Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: January 10, 2026
Who is this page for?
This page explains how lumbar disc herniation causes pain in the lower back and legs, what MRI findings actually mean, and when conservative treatment or surgery should be considered. Reading it first will help you better understand your condition before scheduling a consultation.
- Persistent low back pain or sciatica that does not improve with treatment — during a telehealth consultation, we help determine whether the disc is truly the pain generator and discuss surgical and non-surgical options.
- Surgery was already recommended? Request an online second opinion on microdiscectomy, endoscopic discectomy, or spinal fusion — with a clear explanation of benefits, risks, and long-term outcomes. Lumbar disc herniation is one of the most frequently over-diagnosed and over-treated conditions. Many patients are told their pain is ’caused by a disc,’ but in fact, many herniated discs do not require surgery, and not all sciatica is disc-related.
When patients usually seek a second opinion for lumbar disc herniation & sciatica
- Low back or leg pain persists despite conservative care
- Pain keeps recurring after temporary improvement
- MRI/CT shows a herniated disc but it’s unclear if it’s the pain generator
- You are considering injections, procedures, or surgery
If this reflects your situation, a focused telehealth review can clarify the true pain generator, what treatments are reasonable, and what is — and is not — indicated in your case: Request Consultation
Lumbar disc herniation (often called herniated disc or slipped disc) is among the most common spinal disorders. It is also one of the most frequently over-diagnosed and over-treated conditions. Many patients are told that their back or leg pain is “caused by a disc,” but in fact, most herniated discs do not require surgery, and not all sciatica is disc-related.
Contents
- Who is this page for?
- What Is Lumbar Disc Herniation?
- Terms That Cause Misunderstanding
- Types of Disc Herniation
- Clinical Relevance of Types
- Location of Herniation
- Ways Herniation Causes Symptoms
- Symptoms and Sciatica
- Neurologic Deficits
- Common Lumbar Radiculopathies
- Cauda Equina Syndrome
- Diseases That Mimic Disc Pain
- Diagnosis of Disc Herniation
- Herniation vs Spondylosis/Stenosis
- Misdiagnosis and MRI Overuse
- Pain Contributing Factors That Should Also Be Diagnosed
- Conservative (Non-Surgical) Treatment
- When Do You Need Surgery?
- Surgical Options
- Percutaneous Discectomy and Nucleoplasty
- Potential Risks and Complications
- Chronic Pain After Disc Surgery (FBSS)
- Surgery and Spondylolisthesis
- Interbody Fusion Overview
- Prognosis and Recovery
- Role of Second Opinion/Online Consultation
- FAQ — Lumbar Disc Herniation & Sciatica
- Additional Resources/Information
- Start Telehealth Consultation
Is the Herniated Disc Really Causing Pain — and Is Surgery Needed?
A lumbar disc herniation seen on MRI does not automatically mean that the disc is the true cause of pain or that surgery is required. Many patients have disc bulges and protrusions on MRI without symptoms. At the same time, sciatica-like pain may also come from spinal stenosis, facet joints, sacroiliac joints, piriformis syndrome, peripheral nerve entrapment, myofascial pain, or other pain generators.
The key question is not only whether a herniated disc exists, but whether it truly matches the patient’s pain pattern, neurological findings, and affected nerve root. If the disc is compressing or irritating the correct nerve root, treatment still depends on severity. Many lumbar disc herniations improve without surgery, especially when there is pain without progressive weakness. Surgery is usually considered when severe leg pain persists despite proper treatment, when neurological weakness progresses, or when urgent signs such as cauda equina syndrome appear.
What Is Lumbar Disc Herniation?
The lumbosacral spine consists of five lumbar vertebrae (L1–L5) and the sacrum (S1–S5), which is a single fused bone connecting the spine to the pelvis.
Between each pair of lumbar vertebrae lies an intervertebral disc, forming a total of five lumbar discs, numbered according to the vertebrae they separate — for example, L1–L2, L2–L3, L3–L4, L4–L5, and L5–S1 (the last one being between the fifth lumbar vertebra and the sacrum).
These discs act as flexible cushions that absorb mechanical stress during movement and load-bearing. Each disc has a soft, gelatinous center (nucleus pulposus) surrounded by a tough, fibrous ring (annulus fibrosus) that provides strength and limits excessive motion.

Image: Anatomy of a lumbar spinal segment showing two vertebrae with the disc between them acting as a shock absorber. Learn more on our Pain Anatomy page.
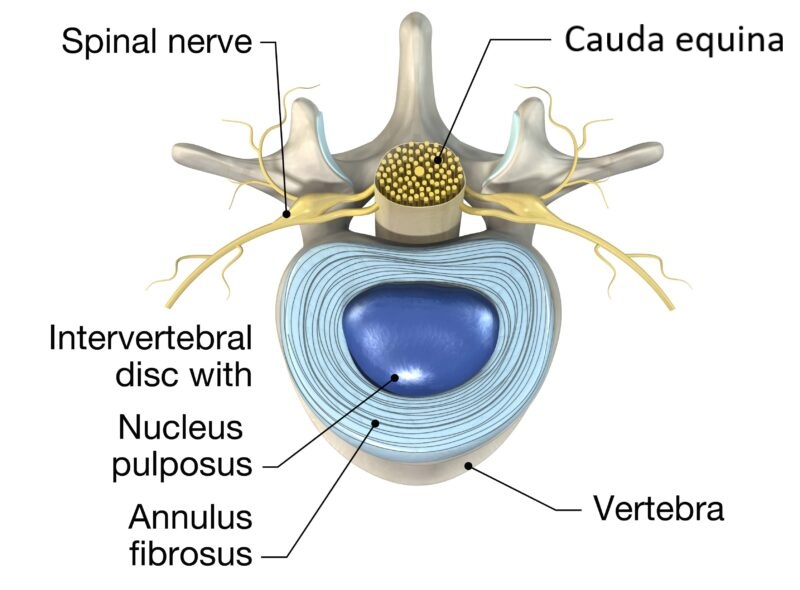
Image: Anatomy of the lumbar intervertebral disc, showing its structure and relation to the spinal canal, nerve roots, and the cauda equina (a bundle of nerve roots, not the spinal cord in this region).

Image: Anatomy of the layers covering the nucleus pulposus (the soft part of the intervertebral disc) — the annulus fibrosus and the posterior longitudinal ligament (a fibrous band covering the anterior wall of the spinal canal).
Terms About Lumbar Disc Herniation That Most Often Cause Misunderstanding
Terms that patients encounter in radiology reports, on websites, or even when speaking with spinal surgeons or physiotherapists can differ and often be confusing. Frequent sources of misunderstanding are:
- Types of herniation — Patients often believe that the terms “bulging,” “protrusion,” “extrusion,” and “sequestration” describe stages of increasing severity of their illness. In reality, they are descriptive terms based on the disc’s anatomy and its relation to surrounding structures, not a strict severity scale.
