Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
March 08, 2026
Who This Parasagittal Meningioma Page Is For
This page is intended for patients in whom MRI or CT has revealed a parasagittal meningioma, a tumor arising from the meninges along the sagittal plane of the brain, typically adjacent to the superior sagittal sinus.
If surgery, stereotactic radiosurgery (such as Gamma Knife), radiotherapy, or long-term MRI monitoring has been proposed — or if specialists have offered different recommendations regarding the urgency or type of treatment — an individualized neurosurgical second opinion may help clarify the expected biological behavior of a parasagittal meningioma, the potential risk of seizures, progressive weakness, or neurological deterioration related to involvement of the motor cortex or superior sagittal sinus, the likelihood of tumor recurrence, and the safest balance between observation, surgery, and radiation therapy based on tumor size, location along the sagittal sinus, growth rate, surrounding brain edema, and overall neurological status.
When patients seek a second opinion for parasagittal meningioma
• MRI or CT shows a parasagittal meningioma and the best treatment strategy is unclear
• The tumor was discovered incidentally and opinions differ between MRI monitoring and surgery
• Progressive weakness, seizures, or neurological symptoms suggest compression of the motor cortex
• Surgery is recommended but risks, involvement of the superior sagittal sinus, or prognosis are uncertain
• Radiosurgery or radiotherapy is proposed but the role of surgery remains unclear
• Specialists recommend different strategies without clear agreement
If your situation involves uncertainty regarding diagnosis, urgency, or treatment strategy, you may request an individualized neurosurgical review here:
Request Second Opinion
Parasagittal Meningioma — Quick Summary (Read This First)
- Parasagittal meningioma is a tumor arising from the meninges (the brain’s protective membranes) along the midline of the brain, usually adjacent to the superior sagittal sinus (a large vein that drains blood from the brain). These membranes surround and protect the brain and spinal cord.
- Most parasagittal meningiomas grow outside the brain tissue. They compress the cerebral cortex and surrounding brain structures without directly invading brain tissue.
- Parasagittal meningiomas account for approximately 20–25% of intracranial meningiomas. They represent one of the most frequent meningioma locations.
- Many parasagittal meningiomas grow slowly and may remain stable for years. A substantial proportion of tumors discovered incidentally on MRI do not require immediate treatment.
- Symptoms depend mainly on the cortical brain region affected. Tumors near the motor cortex may cause progressive weakness or numbness in the opposite leg or arm, while seizures and headaches may occur due to cortical irritation.
- MRI with contrast is the most important diagnostic test. It shows tumor size, location along the sagittal sinus, surrounding brain edema, and the relationship to cortical veins and the superior sagittal sinus.
- Many incidentally discovered parasagittal meningiomas never require treatment. Approximately 60–80% of incidentally discovered meningiomas remain stable and can be safely monitored with periodic MRI without surgery or radiation. Treatment is usually considered only if the tumor shows growth, produces neurological symptoms, or causes significant brain compression. In those situations, smaller growing tumors may be treated with radiosurgery in selected cases, while larger tumors that produce significant mass effect are more often treated surgically.
- Surgery is the main treatment for symptomatic or growing parasagittal meningiomas. The surgical strategy depends on tumor size, involvement of the superior sagittal sinus, and proximity to motor cortex.
- Radiation therapy or stereotactic radiosurgery may be used in selected cases to control tumor growth. It is most commonly used for small tumors (usually up to about 2.5–3 cm in diameter) that demonstrate growth during MRI follow-up. It may also be used for residual or recurrent tumor after surgery.
- Treatment decisions depend mainly on tumor size, involvement of the superior sagittal sinus, growth rate, neurological symptoms, and surrounding brain edema. The safest strategy is usually individualized.
- Prognosis of parasagittal meningioma is often favorable when safe surgical removal is possible. Recurrence risk depends mainly on tumor grade and the extent of surgical removal.
- Most parasagittal meningiomas are benign WHO Grade I tumors. Approximately 80–85% of meningiomas belong to Grade I, while about 10–15% are atypical (WHO Grade II) and roughly 1–3% are malignant (WHO Grade III). Recurrence is more frequent in Grade II and Grade III tumors, and these patients more often require additional treatment such as postoperative radiotherapy and closer long-term MRI follow-up.
- Although many parasagittal meningiomas are benign, large tumors can still cause serious neurological problems due to mass effect on the brain or involvement of major venous structures.
Most readers benefit from reviewing this Quick Summary together with the sections on Symptoms of Parasagittal Meningioma, Diagnosis, Surgical Treatment, Radiation Therapy, and Treatment Decision-Making. Later sections provide more detailed explanations intended for patients seeking a deeper understanding before important treatment decisions are made.
Contents
- Who This Page
- Quick Summary
- Definition
- Tumor Classification
- Tumor Causes
- Tumor Location
- Multiple Tumors
- How They Affect
- Symptoms
- MRI Diagnosis
- When Monitored
- Symptom Relief
- Epilepsy
- Surgical Treatment
- Modern Technologies
- Extent of Removal
- Radiation Therapy
- Tumor Recurrence
- Treatment by Grade
- Long-Term Monitoring
- Treatment Summary
- Experimental Therapies
- Why Opinions Differ
- Overall Prognosis
- Request Second Opinion
- Life-Threatening Risk
- FAQ
What Is a Parasagittal Meningioma
A parasagittal meningioma is a tumor that arises from the dura mater—the tough, outer protective membrane of the brain—covering the parasagittal region, which refers to the area along the top midline of the head. These tumors develop near the falx cerebri (a fold of the dura that separates the two brain hemispheres) and the superior sagittal sinus, a major central vein that drains blood from the brain. Because they grow outside the brain tissue, they typically expand inward, gradually compressing the cerebral cortex (the brain’s surface) and affecting the functions controlled by that specific area.
Most meningiomas arise from specialized cells located within the arachnoid layer, often referred to as arachnoid cap cells. When genetic changes occur in these cells, they may begin to multiply abnormally and gradually form a tumor. Unlike tumors that originate inside the brain tissue, parasagittal meningiomas grow outside the brain, attached to the dura along the parasagittal brain surface near the superior sagittal sinus. As the tumor enlarges, it usually compresses the surrounding brain tissue without direct brain invasion. Because of this growth pattern, many parasagittal meningiomas remain well-defined masses that can often be surgically separated from the brain. However, when the tumor is adherent to or invades the wall of the superior sagittal sinus, the safety of complete removal becomes more limited.
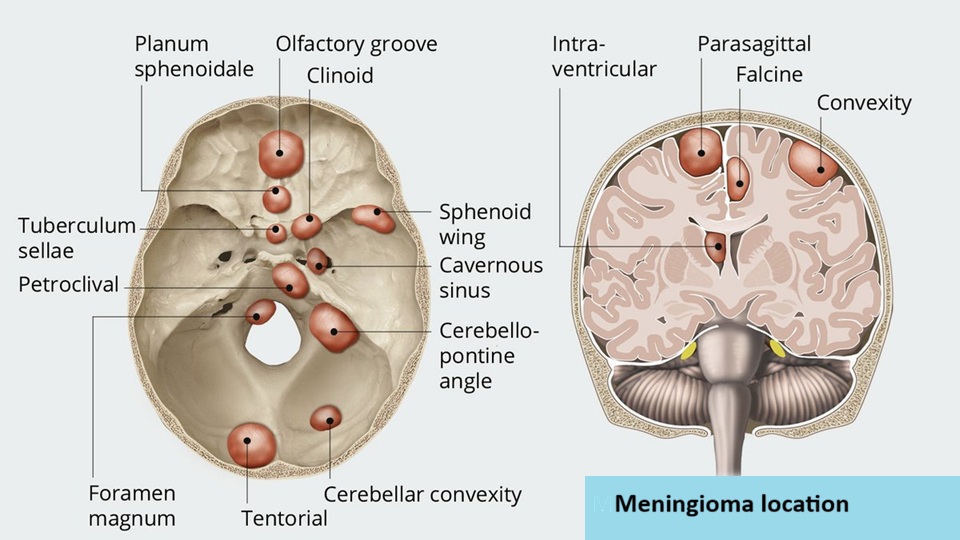
Image: Parasagittal and other meningioma locations.
