Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 10, 2026
Who this page is for
This page is for patients who—despite a thorough work-up (e.g., MRI/CT) that shows no clear cause or moderate degenerative changes that may be incidental or don’t fully match your symptoms—and despite appropriate initial treatment—still have back pain persisting beyond 6–12 weeks.
If you are in this situation and want a detailed evaluation, you can request an online consultation with our specialist.
When patients usually seek a second opinion for low back pain
- Low back pain persists beyond 6–12 weeks despite appropriate treatment
- Pain keeps returning after temporary improvement
- MRI or CT shows disc bulging, degeneration, or findings that do not fully match symptoms
- You are considering injections, procedures, or surgery
If this reflects your situation, a focused telehealth review can clarify the true pain generator, what treatments are reasonable, and what is — and is not — indicated in your case: Request Consultation
Low Back Pain — Quick Summary (Read This First)
- Persistent low back pain usually continues not because treatment is wrong, but because the exact cause has not been identified. The label “low back pain” or “sciatica” does not explain what structure is actually responsible for symptoms.
- Most patients are treated based on imaging findings that may not be the true source of pain. MRI often shows disc bulging or degeneration that can be incidental, while real pain generators in joints, ligaments, muscles, or nerves remain unrecognized.
- Low back pain rarely comes from a single structure. In many cases, multiple pain generators coexist, which is why standard one-directional treatments often fail.
- The exact pain generator is usually very small and specific. Pain typically arises from a localized structure (often less than 1 cm), not from the entire spine or all visible degenerative changes.
- Different causes of low back pain require completely different treatments. Disc herniation, facet joint syndrome, sacroiliac dysfunction, piriformis syndrome, and myofascial pain may produce similar symptoms but need different therapeutic approaches.
- Imaging alone is not sufficient for diagnosis in many patients. A detailed clinical evaluation, including pain mapping and functional testing, is often necessary to identify the true source.
- Contributing factors frequently maintain or amplify pain. Mechanical overload, prolonged sitting, poor posture, metabolic factors, inflammation, and reduced physical conditioning can all prevent recovery.
- This is why many standard treatments provide only temporary or no relief. Treatment may be partially correct, but incomplete if the main generator or contributing factors are not addressed.
- Most cases of persistent low back pain can improve when the correct diagnosis is made. Once the true pain generator is identified, treatment can be targeted and often leads to meaningful and lasting improvement.
- Surgery is required only in a small percentage of patients. The majority of cases can be managed with precise, non-surgical treatment when the correct mechanism is understood.
Most readers benefit from reviewing this Quick Summary together with sections on Common Causes of Low Back Pain, Diagnostic Approach, Pain Contributing Factors, and Treatment Options. These sections explain in detail how different pain mechanisms are identified and why treatment must be tailored to the exact cause.
This page is not mainly about a first episode of low back pain. It is written for patients whose low back pain has persisted beyond the expected recovery period, has returned repeatedly, or has not improved despite medication, physical therapy, injections, or reassurance based on MRI findings. In these cases, the key question is no longer “what is low back pain?” but “which exact structure is still generating pain, and why have previous treatments failed?”
Contents
- Who this page is for
- Low Back Pain Quick Summary
- Why Pain Persist Despite Treatment
- What is Low Back Pain?
- Key Facts About Low Back Pain
- Anatomy of the Spine
- 🎯 Find the Exact Pain Source
- Why Diagnosis Is Too General
- Common Causes of Low Back Pain
- Herniated Disc & Radiculopathy
- Facet Joint Syndrome
- Sacroiliac Joint Dysfunction (SIJ)
- Piriformis Syndrome
- Myofascial Pain
- Autoimmune/Metabolic Disorders
- Referred Pain from Other Organs
- Diseases That Mimic Disc Pain
- Diagnostic Approach
- Pain Contributing Factors That Should Also Be Diagnosed
- Online Consultations & Pain Mapping
- Treatment Options Overview
- Minimally Invasive Surgery
- Ineffective General Treatments
- Success Rates & Lasting Relief
- Conclusion: Solving the LBP Epidemic
- Start Telehealth Consultation
- FAQ – Low Back Pain
- Red Flags – Not for These Situations
- Additional Information (LBP)
Why Low Back Pain Treatment Often Fails — What Is Commonly Missed
In many patients, low back pain persists not because treatment is ineffective, but because key elements are missed.
The exact pain source is not precisely identified, and symptoms are often attributed to imaging findings rather than the true generator (facet joints, sacroiliac ligaments, muscles, fascia, or nerve irritation).
The underlying process is not clearly defined — inflammation, mechanical irritation, instability, or nerve sensitization require different treatment strategies.
Contributing factors continue to maintain pain, including mechanical overload, prolonged sitting, asymmetrical loading, but also metabolic factors, low-grade inflammation, and reduced tissue recovery capacity.
Because of this, treatment may be partially correct but incomplete, leading to persistent or recurrent pain.
What is Low Back Pain
Low back pain is one of the most common health complaints worldwide. Almost everyone experiences it at some point in life — but the reasons behind it can be very different.
A single phrase like “low back pain” or “sciatica” is not a precise diagnosis because it only indicates the location of the pain, not its cause. For effective treatment, it is essential to identify the exact anatomical source of the pain.
The pain is never coming from the whole spine, but from a very specific spot — often no larger than 1 cm. Finding this exact source is the only way to achieve lasting relief.

Part of our Low Back Pain & Sciatica — Patient Hub.
