Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Neurosurgeon and Pain Specialist
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
August 08, 2026
Who Should Read This Page
This page is intended for patients who have pain that increases during sitting and have already tried adjusting their chair, posture, or daily habits — but without clear or lasting improvement. In many cases, pain appears after a period of sitting, worsens in specific positions or environments, or improves when standing or changing position, yet the exact reason for this pattern remains unclear.
The main problem is that sitting is often treated as a general cause of pain, while in reality it acts as a specific mechanical load on particular anatomical structures. As a result, patients frequently try different chairs, cushions, or ergonomic adjustments without success — because the underlying mechanism has not been clearly defined. Without identifying which structure is involved and what process is occurring within it, it is not possible to determine what needs to be changed.
If you are trying to understand why sitting increases your pain despite making adjustments, which chair features may need to be changed, and how these changes should be tested in a precise, mechanism-based way, this page provides a structured explanation of those principles.
Choosing or Adapting a Chair — Quick Summary (Read This First)
- Sitting is not the cause of pain, but a mechanical factor that modifies load. Pain depends on the structure involved and the process occurring within it.
- The same chair can relieve pain in one situation and worsen it in another. This depends on load distribution, body position, and duration of sitting.
- Choosing a chair without understanding the pain mechanism leads to trial-and-error. This is why many patients change chairs without improvement.
- The key step is identifying what actually hurts. The structure and the mechanism determine how sitting must be modified.
- Chair adjustment is always individual. Even patients with the same diagnosis may require completely different sitting strategies.
- Individual chair features must be evaluated separately. Seat firmness, depth, angle, back support, armrests, and pressure-relief designs may help one pain mechanism while worsening another.
- The goal is not comfort, but reduction of load on the pain-generating structure.
- In many cases, the existing chair cannot be sufficiently adapted. Structural limitations may require replacing the chair.
- Short testing is unreliable. A chair must be evaluated under real-life conditions and over time.
- Chair selection is only one part of treatment. Pain persists due to underlying processes and contributing factors that must also be addressed.
- There is no “best chair” — only the right one for your specific mechanism of pain.
Contents
- Who Should Read
- Quick Summary
- Why Sitting Hurts
- Same Chair, Different Pain
- What Actually Hurts
- Why It’s Individual
- Adapting Sitting
- Only Part of Treatment
- Chair Adjustment
- Chair Features Based on Pain Causes
- When Replacement Is Needed
- Choosing the Right Chair
- How to Test
- Key Elements in Chair Testing
- No Best Chair
- Second Opinion
- FAQ
Why Sitting Causes Pain — But Not in the Same Way for Every Patient
Sitting is one of the most common factors that aggravate pain, but it is not the cause by itself. Pain develops because sitting increases mechanical load on specific anatomical structures and interacts with processes already present within those structures.
This is why the same sitting position can relieve pain in one patient and significantly worsen it in another. The difference does not come from posture alone, but from the interaction between:
- the structure involved
- the pathological process within that structure
- and the way sitting modifies load
Because of this, sitting must never be treated as a general cause of pain. It is a specific mechanical and functional factor, and its role can only be understood in the context of an individual patient.

Why the Same Chair Can Cause Pain in One Situation and Not in Another
In clinical practice, patients often describe a very characteristic pattern.
Pain may appear while sitting in an office chair, yet be absent when sitting in a sofa or armchair at home. It may occur during focused work at a computer, but not during more relaxed sitting. In many cases, pain is not present at the beginning, but develops only after prolonged exposure.
These differences are not accidental. They reflect changes in:
- load distribution across the pelvis and spine
- position of the body and angle of sitting
- pressure on specific regions such as the coccyx or perineum
- and the duration and continuity of load
For this reason, analysis must begin with a simple but essential question:
In which exact situation does pain appear, and under what conditions does it not?
The First Step — Identifying What Actually Hurts
Before any decision about a chair is made, the underlying mechanism of pain must be understood.
This requires answering three fundamental questions:
- Which anatomical structure is the source of pain?
- What process is occurring within that structure?
- How does sitting contribute to that process?
Without this step, changing a chair becomes a trial-and-error approach.
Pain during sitting may originate from multiple structures, including:
- intervertebral discs
- facet joints
- sacroiliac joints
- the coccyx
- peripheral nerves such as the pudendal nerve
- muscles, ligaments, fascia, or pelvic floor structures
- conditions such as Tarlov cyst, interstitial cystitis, and pain after surgical discectomy
In many patients, more than one structure is involved, and multiple mechanisms interact at the same time.
