Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: November 7, 2025
Who is this page for?
This page is intended for patients and families who are trying to understand a brain or spinal infection seen on MRI or CT — such as a brain abscess, subdural empyema, epidural abscess, ventriculitis, or post-surgical infection. It explains what these findings mean, how bacteria may reach the nervous system, when antibiotics may be enough, when surgery is considered, and why procedures such as aspiration, burr-hole drainage, or craniotomy may be chosen. For an expert review of your imaging and treatment plan, see our page on neurosurgery second opinion .
When patients and families usually seek a second opinion for brain abscess, empyema, or CNS infection
- MRI or CT shows a brain abscess, subdural empyema, epidural abscess, ventriculitis, or post-surgical infection, but the meaning of the finding is unclear
- It is uncertain whether intravenous antibiotics alone are enough or whether neurosurgical drainage is needed
- Surgery has been proposed, but the family wants to understand why aspiration, burr-hole drainage, or craniotomy is being considered
- The patient is not improving as expected despite antibiotics, or follow-up imaging shows persistent pus, edema, or mass effect
- There are questions about whether the infection is a brain abscess, subdural empyema, epidural abscess, meningitis, ventriculitis, or another related condition
- A previous craniotomy, shunt, EVD, trauma, sinus infection, ear infection, mastoiditis, or dental infection may be related to the intracranial infection
- The family needs help understanding prognosis, seizure risk, neurological recovery, recurrence risk, or the expected duration of treatment
In these situations, an experienced neurosurgical review can help interpret MRI or CT findings, clarify whether the infection behaves like a brain abscess or empyema, assess whether surgery is needed, and explain why one procedure may be preferred over another: Request a Second Opinion
Brain Abscess, Empyema and CNS Infection — Quick Summary (Read This First)
- A brain abscess is a localized collection of pus inside the brain tissue, while subdural or epidural empyema is pus around the brain or spinal cord. This distinction matters because brain abscess and empyema behave differently and often require different treatment decisions.
- Brain abscess usually develops inside the brain tissue, while subdural empyema can spread rapidly across the surface of the brain. For this reason, subdural empyema is often treated more urgently and more surgically than a small, stable brain abscess.
- CNS infections can spread from sinusitis, ear or mastoid infection, dental infection, bloodstream infection, trauma, CSF leak, shunt infection, EVD infection, or previous neurosurgery. Identifying the source of infection is important because treatment must address both the intracranial infection and the original entry point.
- Antibiotics alone may be sufficient for selected small brain abscesses when the patient is stable, there is no major mass effect, and follow-up imaging shows improvement. These cases still require close neurological monitoring and repeated MRI or CT scans.
- Surgery is considered when a brain abscess is large, causes mass effect, worsens neurologically, fails to respond to antibiotics, has uncertain diagnosis, or is at risk of rupturing into the ventricles. In these situations, drainage or removal may be needed in addition to intravenous antibiotics.
- The choice between stereotactic aspiration, burr-hole drainage, and craniotomy depends on the type, location, size, depth, and structure of the infection. Aspiration is often used for deep brain abscesses, while craniotomy may be needed for superficial, multiloculated, recurrent, or compressive collections.
- Sometimes surgery is needed not only to drain the brain abscess or empyema, but also to treat the original source of infection. For example, sinus surgery, mastoid or ear surgery, removal of infected bone, wound revision, or removal of infected shunt or EVD hardware may be required, and drainage of the intracranial collection may be performed as part of the same overall treatment plan.
- Lumbar puncture is not always safe in suspected brain abscess, empyema, or CNS infection with mass effect. When there is brain swelling, hydrocephalus, or risk of herniation, diagnosis usually relies first on CT, MRI, blood cultures, and samples obtained from the infection source or surgical drainage.
- Recovery depends on how early treatment starts, neurological condition, abscess location, organism, immune status, and complications such as seizures, ventriculitis, hydrocephalus, or venous thrombosis. Some patients recover well, while others may have persistent neurological deficits or long-term seizure risk.
- This page explains how brain abscess, empyema, ventriculitis, spinal epidural abscess, and related CNS infections are diagnosed and treated. Use the Contents box to navigate to sections on imaging, bacteria, routes of spread, antibiotics, surgical indications, aspiration versus craniotomy, prognosis, and follow-up.
Contents – Brain Abscess
- Brain Abscess and CNS Infections
- Etiology and Common Bacteria
- How Bacteria Reach the CNS
- Types of CNS Infections
- How Infections Injure System
- Symptoms & Red Flags
- Diagnosing CNS Infections
- **Treatment of CNS Infections**
- How Medical Decisions are Made
- Prognosis & Follow-Up
- Telehealth Second Opinion
- Infections FAQ
- Additional Patient Resources
What “CNS Infections” Means (Central Nervous System Infections)
Central nervous system infections become neurosurgical problems when infection forms pus, causes pressure on the brain or spinal cord, involves implanted hardware, or fails to respond safely to antibiotics alone.
