Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery and neurocritical care, including extensive surgical experience in the treatment of gunshot and shrapnel head injuries.
Last medically reviewed:
January 6, 2026
Who This Gunshot and Shrapnel Head Injury Page Is For
This gunshot and shrapnel head injury resource is designed primarily for
family members of patients with severe penetrating head injury who are being treated in the ICU
(often on a ventilator, under deep sedation, and not waking up as expected),
as well as for patients and caregivers facing prolonged recovery after high-energy head trauma.
This page explains how projectile head injuries damage the brain, why loss of consciousness may persist,
how ICU treatment is structured in the first critical days (including brain swelling and pressure control),
and what families can realistically expect regarding early prognosis and recovery.
If the information feels overwhelming, or if you have additional questions about CT findings,
surgical decisions, ICU strategy (sedation, swelling control, prevention of secondary brain injury),
or long-term outcome, you can contact us to see how we provide an individualized
neurosurgery second opinion
for your specific gunshot or shrapnel injury case.
When families usually seek a neurosurgical second opinion after a gunshot or shrapnel head injury
• The patient remains unconscious or deeply sedated in the ICU
• CT findings look severe, but prognosis is unclear
• Brain swelling may still evolve over the next 48–72 hours
• Families need clarity about current ICU strategy and next steps
In penetrating head injuries, families often need a calm, independent explanation of imaging,
surgical decisions, and ICU management — especially when early recovery is uncertain.
If you need an individualized neurosurgical review of CT findings and treatment strategy,
you can request a second opinion here:
Request Second Opinion
Gunshot & Shrapnel Head Injuries — Quick Summary (Read This First)
- Gunshot and shrapnel head injury is a high-energy penetrating injury. Brain damage is caused not only by the bullet path, but also by massive energy transfer to surrounding brain tissue.
- External wounds can be misleading. Even a small entry wound can be associated with severe deep brain damage, swelling, or bleeding on CT.
- Survival is possible. Many patients survive gunshot head injuries, especially when vital brain structures are spared and early ICU care is optimal.
- Not waking up early is common. Delayed awakening often reflects a combination of direct brain damage, swelling, and ICU sedation — not necessarily treatment failure.
- Brain swelling and high ICP may develop later. ICP (intracranial pressure) can be normal initially and rise unpredictably during the first 48–72 hours.
- Surgery is selective, not automatic. Surgeons prioritize controlling bleeding, evacuating compressive hematomas, debriding necrotic tissue and safely accessible bone fragments, and managing intracranial pressure, rather than the complete removal of every bullet or fragment at all costs.
- Risk of infection is managed early. Penetrating injuries carry a high risk of contamination from debris and bone fragments; therefore, early surgical debridement and broad-spectrum antibiotics are critical standard components of care to prevent meningitis or brain abscess.
- ICU care determines outcome. Preventing secondary injury (low oxygen, low blood pressure, infection, seizures) is often as important as surgery itself.
- Prognosis depends on multiple factors. The severity of injury is largely determined by how much kinetic energy the bullet transfers to the brain at the moment it strikes the skull. This energy depends primarily on the projectile’s speed at impact, which in turn is influenced by the distance from which it was fired. In addition, the projectile’s trajectory, the specific pattern and extent of brain injury, the patient’s initial neurological status (post-resuscitation GCS), and the development of secondary complications are major clinical prognostic indicators.
- Use the Contents box to jump directly to sections on ICU care, first 72 hours, prognosis, complications, or medico-legal aspects.
Most families only need this summary and the First 72 Hours in ICU section. The remaining parts are available for deeper understanding and specific questions.
Contents
- Who This Page Is For
- Key Takeaways
- Introduction
- Injuries Covered
- How Brain Gets Damaged
- Weapon And Distance
- Shrapnel Differences
- Wound Types
- CT Injury Patterns
- Initial Clinical Assessment
- Imaging Overview
- Surgery or Not
- Treatment Principles
- Surgical Options
- Why Coma Happens
- Common ICU Measures
- First 72 Hours
- Day 0–1
- Day 1–2
- Day 2–3
- Request Consultation
- Preventing ICU Complications
- Early Prognosis
- Recovery Pattern
- Long-Term Prognosis
- Medico-Legal Notes
- Gunshot FAQs
- Patient-Friendly Sources
Introduction
Gunshot and shrapnel head injuries belong to a group of high-energy penetrating head injuries. What makes these injuries different from other head traumas is the high speed and energy of the object (projectile or shrapnel) that enters (penetrates) the skull.
Although the skin and skull are penetrated by a metal object, the brain damage is not caused only by the physical path of the projectile. A large part of the injury results from the transfer of kinetic energy of the projectile to brain tissue, which can damage areas far beyond the visible wound and bullet canal.