- Nucleus pulposus coverings – The disc consists of the nucleus pulposus surrounded circumferentially by the annulus fibrosus. Posteriorly, the annulus is further covered by a fibrous band called the posterior longitudinal ligament. The type of disc herniation depends on whether the nucleus simply protrudes, or perforates one or both of these coverings.
- Nerve structures compressed by herniation — Many illustrations incorrectly show the spinal cord inside the lumbar spinal canal. In fact, below the level of the first lumbar vertebra, the spinal cord has already ended, and the canal contains the cauda equina (a bundle of nerve roots). Most lumbar disc herniations occur at L4–L5, L5–S1, and L3–L4. At these levels, a large central herniation typically compresses the cauda equina, not the spinal cord.
Types of Disc Herniation:
Bulging disc
A broad-based extension of the disc beyond the vertebral margins, usually involving more than 25% of the circumference. The annulus fibrosus and posterior longitudinal ligament (PLL) are intact. This is a degenerative finding rather than a true herniation, and it is one of the most over-diagnosed and over-treated conditions seen on spinal imaging.
Disc protrusion
A focal herniation where the annulus fibrosus is ruptured but the posterior longitudinal ligament (PLL) remains intact. This is the most typical form of clinically relevant disc herniation, but even here, symptoms depend on the degree of nerve involvement rather than the size of the lesion.
Disc extrusion
The nucleus material extends beyond the annulus, with the PLL still present but thinned or displaced. The base of the herniated fragment is narrower than its dome, giving a “mushroom-like” appearance. Extrusions may cause acute nerve compression but can also shrink over time.
Disc sequestration (disc prolapse)
The posterior longitudinal ligament is completely ruptured, and a disc fragment becomes separated from the parent disc. In most cases, it migrates downward within the spinal canal. Even when large, sequestrated fragments may shift away from the nerve root, reducing compression. Spontaneous resorption is more common in sequestration than in protrusions or extrusions.
Clinical Relevance of Types of Disc Herniations
Not all disc herniations are painful. MRI studies have consistently shown that many healthy individuals with no symptoms have disc protrusions or even extrusions. Disc degeneration, along with other spinal changes, can also be a normal part of aging.
Importantly, the types of herniation are not stages of increasing severity of illness. In some cases, even a disc protrusion may require surgery, while a sequestration can resolve spontaneously without surgery.
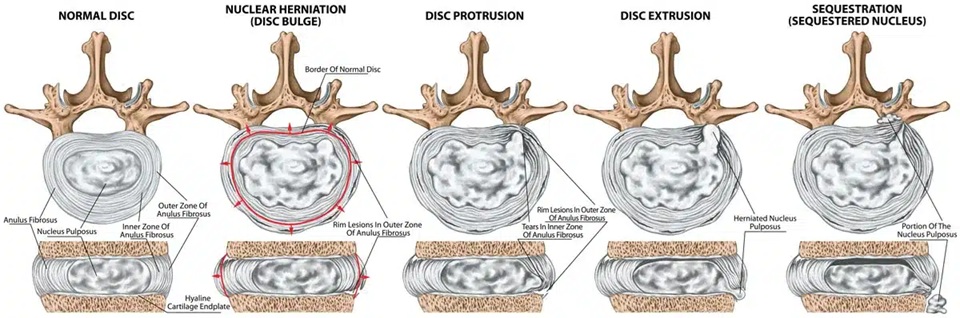
Image: Types of Disc Herniation:
Location of Lumbar Disc Herniation
Foraminal or extraforaminal (lateral/far-lateral) – The disc fragment compresses the exiting nerve root within or just outside the neural foramen. For example, a foraminal L4–L5 herniation compresses the L4 root.
Dorsomedial (central) – If large, this can compress the entire cauda equina, leading to cauda equina syndrome (a rare but urgent condition).
Dorsolateral (paramedian) – The most common type, usually affecting a single nerve root. For example, a dorsolateral L4–L5 disc herniation often compresses the L5 root.

Image : Location of lumbar disc herniation
Ways in Which Lumbar Disc Herniation Causes Symptoms
Any type of herniated fragment can irritate a nerve root by compression, inflammation, or a combination of both. When inflammation is the main factor, pain is more likely to resolve with conservative treatment and without surgery. Even if mechanical compression is dominant, it does not mean that surgery is the only treatment option. Most lumbar disc herniations occur at L4–L5 and L5–S1, and less often at L3–L4.
If the nerve root is only irritated, patients typically experience pain without a deficit. If the nerve root is more severely damaged, patients may develop neurologic deficits such as sensory changes (numbness, tingling) or motor weakness (foot drop, difficulty walking on heels or toes).
Symptoms of Lumbar Disc Herniation and Sciatica
The most characteristic symptom is sciatica — pain radiating from the lower back through the buttock and into the leg, following the course of the sciatic nerve. This pain may feel electric, stabbing, or burning. In cases of disc herniation, sciatica results from irritation of the affected nerve root. The same type of nerve root irritation can also occur in degenerative spinal conditions such as facet joint arthropathy, spondylosis, or spinal stenosis.
However, sciatica is a symptom, not a diagnosis. Pain along the sciatic nerve distribution can also result from irritation of the nerve caused by processes involving the surrounding muscles.
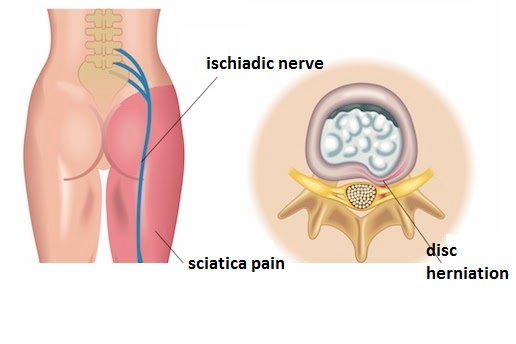
Image: Illustration showing how a lumbar disc herniation irritates or compresses the nerve root, producing sciatica
Neurologic Deficits
Radicular symptoms depend on which lumbar nerve root is affected—most commonly L4, L5, or S1. Deficits can be sensory (numbness/tingling) and/or motor (true weakness).
Sensory changes (numbness or tingling): Patients may experience reduced sensation (hypesthesia) or complete loss of sensation (anesthesia) in a dermatomal pattern along the leg. Others report tingling or pins-and-needles sensations (paresthesia), or even unpleasant burning or electric sensations (dysesthesia).
Motor weakness:
Loss of strength may involve specific muscle groups, depending on which nerve root is affected. Simple gait tests can reveal these deficits:
- Walking on heels tests ankle and toe dorsiflexion, primarily controlled by the L5 root. Weakness causes difficulty lifting the foot or toes upward.
- Walking on toes tests plantarflexion, mainly supplied by the S1 root. Weakness leads to trouble rising on the toes or maintaining balance on the forefoot.
