated quickly, often has a better prognosis than many other severe brain injuries.
However, when EDH is combined with other traumatic brain lesions (such as contusions, diffuse axonal injury, or cerebral swelling), it implies that powerful inertial forces (sudden acceleration/deceleration) also caused the brain to shift and twist, leading to deeper damage, particularly to the nerve fibers (diffuse axonal injury). In these combined cases, the outcome may be as poor as in other severe TBIs, because the deep injury is often more critical for long-term recovery than the surface bleeding.
Acute Subdural Hematoma (ASDH)
In Acute Subdural Hematoma (ASDH) the blood collects between the dura mater and the surface of the brain. ASDH is classically caused by tearing of the bridging veins (small veins running between the protective lining of the brain and the brain) when the brain is violently shaken inside the skull (acceleration-deceleration forces, such as those in a car crash). Cortical arterial lacerations can also contribute. In contrast to an epidural hematoma, the ASDH collection is usually diffuse, spreading over a larger area of the brain’s surface, and is less sharply localized.
Because ASDH frequently coexists with cerebral contusions (bruising of the brain tissue) and significant brain swelling, the overall prognosis is generally worse than that of an isolated Epidural Hematoma (EDH), even after surgical evacuation. This poor outcome is seen particularly in patients who are comatose at presentation.
Chronic Subdural Hematoma
Chronic Subdural Hematomas (CSDHs) often evolve from thin ASDH or initially minor, clinically silent bleeds above the brain (in the subdural space). This most commonly happens in patients with cerebral atrophy (such as elderly individuals or alcoholics) or those taking blood-thinning medications (anticoagulant therapy). Over days to weeks, a fibrous capsule forms around the collection. The blood inside gradually liquefies and increases in volume, and the CSDH gradually enlarges over weeks. So CSDH is not a classic blood clot like in other hematomas (ASDH, EDH). This can lead to slow-onset symptoms such as headache, confusion, or focal neurological deficits. Patients often do not remember having any head trauma a few weeks prior.
When the collection becomes compressive on the brain, it is an indication for surgical evacuation of the liquefied contents within the capsule. In most cases, this can be achieved through one or more burr holes (1 cm drilled holes in the skull, sometimes even under local anesthesia). This is often preferred over a larger craniotomy. Usually, a continuous drainage system is left in place for two additional postoperative days. If the hematoma is not compressive, the patient may be managed conservatively with medications and close clinical and radiological follow-up.
Brain Contusions
Cerebral Contusions are areas of focal parenchymal brain injury, typically visible on CT as regions of mixed density (blood and edema, more white and black on CT compared to gray brain tissue). Brain contusions frequently evolve during the first 48–72 hours. During this critical period, edema increases and additional bleeding may occur, which raises the risk of elevated intracranial pressure (ICP) and neurological deterioration. On CT, these initially spotty hemorrhagic changes may coalesce into a larger intracerebral hematoma, thereby increasing the mass effect.
A traumatic intracerebral hematoma (ICH) may also be present from the onset of injury, independent of evolving contusions.
Brain Concussion
Concussion is considered a form of mild traumatic brain injury (mTBI) and often presents with normal imaging studies. Typical symptoms include transient amnesia, headache, dizziness, and nausea, which may last from a few days to several months in the context of post-concussion syndrome. Symptomatic therapy is prescribed.
In more severe cases, where headache and cognitive or behavioral changes persist, only MRI may reveal subtle post-traumatic changes in the brain. Concussion therefore represents not only a medical challenge, but also a frequent medicolegal issue. This is because the subtle changes revealed by MRI are often the only objective evidence used to validate the persistent, disabling nature of the injury.
Skull Fractures
Skull fractures may be linear, depressed, or multifragmentary, and may be open or closed.
- Open depressed fractures carry a significant risk of infection (meningitis, brain abscess) if the dura mater (the thick, protective membrane of the brain) is breached.
- Fractures communicating with paranasal sinuses or the skull base (i.e., fractures near the nose, eyes, or ear canals) may lead to cerebrospinal fluid (CSF) leaks (leaking of the clear fluid surrounding the brain and spinal cord) from the nose or ear (rhinorrhea, otorrhea). This condition significantly increases the risk of meningitis.
- Depressed (impressed) fractures are sometimes associated with post-traumatic seizures, but the true cause is usually the underlying cortical brain injury beneath the fracture site. In the absence of other indications, the seizure itself is not automatically an indication for surgery of the fracture.
In practice, fractures are frequently managed surgically because of associated hematomas. However, even when isolated, surgery may be indicated to:
- relieve direct pressure on the brain,
- clean contaminated wounds,
- repair and close a lacerated dura (common with depressed fractures),
- prevent infection and persistent CSF leakage,
- and for cosmetic reasons, particularly when the fracture involves the forehead.

Image: Types of skull fractures. Read more on this page about the anatomy of the skull.
The presence of a skull fracture often indicates that the head absorbed a large amount of energy, and significant underlying brain injury may exist even in the absence of immediate symptoms. That is why patients with isolated fracture are usually hospitalised mostly for an observation.
Diffuse Axonal Injury (DAI)
Diffuse Axonal Injury (DAI) is a severe brain injury caused by strong rotational forces like in traffic accidents (the brain twisting inside the skull). DAI is fundamentally different from contusions because it involves numerous, tiny lesions spread across sensitive regions of the brain, often without large areas of bleeding visible on initial CT scans. The presence of DAI usually means that the brain is damaged more extensively, and often the brainstem is damaged as well. That is why coma lasts longer and that awakening is slower and more uncertain, even when the CT scan does not look dramatic. Of all severe traumatic brain injury pathologies, Diffuse Axonal Injury is the most common cause of persistent unconsciousness (coma).
The severity of DAI is determined by the location and extent of the damage:
- Grade I (Mild): Damage primarily involves the white matter of the cerebral hemispheres.
- Grade II (Moderate): Damage extends significantly to the corpus callosum (the main bridge connecting the two sides of the brain).
- Grade III (Severe): Damage significantly involves the brainstem.
Brainstem involvement is critical. The brainstem regulates consciousness, respiration, and autonomic control. Irreversible brainstem failure fulfills the criteria for brain death, the medical definition of death.