This page explains, in patient-friendly terms, how these injuries damage the brain, how they are treated, and what factors influence prognosis.
Penetrating gunshot injuries to the brain are among the most lethal forms of trauma. It is estimated that up to 90% of victims die before reaching hospital care. Among those who arrive alive, early mortality remains high, with a substantial proportion of patients succumbing during the initial resuscitation phase. Outcomes depend heavily on the severity of the primary injury and the rapidity of specialized neurocritical management.
What Types of Injuries Are Included on This Page
This page focuses on high-energy penetrating head injuries, including:
- Gunshot injuries (bullets from firearms)
- Shrapnel injuries (metal fragments caused by explosions)
- Other high-velocity penetrating injuries, such as fast-moving metal fragments in industrial or work-related accidents
- Captive-bolt devices (livestock stunning pistols) — rare but severe penetrating head injuries. Severity depends on device type and kinetic energy.
These injuries share a common feature:
penetration of the scalp and skull by a fast-moving object, with significant energy transfer to the brain.
Low-energy penetrative injuries (such as knife stabs) are not covered here, because they involve a different injury mechanism and clinical course.
How High-Energy Projectiles Damage the Brain
Brain injury occurs through three primary mechanisms:
1) Direct tissue damage
The projectile creates a permanent channel through brain tissue, damaging everything along its path. Bone fragments created when the skull is broken can also act as secondary projectiles, causing further injury as they are pushed deeper into the brain.
2) Energy transfer to the brain
High-velocity projectiles (like rifle bullets) release a massive amount of energy upon impact, causing tissue stretching and tearing far beyond the visible path of the bullet. This explains why damage is often much more extensive than expected based on the external wound. Due to this intense energy transfer, even a tangential wound or a trajectory far from the brainstem can create a shockwave strong enough to damage vital centers, which can be immediately life-threatening.
3) Additional brain injuries
These injuries often cause hematomas (blood clots like epidural, subdural, or intracerebral) and brain edema (swelling). These lesions have a local compressive effect, meaning they press on the brain and increase intracranial pressure (ICP). This pressure can obstruct blood circulation, leading to further dangerous brain damage.
Gunshot Injuries: Why Weapon Type and Distance Matter
Not all gunshot injuries are the same, as the damage depends heavily on the energy the bullet carries.
- High-velocity weapons (typically rifles) cause far more devastating brain damage. Because of the longer barrel and larger gunpowder charge, these bullets travel much faster and carry significantly more energy. This results in a massive shockwave that can destroy vital brain centers even without a direct hit.
- Handguns (pistols and revolvers) generally fire bullets at lower speeds. While still life-threatening, the damage is often more localized to the bullet’s path.
- The distance of the shot is also a critical factor. Shots fired from very close range (contact or near-contact) cause additional destruction because the hot gases and „blast effect“ from the gunpowder explosion enter the wound along with the bullet. As the projectile travels through the air, it progressively loses speed and therefore kinetic energy. For this reason, a bullet fired from a high-velocity rifle may not strike the head with its full destructive potential at longer distances, and not every such injury is inevitably fatal.
- Bullet caliber and shape also play a role. A larger or heavier bullet, or one that deforms (expands) upon impact, will transfer its energy to the brain tissue much faster, increasing the severity of the injury.
In simple terms:
Higher speed and closer distance usually mean more severe injury, but outcomes still vary greatly between patients.
Shrapnel Injuries: What Makes Them Different
Shrapnel injuries differ from gunshot wounds because they often involve:
- Irregular shapes: Unlike smooth, aerodynamic bullets, shrapnel fragments are jagged and irregular. This causes them to „tumble“ through the brain, creating wider and more chaotic paths of destruction.
- Multiple fragments: A single explosion can send dozens of fragments into the brain. Because of this, shrapnel injuries may involve several brain regions at once, making surgical treatment much more complex.
- High risk of infection: Shrapnel pieces are often „dirty“—they carry debris, clothing, and environmental bacteria deep into the brain. This increases the risk of meningitis or brain abscesses compared to gunshot wounds.
- Explosion blast effects: These injuries are often a combination of penetrating injury and blunt force from the pressure wave of the explosion, which can cause additional bruising or bleeding throughout the brain.
- Associated body injuries: Because shrapnel comes from an explosion, it is often associated with other severe injuries to the lungs, limbs, or ears, which can complicate the overall ICU recovery.
