Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: January 17, 2026
Who is this page for?
This page is intended for patients and families who want clear, evidence-based information about epilepsy surgery—when it is considered for drug-resistant epilepsy, how candidates are evaluated, and what procedures (e.g., temporal lobectomy, selective mesial resection, laser ablation, neurostimulation), outcomes, and risks to expect. It is not a substitute for medical advice. For an expert review of your case, see our page on neurosurgery second opinion .
Epilepsy Surgery — Quick Summary (Read This First)
- Most people with epilepsy never need surgery. About 70–75% achieve good seizure control with medication alone.
- Surgery is considered for drug-resistant epilepsy. If seizures persist despite adequate trials of two appropriate medications, further drug changes rarely lead to seizure freedom.
- Epileptic seizures arise from cortical networks. Surgery targets a specific area of the cerebral cortex where seizures begin, even when deeper structures participate in seizure spread.
- Careful presurgical evaluation is essential. MRI, EEG, video-EEG monitoring, and sometimes invasive recordings are used to localize the epileptogenic zone and assess surgical safety.
- Surgery is not “experimental” or a last resort. In properly selected patients, epilepsy surgery is an evidence-based treatment with long-term seizure freedom in 50–80%, depending on the epilepsy type.
- Temporal lobe epilepsy has the best outcomes. Procedures such as anterior temporal lobectomy or selective mesial resection achieve seizure freedom in the majority of suitable patients.
- Not all epilepsy surgeries involve large operations. Minimally invasive options (laser ablation, SEEG-guided thermocoagulation, neurostimulation) may be appropriate in selected cases.
- Secondary (structural) epilepsies often have a surgically treatable cause. In many patients, seizures are triggered by a well-defined lesion that irritates the cerebral cortex — such as a cortical scar after trauma or stroke, cavernous malformation, arteriovenous malformation (AVM), low-grade tumor, focal cortical dysplasia, or post-infectious gliosis. When this epileptogenic lesion can be identified and safely removed, surgery may eliminate seizures rather than only suppressing them with medication.
- The goal is more than seizure reduction. Successful surgery aims to improve quality of life, reduce medication burden, and allow long-term neurological stability.
- Use the Contents box to jump directly to sections on candidacy, diagnostic work-up, specific procedures, risks, outcomes, or recovery.
Most readers only need this summary and the sections on When Surgery Is Considered and Main Surgical Procedures. The remaining sections are available for deeper understanding and specific clinical questions.
Epilepsy affects about 1 % of the general population, making it one of the most frequent chronic neurological disorders worldwide. Most patients with epilepsy never need surgery — but for some, it can offer complete seizure control.
Overall distribution among all people with epilepsy:
• Around 70–75 % achieve long-term seizure control with medication.
• The remaining 25–30 % develop drug-resistant epilepsy (DRE) — seizures that persist despite two or more appropriate anti-seizure drugs.
Within the DRE group (25–30 % of all patients):
• Only 5–10 % of them (≈ 1.5–3 % of everyone with epilepsy) eventually regain full control with further medication adjustments.
• About 25–50 % of DRE patients (≈ 7–15 % of all people with epilepsy) are potential candidates for surgical treatment after detailed presurgical evaluation to locate and assess the epileptogenic zone.
What Is Epilepsy?
Epilepsy is not a single disease but a group of disorders caused by recurrent bursts of abnormal electrical activity within the cerebral cortex — the brain’s outer layer responsible for awareness, movement, and sensation.
These abnormal discharges disrupt normal communication between neurons and lead to epileptic seizures, which vary widely depending on where in the cortex the activity begins and how far it spreads.
In some people, seizures appear as brief lapses of awareness or staring episodes (absence seizures), while in others they cause sudden loss of consciousness and convulsions involving the entire body (generalized tonic–clonic seizures). Seizures usually last from a few seconds to a few minutes and are often followed by tiredness, confusion, or short-term weakness.
Doctors classify seizures based on their site of origin and pattern of spread:
• Focal seizures – start in a limited region of the cerebral cortex and may affect only one side or one function (for example, movement, speech, or vision).
• Generalized seizures – involve both hemispheres of the brain from the very beginning, causing loss of consciousness and bilateral movements.
• Unknown onset – used when the exact cortical origin of the seizure cannot be determined from available data.
Identifying the cortical focus — the area where seizures start — is essential, because in selected patients it can later be treated surgically to reduce or completely eliminate attacks.
Epileptic seizures are generated by cortical networks (gray matter), even when deep structures participate in propagation. Subcortical structures such as the thalamus, basal ganglia, and brainstem cannot initiate seizures, although they can modulate or spread the activity once it begins. Epilepsy therefore occurs when cortical neurons become hyperexcitable and hypersynchronized, forming a network capable of producing spontaneous, recurrent discharges.
Epilepsy is defined as a lasting predisposition to generate unprovoked seizures, typically diagnosed when a person has at least two unprovoked seizures occurring more than 24 hours apart, or one unprovoked seizure with a high (≥60%) likelihood of recurrence over the next 10 years. By contrast, seizures that appear only during a temporary disturbance — for example trauma, infection, metabolic imbalance, or ischemia — are called acute symptomatic seizures and do not in themselves constitute epilepsy.
Historically, epilepsies were divided into three main groups: idiopathic, symptomatic, and cryptogenic.
Idiopathic (or primary) epilepsies referred to cases without visible brain lesions, presumed to have a genetic background and usually starting in childhood.
