Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 10, 2026
Who this page is for
This page is for patients who have pudendal neuralgia or persistent perineal, rectal, pelvic, penile, vulvar, or genital nerve pain that has not improved despite previous treatments. In men, this may appear as perineal pain, penile nerve pain, urethral tingling, pain after sitting, or pain after cycling, pelvic procedures, prostatitis-like symptoms, or pelvic floor tension.
Pain usually continues because not all factors that irritate the pudendal nerve have been properly identified and treated. As a result, even when patients received appropriate single or several medications, the therapy remained incomplete. Once all contributing sources of irritation are recognized, most cases improve only with a targeted combination of medications that addresses every underlying mechanism — supported by vitamin or supplement therapy and physical unloading. If pain still persists, image-guided nerve blocks or, in rare cases, surgical decompression may be considered. A telehealth consultation allows detailed assessment of all contributing factors and guidance on the most effective treatment combination.
If you are unsure whether an online consultation can help after all previous tests and treatment, read why this consultation is different.
When patients usually seek a second opinion for pudendal neuralgia
- Pelvic, genital, perineal, urethral, or rectal pain persists despite medications or physical therapy
- Pain returns after temporary improvement
- The diagnosis feels unclear, such as pudendal neuralgia vs pelvic floor pain, interstitial cystitis, chronic prostatitis, sacral radiculopathy, or another pelvic nerve pain syndrome
- MRI scans, urine tests, gynecologic, urologic, or colorectal examinations did not explain the pain
- Pudendal nerve blocks helped only temporarily, did not help clearly, or gave confusing results
- You are considering nerve blocks, injections, pulsed radiofrequency, neuromodulation, or surgical decompression
- You are unsure whether previous medications failed because the diagnosis was wrong or because the treatment combination was incomplete
If this reflects your situation, a focused telehealth review can clarify the dominant pain generator, contributing factors, treatment options, and what is and is not indicated in your case: Request Consultation
Pudendal Neuralgia — Quick Summary (Read This First)
- Pudendal neuralgia is a nerve pain condition affecting the perineum, genitals, anus, rectum, or urethra. The pain is often described as burning, stabbing, electric, pressure-like, or hypersensitive, and it commonly worsens when sitting.
- Pudendal neuralgia may result from compression, stretching, injury, inflammation, pelvic floor spasm, metabolic neuropathy, or rarely viral irritation affecting the pudendal nerve, its branches, or the sacral nerve roots. Common triggers include prolonged sitting, cycling, childbirth-related stretch injury, pelvic or gynecologic surgery, postoperative scarring, pelvic floor muscle dysfunction, diabetes or inflammatory neuritis, and in selected cases HSV-2 sacral radiculopathy.
- The diagnosis is primarily clinical, not based on MRI alone. Imaging is usually used to exclude other pelvic, spinal, vascular, or tumor-related causes rather than to directly prove pudendal nerve irritation.
- Typical symptoms often worsen with sitting and improve when standing, lying down, or sitting on the toilet. This pattern strongly suggests pudendal nerve involvement, although other pelvic pain conditions can produce similar symptoms.
- Pudendal neuralgia is often confused with urologic, gynecologic, colorectal, or pelvic floor disorders. It may mimic chronic prostatitis, interstitial cystitis, vulvodynia, urethral pain, chronic pelvic pain syndrome, or sacral radiculopathy.
- Pudendal neuralgia should be reassessed when pelvic, perineal, penile, urethral, rectal, vulvar, or genital nerve pain persists despite medication, pelvic-floor therapy, sitting modification, or pudendal nerve blocks. In that situation, the key step is to identify whether the pudendal nerve is truly the main pain generator, whether another pelvic nerve or pelvic-floor disorder is involved, and which contributing factors have kept the pain active.
- Treatment fails when only one presumed cause is treated. Persistent pain often continues because nerve irritation, pelvic floor dysfunction, mechanical pressure, inflammation, sensitization, or metabolic factors are not addressed together.
- A pudendal nerve block can help confirm whether the pudendal nerve is the main pain generator. Temporary pain relief after an image-guided block supports the diagnosis, but one negative block does not always rule it out.
- Most patients are treated first with conservative and medication-based strategies. Sitting modification, pelvic-floor relaxation, neuropathic pain medications, anti-inflammatory measures, and targeted physical unloading are usually tried before invasive procedures.
- Interventional procedures should be considered only when there is a clear target. Pudendal nerve blocks, pulsed radiofrequency, ganglion impar procedures, or peripheral nerve stimulation may help selected patients, especially when symptoms return after temporary relief.
- Surgery is rarely required and should be reserved for carefully selected cases. Pudendal nerve decompression is considered only when entrapment is strongly suspected or confirmed and conservative, medication-based, and interventional treatments have failed.
- In a smaller subset of patients, HSV-2 sacral radiculopathy can mimic pudendal neuralgia. Recurrent genital, urethral, perineal, or anal burning pain with normal urine tests may require consideration of viral-related neuralgia and, in selected cases, antiviral suppression.
- Many persistent cases can improve when the true pain generator and contributing factors are identified. A structured evaluation can clarify whether the pain comes from the pudendal nerve, another pelvic nerve, pelvic floor dysfunction, spinal roots, or overlapping mechanisms.
- Online consultation can help after failed treatment: read why this consultation is different.
Definition of Pudendal Neuralgia
Pudendal neuralgia is a long-lasting nerve pain condition that affects the pudendal nerve — the nerve responsible for sensation in the perineum, genitals, and anal area. The pain is often described as burning, stabbing, electric, or pressure-like and typically worsens when sitting. It affects both sexes, but females predominate (60–70%), probably because the main predisposing factor — complicated vaginal delivery — may lead to symptoms even decades later.
Pudendal neuralgia results from irritation, entrapment, or injury of the pudendal nerve or one of its branches (inferior rectal, perineal, or dorsal genital nerve). The irritation may result from compression, stretching, metabolic or ischemic neuropathy, mechanical injury, or local inflammation. The cause is usually not detected on imaging. Successful treatment depends on identifying which of these processes is involved and the exact location of the problem. In many patients, the main reason for poor treatment response is that this has not been detected, and the right combination of medications was never tried.
The diagnosis is primarily clinical and requires careful differentiation from other pelvic or spinal pain syndromes.
Pudendal neuralgia can mimic UTI-like burning after urination, prostatitis/CPPS, interstitial cystitis, vulvodynia, or HSV-related sacral radiculopathy — so the key is careful differentiation and a stepwise treatment plan.
Causes of Pudendal Neuralgia
The pudendal nerve can be irritated or compressed at several points along its path from the sacral nerve roots (S2–S4) to the perineum.
Common causes include:
- Mechanical compression in the pudendal canal (Alcock’s canal) or between ligaments of the pelvis.
- Direct trauma, prolonged sitting, cycling, or sports with repetitive hip flexion (e.g., jogging).
- Childbirth-related stretch injury, pelvic or gynecologic surgery, or postoperative scarring.