Types of Penetrating Head Wounds
It is a common misconception that one type of wound is „safer“ than another. In reality, doctors classify these injuries to understand the specific pattern of brain damage, but all can be life-threatening:
- Tangential (grazing) injuries – the projectile travels along the surface. Families often think this is just a „flesh wound,“ but it can be extremely dangerous. High-velocity projectiles create a massive shockwave that passes through the bone and can shatter brain tissue underneath, even without the bullet entering the brain.
- Penetrating (blind) injuries – the projectile enters the skull but does not exit. Because the bullet stays inside, 100% of its kinetic energy is absorbed by the brain. This energy transfer, combined with the bullet potentially bouncing (ricocheting) off the inner skull, often creates multiple tracks of damage from a single entry point.
- Perforating injuries – the projectile enters and exits the skull. While some think an exit wound is „better“ because the bullet is gone, it actually means the projectile had immense energy to pass through the entire brain. The exit wound is usually much larger because the pressure wave „blows out“ the skull and skin from the inside as it leaves.
What Types of Brain Damage Can Occur
Depending on the injury, brain imaging may show:
- A narrow injury channel with surrounding bleeding
- Larger intracerebral hematomas (blood collections inside the brain)
- Brain swelling, sometimes involving an entire hemisphere
- Midline shift, where the brain is pushed to one side
- Massive subarachnoid hemorrhage (SAH) when larger blood vessels are injured
- Intraventricular hemorrhage (IVH) and possible hydrocephalus
- Injuries involving the brainstem are among the most severe and often determine survival and long-term outcome.
- Epidural (EDH) or subdural hematomas (SDH) when the projectile or a skull fracture damages meningeal arteries or bridging veins, causing additional bleeding and pressure on the brain.
- Brain contusions along and around the projectile path are common in gunshot and shrapnel injuries. Diffuse axonal injury (DAI) is less typical than in closed head trauma, but may occur in high-energy blast or combined injury mechanisms.
More than one of these findings is often present at the same time.

Image: Patterns of intracranial hemorrhage associated with gunshot and shrapnel head injuries, including epidural, subdural, subarachnoid, and intracerebral hematomas.
Clinical Assessment: What Doctors Look At First
Initial evaluation focuses on:
- Overall condition and vital signs (oxygen levels, blood pressure)
- Level of consciousness, usually measured with the Glasgow Coma Scale (GCS)
- Pupil size and reactions
- Neurological deficits, such as weakness or loss of movement
Even before imaging, these findings help doctors estimate severity and urgency.
Imaging and Diagnosis
CT Scan
A CT scan is the primary and most important diagnostic tool. It shows:
- The injury path – the track the projectile made through the brain.
- Bleeding – any blood clots (hematomas) that may need surgery.
- Swelling and pressure – how much the brain is reacting to the injury.
- Metal and bone fragments – on a CT scan, metal appears bright white. However, metal also causes „artifacts“ (star-like streaks on the image) that can blur the surrounding brain tissue, making it harder to see details near the fragments.
- Skull entry point and additional fractures – it clearly identifies where the object entered and any other skull fractures caused by the impact.
CT Angiography (CTA)
CTA is a specialized scan where a contrast dye is used to look at blood flow. It may be added if there is concern about injury to major blood vessels, which could lead to severe bleeding or a stroke.
MRI is often avoided early if metal fragments are present and may not be safe in some patients. While most civilian handgun bullets consist of a lead core with a copper jacket and are not strongly ferromagnetic, some projectiles—particularly certain military or specialized ammunition—may contain steel components. Because the exact composition of retained fragments is frequently unknown at the time of initial treatment, MRI safety must be carefully assessed on an individual basis. When clinically essential, further evaluation of fragment characteristics and interdisciplinary consultation may help determine whether MRI can be performed safely.
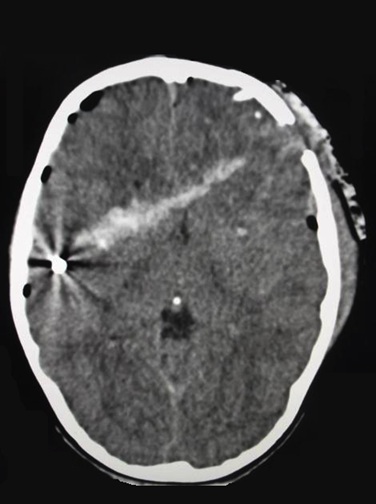
Image: CT scan of a gunshot wound showing the entry site in the left frontal region, the bullet track (hyperdense white line due to blood in the wound canal), intracranial air (pneumocephalus), and the retained projectile in the right parietal region. On a CT scan, metal fragments appear bright white and often cause ‘artifacts’—star-like streaks or shadows that can blur the surrounding brain tissue.