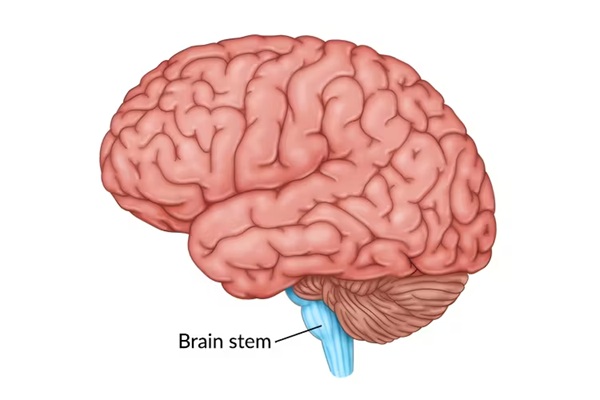
Image: Illustration of the Cerebrum, Cerebellum, and Brainstem
Traumatic Subarachnoid Hemorrhage (tSAH)
In head trauma, subarachnoid bleeding is often located over the convexity of the brain (in the surface grooves of the hemispheres). This pattern is different from the subarachnoid bleeding caused by a ruptured aneurysm, which typically collects at the base of the brain and is more abundant and much more dangerous.
However, traumatic subarachnoid hemorrhage (tSAH) is also possible due to injury to the blood vessels at the base of the brain or brain itself. If that type of tSAH is massive it carries a significantly poorer prognosis.
Intraventricular Hemorrhage (IVH)
Bleeding into the brain’s ventricles (the fluid-filled spaces) can occur after trauma on its own or by extension from nearby brain bleeding. It is often a marker of a severe injury, although not always. Prognosis depends on the amount of blood and associated lesions. When the bleeding is massive, it can block the normal flow of cerebrospinal fluid and cause acute hydrocephalus (a rapid and dangerous buildup of fluid in the brain), which requires urgent drainage of the ventricles. Read more about the anatomy of brain ventricles.
Penetrating and Firearm Injuries
Penetrating head injuries mostly include gunshot wounds and shrapnel injuries. The outcome depends mostly on how much energy the bullet carries and the path it takes through the brain.
- High-speed bullets (for example from military rifles at close range) cause massive damage by transmitting energy to brain tissues also creating a large temporary cavity (a short-lived, expanding bubble of displaced tissue) in the brain. These injuries are often fatal before the patient can reach the hospital.
- Lower-speed bullets (for example small-caliber bullets or those fired from farther away) usually cause more limited damage.
In some of these cases (usually with lower speed bullets where bullet did not damage vital brain structures) surgery can save the patient, especially if they arrive at the hospital fast and stable.
Surgery in these situations is usually aimed at cleaning the wound, stopping bleeding, removing blood clots, bone fragments and bullets if accessible, and closing the protective brain covering (dura). It is also critical to manage the resulting brain swelling and infection risks, as these secondary injuries often determine the final outcome. Sometimes a larger surgery (even decompressive craniectomy—wider opening the skull to relieve pressure) is needed.
Removing the bullet itself is usually not important unless it is easily accessible or causing further damage.
Combined Brain Injuries
Many TBIs are not isolated: for example, a patient may have a skull fracture, subdural hematoma, and brain contusions all at once. Prognosis is shaped by how these injuries interact — cumulative volume, pressure, swelling, and location matter more than any one lesion alone.
How Doctors Classify Traumatic Brain Injury (TBI)
Doctors divide traumatic brain injuries into three groups: mild, moderate, and severe. This classification is based on how awake and responsive the patient is right after the injury, how long they stay unconscious, and how long they remain confused or unable to form new memories. The most common tool is the Glasgow Coma Scale (GCS), which scores patients from 3 (deep coma) to 15 (fully awake). The GCS assesses eye opening, verbal, and motor response. A score ≤8 indicates severe TBI and need for aggressive management.
Mild TBI (Concussion) – GCS 13–15
The person may briefly lose consciousness (less than 30 minutes) or not at all. Confusion or memory gaps usually last less than 24 hours. Typical symptoms include headache, dizziness, fatigue, nausea, and trouble focusing. Most people recover completely, but symptoms may last for weeks or months in some cases, which is called post-concussion syndrome. On CT scans, mild TBI is often normal or shows only very small bruises or swelling. Surgery is almost never needed in this group. CT scanning is generally not required only for patients with GCS 14 or 15 if they are fully awake and oriented, have no loss of consciousness or amnesia, show no signs of skull fracture, have no neurological deficit (focal deficit), are not on blood-thinning medication, and have normal brain injury markers (where routinely available).
Moderate TBI – GCS 9–12
The patient may be unconscious for 30 minutes up to 24 hours. They may not wake up easily, or they may respond slowly or inappropriately. This stage is more than just confusion — patients can be very drowsy, give incorrect words or sounds instead of clear answers, or show weakness on one side of the body. Memory problems or disorientation can last days up to a week. These patients almost always need hospital monitoring and brain imaging (CT/MRI), because they are at real risk of brain swelling or bleeding. Many patients survive, but there is a higher chance of long-term problems such as difficulty with thinking, balance, speech, or personality changes. Rehabilitation is often needed. On brain CT scans, moderate TBI often shows bruises or hematomas compared to mild cases. Surgery can be required if these blood collections or swelling start to compress the brain.
Severe TBI – GCS 3–8
The patient is in a coma, with little or no response to voice or pain. They require treatment in an ICU with neurocritical monitoring (including ICP monitoring — continuous measurement of pressure inside the skull), and sometimes urgent neurosurgery. Severe injuries are commonly associated with dangerous brain swelling, bleeding, and high pressure inside the skull. The risk of death or lasting disability is high, and survivors usually require long-term rehabilitation and support. On CT scans, severe TBI usually shows more widespread brain damage, often including the brainstem. These injuries carry the worst prognosis. Surgery is most often required in this group, more frequently than in mild or moderate cases. When assessing a comatose patient (GCS 3–8) upon initial examination, it is crucial to determine if the impaired consciousness is caused by reversible factors such as alcohol, drugs, medication, or hypotension, after the correction of which the GCS score can then be reliably taken as a prognostic factor.