- Foot drop (catching or tripping over the toes while walking) typically indicates L5-related dorsiflexor weakness.
The Most Common Lumbar Radiculopathies
L4 radiculopathy
- Pain/numbness/tingling: front of the thigh → inner (medial) side of the lower leg.
- Weakness: difficulty straightening the knee (quadriceps weakness); problems rising from a squat or climbing stairs.
- Reflex: reduced knee reflex (patellar reflex).
L5 radiculopathy
- Pain/numbness/tingling: outer (lateral) side of the leg and the top of the foot, often reaching the big toe.
- Weakness: difficulty lifting the foot upward (ankle/toe dorsiflexion — pulling the foot up toward the shin); heel-walking impaired; foot drop may occur.
- Reflex: usually no consistent reflex loss (occasionally the tibialis posterior reflex).
S1 radiculopathy
- Pain/numbness/tingling: back of the thigh/calf, outer edge of the foot, and little toe.
- Weakness: difficulty pushing the foot downward (plantarflexion — like pressing a gas pedal); toe-walking impaired.
- Reflex: reduced or absent Achilles reflex.
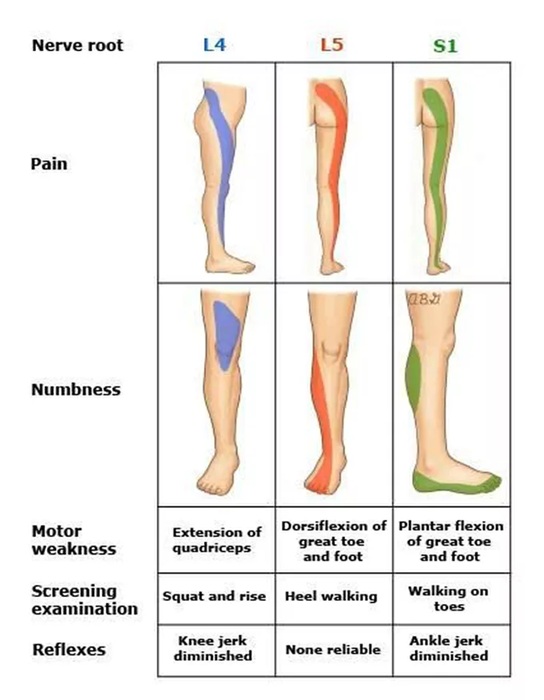
Image: Demonstration of pain and neurologic deficits for radiculopathies L4, L5 and S1
Cauda Equina Syndrome
The cauda equina (“horse’s tail”) is a bundle of lumbar and sacral nerve roots within the spinal canal below the spinal cord. These nerves control the legs as well as bladder, bowel, and sexual function.
Cauda equina syndrome happens when these roots are compressed, most often by a large central disc herniation at L4–L5 or L5–S1.
Symptoms include: severe back pain with pain in both legs, numbness in the “saddle” area (inner thighs, buttocks, perineum), leg weakness, and loss of bladder or bowel control.
It is a neurosurgical emergency. Surgery should ideally be performed within 24–48 hours to relieve pressure.
Early treatment greatly improves recovery of movement, sensation, and bladder function.
If surgery is delayed, permanent weakness or paralysis, incontinence, and sexual dysfunction are much more likely.
Diseases of the Low Back That Mimic Herniated Disc Pain
Several conditions can produce pain that looks similar or identical to sciatica from a herniated disc. Examples include:
- Piriformis muscle syndrome
- Obturator nerve entrapment
- Facet joint syndrome
- Sacroiliac joint inflammation
- Ligament inflammation or tension
- Entrapment neuropathies such as common peroneal nerve compression
- Myofascial trigger points
In such cases, MRI scans may appear normal, or they may show a disc herniation that is not actually responsible for the pain. This explains why some disc surgeries fail to relieve symptoms — the disc was not the real source of pain

Image: Piriformis Syndrome- The spasmodic piriformis muscle can compress the sciatic nerve, causing sciatica pain highly similar to the pain caused by a lumbar disc herniation.
Diagnosis of Lumbar Disc Herniation
The MRI scan is the gold standard for diagnosing lumbar disc herniation. It clearly shows the shape of the disc, its relation to the spinal canal, and whether it comes into contact with nerve roots or the cauda equina. CT can also be useful in some cases, but MRI provides more detail about soft tissues.
Additional tests such as EMG/EMNG (electromyography), SSEP (somatosensory evoked potentials), or nerve conduction studies are rarely needed, and are mainly used when symptoms and imaging do not match, or when there is suspicion of another neurological disorder.
Importantly, the presence of a herniated disc on MRI does not always mean that it is the true source of pain. Many people with herniated discs remain symptom-free, and sometimes multiple levels show abnormalities even though only one is clinically relevant.
Because of this, the final significance of imaging findings must always be assessed by an experienced clinician, who evaluates the MRI in the context of the patient’s history, symptoms, and neurologic examination.

Image: MRI scan of the lumbosacral spine — the left is a sagittal view and the right is an axial (cross-sectional) view. The red arrows mark the part of the disc that has leaked out and is pressing on the nerve roots.
Lumbar Disc Herniation vs Lumbar Spondylosis and Spinal Canal Stenosis
Spondylosis and spinal stenosis are often associated with disc herniations or mistaken for them. Spondylosis means degenerative changes of the vertebrae that lead to bony narrowing of the spinal canal, a condition called spinal canal stenosis. Radiology reports may use the terms central spinal stenosis (usually causing bilateral symptoms) and lateral recess stenosis (usually causing unilateral symptoms).
The narrowing is most commonly caused by different types of bony overgrowths (osteophytes) arising from the vertebrae and joints. Other associated terms include spondylosis, spondylarthrosis, osteophytes, and hypertrophy of the ligamentum flavum.
Clinical differences compared to disc herniation:
- Spinal stenosis usually affects older patients and develops gradually.
- Symptoms more often correspond to neurogenic claudication — pain, numbness, or weakness in the legs that worsen with walking and improve with sitting or bending forward. It is more often bilateral, but sometimes it affects only one side (unilateral).
- Surgical treatment is different from disc herniation surgery, as the goal is to decompress a narrowed canal rather than remove a single disc fragment.
- Recovery after surgery for spinal stenosis is usually less pronounced than after disc herniation surgery, but can still provide significant relief.
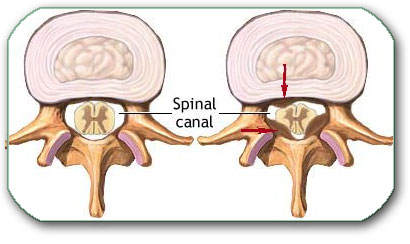
Image: Cross-section of a thoracic vertebra. On the left, the spinal canal is of normal width; on the right, it is narrowed by bony overgrowths (arrows), arising from the vertebral body and the facet (intervertebral) joint.