When Is Surgery Necessary — And When It Is Not
Surgery is not automatically required in all gunshot or shrapnel injuries to the brain, even when fragments are visible on CT. The key question is whether there is a surgically accessible problem that is actively threatening the brain, such as a large hematoma causing mass effect or uncontrolled intracranial pressure.
In many cases, especially when fragments are located deep within the brain and are not causing compression, attempting to remove them may lead to additional neurological damage without improving outcome. For this reason, the decision to operate is based not on the presence of a bullet or fragment itself, but on its effect on brain structures and the overall clinical condition of the patient.
Treatment Principles
Treatment is always individualized and depends on imaging findings and the patient’s neurological status. In patients presenting with extremely poor neurological condition (for example, post-resuscitation GCS 3–5, particularly when associated with bilaterally fixed and dilated pupils), the prognosis is generally very poor, and extensive surgical intervention is rarely beneficial unless a clearly operable mass lesion, such as a hematoma causing significant mass effect, is identified. In such cases, decisions must carefully balance the likelihood of meaningful recovery against the risks of aggressive treatment.
Surgical treatment may include:
- Cleaning and debridement of wounds – removing dirt and damaged tissue from accessible areas to prevent infection.
- Evacuation of compressive hematomas – removing large blood clots that are pressing on the brain, usually performed through a craniotomy (opening the skull).
- Removal of accessible bullet and bone fragments – taking out pieces of bone that were pushed into the brain, strictly only if they can be reached safely.
- Decompressive craniectomy – a procedure used in severe cases where a large part of the skull is removed to give the brain room to swell without being crushed.
- Reconstruction of damaged skin, dura, and bone tissues – noting that in cases of larger bone defects, replacement (cranioplasty) is performed after several months or up to 1 year.
Importantly, doctors do not automatically remove all bullets or fragments. In many cases, attempting to reach and remove deep-seated fragments would cause more harm to healthy brain tissue than benefit. If a fragment is left behind, it is because it is safer for the patient.

Image: Craniotomy depicts the creation of an opening in the skull by making a bone flap to remove a compressive hematoma (epidural, subdural, or intracerebral). The bone flap is eventually replaced and secured to the skull.
Why Patients Usually Do Not Wake Up After Gunshot or Shrapnel Head Injury
This is one of the most common and distressing questions families ask — and, as with other traumatic brain injuries (TBI), the answer is rarely a single reason.
In projectile head injuries, loss of consciousness and delayed awakening are often caused by combined effects of direct brain damage, energy transfer, swelling, and intensive care management.
1) Sedation and ventilator management
In the early phase, many patients appear “comatose” because sedative medications suppress outward responses.
This is particularly common during the first 24–72 hours, when the ICU team prioritizes safe breathing, oxygen delivery, and control of brain pressure rather than frequent wake-up testing.
2) Direct brain tissue destruction along the projectile path
If deep structures or both hemispheres are involved, recovery of consciousness may be delayed or incomplete.
3) Brain swelling and secondary ischemia
Even after surgical treatment or wound stabilization, brain swelling often increases over several days.
Swelling can reduce blood flow and cause secondary, stroke-like injury, further delaying awakening.
4) Residual compression, rebleeding, or expanding contusions
Repeat CT imaging is often required because:
- bleeding along the wound track can evolve,
- contusions may enlarge during the first 48–72 hours,
- associated epidural (EDH) or subdural hematomas (SDH) may develop or progress.
5) Ventricular involvement and CSF circulation disturbance
When the projectile passes near or through the ventricles, blood and tissue debris can interfere with normal cerebrospinal fluid flow. This may contribute to hydrocephalus, which can impair recovery of consciousness.
6) Systemic complications
Hypoxia, hypotension, infection, metabolic disturbances, pulmonary embolism, or organ failure can all secondarily injure the brain, even when neurosurgical treatment was technically correct.
Key message for families:
Not waking up immediately does not automatically mean that treatment has failed. In projectile brain injury, early ICU physiology often determines how much recovery is possible.
ICP and Brain Swelling After Projectile Head Injury (ICU Monitoring Explained Simply)
ICP (intracranial pressure) is the pressure inside the skull.
In projectile injuries, ICP elevation may result from:
- swelling around the wound track,
- bleeding,
- disturbed CSF circulation- hydrocephalus,
- or associated hematomas.
ICU goals include:
- Maintaining oxygenation and blood pressure to protect brain perfusion
- Preventing dangerous pressure spikes
- Detecting deterioration early through neurological exams and repeat imaging
Common measures:
- Head elevation to improve venous drainage
- Sedation and analgesia to reduce agitation and pressure surges
- Osmotherapy (mannitol or hypertonic saline) to reduce swelling
- Ventilation adjustments to control cerebral blood volume during pressure crises
- Seizure prevention, as early seizures are more common after penetrating injuries
- ICP monitoring and/or external ventricular drainage (EVD) in selected severe cases
If swelling becomes refractory, decompressive craniectomy may be considered.