Clinical Assessment of the TBI Patient
The initial clinical assessment is the most critical step, designed to rapidly determine the severity of the brain injury, identify immediate life threats, and establish the patient’s overall condition. These findings dictate the initial diagnosis, treatment, and the urgency of care.
Key Elements of the Evaluation
- Mechanism and External Signs: Detailed information on how the injury occurred (e.g., speed, type of impact, such as motor vehicle accidents, falls from height, or blunt force trauma) is gathered. Doctors also immediately examine the patient for external signs of head trauma (lacerations, wounds, bleeding or clear fluid leaking from the nose or ears) and signs of skull fracture.
- Systemic Stabilization and Associated Injuries: A rapid assessment of vital signs (breathing, circulation, blood pressure) is mandatory. Hypoxia (lack of oxygen) and hypotension (low blood pressure) must be corrected immediately, as they significantly worsen brain damage. The medical team must also rapidly rule out associated injuries to the cervical spine, chest, and abdomen, which often accompany TBI.
- Glasgow Coma Scale (GCS): This is the standardized tool used to objectively measure the patient’s level of consciousness. Crucially, the GCS score is only considered a reliable prognostic factor after any reversible causes of impaired consciousness (such as alcohol, drugs, or severe shock) have been stabilized.
- Neurological Examination: This includes checking for pupil asymmetry (a critical sign of mass effect/pressure) and performing a focal exam to detect specific neurological deficits (e.g., weakness on one side) that pinpoint the location of the brain damage.
- Routine Labs and Brain Biomarkers: In addition to routine laboratory work (which confirms the status of all systemic organs), specialized brain injury biomarkers (blood tests measuring proteins like GFAP) are increasingly used to help physicians safely rule out the need for a CT scan in low-risk mild TBI patients (GCS 14–15).
Diagnosis of Brain Injuries
CT Scan as the Gold Standard
CT is fast, accessible, and detects hematomas, contusions, fractures and mass effect. In severe trauma, a whole-body CT with contrast is often performed as part of the initial workup to rule out associated injuries. Early CT is vital as it guides life-saving intervention.

Image: CT brain images- different types of traumatic lesions
Role of MRI in Selected Cases
MRI is superior in detecting DAI, microhemorrhages, and ischemic changes not seen on CT. It is useful especially in unexplained deficits or prolonged coma.
Importance of Follow-Up Imaging in ICU Patients
Serial CT imaging is mandatory in ICU settings, as hematoma expansion or new bleeds often occur days later. Any neurological deterioration warrants repeat scan.
TBI Treatment: Surgical Procedures, ICU Management, and Rehabilitation
Emergency Neurosurgery: When Is a Craniotomy Required to Save a Life (EDH/SDH)?
Hematomas (epidural, subdural, intracerebral) must be evacuated if they are compressive on the brain by volume or location, or if imaging predicts that they will become compressive within 24 hours. Such decisions require an experienced neurosurgeon who can weigh lesion size, location, and associated injuries. Procedures can include craniotomy (skull opening with removing and fixing bone flap after hematoma evacuation), decompressive craniectomy (not replacing bone flap because of increased brain edema [swelling]), ICP monitor placement, and/or EVD (external ventricular drain) to drain CSF and reduce intracranial pressure.
During this surgery or independently, additional procedures are performed to address major scalp lacerations, depressed skull fractures, dural tears (damage to the dura mater), frontal sinus injuries, and to debride (clean) complex or contaminated wounds, among others.

Image: Surgical opening of the skull (craniotomy) for removal of epidural hematoma
ICP monitor placement, and/or EVD (external ventricular drain) in TBI
ICP monitoring and/or placement of an external ventricular drain (EVD) may be used to monitor and reduce intracranial pressure and to drain cerebrospinal fluid when indicated.
Typical indications include:
- severe traumatic brain lesions with markedly impaired level of consciousness
(Glasgow Coma Scale 8 or lower), - acute hydrocephalus caused by intraventricular blood,
- massive intraventricular hemorrhage with impaired or obstructed cerebrospinal fluid circulation,
- the need for deep sedation and mechanical ventilation in patients with traumatic brain lesions on CT that demonstrate extensive mass effect or are at high risk of secondary intracranial pressure elevation.
In clinical practice, the decision to place an ICP monitor or EVD is individualized. It is influenced by the patient’s overall condition, the pattern and evolution of injury, the treating neurosurgeon’s judgment, and the resources and protocols of the treating ICU.
In a small number of highly specialized neurotrauma centers, additional monitoring techniques may be used alongside ICP measurement. These can include brain tissue oxygen monitoring, which measures oxygen levels in brain tissue near the injured area. This type of monitoring is not routine, is available only in selected centers, and is mainly used in complex cases to fine-tune intensive care management.
Management of Increased Intracranial Pressure (ICP) in the ICU
Raised intracranial pressure (ICP) is a serious complication where the pressure inside the skull dangerously compresses brain tissue, restricting blood flow and causing secondary, stroke-like damage. ICP is continuously measured using a small pressure sensor surgically placed by the neurosurgeon.
Treatment in the intensive care unit focuses on maintaining brain blood flow and reducing pressure through several key measures:
- Positioning: The patient’s head is slightly elevated to help venous drainage (improve blood flow out of the brain).
- Sedation: Sedation and pain medication reduce agitation and pain-related pressure spikes.
- Osmotherapy: Medications (such as mannitol or hypertonic saline) are used to draw excess fluid out of the brain tissue.
- Controlled Hyperventilation (via a respirator/ventilator) is a time-limited intervention used to temporarily lower dangerously high Intracranial Pressure (ICP) by reducing blood CO2 levels, which causes the brain’s blood vessels to constrict and rapidly decreases blood volume inside the skull.
- Seizure Prevention: Antiepileptic drugs (such as levetiracetam) are often given in first 7 days to prevent seizures, which may further increase ICP. (Note: Steroids are generally not used to treat traumatic brain swelling.)