Central Nervous System (CNS) infections are infections that affect the brain, spinal cord, ventricles, meninges, or adjacent structures, and in many cases require neurosurgical intervention. In this context we focus on pyogenic (bacterial) infections such as brain abscesses, subdural and epidural empyemas, ventriculitis, and vertebral osteomyelitis/discitis—i.e., those infections where a neurosurgeon may be required to drain, debride, or remove foreign hardware. All chapters of this article primarily refer to brain abscess, but since other infections (empyema, osteomyelitis, meningitis, etc.) are often found alongside it, they are also covered.
Etiology and Common Bacteria in CNS Infections
Most Central Nervous System (CNS) infections treated by neurosurgeons are caused by bacteria, frequently presenting as a mixed flora. The spectrum of pathogens often encountered is broad, and precise identification of the causative agent is paramount for guiding effective antimicrobial therapy.
The most frequent types include:
Gram-Positive Cocci: These remain the most common isolates, including Streptococcus species (especially the viridans group associated with odontogenic or dental sources) and Staphylococcus aureus (a major concern, particularly MRSA in post-operative or hospital-acquired cases).
Anaerobes: Bacteria thriving in low-oxygen environments, such as Bacteroides and Fusobacterium species, which frequently originate from chronic sinusitis or otitis media.
Gram-Negative Bacilli: A highly significant group that includes Escherichia coli (E. coli), Klebsiella, Proteus, and Serratia species, often seen in immunocompromised patients or following penetrating trauma.
Atypical and Less Common Bacteria: This group comprises organisms that require specialized consideration, such as Nocardia and Actinomyces, which typically cause slowly progressive infections, and Listeria monocytogenes, which is relevant in specific at-risk groups (the elderly, neonates, and the immunocompromised).
While bacteria are the primary focus for neurosurgical intervention, a comprehensive diagnostic assessment always includes screening for less common agents like Fungi (Cryptococcus, Aspergillus) and parasites (Toxoplasma gondii), particularly when managing immunocompromised patients.
Risk factors and predisposing conditions include the following:
- Adjacent infections: ear or mastoid infections, sinusitis, or dental infections.
- Cranial trauma or neurosurgical procedures: open or depressed skull fractures, craniotomy (surgical opening of the skull), ventricular shunts (tubes in brain ventricles containing cerebrospinal fluid – CSF), or external ventricular drains (EVDs- draining excessive CSF from brain ventricles).
- Hematogenous spread: bacteremia (bacteria in the blood), pulmonary infections, or infective endocarditis (inner layer of the heart).
- Immunocompromised state: HIV infection, diabetes, malignancy, or immunosuppressive therapy (e.g. chemotherapy, long-term steroids).
- CSF (Cerebrospinal fluid) leakage or skull base defects: following trauma or previous surgery.
- Intracranial foreign material: ventriculoperitoneal (VP) shunts for hydrocephalus treatment, drains, or retained bone fragments after trauma.
Routes of Infection — How Bacteria Reach the CNS
- Contiguous spread: from sinuses, middle ear, mastoid to adjacent cranial spaces (leading to subdural empyema, epidural abscess, or brain abscess).
- Hematogenous spread: bacteria traveling via bloodstream seed into brain parenchyma.
- Direct inoculation: trauma, penetrating injuries, neurosurgical instrumentation.
- Device/CSF infection: shunts, drains, or ventriculostomy catheters can become colonized with bacteria and lead to ventriculitis (infections of the walls of the brain ventricles) or abscess formation around the implanted hardware.
Types of CNS Infections
The most important practical distinction is whether infection is inside the brain tissue, around the brain or spinal cord, inside the ventricles, in the bone, or around implanted hardware. In practice, this means distinguishing brain abscess, subdural empyema, epidural empyema or epidural abscess, ventriculitis, cranial or spinal osteomyelitis, discitis, spinal epidural abscess, and shunt or EVD infection. Each location changes the urgency, treatment plan, and surgical approach.
Brain abscess is a localized infection within the brain tissue, characterized by inflammation, necrosis, and accumulation of pus. The pus typically contains neutrophils (a type of white blood cell that accumulates rapidly in acute infection), necrotic debris, and bacteria. The lesion develops gradually through four main pathological stages:
- Early cerebritis: acute inflammation of the brain parenchyma without a true pus cavity. There are microabscesses, vascular congestion, and edema, but no capsule formation.
- Late cerebritis: tissue necrosis and liquefaction appear; neutrophils dominate the lesion, forming an early purulent core while granulation tissue begins to develop at the margins.
- Early capsule stage: a thin capsule of granulation tissue forms around the necrotic center, partially limiting the spread of infection.
- Late capsule stage (formed in 2-3rd week of infection): a mature capsule composed of collagen and an outer gliotic layer surrounds the central necrotic and pus-filled core.
Subdural empyema is a collection of pus located in the subdural space, which is situated between the dura mater (the tough outer layer) and the arachnoid mater (the delicate middle layer of the membranes that cover the brain and spinal cord). Because there is no tight anatomic barrier in this compartment, the infection can spread widely over the cerebral convexities or along the falx and tentorium. The inflammatory process may lead to venous thrombosis and secondary cerebral infarction.
Epidural abscess or empyema refers to pus accumulating between the skull and dura or within the vertebral epidural space. The spread is usually more localized than in subdural empyema, but the mass effect and compression of underlying neural tissue can be pronounced.