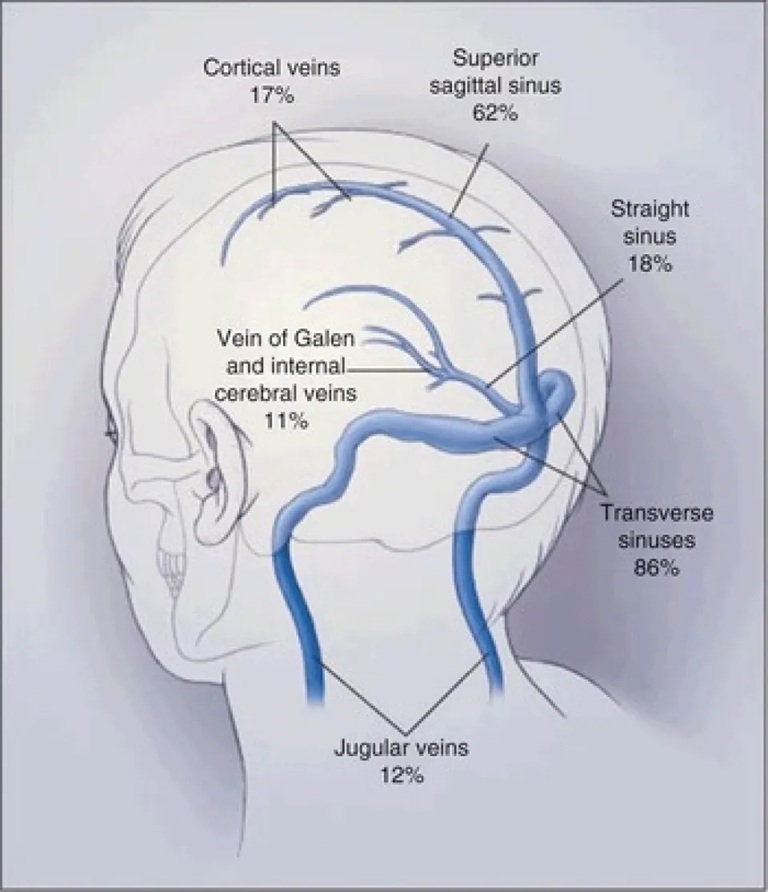
Image: The superior sagittal venous sinus at the midline of the head with its venous tributaries. Parasagittal tumors can occur anywhere along this sinus, either pressing against its walls, infiltrating them partially, or obstructing them completely. If the sinus becomes gradually obstructed, its role in draining blood from the brain is taken over by the venous tributaries, which must therefore be preserved during surgery.
Epidemiological studies show that meningiomas represent approximately 35–41% of all primary intracranial tumors in adults, making them the most common primary brain tumor. Parasagittal meningiomas account for approximately 20–25% of intracranial meningiomas. Small incidental meningiomas may be present in approximately 0.5–1% of the general population, based on autopsy and imaging studies. Most of them never cause symptoms or require treatment.
Meningiomas are also rare in children, representing less than 2% of all pediatric brain tumors. When they occur in younger patients, they are more frequently associated with genetic syndromes such as neurofibromatosis type 2 (NF2).
You can read more about other brain tumors on our Brain Tumors page.
Biological Classification of Parasagittal Meningioma
The biological behavior of parasagittal meningiomas is determined through histopathological analysis using the World Health Organization (WHO) classification.
Three main categories are recognized:
• WHO grade I — benign meningioma. This is the most common form, representing roughly 80–85% of meningiomas. These tumors typically grow slowly and often remain stable for long periods. When completely removed surgically, the chance of recurrence is relatively low.
• WHO grade II — atypical meningioma. Atypical meningiomas account for approximately 10–15% of cases in surgical series of meningiomas. These tumors show increased cellular activity and a higher likelihood of recurrence after surgery. After complete tumor removal, some patients may be managed with MRI follow-up rather than immediate radiation therapy.
• WHO grade III — malignant (anaplastic) meningioma. These tumors are rare, representing roughly 1–3% of cases in surgical series of meningiomas. They grow more aggressively, recur more frequently, and usually require combined treatment with surgery and radiation therapy.
Although histological grade is important, clinical outcome also depends strongly on the exact parasagittal location of the tumor, the degree of superior sagittal sinus involvement, and the possibility of complete but safe surgical removal.
Genetic and Biological Causes of Parasagittal Meningioma
Most parasagittal meningiomas arise from sporadic genetic mutations that occur during life rather than inherited genetic disorders. At the molecular level, tumor development usually results from two main biological mechanisms:
• inactivation of tumor suppressor genes, which normally prevent uncontrolled cell growth
• activation of oncogenic signaling pathways, which stimulate cell proliferation
The most frequently involved gene is NF2, located on chromosome 22. Loss of function of this gene disrupts normal cell growth control and allows tumor formation. Other molecular alterations identified in meningiomas include mutations involving genes such as TRAF7, AKT1, SMO, and KLF4, while additional less common alterations may involve genes such as PIK3CA or TERT.
These molecular differences partly explain why tumors in different anatomical regions may behave differently.
The only clearly established environmental risk factor is exposure to ionizing radiation, particularly during childhood.
Meningiomas occur approximately two to three times more frequently in women than in men, suggesting that hormonal influences may play a role in tumor development and growth.
Although most meningiomas arise sporadically, a small proportion occur in the context of inherited genetic syndromes. The best known example is neurofibromatosis type 2 (NF2), a hereditary condition caused by mutations of the NF2 gene on chromosome 22. Patients with NF2 frequently develop multiple meningiomas, a condition referred to as meningiomatosis, in which several tumors arise in different intracranial and spinal locations. Multiple meningiomas may also appear sporadically without a hereditary syndrome, but they are particularly characteristic of NF2. In addition, meningiomas may occur in association with other rare genetic disorders such as schwannomatosis or Cowden syndrome, although these situations are much less common. Overall, hereditary syndromes account for only a small minority of meningioma cases.
Location of Parasagittal Meningiomas
Parasagittal meningiomas arise along the midline surface of the brain near the superior sagittal sinus. They develop from the dura covering the parasagittal cerebral convexity rather than from deep skull base structures.
They account for approximately 20–25% of intracranial meningiomas, making them one of the most common meningioma locations.
The exact cortical region involved is extremely important because it determines both the symptoms and the complexity of surgical treatment.
Parasagittal meningiomas may arise over different functional parts of the cerebral hemispheres. Tumors in the frontal parasagittal region may cause headaches, behavioral change, or weakness, whereas tumors near the paracentral lobule (in the middle third of the sinus) may produce weakness or sensory symptoms affecting the opposite leg, gait difficulty, or seizures. More posterior parasagittal tumors may produce sensory symptoms, spatial difficulties, or focal seizures depending on the dominant or nondominant hemisphere involved.
An additional factor of major importance is the tumor’s relationship to the superior sagittal sinus and bridging veins, because this often determines whether complete removal can be achieved safely.
Multiple Meningiomas (Meningiomatosis)
Most patients develop a single meningioma, but approximately 5–10% of patients present with multiple tumors. This condition is referred to as multiple meningiomas or meningiomatosis.
Multiple meningiomas may occur sporadically, but they are particularly associated with neurofibromatosis type 2, in which patients may develop numerous tumors along the meninges.
Management of multiple meningiomas is individualized. In many cases only the symptomatic or growing tumors are treated, while the remaining lesions are monitored with periodic imaging.