Image: An External Ventricular Drain (EVD) system at the bedside. A thin tube from the ventricles connects to a clear chamber with measurement markings, allowing doctors to monitor pressure and drain excess fluid when necessary.
Important for families:
ICP treatment is not just about numbers. Doctors balance pressure control with blood pressure to preserve cerebral perfusion — the blood flow that keeps brain tissue alive.
What to Expect in the First 72 Hours (Day-by-Day ICU Pattern)
Day 0–1 (first 24 hours)
What families usually see:
- Patient on a ventilator, deeply sedated
- Limited neurological examination
- Early control CT scan to assess bleeding, swelling, and surgical effects
What matters most:
- Stable oxygen levels and blood pressure
- No signs of brain herniation
- Early detection of evolving bleeding or swelling
Lack of awakening at this stage is expected.
Day 1–2 (24–48 hours)
This phase is often the most dangerous.
What may happen:
- Swelling can increase
- Contusions and bleeding along the wound track may progress
- Sedation adjustments are made cautiously
What families may misinterpret:
- Absence of eye opening
- Fluctuating or asymmetric movements
These findings are common and often reflect swelling dynamics or sedation, not final outcome.
Day 2–3 (48–72 hours)
If the patient remains stable:
- Sedation may be gradually reduced
- Early neurological responses may appear
- In some patients, improvement is slow or absent due to the severity of injury
What matters most:
- Trend over time, not a single exam
- Pupillary findings
- Imaging evolution
- Prevention of systemic complications
Request Gunshot or Shrapnel Head Injury Neurosurgery Consultation — 24-Hour Review or Priority Option (Usually Within 3 Hours)
When a loved one is hospitalized after a gunshot or shrapnel head injury, families are often faced with urgent and confusing decisions — especially when CT findings look severe, brain swelling may evolve over 48–72 hours, or the patient does not wake up as expected in the ICU.
An independent neurosurgical second opinion can help clarify the true clinical significance of imaging findings, provide a deeper understanding of current surgical and ICU management, and offer a realistic perspective on what to expect during the critical early phase following a high-energy penetrating brain injury.
- ✔ Send a short message describing the gunshot or shrapnel injury situation and your main concerns
- ✔ You’ll receive a reply within 24 hours explaining if and how we can help in your specific case
- ✔ Time-sensitive ICU cases: consultations can often be arranged within a few hours — write PRIORITY in your first message
- ✔ If available, CT scans and hospital reports can be reviewed once initial contact is established
- ✔ During the video consultation, we explain the injury pattern, surgical decisions, ICU strategy (sedation, swelling control, complication prevention), and prognosis in clear, practical terms, with up to 10 days of follow-up for brief questions
Consultation fees typically range from $180–250, depending on case complexity.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth second opinions in neurosurgery. Telehealth second opinion does not replace emergency care and does not change immediate ICU treatment decisions made by the local team.
Complications of Penetrating Brain Gunshot Injuries
The most important secondary complications after penetrating cranial gunshot injuries—beyond the immediate damage to neural and surrounding tissues—include intracranial infection, post-traumatic epilepsy, and cerebrospinal fluid (CSF) leakage.
Intracranial infection may present as meningitis, cerebritis, or brain abscess and is more likely when bone or metallic fragments are retained, when the projectile passes through air-containing sinuses, or when a persistent CSF fistula is present. Prevention relies on early surgical debridement, meticulous watertight dural closure, and appropriate antibiotic prophylaxis. Treatment requires targeted antimicrobial therapy and, in selected cases, surgical drainage.
Post-traumatic epilepsy develops in a substantial proportion of patients with penetrating brain injury. Early seizures may occur within the first week and are commonly managed with short-term anticonvulsant prophylaxis. Late epilepsy can develop months or years later and requires long-term antiepileptic therapy based on clinical course rather than solely on the presence of retained fragments.
A CSF leak represents both a complication and a major risk factor for infection. It is particularly common when the projectile traverses the skull base or paranasal sinuses, creating a communication between the intracranial space and contaminated air-filled cavities. For this reason, special attention is paid during the initial surgery to meticulous debridement and secure, watertight dural closure in order to prevent persistent fistula formation. Persistent CSF leaks significantly increase the likelihood of meningitis and therefore require prompt recognition and, when necessary, surgical repair.
Systemic lead toxicity from retained intracranial fragments is possible but uncommon and is generally not a primary clinical concern compared with infection or seizure-related complications.