Go to Hub →
🎯 Low Back Pain — Different Causes, One Goal: Find the Exact Source
“Low back pain” is not a precise diagnosis — it’s a label for many conditions. Effective therapy starts when we identify the exact anatomical pain generator (often a spot < 1 cm): disc, nerve root, facet joint, sacroiliac joint, piriformis, ligament, or myofascial trigger.
Imaging alone is not enough. MRI frequently shows changes that are not the cause of pain, while real irritation in soft tissues can be invisible. That’s why the most important step is a detailed clinical interview and functional testing — which we can perform during an online (telehealth, remote) video consultation.
Before the consultation, the doctor reviews your medical records. During the video visit we:
- ask targeted questions about pain location, radiation, and triggers,
- guide you through specific movements and posture tests,
- show you how to press precise points (lumbar paraspinals, SI joint, piriformis, facet line) to map pain reactions,
- use your responses (pain ↑/↓) to pinpoint the pain generator and exclude look-alike causes.
Once the source is identified, treatment becomes specific — usually a targeted medication plan with close adjustments during the first 1–2 weeks. If needed, we add recommendations for the exact type of image-guided intervention (ultrasound, fluoroscopy, or CT) to deliver therapy precisely to the affected structure. Most patients who fit the profile described on this page start to improve once treatment is finally tailored to the true pain generator, even if previous general therapies failed. In practice, the first consultation defines this direction and the initial 1–2 week plan, while brief follow-up messaging allows fine-tuning and confirmation that we are on the right track.
Most low back pain cases do not require surgery. When surgery is indicated, it is typically minimally invasive. What truly makes the difference is not a generic “back exam”, but a conversation with a specialist who knows the anatomy of pain and can translate that knowledge into the right therapy.
Anatomy of the Spine
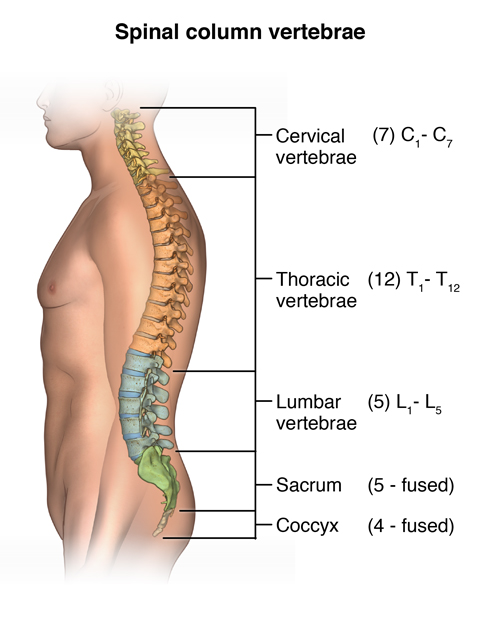
Image: Anatomy of the spine. Learn more on our Pain Anatomy page.
The human spine allows us to stand upright and move freely. It is composed of 33–35 vertebrae with discs in between, acting as shock absorbers.
The spine has three main regions:
- Cervical (neck region)
- Thoracic (mid-back)
- Lumbosacral (lower back and sacrum)
Muscles attach to the spine externally and allow movement. Inside the spinal canal lies the spinal cord and the roots of spinal nerves, which carry signals to and from the body.
Sometimes diseases of the spine create pressure on a nerve root, patients often feel pain, tingling, or weakness radiating along the nerve. For example, a herniated disc between the 4th and 5th lumbar vertebrae can compress the L5, and sometimes the L4, nerve root, causing pain in the lumbosacral region and leg — often accompanied by numbness in the toes and weakness of the calf muscles.
Although disc herniation is the best-known generator of low back pain, most cases are not generated by a herniated disc. In the majority of people, MRI scans show degenerative disc changes — however, the real truth is that these changes are not the actual source of pain.
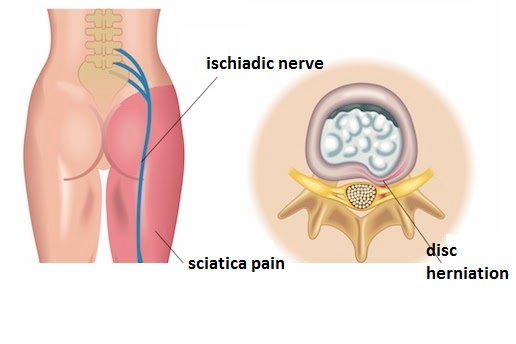
Image: Herniated disc between the 4th and 5th lumbar vertebrae can compress the L5, and sometimes the L4, nerve root, causing pain in the lumbosacral region and leg
Why “Low Back Pain” Is Too General a Diagnosis
Low back pain is extremely common. While many people experience only occasional discomfort, others live with constant or recurring pain that significantly affects their quality of life.
In many cases, patients receive vague labels such as lumbago, sciatica, spondylosis, or back rheumatism. These terms are not precise diagnoses. They are often enough to justify temporary treatments like painkillers or physical therapy, but if the pain persists, the real source must be identified.
It is never the “whole spine” or all degenerative changes seen on an MRI that provoke pain. Instead, the pain always comes from one or more specific points — often no larger than 1 cm. The lumbosacral region has around 30 potential pain generators. Only with detailed knowledge of pain anatomy can we target the true source and apply effective therapy.