Cranial osteomyelitis is an infection of the skull bones that usually follows chronic ear or sinus infection, head trauma, or neurosurgical procedures. The infection causes bone marrow inflammation, vascular thrombosis, and necrosis with formation of sequestra (dead bone fragments). In advanced cases, the process may spread to the dura, producing an epidural abscess.
Ventriculitis represents inflammation and infection of the ventricular system, most often related to neurosurgical procedures or colonization of ventricular shunts and external drains (EVDs). It is typically accompanied by fever, altered consciousness, and turbid cerebrospinal fluid.
Vertebral osteomyelitis, discitis, and spinal epidural abscess involve infection of the vertebral bodies or intervertebral discs, sometimes extending into the epidural space and compressing the spinal cord or nerve roots, leading to neurological deficits and severe back pain.
How CNS Infections Injure the Nervous System
- Mass effect and pressure: the abscess compresses surrounding brain tissue, leading to local ischemia and neurological deficits.
- Edema: inflammatory brain swelling around the lesion increases intracranial pressure and worsens tissue injury.
- Vascular involvement: inflammation or thrombosis of nearby vessels may cause secondary ischemic infarction.
- Rupture into the ventricles: can result in ventriculitis or secondary meningitis with rapid clinical deterioration.
- Compression of the spinal cord or nerve roots: in spinal epidural abscesses, pressure on neural structures causes pain, weakness, or paralysis.
Symptoms & Red Flags of CNS Infections
Common signs include:
- Headache
- Fever / chills
- Focal neurologic deficits (hemiparesis, cranial nerve palsies)
- Seizures
- Altered consciousness or mental status
- Nausea, vomiting (especially if increased intracranial pressure)
- Nuchal Rigidity: Meningeal sign due to meningitis or infection penetration into the brain ventricles.
- For spinal forms: back pain, radiculopathy, motor/sensory deficits, sometimes bladder/bowel dysfunction
Red flags: rapid deterioration, new seizures, signs of herniation, acute neurological deficits.
Diagnosing CNS Infections — Imaging, Laboratory & Key Diagnostic Questions
Diagnosis is not only about confirming infection; it must show where the pus or inflammation is located, whether there is mass effect, whether lumbar puncture is safe, and where the best microbiological sample can be obtained.
In every suspected CNS infection, clinicians — especially neurosurgeons — must find answers to several key questions:
- Which CNS structure is involved?
Neuroimaging (CT, MRI) determines brain, spinal cord, ventricles, epidural/subdural spaces. - Is there a localized pus collection and where?
MRI with contrast (and diffusion-weighted imaging) can localize abscess or empyema. Supporting lab markers: elevated ESR, CRP, fibrinogen; neutrophilia with left shift; high procalcitonin. - What are the local risk factors or entry sources?
Perform an ENT examination to exclude sinusitis or otitis. Consider possible skull fracture, cerebrospinal fluid (CSF) leakage, previous neurosurgical procedures, or an underlying immunodeficiency. - Is meningitis present?
May allow culture of pathogen from CSF, but lumbar puncture only if safe (no mass effect). - What is the causative organism?
Microbiologic tests: swabs from the primary infection site (sinus, ear, or wound), blood cultures, cerebrospinal fluid (if meningitis is suspected), aspirated material from the abscess or pus cavity, and CSF samples obtained from a VP shunt or external drainage system. - Is there neurological damage, how severe?
Clinical examination (level of consciousness, motor/sensory deficits) guides urgency and approach. - Are there infections elsewhere in the body, or is this part of systemic sepsis? It is essential to look for other infection sites such as the lungs, heart (endocarditis), abdominal organs, urinary tract, or skin and soft tissues. Blood cultures and full systemic evaluation help distinguish an isolated CNS abscess from generalized sepsis or metastatic infections spreading from another focus.
- It is equally important to assess for significant comorbidities that may influence the course or treatment of CNS infections, including diabetes, chronic kidney or liver disease, malignancy, or immune suppression. These factors often determine prognosis and antibiotic response.
- Is this part of a cluster or nosocomial chain?
Particularly in hospital-acquired infections, epidemiologic tracing and infection control must be considered.
Diagnostic workflow: neurological examination, laboratory tests, and imaging (CT or MRI with contrast and special sequences for pus detection), followed by additional evaluations when needed (ENT or infectious disease specialist). The results then guide where sampling is possible, always considering the risk of lumbar puncture in patients with mass lesions.
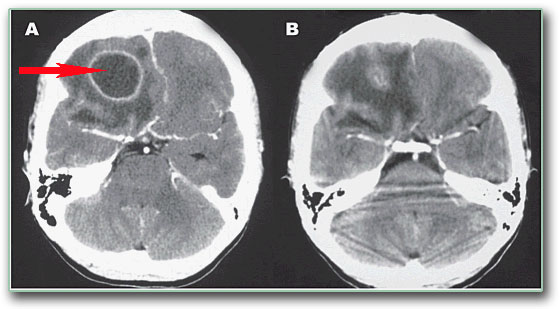
Image: CT scan of the brain. The arrow indicates a pus collection in the frontal lobe.
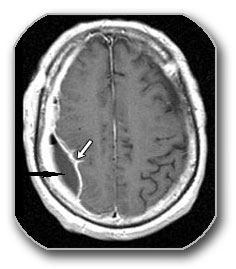
Image: CT scan of the brain. The arrow indicates a pus collection beneath the dura mater.