Misdiagnosis and Overuse of MRI Findings in Back Pain and Sciatica
Not all disc herniations are painful. MRI studies have consistently shown that many healthy individuals with no symptoms have disc protrusions or even extrusions. Early disc degeneration appears as a loss of water content, visible on MRI as a so-called “black disc.” This finding is often uncritically labeled as the main cause of low back pain, although it frequently represents a natural, age-related change rather than the true pain generator.
Modern practice often relies too heavily on MRI reports. Terms like “disc protrusion,” “degeneration,” or “bulging” alarm patients, even though these are common age-related findings. Surgery based solely on MRI without a strong clinical correlation frequently leads to persistent pain, since the real source was never treated.
Pain Contributing Factors That Should Also Be Diagnosed in Back Pain and Sciatica
In patients with persistent back pain and sciatica, treatment should not focus only on the primary anatomical pain generator. It is also important to identify additional factors that can maintain pain, increase sensitivity, delay recovery, or reduce the effectiveness of otherwise appropriate treatment.
- Mechanical overload and daily habits — prolonged sitting, poor posture, repetitive bending, lifting, or asymmetrical loading may continue to irritate already sensitized structures. Biomechanical factors such as leg length discrepancy, pelvic tilt, or degenerative conditions of the hip, knee, or foot joints may further alter load distribution and contribute to persistent pain.
- Reduced physical activity and deconditioning — loss of strength, endurance, and spinal stability often develops after long-lasting pain and makes recovery more difficult
- Metabolic factors, pro-inflammatory diet and low-grade inflammation — obesity, insulin resistance, chronic inflammation, and processed/high-sugar diet increase pain sensitivity and impair recovery
- Nutritional deficiencies — low levels of vitamin D, vitamin B12, magnesium, or iron may contribute to nerve dysfunction and slower healing
- Vitamin-related factors — both deficiency and excess of vitamin B6 may contribute to burning pain, tingling, or hypersensitivity
- Sleep disturbance and pain cycle — poor sleep increases pain perception and reduces recovery capacity
- Stress and increased muscle tone — stress does not cause the pain, but increases muscle tension and nervous system reactivity, helping maintain symptoms
- Central sensitization — in long-standing pain, the nervous system may become more reactive, amplifying pain signals even when the original irritation is reduced
- Medications and long-term drug effects — certain medications and treatment patterns may contribute to persistent symptoms or altered pain processing. For example, statins may be associated with muscle pain in some patients; prolonged use of analgesics, especially opioids, may lead to increased pain sensitivity (opioid-induced hyperalgesia); repeated corticosteroid exposure may affect tissue balance and recovery; and polypharmacy can alter symptom perception without addressing the underlying mechanism.
- Other medical conditions and comorbidities — diabetes, thyroid disorders, autoimmune diseases, fibromyalgia, osteoporosis, and chronic inflammatory conditions may increase pain sensitivity and reduce treatment response
These factors should be identified and treated, but they should not replace the central task: the primary anatomical source of pain must still be correctly diagnosed and treated. In most patients, meaningful improvement requires addressing both.
How Treatment Decisions Are Made in Lumbar Disc Herniation
Treatment decisions in lumbar disc herniation are not based on a single factor, such as MRI appearance or pain intensity alone. Instead, they depend on a combined clinical assessment of neurological findings, symptom severity, duration of symptoms, and correlation between imaging and the patient’s complaints.
In most cases, conservative treatment is the first-line approach, as the majority of disc herniations improve over time without surgery. The decision to continue non-surgical treatment or proceed to surgery is therefore based on how symptoms evolve and whether there are clear signs of neurological compromise.
Surgery is typically considered when there is progressive motor weakness, severe and persistent leg pain that does not respond to adequate therapy, or urgent neurological conditions such as cauda equina syndrome. Even in these situations, it is essential that clinical findings and MRI results clearly match, confirming that the disc herniation is the true source of symptoms.
At the same time, different specialists may reasonably recommend different approaches in borderline cases. This is because treatment decisions must balance expected pain relief, neurological recovery potential, and risks associated with surgery, while also taking into account the natural tendency of many disc herniations to regress spontaneously.
For patients, this often creates real uncertainty — one specialist may recommend continuing conservative treatment, while another suggests surgery based on the same MRI finding.
The key question is therefore not only whether a disc herniation exists, but whether it is truly responsible for the symptoms and whether waiting or surgery offers the better outcome in that specific case.
For this reason, treatment planning in lumbar disc herniation is best understood as a structured clinical decision process, rather than a fixed rule based solely on imaging findings.
Conservative (Non-Surgical) Treatment for Lumbar Disc Herniation
Around 90% of lumbar disc herniations visible on MRI — even those associated with acute sciatica — do not require surgery and typically improve with conservative treatment.
Most patients recover with conservative care:
- Medical/Conservative Treatment: The initial focus is on aggressive pain management and anti-inflammatory therapy. This often includes a combination of non-steroidal anti-inflammatory drugs (NSAIDs), pain relievers, muscle relaxants, and short-term oral corticosteroids. For persistent nerve symptoms, medications specifically targeting neuropathic pain (e.g., gabapentin or pregabalin) and certain antidepressants (e.g., tricyclics like amitriptyline or SNRIs like duloxetine) may also be used. It is essential to select an adequate combination of medications and doses, which must be closely monitored and adjusted (titrated) over an 8-week period to achieve maximal efficacy before considering the treatment a failure.
- Physical therapy: Targeted exercise programs that strengthen the core muscles and improve spinal stability. Other physical therapy protocols may be used for sciatica. Methods like Back School and certain types of spinal manipulation (manual or machine-assisted), which aim at nerve decompression, are often moderately suggested for subacute pain, though expectations often exceed their achievable clinical benefit. Conversely, traction, strict bed rest, and prolonged bracing are generally not accepted in modern protocols. Instead, relative rest is the recommended approach, which includes avoidance of prolonged sitting and limiting activities that cause pain.
- Lifestyle measures: posture correction, avoidance of prolonged sitting, chair adjustments, weight management.
- Interventional options: In selected cases, epidural steroid injections may help. The goal of these injections is to apply the medication directly to the area of the disc herniation and the nerve root to primarily reduce inflammation and achieve pain relief. The injection mixture also provides immediate pain relief via the local anesthetic and can mechanically flush irritating chemical mediators away from the nerve root. Depending on the needle path used to achieve this, there are three main approaches: the caudal approach (through a small opening at the base of the spine near the tailbone), the interlaminar approach (between the vertebral arches/laminae, which are the posterior parts of the vertebrae), and the transforaminal approach (through the small opening between two vertebrae where the nerve root exits the spinal canal). Caution is advised to limit the total cumulative dose and frequency of particulate (depot) steroids, as it is generally recommended not to exceed four epidural injections with maximum doses within a 12-month period
In the absence of severe neurological deficits, observation and conservative treatment for 6–12 weeks is the standard recommendation. Many disc herniations regress spontaneously.