Symptomatic epilepsies were those secondary to a known brain disorder such as traumatic brain injury, ischemic or hemorrhagic stroke, brain tumors, cortical malformations, vascular malformations (including cavernomas and arteriovenous malformations), prior neurosurgical injury, or central nervous system infection.
Cryptogenic epilepsies were clinically similar to symptomatic forms, but the cause remained undetected despite extensive testing.
This simple classification served clinicians for decades and is still used informally because it directly reflects whether a structural lesion can be found and treated. With the progress of MRI and other diagnostic techniques, many cases previously labeled as “idiopathic” or “cryptogenic” were later shown to have subtle cortical scars, malformations, or other structural causes — effectively reclassifying them as symptomatic epilepsies.
Modern understanding of epilepsy, however, is based on the framework proposed by the International League Against Epilepsy (ILAE).
According to this model, causes of epilepsy are grouped into six categories that may overlap in a single patient. Population studies suggest that structural causes account for about 60–70 % of adult cases, genetic forms for 10–15 %, infectious for 5–10 %, metabolic and immune together for about 5–8 %, while unknown (cryptogenic) etiologies represent roughly 10–15 %.
Structural causes include permanent or evolving lesions of the cerebral cortex that form an epileptogenic network. Typical examples are cortical contusion, scarring after trauma or stroke, chronic subdural hematoma, cortical malformations, brain tumors, cavernoma or arteriovenous malformations. Seizures can also appear while such lesions are still evolving, for instance during the acute phase of head injury or stroke, but these are considered acute symptomatic seizures rather than epilepsy. When a stable cortical lesion continues to generate recurrent seizures, the condition is classified as structural epilepsy. Structural etiologies are the most common in adults and often suitable for surgical treatment if a discrete cortical focus can be identified.
Genetic causes involve pathogenic variants in genes that regulate neuronal excitability or synaptic transmission. They usually appear in childhood or adolescence and may occur without visible lesions on MRI, as in Dravet syndrome, Lennox–Gastaut syndrome, or idiopathic generalized epilepsies. In many cases, these epilepsies are part of broader hereditary or neurodevelopmental syndromes, where seizures represent only one of several neurological manifestations.
Infectious causes include active or previous infections of the central nervous system that involve the cortex, such as encephalitis, meningitis, brain abscess, or neurocysticercosis. Seizures may occur during the acute infection, which are then classified as acute symptomatic, or later, when residual cortical scarring persists and acts as a focus of structural epilepsy.
Metabolic causes result from systemic or inherited disorders that transiently disturb cortical excitability — for example hypoglycemia, hyponatremia, hepatic or uremic encephalopathy, mitochondrial disease, or vitamin B6 deficiency. Seizures occurring only during the acute imbalance are acute symptomatic, whereas epilepsy develops only if repeated or severe disturbances cause permanent cortical injury.
Immune causes refer to autoimmune or paraneoplastic inflammation directly involving the cortex, such as anti-NMDA, LGI1, CASPR2, or GAD65 encephalitis. During the active inflammatory phase, seizures reflect acute cortical irritation, but over time, this process may lead to localized neuronal loss, gliosis, and the formation of a stable epileptogenic focus — resulting in persistent immune-mediated epilepsy.
Unknown or cryptogenic epilepsies are diagnosed when no definite cause is found despite detailed MRI, EEG, and laboratory evaluation. Many such cases are later reclassified as genetic or structural once new diagnostic information becomes available.
From a neurosurgical standpoint, a complementary and very practical classification is used based on the location of the epileptogenic focus.
The main clinical types are temporal lobe epilepsy (≈60–70 %), frontal lobe epilepsy (≈20 %), parietal lobe epilepsy (≈5–10 %), and occipital lobe epilepsy (≈3–5 %), while multifocal or generalized forms account for less than 5 % of surgical candidates.
This anatomic classification is crucial for surgical planning because localization — rather than etiology — determines whether the epileptogenic cortex can be safely removed or disconnected.
In surgical series, about 70–80 % of candidates for epilepsy surgery have a structural cortical lesion such as hippocampal sclerosis, scar, or low-grade tumor, while purely genetic or metabolic forms are rarely operable.
In summary, all epileptic activity originates in the cerebral cortex. Subcortical structures may influence or propagate this activity but cannot generate seizures independently. Seizures provoked by acute cortical irritation are temporary and classified as acute symptomatic, whereas recurrent seizures arising from a stable cortical lesion or enduring hyperexcitability define true epilepsy.
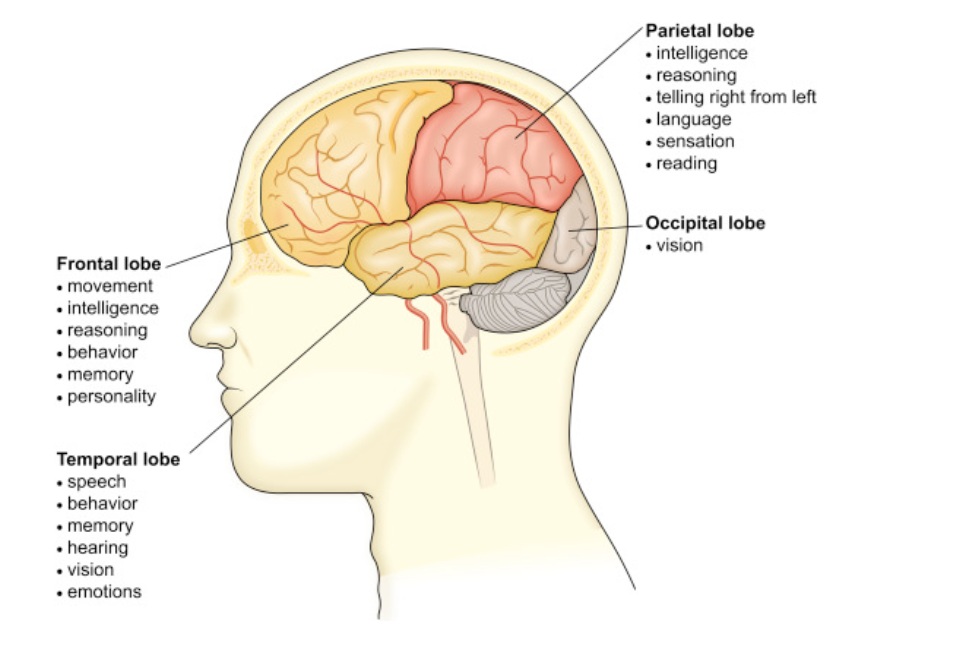
Image: Anatomy of the brain: 4 brain lobes and their functions.