Treatment of CNS Infections— Medical & Surgical
Treatment depends on whether the infection can be controlled with intravenous antibiotics alone or whether neurosurgical drainage is needed because of pus collection, mass effect, neurological worsening, uncertain diagnosis, infected hardware, or failure to improve.
Medical (Antibiotic) Therapy
- The primary goal of antibiotic therapy is to sterilize the abscess cavity, control surrounding edema, and prevent recurrence or dissemination.
- Empiric broad-spectrum intravenous antibiotics, ideally combinations that penetrate CNS. Recent guidelines suggest for post-neurosurgical brain abscess: carbapenem + vancomycin or linezolid (conditional recommendation)
- Adjust antibiotics after culture & sensitivity results
- Duration: often 4–8 weeks or more, depending on organism, location, surgical result
- Other medications: antiedematous drugs (mannitol, hypertonic saline, short-course dexamethasone), antiepileptics (levetiracetam, phenytoin, or valproate), analgesics and antipyretics (paracetamol), gastroprotectives (PPIs with steroids), and supportive therapy for hydration, glucose, and electrolytes. Anticoagulation only if cerebral venous thrombosis is proven.
Surgical / Interventional Approaches for CNS Infections
- Brain abscess – Drainage/aspiration or Resection (partial or complete removal).
- Subdural and epidural empyemas usually require urgent surgical evacuation. Because the pus is often thick and multiloculated, burr-hole drainage (drainage through a small hole in the skull, around 1 cm in diameter) may be insufficient. A formal craniotomy (a wider opening of the skull using a bone flap, usually more than 3 cm) is often required for complete evacuation and decompression.
- Shunt / hardware removal: If infection involves devices surgically implanted in the brain (like shunts), they require removal plus external drainage of brain ventricles (EVD) and antibiotics.
- Spinal epidural abscess: Decompression surgery is necessary if a neurologic deficit (loss of movement or sensation) or cord compression (pressure on the spinal cord) appears.
Multidisciplinary management: neurosurgeon + infectious disease + radiology + critical care.
Indications for Surgery and Conservative Treatment in Brain Abscess
The key question is not only the size of the brain abscess, but whether it is causing pressure, neurological deterioration, ventricular risk, diagnostic uncertainty, or poor response to antibiotics.
Many brain abscesses can initially be managed with targeted intravenous antibiotics and antiedematous treatment and close imaging follow-up. Surgical intervention is reserved for larger lesions, those causing mass effect, or cases that fail to respond to medical therapy. Only an experienced neurosurgeon can evaluate and interpret the overall significance of all surgical indications together.
Conservative (medical) treatment may be considered when:
- The abscess is small (less than 2–2.5 cm) especially if it is deep in critical brain areas (critical brain zones) and without significant mass effect (meaning it is not large enough to compress or push the surrounding healthy brain tissue).
- the patient is neurologically stable,
- the causative organism is identified and sensitive to antibiotics,
- there is no evidence of raised intracranial pressure or ventricular rupture.
Patients under conservative management require serial MRI or CT imaging to confirm reduction in abscess size and resolution of edema.
Surgical Treatment of Brain Abscess
Decisions are individualized but most guidelines and reviews support the following indications for a surgical treatment of brain abscess:
- Large abscess ≥ 2.5–3 cm or causing significant mass effect
- Neurological deterioration or signs of raised intracranial pressure (a worsening of symptoms, such as new or increased weakness in the limbs – hemiparesis, or a decreased level of consciousness).
- Abscess close to the ventricular system or risk of rupture into ventricles
- Failure of antibiotic therapy — enlargement or no reduction after ~3–4 weeks of adequate antibiotics
- Uncertain diagnosis — when biopsy or aspiration is needed to exclude tumor or metastasis
- Multiloculated abscess where single aspiration is unlikely to be effective
- Associated cranial source requiring surgery, e.g. otitis, sinusitis, or mastoiditis with dural involvement
- Foreign body or surgical material (e.g. bone fragments, infected shunt or drain) requiring removal
- Fungal abscess or other atypical pathogens with poor antibiotic response
Choice of surgical technique:
- Stereotactic (spatial neurosurgical navigation to the lesion inside the skull) or burr-hole aspiration (drainage through a small hole in the skull, around 1 cm in diameter) is preferred when the abscess is deep-seated, multiple, or located in eloquent (dangerous or critical) brain regions.
- Pros: minimally invasive, allows microbiological sampling, lower morbidity.
- Cons: may require repeated aspirations; incomplete evacuation possible.
- Craniotomy (bigger skull opening with or without abscess capsule excision) is performed for more superficial, single, or encapsulated abscesses causing significant compression.
- Pros: definitive drainage, removal of necrotic tissue and capsule if safe, lower recurrence rate.
- Cons: higher operative risk, possible neurological deficits, and longer recovery.

Image: Burr-hole aspiration of brain abscess (drainage through a small hole in the skull, around 1 cm in diameter)
In all cases, broad-spectrum intravenous antibiotics are continued postoperatively for several weeks, adjusted according to culture results.