Online pain consultation for low back pain and sciatica in detail
Schematic explanation of the video consultation for low back pain and sciatica
Possible Reasons Why Chronic Pain Treatment Fails
Start Your Telehealth Consultation with a Pain Specialist
If your pain treatment has failed or you’re unsure what to do next — don’t wait. A detailed telehealth consultation can help identify the exact cause of your pain, even if previous therapies didn’t work.
- ✔ First, send a short message describing your problem
- ✔ You’ll receive a reply within 24 hours if and how we can help — including the consultation cost and a suggested time
- ✔ Only then, you can send your medical documentation
- ✔ A written summary is provided when appropriate, and you may send free follow-up questions for up to 10 days
- ✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Consultation fees typically range from $180–250, depending on the complexity of your case.
This is within the usual range for specialist telehealth consultations worldwide. Thousands of patients worldwide already use telehealth consultations for second opinions — it’s safe, accepted, and effective.
Before contacting us, please read our Privacy Policy and Terms of Use.
When Do You Need Surgery for a Lumbar Disc Herniation?
Surgery is not the rule for disc herniation. It is reserved for carefully selected patients:
- Absolute indications:
- Cauda equina syndrome (loss of bladder or bowel control, saddle anesthesia)
- Progressive motor weakness
- Relative indications:
- Severe, disabling leg pain persisting beyond 6–12 weeks despite proper therapy
- Pain preventing daily functioning, sleep, or mobility
Even in these situations, surgery should only be performed if symptoms and MRI findings clearly match.
Surgical Options for Lumbar Disc Herniation
The goal of surgery is to remove the herniated fragment and decompress the nerve root.
Main procedures include:
- Microdiscectomy (The Gold Standard): This procedure is defined by its minimal access approach to the spine: using a small skin incision (typically 3–4 cm), the deep paraspinal muscles are retracted, not cut. To safely access the disc in the spinal canal, only a minimal opening is created in the posterior wall of the canal (e.g., partial laminectomy or flavectomy), which preserves spinal stability. The removal of the fragment is then performed using an operating microscope for precise visualization and specialized instruments, such as disc forceps. Crucially, the surgeon always checks and addresses any existing bony compression (spinal stenosis) of the nerve root to ensure complete decompression. Due to its superior visualization, this reliable method is often the preferred approach for complex or migrated herniations. Furthermore, it facilitates fast recovery, with patients usually able to stand and walk the same day.
- Tubular Microdiscectomy (Minimally Invasive Access): A variation of microdiscectomy where the surgeon accesses the spine by inserting a series of progressively wider tubular dilators. This process dilates (stretches) the skin and muscle fibers to create a narrow surgical corridor, thus minimizing trauma. The final tubular retractor is then placed, and the procedure is performed with the help of a microscope for visualization.
- Endoscopic Discectomy (Percutaneous Technique): The most advanced minimal access method, using a tiny incision and a rigid endoscope (camera) for visualization. It is performed percutaneously (through the skin) and can be done either transforaminally (through the spine’s natural side opening) or interlaminarily (between the back bones).
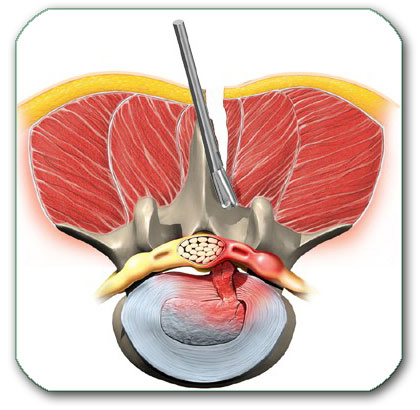
Image: Microdiscectomy — surgical introduction of instruments (forceps), with or without removal of a small portion of the posterior bony wall of the spinal canal, to access the canal and remove the disc fragment pressing on the nerve root.
The Surgical Decision: Pathology Over Technology
The choice between Microdiscectomy, Tubular, or Endoscopic techniques is not driven by technological trends, but strictly by the patient’s specific disc pathology (fragment migration, stenosis, recurrence) and anatomy. The experienced surgeon prioritizes the method that guarantees the safest and most complete removal of the fragment and additional nerve decompression if needed, recognizing that Microdiscectomy remains the most reliable baseline for complex cases. Crucially, the primary cause of persistent pain after disc surgery is not that one method is inherently less effective than another, but rather the result of inadequate decompression during the procedure, surgical complications, or failure to correctly identify and address all additional pain generators prior to the operation.
All these procedures are considered safe and effective for leg pain relief. In most cases, patients are discharged from the hospital the same day or the following morning. However:
- These procedures mainly address leg pain (sciatica), not chronic back pain.
- They do not treat the underlying degenerative process of the spine itself. This process may continue to progress and can cause other symptoms over time.
- They may have complications, especially if bone or ligament must be removed.
Minimally Invasive (Percutaneous) Disc Procedures
These procedures are performed through the skin (percutaneously) and are designed to reduce pressure within the disc without the need for a surgical incision. The goal is to reduce the volume of the inner disc material (nucleus pulposus) to achieve the retraction of the disc protrusion away from the nerve root.
This goal can be achieved by different methods, often grouped under the umbrella term of percutaneous disc decompression:
- Mechanical Reduction (Percutaneous Discectomy): Uses specialized mechanical instruments (nucleotomes) to remove a portion of the nucleus pulposus.
- Thermal/Radiofrequency Ablation (Nucleoplasty): Uses heat, radiofrequency energy, or laser to evaporate or shrink the volume of the nucleus pulposus.
Crucial Indication: These methods are effective exclusively for contained disc protrusions, where the posterior longitudinal ligament is intact.
Clinical Status: Due to the risk of complications and often lower long-term efficacy compared to modern micro- and endoscopic discectomies, these procedures are increasingly less recommended as a routine method in most major neurosurgical and pain management protocols.
Potential Risks and Complications of Surgery
Even in experienced hands, spine surgery carries risks:
- Infection, bleeding, or cerebrospinal fluid leakage
- Nerve root injury (rare but possible)
- Recurrence of herniation (in up to 10–15% of cases)
- A new herniation can occur at another level, since surgery does not stop the degenerative process.
- Chronic pain continues to persist if the wrong pain generator was targeted
- Postoperative extensive hematoma or seroma — early radicular pain or cauda equina–type symptoms with new neurological deficits require urgent evaluation. MRI helps to determine whether a compressive fluid collection is present and to characterize its nature — for example, blood, cerebrospinal fluid (CSF), or pus.
Spinal instability: Removing too much bone or ligament can destabilize the spine. This may lead to recurrent pain and, in some cases, the need for fusion surgery (instrumentation with screws and rods).
Chronic Pain After Lumbar Disc Surgery
Surgery for lumbar disc herniation often provides quick and significant relief of acute leg pain (sciatica). However, up to one in four patients may continue to experience some degree of pain after surgery, most commonly in the lower back.