Preventing Systemic Complications in the ICU
Late deterioration often results not from the original brain injury, but from systemic complications. Preventing these is a core part of the treatment strategy, as any of these can cause secondary brain damage:
- Ventilator-associated pneumonia (lung infection that can lower oxygen levels to the brain)
- Sepsis (a severe body-wide infection that can cause blood pressure to drop dangerously)
- Pulmonary embolism (blood clots from the legs that travel to the lungs)
- GI bleeding (stomach ulcers caused by the extreme stress the body is under)
- Electrolyte and metabolic disturbances (imbalances in blood chemistry that can increase brain swelling)
Early Prognosis in Coma After Projectile Brain Injury
Prognosis depends on:
- initial GCS and pupillary responses,
- projectile velocity and shape
- depth and trajectory of the projectile,
- involvement of deep brain structures or both hemispheres,
- degree of swelling and mass effect,
- systemic complications.
Typical recovery pattern (when recovery occurs):
- stabilization of vital brainstem functions
- defensive or withdrawal movements
- eye opening and sleep–wake cycles
- purposeful movements and command following
- speech and higher cognitive recovery
This process may take weeks, and progress is often uneven.
Eye opening alone does not equal awareness and must be interpreted carefully.
Recovery and Long-Term Prognosis
Overall survival after gunshot or shrapnel head injury ranges roughly from 40–60%, but outcomes vary widely. Patients who arrive awake or only mildly impaired often survive, while those with deep coma, brainstem injury, or extensive ventricular involvement face a much poorer prognosis.
In survivors:
- the greatest improvement usually occurs within the first 3–6 months,
- rehabilitation remains crucial,
- long-term outcomes range from good recovery to severe disability.
Possible long-term consequences include:
- cognitive and behavioral changes,
- motor deficits,
- post-traumatic epilepsy,
- hydrocephalus,
- long-term dependency.
Medico-Legal Considerations (Important in Projectile Injuries)
In gunshot and shrapnel injuries, accurate medical documentation is critical.
Important principles include:
- Precise description of entry and exit wounds
- Careful documentation of fracture patterns and intracranial damage
- Proper handling and preservation of extracted projectiles
- Timely communication with law-enforcement authorities
- Early collection of forensic samples when indicated
These steps protect both the patient’s legal interests and the medical team, and they are a standard part of responsible trauma care.
Frequently Asked Questions About Gunshot and Shrapnel Head Injuries
What is a gunshot or shrapnel head injury?
A gunshot or shrapnel head injury is a penetrating brain injury in which a bullet, metal fragment, bone fragment, or other high-energy object enters the skull and damages the brain. The injury is not limited to the visible wound or the narrow path of the projectile. High-energy transfer can tear brain tissue, rupture blood vessels, create swelling, and cause bleeding far beyond the entry site. These injuries are usually managed as severe traumatic brain injuries, often requiring emergency CT imaging, neurosurgical assessment, ICU care, infection prevention, seizure prevention, and repeated evaluation during the first critical days.
Can a gunshot or shrapnel head injury be survived?
Yes, survival is possible after a gunshot or shrapnel head injury, but outcome depends on the pattern and severity of brain damage. Prognosis is better when the patient arrives alive with preserved brainstem function, reactive pupils, higher post-resuscitation Glasgow Coma Scale, and no devastating injury to both hemispheres or deep vital structures. Prognosis is worse with brainstem involvement, fixed dilated pupils, massive swelling, major vascular injury, ventricular injury, or severe systemic complications. Early survival does not always predict final recovery. The first 48–72 hours are especially important because swelling, bleeding, infection risk, and ICU complications can still evolve.
Why can a gunshot head injury look small externally but severe on CT?
A gunshot head injury can look small on the outside because the skin entry wound does not show how much energy entered the skull. A small external hole may hide extensive internal damage, including a long bullet track, bone fragments driven into the brain, bleeding, swelling, contusions, or injury to deep structures. High-energy projectiles can create a temporary cavity and pressure wave that injures tissue beyond the visible path. This is why CT findings are much more important than the appearance of the skin wound. Families should not assume that a small entry wound means a mild brain injury.
How are gunshot and shrapnel head injuries treated?
Treatment of gunshot and shrapnel head injuries is individualized and usually begins with emergency stabilization. Doctors first protect breathing, oxygen levels, blood pressure, and circulation because low oxygen or low blood pressure can cause secondary brain injury. CT imaging defines the projectile path, bleeding, swelling, fractures, and retained fragments. ICU treatment may include sedation, ventilation, seizure prevention, antibiotics, repeat CT scans, intracranial pressure control, and prevention of systemic complications. Surgery is performed when there is a clear surgical target, such as a compressive hematoma, contaminated wound, CSF leak, accessible fragments, open skull defect, or dangerous brain swelling.