If pressure remains high despite these treatments, surgical options may be necessary: EVD (external ventricular drain) to drain CSF (fluid) or decompressive craniectomy (removing a skull bone flap to give the swollen brain more room).
Intensive Care and Monitoring (ICU): Stabilizing Vitals and Preventing Secondary Brain Damage
ICU care involves the continuous management of homeostasis (maintaining the body’s stable internal environment). This includes managing oxygenation, blood pressure, sedation, ventilation (breathing support), and fluid and electrolyte balance (managing water and essential body salts and other important molecules in blood). The primary goal is to prevent secondary ischemic injury (damage caused by restricted blood flow or lack of oxygen that occurs after the initial trauma) and other complications.
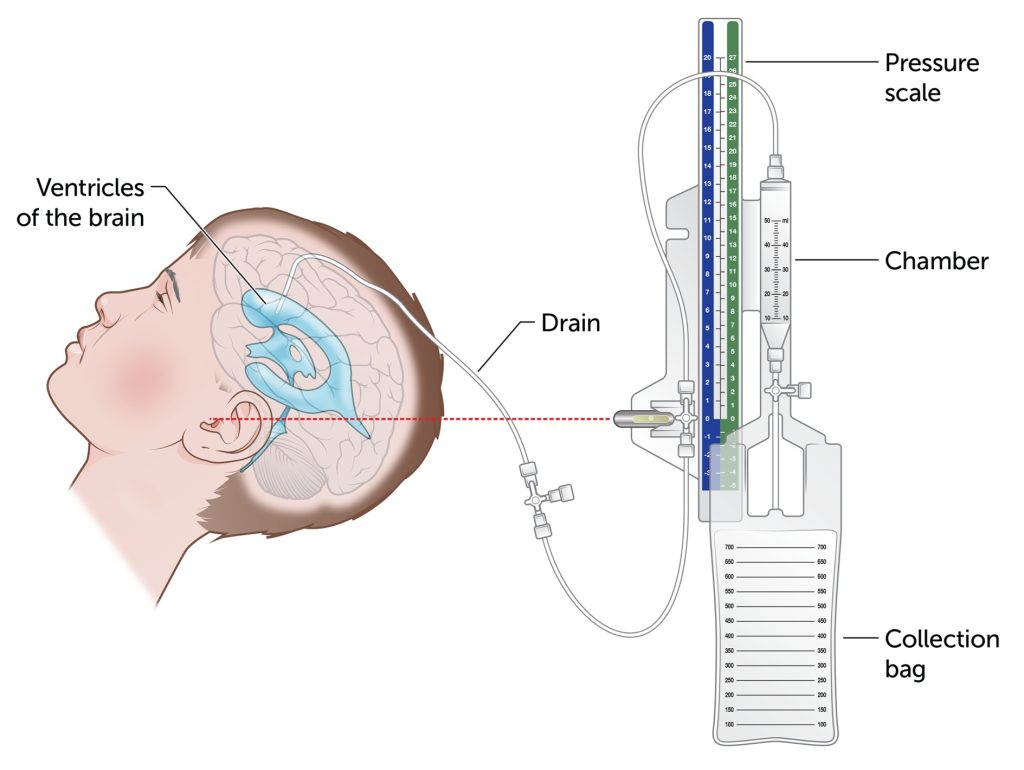
Image: Placement of an external ventricular drain (EVD) for monitoring and lowering intracranial pressure
Expected ICU Recovery Pattern in the First 72 Hours
The first 72 hours after a traumatic brain injury are often the most unpredictable. During this period, the medical team focuses on stabilizing vital functions, controlling intracranial pressure, deciding about surgery, adjusting sedation, and preventing secondary brain injury. It is common for patients with severe and moderate TBI to remain unresponsive or minimally responsive even after surgery or initial treatment — this does not automatically indicate deterioration. Typical day-to-day changes include fluctuations in eye-opening, breathing patterns, limb movements, and ICP trends, which are often influenced by sedation and swelling rather than permanent damage. Families should know that meaningful neurological changes usually appear gradually, and some findings that look concerning (such as lack of eye-opening) can still be part of a normal early trajectory.
Families often feel overwhelmed during the first days after a traumatic brain injury — not knowing whether slow awakening, fluctuating movements, or continued ventilation are normal. These questions are extremely common, and many early signs can look alarming even when the patient is following a typical recovery pattern. Clear, individualized explanations often bring the reassurance and direction families need during this uncertain time. We aim to provide that clarity on this page — and, when needed, through an online neurosurgical consultation.
Preventing Late Fatalities: Management of Systemic Complications (Pneumonia, Sepsis, Organ Failure)
Many late fatalities result from systemic complications: pneumonia, sepsis, multiorgan failure, pulmonary embolism, gastrointestinal (GI) bleeding, renal/hepatic dysfunction, pressure sores and constipation. Vigilant prevention, early diagnosis, and prompt treatment are essential. Addressing systemic complications such as sepsis, pneumonia, and organ failure is paramount, as these conditions significantly increase the risk of secondary ischemic injury and late fatalities.
Multidisciplinary Rehabilitation
Rehabilitation should begin as early as possible (in ICU and beyond), with physical, occupational, and speech therapies to support functional recovery via neuroplasticity.
Early Prognosis in Patients with Coma
Prognosis depends on the severity and location of the brain injury, as well as on systemic complications (such as infections, pneumonia, or blood clots) during the ICU stay.
In patients in deep coma, recovery often follows a stepwise pattern:
- first, return of basic vital brainstem functions such as spontaneous breathing, coughing, swallowing, and stabilization of blood pressure
- then defensive movements of the limbs (for example withdrawing from pain)
- later, recovery of functions such as eye opening and purposeful limb movements. It is also important to know that after days to weeks, many patients in coma begin to open their eyes as sleep–wake cycles return; this can reflect wakefulness without awareness (vegetative state/unresponsive wakefulness syndrome), not true alertness
- finally, return of higher brain functions including speech, awareness of surroundings, and purposeful interaction.
This staged recovery may take days to weeks, and the pace and extent of improvement vary greatly among patients.