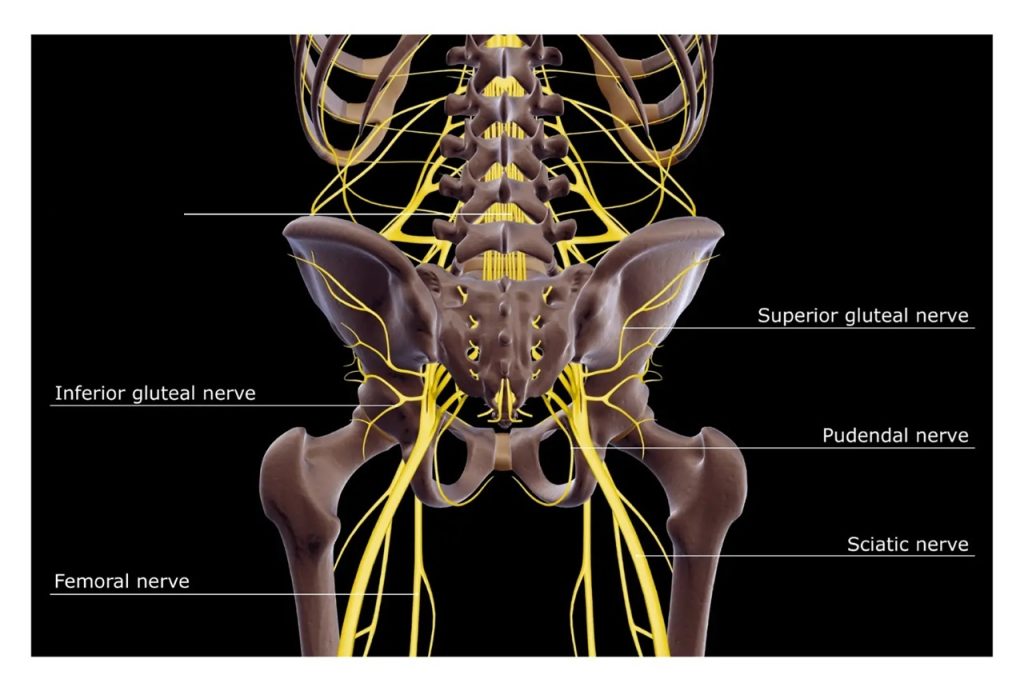
Image: This illustration shows only some of the many structures that can be a source of pain. All of them may present with the same symptoms, such as lumbago or sciatica. However, they must be precisely diagnosed because their treatments differ.
Common Causes of Low Back Pain
Herniated Disc and Radiculopathy
When the soft part of the disc protrudes and presses on a nerve root, it can produce sharp, radiating pain (sciatica).
Facet Joint Syndrome
Small joints between vertebrae may become unstable and/or inflamed, causing localized or radiating pain.
Sacroiliac Joint Dysfunction
Inflammation or instability of the SI joint often produces pain in the lower back, buttocks, and sometimes the thigh. Normal images of the sacroiliac joint do not rule out its structures as potential sources of pain (such as ligaments and their attachments, attached muscles, and nearby passing nerves).
Piriformis Syndrome
A tight piriformis muscle can compress the sciatic nerve, mimicking herniated disc symptoms.
Myofascial Pain
Inflammation and spasm in different paraspinal muscles, ligaments, or fascia can trigger pain, but are often overlooked in standard examinations. Repetitive strain, poor posture, or sudden movement can injure supportive tissues around the spine.
Autoimmune or Metabolic Disorders
Conditions such as rheumatoid arthritis or osteoporosis can involve the spine and present as back pain.
Referred Pain from Other Organs
Kidneys, uterus, ovaries, and intestines can sometimes create pain that feels like it comes from the spine.
Diseases of the Low Back That Mimic Herniated Disc Pain
Several conditions produce pain that looks identical to sciatica from a herniated disc. Examples include:
- Piriformis muscle syndrome
- Obturator nerve entrapment
- Facet joint syndrome
- Sacroiliac joint inflammation
- Ligament inflammation or tension
- Entrapment neuropathies
- Myofascial trigger points
In these cases, MRI scans may be normal, or they may show a disc herniation that is not actually causing pain. This is why many disc surgeries fail to relieve symptoms — the disc was not the real source of pain.
Diagnostic Approach
MRI and CT scans are valuable, but they do not always reveal the true pain generator.
The most important step is a detailed conversation with the patient, including:
- History of symptoms
- Pain mapping (location, radiation, triggers)
- Movement and pressure tests during the exam (most of which patients can even perform during a video consultation).
In everyday practice, we often encounter situations where all pathological changes found on a spinal MRI are cited as the cause of pain. However, a detailed physical exam or even a video consultation often reveals that they are not the true source. These findings may include discopathy, spondylotic changes (especially diffuse ones), disc bulging, hypertrophy of the ligamentum flavum, mild listhesis, osteophytes, moderately enlarged facet joints, and others. Patients—and frequently their doctors—tend to assume that these findings explain the pain. Once the “cause” is believed to be identified, further investigation is often abandoned. By investigation, this primarily refers to an examination by a specialist with expertise in pain anatomy—someone who understands the possible causes of low back pain and knows how to pinpoint them.
Sometimes the next step is to use diagnostic blocks, which can also have a therapeutic effect. These procedures make sense only after a specialist narrows the problem to one or two likely structures. A diagnostic block cannot identify the cause of pain on its own; it simply confirms or excludes a hypothesis that was already formed during the clinical evaluation. When correctly indicated, these targeted tests—such as facet, sacroiliac, myofascial trigger-point, or selective nerve-root blocks—can reveal the true pain generator and, in many cases, provide meaningful relief at the same time. In many pain clinics, the decision about which structure to block is based more on the routine list of available procedures than on a detailed analysis of the actual pain generator. As a result, patients sometimes receive an injection that is technically correct but diagnostically misplaced — simply because the underlying mechanism was never truly identified.