How Parasagittal Meningiomas Grow and Affect the Brain
Parasagittal meningiomas usually grow slowly over many years. Because they arise outside the brain tissue, they primarily damage the brain through compression without direct invasion. As the tumor enlarges, it gradually presses on adjacent cortical brain structures. This pressure interferes with normal neuronal activity and may lead to neurological deficits.
Another important mechanism is peritumoral brain edema, a form of swelling in the surrounding brain tissue caused by leakage of fluid from nearby blood vessels. This swelling increases intracranial pressure and often worsens symptoms.
Together with the tumor itself, this edema can produce a mass effect, meaning that the expanding lesion compresses and displaces normal brain structures. Because the skull is a rigid, closed cavity with very limited space for expansion, increasing pressure may force parts of the brain to shift from their normal position. In severe cases, brain tissue can be pushed through natural openings within the skull, a condition known as brain herniation. Herniation represents a dangerous stage of mass effect in which displaced brain structures may compress vital centers in the brainstem responsible for consciousness, breathing, and circulation.
Large tumors may also compress nearby arteries or veins, disrupting normal blood circulation in the brain. In parasagittal meningiomas, this issue is especially important when the tumor compresses, invades, partially or completely occludes the superior sagittal sinus, because impaired venous drainage may contribute to edema, increased intracranial pressure, and secondary neurological deterioration.
Even though most parasagittal meningiomas do not invade brain tissue, prolonged compression may still cause permanent neurological damage if the tumor becomes very large.
Studies following patients with untreated meningiomas have shown that a substantial proportion of tumors remain stable for long periods. Approximately 30–35% of meningiomas show no measurable growth during long-term imaging follow-up. Among tumors that do grow, the increase in size is usually slow and gradual, often measured in millimeters per year rather than rapid expansion.
Symptoms of Parasagittal Meningioma
The symptoms caused by parasagittal meningiomas depend largely on their exact anatomical location, tumor size, surrounding edema, and the cortical region involved.
Parasagittal meningiomas often produce seizures because they irritate the surface of the brain.
Tumors located near the motor cortex and paracentral lobule (middle third of the sagittal sinus) may produce progressive weakness, clumsiness, or loss of fine motor control on the opposite side of the body, often with special prominence in the leg. Tumors over the sensory cortex may cause numbness, altered sensation, or sensory neglect. Frontal parasagittal tumors may lead to headaches, slowed thinking, reduced concentration, personality changes, or behavioral changes when significant edema affects the frontal lobes. More posterior parasagittal tumors may produce sensory symptoms, difficulties with spatial orientation, gait disturbance, or focal seizures depending on the dominant or nondominant hemisphere involved.
Headache is common, particularly in larger tumors associated with significant edema or raised intracranial pressure. Headache in patients with small meningiomas does not necessarily mean that the tumor is the cause. Many patients have common primary headache disorders such as tension-type headache, migraine, or cervicogenic headache, which are frequent in the general population and may occur independently of the tumor. For this reason, the type of headache should be carefully evaluated and defined before attributing the symptoms to the meningioma, and the presence of headache alone is usually not a sufficient reason to recommend immediate surgical removal of a small, otherwise asymptomatic tumor.
Some patients remain entirely asymptomatic, especially when the tumor is discovered incidentally on MRI or CT performed for unrelated reasons.
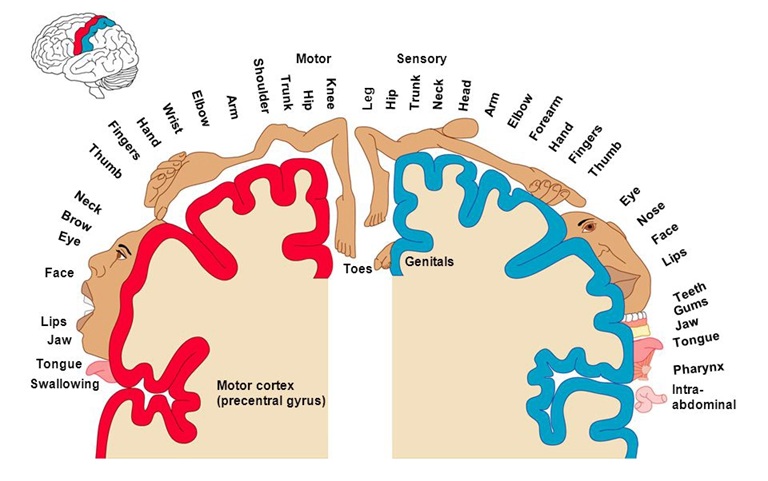
Image: Parasagittal location of sensory and motor centers for the opposite leg, and convexity presentations of other parts of the body. Due to this anatomical presentation of motor and sensory centers, parasagittal meningiomas located in the middle third of the sagittal sinus cause the most significant neurological deficits in the opposite leg.
Diagnosis of Parasagittal Meningioma
The most important diagnostic test is MRI of the brain with contrast.
During this examination, the patient lies inside the MRI scanner while magnetic fields generate highly detailed images of the brain. A contrast agent injected through a vein highlights tumor tissue.
MRI allows physicians to determine:
• tumor size
• precise location
• relationship to the parasagittal brain surface, superior sagittal sinus, and nearby vessels
• presence of surrounding brain edema
Parasagittal meningiomas typically appear as well-defined tumors located outside the brain tissue, attached to the dura along the parasagittal region, often accompanied by a characteristic imaging feature known as the dural tail.
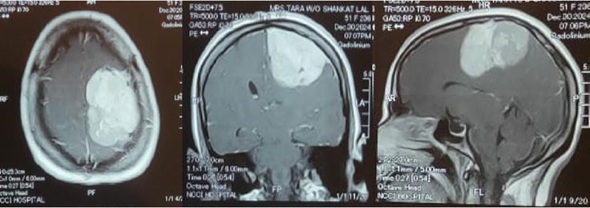
Image: Contrast-enhanced T1-weighted brain MRI showing a large, bright parasagittal meningioma in three projections.
The final diagnosis is confirmed through histopathological analysis after surgery or biopsy.
However, several other conditions may produce similar MRI findings and must be considered in the differential diagnosis.
These include:
• dural metastases, which may mimic meningiomas when metastatic cancer spreads to the meninges
• hemangiopericytoma (solitary fibrous tumor), a rare dural tumor that can appear very similar radiologically but behaves more aggressively
• lymphoma involving the dura
• other dural-based lesions that may resemble parasagittal meningioma on imaging
Because imaging findings may overlap, the final diagnosis is often confirmed by histopathological examination of the tumor after surgical removal or biopsy.
Although MRI is the main imaging method used to diagnose parasagittal meningiomas, other techniques may occasionally provide additional information. CT scans are particularly useful for evaluating changes in the skull bone, such as hyperostosis or calcification within the tumor.
Vascular imaging such as CT angiography, MR angiography, MR venography, or CT venography may be performed to assess the relationship of the tumor to the superior sagittal sinus, major cortical veins, and adjacent arteries when surgical planning requires more detailed evaluation. In parasagittal meningiomas, particular attention is given to the degree of involvement of the superior sagittal sinus. Imaging helps determine whether the sinus is still patent, shows reduced flow, or is completely occluded by the tumor. When the sinus is partially or completely obstructed, it becomes especially important to identify the collateral venous pathways through which cerebral venous drainage is maintained, because these veins must be carefully preserved during surgery.
Conventional catheter angiography (DSA) is now rarely required and is mainly performed when preoperative tumor embolization is being considered.
Monitoring Without Treatment: When Parasagittal Meningiomas Are Only Observed
Not all parasagittal meningiomas require immediate treatment.
Approximately 30–50% of newly diagnosed meningiomas are initially managed with active surveillance rather than immediate surgery. Among incidentally discovered tumors, however, observation without surgery is chosen in the majority of patients, often around 60–80%, particularly when the tumor is small and not causing symptoms.