This is why identifying the structure alone is not sufficient. The mechanism of pain must also be understood, because it determines how load should be modified.
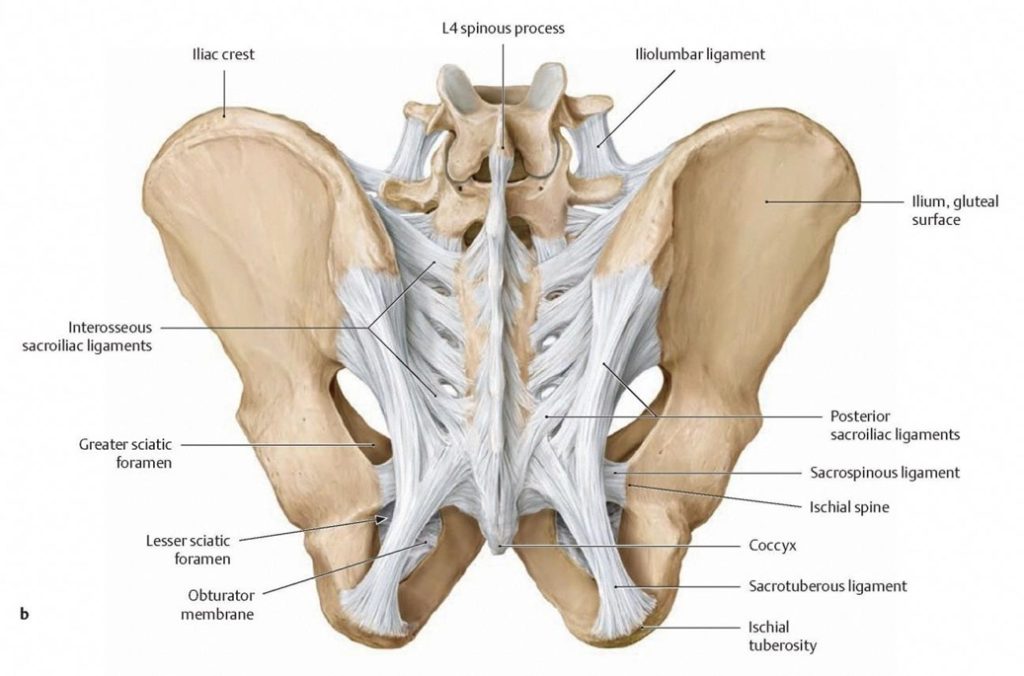
Image: These are some of the lower back and pelvic structures that may become overloaded or painful during prolonged sitting, including the facet and sacroiliac joints, coccyx, and associated ligaments.
Why Chair Adjustment Is Always Individual — Not Based on Diagnosis Alone
Even when two patients share the same diagnosis, their sitting strategy may be completely different.
This is because pain is not defined only by diagnosis, but by:
- the specific mechanism within the structure
- the pattern of load during sitting
- and the presence of contributing factors
For example, two patients with coccyx pain may require entirely different approaches depending on whether the problem is mechanical instability, inflammation, or neuropathic irritation.
For this reason, chair adjustment cannot be standardized. It must always be individualized and mechanism-based.
How Sitting Must Be Adapted for Different Pain Mechanisms
Once the mechanism is understood, sitting can be modified in a targeted way. The goal is not general comfort, but reduction of load on the structure responsible for pain.
In sacroiliac joint pain, sitting must emphasize symmetrical loading. Asymmetry in pelvic position often increases stress on the joint, and even small differences in weight distribution can sustain pain. In many cases, it is also necessary to reduce indirect load on the coccyx, which may influence how forces are transmitted through the pelvis.
In pudendal neuralgia, the key principle is reduction of pressure in the region where the nerve is irritated. This often requires redistribution of load away from the perineal area and, in some cases, additional attention to areas of trigger-induced sensitivity or allodynia, where even minimal pressure can provoke pain.
In coccyx pain, unloading the coccyx is often necessary, but this must be done carefully. Some patients instinctively lean forward to avoid pressure, but this may increase load on other structures and worsen symptoms. In these cases, not only the chair but also the entire working position must be adjusted.
In lumbar disc-related pain, seat depth, pelvic position, backrest angle, and lumbar support may influence how much flexion and sustained load is placed on the painful segment. However, excessive or rigid lumbar support may also worsen symptoms in patients who do not tolerate extension or local pressure.