Request a Neurosurgery Second Opinion
If you or a family member has been diagnosed with a brain or spinal infection — such as abscess, empyema, meningitis, ventriculitis, or post-surgical infection — an independent neurosurgical second opinion can help confirm the diagnosis, review imaging, and clarify treatment options.
- ✔ Send a short message describing the infection, available MRI/CT findings, and your main questions
- ✔ You’ll receive a reply within 24 hours with information on whether and how we can help — including the consultation fee and proposed time
- ✔ Only then, send your medical documentation (MRI/CT scans, lab results, hospital reports)
- ✔ During the video consultation, we will review the case in detail and answer all your questions clearly
Consultation fees typically range from $180–250, depending on the complexity of the infection and prior treatments.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for neurosurgical telehealth second opinions. Many patients request a review to confirm whether surgery is needed, to interpret MRI/CT results, or to understand next treatment steps.
Before contacting us, please read our Privacy Policy and Terms of Use.
How Treatment Decisions Are Made in Brain Abscess, Empyema, and Related Infections — When Surgery Is Needed and Which Procedure Is Chosen
How Treatment Decisions Are Made in Practice
Treatment decisions in intracranial infections are not based on a single rule such as lesion size or imaging appearance. They are based on a combination of clinical condition, imaging findings, type of infection, and dynamic evolution over time. The same finding on imaging may lead to a different decision depending on whether the patient is stable, improving, or deteriorating.
Key Factors That Influence the Decision
The most important factors include size of the lesion, mass effect, neurological status, and number and location of lesions. However, a critical distinction is whether the condition is a brain abscess or an empyema, because they behave differently. Response to antibiotic therapy in the first 48–72 hours is often a key decision point and may shift the approach from conservative to surgical.
When Surgery Is Considered
Surgery is considered when there is a larger collection, significant mass effect, neurological deterioration, or lack of response to antibiotics. Smaller abscesses without mass effect may sometimes be managed conservatively with close monitoring. In contrast, subdural empyema is more often treated surgically and urgently, because it tends to spread rapidly and compress the brain.
Which Surgical Procedure Is Chosen
The procedure depends on the type, location, and extent of infection. Brain abscesses are often treated with stereotactic or burr-hole aspiration, especially when located deep. In selected cases, open surgery may be required. Empyema, particularly subdural empyema, usually requires more aggressive surgical drainage, often via craniotomy, to achieve adequate decompression and removal of infected material.
Why Decisions May Appear Different Between Centers
Although general principles exist, decisions may appear different because they are individualized. Different teams may weigh clinical and radiological factors differently in each patient. This does not represent disagreement, but reflects the fact that these conditions require case-by-case assessment rather than rigid protocols.
Prognosis & Follow-Up of CNS Infections
Prognosis after brain abscess, empyema, or related CNS infection depends mainly on how early treatment begins, the patient’s neurological condition, the size and location of the infection, the causative organism, immune status, and the presence of complications. Outcome is worse when there is reduced consciousness, seizures, neurological deficit, marked edema, ventricular rupture, ventriculitis, hydrocephalus, venous thrombosis, or delayed treatment.
Mortality has decreased with modern imaging, antibiotics, intensive care, and neurosurgical drainage, but recovery can still be prolonged. Some patients recover well, while others may have persistent neurological deficits, cognitive changes, balance problems, or long-term seizure risk.
Follow-up usually includes repeat MRI or CT scans, monitoring of CRP and ESR, and clinical assessment. In spinal infections, follow-up also evaluates vertebral healing, spinal stability, and residual compression of the spinal cord or nerve roots.
Frequently Asked Questions About CNS Infections, Brain Abscess and Empyema
What are CNS infections such as brain abscess, subdural empyema and epidural empyema?
CNS infections are infections involving the brain, spinal cord, meninges, ventricles, epidural space, subdural space, or adjacent skull and spinal structures. In neurosurgical practice, the most important forms are bacterial brain abscess, subdural empyema, epidural empyema or abscess, ventriculitis, infected shunts or drains, vertebral osteomyelitis, discitis, and spinal epidural abscess. These conditions are different from simple systemic infections because pus, swelling, pressure, vascular involvement, or compression can directly injure nervous tissue. A brain abscess forms inside the brain, while empyema is pus in a space around the brain or spinal cord. Treatment depends on location, mass effect, neurological status, organism, source of infection, and whether surgery is needed.
Are brain abscess, subdural empyema or spinal epidural abscess contagious?
Brain abscess, subdural empyema, and spinal epidural abscess are usually not contagious in the usual sense. They most often develop when bacteria spread from another infection site, such as sinusitis, otitis, mastoiditis, dental infection, bloodstream infection, endocarditis, trauma, neurosurgical procedures, infected shunts, drains, or spinal infection. The patient’s underlying infection source may sometimes involve organisms that can spread in other contexts, but the abscess or empyema itself is not usually passed from one person to another. The more important clinical question is how bacteria reached the central nervous system and whether the source is still active. Identifying sinus, ear, dental, lung, heart, wound, urinary, or device-related infection is essential to prevent recurrence and guide antibiotics.
What symptoms suggest CNS infection, brain abscess or subdural empyema?