MRI and CT imaging are indispensable for diagnosing conditions that truly cause back pain or sciatica—such as significant disc herniation, spinal stenosis with nerve-root compression, tumors, angiomas (e.g., vertebral hemangiomas), cysts, infections, spinal malformations, segmental instability, and injuries. Electrophysiological and laboratory tests can also detect various neurological diseases that may lead to spine pain.
Low back pain can also occur as part of certain psychiatric conditions. There are also non-organic or feigned presentations of low back pain, which a physician experienced in the anatomy of pain can usually recognize and rule out.
This page does not focus on those conditions, because in most such cases the combination of clinical presentation, neurological deficits, and imaging findings establishes the diagnosis before low back pain becomes chronic as the leading symptom.
Artificial intelligence can also support the process by analyzing complex data, but clinical expertise remains essential.
Sometimes, the real source of pain becomes clear only after diagnostic and therapeutic interventional procedures. In properly selected cases where the pain generator is confirmed and treated directly, most patients experience durable improvement.
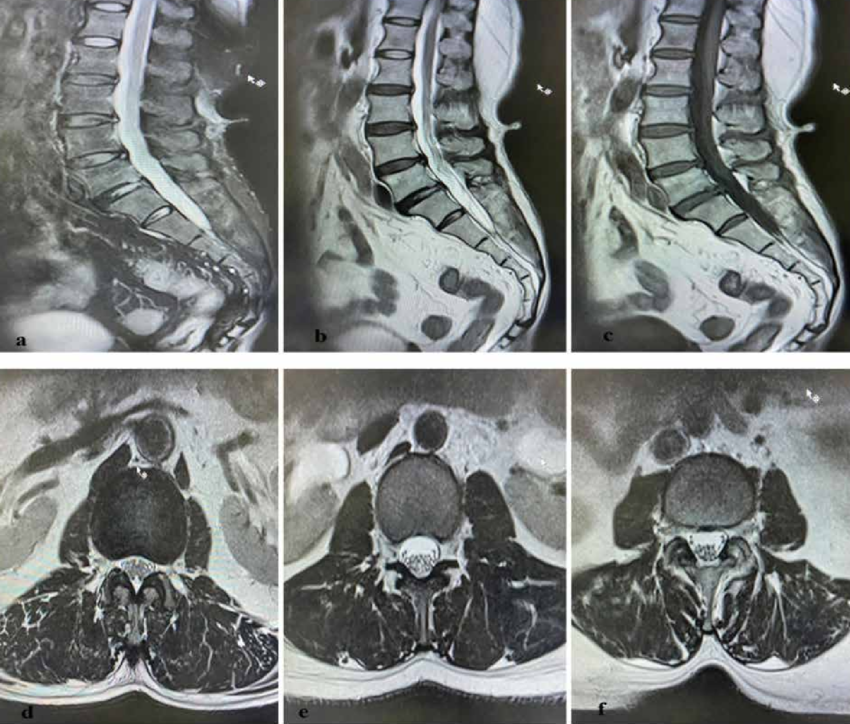
Image: MRI of the lumbar spine may show moderate degenerative changes that are actually not the cause of low back pain. The real reason can be inflammation of posterior ligament attachments of the sacroiliac joints, which are not visible on MRI.
Pain Contributing Factors That Should Also Be Diagnosed in Back Pain and Sciatica
In patients with persistent back pain and sciatica, treatment should not focus only on the primary anatomical pain generator. It is also important to identify additional factors that can maintain pain, increase sensitivity, delay recovery, or reduce the effectiveness of otherwise appropriate treatment.
- Mechanical overload and daily habits — prolonged sitting, poor posture, repetitive bending, lifting, or asymmetrical loading may continue to irritate already sensitized structures. Biomechanical factors such as leg length discrepancy, pelvic tilt, or degenerative conditions of the hip, knee, or foot joints may further alter load distribution and contribute to persistent pain.
- Reduced physical activity and deconditioning — loss of strength, endurance, and spinal stability often develops after long-lasting pain and makes recovery more difficult
- Metabolic factors, pro-inflammatory diet and low-grade inflammation — obesity, insulin resistance, chronic inflammation, and processed/high-sugar diet increase pain sensitivity and impair recovery
- Nutritional deficiencies — low levels of vitamin D, vitamin B12, magnesium, or iron may contribute to nerve dysfunction and slower healing
- Vitamin-related factors — both deficiency and excess of vitamin B6 may contribute to burning pain, tingling, or hypersensitivity
- Sleep disturbance and pain cycle — poor sleep increases pain perception and reduces recovery capacity
- Stress and increased muscle tone — stress does not cause the pain, but increases muscle tension and nervous system reactivity, helping maintain symptoms
- Central sensitization — in long-standing pain, the nervous system may become more reactive, amplifying pain signals even when the original irritation is reduced
- Medications and long-term drug effects — certain medications and treatment patterns may contribute to persistent symptoms or altered pain processing. For example, statins may be associated with muscle pain in some patients; prolonged use of analgesics, especially opioids, may lead to increased pain sensitivity (opioid-induced hyperalgesia); repeated corticosteroid exposure may affect tissue balance and recovery; and polypharmacy can alter symptom perception without addressing the underlying mechanism.
- Other medical conditions and comorbidities — diabetes, thyroid disorders, autoimmune diseases, fibromyalgia, osteoporosis, and chronic inflammatory conditions may increase pain sensitivity and reduce treatment response
These factors should be identified and treated, but they should not replace the central task: the primary anatomical source of pain must still be correctly diagnosed and treated. In most patients, meaningful improvement requires addressing both.
Online Consultations & Pain Mapping
Video consultations allow a specialist to perform targeted pain analysis remotely.
During the session:
- Patients describe their sensations in detail.
- They are guided to press or move in specific ways.