Clinical Forms of Epilepsy
Clinically, epilepsies are divided according to how seizures begin and spread within the brain. In the current ILAE terminology, seizures are described as focal, generalized, or unknown onset, with additional motor or non-motor subtypes. Older names such as Jacksonian epilepsy, temporal lobe epilepsy, petit mal, or grand mal remain widely used in clinical language because they accurately describe recognizable patterns that correspond to specific cortical networks.
In this section we describe the most frequent clinical forms of epilepsy, which together account for over 90 % of all patients seen in general and adult neurology practice.
Congenital or syndromic epilepsies such as Lennox–Gastaut, Dravet, or other genetically determined childhood syndromes are not detailed here, as they represent distinct developmental disorders rather than typical focal or generalized epilepsies of adult onset.
Temporal lobe epilepsy (TLE) is the most frequent focal epilepsy in adults and often originates in the mesial (inner, medial) temporal structures — the hippocampus and amygdala. Seizures usually start with a characteristic aura, such as a rising abdominal sensation, déjà-vu, or distorted smells, followed by loss of awareness and small repetitive movements. MRI often reveals hippocampal sclerosis or post-infectious scarring. If patients with temporal lobe epilepsy (TLE) become drug-resistant, surgical removal of the affected hippocampus or adjacent cortex can achieve long-term seizure freedom in about two-thirds of cases. Temporal lobe epilepsy (TLE) represents about 60-70% of surgical cases.
Frontal lobe epilepsy (FLE) presents with brief, sometimes nocturnal attacks of sudden motor activity, tonic posturing, or vocalization. Consciousness may be preserved or impaired, and the seizures tend to cluster — several episodes within hours or days. The epileptic focus is located in the frontal motor or premotor cortex. Because of rapid propagation and complex semiology, diagnosis often requires prolonged video-EEG monitoring. Frontal lobe seizures represent about 10–20 % of surgical series, with variable postoperative outcomes depending on localization precision.
Jacksonian epilepsy (focal-onset motor seizures) is named after Hughlings Jackson, who first described the progressive “march” of muscle twitching or tingling along the limb or face as the discharge spreads through the motor or sensory cortex. These seizures are usually brief and awareness is preserved. They typically arise from a circumscribed cortical lesion — a scar, small stroke, or tumor — and often have a clear anatomic correlate visible on MRI. Because the focus is well defined, Jacksonian seizures are among the most classical examples of operable focal epilepsy.
Generalized tonic–clonic seizures, (formerly called grand mal) involve sudden loss of consciousness, body stiffening, and rhythmic jerking of all limbs, followed by sleep or confusion.
They can be primary generalized, arising simultaneously in both hemispheres without a cortical focus (often genetic), or secondary generalized, beginning as focal discharges that rapidly engage both hemispheres. Among patients with generalized tonic–clonic seizures, roughly 60–70% are secondary generalized, while 30–40% are primary generalized from the outset.
When looking at epilepsy overall, approximately 65–70% of all epilepsies have a focal (localized) onset, whereas 30–35% are primarily generalized. Within the focal group, 20–40% of patients may experience secondary generalization during the course of their disease.
In total, about half to two-thirds of all patients with epilepsy experience generalized tonic–clonic seizures at some point — either as their main seizure type or as the secondary generalization of a focal onset.
The distinction matters clinically: secondary generalized seizures often arise from a resectable cortical focus, most commonly in the temporal or frontal lobes, while primary generalized epilepsies involve diffuse thalamocortical networks and are not suitable for surgical treatment.
Absence seizures, previously known as petit mal, are generalized non-convulsive seizures characterized by brief episodes of staring and unresponsiveness lasting only a few seconds, most common in children aged 5–12 years.
During these attacks, awareness is transiently lost, and the child typically has no memory of the event afterward. The EEG shows the classic 3 Hz bilateral spike-and-wave pattern, often provoked by hyperventilation.
These seizures originate from diffuse thalamocortical circuits rather than a single cortical focus, which is why surgical treatment is not indicated. They account for about 10–15 % of all epilepsies and usually respond completely to ethosuximide or valproate, with fewer than 10 % remaining drug-resistant.
In summary, focal epilepsies — including temporal, frontal, parietal, and Jacksonian forms — make up about 60% of all epilepsy cases, while generalized types from onset, such as absence and tonic–clonic seizures, represent roughly 30–35%. Considering both primary and secondary forms, about 50–60 % of all patients experience generalized tonic–clonic seizures at some point during their illness. The remaining small group includes mixed or unclassified forms. Approximately one-quarter to one-third of all patients develop drug-resistant epilepsy, and among them 10–20 % have a well-defined cortical focus suitable for neurosurgical treatment.