What surgical treatments are used for gunshot or shrapnel head injuries?
Surgical treatment may include wound cleaning and debridement, removal of contaminated or dead tissue, evacuation of epidural, subdural, or intracerebral hematomas, removal of safely accessible bone or metal fragments, repair of the dura, closure of scalp defects, and control of bleeding. In severe swelling, decompressive craniectomy may be used to give the brain space to expand. If there is skull base injury or CSF leakage, watertight dural repair is important to reduce infection risk. Later, cranioplasty may be needed to reconstruct a skull defect. Surgery is guided by CT findings, neurological status, infection risk, and whether intervention can improve outcome.
Does every gunshot or shrapnel head injury require surgery?
No. Not every gunshot or shrapnel head injury requires surgery, even when metal or bone fragments are visible on CT. Surgery is usually considered when there is a compressive hematoma, uncontrolled bleeding, severe brain swelling, contaminated open wound, CSF leak, depressed skull fracture, safely accessible fragments, or rising intracranial pressure. If a fragment is deep, stable, and not causing compression or infection, attempting to remove it may damage more healthy brain tissue than it helps. The decision is based on the patient’s neurological condition, imaging findings, surgical accessibility, infection risk, and expected benefit of intervention.
Why aren’t bullets or shrapnel fragments always removed from the brain?
Bullets or shrapnel fragments are not always removed because the safest operation is not always the most aggressive one. Deep fragments may lie close to important brain areas, blood vessels, ventricles, or the brainstem. Trying to reach them can enlarge the injury, cause bleeding, or create new neurological deficits. Neurosurgeons usually remove fragments that are superficial, contaminated, accessible, compressive, associated with infection, or involved in a CSF leak. Fragments that are deep and stable may be left in place if removal would create more harm than benefit. The priority is brain protection, not complete fragment removal at any cost.
Is MRI safe with retained bullet or shrapnel fragments in the head?
MRI safety with retained bullet or shrapnel fragments must be assessed carefully and individually. Some civilian handgun bullets are mainly lead with a copper jacket and may not be strongly magnetic, but some military, industrial, or unknown fragments may contain steel or other ferromagnetic material. MRI can be dangerous if a fragment moves, heats, or distorts the image near critical structures. Early CT is usually the main imaging test. If MRI is clinically important, the medical team may review the fragment’s appearance, likely composition, location, injury history, and available safety information before deciding whether MRI can be performed.
Why doesn’t a patient wake up after a gunshot or shrapnel head injury?
A patient may not wake up after a gunshot or shrapnel head injury for several reasons. Direct destruction of brain tissue, deep brain injury, bleeding, swelling, high intracranial pressure, hydrocephalus, seizures, low oxygen, low blood pressure, infection, and metabolic problems can all delay awakening. ICU sedation and ventilator management can also suppress visible responses during the first 24–72 hours. Lack of early awakening does not automatically mean that treatment has failed, but it is a serious sign that must be interpreted together with CT scans, pupil responses, neurological examinations, sedation level, and the overall trend over time.
Can sedation hide recovery after a penetrating brain injury?
Yes. Sedation can hide early neurological recovery after a penetrating brain injury because sedative drugs reduce movement, eye opening, breathing effort, and responses to commands. In severe gunshot or shrapnel head injury, sedation is often necessary to keep the patient safely ventilated, reduce agitation, control pain, prevent dangerous pressure spikes, and support intracranial pressure management. Doctors may reduce sedation when it is safe, but this is not always possible during unstable swelling, respiratory problems, or repeated procedures. Families should ask whether poor responsiveness reflects brain injury, medication effect, swelling, or a combination of these factors.
Can brain swelling worsen days after a gunshot or shrapnel head injury?
Yes. Brain swelling can worsen during the first days after a gunshot or shrapnel head injury, even if the first CT scan is already known. Swelling around the projectile path, evolving contusions, bleeding, disturbed CSF circulation, and inflammation may progress over 48–72 hours. This is why ICU teams repeat neurological examinations and often repeat CT imaging. A patient may appear stable at first and then deteriorate if intracranial pressure rises or brain perfusion falls. Early treatment focuses on oxygenation, blood pressure, sedation, osmotherapy, seizure prevention, infection prevention, and timely surgery when swelling or bleeding becomes dangerous.
What is intracranial pressure after a penetrating brain injury?