Monitoring is usually recommended when:
• the tumor causes no neurological symptoms, especially if it is small
• imaging shows little or no growth over time
• the tumor is not compressing important parasagittal cortical brain structures
• there is little or no surrounding brain edema
• there is no evidence that the lesion is significantly compromising major venous drainage
• the patient is elderly or has serious medical conditions
On imaging studies, meningiomas that are partially or extensively calcified often represent tumors with long-standing slow growth, and this finding may further support a decision for observation rather than immediate surgery. Follow-up generally involves MRI examinations every 6–12 months initially.
Symptomatic Treatment for Parasagittal Meningioma
Medications are often used to control complications caused by the tumor.
• Brain swelling (edema) is commonly treated with corticosteroids, most often dexamethasone, which reduces edema in the surrounding brain tissue.
• Seizures are treated with antiepileptic medications, such as levetiracetam or other modern antiseizure drugs.
These medications stabilize the patient but do not eliminate the tumor itself.
Parasagittal Meningioma and Epilepsy
Seizures may sometimes be the first symptom of a parasagittal meningioma, particularly when the tumor is located near the cerebral cortex.
However, it is important to understand that not every seizure in a patient with a parasagittal meningioma is necessarily caused by the tumor. Epilepsy is relatively common in the general population, and the coexistence of a small incidental meningioma does not automatically mean that the tumor is responsible for the seizures.
For this reason, physicians must carefully evaluate whether the tumor is actually the source of epileptic activity. This assessment usually includes:
• analysis of tumor location relative to the cerebral cortex
• evaluation of peritumoral brain edema
• correlation between EEG findings and the tumor region
• consideration of other possible causes of epilepsy
When seizures are clearly related to the tumor, surgical removal of the parasagittal meningioma often significantly reduces seizure frequency, and in some patients seizures may stop completely.
Antiepileptic medications are usually used to control seizures before and for some period after surgery.
Surgical Treatment of Parasagittal Meningioma
Surgery remains the primary treatment for symptomatic or progressively growing parasagittal meningiomas. The procedure is performed through a craniotomy, which involves temporarily removing a portion of the skull to access the tumor.
In most cases the operation proceeds through several stages:
• Skin incision and craniotomy
The scalp is opened using a carefully planned incision. Depending on the location of the tumor, the incision may be linear, curved, or horseshoe-shaped. Whenever possible, it is placed within the hairline for cosmetic reasons. In most modern neurosurgical procedures the hair does not need to be completely shaved. A craniotomy is then performed directly above the tumor and the involved segment of the superior sagittal sinus, allowing adequate exposure of both the tumor and the adjacent venous structures.
• Opening of the dura
The dura mater is carefully opened to expose the tumor and the surrounding brain structures. The dura is circumferentially incised around the tumor attachment when possible, which helps interrupt a major portion of the arterial blood supply entering the tumor and reduce intraoperative bleeding during subsequent tumor removal. Smaller feeding vessels may also arise from cortical (brain) arteries at the tumor–brain interface. In parasagittal meningioma, special attention must also be paid to the superior sagittal sinus and bridging veins.
• Internal tumor debulking
The tumor is then reduced from the inside, most often using an ultrasonic aspirator (CUSA). This internal debulking decreases tumor volume and pressure, making subsequent dissection from the surrounding brain, cortical vessels, bridging veins, and adjacent tissues safer.
• Tumor removal
After internal decompression of the tumor, the remaining peripheral tumor remnants are carefully separated from the surrounding brain tissue and cortical vessels and then removed piece by piece. If the tumor is densely adherent to the superior sagittal sinus or important draining veins, a small remnant may sometimes be intentionally left behind to preserve venous outflow and reduce neurological risk.
• Treatment of the dural attachment and dural defect
Because parasagittal meningiomas arise from the dura, the involved portion of the dura is removed together with the tumor to reduce the risk of recurrence when this can be done safely. When complete removal is not safe, the dural base may be coagulated. If a segment of dura is removed, the defect is typically reconstructed using a dural graft to restore a watertight barrier around the brain. This graft may be created from the patient’s own tissue, such as periosteum elevated from the skull during the operation or muscle fascia. The dura can also be replaced by biocompatible artificial dural substitutes specifically designed for neurosurgical reconstruction.
• Management of superior sagittal sinus involvement
When parasagittal meningiomas involve the superior sagittal sinus, surgical strategy depends on whether the sinus is patent, partially infiltrated, or completely occluded. If the anterior third of the sinus is already completely occluded, some surgeons may, in selected cases, remove the involved sinus segment together with the tumor while preserving cortical venous drainage. When the sinus remains partially patent, removal of the infiltrated sinus wall with venous reconstruction may be performed in selected cases. In contrast, tumors involving the middle or posterior third of the superior sagittal sinus are usually managed more conservatively because these regions drain critical cortical veins. In such situations surgeons often preserve the sinus and leave a small residual tumor within the sinus, which can later be treated with stereotactic radiosurgery (SRS) if growth occurs.
• Removal of infiltrated bone (when present)
Some parasagittal meningiomas cause thickening or infiltration of the adjacent skull bone (hyperostosis). In such cases the abnormal bone may be drilled away, and occasionally a larger bone segment must be removed and at the same surgery or later reconstructed with a cranioplasty.
• Dural reconstruction and closure
After tumor removal the dura is reconstructed using a dural graft if necessary. The bone flap is replaced, or reconstructed if bone was removed, and the scalp is closed.
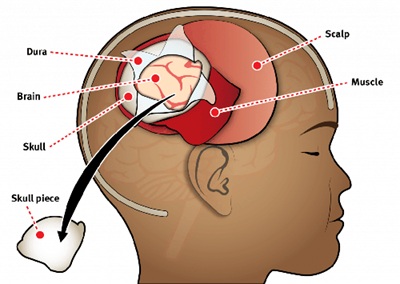
Image: The image illustrates a craniotomy. Both the skin incision and the skull opening are performed within the hair-bearing area of the scalp. The dura is opened to expose the tumor or the brain as part of the surgical approach to the tumor. After the procedure, the bone flap is secured and the scalp is reconstructed, ensuring no cosmetic defect remains after healing. In parasagittal meningiomas, this type of craniotomy is performed at the midline of the head, directly above the tumor.
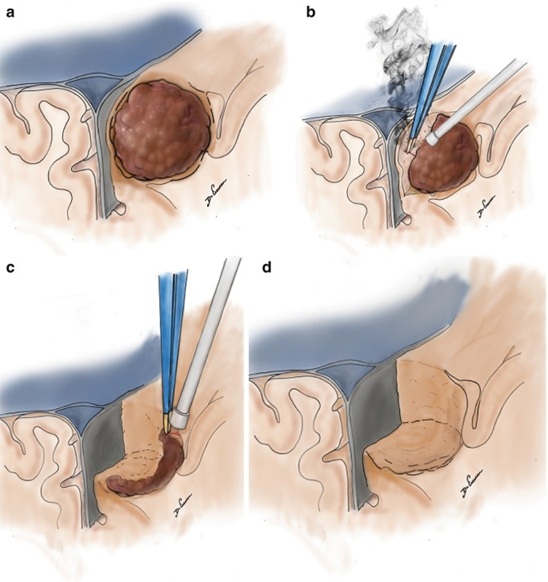
Image: Stages of surgical removal of a parasagittal meningioma. After craniotomy and opening of the dura, image (a) shows the dark brown parasagittal meningioma. Image (b) illustrates its separation from the brain, sagittal sinus, blood vessels, and other normal tissues, followed by its piecemeal reduction. Image (c) shows the removal of the remaining peripheral parts of the meningioma. Image (d) shows the condition after the meningioma has been completely removed.
Modern Surgical Technologies for Parasagittal Meningioma
Modern neurosurgery employs several technologies to increase precision and safety.
• Neuronavigation systems function as intraoperative GPS, allowing the surgeon to navigate within the skull with millimeter accuracy.
• Ultrasonic aspirators (CUSA) fragment and aspirate tumor tissue while preserving surrounding blood vessels and brain tissue.