Each stage carries unique risks — aspiration, pneumonia, sepsis, thrombosis, metabolic derangements — so intensive monitoring and intervention are required. Families often are not aware of these phases and may request second opinion during the ICU phase.
Brain Death After Severe Traumatic Brain Injury — What Families Need to Know
In the most severe forms of traumatic brain injury (TBI), the brain can suffer irreversible damage, including the complete failure of the brainstem. This condition is called brain death.
Understanding the Appearance of Life
It can be deeply confusing to see a loved one who appears “alive” because their heart is still beating and a ventilator is moving their lungs. However, brain death means that the brain has permanently lost the ability to control:
- Consciousness (the person cannot wake up)
- Breathing (the person cannot breathe without the machine)
- Vital reflexes (automatic responses that keep us alive)
Medically and legally, brain death is considered death. The heart continues to beat only because it has its own internal electrical system and is being supplied with oxygen by the ventilator.
How Is Brain Death Confirmed?
Clinically, brain death is suspected when a patient shows no response after all sedation has completely worn off. Doctors follow a strict, multi-step medical protocol to confirm the diagnosis:
- Brainstem reflex checks: Testing for brainstem reflexes, including the reaction of the pupils to light, corneal reflexes (the eye surface response to gentle touch), and protective airway reflexes such as coughing or gagging, which normally prevent choking.
- Apnea testing: A carefully controlled clinical procedure in which mechanical ventilation is briefly paused to determine whether the brain can initiate breathing on its own as carbon dioxide levels rise. In brain death, no spontaneous breathing effort is observed despite this natural stimulus. The test is performed under strict monitoring and safety protocols. Safety First: The apnea test is only performed if blood pressure and oxygen levels are stable. If these safety criteria cannot be met, doctors will use alternative confirmatory tests instead.
- Spinal reflexes: Families may sometimes observe small movements (such as a twitch or brief limb movement). These are spinal reflexes originating from the spinal cord, not the brain, and do not indicate consciousness or recovery.
- Confirmatory tests: To ensure absolute certainty, doctors may perform additional studies such as EEG, CT angiography, or nuclear medicine scans to confirm the absence of electrical brain activity or cerebral blood flow.
These examinations are often repeated after a defined time interval to ensure that the findings are permanent and not influenced by medications, metabolic disturbances, or temporary suppression of brain function.
The Crucial Difference
It is important to understand that brain death is not the same as coma or a persistent vegetative state.
- In a coma, some brain activity is still present, and recovery may be possible.
- In brain death, the damage is complete and irreversible.
This process is designed to protect both the patient and the family, ensuring that the diagnosis is accurate, ethical, and beyond doubt. Once brain death is confirmed according to these strict protocols, physicians will discuss the next steps with the family, which may include withdrawal of mechanical support or, when appropriate, the possibility of organ donation.
Families Often Need Additional Explanation During the Early ICU Phase
Many families visit this page because they want to understand the prognosis — whether the signs they are observing are good, bad, or simply expected at this early stage. After a traumatic brain injury, dozens of clinical parameters influence recovery, and some of the most important prognostic indicators are not obvious to non-medical observers. Certain findings that look alarming may still be compatible with a stable trajectory, while other subtle changes — which families may not even notice — can carry meaningful prognostic value.
Interpreting these patterns requires experience. The early post-injury period includes complex interactions between the type of injury, baseline neurological status, the degree of swelling, the effects of sedation, ICP trends, ventilator settings, and the patient’s spontaneous responses. No single finding can predict recovery; what matters is how these elements fit together. This is why two patients with seemingly similar injuries may progress very differently in the first hours and days.
Families often receive brief or highly technical updates, leaving them unsure how to interpret what they see at the bedside. They want to know whether slow awakening, minimal movement, or fluctuating responsiveness indicate improvement or deterioration — and whether certain changes should be considered warning signs or normal early-phase variability. Without clinical context, it is nearly impossible to make sense of these observations.
On this page, we aim to offer clear, structured explanations of the principles behind early ICU recovery. And when needed, we can help you understand what the current findings may mean in your specific case through an individualized neurosurgical consultation.
If you need help understanding your loved one’s early ICU findings, you may send a brief description of the situation. Most families receive a neurosurgical consultation within 24 hours or within 3 hours with the priority option.
We can help you understand whether the current signs are expected, concerning, or simply part of the early recovery pattern.
Details about how the consultation works and the consultation fee are explained here .
Recovery and Long-Term Prognosis of Brain Injuries
Rehabilitation After Brain Injury
Structured therapy targeting motor, cognitive, and speech deficits is key. Most improvement occurs in first 6–12 months, but plasticity allows gradual gains even beyond.
Possible Complications
Long-term risks include epilepsy, hydrocephalus, cognitive/behavioral deficits, mood disorders, hormonal dysregulation, motor disabilities.
Quality of Life After Severe Brain Trauma
Outcomes range from full independence to need for lifelong care. The degree of recovery depends heavily on the initial severity, lesion location (especially brainstem), and how well complications were prevented and managed.
Levels of Recovery After Severe Brain Injury
Good recovery
The person returns to normal daily life, including work or school. They may notice minor issues (headaches, fatigue, slower thinking), but function independently.
Moderate disability
Lives independently at home and manages basic needs, but often can’t return to the previous job or school level. Lasting issues can include memory and attention problems, balance troubles, or personality changes.
Severe disability
Awake, but needs daily help for basic activities (dressing, eating, hygiene). May sit or move only with assistance; speech, memory, or movement are markedly limited. Cannot live independently.
No meaningful awareness (also called a vegetative state)
Sleep–wake cycles and breathing may be present, but there is no clear awareness of self or surroundings. The person does not communicate or follow commands.
Medico-Legal Questions
Many patients and families wonder during treatment whether all needed tests and treatments were done. If these concerns remain unresolved, they can leave lasting doubts and may even become medicolegal issues later. We can provide an independent online second opinion to review your case.
Online consultation is already widely used in the developed world, and that is why it has many synonyms such as video consultation, virtual consultation, teleconsultation, telehealth consultation, telemedicine consultation, remote consultation, online doctor visit, virtual doctor visit, online doctor appointment, online medical advice, ask a doctor online, doctor chat online, video call with a doctor, and online second opinion.