Diagnosis — How the Source of Seizures Is Found
Evaluation of epilepsy begins with a detailed clinical history, analysis of EEG recordings, and high-resolution MRI to identify structural brain changes that could explain the origin of seizures.
Additional techniques — such as functional MRI (fMRI), PET, SPECT, and video-EEG monitoring — help determine whether the abnormal activity arises from a specific cortical region and how it spreads.
This process distinguishes between generalized forms and focal epilepsies, where seizures consistently start from the same cortical focus.
If seizures continue despite trials of two appropriately chosen and tolerated medications, the condition is defined as drug-resistant epilepsy (DRE).
Patients with DRE should be referred to a specialized epilepsy center for advanced presurgical evaluation. The aim is to locate the “seizure focus” — the small brain region where seizures begin.
The evaluation includes:
- Video-EEG monitoring, which records brain waves and behavior during seizures.
- MRI of the brain using high-resolution protocols that can reveal even small scars or malformations.
- Functional imaging (PET or SPECT scans) to detect areas with abnormal metabolism or blood flow.
- Neuropsychological testing, to estimate possible cognitive risks of surgery.
- Invasive EEG (SEEG) is an advanced method used to precisely map where seizures begin when MRI or surface EEG cannot clearly identify the source. Through a minimally invasive procedure, thin electrodes are placed into deep brain structures to record electrical activity from multiple regions at the same time. SEEG is the most accurate way to distinguish a single epileptogenic focus from a wider network, and it is essential for planning modern epilepsy surgeries such as laser therapy (LITT), selective resections, or SEEG-guided radiofrequency thermocoagulation.
All this information helps decide if surgery is possible and safe.
Treatment Options in Epilepsy
- Medication – remains the first-line therapy for most patients. Dozens of modern anti-seizure drugs exist, and the correct combination must be personalized.
- Dietary therapy — (ketogenic / modified Atkins) can help in selected drug-resistant epilepsies and should be guided by an epilepsy team.
- Avoidance of seizure-provoking factors is an essential part of long-term control. These include sleep deprivation, flashing lights or visual stimuli, alcohol consumption, psychological stress, fever, and irregular medication use. In photosensitive forms, patients should avoid strobe lighting, video games with rapid flicker, or certain television and smartphone displays.
- Neurostimulation – devices like vagus nerve or deep brain stimulators that modulate abnormal activity.
- Surgical treatment, when seizures arise from a well-defined brain area that can be safely operated on.
When Surgery Becomes an Option in Epilepsy
Surgery is considered when:
- Seizures come from a single, identifiable area of the brain.
- The area can be removed without causing major functional loss (speech, memory, movement).
- Medications have failed to control the condition.
Contrary to common belief, epilepsy surgery is not a “last resort”, but an evidence-based treatment for selected patients.
The main goals are seizure freedom, better quality of life, and fewer medication side effects.
Main Surgical Procedures in Epilepsy
Surgical treatment for epilepsy is considered when seizures persist despite trials of at least two appropriate medications and when a focal region of the brain can be identified. Below are the main procedures used in epilepsy surgery, the brain regions they target, and typical outcome figures:
Temporal lobectomy (anterior or mesial resection)
This is the most common operation for drug-resistant epilepsy, performed in about 60–70 % of all epilepsy surgeries.
It targets seizures that start in the temporal lobe, most often in the inner (mesial) structures such as the hippocampus and amygdala.
Two main surgical styles are used:
- Anterior temporal lobectomy (ATL) removes both the front and inner parts of the temporal lobe. It is still the standard operation (about 70 % of temporal surgeries) and gives long-term seizure freedom in 65–80 % of properly selected patients.
- Selective mesial resection (SAH/MTR) removes only the deep structures (hippocampus + amygdala) and is chosen more often on the left, language-dominant side to protect speech and memory. It achieves freedom from seizures in about 55–70 % of cases.
In recent years, minimally invasive laser therapy (LITT) has become an option for selected patients, offering shorter recovery and fewer memory problems, though seizure control is somewhat lower (around 50–60 %).
SEEG-guided Radiofrequency Thermocoagulation (RFTC) is a minimally invasive technique performed through the same SEEG electrodes used to map the seizure focus. Once the epileptogenic zone is precisely identified, controlled thermal energy is applied to create small, targeted lesions without craniotomy. RFTC can reduce or eliminate seizures in 30–60% of well-selected patients, and often provides additional diagnostic value by confirming the true seizure-generating network. Recovery is rapid, risks are low, and the method is especially useful for deep or small foci that are not suitable for open surgery or when a less invasive first-step treatment is preferred.
Stereotactic radiosurgery (SRS) — using focused radiation such as Gamma Knife or CyberKnife — can achieve a similar effect by gradually destroying the epileptogenic tissue without open surgery. It is typically reserved for patients who are not candidates for conventional resection and acts more slowly, with seizure reduction developing over 6–12 months. Long-term seizure control rates are also around 50–60 %, making SRS a valuable but still nonstandard alternative for carefully selected cases of mesial temporal lobe epilepsy.
Minor visual-field changes are possible after surgery, and temporary word-finding or memory issues may occur on the left (dominant) side.