- Their responses (pain increase or decrease) help identify the generator.
This approach often matches the accuracy of an in-person exam. It provides fast access to expertise without traveling, especially valuable for international patients. Online consultation is already widely used in the developed world, and that is why it has many synonyms such as video consultation, virtual consultation, teleconsultation, telehealth consultation, telemedicine consultation, remote consultation, online doctor visit, virtual doctor visit, online doctor appointment, online medical advice, ask a doctor online, doctor chat online, video call with a doctor, and online second opinion.
Online pain consultation for low back pain in detail
Schematic explanation of the video consultation for low back pain
Answers to questions about the process and success of video consultations for low back pain
Treatment Options for Low Back Pain: Medications, Interventions, and When to Consider Surgery
Targeted Medication Strategy
Carefully selected and properly adjusted medications for the true generators of low back pain can reduce symptoms within days. In most cases this includes a combination of anti-inflammatory medication (NSAIDs or a short corticosteroid course), a neuropathic pain agent (such as gabapentin or pregabalin) when the nerve component is present, and in some cases an SNRI or tricyclic agent when the pain pattern suggests a mixed nociceptive–neuropathic mechanism. Short-term muscle relaxants are added only if protective spasm prevents normal movement.
The key is introducing the right combination early and adjusting it over several weeks — because even long-lasting or previously “medication-resistant” pain often improves once the correct targets are treated.
As the dominant pain generator becomes clearer, these medications are adjusted over 4–8 weeks. If pain remains under control for about six weeks, the improvement is often long-lasting.
Image-Guided Interventions & Local Injections
When medications are not enough, precise injections or procedures can directly target the pain generator. Modern methods use ultrasound, fluoroscopy, or CT guidance — unlike blind “blocks” that often miss the target. These interventions typically include medications that often breaks the cycle of inflammation and mechanical irritation as well as starting regeneration (steroids, local anesthetics, PRP) and allows medications to work more effectively.
Physical Therapy, Rehabilitation & Osteopathy
When medications are not enough, precise injections or procedures can directly target the pain generator. Modern methods use ultrasound, fluoroscopy, or CT guidance — unlike blind “blocks” that often miss the target. These interventions typically deliver targeted agents that break the cycle of inflammation and mechanical irritation — and in some cases stimulate early regeneration — such as corticosteroids, local anesthetics, or PRP. This targeted approach often allows systemic medications to work more effectively.
Treating Associated Conditions
Managing associated conditions such as metabolic disorders, poor posture, bad nutrition, obesity, rheumatic and other autoimmune disorders and psychiatric problems are often an important part of therapy. Addressing these factors can significantly support the treatment of the primary pain generator and help prevent the pathological process from redeveloping after the pain has been resolved.
Pain Relief for Back Pain Caused by Prolonged Sitting
The solution for pain provoked by prolonged sitting is to identify which parts of the spine and back are overloaded and become painful due to inflammation, stretching, or spasm (these are not the same in every person). Those areas can then be relieved by adjusting the chair and using specially designed seat cushions that unload exactly the overloaded low back segments. The size and firmness of these cushions are often recommended after consultation, based on the specific cause of pain and the patient’s body dimensions.
Minimally Invasive Surgery
Only a small percentage of patients with low back pain require surgery. When needed, procedures are usually minimally invasive, aimed at relieving severe nerve compression or spinal instability.

Image: Diagnostic and therapeutic pain procedures guided by ultrasound in different pain syndromes
General Treatments That Are Often Not Enough for Chronic Low Back Pain
Many therapeutic approaches are commonly recommended for low back pain, but they are usually insufficient if the exact source of persistent LBP is not identified. Examples include:
- General back exercises — some exercises may relieve one type of pain but worsen another.
- General Physical Therapy, Rehabilitation & Osteopathy — when these methods are applied generally for “low back pain” and not directed at the actual cause.
- Waiting for pain to improve only with weight loss — reducing weight supports overall health, but it does not replace identifying the pain generator. On the other hand, losing weight can be difficult if movement is limited by LBP. Actually systemic inflammation related to diet can amplify low back pain in selected patients. In some individuals, a high intake of refined sugars and carbohydrates contributes to a pro-inflammatory state, which may worsen pain sensitivity and delay recovery — even when imaging findings are mild or unchanged. Early dietary normalization can have an anti-inflammatory effect even before significant weight loss occurs. This aspect is addressed individually during consultation, together with appropriate specialist guidance.
- Treating osteoporosis as the main generator of pain — bone density matters, but most back pain originates from discs, joints, or soft tissues.
- Generic physical therapy sessions — when not tailored to the true cause, they usually provide only temporary relief.
- Psychiatric treatment for depression or anxiety — mood problems often result from months or years of uncontrolled pain, not the other way around.
- Shoe inserts, supplements, massage, relaxation therapy, aromatherapy, anti-inflammatory diets, and “alternative” methods — they may help some people, but without diagnosing the pain source, results are usually limited. The biggest problem is when strong marketing takes advantage of patients’ desperation — promoting well-presented solutions that specialists can immediately recognize as inappropriate for the real cause.
Did these types of treatments help some patients with LBP?
Yes — and such patients will often recommend them to others. But their situation may have been quite different from yours: they may have had an acute episode where natural healing played the main role, the treatment may have coincided with the real cause of their pain, or they may have received additional specific therapy alongside.
If you are being treated under the label “LBP” but no one has explained what exactly hurts (for example, a piriformis muscle spasm, a sacroiliac ligament, or a facet joint), it may be time to seek a second opinion.
There are several common reasons for poor therapeutic outcomes in the treatment of chronic pain, which are often seen in patients with low back pain.