- Pelvic floor muscle spasm or hypertrophy compressing the nerve.
- Metabolic neuropathies such as diabetes or inflammatory neuritis.
- Rarely, viral neuralgia — especially HSV-2 reactivation in the sacral ganglia, which can mimic pudendal nerve pain even without visible lesions.
- Less commonly, vascular entrapment, tumors, or structural deformities of the pelvis.
Often, several factors coexist, which makes diagnosis and treatment complex.
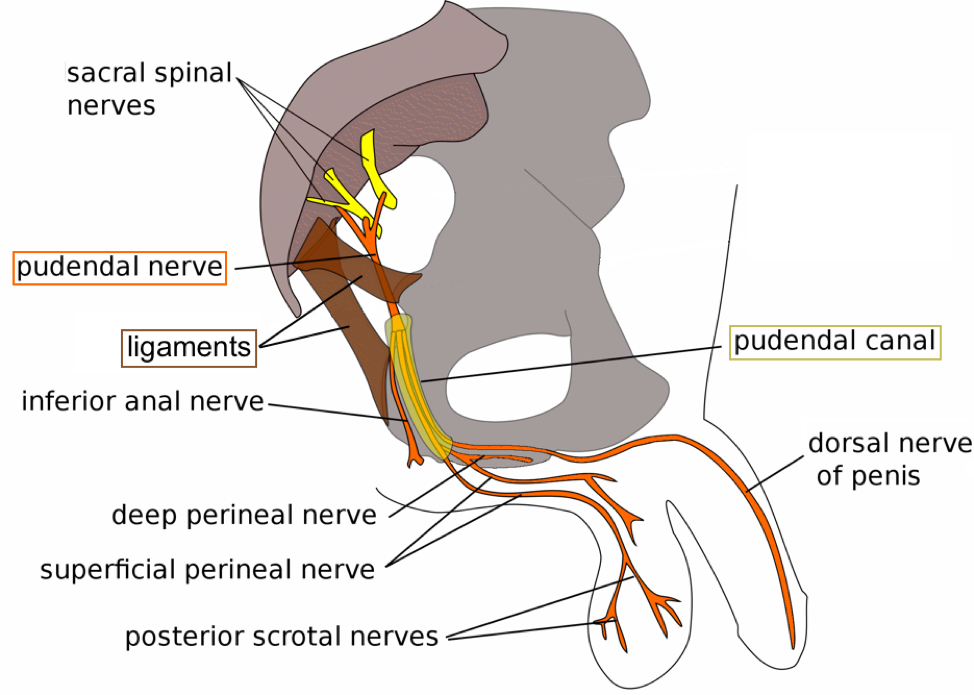
Image: Anatomy of the pudendal nerve, its origin and branches. Learn more about nerve anatomy here.
Symptoms of Pudendal Neuralgia
Typical symptoms include pain, burning, or tingling in the genital area, perineum, anus, rectum or urethra:
- Worsens while sitting and improves when standing, lying down, or sitting on the toilet.
- The pain may occasionally disturb sleep, especially when certain positions increase pelvic or ligament tension.
- Sometimes accompanied by numbness, altered sensation, or allodynia — pain triggered by light touch, clothing, or hygiene.
- In men may cause scrotal or penile pain; in women, vulvar or vaginal pain during intercourse.
- Does not usually awaken the patient at night.
The pain often has two components. A constant background discomfort may be present at rest, while sudden attacks bring sharper, burning, or electric sensations. These flares are frequently triggered by sitting, bowel movements, urination, or physical strain.
Symptoms related to the lesion of the motor fibers of the pudendal nerve — such as bowel or urinary incontinence (sphincter insufficiency) or sexual dysfunction — usually occur only when both pudendal nerves are affected.
Because the pudendal nerve has several branches, symptoms can vary depending on which branch is affected:
- Inferior rectal branch — pain around the anus or during bowel movements.
- Perineal branch — pain in the perineum, worsened by sitting.
- Dorsal genital branch — burning or hypersensitivity in the penis or clitoris, sometimes with discomfort during arousal or orgasm.
Some patients experience urinary urgency or urethral pain (dysuria-like symptoms) when distal branches of the pudendal nerve — particularly the perineal or dorsal genital branch — are affected. At the beginning, many patients believe their symptoms are caused by an infection or urological problem, but all tests usually come back normal. Many other nerve-related pain syndromes can feel as if they originate from internal organs, even though the source is actually a nerve.
Over time, secondary muscle tension, anxiety, and sleep disturbances can aggravate the condition. Because the nerve also carries autonomic fibers, some patients develop urinary or sexual dysfunction.

Image: Male perineum region nerve innervation
Diagnosis of Pudendal Neuralgia
The diagnosis of pudendal neuralgia is primarily clinical. However, because urologic and gynecologic problems manifesting with similar complaints are more frequent, the patient should visit a urologist or a gynecologist first.
Key diagnostic features include:
- Pain located in the sensory territory of the pudendal nerve – genital area, perineum, anus, rectum or urethra.
- Typically worsened the most by sitting, although other activities may also provoke symptoms.
- Altered sensation in a specific region supports the diagnosis and may include numbness or allodynia.
- Pain relief after a pudendal nerve block supports the diagnosis but is not required in every case.
These criteria are not absolute. They serve as practical clinical guidance rather than strict rules, since the presentation of pudendal neuralgia can vary between patients and may overlap with other pelvic pain syndromes.
During examination, the doctor may find a tender spot — either on the skin or through gentle transrectal palpation — near the course of the pudendal nerve. Pressing this area may reproduce pain or tingling that radiates along the regions supplied by the pudendal nerve. It is important to be examined in person or during a video consultation by a specialist who knows the pain anatomy of this region and how to check and treat all of the roughly 20 possible causes of this pain.
Imaging (MRI or CT) is mainly used to exclude other pelvic or spinal causes — such as tumors, vascular malformations, or fractures — rather than to visualize the pudendal nerve itself.
Specialized MRI scans of the pudendal nerve can sometimes show changes in the nerve. However, their overall diagnostic value is limited, and results are often nonspecific or even normal in people with confirmed long-lasting pudendal neuralgia.
Neurophysiological testing is not routinely required. When indicated, tests such as pudendal nerve terminal motor latency (PNTML), EMG of the anal sphincter, or somatosensory evoked potentials (SSEP) can be performed to assess nerve function. These tests are usually done selectively rather than all at once, depending on the specific clinical findings. Results are often within normal limits, especially in cases of partial or intermittent nerve irritation. Clinical examination and patient history usually provide more reliable information for identifying the pain generator.
A diagnostic pudendal nerve block, performed under ultrasound, X-ray, or CT guidance, remains the most specific confirmatory test, although it is not required when the clinical presentation is already clear. The injection of a local anesthetic temporarily numbs the pudendal nerve, stopping the pain and helping to determine whether the pain originates from this nerve or its branches. Pain relief >50% after the block supports the diagnosis, but a single negative result does not rule it out. At least two negative blocks performed by different specialists are usually required before considering alternative diagnoses.