Serious complications are rare (mortality < 1 %). Overall, temporal surgery remains the most effective and safest procedure for adults with drug-resistant temporal lobe epilepsy
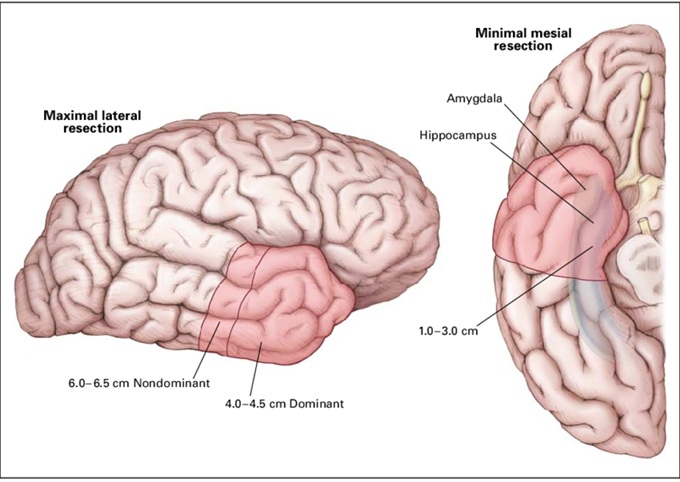
Image: Anterior temporal lobectomy (ATL)
Other Surgical Procedures for Epilepsy
Lesionectomy (resection of a small scar, malformation, tumor, or vascular abnormality) – A targeted removal of a clearly visible structural lesion within the cerebral cortex (e.g., focal cortical dysplasia, astrocytoma, oligodendroglioma, cavernous malformation) that is determined to be the epileptogenic focus. Success rates vary depending on the pathology, but many series report ~50-70 % freedom from seizures when complete resection is achieved.
Corpus callosotomy – A palliative disconnection procedure that severs part of the corpus callosum (the large nerve bridge connecting the two brain hemispheres) to prevent seizure spread from one hemisphere to the other, often used in drop attacks or multifocal epilepsy when a single focus cannot be safely removed. Long-term complete seizure freedom is achieved less frequently (often <30 %), but many patients experience significant reduction in seizure burden.
Multiple subpial transections (MST) – These are fine cuts made in the cortex to interrupt the horizontal spread of seizures in eloquent regions (motor, sensory, or language areas) where full resection would carry an unacceptable risk of deficit. The procedure is performed through a limited craniotomy under direct microsurgical visualization, not stereotactically, since precise identification of cortical layers is required. It is therefore not a “closed” or radiosurgical technique, but a conventional open neurosurgical approach with minimal cortical disruption. Seizure-free rates are lower (often around 20–40 %), but the procedure can significantly reduce the frequency or severity of seizures when resection is not feasible.
Neurostimulation implants (Vagus Nerve Stimulator – VNS, Responsive Neurostimulation – RNS, Deep Brain Stimulation – DBS) – These devices monitor or modulate abnormal electrical activity rather than removing brain tissue. They are used when resection is not safe or feasible. While full seizure freedom is less common, many patients achieve major reduction in seizure frequency (often 40-60 % reduction).
Each patient’s surgical plan is individualized and discussed by a multidisciplinary epilepsy surgery board, which considers the anatomy of the epileptogenic zone, risks of cognitive/motor/memory deficits, MRI/EEG concordance, and long-term prognosis.
Lesionectomy in the Treatment of Epilepsy
Lesionectomy refers to the targeted surgical removal of a clearly defined structural brain lesion that has been identified as the source of epileptic seizures. Such lesions may include cavernoma, brain tumors, arteriovenous malformations, arachnoid cyst, post-traumatic cortical scars or contusions (including those beneath depressed skull fractures), and selected cases of chronic subdural hematoma–related cortical injury, ICH, all of which are discussed in detail below. Unlike broader epilepsy surgery concepts focused on primary drug-resistant epilepsy, lesionectomy is based on the presence of a visible, localized abnormality that directly generates seizures.
This approach is particularly effective when there is strong concordance between clinical seizure semiology, EEG findings, and imaging, indicating that the lesion itself represents the epileptogenic focus. When these criteria are met and the lesion can be completely removed, lesionectomy offers some of the highest rates of long-term seizure freedom in epilepsy surgery.
However, the key principle is certainty. The lesion must truly be the cause of epilepsy, not merely an incidental finding.
Structural Lesions Suitable for Lesionectomy
Lesionectomy may be considered in several well-defined conditions:
Cavernous malformations
Cavernomas are a classic cause of focal epilepsy. Seizures often result from chronic cortical irritation and hemosiderin deposition around the lesion. Surgical removal of the cavernoma together with the surrounding epileptogenic tissue is frequently associated with excellent seizure outcomes.
Brain tumors
Low-grade tumors such as meningiomas (olfactory, convexity, parasagittal, sphenoid), gangliogliomas, DNETs, and certain gliomas often present with seizures as the dominant symptom. In these cases, tumor resection is not only oncologically indicated but may also serve as an effective epilepsy treatment when the tumor corresponds to the seizure focus. Seizure can be also a first symptom in glioblastoma and other malignant brain tumors.
Arteriovenous malformations (AVMs)
AVMs can cause epilepsy through chronic cortical irritation or prior microhemorrhage. Lesionectomy may be considered in selected cases, often as part of a broader multimodal strategy that may include endovascular or radiosurgical treatment.
Post-traumatic lesions and contusions
Traumatic brain injury may leave behind focal cortical scars or contusional damage that later becomes epileptogenic. When seizures clearly originate from such a lesion, targeted resection can be considered. Depressed skull fractures with underlying cortical injury represent a specific traumatic scenario in which lesion-based epilepsy surgery may be relevant. Detailed information on all types of traumatic brain injuries can be found on this page.