• Intraoperative neurophysiological monitoring allows continuous monitoring of motor or sensory pathway function during surgery when the tumor is close to eloquent cortical areas, helping avoid surgical damage to important functional regions.
These technologies significantly reduce the risk of neurological injury.
In selected cases, surgeons may perform preoperative embolization before surgical removal of a parasagittal meningioma. This procedure involves inserting a catheter into arteries supplying the tumor and injecting materials that reduce blood flow to the tumor in order to decrease intraoperative bleeding. Embolization is mainly considered for large, highly vascular meningiomas supplied by branches of the external carotid artery. Today it is used in a relatively small proportion of cases because the procedure itself may carry risks such as stroke or unintended embolization of normal vessels, and advances in modern microsurgical techniques have reduced the need for routine embolization.
Extent of Parasagittal Meningioma Removal — Simpson Classification
The completeness of tumor removal is classified using the Simpson grading system.
• Simpson Grade I — complete removal of the tumor and its dural attachment
– recurrence risk approximately 5–10% over long-term follow-up
– probability of needing another intervention ~3–5%
• Simpson Grade II — tumor removed, dural attachment coagulated
– recurrence risk approximately 10–20%
– probability of further treatment ~5–10%
• Simpson Grade III — tumor removed but dura left intact
– recurrence risk approximately 20–25%
– probability of additional treatment ~10–20%
• Simpson Grade IV — subtotal removal
– recurrence risk approximately 40–60%
– additional treatment (surgery or radiotherapy) often required in 30–50%
• Simpson Grade V — biopsy or decompression only
– tumor progression expected in most patients (>80–90%)
– further definitive treatment usually necessary
The Simpson grade strongly influences the likelihood of tumor recurrence.
Because parasagittal meningiomas may involve the superior sagittal sinus, complete removal including the dural attachment is not always safely achievable, and this is one of the major reasons why their long-term prognosis depends not only on tumor grade but also on venous anatomy and surgical strategy.
Radiation Therapy for Parasagittal Meningioma
Radiation therapy is used when complete surgical removal is not possible, when tumors recur, or when a small residual tumor remains after surgery. It may also be considered for small parasagittal meningiomas that demonstrate clear growth during imaging follow-up, particularly when surgery carries increased risk or in situations where the patient prefers a non-surgical treatment option after discussion of the risks and benefits.
Typical radiation doses for meningiomas are:
• 12–14 Gy delivered in a single session in stereotactic radiosurgery
• less commonly, about 50–54 Gy in conventionally fractionated radiotherapy
Radiosurgery is generally most suitable for tumors smaller than about 2.5–3 cm that do not cause significant compression of the brain.
Radiation therapy can effectively stop tumor growth in many patients. Modern radiation techniques provide long-term tumor control in approximately 85–95% of benign meningiomas, especially when small residual or recurrent tumors are treated with stereotactic radiosurgery.
Even in parasagittal meningiomas, radiation therapy is not appropriate for all tumors. Large lesions with marked edema, significant mass effect, symptomatic cortical compression, or lesions requiring decompression because of neurological deficit are usually better managed surgically.
The final treatment decision is usually made after careful evaluation of tumor size, exact parasagittal location, patient age, symptoms, surrounding edema, superior sagittal sinus involvement, and overall medical condition.
Treatment Decision Summary for Parasagittal Meningioma
Treatment decisions for parasagittal meningioma usually follow several general principles.
1. Before treatment
If the tumor is small, causes no symptoms, and does not significantly compress the brain, MRI monitoring is often the safest first step.
If the tumor causes neurological symptoms, produces significant mass effect or edema, or shows documented growth on follow-up imaging, active treatment is more often recommended.
2. Choosing the main treatment
Surgery is usually preferred when the patient is in good overall condition and the tumor can be removed with acceptable neurological risk, taking into account possible involvement of the superior sagittal sinus and nearby cortical veins.
Radiotherapy or radiosurgery may be considered when surgery carries higher risk, when the tumor is small, when there is residual or recurrent tumor, or when the patient prefers radiation treatment after discussion of the available options.
3. After surgery
WHO Grade I + complete removal: MRI follow-up is usually sufficient.
WHO Grade I + residual tumor: follow-up or radiosurgery/radiotherapy may be considered depending on tumor growth and location.
WHO Grade II: postoperative radiotherapy is usually recommended after incomplete tumor removal. After complete resection, some patients may be managed with MRI follow-up or radiotherapy depending on recurrence risk.
WHO Grade III: surgery is usually followed by radiotherapy regardless of the completeness of tumor removal, together with close imaging follow-up.
This is a simplified overview. In real clinical practice, treatment decisions also depend on tumor size, exact cortical location, involvement of the superior sagittal sinus, growth rate, surrounding brain edema, proximity to eloquent brain regions, patient age, and overall neurological condition.
Recurrence of Parasagittal Meningioma
Recurrence of parasagittal meningioma is uncommon after complete removal, but it may still occur depending on the WHO tumor grade, the extent of surgical resection, and whether residual tumor remains along or within the superior sagittal sinus.
After complete removal of benign (WHO Grade I) meningiomas, long-term recurrence rates are usually around 5–10%.
When subtotal removal is performed, recurrence rates are higher.
Atypical (WHO Grade II) meningiomas recur more frequently, while malignant (WHO Grade III) tumors have the highest recurrence risk and usually require additional radiotherapy.
Because recurrence may appear many years after treatment, long-term MRI follow-up is essential.
➡ Detailed explanation of recurrence patterns, risk factors, and treatment options is explained here:
Meningioma Recurrence — Causes, Risk, and Treatment
Treatment Strategy by Tumor Grade in Parasagittal Meningioma
Management also depends strongly on the WHO tumor grade.
• WHO grade I meningiomas. After complete surgical removal, most patients require only periodic MRI follow-up. If the tumor recurs during follow-up, management may include continued observation, repeat surgery, or stereotactic radiosurgery, depending on the rate of growth, sinus involvement, and clinical symptoms.
• WHO grade II (atypical) meningiomas. These tumors recur more frequently. Postoperative radiotherapy is often recommended, particularly after incomplete tumor removal, although some patients may be managed with close MRI follow-up after complete resection.
• WHO grade III (malignant) meningiomas. These aggressive tumors typically require postoperative radiotherapy regardless of the completeness of surgical removal, together with close imaging follow-up.
Request Parasagittal Meningioma Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Being told that an MRI has revealed a parasagittal meningioma often raises important questions:
Is the tumor dangerous?
Should it be monitored or surgically removed?
What is the risk of progressive weakness, seizures, or tumor growth?
Is radiosurgery an appropriate alternative?
An independent neurosurgical second opinion may help clarify the urgency of treatment,
expected neurological outcome, likelihood of tumor growth or recurrence, and the safest balance between
observation, surgical removal, and radiation therapy based on MRI findings, tumor size, involvement of the superior sagittal sinus,
surrounding brain edema, and the patient’s overall neurological condition.
- ✔ Send a brief message describing your current symptoms and the key findings from your MRI or CT report
- ✔ You will receive a reply within 24 hours explaining whether an online consultation is appropriate and which documentation is required
- ✔ Priority cases: rapidly worsening neurological symptoms, new seizures, tumors affecting the motor cortex or superior sagittal sinus, proposed urgent surgery, or conflicting specialist recommendations — write PRIORITY in your first message
- ✔ MRI images (DICOM format if you have it), radiology reports, and relevant documentation can be reviewed.
- ✔ During consultation we explain whether observation, microsurgical removal, radiosurgery, or combined treatment is most appropriate — including expected neurological risks and up to 10 days of follow-up clarification
Consultation fees typically range from $180–250 depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This corresponds to typical international specialist telehealth neurosurgical second-opinion services.
Long-Term Monitoring of Parasagittal Meningioma
Because parasagittal meningiomas may recur many years after treatment, long-term follow-up is essential.