Success Rates & When Relief Becomes Lasting
When the exact pain source is identified and treated, most patients achieve long-term relief.
Even pain lasting for years can improve significantly once the real generator is targeted.
Failure usually happens when treatment addresses symptoms instead of the underlying structure.
Conclusion: How This Page Can Contribute to Solving the Epidemic of Persistent LBP
This page may appear to be just an exhaustive list of reasons, but its true purpose is to provide a framework for understanding the numerous possible complex combinations that drive the majority of persistent low back pain.
The global LBP epidemic exists because standard treatments often miss the subtle „interplay“ between biology and lifestyle. For instance, a constitutionally weaker ligament might remain asymptomatic for years, only to become chronically inflamed when triggered by a specific metabolic shift (like insulin resistance caused by bad nutrition) and a static occupational load.
Listing and sorting almost all possible factors on this page allows us to map how they overlap. Chronic pain is rarely a single „broken part“; it is a unique cocktail of triggers. What looks like a mere list is actually a diagnostic map designed to identify these hidden intersections that standard protocols overlook. This is why two patients with similar MRI findings may require completely different treatment strategies.
Identifying these specific combinations—such as the link between tissue quality, systemic inflammation, and physical strain—is the only way to solve pain that has resisted conventional care. We don’t just follow a general recipe; we analyze the „consistency“ of your unique story to find the exact combination that needs to be treated.
Start Your Telehealth Consultation with a Pain Specialist
If your pain treatment has failed or you’re unsure what to do next — don’t wait. A detailed telehealth consultation can help identify the exact cause of your pain, even if previous therapies didn’t work.
- ✔ First, send a short message describing your problem
- ✔ You’ll receive a reply within 24 hours if and how we can help — including the consultation cost and a suggested time
- ✔ Only then, you can send your medical documentation
- ✔ The video consultation is followed by a written report and follow-up questions (up to 10 days)
- ✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Consultation fees typically range from $180–250, depending on the complexity of your case.
This is within the usual range for specialist telehealth consultations worldwide. Thousands of patients worldwide already use telehealth consultations for second opinions — it’s safe, accepted, and effective.
Before contacting us, please read our Privacy Policy and Terms of Use.
Frequently Asked Questions About Persistent and Chronic Low Back Pain
Why does persistent low back pain continue despite treatment?
Persistent low back pain often continues because treatment is directed at a general label rather than the true pain generator. Terms such as low back pain, lumbago, sciatica, degeneration, or disc bulge do not explain which structure is actually responsible for symptoms. The source may be a disc, nerve root, facet joint, sacroiliac joint, ligament, piriformis muscle, myofascial trigger point, or several structures acting together. Treatment may provide only temporary relief if it reduces symptoms but does not address the underlying mechanism, such as inflammation, mechanical overload, instability, muscle spasm, or nerve sensitization. The key step is precise diagnosis before repeating more general therapy.
What is chronic low back pain?
Chronic low back pain usually means pain in the lower back that persists beyond the expected healing period, commonly longer than 6–12 weeks. It does not describe one specific disease. It is a clinical situation in which the original trigger may have improved, but pain continues because one or more structures remain irritated or sensitized. Chronic low back pain may come from discs, facet joints, sacroiliac joints, muscles, ligaments, nerve roots, or referred sources. In many patients, additional factors such as prolonged sitting, deconditioning, metabolic inflammation, poor sleep, stress-related muscle tone, or central sensitization maintain symptoms. Effective treatment requires identifying the dominant pain generator and the factors that keep it active.
Why can chronic low back pain persist even when MRI findings are mild?
Chronic low back pain can persist even when MRI findings are mild because MRI shows anatomy, but not always the active pain process. Disc bulges, degeneration, facet arthropathy, mild listhesis, and ligament thickening may be incidental or only part of the story. At the same time, important pain generators may be poorly visible or invisible on routine MRI. These include sacroiliac ligament irritation, facet capsule inflammation, myofascial trigger points, piriformis-related irritation, small enthesopathies, or nerve sensitization without clear compression. This is why MRI must be interpreted together with pain location, movement triggers, sitting tolerance, walking response, neurological signs, and targeted clinical testing.
Can low back pain come from a small pain generator not visible on MRI?
Yes. Low back pain can come from a very small anatomical source that may not be visible on MRI. The active pain generator may be a facet joint capsule, sacroiliac ligament, piriformis muscle, lumbar paraspinal trigger point, nerve root, or soft-tissue attachment. In some patients, the painful structure is very localized, while MRI shows broader age-related or degenerative findings that are not the real cause. This explains why a patient may have severe pain despite a “normal” scan, or why another person with obvious MRI degeneration may have little pain. Pain mapping, movement tests, pressure tests, and sometimes diagnostic blocks are needed to identify the responsible structure.
Why is “lumbago” or “sciatica” not enough as a diagnosis?
“Lumbago” and “sciatica” describe symptoms, not the exact cause. Lumbago usually means pain in the lower back, while sciatica describes pain radiating toward the leg. Neither term identifies whether the source is a disc herniation, nerve-root irritation, facet joint, sacroiliac joint, piriformis syndrome, ligament inflammation, myofascial trigger point, or another structure. This matters because each mechanism requires a different treatment strategy. A patient with sacroiliac joint pain does not need the same treatment as a patient with true lumbar radiculopathy from disc compression. When chronic low back pain is treated only under a broad label, treatment often becomes too general and incomplete.
What are the most common hidden causes of chronic low back pain?