In sciatica or nerve-root irritation, the sitting strategy must consider both spinal load and tension along the affected nerve. A position that reduces lower back discomfort may still increase leg pain if hip position, seat edge pressure, or prolonged immobility aggravates neural sensitivity.
In pelvic floor-related pain, including pain associated with bladder pain syndrome or interstitial cystitis in selected patients, the aim may be to reduce sustained pelvic tension and avoid concentrated pressure on the perineum or sitting bones. Excessively firm seating, poorly positioned cut-outs, or a rigid upright posture may worsen symptoms in some patients.
In symptomatic Tarlov cysts, prolonged sitting may aggravate sacral, perineal, coccygeal, or radicular pain by increasing pressure and tension around affected sacral nerve roots. Chair adaptation may therefore require redistribution of pressure away from the sacrum and perineum, while avoiding positions that increase nerve tension or worsen associated leg, pelvic, bladder, or bowel symptoms. However, the presence of a Tarlov cyst on MRI alone does not establish that it is the pain generator.
In persistent pain after lumbar spine surgery, chair selection must be based on the current pain generator rather than the previous operation alone. Residual disc or nerve-root irritation, scar-related sensitivity, sacroiliac loading, muscle dysfunction, or another mechanism may each require a different sitting strategy.
The number of possible adjustments is practically unlimited. Each patient requires a specific combination of modifications, and these changes are always part of a broader treatment strategy.
Chair Adjustment Is Only One Part of Treatment
It is important to understand that adjusting a chair is not a treatment in itself.
Pain persists because of processes occurring within a structure, and because of factors that maintain those processes. Sitting is often one of these factors, but rarely the only one.
Effective management requires:
- addressing the underlying pathological process
- identifying and modifying contributing factors
- and reducing mechanical load over time
Chair adjustment plays a role in this, but only as part of a comprehensive approach.
What Chair Adjustment Actually Means in Practice
In practice, adjusting a chair involves more than simply choosing a different model.
It includes modifying the elements of the chair itself, such as seat angle, backrest position, height, and arm support, if the chair allows these adjustments.
In addition, external modifications are often necessary. These may include specialized cushions for pressure relief, supports that change pelvic positioning, or elements that influence the position of the legs and load distribution.
However, even with these adjustments, there are many situations in which the existing chair cannot be adequately adapted.
Chair Features Based on the Cause of Sitting Pain
No single chair feature is beneficial for every patient. Each element must be evaluated according to the pain-generating structure, the mechanism of pain, and the way symptoms change during prolonged sitting.
These chair features may have different effects in patients with lower back pain, sciatica, sacroiliac joint pain, coccyx pain, pudendal neuralgia, pelvic pain, or persistent pain after spinal surgery. However, diagnosis alone is not sufficient to determine the appropriate chair. Patients with the same diagnosis may have different pain generators and may therefore require very different, or even opposite, sitting modifications.
Seat firmness and pressure distribution — A firmer seat may improve pelvic stability in some patients with mechanical lower back or sacroiliac pain, but it may increase localized pressure in coccyx pain, pudendal neuralgia, or pain over the ischial regions. A very soft seat may reduce direct pressure but can allow excessive pelvic sinking and worsen spinal or sacroiliac loading.
Seat depth — Greater seat depth may provide better thigh support, but an excessively deep seat can push the patient forward and reduce effective back support. A shorter seat may help smaller patients maintain contact with the backrest, but it can concentrate pressure beneath the thighs and sitting bones.
Seat angle and pelvic position — A slight forward tilt may help some patients with lumbar or hip-related pain, while increasing load on the perineum or allowing the pelvis to slide forward. A backward tilt may unload the lumbar spine in some cases but increase pressure on the coccyx.
Backrest and lumbar support — Lumbar support may reduce strain in some patients with lower back pain, but excessive or fixed support can worsen symptoms when extension, local pressure, or a rigid posture is poorly tolerated. The backrest should permit position changes rather than impose one supposedly ideal posture.
Armrests and chair height — Properly positioned armrests may reduce trunk and shoulder load and make changing position easier. Armrests that are too high or too low can create asymmetry, while an unsuitable chair height may increase pressure beneath the thighs or prevent stable foot support.