A diagnostic pudendal nerve block is considered positive if the patient experiences temporary pain relief in the typical pudendal distribution after the injection. In some cases, a brief flare-up or increase in the usual pain may follow the block — this does not necessarily mean the test is negative, especially if an initial improvement occurred. Such a reaction can indicate nerve hypersensitivity or central sensitization rather than incorrect targeting.
Apart from its diagnostic role, this block can also have a therapeutic effect — especially when a corticosteroid is added. When diagnostically successful, it typically provides relief for several hours, and with an added corticosteroid, pain reduction often lasts 3–5 weeks. A minority of patients experience longer improvement. About 25% of patients still feel some benefit six months after the injection. This response is most often seen when the irritation is located near the ischial spine or within Alcock’s canal — the area where the medication is injected. This also happens if irritation is not mainly caused by mechanical effects like nerve compression or stretching without influence of muscular spasm and inflammation.
Because symptoms often overlap with urologic, gynecologic, or colorectal disorders, evaluation by a pain specialist or neurosurgeon familiar with pelvic neuroanatomy is essential.
Treatment Options for Pudendal Neuralgia
Effective treatment requires identifying and addressing the exact mechanism of pain rather than relying on a single therapy.
Conservative measures
- Avoid prolonged sitting. When sitting is necessary, use a U-shaped or open-center cushion that off-loads the coccyx and the midline perineal area while maintaining support under the ischial tuberosities and trochanters.
- Modify activities such as cycling or horse riding.
- Address contributing factors — constipation, pelvic floor overuse, or postural asymmetry.
- Usually, 20–30% of patients report improvement with this therapy alone.
Medications
Drugs used for neuropathic pain (gabapentinoids, tricyclic antidepressants, SNRIs) are the mainstay of initial therapy and can reduce nerve hypersensitivity. Short-term use of NSAIDs, muscle relaxants, antihistamines, and, in some cases, corticosteroids may help if local inflammation or pelvic floor spasm is present, which is often the case. Proper combinations of medications that cover sensitized nerve and all possible irritants is very important. Treatment is started with an adequate combination of medications and doses, and these are titrated over several weeks to achieve symptom control. Topical agents such as lidocaine or amitriptyline cream can reduce localized hypersensitivity.
Previous medication failure does not always mean medication cannot help; in many persistent cases, the problem is that the right combination of mechanisms was not treated together.
Physical therapy
Pelvic-floor physical therapy focuses on relaxing overactive pelvic muscles, improving posture, and releasing myofascial tension. The benefit varies between individuals, but it is often most effective when muscle tension or spasm contributes to the pain. Treatment may include manual therapy, stretching, biofeedback, gentle electrical stimulation (TENS), heat therapy, or magnetic field therapy, depending on individual tolerance and findings.
Interventional procedures
Diagnostic and therapeutic nerve blocks (local anesthetic ± corticosteroid) can provide diagnostic confirmation and temporary — or occasionally longer-lasting — pain relief, as described above. In some patients, periodic blocks (usually a monthly block, three times) combined with medication and physical therapy offer sufficient long-term control without the need for invasive procedures.
Pulsed radiofrequency (PRF) of the pudendal nerve may be considered in patients who continue to experience pain even after diagnostic or therapeutic nerve blocks and medication. The procedure is performed under imaging guidance by placing a fine needle electrode very close to the pudendal nerve and delivering short, low-temperature electrical pulses that modulate its activity without causing thermal damage.
During PRF, the electrode remains near the nerve for about eight minutes. The temperature is carefully kept below 42 °C to avoid tissue injury. PRF does not destroy the nerve; instead, it helps to “reset” abnormal pain signaling. It is typically used in selected cases when pain relief from nerve blocks is temporary but confirms that the pudendal nerve is involved. Reported results vary across studies, with meaningful improvement observed in roughly 30–50 % of patients, usually lasting a few months.
The ganglion impar (also called the coccygeal ganglion) is a small sympathetic nerve center located in front of the coccyx (tailbone). PRF of this ganglion is not specific for pudendal neuralgia but can be used in patients with mixed or poorly localized pelvic or perineal pain—especially when discomfort extends beyond the pudendal nerve distribution.
The procedure is usually performed once, and if the effect is positive, it can be repeated after several months when symptoms gradually return.
Peripheral nerve stimulation (PNS) is considered for carefully selected patients who responded well to a diagnostic pudendal nerve block but whose pain keeps returning. Unlike a nerve block or pulsed radiofrequency, which act temporarily, PNS provides continuous, long-term neuromodulation of the nerve.
The stimulation produces a mild tingling (paresthesia) in the same area where pain is usually felt. This sensation overlaps the pain signal and reduces its intensity. Some patients, however, find the paresthesia uncomfortable or distracting, and in such cases, the device can be reprogrammed or removed.
The procedure begins by inserting a thin stimulation lead (a fine insulated wire) near the pudendal nerve — typically at the same anatomical location where a diagnostic nerve block is performed. The lead is placed within a few millimeters of the nerve, without direct contact. The puncture technique is similar to that used for a pudendal nerve block and is performed under fluoroscopic, CT, or ultrasound guidance. In selected cases, the electrode can also be implanted during laparoscopic decompression of the pudendal nerve.
In the first stage, the lead is connected to an external battery and stimulator worn outside the body for several days to test whether pain relief is significant and consistent. If the response is favorable, a small permanent pulse generator (battery) is implanted under the skin—usually in the upper buttock or lower abdominal wall—and connected to the lead by a thin extension wire.
The implanted system delivers gentle electrical impulses that continuously modulate pain signaling in the pudendal nerve and surrounding tissues. When successful, it can provide long-lasting pain relief and improved quality of life. However, this therapy is reserved for rare, treatment-resistant cases of pudendal neuralgia, and only a small percentage of patients are candidates.
Clinical studies report that around 60% of implanted patients experience at least a 50% reduction in pain, with benefits that may remain stable for one to three years.
Surgical Treatment of Pudendal Neuralgia
Surgical decompression of the pudendal nerve is reserved for confirmed entrapment that fails all conservative measures. Today, the laparoscopic transperitoneal approach is the most commonly used surgical method, while transgluteal and transperineal routes are applied in selected cases. The operation aims to release the pudendal nerve along its course in Alcock’s canal and between the pelvic ligaments, and to remove any remaining compressive structures. Because of the complex pelvic anatomy, success rates are modest—around 60–70% when performed in specialized centers—and the procedure is required in less than 10% of patients with pudendal neuralgia. Unlike carpal tunnel surgery, the anatomical variability and multifactorial causes of pain make decompression outcomes less predictable. Symptoms can improve partially immediately after surgery, but additional improvement can occur 6–24 months after surgery.