Hidden causes of chronic low back pain include structures that are frequently missed when treatment focuses only on MRI findings. Common examples include facet joint pain, sacroiliac joint dysfunction, sacroiliac ligament irritation, piriformis syndrome, myofascial trigger points, paraspinal muscle spasm, entrapment neuropathies, and nerve-root irritation that does not clearly match a large disc herniation. In some patients, several generators coexist. Contributing factors may include prolonged sitting, asymmetrical loading, weak stabilizing muscles, obesity, insulin resistance, low-grade inflammation, vitamin deficiencies, poor sleep, stress-related muscle tone, and central sensitization. The hidden cause is often not a rare disease, but a missed combination of local anatomy and maintaining factors.
Can severe lower back pain have different causes in different patients?
Yes. Severe lower back pain can have very different causes in different patients, even when the pain intensity feels similar. In one patient, severe pain may come from an acute disc herniation irritating a nerve root. In another, it may come from a facet joint, sacroiliac joint, muscle spasm, ligament inflammation, vertebral fracture, infection, tumor, or referred pain from another organ. Severe pain does not automatically mean surgery is needed, but it does require careful assessment. The pattern matters: whether pain radiates to the leg, worsens with movement, appears at night, follows trauma, causes weakness, or is associated with fever, weight loss, or bladder symptoms.
How can doctors tell if low back pain is from a disc, facet joint, or sacroiliac joint?
Doctors distinguish disc, facet, and sacroiliac joint pain by combining history, pain location, radiation pattern, movement triggers, examination, imaging, and sometimes diagnostic blocks. Disc-related pain may worsen with sitting, bending, coughing, or nerve-root tension and may radiate down the leg if radiculopathy is present. Facet joint pain often worsens with extension, rotation, or standing and may refer to the buttock or thigh. Sacroiliac joint pain often localizes near the posterior pelvis and may worsen with asymmetrical loading, turning in bed, standing on one leg, or prolonged sitting. MRI can help, but it is not enough by itself. The clinical pattern must match the suspected source.
Can sacroiliac joint dysfunction mimic lumbar disc pain?
Yes. Sacroiliac joint dysfunction can mimic lumbar disc pain because it may cause lower back pain, buttock pain, groin discomfort, and pain spreading into the thigh. Patients are sometimes told the problem is disc-related because MRI shows lumbar degeneration or a mild disc bulge, even when the sacroiliac joint or its ligaments are the dominant pain generator. Sacroiliac pain is often influenced by asymmetrical loading, prolonged sitting, standing, walking, stairs, turning in bed, or transitions from sitting to standing. Normal imaging does not fully exclude sacroiliac-related pain. Clinical provocation tests, precise pain mapping, and in selected cases diagnostic sacroiliac blocks may clarify the diagnosis.
Can piriformis syndrome mimic sciatica from a herniated disc?
Piriformis syndrome can mimic sciatica because the piriformis muscle lies close to the sciatic nerve and may irritate it through spasm, inflammation, or mechanical compression. Symptoms may include buttock pain, pain radiating down the back of the thigh, tingling, or discomfort that worsens with sitting, hip rotation, or prolonged walking. Unlike true lumbar radiculopathy, the source is outside the spinal canal, so lumbar MRI may be normal or may show disc changes that are not the true cause. Diagnosis depends on symptom pattern, hip and buttock examination, pressure sensitivity, movement testing, and exclusion of lumbar nerve-root compression. Treatment is different from disc herniation treatment.
Can myofascial pain cause chronic low back pain?
Yes. Myofascial pain is a common cause of chronic low back pain and is often overlooked. It arises from muscles, fascia, and trigger points in the lumbar paraspinals, quadratus lumborum, gluteal muscles, piriformis, or related soft tissues. Pain may be localized or referred to the buttock, hip, pelvis, or thigh. It can develop after repetitive strain, prolonged sitting, poor posture, sudden movement, muscle imbalance, or protective spasm around another painful structure. Myofascial pain may not appear clearly on MRI. It is diagnosed through pain mapping, pressure testing, movement response, and clinical pattern recognition. Treatment may include targeted medication, unloading, trigger-point therapy, guided rehabilitation, and correction of maintaining factors.
Why do physical therapy and exercises sometimes fail in persistent low back pain?
Physical therapy and exercises sometimes fail because the program does not match the true pain generator. General back exercises may help one mechanism but worsen another. For example, flexion-based exercises may aggravate some disc-related pain, while extension or rotation may irritate facet joints. Strengthening may help instability and deconditioning, but it may be too aggressive if an inflamed joint, ligament, nerve root, or trigger point remains active. Therapy also fails when sitting load, metabolic inflammation, sleep disturbance, stress-related muscle tone, or central sensitization continue to maintain symptoms. Physical therapy works best when the source of pain is identified first and exercises are chosen for that mechanism.
When does chronic low back pain need medication for nerve pain?
Chronic low back pain may need medication for nerve pain when symptoms suggest a neuropathic component. This may include burning, electric, shooting, tingling, numbness, hypersensitivity, or pain radiating from the back into the buttock, thigh, calf, or foot. Nerve pain may come from lumbar radiculopathy, nerve-root inflammation, entrapment neuropathy, piriformis-related sciatic irritation, or a mixed nociceptive-neuropathic pain pattern. Medications such as gabapentin, pregabalin, SNRIs, or tricyclic agents may be considered in selected cases, often together with anti-inflammatory treatment and mechanical unloading. They work best when matched to the correct mechanism and adjusted carefully rather than used as a generic painkiller.
When are image-guided injections useful for persistent low back pain?