Pressure-relief cushions and cut-outs — Coccyx cut-outs may help when direct coccygeal pressure is the main trigger, while perineal relief channels may help selected patients with pudendal neuralgia or pelvic pain. However, an unsuitable cut-out can concentrate pressure on surrounding tissues, the ischial regions, thighs, or sacroiliac area and may worsen symptoms.
Adjustability — Adjustable seat height, depth, angle, lumbar support, and armrests allow the chair to be adapted to different pain mechanisms. This is often more important than the chair brand itself.
Return or trial period — A chair that feels comfortable for several minutes may still provoke symptoms after prolonged sitting. Testing should therefore reproduce the patient’s usual activity and the duration that normally triggers pain.
These examples are not fixed recommendations for particular diagnoses. Their purpose is to show why the painful structure and the effect of load must be identified before a chair is selected.
When the Chair Cannot Be Adapted — and Must Be Replaced
In a significant number of cases, the current chair does not allow sufficient modification.
This may be due to its design, its materials, or limitations in how load is distributed across the sitting surface. In such situations, replacing the chair becomes necessary.
Some manufacturers design chairs that provide a degree of general unloading through their shape and materials, but even then, the choice cannot be based on general recommendations.
The final selection must always be individual, based on how that specific chair interacts with the patient’s condition.
How to Choose the Right Chair — A Medical Approach
Choosing a chair should not be reduced to ergonomic features or marketing descriptions.
It requires a structured approach in which the patient understands:
- which types of chairs may be appropriate
- how their pain is triggered
- and how to evaluate whether a chair actually improves their condition
A physician plays an important role in this process by defining the criteria for selection and explaining what needs to be tested.
How to Test a Chair Properly (This Is Where Most Patients Make a Mistake)
A chair cannot be evaluated during a short trial. This is one of the most common reasons why patients make incorrect decisions.
In some cases, pain appears immediately on an unsuitable chair. However, much more often it develops only after prolonged sitting, sometimes after one or two hours. This difference is frequently overlooked.
Because of this, testing must be done under real-life conditions, not in a brief or relaxed setting.
Another common mistake is testing without a reference point. Comparing a new chair with one that reliably provokes your pain makes differences much easier to recognize.
Finally, many patients test chairs in positions that do not reflect how they actually sit. Pain is not determined only by the chair, but by the interaction between chair, posture, and activity.
This is why a structured approach to testing is necessary — not just trying a chair, but understanding how it behaves under the conditions that trigger your pain.
Key Elements of Chair Testing for Sitting Pain
Testing a chair must follow a structured approach, otherwise it gives false conclusions and leads to the wrong choice.
First, you must go to a place where chairs are clinically relevant for testing — meaning chairs that already reduce load through their shape and materials. Testing poor-quality chairs does not provide useful information, because they do not change the load in any meaningful way.
Second, you must bring yourself into a state where sitting can provoke your pain. If you test chairs while pain is absent, the result is unreliable. This usually means arriving after an activity that normally triggers your symptoms, such as desk work, driving, or prolonged sitting.
Third, you need both a clearly inadequate chair and a potentially adequate chair. The inadequate chair is used to reproduce your pain pattern, while the better chair is used for comparison. Without this contrast, testing becomes subjective and misleading.
Fourth, chairs must be compared under the same conditions — same position, same activity, and sufficient time. A chair that feels better at the beginning may behave the same as a poor chair after longer sitting. What matters is how it affects pain over time.
Fifth, testing must be performed in the position that provokes your pain the most. Avoiding that position gives a false sense of improvement. The most important test condition is not comfort, but reproducibility of symptoms.
Finally, the goal is not to find a chair that feels comfortable immediately, but one that changes the mechanism of pain — delays it, reduces it, or alters its pattern in a meaningful way.
Only when these elements are respected can chair testing lead to a correct and individualized decision.
Why There Is No “Best Chair” — Only the Right One for Your Mechanism
There is no universal solution.
A chair that is effective for one patient may be completely ineffective for another, even when the diagnosis appears similar.
The goal is not to find a more comfortable chair, but to understand the mechanism of pain and adapt sitting in a way that reduces the load sustaining that mechanism.
Only when this principle is respected can chair selection and adjustment become clinically meaningful.
Choosing the Right Chair — Second Opinion (How to Find What Actually Works for Your Pain)
Many patients try different chairs, cushions, or posture adjustments without improvement.
In most cases, the problem is not the chair itself, but how it interacts with the structure causing pain and the mechanism involved.
The same chair can relieve symptoms in one patient and significantly worsen them in another.
This depends on load distribution, body position, and the specific process within the affected structure.