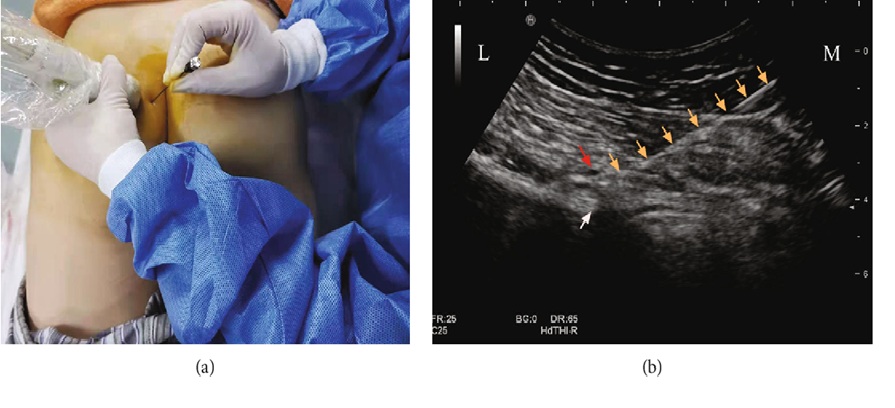
Image: Ultrasound-guided pudendal block. a) performance b) ultrasound image showing needle and target
What to Do If Pudendal Neuralgia Does Not Improve
If pain persists despite medication, physical therapy, or nerve blocks, the key step is not to repeat the same treatments, but to reassess the diagnosis and identify what has been missed.
In many patients, persistent pain is not caused by a single mechanism, but by a combination of factors — such as ongoing nerve irritation, pelvic floor dysfunction, biomechanical stress, or sensitization of the nervous system.
At this stage, the most important questions are:
- Is the pudendal nerve truly the main pain generator?
- Are there additional sources of irritation that have not been addressed?
- Was the treatment strategy complete, or only partial?
In addition, failure to determine which anatomical structure is responsible for the pain, what pathological process is occurring within that structure, and which contributing factors are maintaining the pain is a key reason why symptoms persist despite treatment. A structured re-evaluation — including detailed symptom analysis and targeted functional assessment — often reveals why previous treatments failed and what the next step should be.
Only after this step should further interventions be considered, based on clearly identified mechanisms rather than assumptions. A structured video-based pain assessment can help when previous examinations, MRI scans, medications, or blocks did not explain why pudendal neuralgia pain persists.
Viral-Related Pudendal Neuralgia (Sacral HSV Radiculopathy)
Although pudendal neuralgia is most frequently related to mechanical compression, pelvic floor muscle dysfunction, postoperative scarring, childbirth, or prolonged sitting, in a smaller subset of patients the pain originates from viral irritation of the nerve itself. Herpes simplex virus type 2 (HSV-2), also known as the genital herpes virus, remains latent in the sacral sensory ganglia (S2–S4) — the same anatomical level from which the pudendal nerve originates, whereas pudendal neuralgia caused by herpes zoster (shingles) is extremely rare. When reactivated, the virus can inflame or sensitize the pudendal nerve or its branches, producing burning, hypersensitive, electric, or stabbing pain along the genital, perineal, anal, or urethral region. This can clinically mimic pudendal neuralgia, vulvodynia, or “unexplained pelvic pain.”
Clinical picture (symptoms)
In some patients the pain is constant, with episodic worsening during viral reactivation; in others, pain appears only in recurrent episodes.
Symptoms may include:
- burning, sharp, or electric pain in the vulva, scrotum, perineum, anus, or deep within the pelvis
- urethral pain without infection (sterile dysuria), often described as burning during or after urination
- persistent urethral sensitivity or a constant urge to urinate (false urinary urgency)
- episodic worsening triggered by stress, fatigue, sexual activity, friction, menstrual cycle, or illness
- recurrence of symptoms in the same dermatomal area (S2–S4) each time, suggesting sacral ganglion involvement
Many patients report previous episodes of genital herpes before neuralgia begins, but neuralgia may also occur without visible skin lesions — the virus can reactivate within the ganglion itself (herpes simplex sine herpete). Because urine tests, cultures, and imaging typically remain normal, these patients are often misdiagnosed with chronic UTI, prostatitis, interstitial cystitis, vulvodynia, or pelvic floor dysfunction.
Rash (when present)
The rash appears as small, grouped, painful blisters (vesicles) on red skin or mucosa.
It may occur on: vulva or perineum (women), penile shaft, glans, or scrotum (men), around the anus or at the urethral opening. Urethral mucosal changes are usually not visible; in many patients, no rash is present at all — the virus reactivates in the ganglion (ganglionitis), causing neuropathic pain without skin lesions.
Diagnosis (DG)
Diagnosis is clinical and relies on:
- Dermatomal pain pattern — recurrent focal neuralgia in the S2–S4 pudendal distribution
- PCR from a lesion (if present) — gold standard (CDC)
- Negative urine cultures and normal urologic/gynecologic evaluation, despite persistent urethral/genital pain
- Correlation with triggers or recurrence pattern (stress, intercourse, illness, menstrual cycle)
- Therapeutic trial of antiviral suppression — reduction of symptoms supports HSV as the source (supported by NEJM and CDC guidance)
Serology (HSV IgG) confirms past exposure but does not prove causation. IgM testing has limited diagnostic value and is not recommended for guiding clinical decisions.
Indications for antiviral treatment (suppressive therapy)
Daily antiviral suppression (valacyclovir or acyclovir) is considered when:
- pain episodes clearly recur in the same pudendal dermatome
- there are frequent recurrences (≥ 4 symptomatic outbreaks/year, CDC)
- symptoms correlate with herpes prodrome or triggers
- urethral pain or urinary urgency persists despite normal urine findings
- the clinical picture suggests sacral HSV radiculopathy even when no rash is visible (herpes simplex sine herpete)
Suppressive therapy may reduce frequency and intensity of neuralgic episodes by preventing viral reactivation in the sacral ganglion. Therapeutic trial of antiviral suppression may help confirm the diagnosis when symptoms improve during treatment.
Why this matters
This is one of the very few causes of pudendal neuralgia where treatment can target the cause, not just the symptoms. While mechanical pudendal neuralgia requires decompression or muscle therapy, HSV-related pudendal neuralgia can improve with neuropathic medications plus antiviral suppression.
Many case reports and small series describe HSV-2 sacral radiculopathy presenting with genital/perineal/urethral neuralgic pain; PCR is preferred to confirm active infection. While large trials are lacking, antiviral therapy (episodic or suppressive) has been reported to reduce symptoms or recurrences in selected patients with clinical features suggestive of sacral HSV reactivation. Therefore, testing or a therapeutic trial of suppressive antivirals is reasonable only in a smaller subset of patients with recurrent dermatomal S2–S4 pain, compatible prodromal features, or persistent urethral symptoms despite a normal urologic workup.
Treatment of Pain Contributing Factors in Pudendal Neuralgia
Effective treatment of pudendal neuralgia begins with identifying the primary pain generator — whether the dominant mechanism is pudendal nerve irritation, compression, entrapment, or sensitization along its anatomical course.