CNS infection may present with headache, fever, chills, nausea, vomiting, seizures, confusion, reduced consciousness, neck stiffness, or focal neurological deficits such as weakness, cranial nerve palsy, speech difficulty, sensory loss, or visual symptoms. Brain abscess often causes symptoms through inflammation, edema, mass effect, and irritation of the surrounding cortex. Subdural empyema may deteriorate rapidly because pus can spread widely over the brain surface and cause venous thrombosis or infarction. Spinal epidural abscess may cause severe back pain, radiculopathy, weakness, sensory loss, or bladder and bowel dysfunction. Symptoms are not always complete at the beginning. A patient may initially have headache or fever only, then worsen as pressure, edema, seizures, or neurological injury develop.
Which red flags in CNS infection, brain abscess or empyema require urgent hospital evaluation?
Red flags in suspected CNS infection include rapid worsening, new seizures, altered consciousness, severe or progressive headache, vomiting with signs of raised intracranial pressure, new weakness, speech disturbance, cranial nerve palsy, neck stiffness, or signs of brain herniation. In spinal infections, severe back pain with weakness, numbness, difficulty walking, or bladder and bowel symptoms is urgent because spinal cord or nerve root compression may become irreversible. Subdural empyema is particularly dangerous because it can spread quickly and compress the brain, often requiring urgent surgery. Brain abscess close to the ventricles is also high-risk because rupture into the ventricular system can cause ventriculitis or meningitis with rapid deterioration. These situations require immediate in-person emergency care, not routine telehealth review.
How are CNS infections such as brain abscess and empyema diagnosed?
Diagnosis of CNS infection requires combining clinical examination, laboratory tests, imaging, microbiology, and search for the infection source. CT or MRI determines whether the infection involves brain tissue, subdural or epidural spaces, ventricles, skull bone, spine, or spinal epidural space. MRI with contrast and diffusion-weighted imaging is especially useful for detecting pus collections and distinguishing abscess from other lesions. Blood tests may show inflammation, such as elevated CRP, ESR, fibrinogen, neutrophilia, or procalcitonin. Microbiological diagnosis may require blood cultures, swabs from sinus, ear or wound infection, CSF sampling when safe, abscess aspiration, or shunt/EVD sampling. ENT, infectious disease, radiology, neurosurgery, and critical care input may all be needed.
When is MRI better than CT for brain abscess, subdural empyema or CNS infection?
MRI is usually better than CT when doctors need to define the extent, stage, and exact location of CNS infection. MRI with contrast and diffusion-weighted imaging can better identify pus, cerebritis, abscess capsule, subdural empyema, epidural collections, ventriculitis, spinal epidural abscess, and associated edema. CT is often used first in emergencies because it is fast and widely available, and it can detect mass effect, hydrocephalus, hemorrhage, bone disease, and large collections. However, early cerebritis, small abscesses, posterior fossa infection, spinal infection, or subdural empyema may be better evaluated with MRI. Imaging must also answer practical surgical questions: is there mass effect, ventricular risk, multiloculation, spinal cord compression, or a collection that needs drainage?
Is lumbar puncture always safe in suspected CNS infection or brain abscess?
Lumbar puncture is not always safe in suspected CNS infection. It may help diagnose meningitis and identify an organism, but it can be dangerous when there is a brain abscess, empyema, mass effect, raised intracranial pressure, hydrocephalus, or risk of herniation. Removing cerebrospinal fluid below the brain in a patient with a mass lesion can worsen pressure gradients and cause neurological deterioration. For this reason, CT or MRI is often performed before lumbar puncture when focal deficits, seizures, altered consciousness, papilledema, or mass effect are suspected. If CSF sampling is unsafe, microbiology may come from blood cultures, sinus or wound cultures, abscess aspiration, or ventricular/shunt drainage. The decision must be individualized and safety comes first.
Can antibiotics alone cure a brain abscess or CNS infection?
Antibiotics alone can sometimes treat a brain abscess, but only in selected situations. Conservative treatment is more reasonable when the abscess is small, usually under about 2–2.5 cm, the patient is neurologically stable, there is no significant mass effect or raised intracranial pressure, the organism is known or likely to respond to antibiotics, and there is no ventricular rupture. Deep abscesses in critical brain regions may also be managed conservatively if surgery carries high risk. However, larger abscesses, multiloculated lesions, neurological deterioration, mass effect, uncertain diagnosis, poor antibiotic response, fungal abscess, foreign material, or risk of ventricular rupture usually require surgical aspiration or drainage. Conservative treatment always requires close clinical and repeat imaging follow-up.
How long are antibiotics needed for brain abscess, empyema or CNS infection?
Antibiotic duration for brain abscess, empyema, or CNS infection depends on the organism, location, surgical result, immune status, imaging response, and whether foreign material is present. Treatment often requires prolonged intravenous antibiotics, commonly several weeks, and may last 4–8 weeks or longer in complex cases. Empiric broad-spectrum therapy is started early, then adjusted according to cultures and sensitivity results from blood, CSF when safe, wound samples, abscess material, or infected hardware. Antibiotics must penetrate the CNS and cover likely pathogens, including streptococci, staphylococci, anaerobes, gram-negative bacteria, or atypical organisms depending on source and risk factors. Duration is not based only on time; follow-up MRI/CT, inflammatory markers, and clinical recovery guide the final decision.