Chronic subdural hematoma–related cortical injury
Although chronic subdural hematoma itself is not a primary epileptogenic lesion, prolonged cortical irritation and residual cortical changes may create a seizure focus in selected patients. In rare, carefully selected cases, surgical intervention addressing the underlying cortical pathology may be part of epilepsy management.
The Critical Challenge: Multiple Lesions
Lesionectomy becomes significantly more complex when multiple potential epileptogenic abnormalities are present. Examples include multiple cavernomas, several traumatic cortical scars, coexisting meningiomas, or combined post-hemorrhagic and post-traumatic changes.
In such cases, the main challenge is determining which lesion is actually responsible for epilepsy. Removing a visible lesion that is not the true epileptogenic focus may fail to control seizures and exposes the patient to unnecessary surgical risk. For this reason, lesionectomy should only be performed after careful evaluation confirming that the targeted lesion is causally linked to seizure generation.
Decision-Making and Limitations
Lesionectomy is not automatically indicated simply because a lesion is visible on imaging. The decision requires correlation between imaging, seizure characteristics, and electrophysiological data, and must consider the functional importance of the surrounding brain tissue.
When the lesion lies within or near eloquent cortex, or when epileptogenicity cannot be confidently assigned to a single abnormality, alternative surgical strategies or non-resective approaches may be more appropriate.
Key Message
Lesionectomy represents one of the most effective surgical treatments for epilepsy when a single, well-defined structural cause is responsible for seizures. Its success depends not on the size or appearance of the lesion, but on the certainty that it is the true source of epilepsy. Careful patient selection remains the most important determinant of outcome.
After Epilepsy Surgery — Recovery and Follow-Up
Hospital stay is usually 4–7 days.
Patients are monitored for neurological function, wound healing, and medication adjustment.
Seizure frequency typically declines over months, and many people eventually reduce or stop drugs under supervision.
Telehealth consultations allow international patients to stay in touch with their neurosurgeon or neurologist after returning home — to discuss medication changes, MRI results, or seizure diaries.
When to Seek a Specialist Opinion in Epilepsy
A specialist (epileptologist or neurosurgeon) should be consulted if:
- Seizures persist despite two or more medications.
- MRI shows a structural lesion (scar, malformation, tumor).
- You have severe side effects from drugs.
- You are uncertain whether your seizures are truly epileptic.
Even a brief telehealth second opinion can help determine if you might benefit from surgical evaluation.
Epilepsy Summary and Key Points
Epilepsy remains a complex neurological disorder, but with modern diagnostics, medication, and—when appropriate—surgical treatment, the majority of patients can achieve long-term seizure control.
When medications fail, surgery can offer long-term seizure control and better life quality for carefully selected patients.
Modern imaging, detailed EEG monitoring, and multidisciplinary evaluation make epilepsy surgery safer and more effective than ever before.
FAQ about Epilepsy Surgery
Who is a candidate for epilepsy surgery?
A candidate for epilepsy surgery is usually a patient whose seizures continue despite adequate trials of two properly chosen and tolerated anti-seizure medications. This situation is called drug-resistant epilepsy. Surgery is not considered only because seizures are frequent; the key question is whether seizures repeatedly start from a defined cortical area that can be treated safely. Presurgical evaluation must show that the epileptogenic zone is localized and that removing, disconnecting, ablating, or modulating it would not cause unacceptable loss of speech, memory, movement, vision, or other essential functions. The best candidates often have focal epilepsy, temporal lobe epilepsy, or a structural lesion such as a scar, tumor, cavernoma, AVM, or cortical malformation.
What does “drug-resistant epilepsy” mean?
Drug-resistant epilepsy means that seizures continue despite trials of two appropriate anti-seizure medications, chosen correctly for the seizure type and used at tolerated doses. This does not mean that every medication has failed, but after two adequate medication trials, the chance of complete seizure freedom with further drug changes alone becomes much lower. At that point, the patient should not simply continue changing medications for years without reassessment. A specialized epilepsy center can evaluate whether seizures arise from a focal cortical region, whether there is a structural cause, and whether surgery, laser ablation, SEEG-guided treatment, neurostimulation, dietary therapy, or another advanced option may be more appropriate than repeated medication adjustments alone.
How successful is epilepsy surgery?
The success of epilepsy surgery depends on epilepsy type, localization accuracy, MRI findings, EEG concordance, and whether the epileptogenic zone can be safely treated. The best outcomes are usually seen in well-selected temporal lobe epilepsy, especially mesial temporal lobe epilepsy with a clear structural abnormality. In these patients, anterior temporal lobectomy may achieve long-term seizure freedom in about 65–80%, while selective mesial resection often achieves seizure freedom in about 55–70%. Laser ablation may offer seizure freedom in roughly 50–60% of carefully selected cases. Lesionectomy for a clearly epileptogenic tumor, cavernoma, scar, or malformation can also be very effective. Outcomes are lower when seizures are multifocal, poorly localized, or arise near eloquent cortex.
What is the difference between anterior and mesial (selective) resection in epilepsy surgery?
Anterior temporal lobectomy and selective mesial resection are both operations used mainly for drug-resistant temporal lobe epilepsy, but they remove different amounts of tissue. Anterior temporal lobectomy removes the front part of the temporal lobe together with mesial structures such as the hippocampus and amygdala. Selective mesial resection removes mainly the deep mesial temporal structures while preserving more of the lateral temporal cortex. The selective approach may be chosen more often on the dominant, usually left, side because speech and verbal memory are important concerns. The decision depends on seizure localization, MRI findings, neuropsychological testing, language dominance, memory risk, and whether the epileptogenic zone extends beyond the mesial temporal structures.