Image-guided injections are useful when persistent low back pain has a likely anatomical target and medications or general therapy are not enough. They may be considered for facet joint pain, sacroiliac joint pain, selective nerve-root irritation, piriformis-related pain, myofascial trigger points, or other localized pain generators. Guidance with ultrasound, fluoroscopy, or CT improves accuracy compared with blind injections. The purpose may be diagnostic, therapeutic, or both. A well-selected injection can reduce inflammation, confirm the responsible structure, and allow rehabilitation or medications to work better. However, injections should not be chosen randomly or only from a standard clinic menu; they should follow a precise diagnostic hypothesis.
How are diagnostic blocks used to find the source of low back pain?
Diagnostic blocks are used to test whether a specific structure is responsible for low back pain. A small amount of local anesthetic, sometimes combined with an anti-inflammatory agent, is placed near a suspected pain generator such as a facet joint, medial branch nerve, sacroiliac joint, selective nerve root, piriformis region, or trigger point. If the patient experiences clear temporary relief in the expected pain pattern, the blocked structure is more likely to be involved. A diagnostic block does not discover the cause by itself; it confirms or rejects a hypothesis formed from history, examination, imaging, and pain mapping. Used correctly, it helps avoid unnecessary or misplaced treatment.
Do most people with lumbar disc herniation need surgery?
No. Most people with lumbar disc herniation do not need surgery. Many improve with time, medication, activity modification, targeted physical therapy, and sometimes image-guided injections. A disc herniation seen on MRI is important only if it matches the patient’s symptoms, neurological findings, and pain distribution. Surgery becomes more relevant when there is progressive weakness, severe nerve-root compression, cauda equina syndrome, or disabling leg pain that does not improve despite appropriate non-surgical treatment. Surgery is not usually performed for MRI appearance alone. The key question is whether the disc herniation is truly the active pain generator and whether the expected benefit outweighs risk.
When is spine surgery necessary for low back pain or sciatica?
Spine surgery is necessary only in selected cases of low back pain or sciatica. Urgent surgery may be needed for cauda equina syndrome, progressive neurological weakness, severe nerve-root compression, spinal instability, tumor, infection, fracture, or another clearly surgical condition. In non-emergency cases, surgery may be considered when disabling leg pain or neurological deficit persists despite well-directed conservative and interventional treatment, and imaging clearly matches the clinical problem. Most chronic low back pain does not require surgery, especially when the pain generator is a facet joint, sacroiliac joint, muscle, ligament, or mixed pain mechanism. Surgery should treat a confirmed structural problem, not a vague diagnosis.
Can chronic low back pain improve after months or years of failed treatment?
Chronic low back pain can improve even after months or years of failed treatment if the true pain generator and maintaining factors are finally identified. Long-lasting pain does not always mean the condition is irreversible. Many patients fail previous therapy because treatment was too general, based only on MRI findings, or aimed at symptoms rather than the active mechanism. Once the main source is clarified, treatment can become more specific: targeted medication, image-guided procedures, ergonomic unloading, correction of contributing factors, or carefully selected rehabilitation. Improvement is most realistic when the plan addresses both the local pain generator and factors that keep it irritated, such as sitting, inflammation, deconditioning, or sensitization.
Can sitting, chair position, or cushions help chronic low back pain?
Sitting, chair position, and cushions can help chronic low back pain when they reduce load on the structure that is actually causing pain. However, there is no universal best chair or cushion. Some patients need lumbar support, some need pelvic unloading, some need reduced sacroiliac stress, and others need pressure relief around the buttock, coccyx, or piriformis region. A cushion that helps one patient may worsen another if it shifts load to the wrong structure. Sitting-related treatment works best after the pain generator is identified. The goal is not simply to sit “correctly,” but to reduce mechanical stress on the specific structure maintaining symptoms.
When is low back pain a red flag that needs urgent in-person care?
Low back pain needs urgent in-person care when it is associated with new or progressive leg weakness, numbness in the groin or perineal region, loss of bladder or bowel control, fever, chills, recent significant trauma, severe night pain, unexplained weight loss, history of cancer, infection risk, immunosuppression, long-term steroid use, or rapidly worsening pain after surgery. These signs may suggest cauda equina syndrome, spinal infection, fracture, tumor, severe nerve compression, or another serious condition. This page focuses on persistent low back pain without obvious urgent structural findings. Red-flag symptoms should not be managed only through online advice or ergonomic changes; they require direct medical evaluation.
When should patients seek a second opinion for persistent or chronic low back pain?
Patients should consider a second opinion when low back pain persists despite medications, physical therapy, injections, ergonomic changes, or unclear explanations from MRI. A second opinion is especially useful when pain keeps returning after temporary relief, when surgery or repeated procedures are proposed, when MRI findings do not match symptoms, or when the diagnosis remains limited to labels such as lumbago or sciatica. The goal is not to repeat general advice, but to identify the exact pain generator and the mechanism that maintains symptoms. A structured review can clarify whether the problem is disc-related, nerve-related, facet-related, sacroiliac, myofascial, systemic, or mixed.
Red flags — this page is not for these situations
This page focuses on persistent low back pain without obvious structural causes on imaging. It is not intended for situations that require urgent in-person evaluation, such as: new or progressive leg weakness; numbness in the groin/perineum (saddle anesthesia); loss of bladder or bowel control; recent significant trauma; fever or chills, severe night pain, or unexplained weight loss; history of cancer, osteoporosis, immunosuppression, or long-term steroid use; suspected spinal infection or fracture; rapidly worsening pain after surgery; or MRI/CT already showing a mass, fracture, or severe stenosis with clear nerve-root/cord compression. If any of these apply, please seek immediate in-person medical care.
Additional Information for Low Back Pain (LBP)
English homepage – overview of neurosurgery and pain consultation