However, in many patients, pain persists not only because of the primary nerve problem, but because additional contributing factors are not recognized or adequately addressed. These factors rarely represent the main cause of pain, but they can maintain nerve irritation, increase pain sensitivity, delay recovery, and reduce the effectiveness of otherwise appropriate treatment.
For that reason, successful management requires not only identifying the dominant source of pain, but also understanding the broader mechanical, neurological, and systemic context in which the pain persists.
What contributing factors may play a role in pudendal neuralgia?
- Prolonged sitting and mechanical pressure — long periods of sitting (especially on hard surfaces or cycling) can maintain continuous pressure on the pudendal nerve and worsen symptoms
- Pelvic floor muscle dysfunction — increased muscle tone, spasm, or poor coordination of pelvic floor muscles may compress or irritate the nerve and maintain pain
- Postural and biomechanical factors — pelvic tilt, asymmetry, or altered load distribution (including leg length discrepancy or hip dysfunction) may contribute to persistent irritation along the nerve pathway
- Repetitive strain and daily habits — activities such as cycling, prolonged sitting, or certain exercises may perpetuate symptoms
- Scar tissue and prior procedures — previous surgeries, childbirth trauma, or local interventions may lead to fibrosis or altered tissue mobility around the nerve
- Central sensitization — over time, the nervous system may amplify pain signals, so that symptoms persist even when the original irritation is reduced
- Sleep disturbance and pain cycle — poor sleep increases pain perception and reduces recovery capacity
- Stress and increased muscle tone — stress does not cause the pain, but increases pelvic floor tension and nervous system reactivity, helping maintain symptoms
- Metabolic factors, pro-inflammatory state and low-grade inflammation — obesity, insulin resistance, and chronic inflammation may increase nerve sensitivity and impair recovery
- Nutritional deficiencies — low levels of vitamin B12, vitamin D, magnesium, or iron may affect nerve function and healing
- Vitamin-related factors — both deficiency and excess of vitamin B6 may contribute to burning pain, tingling, or hypersensitivity
- Medications and previous treatments — repeated ineffective treatments or long-term use of certain medications may alter pain perception without resolving the underlying mechanism
- Other medical conditions and comorbidities — diabetes, hormonal factors, autoimmune diseases, and chronic inflammatory conditions may increase nerve vulnerability and reduce treatment response
- Physical inactivity and deconditioning — reduced activity due to pain may worsen muscle imbalance and increase overall sensitivity
Why this matters in practice
In many cases, treatment fails because the primary pain generator is not correctly identified, or therapy is directed only at one part of the problem — most often medications alone or a single presumed anatomical cause. Conversely, even when the main cause is recognized, failure to address contributing factors often leads to only partial or temporary improvement.
The most effective approach is a carefully selected combination of treatment that addresses both the dominant pain source and all relevant contributing factors. An incomplete approach — even when it includes individually effective methods — is one of the most common reasons why pudendal neuralgia becomes persistent.
In practice, many patients try to address parts of this problem on their own — through posture correction, pelvic floor exercises, cushions for sitting, supplements, or different medications. While these approaches may provide partial relief, they rarely lead to lasting improvement if the primary pain generator is not clearly identified and treated. On the other hand, even well-targeted medical treatment may fail if contributing factors are not recognized and corrected.
Many patients recognize that they have already tried one part of this approach — but not the complete strategy. This is one of the most common reasons why pudendal neuralgia becomes chronic.
Prognosis in Pudendal Neuralgia
Prognosis depends on how early the diagnosis is made and whether the underlying cause—such as compression or irritation—can be corrected. When treated promptly, many patients experience partial or complete pain relief.
Chronic untreated cases may become centrally sensitized, making therapy more difficult and recovery slower. Even in persistent cases, symptom control and quality of life can often be significantly improved through a personalized, multimodal treatment plan. In many patients with long-lasting pain, previous therapies were unsuccessful simply because the true cause was never identified, or because multiple mechanisms of pudendal nerve irritation were not addressed together with an adequate combination of medications, carefully adjusted over a period of six to eight weeks. (Pudendal neuralgia is not always caused only by mechanical compression of a sensitized nerve; other sources of nerve irritation should also be considered.)
When conservative measures and pudendal nerve blocks fail, interventional procedures such as pulsed radiofrequency (PRF), peripheral nerve stimulation (PNS), or surgical decompression may be considered. These techniques are performed only in very carefully selected patients with a clearly confirmed pain generator and after a positive response to diagnostic blocks.
Even in such cases, pain reduction varies widely—typically between 30% and 70%—and complete recovery is uncommon. The overall prognosis depends on the duration of symptoms, the underlying cause, and how the patient responds to earlier treatments.
Why an Online Consultation Can Help When Pudendal Neuralgia Pain Persists
A video consultation for pudendal neuralgia can help identify the exact source of your pain — one or more pain generators — as well as the factors that trigger and maintain it. This is achieved through a detailed conversation, review of your MRI scans and medical records, and specific movements or finger-pressure tests you perform during the session, which may increase, reduce, or change your pain. Many of these pain generators and sustaining factors cannot be seen on MRI.
This may sound like examinations you have already had. It is not — because what matters most is not the test itself, but who interprets it. Only a specialist with deep knowledge of pain anatomy in this region knows which questions to ask, where to instruct you to press, which movements to test, and how to confirm which pain source is active. This is not just another opinion.
You will also receive advice on which additional factors that trigger and sustain pain should be investigated — such as hormonal factors, vitamin deficiencies, side effects of other medications, inadequate diet, metabolic disorders, physical strain during daily activities or work, and other overlooked contributors. In many patients who have already visited several specialists, these factors have still not been fully investigated.
Once the main pain mechanism behind pudendal neuralgia symptoms is identified, treatment follows: a targeted combination of medications covering all identified mechanisms, carefully introduced and adjusted over 6–8 weeks, with regular communication during the treatment period, especially when you need it. The aim is to achieve early pain reduction during the first 10 days, then stabilize the result over the following weeks for a longer-lasting effect. When selecting medications, we take into account whether patients are older or have other health conditions, and we prescribe them in a safe combination for the shortest possible duration to avoid medication overload. All recommendations are explained during the conversation and are also given in a written medical report.
Many patients assume that because medications have already failed, a specific procedure is now needed. In most cases, this is not true — previous medications often did not cover the right combination of mechanisms, were not individualized, or were not adjusted over a sufficient period of time. In the minority of patients where medication alone is not sufficient, we recommend the exact intervention or procedure — chosen based on the confirmed pain generator, not assumptions.
Based on our written medical report, reimbursement may often be possible if your insurance plan allows it.
Pudendal Neuralgia & Persistent Pelvic Pain — Start Your Telehealth Consultation
If you have long-lasting pelvic, perineal, genital, or anal pain — or a confirmed diagnosis of pudendal neuralgia — a detailed telehealth consultation helps identify the likely pain generator (pudendal nerve or another pelvic nerve) and plan the next diagnostic or therapeutic steps.