Typical surveillance includes:
• annual MRI for several years after treatment
• longer imaging intervals if the tumor remains stable
Early detection of recurrence allows treatment before significant neurological damage develops.
Experimental and Targeted Therapies for Parasagittal Meningioma
Several medications have been studied for recurrent or progressive meningiomas when surgery and radiotherapy are no longer sufficient. These include bevacizumab, which targets tumor blood vessel growth, as well as drugs acting on molecular pathways such as AKT or SMO inhibitors. Somatostatin-receptor-based treatments such as octreotide and combinations including everolimus have also been investigated. However, current evidence remains limited, and surgery and radiation therapy remain the main treatments for most meningiomas.
When Expert Opinions May Differ in Parasagittal Meningioma
In many patients diagnosed with parasagittal meningioma, different specialists may recommend different treatment strategies. This situation is common in neurosurgery and does not necessarily indicate that one opinion is correct while another is wrong.
Treatment decisions for parasagittal meningiomas depend on multiple clinical factors, including:
• tumor size
• exact parasagittal cortical location
• growth rate observed on MRI
• presence of surrounding brain edema or mass effect
• patient age and overall health
• presence or absence of neurological symptoms
• relationship of the tumor to the superior sagittal sinus, important cortical veins, arteries, or eloquent brain regions
• tumor grade if histological diagnosis is already known
Because these factors interact in complex ways, reasonable specialists may arrive at different conclusions regarding the safest management strategy.
Observation vs. Early Surgery in Parasagittal Meningioma
One of the most common differences in opinion occurs when a parasagittal meningioma is discovered incidentally on MRI and the patient has no symptoms. Some specialists recommend active surveillance, particularly when the tumor is small and shows no signs of growth. Others may recommend early surgery, especially if the tumor is located near an important motor parasagittal region where future growth could threaten neurological function or make later treatment more difficult because of increasing superior sagittal sinus involvement. Both approaches may be appropriate depending on the individual clinical situation.
Differences in Surgical Strategy for Parasagittal Meningioma
Even when surgery is recommended, surgeons may disagree about the optimal surgical strategy. In some cases a surgeon may aim for more complete removal including treatment of the dural attachment, while another may prefer a more conservative removal if the tumor lies close to the superior sagittal sinus, important cortical veins, or eloquent brain tissue.
Surgery vs. Radiation Therapy in Parasagittal Meningioma
Another area where opinions may differ involves the use of radiation therapy. Some specialists recommend surgical removal first, followed by radiation only if residual tumor remains. Others may recommend primary stereotactic radiosurgery, particularly for small tumors without significant mass effect. Decisions between surgery and radiation therapy may also depend on tumor size, location, growth rate, proximity to important functional cortical regions, degree of superior sagittal sinus involvement, and the expected surgical risk for the individual patient.
Because treatment decisions depend on many individual variables, careful review of MRI images and clinical history often allows specialists to explain why different recommendations may exist and which option is most appropriate for a specific patient.
Superior sagittal sinus involvement is one of the most important factors influencing differences in specialist recommendations.
When a parasagittal meningioma involves the superior sagittal sinus, treatment decisions become significantly more complex. The key issue is not only whether the tumor can be removed, but whether complete removal is safe given the degree of sinus involvement and the role of venous drainage.
When the sinus remains patent and functional, aggressive removal carries a higher risk of venous infarction, brain swelling, or neurological deficit, and some surgeons may recommend leaving a small residual tumor within the sinus wall rather than risking damage to venous outflow. Others may consider more extensive resection with venous reconstruction in selected cases, while a third approach may favor primary radiosurgery to avoid sinus-related surgical risks.
Because of this, the same MRI finding — a tumor touching, partially infiltrating, or involving the superior sagittal sinus — may lead to fundamentally different recommendations depending on surgical experience, institutional strategy, and how each specialist weighs the risk of venous injury against the benefit of more complete tumor control.
How Parasagittal Meningioma Prognosis Depends on Location, Grade, and Extent of Removal
The prognosis of parasagittal meningioma depends primarily on three major factors: the biological grade of the tumor, its exact anatomical location, and the extent to which it can be safely removed.
In general, WHO Grade I meningiomas have the most favorable prognosis. They usually grow slowly, and when they are completely removed together with their dural attachment, long-term tumor control is often excellent. By contrast, atypical and malignant meningiomas have a higher risk of recurrence, even after apparently complete surgery, and therefore usually require closer follow-up and often additional radiation therapy.
Tumor location is equally important. Parasagittal meningiomas are often surgically treatable, but their prognosis is influenced not only by cortical location but also by their relationship to the superior sagittal sinus and bridging veins. Tumors located over eloquent motor or sensory cortex, or near important venous structures, may still require the surgeon to choose between more radical removal and preservation of neurological function.
For this reason, the extent of tumor removal strongly influences long-term outcome. The smaller the amount of residual tumor left behind, the lower the probability of recurrence. However, in modern neurosurgery, the best result does not always mean the most aggressive resection. In some patients, intentionally leaving a very small tumor remnant densely adherent to the superior sagittal sinus, critical cortical veins, or eloquent brain tissue may provide a better overall outcome than attempting complete removal at the cost of permanent neurological damage.
In practical terms, prognosis is best in patients with benign parasagittal meningiomas located in surgically favorable regions and removed completely. It is generally less favorable in higher-grade tumors and in cases where only subtotal removal is possible because of the risk to important functional brain structures or venous anatomy.
Can a Parasagittal Meningioma Become Life-Threatening?
Yes, a parasagittal meningioma can become life-threatening, although this is not the usual course in most patients.
Most parasagittal meningiomas are slow-growing tumors, and many remain stable for years without causing major neurological problems. However, if the tumor becomes large enough, it may produce severe pressure on the brain, significant surrounding edema, progressive cortical dysfunction, marked intracranial pressure elevation, or brain herniation. In addition, when the lesion significantly affects the superior sagittal sinus, impaired venous drainage may worsen edema and neurological deterioration. In such situations, the danger does not arise only from the biological nature of the tumor itself, but from its mass effect on vital brain structures and, in some cases, its effect on venous outflow.
A parasagittal meningioma may therefore become life-threatening when it causes marked intracranial pressure elevation, brain herniation, repeated seizures with progressive neurological deterioration, or severe mass effect on the brain. This risk is higher in large tumors, tumors associated with extensive edema, tumors involving major venous structures, and in more aggressive histological forms such as atypical or malignant meningioma.
For this reason, even though parasagittal meningiomas are often described as benign tumors, they should never be considered harmless solely on the basis of histological grade. Their real clinical significance depends on tumor size, exact cortical location, rate of growth, degree of superior sagittal sinus involvement, and the effect they produce on surrounding brain structures.
Frequently Asked Questions About Parasagittal Meningioma
Can a parasagittal meningioma cause progressive leg weakness or walking difficulty?
Yes. A parasagittal meningioma can cause progressive leg weakness or walking difficulty when it grows near the motor cortex or paracentral lobule, especially in the middle third of the superior sagittal sinus. This region contains important motor and sensory areas for the opposite leg. As the tumor enlarges, it compresses the adjacent cerebral cortex and may interfere with normal movement control. Patients may notice clumsiness, loss of fine motor control, heaviness of the leg, gait difficulty, or progressive weakness on the opposite side of the body. Surrounding brain edema can worsen these symptoms. The degree of recovery depends on tumor size, duration of compression, edema, and whether the tumor can be removed safely without injuring motor pathways or venous drainage.
Why are seizures common in parasagittal meningioma?
Seizures are common in parasagittal meningioma because these tumors lie close to the cerebral cortex. Even though the tumor usually grows outside the brain tissue, it can irritate the brain surface by compression, local inflammation, or surrounding edema. When the cortex becomes irritated, abnormal electrical activity may occur and trigger seizures. However, not every seizure in a patient with a parasagittal meningioma is automatically caused by the tumor. Doctors usually consider tumor location, edema, the seizure pattern, EEG findings, and other possible causes of epilepsy. When seizures are clearly related to the tumor, surgical removal often reduces seizure frequency, and in some patients seizures may stop completely. Antiepileptic medication is commonly used before and after surgery.