When is surgery indicated for brain abscess or intracranial empyema?
Surgery is considered for brain abscess or intracranial empyema when infection produces significant mass effect, neurological deterioration, raised intracranial pressure, poor response to antibiotics, uncertain diagnosis, or risk of rupture into the ventricles. Brain abscesses larger than about 2.5–3 cm, multiloculated abscesses, superficial encapsulated lesions, fungal abscesses, abscesses with foreign bodies, infected shunts, drains, or bone fragments may require intervention. Subdural and epidural empyemas often need urgent drainage because pus in these spaces can compress the brain or spread quickly. Surgery also provides material for microbiological diagnosis, allowing targeted antibiotics. The decision is never based on size alone. A neurosurgeon must integrate imaging, clinical condition, infection type, source, organism, and evolution over time.
Why does subdural empyema usually require more urgent surgery than brain abscess?
Subdural empyema usually requires more urgent surgery than many brain abscesses because pus lies in the subdural space, where it can spread widely over the brain surface. Unlike a mature brain abscess, which may become partly encapsulated, subdural empyema often has less anatomical containment. It can rapidly compress the brain, provoke seizures, increase intracranial pressure, and cause venous thrombosis or secondary infarction. Antibiotics are essential, but they may not drain thick or multiloculated pus quickly enough. Burr holes can be insufficient if the collection is extensive, and craniotomy may be needed for adequate evacuation and decompression. This is why stable small brain abscesses can sometimes be observed with antibiotics, while subdural empyema is usually treated more aggressively.
What is the difference between aspiration and craniotomy for brain abscess?
Aspiration and craniotomy are different surgical strategies for brain abscess. Stereotactic or burr-hole aspiration uses a small opening and image guidance to drain pus and obtain material for culture. It is often preferred for deep abscesses, multiple abscesses, or lesions in eloquent brain regions where open surgery would carry higher risk. The disadvantage is that aspiration may be incomplete and sometimes must be repeated. Craniotomy creates a larger skull opening and allows more direct evacuation, removal of necrotic material, and sometimes capsule excision when safe. It may be preferred for superficial, single, encapsulated abscesses, large collections causing compression, or empyemas requiring decompression. The choice depends on location, size, capsule, neurological status, and surgical risk.
When is stereotactic aspiration preferred for brain abscess?
Stereotactic aspiration is often preferred for brain abscess when the lesion is deep, multiple, close to eloquent brain areas, or when the main goal is to drain pus and obtain microbiological diagnosis with lower surgical morbidity. It uses spatial navigation to guide the needle accurately into the abscess cavity through a small opening. This approach can reduce mass effect, identify the organism, and allow targeted antibiotic therapy. It is especially useful when open surgery would risk speech, movement, vision, or other critical functions. However, aspiration is not always definitive. Thick pus, multiloculated abscesses, recurrence, incomplete drainage, or failure to improve may require repeated aspiration or craniotomy. The surgical plan is adjusted according to response and imaging follow-up.
When is craniotomy preferred for brain abscess or subdural empyema?
Craniotomy is preferred when a brain abscess or empyema requires wide exposure, complete evacuation, decompression, or removal of infected material that cannot be adequately treated through a small opening. It may be chosen for superficial single abscesses with a mature capsule, large abscesses with significant compression, multiloculated collections, associated necrotic tissue, foreign bodies, or uncertain diagnosis. In subdural empyema, craniotomy is often needed because pus may be thick, widespread, and multiloculated over the brain surface. Burr-hole drainage can be insufficient if the collection is extensive or if decompression must be reliable. Craniotomy has greater operative exposure and potential risk, but it may provide better control when aspiration or small drainage is unlikely to solve the problem.
Do patients with brain abscess, empyema or CNS infection need anti-seizure medication?
Many patients with brain abscess, empyema, or CNS infection may need anti-seizure medication, especially if seizures occurred, if the infection irritates the cortex, if there is edema, hemorrhage, cortical scarring, or if surgery was performed near seizure-prone brain tissue. Brain abscess and subdural empyema can trigger seizures through inflammation, mass effect, vascular injury, and cortical irritation. Medication such as levetiracetam, phenytoin, or valproate may be used depending on the patient and local protocol. The duration is individualized. Some patients need temporary prophylaxis, while others remain at risk for later epilepsy if cortical damage, gliosis, infarction, or residual scarring persists. Seizure history, EEG, imaging, and neurological status help guide treatment.
When are steroids, mannitol or hypertonic saline used in CNS infection with brain swelling?
Steroids, mannitol, or hypertonic saline may be used in CNS infection when brain swelling, mass effect, or raised intracranial pressure threatens neurological function. Mannitol and hypertonic saline are antiedematous treatments used to reduce dangerous pressure in selected acute situations. Dexamethasone or other corticosteroids may reduce edema, but they are used carefully because inflammation is also part of the immune response and steroids can sometimes affect infection control or capsule formation. These treatments do not replace antibiotics or surgical drainage when pus collection requires evacuation. They are supportive measures used when swelling contributes to deterioration, herniation risk, or severe neurological symptoms. The decision depends on imaging, consciousness level, deficits, mass effect, and overall infection control strategy.