Request TBI Neurosurgery Consultation — 24-Hour Review or Priority Option (Usually Within 3 Hours)
When a loved one is hospitalized with a traumatic brain injury, families need both clarity and reassurance. An independent second opinion helps you understand what the current findings mean — CT/MRI results, GCS, ICP trends, and the effects of sedation — while also reviewing whether the treatment plan follows best neurocritical-care practices and identifying any additional steps worth considering. The goal is to give you clear, confident guidance during a deeply uncertain time. We also provide clear guidance after the acute treatment is over — for both mild and severe brain injuries — helping patients and families understand persistent symptoms, long-term consequences, and what the recovery path realistically looks like.- ✔ Send a short message describing the condition and your main questions
- ✔ You’ll receive a reply within 24 hours if and how we can help — including the consultation cost and a suggested time
- ✔ In cases of high urgency, we can usually arrange a consultation within a few hours. If you need this, write PRIORITY in your initial messages.
- ✔ If you have them available, please send your medical documentation (CT/MRI images and hospital reports) after the initial reply.
- ✔ During the video consultation, we will explain your case clearly and answer all your questions
Consultation fees typically range from $180–250, depending on the complexity of your case.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for specialist telehealth second opinions in neurosurgery. Many patients use second opinions to confirm the diagnosis, compare treatment options, and feel confident about the next step.
Before contacting us, please read our Privacy Policy and Terms of Use.
Glossary – Key Terms in Brain Injury
GCS (Glasgow Coma Scale)
A scale from 3 (deep coma) to 15 (fully awake) used to measure brain function based on eye, verbal, and motor responses.
ICP (Intracranial Pressure)
The pressure inside the skull. High ICP can damage the brain and requires urgent treatment.
Cerebral Perfusion Pressure (CPP)
Cerebral Perfusion Pressure (CPP) is the pressure that ensures blood flow through the brain. ICU teams carefully balance Mean Arterial Pressure (MAP)—as higher blood pressure increases CPP—and Intracranial Pressure (ICP)—as higher ICP reduces CPP—in order to maintain adequate CPP.
EVD (External Ventricular Drain)
A tube placed into a brain ventricle to drain excess cerebrospinal fluid (CSF) and monitor ICP.
ICP Monitor
An ICP Monitor is a small pressure sensor inserted into the skull to continuously measure Intracranial Pressure (ICP). The monitor is typically placed inside the brain ventricles or directly into the brain tissue.
Midline Shift
Midline Shift is a displacement of the brain structures from the center, usually observed on a brain CT image. It occurs when swelling or a hematoma exerts pressure, pushing the brain away from the midline. Larger shifts indicate a more serious injury.
Mass Effect
Mass Effect – Pressure on brain tissue caused by swelling or blood collections, usually observed on a brain CT image.
Contusion
Contusion – A bruise of the brain, often seen as mixed blood and swelling on CT.
Hematoma
Hematoma – A collection of blood. In brain trauma this includes epidural (EDH), subdural (SDH), and intracerebral (ICH) hematomas.
DAI (Diffuse Axonal Injury)
DAI (Diffuse Axonal Injury) – Widespread shearing of nerve fibers, usually due to rapid acceleration or deceleration. Often explains why a person remains in coma even when CT looks mild.
tSAH (Traumatic Subarachnoid Hemorrhage)
tSAH (Traumatic Subarachnoid Hemorrhage) – Bleeding into the fluid-filled space (subarachnoid space) around the brain after trauma.
IVH (Intraventricular Hemorrhage)
IVH (Intraventricular Hemorrhage) – Bleeding into the brain’s ventricles, sometimes causing hydrocephalus.
Craniectomy (Decompressive Craniectomy)
Craniectomy (Decompressive Craniectomy) is the surgical removal of a section of the skull to allow a swollen brain to expand outward. This prevents the brain from being compressed against the skull or pushing on the brainstem, either of which can otherwise produce dangerous ischemic lesions.
Craniotomy
Craniotomy is a surgical procedure involving the temporary opening of the skull to access the brain, usually to remove a hematoma or repair other injuries. The procedure creates a bone flap which is then replaced and secured after the surgery is complete.
Brain Herniation
Brain Herniation is a life-threatening complication that occurs when swelling forces brain tissue into adjacent areas where it does not belong. This process compresses the brainstem, where the most important vital centers for survival are located.
Sedation
Sedation involves the use of medications to keep the patient calm or asleep while in the ICU. This practice helps control and reduce Intracranial Pressure (ICP), but the level of sedation must be temporarily lowered at intervals to allow for an accurate neurological assessment of the patient.
Vegetative State (Unresponsive Wakefulness Syndrome)
Vegetative State (Unresponsive Wakefulness Syndrome) – The patient opens eyes but has no awareness of themselves or surroundings.
Minimally Conscious State – A state between coma and full awareness where the patient shows small but definite signs of consciousness.
Post-Traumatic Hydrocephalus
A buildup of cerebrospinal fluid (CSF) after trauma; may require temporary or permanent drainage.
Post-Traumatic Epilepsy
Seizures occurring days to years after brain injury; often treated with antiepileptic medications.
Red Flags — When to Seek Emergency Care
If any of the following occur after a head injury, go for an urgent in-person medical evaluation (ER/urgent care):
- Sudden loss of consciousness or worsening consciousness
- Persistent or worsening headache with vomiting
- One pupil larger than the other (anisocoria)
- New weakness or numbness in one limb or side of face
- Seizure after injury
- Repeated vomiting
- Confusion, agitation, or unusual behavior
- Bleeding or clear fluid leaking from nose or ears (possible CSF)
Frequently Asked Questions About Traumatic Brain Injury (TBI)
What is a traumatic brain injury (TBI), and is it the same as a head injury?
Traumatic brain injury (TBI) is the medical term for brain injury caused by head trauma. Families may hear different terms — head injury, brain injury, brain trauma, brain bleed, skull fracture, concussion, or severe TBI — but the key question is whether the brain itself has been affected. TBI can range from mild concussion with normal CT to life-threatening bleeding, swelling, coma, raised intracranial pressure, or several traumatic lesions at the same time. A patient may have brain contusions, subdural hematoma, epidural hematoma, diffuse axonal injury, skull fracture, traumatic subarachnoid hemorrhage, or hydrocephalus after the same injury.