In the majority of cases, this residual back pain is not directly caused by the disc herniation or the surgery itself. Often, an additional pain generator was already present before the operation, such as facet joint syndrome, ligament inflammation, myofascial pain, or muscle-related conditions. If these contributing factors were not recognized and treated beforehand, they may continue to cause pain after the disc is removed. Visit our page to read about causes, diagnosis and treatment of Low back pain.
The best approach is to identify such additional sources of pain before surgery, because their proper management may even help avoid surgery, or at least allow combined treatment (for example, interventional procedures performed during the same anesthesia session as the disc removal). After surgery, persistent pain generators should still be detected and treated.
Another well-known entity is Failed Back Surgery Syndrome (FBSS), where pain persists despite technically successful disc removal. Common causes include:
- Scar tissue forming around the nerve root
- Persistent nerve sensitization after long-standing compression
- Misdiagnosis — the disc was not the true source of pain
- Spinal instability introduced or unmasked during surgery
Because of these possibilities, every surgical decision must be carefully weighed, balancing the expected relief against the risk of persistent or new pain.
More about chronic pain after lumbar discectomy.
Prognosis and Recovery
- With conservative management, most patients improve within weeks to months.
- Surgery, when indicated, provides faster relief of sciatica, but long-term results (after 1–2 years) are often similar to conservative treatment.
- Chronic pain or recurrent symptoms are possible, especially if the diagnosis was not precise.
Lumbar disc surgery and spondylolisthesis (listhesis).
Spondylolisthesis (listhesis) is the forward or backward slipping of one vertebra in relation to the one below it, most often occurring in the lumbar spine (L4-L5 and L5-S1 levels). In patients with lumbar disc herniation, listhesis is most often degenerative, though isthmic, traumatic, and pathological forms also exist.
Listhesis is typically graded I–IV, based on the percentage of vertebral body slippage seen on the lateral (profile) view:
Grade I: <25% of the vertebral body width
Grade II: 25–50%
Grade III: 50–75%
Grade IV: >75% displacement — the most severe form.
When a grade I slip coexists with a herniated disc, stabilization is not always required—especially if a limited discectomy is planned without substantial facet resection and dynamic imaging does not show abnormal vertebral movement. Surgeons more often choose stabilization when dynamic flexion–extension films show increased translation/angulation and when facet blocks suggest the facet joint is a pain generator. Conversely, some centers fuse routinely with discectomy—even without clear indications—particularly when performing interbody fusion (e.g., PLIF/TLIF/ALIF); note these are fusion techniques (not true “disc replacement,” which is Total Disc Replacement-TDR). In brief, stabilization surgery means decompression as needed plus interbody fusion with cage and bone graft and pedicle-screw instrumentation to immobilize the segment until bony fusion occurs. The decision should balance symptom relief, proven instability, and the added risks of fusion versus a more limited decompression/discectomy.
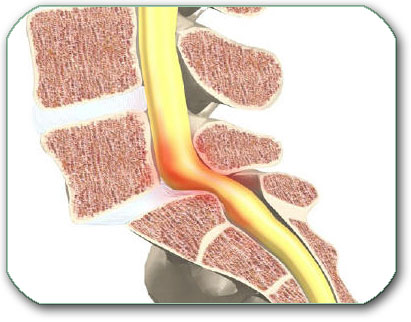
Image: The figure shows the most common type of instability, characterized by forward slippage of the last lumbar vertebra (spondylolisthesis). If it causes symptoms, stabilization surgery is indicated, as illustrated in the next image.
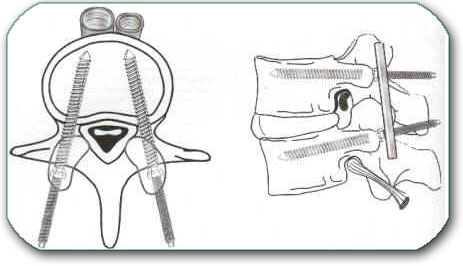
Image: Lumbar spinal fusion with pedicle screws and connecting rods. This procedure prevents further vertebral slippage and, when possible, allows the vertebrae to be realigned into a more normal position.
Interbody Fusion With Lumbar Disc Surgery
Interbody fusion is a type of spine surgery in which the diseased disc is removed and the space between two vertebrae is filled with a cage or bone graft, so that the bones can grow together (fuse) and stop moving at that level. Interbody fusion (e.g., PLIF/TLIF/ALIF) is indicated when discectomy is performed in the setting of proven segmental instability—most commonly degenerative spondylolisthesis—or when instability is demonstrated by dynamic flexion–extension radiographs (abnormal translation/angulation), adjunct MRI/CT signs (e.g., facet effusion), or intraoperative assessment, even in the absence of overt listhesis. In a stable, single-level disc herniation without evidence of instability, fusion is generally not required.
In some hospitals, lumbar spinal fusion is performed more frequently than in others, so equally qualified specialists may offer different recommendations depending on institutional practice patterns and individual clinical findings.
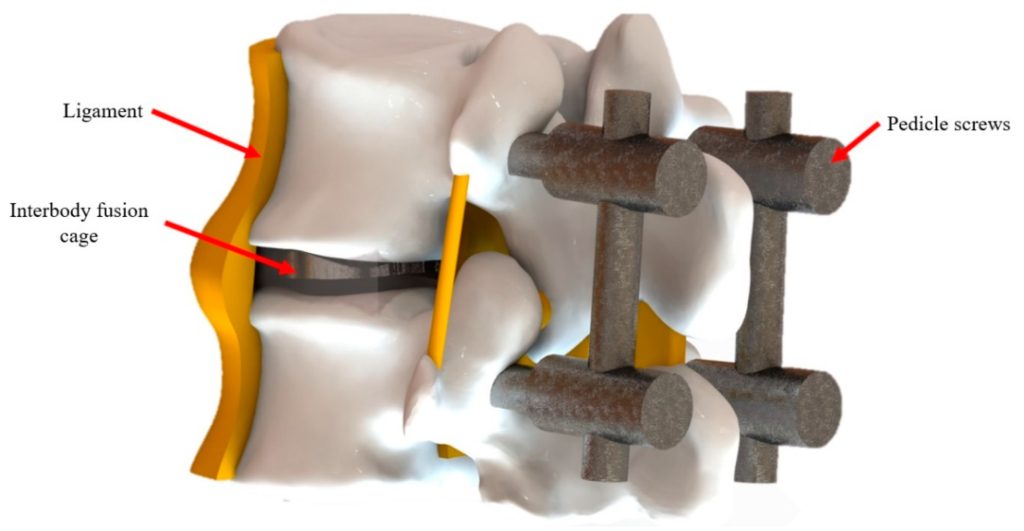
Image: Interbody fusion with cage placement and posterior screws for spinal stabilization
The Role of Second Opinion and Online Consultation
A second opinion can help prevent unnecessary surgery — or confirm that surgery is truly needed if you have doubts. Online consultations allow patients to:
- Clarify whether the disc is the true source of pain
- Learn if conservative treatment is still reasonable
- Understand surgical risks and alternatives
- Plan long-term pain management strategies
Online consultation is already widely used in the developed world, and that is why it has many synonyms such as video consultation, virtual consultation, teleconsultation, telehealth consultation, telemedicine consultation, remote consultation, online doctor visit, virtual doctor visit, online doctor appointment, online medical advice, ask a doctor online, doctor chat online, video call with a doctor, and online second opinion.