What tests are done before epilepsy surgery?
Before epilepsy surgery, the goal is to identify where seizures start and whether that region can be treated safely. Evaluation usually includes detailed seizure history, neurological examination, video-EEG monitoring, high-resolution epilepsy-protocol MRI, and neuropsychological testing. PET or SPECT may be used when MRI and EEG do not fully agree or when the seizure focus is difficult to localize. Functional MRI may help assess speech or memory-related risk. In complex cases, stereo-EEG, or SEEG, is used to record seizures directly from deep or multiple brain regions through implanted electrodes. These tests must answer two questions: is there a consistent epileptogenic zone, and can treatment be performed without unacceptable neurological or cognitive deficit?
What are possible complications of epilepsy surgery?
Possible complications of epilepsy surgery depend on the type of operation and the brain region being treated. After temporal lobe surgery, mild upper visual-field loss can occur because visual pathways pass near the surgical area. On the dominant, usually left, side, temporary or persistent word-finding difficulty or verbal memory decline may occur, especially when mesial temporal structures are involved. Any brain surgery also carries risks of bleeding, infection, stroke, neurological deficit, wound problems, or anesthesia-related complications, although serious complications are uncommon in experienced centers. The purpose of presurgical evaluation is to estimate these risks before treatment. Surgery is recommended only when the expected benefit in seizure control and quality of life outweighs the predicted risk.
What is the recovery like after epilepsy surgery?
Recovery after epilepsy surgery depends on the procedure performed, but hospital stay after open surgery is often around 4–7 days. During this period, doctors monitor neurological function, wound healing, seizures, medication tolerance, and early postoperative changes. Seizure improvement may occur immediately, but in some patients seizure frequency declines gradually over months. Anti-seizure medications are usually not stopped suddenly; they are adjusted slowly and only under specialist supervision. Patients may need follow-up MRI, EEG review, seizure diary assessment, and medication monitoring. Recovery also includes practical issues such as fatigue, return to work, driving restrictions, and cognitive changes. Telehealth follow-up can help international patients discuss seizure control, medication changes, and new symptoms after returning home.
Is telehealth useful in epilepsy surgery?
Telehealth can be useful in epilepsy surgery both before and after treatment. Before surgery, an online second opinion may help review MRI findings, EEG reports, seizure history, medication trials, and whether the patient should be evaluated in a specialized epilepsy center. It can also clarify whether the case suggests focal epilepsy, structural epilepsy, drug-resistant epilepsy, or a situation where surgery is unlikely. After surgery, telehealth can support follow-up by reviewing seizure diaries, medication changes, MRI results, new symptoms, and recovery questions. Telehealth does not replace emergency care, video-EEG admission, SEEG, or surgery itself, but it can help patients and families understand whether advanced evaluation is justified and what the next step should be.
How common are temporal brain lobe surgeries compared to other types of epilepsy surgery?
Temporal lobe surgery is the most common form of epilepsy surgery because temporal lobe epilepsy is the most frequent surgically treatable focal epilepsy in adults. In surgical series, temporal lobe epilepsy often represents around 60–70% of epilepsy operations. This is partly because seizures from the mesial temporal structures, especially the hippocampus and amygdala, can often be localized with MRI, EEG, seizure semiology, and neuropsychological testing. Outcomes are also generally better than in many extratemporal epilepsies when the case is well selected. Frontal lobe epilepsy is less common and can be harder to localize because seizures may spread rapidly. Parietal, occipital, multifocal, and generalized epilepsies are less frequently suitable for resective surgery.
Why is a selective approach in epilepsy surgery preferred on the left (dominant) side?
A selective approach in epilepsy surgery may be preferred on the left, usually language-dominant, side because speech and verbal memory functions are more vulnerable. In temporal lobe epilepsy, the epileptogenic zone may involve the hippocampus and amygdala, but removing too much lateral temporal tissue can increase the risk of naming difficulty, word-finding problems, or memory decline. Selective mesial resection attempts to remove the deep seizure-generating structures while sparing more surrounding cortex. This does not mean that selective surgery is always safer or always better. The choice depends on seizure localization, MRI findings, EEG data, neuropsychological results, language dominance, and whether the seizure network extends beyond mesial temporal structures. The operation must match the individual risk map.
Can generalized epilepsies be treated surgically?
Primary generalized epilepsies are usually not treated with resective surgery because seizures begin in diffuse bilateral networks rather than from one removable cortical focus. Examples include many absence epilepsies and genetic generalized epilepsies. Surgery becomes more relevant when seizures are actually focal at onset and then secondarily generalize, meaning they start in one cortical region and rapidly spread to both hemispheres. This distinction is critical because generalized tonic–clonic seizures can look similar clinically, even when their origin is different. If a focal onset is identified, surgery may be possible. If seizures are truly generalized from the beginning, treatment usually relies on medication, lifestyle measures, dietary therapy in selected cases, or neurostimulation rather than removing brain tissue.
When is lesionectomy used in epilepsy surgery?
Lesionectomy is used in epilepsy surgery when a clearly defined structural brain lesion is believed to be the source of seizures. Examples include cavernous malformation, low-grade tumor, focal cortical dysplasia, arteriovenous malformation, post-traumatic cortical scar, post-stroke scar, or selected cortical changes after hemorrhage or infection. The key requirement is concordance: seizure history, EEG, MRI, and clinical pattern should all support that the visible lesion is the epileptogenic focus. Removing a lesion simply because it is visible can fail if it is not the true seizure source. When the lesion and seizure focus match and complete safe removal is possible, lesionectomy can produce high rates of seizure control. The decision becomes harder when multiple lesions are present.