What are the main types of traumatic brain injury?
The main types of traumatic brain injury include concussion, epidural hematoma, acute or chronic subdural hematoma, brain contusions, traumatic intracerebral hemorrhage, diffuse axonal injury, traumatic subarachnoid hemorrhage, intraventricular hemorrhage, skull fractures, and penetrating or firearm injuries. Some TBI lesions are focal, such as a hematoma compressing one area of the brain. Others are diffuse, such as diffuse axonal injury, where widespread microscopic damage affects brain connections. Each type of brain injury has different risks, treatment priorities, and prognostic meaning, so the full injury pattern matters more than one label alone.
Can severe TBI include several brain lesions at the same time?
Yes. Severe TBI often includes several brain lesions at the same time, and this combined injury pattern is one of the main reasons prognosis can be difficult to explain early. A patient may have a skull fracture, acute subdural hematoma, brain contusions, diffuse swelling, traumatic subarachnoid hemorrhage, intraventricular hemorrhage, or diffuse axonal injury together. The final risk depends on lesion size, location, brainstem involvement, swelling, midline shift, intracranial pressure, hydrocephalus, and how findings evolve during the first 48–72 hours. One CT finding never tells the whole story in complex traumatic brain injury.
What is the difference between mild, moderate, and severe TBI?
Traumatic brain injury is usually classified as mild, moderate, or severe according to the clinical state after injury, especially the Glasgow Coma Scale, duration of unconsciousness, and duration of confusion or memory loss. Mild TBI usually means GCS 13–15 and often includes concussion, with normal CT or only minor findings. Moderate TBI usually means GCS 9–12 and requires hospital observation because bleeding or swelling may evolve. Severe TBI usually means GCS 3–8, coma, ICU care, mechanical ventilation, intracranial pressure monitoring, and sometimes urgent neurosurgery. Imaging and clinical evolution refine the prognosis.
Which TBI findings can be seen on CT or MRI after head trauma?
CT and MRI after head trauma can show different traumatic brain injury findings. CT is usually the first emergency scan because it quickly detects epidural hematoma, subdural hematoma, intracerebral bleeding, brain contusions, skull fractures, mass effect, midline shift, swelling, intraventricular blood, and hydrocephalus. MRI is more sensitive for diffuse axonal injury, microhemorrhages, small ischemic changes, and subtle post-traumatic lesions not clearly visible on CT. A normal early CT does not always exclude clinically important TBI, especially concussion, diffuse axonal injury, or evolving injury that becomes clearer on repeat imaging.
When should a CT scan be done after a head injury?
A CT scan after a head injury is needed when there are signs that traumatic brain injury may include bleeding, swelling, skull fracture, or neurological risk. Urgent imaging is especially important after loss of consciousness, worsening headache, repeated vomiting, confusion, seizure, weakness, unequal pupils, clear fluid from the nose or ear, anticoagulant use, high-energy trauma, or declining alertness. CT is also required in moderate or severe TBI and in many elderly patients even after seemingly minor trauma. The goal is to detect surgically important lesions such as epidural hematoma, subdural hematoma, contusions, fractures, or mass effect early.
Can traumatic brain injury worsen even if the first CT scan looks stable?
Yes. Traumatic brain injury can worsen even when the first CT scan looks stable because bleeding, swelling, contusions, hydrocephalus, or intracranial pressure may evolve over time. Brain contusions often enlarge or become more swollen during the first 48–72 hours. A small subdural hematoma or intracerebral hemorrhage may expand. Intraventricular blood can obstruct cerebrospinal fluid flow and cause acute hydrocephalus. Diffuse swelling can increase pressure inside the skull. This is why severe TBI requires repeated neurological examinations, ICU monitoring, and sometimes follow-up CT scans even when the initial imaging does not appear dramatic.
Why are the first 48–72 hours after severe TBI so important?
The first 48–72 hours after severe TBI are critical because traumatic brain injury is dynamic, not fixed. During this early period, brain contusions may enlarge, swelling may increase, intracranial pressure may rise, hydrocephalus may appear, seizures may occur, and systemic problems such as low oxygen or low blood pressure can worsen secondary brain injury. ICU teams monitor neurological signs, CT changes, sedation level, ventilation, blood pressure, electrolytes, and intracranial pressure when indicated. Families should understand that slow awakening, fluctuating movements, or continued ventilation during this phase do not automatically define the final prognosis.
Which types of traumatic brain injury most often need surgery?
TBI surgery is most often needed when bleeding, swelling, fracture, hydrocephalus, or mass effect threatens brain tissue or brain blood flow. Common surgical situations include compressive epidural hematoma, acute subdural hematoma with mass effect, large traumatic intracerebral hematoma, expanding brain contusions, depressed skull fracture, open contaminated fracture, dural tear, persistent cerebrospinal fluid leak, frontal sinus injury, penetrating brain injury, or severe swelling requiring decompressive craniectomy. Surgery does not “repair” damaged brain tissue directly; it removes compression, drains fluid or blood, closes protective layers, prevents infection, and gives the brain more room when pressure is dangerous.
Which types of TBI usually need ICU monitoring?
TBI usually needs ICU monitoring when the patient has severe brain injury, impaired consciousness, high risk of swelling, mass effect, intracranial pressure elevation, seizures, hydrocephalus, or respiratory failure. ICU monitoring is common in acute subdural hematoma with swelling, large contusions, traumatic intracerebral hemorrhage, diffuse axonal injury with coma, intraventricular hemorrhage, traumatic hydrocephalus, penetrating injuries, and severe skull fractures with associated brain damage. ICU care focuses on preventing secondary brain injury by controlling oxygenation, blood pressure, ventilation, sedation, seizures, temperature, electrolytes, infections, and intracranial pressure when monitoring is used.
What is the difference between bleeding, swelling, brain contusion, and diffuse axonal injury after TBI?