Can a parasagittal meningioma be dangerous even if it is benign?
Yes. A parasagittal meningioma can be dangerous even if it is biologically benign because the clinical risk depends not only on tumor grade, but also on size, location, edema, and involvement of major venous structures. Most parasagittal meningiomas are WHO Grade I tumors and grow slowly, but a large tumor can compress the brain, produce significant edema, increase intracranial pressure, or affect important motor and sensory regions. When the superior sagittal sinus is compressed, infiltrated, or occluded, venous drainage may be impaired and neurological deterioration may worsen. Therefore, a benign parasagittal meningioma should not be considered harmless only because of its histology. Its real significance depends on growth, symptoms, venous anatomy, and mass effect.
Why may parasagittal meningioma remain unnoticed for years before diagnosis?
Parasagittal meningioma may remain unnoticed for years because many of these tumors grow slowly and initially produce few or no symptoms. Since they arise outside the brain tissue, they often compress the cortex gradually rather than causing sudden damage. Some tumors are discovered incidentally on MRI or CT performed for unrelated reasons. Symptoms may appear only when the tumor becomes large enough to irritate the cortex, cause seizures, produce edema, compress motor or sensory regions, or affect venous drainage through the superior sagittal sinus. Even when symptoms appear, they may be subtle at first, such as mild leg clumsiness, headache, or occasional seizures. This is why MRI is often required to clarify the diagnosis and anatomical risk.
Can headaches from parasagittal meningioma be confused with migraine or tension headache?
Yes. Headaches in a patient with parasagittal meningioma can be confused with common headache disorders such as migraine, tension-type headache, or cervicogenic headache. Headache is frequent in the general population, so the presence of a small meningioma does not automatically mean the tumor is the cause. A parasagittal meningioma is more likely to be responsible when the tumor is large, produces significant edema, increases intracranial pressure, or causes mass effect on nearby brain structures. For this reason, the headache pattern should be carefully evaluated before recommending surgery only because a tumor is present. Headache alone is usually not enough to justify immediate removal of a small, otherwise asymptomatic parasagittal meningioma.
How does parasagittal meningioma affect the motor cortex and sensory cortex?
Parasagittal meningioma affects the motor and sensory cortex by compressing the brain surface near the midline. Tumors in the middle third of the superior sagittal sinus are especially important because this region includes motor and sensory representation for the opposite leg. Compression may cause progressive weakness, clumsiness, gait difficulty, numbness, altered sensation, or loss of fine motor control. Tumors over sensory cortex may cause sensory disturbance or sensory neglect, while tumors near motor cortex may produce weakness or seizures. The effect depends on exact cortical location, tumor size, surrounding edema, and whether important veins or the superior sagittal sinus are involved. This anatomical relationship strongly influences both symptoms and surgical risk.
Can a parasagittal meningioma cause symptoms by compressing the superior sagittal sinus?
Yes. A parasagittal meningioma can cause symptoms by compressing, invading, partially obstructing, or completely occluding the superior sagittal sinus. This sinus is a major venous channel that drains blood from the brain. When venous drainage is impaired, pressure in the venous system may rise, contributing to brain edema, increased intracranial pressure, and neurological deterioration. If the sinus becomes gradually obstructed, collateral venous pathways may take over part of the drainage, and these veins must be carefully preserved during surgery. Symptoms may therefore result not only from direct cortical compression, but also from disturbed venous outflow. This is one of the main reasons why parasagittal meningioma treatment requires careful imaging and individualized surgical planning.
What does parasagittal mean in the brain?
Parasagittal means “near the sagittal midline” of the brain. In practical MRI language, the parasagittal region is the area close to the midline of the head, near the falx cerebri and the superior sagittal sinus. A parasagittal meningioma grows from the dura in this region and may lie close to important motor and sensory areas, especially those controlling the opposite leg. This is why parasagittal meningiomas may cause leg weakness, walking difficulty, numbness, seizures, or symptoms related to pressure on the brain. The exact location matters because tumors near the superior sagittal sinus and cortical veins can be more complex to remove safely.
What is a parasagittal craniotomy for meningioma?
A parasagittal craniotomy for meningioma is a skull opening planned near the midline of the head, directly over the parasagittal tumor and the involved segment of the superior sagittal sinus. The goal is to reach the tumor safely, reduce its volume, separate it from the brain surface, protect cortical veins and venous drainage, and remove the dural attachment when this can be done safely. This operation is more complex when the meningioma touches, narrows, invades, or obstructs the superior sagittal sinus. In those situations, preserving venous outflow may be more important than forcing complete tumor removal.
Why is superior sagittal sinus involvement so important in parasagittal meningioma?
Superior sagittal sinus involvement is important in parasagittal meningioma because it often determines whether complete removal is safe. The sinus is a major venous drainage pathway for the brain. A tumor may only touch the sinus, partially infiltrate its wall, narrow its flow, or completely occlude it. If the sinus remains patent and functional, aggressive removal can risk venous infarction, brain swelling, or neurological deficit. If it is already completely occluded, surgery may sometimes be planned differently because collateral veins may have taken over drainage. Imaging such as MR venography, CT venography, or angiography may be needed to assess sinus flow and collateral pathways. This factor often explains why specialists recommend different strategies.
Can parasagittal meningioma become life-threatening because of brain edema or mass effect?
Yes. Parasagittal meningioma can become life-threatening when it becomes large enough to produce severe brain compression, extensive surrounding edema, marked intracranial pressure elevation, or brain herniation. Most parasagittal meningiomas grow slowly, and many remain stable for years, but large tumors can create a mass effect inside the closed skull. Because the skull has limited space, increasing pressure may displace brain structures from their normal position. In severe cases, brain tissue can be pushed through natural openings, compressing vital centers responsible for consciousness, breathing, and circulation. The risk is higher when the tumor is large, associated with extensive edema, involves major venous structures, or belongs to a more aggressive histological grade.
Does every parasagittal meningioma require surgery?
No. Not every parasagittal meningioma requires surgery. Many incidentally discovered tumors, especially small tumors without symptoms, growth, significant edema, or important venous involvement, may be safely monitored with periodic MRI. Observation is often chosen when the tumor does not compress important parasagittal cortical regions and does not compromise the superior sagittal sinus or major venous drainage. Treatment becomes more likely when the tumor grows, causes seizures, progressive weakness, sensory symptoms, significant edema, mass effect, or neurological deterioration. Surgery is generally preferred when a symptomatic or growing tumor can be removed with acceptable neurological risk. Smaller growing tumors may sometimes be treated with radiosurgery if they do not cause significant compression.
When can parasagittal meningioma be safely monitored without treatment?
Parasagittal meningioma can be monitored without treatment when it is small, causes no neurological symptoms, shows little or no growth, produces little or no edema, and does not compress important cortical areas or compromise venous drainage. This is especially common for incidentally discovered meningiomas. Follow-up usually involves MRI every 6–12 months at first. Partially or extensively calcified tumors may represent long-standing slow growth and can further support observation. Monitoring is less appropriate if the tumor grows, produces seizures, progressive weakness, gait difficulty, sensory symptoms, significant edema, mass effect, or involvement of the superior sagittal sinus. Observation must therefore be active surveillance, not neglect, because treatment decisions can change if imaging or symptoms evolve.
How is treatment decision-making performed in parasagittal meningioma?