- ✔ Send a short message describing your symptoms and prior treatments
- ✔ You’ll receive a reply within 24 hours with details on whether and how we can help, including consultation cost and scheduling
- ✔ Only then, you can send your medical documentation (reports, imaging)
- ✔ The video consultation is followed by a written plan and free follow-up questions for 10 days
- ✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Consultation fees typically range from $180–250, depending on case complexity.
Based on our medical report, reimbursement can often be obtained (if your insurance plan allows it).
This reflects the usual international range for specialist telehealth consultations. A session helps clarify the cause of perineal pain and whether targeted medication, nerve blocks, neuromodulation, or other options are appropriate.
Differential Diagnosis of Perineal Pain and Pudendal Neuralgia
Pain in the perineal or genital area can originate from many other sources:
- Chronic prostatitis
- Chronic pelvic pain syndrome (CPPS).
- Interstitial cystitis or bladder pain syndrome.
- Vulvodynia or vestibulodynia.
- Myofascial pain of the pelvic floor muscles.
- Sacral radiculopathy (L5–S2 roots).
- Hemorrhoidal, anal, or rectal disorders.
Accurate differentiation prevents unnecessary treatments and helps target the correct pain generator.
Related Nerves That Can Mimic Pudendal Neuralgia
Neuropathic pain in the pelvis does not always originate from the pudendal nerve. Several nearby nerves may produce overlapping symptoms.
| Nerve (Nerve roots origin) | Typical Pain Distribution | Distinguishing Features / Clinical Clues |
|---|---|---|
| Pudendal nerve (S2–S4) | Perineum, genitals, anus | Pain worsens when sitting; sparing of gluteal and posterior thigh; often burning or electric in nature. |
| Coccygeal nerves (S4–Co1) | Tip of tail-bone, lower sacrum, anus | Pain localized to the coccyx (tailbone), aggravated by sitting and sometimes by leaning back; the condition is referred to as coccygodynia. |
| Ganglion impar | Midline perineal, anal, or coccygeal pain | Symmetrical midline pain, often deep or visceral; responds to ganglion impar block. |
| Posterior femoral cutaneous nerve (S1–S3) | Posterior thigh, sometimes gluteal fold | Pain extends downward to thigh; less genital involvement; tenderness over ischial tuberosity. |
| Ilioinguinal nerve (L1) | Upper medial thigh, mons pubis, upper scrotum/labia | Pain above inguinal ligament; often post-surgical (hernia, appendectomy, C-section). |
| Genitofemoral nerve (L1–L2) | Groin, upper anterior thigh, genital area | Pain more anterior; worsened by hip extension; hypoesthesia on upper inner thigh. |
| Inferior cluneal nerves | Inferior buttock, near ischial tuberosity | Pain near sitting area but without perineal sensory loss; often after prolonged sitting or local trauma. |
| Anterior cutaneous branches of obturator nerve | Medial thigh, perineal edge | Pain provoked by leg adduction or hip movement; sometimes after pelvic trauma or surgery. |
| Pelvic splanchnic nerves / hypogastric plexus | Deep pelvic, bladder, rectal pain | Visceral, dull, deep pain; may accompany urinary urgency or bowel symptoms; responds to plexus block. |
Clinical tip: Allodynia in the upper third of the vulva usually suggests ilioinguinal or genitofemoral origin, while involvement of the lower two-thirds, the perineum, or the posterior part of the labia and scrotum indicates a pudendal distribution. Pain radiating into the penis, urethra, or distal vagina also supports pudendal nerve involvement. Midline perineal or coccygeal pain should raise suspicion of ganglion impar or coccygeal nerve irritation. Rarely, posterior femoral cutaneous nerve branches may contribute to pain near the ischial or lower gluteal region. Careful sensory mapping across these territories helps identify the true pain generator.

Image: Female perineal region nerve innervation..
Multidisciplinary Approach in Treatment of Pudendal Neuralgia
Combining medication, targeted physiotherapy, interventional blocks, and psychological support yields the best outcomes. Coordination between neurologists, neurosurgeons, urologists, and pain specialists is often required.
Before contacting us, please read our Privacy Policy and Terms of Use.
Online pain consultation in detail for pudendal neuralgia
Schematic explanation of the video consultation in pudendal neuralgia
Answers to questions about the process and success of video consultations for pudendal neuralgia
See the page “Possible Reasons for Poor Pain Treatment Effectiveness in Pudendal Neuralgia ” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
FAQs About Pudendal Neuralgia
What is pudendal neuralgia?
Pudendal neuralgia is a chronic nerve pain condition involving the pudendal nerve, which supplies sensation to the perineum, genitals, anus, rectum, and parts of the urethral region. The pain is often described as burning, stabbing, electric, pressure-like, or hypersensitive. A typical feature is that symptoms worsen while sitting and improve when standing, lying down, or sitting on the toilet. Pudendal neuralgia may result from compression, stretching, inflammation, pelvic floor muscle spasm, surgical or childbirth-related injury, metabolic neuropathy, or rarely viral irritation affecting the sacral nerve roots.
What are the main causes of pudendal neuralgia?
Pudendal neuralgia can be caused by irritation, compression, stretching, or injury of the pudendal nerve or one of its branches. Common mechanisms include compression in Alcock’s canal, irritation near the sacrospinous and sacrotuberous ligaments, pelvic floor muscle spasm, prolonged sitting, cycling, childbirth-related stretch injury, pelvic or gynecologic surgery, postoperative scarring, local inflammation, diabetes-related neuropathy, or inflammatory neuritis. In a smaller subset of patients, HSV-2 sacral radiculopathy can mimic pudendal neuralgia. Often, more than one mechanism is present, which is why diagnosis and treatment can be difficult.
What are the typical symptoms of pudendal neuralgia?
Typical symptoms include burning, stabbing, electric, tingling, pressure-like, or hypersensitive pain in the perineum, genitals, anus, rectum, urethra, penis, scrotum, vulva, or vagina. Pain usually worsens the most while sitting and often improves when standing, lying down, or sitting on the toilet. Some patients also have numbness, allodynia, urinary urgency, urethral burning, sexual discomfort, pain during bowel movements, or flares triggered by physical strain. Symptoms vary depending on which branch of the pudendal nerve is affected and whether pelvic floor muscle tension or other pain generators are also present.
Why does pudendal neuralgia treatment sometimes fail?
Pudendal neuralgia treatment often fails because only one presumed cause is treated while other pain-maintaining factors are missed. A patient may receive neuropathic medication, pelvic floor therapy, or a nerve block, but pain can persist if the true pain generator has not been confirmed or if several mechanisms coexist. Ongoing nerve compression, pelvic floor spasm, scar tissue, mechanical sitting pressure, inflammation, central sensitization, metabolic factors, or another pelvic nerve can all maintain symptoms. In many persistent cases, the problem is not that every treatment was wrong, but that the treatment strategy was incomplete.
What should be reassessed if pudendal neuralgia does not improve?