A medical second opinion focuses on identifying the true pain generator and how sitting load affects it.
The goal is to define which type of chair, position, and modifications are appropriate in your specific case.
In most cases, this analysis is part of a broader evaluation of your pain condition.
However, when sitting is a major trigger, a more detailed and structured analysis of chair selection and sitting mechanics may be required.
- ✔ Describe when pain appears and which chairs or positions make it worse or better
- ✔ Send available reports (MRI, CT, previous diagnoses), but emphasis is on how pain behaves during sitting
- ✔ You will receive a reply within 24 hours explaining whether consultation is appropriate
- ✔ During consultation, we analyze how different chairs and positions affect load and symptoms
- ✔ You receive clear guidance on which type of chair and adjustments are likely to reduce your pain
Consultation fees typically range from $180–250 depending on case complexity.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Frequently Asked Questions About Choosing a Chair for Sitting Pain
Why doesn’t changing a chair automatically reduce pain?
Changing a chair does not automatically reduce pain because the chair is only one part of the mechanical environment. Pain during sitting depends on which anatomical structure is involved, what process is occurring inside that structure, and how sitting modifies load. A chair may feel more comfortable at first but still fail to unload the true pain generator. For example, a softer seat may reduce pressure on the coccyx but increase pelvic instability or perineal pressure in another patient. This is why chair selection should not begin with the chair itself, but with identifying what actually hurts: disc, facet joint, sacroiliac joint, coccyx, pudendal nerve, muscles, ligaments, fascia, or pelvic floor structures.
Why can the same chair cause pain in one situation and not in another?
The same chair can cause pain in one situation and not in another because pain depends on load distribution, body position, activity, and duration of sitting. A chair may be tolerated during relaxed sitting at home but provoke pain during focused computer work, where posture becomes fixed and movement is reduced. Pain may also be absent initially and appear only after prolonged exposure. This pattern reflects how sitting interacts with the painful structure over time. The important question is not whether a chair is “good” or “bad” in general, but under which exact conditions pain appears. Chair analysis must therefore include the situation, posture, duration, pressure points, and the structure being loaded.
Why is sitting not the same mechanical load for every patient?
Sitting is not the same mechanical load for every patient because each person has different anatomy, pain mechanisms, posture, body proportions, pelvic structure, tissue sensitivity, and contributing factors. In one patient, sitting may increase pressure on the intervertebral disc. In another, it may overload the sacroiliac joint, compress the coccyx, irritate the pudendal nerve, or increase pelvic floor tension. Even the same diagnosis may behave differently depending on whether the dominant mechanism is inflammation, instability, nerve sensitization, muscle spasm, or mechanical compression. For this reason, chair adjustment cannot be standardized. It must be based on how that patient’s specific pain-generating structure responds to sitting load.
Why must the pain-generating structure be identified before choosing a chair?
The pain-generating structure must be identified before choosing a chair because different structures require different unloading strategies. A chair that reduces pressure on the coccyx may not help sacroiliac joint pain. A position that helps pudendal neuralgia by reducing perineal pressure may increase lumbar disc loading. A chair that feels comfortable may still fail if the real source is the pelvic floor, fascia, ligament attachments, or a peripheral nerve. The first step is therefore to answer three questions: which anatomical structure hurts, what process is occurring within it, and how sitting contributes to that process. Without this, chair choice becomes trial-and-error rather than medical reasoning.
Which anatomical structures can become painful during sitting?
Several anatomical structures can become painful during sitting. Intervertebral discs may be affected by flexed posture and increased internal pressure. Facet joints may become painful when spinal curvature and load distribution change. Sacroiliac joints may react to asymmetrical pelvic loading. The coccyx can be directly compressed by the sitting surface. Peripheral nerves such as the pudendal nerve may be compressed or stretched in narrow pelvic spaces. Muscles, ligaments, fascia, and pelvic floor structures may also become overloaded or tense. In some patients, sitting-related pain may interact with Tarlov cysts, interstitial cystitis, or pain after lumbar discectomy. The chair must therefore be chosen according to the structure involved.
Why is identifying the painful structure not enough without understanding the sitting pain mechanism?