Treatment decision-making in parasagittal meningioma depends on tumor size, exact cortical location, growth rate, symptoms, edema, involvement of the superior sagittal sinus, relationship to cortical veins, and patient health. If the tumor is small, stable, asymptomatic, and not compressing important brain regions or venous structures, MRI monitoring may be safest. If it causes seizures, progressive weakness, sensory symptoms, significant mass effect, edema, or documented growth, active treatment is more often recommended. Surgery is usually preferred when the tumor can be removed with acceptable neurological risk. Radiosurgery or radiotherapy may be considered for small tumors, residual or recurrent tumor, or when surgery carries higher risk. The safest strategy is individualized, not automatic.
Why may specialists recommend observation while others advise early surgery for parasagittal meningioma?
Specialists may disagree between observation and early surgery for parasagittal meningioma because the decision depends on several interacting risks. Observation may be reasonable when the tumor is small, incidental, stable, and not causing symptoms, edema, cortical compression, or venous compromise. Early surgery may be recommended if the tumor is near the motor cortex, shows growth, causes seizures or weakness, produces edema, or begins to involve the superior sagittal sinus. Some specialists may worry that waiting could make later surgery harder if sinus involvement increases. Others may prioritize avoiding surgical risk while the tumor is still asymptomatic. Both approaches can be reasonable depending on MRI findings, symptoms, age, and venous anatomy.
How is surgery for parasagittal meningioma performed?
Surgery for parasagittal meningioma is performed through a craniotomy placed directly over the tumor and the involved segment of the superior sagittal sinus. The scalp incision is planned carefully, usually within the hairline when possible. After opening the skull and dura, the surgeon exposes the tumor, brain surface, cortical vessels, bridging veins, and sinus region. The tumor is often reduced internally first, usually with an ultrasonic aspirator, to decrease pressure and make separation safer. The remaining tumor is then dissected from the brain, vessels, sagittal sinus, and surrounding tissues. The dural attachment is removed or coagulated when safe, and the dura is reconstructed. If the tumor is adherent to critical veins or sinus, a small remnant may be left.
Can a parasagittal meningioma be completely removed when it involves the superior sagittal sinus?
A parasagittal meningioma can sometimes be completely removed when it involves the superior sagittal sinus, but this depends on which part of the sinus is involved and whether the sinus is still functioning. If the anterior third is already completely occluded, some surgeons may remove the involved sinus segment in selected cases while preserving cortical venous drainage. If the sinus is partially patent, more complex resection with venous reconstruction may occasionally be considered. However, tumors involving the middle or posterior third of the sinus are usually managed more conservatively because these regions drain critical cortical veins. In such cases, preserving venous outflow may be more important than complete removal, and residual tumor can be monitored or treated later.
Why may surgeons intentionally leave part of a parasagittal meningioma behind?
Surgeons may intentionally leave part of a parasagittal meningioma behind when complete removal would create a high risk of venous injury or neurological deficit. This most often occurs when the tumor is densely adherent to the superior sagittal sinus, important cortical veins, or eloquent motor and sensory brain regions. If the sinus remains patent and functional, aggressive removal may cause venous infarction, brain swelling, or permanent weakness. In modern neurosurgery, the best outcome does not always mean the most radical resection. Leaving a small remnant within the sinus wall or near critical veins can preserve venous drainage and neurological function. The remnant may later be monitored or treated with stereotactic radiosurgery if it grows.
What is Simpson grading and why does it matter in parasagittal meningioma surgery?
Simpson grading describes how completely a meningioma and its dural attachment have been removed. In general, more complete removal lowers recurrence risk. Simpson Grade I means complete removal of the tumor and its dural attachment. Grade II means the tumor is removed and the dural attachment is coagulated. Grade IV means subtotal removal, and Grade V means biopsy or decompression only. In parasagittal meningioma, Simpson grade is important but must be balanced against venous safety. Because the tumor may involve the superior sagittal sinus or important cortical veins, complete removal is not always safe. A lower recurrence risk is desirable, but preserving venous drainage and neurological function may be more important than achieving the most aggressive Simpson grade.
When is radiosurgery or radiotherapy used for parasagittal meningioma?
Radiosurgery or radiotherapy may be used for parasagittal meningioma when complete surgical removal is not possible, when residual tumor remains after surgery, when the tumor recurs, or when a small growing tumor is suitable for non-surgical control. Stereotactic radiosurgery is generally most suitable for small tumors, usually up to about 2.5–3 cm, that do not cause significant brain compression or severe edema. Radiation may also be considered when surgery carries higher risk, or when the patient prefers a non-surgical option after discussion of risks and benefits. Large tumors with marked edema, mass effect, neurological deficits, or need for decompression are usually better treated surgically. Final decisions depend on size, location, sinus involvement, symptoms, and medical condition.
How do doctors determine whether a parasagittal meningioma is truly causing my seizures?
A parasagittal meningioma is more likely to be responsible for seizures when it lies directly next to the cerebral cortex, causes cortical compression or surrounding brain edema, and the seizure pattern corresponds to the function of the affected brain region. Doctors also assess whether the seizures began after the tumor became clinically significant and whether another neurological condition could explain them.
Evaluation usually includes a detailed seizure history, neurological examination, EEG findings, and careful MRI review. The connection is more convincing when EEG abnormalities and seizure semiology correspond to the same cortical region as the tumor, particularly when significant edema is present. Other possible causes of epilepsy must also be excluded. When the relationship remains uncertain or seizures continue despite appropriate medication, a more structured epilepsy assessment may be required. More information is available on our epilepsy surgery page.
What are the specific risks and complications of parasagittal meningioma surgery?
The risks depend mainly on tumor size, surrounding brain edema, proximity to the motor or sensory cortex, and the degree of involvement of the superior sagittal sinus, bridging veins, and parasagittal cortical draining veins. Possible complications include bleeding, postoperative hematoma, brain swelling, seizures, infection, cerebrospinal fluid leakage, stroke, venous infarction, wound-healing problems, and new neurological deficits.
Damage to parasagittal veins, bridging veins, or the superior sagittal sinus may impair venous drainage and cause venous congestion, thrombosis of the superior sagittal sinus or cortical veins, severe postoperative edema, hemorrhagic venous infarction, raised intracranial pressure, and neurological deterioration. These complications may lead to weakness, sensory loss, seizures, reduced consciousness, or difficulty walking, especially when the tumor lies near the cortical region controlling the opposite leg. For this reason, a small residual tumor may sometimes be intentionally left within the sinus or around critical veins to preserve venous outflow. Residual or recurrent tumor may later require MRI monitoring, radiosurgery, radiotherapy, or further surgery. A broader explanation is available on our craniotomy and brain surgery complications page.
Can parasagittal meningioma recur after surgery or radiation treatment?
Yes. Parasagittal meningioma can recur after surgery or radiation treatment, although recurrence risk depends mainly on WHO grade, extent of removal, and whether residual tumor remains along or within the superior sagittal sinus. After complete removal of benign WHO Grade I meningiomas, long-term recurrence risk is relatively low. Subtotal removal carries higher recurrence risk, especially when tumor must be left in the sinus wall or near important veins. WHO Grade II atypical meningiomas recur more often, while WHO Grade III malignant tumors have the highest recurrence risk and usually require radiotherapy. Because recurrence may appear many years after treatment, long-term MRI follow-up is essential. Small recurrences may be monitored, treated with radiosurgery, or reoperated depending on growth and symptoms.
Can an online second opinion help clarify treatment decisions for parasagittal meningioma?
Yes. An online second opinion can help clarify treatment decisions for parasagittal meningioma when MRI or CT has shown the tumor but the safest strategy is unclear. It is especially useful when specialists disagree between observation, surgery, radiosurgery, or radiotherapy; when the tumor involves the superior sagittal sinus; when seizures, progressive weakness, or sensory symptoms are present; or when surgery has been recommended but neurological risk is uncertain. MRI images, reports, and clinical history can be reviewed to assess tumor size, growth, edema, exact cortical location, sinus involvement, and relationship to important veins. The goal is to explain whether monitoring, microsurgical removal, radiosurgery, or combined treatment is most appropriate for that specific case.