If pudendal neuralgia does not improve, the first step is to reassess the diagnosis and identify what may have been missed. The key questions are whether the pudendal nerve is truly the main pain generator, whether another pelvic nerve or spinal root is involved, whether pelvic floor dysfunction is maintaining symptoms, and whether previous treatment addressed all contributing factors. Repeating the same medication, physical therapy, or injection without this reassessment often leads to temporary or no improvement. A structured review of pain location, triggers, sitting tolerance, sensory changes, prior blocks, and response to treatment is usually more useful than simply adding another procedure.
How is pudendal neuralgia diagnosed?
Pudendal neuralgia is diagnosed primarily by clinical evaluation. The diagnosis is based on pain location, sitting-related worsening, sensory symptoms, exclusion of more common urologic, gynecologic, colorectal, or spinal causes, and sometimes response to a pudendal nerve block. Imaging may help exclude tumors, fractures, vascular malformations, or spinal disorders, but it often does not show the pudendal nerve abnormality directly. A careful examination may identify tenderness along the course of the nerve or reproduce pain in the pudendal distribution. In many cases, history and symptom mapping are more useful than imaging alone.
What imaging tests help in pudendal neuralgia?
MRI or CT may help in pudendal neuralgia mainly by excluding other causes of pelvic, genital, rectal, or perineal pain. Imaging can detect tumors, fractures, pelvic masses, vascular abnormalities, postoperative changes, or spinal pathology that may mimic pudendal nerve pain. Dedicated pudendal nerve MRI or MR neurography can sometimes show nerve thickening, signal change, or surrounding scar tissue, but results are often normal or nonspecific even in patients with real pudendal neuralgia. For this reason, imaging should be interpreted together with symptoms, examination, and response to diagnostic procedures.
Which conditions can mimic pudendal neuralgia?
Several conditions can mimic pudendal neuralgia, which is why differential diagnosis is essential. These include chronic prostatitis, chronic pelvic pain syndrome, interstitial cystitis or bladder pain syndrome, vulvodynia, pelvic floor myofascial pain, sacral radiculopathy, hemorrhoidal or rectal disorders, coccygeal nerve pain, ganglion impar pain, ilioinguinal neuralgia, genitofemoral neuralgia, and posterior femoral cutaneous nerve irritation. The correct diagnosis depends on pain location, sitting pattern, sensory mapping, urinary or bowel symptoms, neurological findings, and response to targeted blocks. Treating the wrong pain generator is a common reason for persistent symptoms.
Can pudendal neuralgia cause urinary or sexual problems?
Yes, pudendal neuralgia can cause urinary or sexual symptoms, especially when distal branches of the pudendal nerve are affected or when pelvic floor dysfunction is present. Patients may describe urethral burning, urinary urgency, pain after urination, genital hypersensitivity, pain during intercourse, discomfort during arousal or orgasm, penile pain, scrotal pain, vulvar burning, or vaginal pain. These symptoms often lead patients first to urologists or gynecologists. When urine tests, cultures, and standard examinations are normal, a nerve-related pelvic pain source should be considered, especially if symptoms worsen with sitting.
Can pudendal neuralgia affect men and women differently?
Yes, pudendal neuralgia can affect men and women differently because the sensory distribution of the pudendal nerve involves different genital structures. In men, symptoms may include penile pain, scrotal pain, perineal burning, urethral discomfort, pain after ejaculation, or rectal pain. In women, symptoms may include vulvar burning, vaginal pain, clitoral hypersensitivity, pain during intercourse, perineal discomfort, or rectal pain. Childbirth-related stretch injury and pelvic surgery are important risk factors in women. Despite these differences, the core pattern is similar: nerve-type pain in the pudendal distribution, usually worse with sitting.
What is a pudendal nerve block?
A pudendal nerve block is an image-guided injection of local anesthetic, sometimes combined with corticosteroid, around the pudendal nerve. It is usually performed under ultrasound, CT, or fluoroscopic guidance. The block can help confirm whether the pudendal nerve is the main pain generator if it produces temporary relief in the typical pain distribution. It may also provide therapeutic benefit, especially when inflammation or local irritation contributes to symptoms. Relief may last only a few hours after anesthetic alone, but with steroid it may last several weeks in selected patients.
Can a pudendal nerve block cure pudendal neuralgia?
A pudendal nerve block usually does not cure pudendal neuralgia, but it can reduce pain and help confirm the diagnosis. Some patients experience meaningful relief for several weeks, especially when inflammation, muscle spasm, or localized irritation near the injection site is important. A smaller group may have longer improvement, particularly when the block is combined with medication, physical unloading, and correction of contributing factors. However, if the nerve is mechanically compressed, repeatedly irritated, or if central sensitization is established, the effect of a block may be temporary or incomplete.
What happens if a pudendal nerve block does not help?
If a pudendal nerve block does not help, the diagnosis should be reassessed, but one negative block does not always rule out pudendal neuralgia. The block may have missed the nerve, the irritated branch may be distal to the injection site, or another pain generator may be more important. Sometimes pain briefly worsens after injection because of nerve hypersensitivity or central sensitization. If symptoms strongly suggest pudendal neuralgia, a second image-guided block by an experienced specialist may be reasonable. If repeated well-performed blocks are negative, other causes of pelvic pain should be investigated.
How is pudendal neuralgia treated?
Pudendal neuralgia is treated by identifying the dominant pain generator and correcting the factors that continue to irritate the nerve. Treatment usually begins with sitting modification, reduction of mechanical pressure, pelvic floor relaxation, neuropathic pain medications, and management of inflammation or muscle spasm when present. Physical therapy can help when pelvic floor overactivity contributes to symptoms. Image-guided nerve blocks may be used diagnostically and therapeutically. More advanced procedures such as pulsed radiofrequency, peripheral nerve stimulation, or surgical decompression are reserved for selected patients with persistent symptoms and a clearer pain mechanism.
Which medications help in pudendal neuralgia?
Medications for pudendal neuralgia usually target neuropathic pain, inflammation, muscle spasm, and nerve hypersensitivity. Common options include gabapentinoids, tricyclic antidepressants, and SNRIs. In selected patients, short-term NSAIDs, muscle relaxants, antihistamines, or corticosteroids may help if inflammation or pelvic floor spasm contributes to symptoms. Topical lidocaine or compounded creams may reduce localized hypersensitivity. The main point is that one medication alone is often insufficient. Many persistent cases require a carefully selected combination of treatments, titrated over several weeks, based on the specific mechanisms maintaining pain.
Can physical therapy improve pudendal neuralgia?
Yes, physical therapy can improve pudendal neuralgia when pelvic floor muscle tension, spasm, poor coordination, postural overload, or myofascial pain contributes to nerve irritation. The goal is usually relaxation and unloading, not aggressive strengthening. Treatment may include pelvic floor release, posture correction, stretching, biofeedback, gentle manual therapy, TENS, heat, or other modalities depending on tolerance. Physical therapy can be less effective or even aggravating if the wrong exercises are used or if the dominant pain generator is not pelvic floor dysfunction. It should be part of a targeted plan, not a generic exercise program.