Identifying the structure is not enough because the same structure can produce pain through different mechanisms. Coccyx pain, for example, may be caused by mechanical instability, inflammation, bursitis, neuropathic irritation, or a specific anatomical shape that changes how pressure is transmitted during sitting. These mechanisms do not require the same chair or posture. Sacroiliac pain may depend on asymmetry and pelvic load transfer, while pudendal neuralgia depends more on pressure around the nerve and perineal region. A correct chair strategy must therefore be mechanism-based. The goal is not to unload a region in a general way, but to reduce the specific load that sustains the painful process.
Why is chair adjustment always individual and not based on diagnosis alone?
Chair adjustment is always individual because the same diagnosis can involve different mechanisms. Two patients with coccyx pain may require completely different strategies if one has mechanical instability and another has neuropathic irritation or local inflammation. Two patients with pelvic pain may differ depending on whether the dominant issue is pudendal nerve pressure, pelvic floor tension, sacroiliac load, or fascial pain. Diagnosis gives only a general category. It does not explain how sitting modifies load in that particular patient. Chair adjustment must therefore consider the anatomical structure, the process within it, the patient’s posture, the duration of sitting, pressure distribution, and contributing factors that maintain pain.
How must sitting be adapted differently for sacroiliac joint pain?
In sacroiliac joint pain, sitting must usually emphasize symmetrical pelvic loading. Even small asymmetries in weight distribution can increase stress on the sacroiliac joint and maintain pain. This is different from disc-related pain, where flexion and disc pressure may be more important, and different from pudendal neuralgia, where perineal pressure is the main concern. In sacroiliac pain, chair height, seat angle, pelvic position, and support may all influence how forces pass from the spine into the pelvis. It may also be necessary to reduce indirect loading through the coccyx because coccygeal pressure can alter pelvic load transfer. The aim is stable, balanced support rather than simply softer sitting.
How does pudendal neuralgia require a different sitting strategy and pressure redistribution?
Pudendal neuralgia requires a sitting strategy focused on reducing pressure where the pudendal nerve is irritated. The nerve passes through narrow pelvic regions and can be compressed or stretched during sitting. This is why patients often report perineal or genital burning, sharp pain, or electric pain that worsens while sitting and improves when standing or sitting on a toilet seat. A standard ergonomic chair may not help if it does not redistribute pressure away from the perineal region. In some patients, even minimal pressure can provoke symptoms because of allodynia or trigger-induced sensitivity. The chair must therefore reduce nerve load, not simply support the back.
Why does coccyx pain require individualized chair adaptation?
Coccyx pain requires individualized chair adaptation because the coccyx is directly exposed to pressure during sitting, but the mechanism differs between patients. Some patients need direct unloading of the coccyx. Others instinctively lean forward to avoid pressure, but this may increase load on the lumbar spine, sacroiliac joints, or pelvic floor. Coccyx pain may be mechanical, inflammatory, unstable, or neuropathic. It may also depend on whether the coccyx is straight, curved forward, or mobile between segments. For this reason, a cushion or cut-out seat is not automatically the solution. The entire working position, pelvic angle, pressure distribution, and duration of sitting must be adapted to the specific mechanism.
How does a symptomatic Tarlov cyst affect sitting and chair selection?
In symptomatic Tarlov cysts, prolonged sitting may aggravate sacral, perineal, coccygeal, or radicular pain by increasing pressure and tension around the affected sacral nerve roots. Chair adaptation may therefore require redistribution of pressure away from the sacrum and perineum, while avoiding positions that increase nerve tension or worsen associated leg, pelvic, bladder, or bowel symptoms. As with other nerve-related sitting pain, the goal is to reduce load on the irritated structure rather than to find a generally comfortable chair. However, the presence of a Tarlov cyst on MRI alone does not establish that it is the pain generator, so chair strategy should follow clinical correlation rather than the imaging finding alone.
How should sitting be adapted for lumbar disc-related pain?
In lumbar disc-related pain, sitting strategy depends on seat depth, pelvic position, backrest angle, and lumbar support, all of which influence how much flexion and sustained load is placed on the painful segment. A seat that allows an appropriate hip angle and adjustable lumbar contact may reduce sustained flexion and loading in some patients. However, excessive or rigid lumbar support may worsen symptoms in patients who do not tolerate extension, local pressure, or a fixed posture. The backrest should therefore permit position changes rather than enforce one supposedly ideal alignment.
How does sciatica or nerve-root irritation change the approach to chair selection?