Can structural epilepsy from a tumor, cavernoma, AVM, scar, or trauma be treated surgically?
Yes. Structural epilepsy from a tumor, cavernoma, AVM, cortical scar, traumatic contusion, focal cortical dysplasia, or post-infectious gliosis can sometimes be treated surgically when the lesion is responsible for seizure generation and can be safely removed or treated. These cases are different from epilepsies without a visible focus because there may be a defined anatomical target. Surgery can reduce or eliminate seizures when the epileptogenic lesion and surrounding irritative zone are correctly identified. However, a structural abnormality on MRI is not automatically the cause of epilepsy. The surgical team must confirm the relationship between the lesion, seizure semiology, EEG findings, and functional brain areas. Treatment may include lesionectomy, broader resection, radiosurgery, embolization, ablation, or neurostimulation depending on the lesion.
What is SEEG and when is it needed before epilepsy surgery?
SEEG, or stereo-electroencephalography, is an invasive recording method used when noninvasive tests cannot clearly define where seizures begin. Thin electrodes are placed into selected brain regions through small openings, allowing direct recording from deep and superficial structures at the same time. SEEG is especially useful when MRI is normal, when EEG and MRI disagree, when seizures may arise from deep or multiple regions, or when the focus is near important functional cortex. It helps distinguish a single epileptogenic focus from a wider seizure network. SEEG can also guide minimally invasive treatments such as radiofrequency thermocoagulation. The goal is to make epilepsy surgery safer and more precise, not to operate blindly.
Are laser ablation, SEEG-guided thermocoagulation, or neurostimulation alternatives to open epilepsy surgery?
Yes. Laser ablation, SEEG-guided radiofrequency thermocoagulation, and neurostimulation can be alternatives to open epilepsy surgery in selected patients. Laser interstitial thermal therapy, or LITT, uses heat to ablate a defined deep focus, often with shorter recovery than open surgery. SEEG-guided thermocoagulation can create small targeted lesions through diagnostic electrodes after the seizure network is mapped. Neurostimulation methods such as VNS, RNS, or DBS do not remove brain tissue; they modulate abnormal activity and are used when resection is unsafe or seizures are multifocal. These approaches usually have different seizure-freedom rates than classic temporal lobectomy. The best option depends on localization, anatomy, risk, seizure type, and treatment goal.
When should a patient with epilepsy seek a specialist opinion about surgery?
A patient with epilepsy should seek a specialist opinion about surgery when seizures continue despite two appropriate anti-seizure medications, when MRI shows a possible structural lesion, when medication side effects are severe, or when there is uncertainty about whether seizures are focal or generalized. Referral should not wait for many years of failed medication trials if drug-resistant epilepsy is already present. A specialist opinion is also important when seizures affect driving, work, school, independence, injury risk, or quality of life. The goal is not to rush into surgery, but to determine whether advanced evaluation is needed. Many patients are not surgical candidates, but they still benefit from knowing why surgery is or is not appropriate.
Can an online second opinion help when epilepsy surgery opinions differ?
Yes. An online second opinion can help when epilepsy surgery opinions differ, especially if one team recommends continued medication while another suggests presurgical evaluation or surgery. The review can clarify whether seizures meet the definition of drug-resistant epilepsy, whether MRI shows a structural lesion, whether EEG and symptoms suggest focal onset, and whether advanced tests such as video-EEG, PET, SPECT, neuropsychological testing, or SEEG are needed. It can also explain the difference between temporal lobectomy, selective mesial resection, lesionectomy, laser ablation, thermocoagulation, and neurostimulation. The goal is not to replace an epilepsy center, but to help patients understand whether the next step should be referral, further testing, surgery, or non-surgical treatment.
Additional Sources for Patients
Reliable, easy-to-understand resources that follow the terminology and recommendations of the International League Against Epilepsy (ILAE).
-
Epilepsy Foundation – What Is Epilepsy?
Plain-language overview of seizure types, causes, and treatments, written in accordance with ILAE definitions. -
Epilepsy Foundation – Surgery for Epilepsy
Patient-friendly explanation of surgical options (temporal lobectomy, lesionectomy, callosotomy, neurostimulation) and expected results, consistent with current ILAE and American Epilepsy Society guidance. -
ILAE – Patient Care Resources
Official International League Against Epilepsy page with educational materials, links to centers, and global standards for epilepsy care. -
NICE Guideline NG217 – Epilepsies: Diagnosis and Management (2025 review)
National Institute for Health and Care Excellence guideline reflecting ILAE terminology and evidence-based recommendations, accessible to both patients and clinicians. -
Mayo Clinic – Epilepsy: Diagnosis and Treatment
Describes diagnostic tests and surgical options in language understandable to non-specialists, referencing international standards (ILAE). -
Barrow Neurological Institute – Epilepsy Surgery
Comprehensive explanation of modern surgical approaches (including MRI-guided laser therapy) used in accredited epilepsy centers. -
Epilepsy Society (UK) – Epilepsy Surgery
UK patient resource aligned with ILAE standards, explaining step-by-step evaluation before surgery and recovery expectations.
Lesionectomy (resection of a small scar, malformation, tumor, or vascular abnormality) – A targeted removal of a clearly visible structural lesion within the cerebral cortex (e.g., focal cortical dysplasia, glioma, cavernous malformation) that is determined to be the epileptogenic focus. Success rates vary depending on the pathology, but many series report ~50-70 % freedom from seizures when complete resection is achieved.