What is pulsed radiofrequency treatment for pudendal neuralgia?
Pulsed radiofrequency is an image-guided procedure that uses short, low-temperature electrical pulses to modulate abnormal pain signaling in the pudendal nerve. It does not destroy the nerve and is different from destructive thermal radiofrequency. The procedure is considered in selected patients who had temporary benefit from pudendal nerve blocks but whose pain keeps returning. Results vary, and improvement is usually partial and temporary, often lasting a few months. PRF is most reasonable when the pudendal nerve has been confirmed as an important pain generator and conservative treatment has not provided enough control.
What is peripheral nerve stimulation for pudendal neuralgia?
Peripheral nerve stimulation is a neuromodulation treatment for rare, treatment-resistant cases of pudendal neuralgia. A thin stimulation lead is placed near the pudendal nerve, usually at a location similar to where a diagnostic nerve block is performed. A temporary trial is done first to see whether stimulation meaningfully reduces pain. If the response is good, a permanent pulse generator can be implanted under the skin. PNS does not cure the cause of nerve irritation, but it can reduce pain signaling and improve quality of life in carefully selected patients who respond to testing.
Is surgery ever needed for pudendal neuralgia?
Surgery is rarely needed for pudendal neuralgia and should be reserved for carefully selected patients with suspected or confirmed nerve entrapment who have not improved with conservative, medication-based, physical therapy, and interventional treatments. Pudendal nerve decompression aims to release the nerve along areas such as Alcock’s canal or between pelvic ligaments. Outcomes are less predictable than in simpler entrapment syndromes because pelvic anatomy is complex and pain is often multifactorial. Surgery is usually considered only when the pain generator is clear and the expected benefit outweighs the risk.
What is the prognosis for pudendal neuralgia?
The prognosis for pudendal neuralgia depends on how early the diagnosis is made, whether the true pain generator is identified, and whether all contributing factors are treated. Many patients improve significantly when nerve irritation, pelvic floor dysfunction, sitting pressure, inflammation, or sensitization are addressed together. Long-standing untreated pain can become centrally sensitized, making recovery slower and less complete. Even then, meaningful symptom control is often possible with a personalized multimodal plan. Complete cure is not guaranteed, but improved sitting tolerance, reduced flares, and better quality of life are realistic goals in many patients.
How can I sit without worsening pudendal neuralgia?
Sitting should reduce direct pressure on the perineum and pudendal nerve pathway. Many patients benefit from a U-shaped or open-center cushion that unloads the coccyx and midline perineal area while supporting the ischial tuberosities and thighs. Very soft cushions can sometimes worsen symptoms by increasing pressure around the pelvis, while hard surfaces often aggravate pain directly. Frequent position changes, standing breaks, avoiding cycling or prolonged sitting, and correcting posture may help. Cushion choice is individual, and the goal is mechanical unloading rather than simply adding padding.
Can genital herpes cause pudendal neuralgia or urethral pain?
Yes, in a smaller subset of patients, HSV-2 can irritate the sacral sensory ganglia and mimic pudendal neuralgia. This may cause recurrent burning, electric, stabbing, or hypersensitive pain in the genital, perineal, anal, or urethral region. Visible blisters may be absent, because the virus can reactivate within the ganglion without obvious skin lesions. Patients may have normal urine tests and normal urologic or gynecologic evaluation despite persistent urethral or genital burning. HSV-related neuralgia should be considered mainly when pain recurs in the same S2–S4 distribution or follows typical herpes triggers.
When should antiviral suppression be considered for suspected HSV-related pudendal neuralgia?
Antiviral suppression may be considered when symptoms suggest sacral HSV-related neuralgia rather than ordinary mechanical pudendal nerve irritation. This is more likely when burning genital, urethral, perineal, or anal pain recurs in the same S2–S4 region, episodes follow typical triggers such as stress, illness, intercourse, or menstruation, there is a history of genital herpes, or urine and urologic tests remain normal despite repeated symptoms. PCR from an active lesion is the best confirmation when lesions are present. Improvement during suppressive therapy may support the diagnosis, but antiviral treatment is not indicated for every patient with pudendal neuralgia.
Can telehealth help with pudendal neuralgia diagnosis and treatment?
Yes, telehealth can help in pudendal neuralgia when the consultation is performed by a specialist familiar with pelvic pain neuroanatomy. A video consultation can review the pain pattern, sitting triggers, genital, perineal, rectal, urethral, or pelvic distribution, previous tests, medication response, physical therapy response, and results of nerve blocks. Pain mapping and detailed history often clarify whether the pudendal nerve, another pelvic nerve, pelvic floor dysfunction, or spinal root irritation is more likely. Telehealth cannot replace every examination or procedure, but it can guide the next diagnostic and therapeutic steps.
Is pudendal neuralgia a lifelong condition?
Pudendal neuralgia is not necessarily lifelong. Many patients improve when the true pain generator is identified and the treatment plan addresses all relevant mechanisms, including nerve irritation, pelvic floor dysfunction, mechanical pressure, inflammation, sensitization, and contributing systemic factors. Recovery is usually slower when symptoms have been present for a long time or when central sensitization has developed. Some patients achieve major improvement, while others need long-term symptom control strategies. The key is not to repeat ineffective treatment indefinitely, but to reassess why pain persists and tailor treatment to the actual mechanism.
Can I get reimbursed by my health insurance for this consultation?
Reimbursement depends on your individual insurance plan, country, and type of coverage. We do not bill insurance companies directly, but many patients with out-of-network or international consultation benefits may submit the documentation themselves. After the consultation, we can provide a formal medical report and a detailed invoice containing the clinical information typically required for reimbursement claims. Approval is always decided by the insurance provider. Patients should check in advance whether their plan covers specialist telehealth consultations, second opinions, or international medical reviews.
Related topics about pudendal neuralgia – Neurosurgery and Pain Treatment
Treatment of complex cases of pain in pudendal neuralgia can be analyzed by artificial intelligence (AI)
Similar neuropathic pain is trigeminal neuralgia
Additional Information on Pudendal Neuralgia
For those who wish to learn more about pudendal neuralgia, its diagnostic process, and available treatments, the following trusted sources provide reliable and up-to-date information:
- Cleveland Clinic — Pudendal Neuralgia: Causes, Symptoms & Treatment
A clear and patient-oriented overview of the condition, including typical symptoms, risk factors, and conservative management options. - StatPearls (NCBI Bookshelf) — Pudendal Neuralgia
A professional reference covering anatomy, diagnostic criteria, and both non-surgical and interventional treatment strategies. - NHS UK — Pudendal Neuralgia
Guidance for patients and caregivers on recognizing symptoms, when to seek medical advice, and how pain is managed in clinical practice. - Pelvic Pain Foundation of Australia — Pain Where You Sit
Describes practical aspects of daily living with pudendal neuralgia, including ergonomic adjustments and cushion use.