In sciatica or nerve-root irritation, the sitting strategy must consider both spinal load and tension along the affected nerve, not only lower back comfort. A position that reduces lower back discomfort may still increase leg pain if hip position, pressure from the seat edge, or prolonged immobility aggravates neural sensitivity. For this reason, chair evaluation in sciatica should track leg symptoms separately from back pain, because the two may respond differently to the same adjustment. The appropriate chair is one that reduces the patient’s characteristic nerve-related symptoms over time, not simply one that feels comfortable initially.
How does chair selection differ for pelvic floor-related pain and bladder pain syndrome?
In pelvic floor-related pain, including pain associated with bladder pain syndrome or interstitial cystitis in selected patients, the aim may be to reduce sustained pelvic tension and avoid concentrated pressure on the perineum or sitting bones. Excessively firm seating, poorly positioned cut-outs, or a rigid upright posture may worsen symptoms in some patients. However, chair modification must remain secondary to identifying and treating the underlying bladder and pelvic floor mechanisms. Seating changes alone do not address the primary condition, but they may reduce one of the mechanical factors that aggravate symptoms.
How should chair selection be approached after lumbar spine surgery?
In persistent pain after lumbar spine surgery, chair selection must be based on the current pain generator rather than the previous operation alone. Residual disc or nerve-root irritation, scar-related sensitivity, sacroiliac loading, muscle dysfunction, or another mechanism may each require a different sitting strategy. Because postoperative pain can originate from several different structures, the same recommendation cannot be applied to all patients who have undergone spinal surgery. Chair adjustment should therefore follow the same structure-and-mechanism analysis used for patients who have not had surgery.
Can several pain mechanisms be active at the same time while sitting?
Yes. Several pain mechanisms can be active at the same time while sitting. A patient may have sacroiliac joint irritation together with pelvic floor tension, coccyx pressure combined with pudendal nerve sensitivity, or disc-related pain with muscular and fascial overload. In such cases, changing the chair may improve one mechanism but worsen another. This is one reason why patients often try many chairs without clear success. The analysis must identify the dominant pain generator, but also secondary factors that maintain symptoms. Chair selection then becomes part of a broader strategy: reduce mechanical load, address the underlying pathological process, and modify contributing factors that keep the pain active.
Why is chair adjustment only one part of pain treatment?
Chair adjustment is only one part of treatment because pain persists due to processes occurring inside a structure and the factors that maintain those processes. Sitting may aggravate the problem, but it is rarely the only cause. If the pain generator is inflamed, unstable, neuropathic, or sensitized, changing the chair may reduce load but will not fully treat the condition by itself. Effective management may also require medication, targeted procedures, physical therapy, pelvic floor treatment, lifestyle modification, or treatment of contributing factors. The chair helps only when it reduces mechanical stress on the correct structure. It should be viewed as part of a comprehensive pain strategy, not as a standalone cure.
What does chair adjustment for sitting pain actually mean in practice?
Chair adjustment means more than simply choosing another chair. It may include changing seat angle, seat height, backrest position, lumbar support, arm support, pelvic position, and the way the legs are supported. External modifications may also be needed, such as cushions that reduce pressure, supports that change pelvic alignment, or elements that modify load through the thighs and feet. The correct adjustment depends on the painful structure. Disc-related pain, sacroiliac joint pain, coccyx pain, pudendal neuralgia, and pelvic floor-related pain require different load strategies. In some cases, the existing chair cannot be modified enough because its shape, materials, or pressure distribution are structurally unsuitable.
When can a chair for sitting pain be adapted and when must it be replaced?
A chair can be adapted when its basic design allows meaningful changes in load distribution. If seat height, angle, backrest support, arm support, or external cushions can reduce pressure on the painful structure, adaptation may be enough. However, some chairs cannot be sufficiently modified because their seat shape, materials, depth, firmness, or pressure pattern continue to load the same painful region. In that situation, replacing the chair becomes necessary. The decision should not be based on whether the chair is expensive or labeled ergonomic. It should be based on how that specific chair interacts with the patient’s anatomy and pain mechanism during real-life sitting.
Why should a chair for sitting pain not be chosen based on ergonomic labels or marketing claims?
Chair selection should not be based only on ergonomic labels or marketing claims because those descriptions usually address general comfort, not a specific pain mechanism. A chair may be marketed as ergonomic, adjustable, or supportive, but still fail to unload the coccyx, sacroiliac joint, pudendal nerve, lumbar disc, or pelvic floor in a particular patient. The goal is not to buy the “best” chair in general, but to find a chair that reduces load on the structure responsible for pain. This requires medical reasoning: which structure hurts, what process is active, how sitting modifies load, and whether the chair changes that mechanism under real-life conditions.