What is a shunt or EVD infection in CNS infection and how is it managed?
A shunt or EVD infection occurs when bacteria colonize implanted cerebrospinal fluid drainage systems, such as a ventriculoperitoneal shunt or external ventricular drain. This can lead to ventriculitis, meningitis, abscess formation, fever, altered consciousness, abnormal CSF findings, or worsening hydrocephalus. Management usually requires microbiological sampling of CSF from the device, intravenous antibiotics adjusted to cultures, and often removal or replacement of infected hardware. If the shunt remains infected, antibiotics alone may fail because bacteria can persist on the device surface. In some cases, an external ventricular drain is used temporarily while infection is treated, followed by later shunt reconstruction when CSF is sterile. Treatment requires neurosurgery, infectious disease, and critical care coordination.
Can ventriculitis occur after brain abscess rupture or infected shunt or EVD?
Yes. Ventriculitis can occur when infection spreads into the ventricular system, either from rupture of a brain abscess into the ventricles or from colonization of a shunt, EVD, or ventriculostomy catheter. This is a serious complication because infected cerebrospinal fluid can circulate through the ventricular system and meninges, causing rapid clinical deterioration, fever, altered consciousness, hydrocephalus, and abnormal CSF findings. Brain abscesses located near the ventricles are especially concerning because rupture can convert a localized infection into a much more diffuse and dangerous process. Management may require urgent antibiotics, CSF sampling, ventricular drainage, removal of infected hardware, and intensive monitoring. Prognosis depends on speed of diagnosis, organism, neurological condition, and infection control.
What is spinal epidural abscess and when does it require surgery?
Spinal epidural abscess is a collection of pus in the epidural space of the spine, where it can compress the spinal cord or nerve roots. It may occur with vertebral osteomyelitis, discitis, bloodstream infection, diabetes, immune suppression, invasive procedures, or other infection sources. Symptoms may include severe back pain, radicular pain, weakness, sensory changes, fever, and bladder or bowel dysfunction. Surgery is usually required when there is neurological deficit, spinal cord compression, rapid progression, instability, or failure of antibiotics. Conservative treatment may be considered in carefully selected stable patients without deficits, but close monitoring is essential. Delay can lead to permanent paralysis or disability, so new weakness or bladder symptoms require urgent hospital evaluation.
What is the prognosis after brain abscess, subdural empyema or CNS infection?
Prognosis after brain abscess, subdural empyema, or CNS infection depends on early diagnosis, neurological status at presentation, lesion size and location, organism, immune status, comorbidities, complications, and speed of effective treatment. Modern imaging, antibiotics, intensive care, and surgery have reduced mortality in brain abscess, but serious outcomes still occur. Some patients recover well, while others have residual weakness, cognitive problems, seizures, hydrocephalus, vascular injury, or chronic neurological deficits. Subdural empyema and ventriculitis can be more dangerous if diagnosis or drainage is delayed. Prognosis is best when treatment begins before severe deterioration, herniation, ventricular rupture, or spinal cord compression. Follow-up imaging and inflammatory markers are needed to confirm resolution and detect recurrence.
How can recurrence of brain abscess or CNS infection be prevented?
Recurrence of brain abscess or CNS infection is prevented by treating both the intracranial or spinal infection and the original source. Antibiotics must be long enough and targeted to the organism when cultures are available. Follow-up MRI or CT should confirm that the abscess, empyema, edema, or spinal infection is resolving. ENT sources such as sinusitis, otitis, mastoiditis, dental infection, skull base defects, CSF leakage, infected bone, foreign bodies, shunts, drains, or retained fragments must be addressed when present. Systemic sources such as endocarditis, lung infection, urinary infection, skin infection, diabetes, immune suppression, or sepsis also need management. Recurrence is more likely when the source remains active, hardware stays infected, or imaging follow-up is incomplete.
Why can treatment decisions differ between centers in brain abscess and empyema?
Treatment decisions in brain abscess and empyema can differ between centers because these conditions are individualized and dynamic. The same MRI finding may be treated conservatively in one patient and surgically in another depending on neurological status, mass effect, lesion size, location, number of collections, organism, source of infection, comorbidities, and response to antibiotics in the first 48–72 hours. Brain abscess and subdural empyema also behave differently, so one rule cannot apply to all infections. Some teams may prefer early aspiration for diagnosis, while others may observe a small stable abscess with close imaging. Differences do not always mean disagreement. They often reflect different weighting of surgical risk, antibiotic response, and urgency in a specific patient.
Can a telehealth second opinion help with brain abscess, empyema or CNS infection?
A telehealth second opinion can help in non-emergency cases of brain abscess, empyema, spinal infection, ventriculitis, or post-surgical CNS infection by reviewing MRI or CT images, hospital reports, laboratory results, culture data, and the proposed treatment plan. It can clarify whether surgery may be needed, whether the imaging pattern is consistent with abscess or empyema, whether the collection is responding to treatment, and what questions should be discussed with the local team. However, telehealth is not appropriate for urgent deterioration, new seizures, weakness, reduced consciousness, herniation signs, or spinal cord compression. Those require immediate in-person emergency care. The role of second opinion is to improve understanding and decision-making, not delay urgent treatment.