FAQ — Lumbar Disc Herniation & Sciatica
What is a lumbar disc herniation?
A lumbar disc herniation occurs when part of an intervertebral disc in the lower back moves beyond its normal boundary and may irritate or compress a nearby nerve root. Patients often call this a herniated disc, slipped disc, disc protrusion, disc extrusion, or disc prolapse. The clinical importance of a lumbar disc herniation depends on whether it matches the patient’s symptoms, neurological findings, and MRI appearance. Some herniated discs cause severe sciatica, while others are incidental MRI findings and do not require surgery. The key issue is not only whether a disc herniation exists, but whether it is truly responsible for the pain.
Can a lumbar disc herniation on MRI be unrelated to pain?
Yes. A lumbar disc herniation seen on MRI can be unrelated to pain, especially when the disc finding does not match the patient’s pain pattern, neurological examination, or affected nerve root. Many people have disc bulges, protrusions, extrusions, or degenerative disc changes on MRI without symptoms. At the same time, low back pain or sciatica-like leg pain may come from spinal stenosis, facet joints, sacroiliac joints, piriformis syndrome, peripheral nerve entrapment, myofascial pain, or other pain generators. This is why treatment should not be based on the MRI report alone. The MRI must be interpreted together with the clinical picture.
How do doctors know if a lumbar herniated disc is the true pain generator?
Doctors determine whether a lumbar herniated disc is the true pain generator by comparing three things: symptoms, neurological findings, and MRI anatomy. The pain should follow the distribution of the compressed or irritated nerve root, such as L4, L5, or S1. The examination may show matching sensory change, reflex change, or weakness. MRI should then show a disc fragment touching, displacing, or compressing the same nerve root at the correct level and side. If the pain pattern and MRI do not match, the disc may not be the main cause. In that situation, other sources of sciatica-like pain should be considered before injections or surgery are chosen.
Is sciatica always caused by a herniated lumbar disc?
No. Sciatica describes pain radiating from the lower back or buttock into the leg, but it is a symptom, not a diagnosis. A herniated lumbar disc is one common cause of sciatica when it irritates or compresses a lumbar or sacral nerve root. However, similar pain can also come from lumbar spinal stenosis, facet joint disease, sacroiliac joint dysfunction, piriformis syndrome, deep gluteal nerve irritation, peripheral nerve entrapment, or myofascial trigger points. Some patients also have a disc herniation on MRI that is not responsible for the pain. Correct treatment depends on identifying the true pain generator, not only naming the symptom as sciatica.
Why can MRI of the lumbar spine be misleading in disc herniation?
MRI of the lumbar spine can be misleading because it often shows abnormalities that are not the true cause of pain. Disc bulges, black discs, protrusions, annular tears, facet changes, and mild stenosis are common, especially with aging. A radiology report may describe these findings accurately, but that does not prove they are clinically important. The disc becomes meaningful only when it matches the patient’s symptoms, side of pain, nerve-root distribution, and neurological findings. Misinterpreting MRI findings can lead to unnecessary injections, procedures, or surgery. This is one reason why some patients continue to have pain after technically successful disc treatment: the wrong pain generator was targeted.
Can lumbar disc herniation heal without surgery?
Yes. Many lumbar disc herniations improve without surgery, especially when symptoms are mainly pain and there is no progressive neurological weakness or cauda equina syndrome. Disc inflammation often decreases over time, nerve irritation may settle, and some extruded or sequestrated fragments can shrink or resorb spontaneously. Conservative treatment may include medication, activity modification, physical therapy, avoidance of prolonged sitting or aggravating movements, and selected epidural steroid injections. Improvement usually occurs over weeks to months. Non-surgical treatment is most reasonable when pain is improving, neurological function is stable, and MRI findings match a condition that can be safely observed. Surgery is reserved for selected cases where waiting is unsafe or ineffective.
How long should conservative treatment be tried for sciatica and a proven lumbar disc herniation?
In many patients with sciatica and a proven lumbar disc herniation, conservative treatment is usually tried for about 6 to 12 weeks, provided there is no progressive motor weakness, cauda equina syndrome, or severe uncontrolled pain requiring earlier action. This period allows nerve inflammation to decrease and the disc fragment to stabilize or shrink. Conservative treatment should not mean passive waiting only. It should include adequate pain control, anti-inflammatory treatment when appropriate, neuropathic pain medication if needed, activity modification, and rehabilitation adapted to symptoms. If disabling leg pain remains severe despite properly applied treatment, or if neurological weakness progresses, surgery becomes more reasonable.
When do you need surgery for a lumbar disc herniation?
Surgery for lumbar disc herniation is usually needed when the disc clearly compresses the matching nerve root and symptoms are severe, persistent, or neurologically dangerous. Absolute or strong indications include cauda equina syndrome, progressive motor weakness, or significant neurological deficit. Surgery is also considered when severe leg pain persists beyond an adequate period of conservative treatment and prevents normal sleep, walking, work, or daily function. Even then, surgery should be performed only when the clinical picture and MRI findings match. A visible disc herniation alone is not enough. The goal of surgery is to decompress the affected nerve root and relieve sciatica, not to treat every MRI abnormality.
When is conservative treatment no longer enough for lumbar disc herniation?
Conservative treatment may no longer be enough when lumbar disc herniation causes progressive weakness, severe persistent leg pain, worsening neurological signs, or loss of bladder or bowel control. It may also be insufficient when pain remains disabling after a properly applied treatment plan, usually over several weeks, and MRI confirms compression of the correct nerve root. The decision is not based only on time. Some patients improve slowly and can continue non-surgical care safely, while others need earlier surgery because nerve function is worsening. The key question is whether waiting is likely to improve symptoms without risking permanent nerve damage or prolonged disability.
What is the difference between pain and a neurological deficit in lumbar disc herniation?
Pain and neurological deficit are not the same. Pain means the nerve root is irritated and sending pain signals, often felt as sciatica, burning, electric pain, or stabbing pain down the leg. A neurological deficit means that nerve function is impaired. This may appear as numbness, loss of sensation, reduced reflexes, foot drop, difficulty walking on heels or toes, or true muscle weakness. Pain alone often improves with conservative treatment. Progressive weakness is more concerning because it may indicate ongoing nerve damage. Treatment decisions in lumbar disc herniation depend heavily on whether the patient has pain only, stable sensory symptoms, or worsening motor deficit.