Why is short chair testing unreliable for sitting pain?
Short chair testing is unreliable because many sitting-related pain patterns appear only after prolonged exposure. A chair may feel comfortable during the first few minutes but fail after one or two hours, when cumulative load, reduced movement, pressure concentration, muscle fatigue, or nerve sensitivity becomes relevant. Testing in a relaxed showroom position also may not reproduce the conditions that trigger pain during desk work, driving, or focused activity. This is why patients often buy a chair that felt good initially but later provides no real benefit. Chair testing must evaluate whether the chair changes the pain mechanism over time, not whether it feels pleasant at the beginning.
How should a chair for sitting pain be tested properly under real-life conditions?
A chair should be tested under conditions that reproduce the patient’s real pain pattern. If pain usually appears during computer work, the chair should be tested in that posture and activity. If pain appears after driving or prolonged sitting, the test should include enough time to provoke symptoms. The patient should compare a clearly inadequate chair with a potentially better one, under the same position, same activity, and similar duration. Testing while pain is absent may give a false result. The goal is not to find a chair that feels comfortable immediately, but one that delays pain, reduces intensity, changes the pain pattern, or meaningfully unloads the responsible structure.
What are the key elements of proper chair testing for sitting pain?
Proper chair testing requires several elements. First, the chair should be clinically relevant, meaning it actually changes load through its shape or materials. Second, the patient should test when sitting can provoke pain; otherwise the result is unreliable. Third, comparison is needed between an inadequate chair and a potentially useful chair. Fourth, both chairs should be tested under the same conditions: same posture, same activity, and enough time. Fifth, testing must include the position that usually provokes pain, rather than avoiding it. The most important result is not immediate comfort, but whether the chair changes the pain mechanism by delaying, reducing, or altering symptoms.
Why do many patients change chairs for sitting pain without improvement?
Many patients change chairs without improvement because they choose based on comfort, recommendations, or ergonomic labels rather than their specific pain mechanism. If the true pain generator is not identified, each new chair becomes another trial-and-error attempt. A chair may fail because it does not reduce pressure on the coccyx, does not correct pelvic asymmetry, does not unload the pudendal nerve, or does not change disc or muscle load during prolonged sitting. In other cases, chair adjustment helps only briefly because the underlying pathological process and contributing factors remain untreated. Chair selection works best when it follows medical analysis of the structure, mechanism, and load response.
Which chair features should be evaluated for sitting pain?
The main chair features to evaluate are seat firmness, pressure distribution, seat depth, seat angle, backrest and lumbar support, armrest position, chair height, adjustability, and the use of pressure-relief cushions or cut-outs. Each feature can change how load is distributed across the lumbar spine, pelvis, coccyx, perineum, thighs, and sitting bones.
However, no individual feature is universally beneficial. A firm seat may improve pelvic stability but worsen coccyx or perineal pressure, while a soft seat may reduce localized pressure but allow excessive pelvic sinking. Similarly, a cut-out may unload one painful area while transferring pressure to another. These features must therefore be tested according to the pain generator, pain mechanism, and the conditions in which symptoms normally appear.
Why is there no single “best chair” for sitting pain?
There is no single best chair for sitting pain because different pain mechanisms require different unloading strategies. A chair that helps coccyx pain may fail in pudendal neuralgia. A chair that improves lumbar support may not reduce sacroiliac asymmetry. A soft chair may reduce pressure but increase instability. A firm chair may support posture but aggravate perineal or tailbone pressure. Even within the same diagnosis, two patients may need different adjustments depending on anatomy, mechanism, and contributing factors. The right chair is therefore not the most expensive or most ergonomic model. It is the one that reduces load on the specific pain-generating structure in that individual patient.
How can medical analysis help identify the right chair and sitting strategy for sitting pain?
Medical analysis helps identify the right chair by first defining the pain generator and mechanism. The patient describes when pain appears, which chairs or positions worsen it, which positions improve it, and how long sitting is tolerated. MRI or other reports may help, but the emphasis is on pain behavior during sitting and load response. A specialist can then determine whether the main issue is disc pressure, sacroiliac loading, coccyx compression, pudendal nerve pressure, pelvic floor tension, muscle or fascia overload, or a mixed mechanism. The chair strategy is then chosen to reduce load on the relevant structure, while broader treatment addresses the process and contributing factors maintaining pain.