After traumatic brain injury, bleeding, swelling, brain contusion, and diffuse axonal injury describe different mechanisms. Bleeding means blood collects in or around the brain, as in epidural hematoma, subdural hematoma, traumatic intracerebral hemorrhage, traumatic subarachnoid hemorrhage, or intraventricular hemorrhage. Swelling means brain tissue becomes edematous and may raise intracranial pressure. A brain contusion is a bruised area of brain tissue that can bleed and swell over days. Diffuse axonal injury is a deeper wiring injury caused by rotational forces, often explaining coma when CT does not show a large compressive hematoma.
Why can a TBI patient stay unconscious even when CT does not look dramatic?
A TBI patient can remain unconscious even when CT does not look dramatic because some severe brain injuries are not well seen on early CT. Diffuse axonal injury is the classic example: rotational forces damage widespread brain connections, especially in white matter, corpus callosum, or brainstem, while CT may show only small hemorrhages or appear relatively mild. Sedation, seizures, metabolic problems, hypoxia, hydrocephalus, swelling, or brainstem involvement can also delay awakening. In this situation, MRI, neurological examination, EEG when seizures are suspected, and clinical evolution over time are often more informative than the first CT alone.
What is intracranial pressure (ICP), and why is high ICP dangerous after TBI?
Intracranial pressure (ICP) is the pressure inside the skull, and high ICP after TBI is dangerous because the skull cannot expand. Bleeding, swelling, hydrocephalus, or mass effect can raise pressure and compress brain tissue. High ICP can reduce cerebral blood flow and cause secondary ischemic injury, similar to a stroke-like process after the original trauma. Severe TBI patients may need sedation, head elevation, osmotherapy, controlled ventilation, EVD drainage, ICP monitoring, or decompressive surgery to control pressure. The treatment target is not only the visible hematoma, but also preservation of brain blood flow and prevention of secondary damage.
What is an external ventricular drain (EVD), and when is it used after traumatic brain injury?
An external ventricular drain (EVD) is a tube placed into a brain ventricle to drain cerebrospinal fluid and help monitor or reduce intracranial pressure after traumatic brain injury. It may be used when severe TBI causes acute hydrocephalus, intraventricular hemorrhage, obstructed cerebrospinal fluid flow, or dangerous pressure elevation. An EVD can both measure pressure and remove fluid when pressure rises. It is especially important when blood blocks the normal fluid pathways or when swelling and pressure dynamics require active drainage. The decision to place an EVD depends on CT findings, neurological status, pressure risk, and ICU resources.
Why is my loved one still not waking up after traumatic brain injury?
A patient may not wake up after traumatic brain injury for several reasons, and early non-awakening is not always a final prognosis. Deep sedation, brain swelling, high intracranial pressure, hydrocephalus, seizures, diffuse axonal injury, brainstem involvement, metabolic problems, infection, low oxygen, or systemic complications can all delay responsiveness. After severe TBI, awakening often happens gradually and may fluctuate from day to day. The important question is not only whether the patient wakes immediately, but how the neurological examination, CT or MRI findings, ICP trends, sedation reduction, breathing, reflexes, and systemic condition evolve over time.
Can sedation make a severe TBI patient look worse than they really are?
Yes. Sedation can make a severe TBI patient look less responsive than the true brain injury alone would suggest. In the ICU, sedation is often necessary to control agitation, pain, ventilation, seizures, and intracranial pressure spikes. A deeply sedated patient may not open the eyes, move purposefully, or respond to commands even if some brain function is preserved. Doctors periodically reduce sedation when safe to reassess neurological status. However, sedation is only one part of the picture. Diffuse axonal injury, swelling, hydrocephalus, seizures, metabolic problems, and brainstem injury must also be considered when a patient is not waking.
Does opening the eyes mean consciousness has returned after severe brain injury?
Eye opening after severe brain injury does not always mean that consciousness has returned. After days or weeks, some TBI patients begin to open their eyes as sleep–wake cycles recover, but they may still have no clear awareness of themselves or the environment. This is called unresponsive wakefulness syndrome, also known as vegetative state. A minimally conscious state is different because the patient shows small but definite signs of awareness, such as inconsistent command following or purposeful behavior. Families should not judge recovery only by eye opening; interaction, command response, purposeful movement, and neurological trajectory are more important.
How do doctors estimate prognosis after severe traumatic brain injury?
Prognosis after severe traumatic brain injury is estimated from the whole clinical and imaging pattern, not from one CT finding alone. Doctors consider the Glasgow Coma Scale, pupil reactions, age, mechanism of injury, CT or MRI lesions, brainstem involvement, diffuse axonal injury, swelling, midline shift, intracranial pressure control, hydrocephalus, seizures, oxygenation, blood pressure, and ICU complications. Evolution over time is crucial. Two patients with similar initial CT scans may recover differently if one develops high ICP, pneumonia, sepsis, hydrocephalus, or persistent seizures. Prognosis is therefore a process of repeated assessment, not a single early prediction.
What complications are common in the ICU after severe TBI?
Severe TBI can lead to both neurological and systemic ICU complications. Neurological complications include high intracranial pressure, worsening swelling, hydrocephalus, seizures, new bleeding, ischemic injury, brain herniation, and delayed awakening. Systemic complications include pneumonia, sepsis, pulmonary embolism, gastrointestinal bleeding, kidney or liver dysfunction, electrolyte disturbances, pressure sores, constipation, malnutrition, and blood pressure or oxygenation instability. These complications can strongly influence recovery because they may cause secondary brain injury after the original trauma. Good ICU care is therefore focused not only on the CT findings, but also on preventing and treating complications early.
When should families seek a second opinion after traumatic brain injury?
Families should seek a second opinion after traumatic brain injury when the patient is not waking as expected, explanations feel unclear, CT or MRI findings are difficult to understand, surgery or ICU decisions are being discussed, or the prognosis remains uncertain. A second opinion may also help when there are combined lesions such as subdural hematoma, contusions, diffuse axonal injury, swelling, hydrocephalus, skull fracture, or high intracranial pressure. The goal is not to replace the treating ICU team, but to help families understand what the findings mean, which risks are most important, and whether the treatment strategy is reasonable.