What is cauda equina syndrome and why is it urgent?
Cauda equina syndrome is a rare but serious emergency that occurs when a large central lumbar disc herniation compresses the bundle of nerve roots at the lower end of the spinal canal. Symptoms may include severe back pain, pain in both legs, saddle numbness around the inner thighs or perineum, new bladder or bowel dysfunction, sexual dysfunction, or progressive leg weakness. This condition is urgent because delayed decompression can lead to permanent weakness, numbness, incontinence, or sexual dysfunction. Patients with suspected cauda equina syndrome need immediate medical evaluation and urgent MRI. Surgery is usually performed as soon as possible to relieve nerve-root compression.
Will surgery for a lumbar disc herniation cure back pain or mainly leg pain?
Surgery for lumbar disc herniation is most reliable for relieving leg pain caused by nerve-root compression, also called sciatica or radicular pain. It is less predictable for chronic low back pain. Many patients have both leg pain and back pain, but the disc fragment removed during microdiscectomy or endoscopic discectomy mainly decompresses the nerve root. If back pain comes from facet joints, disc degeneration, sacroiliac joints, muscle overload, instability, or central sensitization, it may persist after successful disc surgery. This is why preoperative evaluation must clarify whether the main complaint is true radicular leg pain or chronic mechanical low back pain with an incidental disc finding.
What surgical options exist for lumbar disc herniation?
The main surgical options for lumbar disc herniation are microdiscectomy, tubular microdiscectomy, and endoscopic discectomy. Microdiscectomy is a reliable standard method using a small incision, microscopic visualization, and direct decompression of the affected nerve root. Tubular microdiscectomy uses a narrow muscle-splitting corridor. Endoscopic discectomy uses an endoscope through a very small access route and may be transforaminal or interlaminar depending on anatomy and disc location. The best technique depends on fragment position, migration, stenosis, recurrence, anatomy, and surgeon experience. The goal is not to choose the newest technology, but the safest method that fully decompresses the correct nerve root.
When is fusion needed with lumbar disc herniation surgery?
Fusion is not routinely needed for a simple, stable, single-level lumbar disc herniation. Standard disc surgery usually removes the herniated fragment and decompresses the nerve root without stabilizing the spine. Fusion may be considered when there is proven segmental instability, significant spondylolisthesis, recurrent herniation with instability, severe degenerative collapse, deformity, or when enough bone and joint tissue must be removed that instability would be created. The decision should be based on clinical findings, dynamic flexion-extension X-rays, MRI or CT signs, and surgical anatomy. Fusion adds operative risk and should not be performed only because a herniated disc is present.
What are the risks and recurrence rates after lumbar disc herniation surgery?
Lumbar disc herniation surgery is commonly effective for properly selected patients, but it still carries risks. Possible complications include infection, bleeding, cerebrospinal fluid leak, nerve-root injury, postoperative hematoma, recurrent herniation, persistent numbness, or continued pain if another pain generator was missed. Recurrent disc herniation can occur at the operated level, often quoted in the range of several percent and sometimes higher depending on patient factors, disc anatomy, and activity. A new herniation can also occur at another level because surgery does not stop the underlying degenerative process. Careful selection, correct level diagnosis, and adequate decompression reduce the chance of poor outcome.
Why can pain persist after lumbar disc surgery?
Pain can persist after lumbar disc surgery for several reasons. The disc may not have been the true pain generator, or another source of pain may have existed before surgery, such as facet joint pain, sacroiliac pain, myofascial pain, spinal stenosis, instability, or peripheral nerve irritation. Pain may also continue because of long-standing nerve sensitization, scar tissue around the nerve root, recurrent disc herniation, incomplete decompression, or a new problem at another spinal level. Surgery is most effective when symptoms, neurological findings, and MRI clearly match. If pain persists after surgery, the next step is not simply repeating treatment, but reassessing all possible pain generators.
How do spondylosis and spinal stenosis differ from lumbar disc herniation?
Lumbar disc herniation usually involves a focal disc fragment irritating or compressing a nerve root, often causing acute or subacute sciatica down one leg. Spondylosis refers to degenerative changes of the spine, including disc degeneration, facet joint arthritis, osteophytes, and ligament thickening. Spinal stenosis means narrowing of the spinal canal or lateral recess, usually from degenerative bone and ligament overgrowth rather than a single soft disc fragment. Stenosis often causes neurogenic claudication: leg pain, numbness, or weakness that worsens with walking and improves with sitting or bending forward. Treatment differs because stenosis surgery requires canal decompression, not simply removal of a disc fragment.
Bulging disc, protrusion, extrusion, and sequestration — what do these lumbar MRI terms mean?
Bulging disc, protrusion, extrusion, and sequestration are MRI terms describing the shape and extent of disc displacement. A bulging disc is a broad extension of the disc and is often degenerative. A protrusion is a more focal herniation where the base is broader than the outward part. An extrusion means the herniated material extends farther, often with a narrower base. Sequestration means a disc fragment has separated from the parent disc. These terms do not automatically determine pain severity or need for surgery. A small protrusion may cause severe sciatica if it compresses the right nerve root, while a large sequestration may improve without surgery if symptoms are stable.
Can a small lumbar disc herniation cause severe sciatica?
Yes. A small lumbar disc herniation can cause severe sciatica if it irritates or compresses the right nerve root in a sensitive location, especially in the lateral recess, foramen, or far-lateral zone. Pain severity depends not only on disc size, but also on inflammation, nerve-root contact, canal anatomy, individual sensitivity, and whether the fragment affects the clinically relevant nerve. Conversely, a large herniation may cause surprisingly mild symptoms if it does not significantly irritate a nerve root or if the fragment migrates away from the nerve. This is why MRI size alone should not determine treatment. Clinical correlation is essential.
Can I get an online second opinion for lumbar disc herniation surgery?
Yes. An online second opinion can help clarify whether lumbar disc herniation surgery is truly indicated, whether conservative treatment is still reasonable, and whether the MRI finding matches the symptoms. This is especially useful when surgery has been recommended, pain persists despite treatment, MRI shows several abnormal levels, or previous surgery did not help. A review can assess whether the disc is the likely pain generator, whether symptoms suggest nerve-root compression, whether there are urgent signs, and whether microdiscectomy, endoscopic discectomy, fusion, injections, rehabilitation, or continued observation is most appropriate. The most useful documents include MRI images, radiology reports, symptom description, neurological findings, and prior treatment history.
Artificial intelligence can also support the process by analyzing complex data, but clinical expertise remains essential.
Additional Resources/Information Regarding Lumbar Disc Herniation
Treatment for Lumbar Disc Herniation
Indications for Surgical Treatment of Disc Herniation
Lumbar Disc Herniation – Detailed Description
Read More about Lumbar Disc Herniation