Intracranial pressure, or ICP, is the pressure inside the skull. After a penetrating brain injury, ICP can rise because of swelling, bleeding, hydrocephalus, brain contusions, or associated epidural, subdural, or intracerebral hematomas. High ICP is dangerous because it can reduce blood flow to injured brain tissue and increase the risk of brain herniation. ICU treatment aims to preserve cerebral perfusion by balancing pressure control with oxygenation and blood pressure. Selected patients may need ICP monitoring, an external ventricular drain, osmotherapy, ventilation adjustments, sedation, or decompressive surgery if pressure remains dangerously high.
Can epidural or subdural hematomas occur after gunshot or shrapnel head injury?
Yes. Epidural and subdural hematomas can occur after gunshot or shrapnel head injury when the projectile, skull fracture, or bone fragments tear blood vessels around the brain. An epidural hematoma usually forms between the skull and dura, while a subdural hematoma forms between the dura and brain surface. These collections can compress the brain and worsen neurological status, even when the original projectile injury is already severe. CT scan is used to identify whether a hematoma is large enough to require surgical evacuation. The key question is whether the blood clot is causing mass effect, midline shift, or rising pressure.
What does ventricular involvement mean after a gunshot or shrapnel brain injury?
Ventricular involvement means that the bullet, shrapnel fragment, bleeding, or tissue debris has reached the brain’s fluid-filled spaces, called ventricles. This is important because blood and debris inside the ventricles can block normal cerebrospinal fluid circulation and contribute to hydrocephalus or increased intracranial pressure. Ventricular injury may also indicate a deeper projectile path and more severe brain damage. In selected cases, doctors may place an external ventricular drain to monitor pressure or drain CSF. Prognosis depends on the overall injury pattern, associated brain damage, level of consciousness, pupil findings, swelling, and systemic stability.
What factors most influence prognosis after a gunshot or shrapnel head injury?
Prognosis after a gunshot or shrapnel head injury depends on several factors rather than one CT finding alone. Important predictors include post-resuscitation Glasgow Coma Scale, pupil reactions, blood pressure and oxygenation, projectile velocity, trajectory, deep brain or brainstem involvement, injury to both hemispheres, ventricular injury, major vascular injury, degree of swelling, mass effect, infection, seizures, and systemic ICU complications. Patients who arrive awake or with preserved brainstem responses generally have a better chance of meaningful recovery. Deep coma, fixed dilated pupils, massive bilateral injury, or uncontrolled swelling usually indicate a much poorer prognosis.
What complications can occur after gunshot or shrapnel brain injury?
Complications after gunshot or shrapnel brain injury may include brain swelling, high intracranial pressure, expanding hematomas, hydrocephalus, CSF leak, meningitis, cerebritis, brain abscess, seizures, post-traumatic epilepsy, delayed bleeding, vascular injury, stroke, pneumonia, sepsis, pulmonary embolism, metabolic disturbances, and long-term cognitive or motor disability. Retained fragments may increase concern for infection or seizures in selected cases, but deep stable fragments are not automatically removed. The most important early goal is preventing secondary brain injury from low oxygen, low blood pressure, infection, uncontrolled pressure, or systemic ICU complications.
Can retained bullet or shrapnel fragments cause infection or seizures later?
Retained bullet or shrapnel fragments can sometimes be associated with later infection, seizures, or chronic irritation, but risk depends on fragment location, contamination, sinus involvement, CSF leak, bone fragments, and the amount of injured cortex. Infection risk is higher when the wound is contaminated, when the projectile passes through air-filled sinuses, or when dural closure is not secure. Seizures can occur because of cortical scarring, hemosiderin, retained debris, or previous bleeding. However, retained fragments are not removed automatically. If a fragment is deep and stable, observation may be safer than surgery that risks additional brain damage.
What are the long-term recovery prospects after gunshot or shrapnel head injury?
Long-term recovery after gunshot or shrapnel head injury varies widely. Some survivors regain meaningful independence, especially when vital structures are spared and early ICU complications are controlled. Others remain with severe disability because of direct brain destruction, deep injury, seizures, hydrocephalus, cognitive impairment, behavioral changes, weakness, speech problems, or prolonged disorders of consciousness. The greatest improvement often occurs during the first 3–6 months, but recovery can continue with rehabilitation. Early prognosis should be cautious because sedation, swelling, infection, and systemic complications can obscure the neurological picture during the first days.
Why is documentation important in gunshot and shrapnel head injuries?
Documentation is important in gunshot and shrapnel head injuries because these cases often have medical, legal, and forensic implications. Accurate records should describe entry and exit wounds, fracture patterns, CT findings, projectile path, removed fragments, associated injuries, and neurological status. Preserved projectiles may need proper handling according to local legal requirements. Clear documentation also helps future medical teams understand what was treated, what fragments remain, and what complications should be watched for. For families, good documentation may be essential when seeking a second opinion, rehabilitation planning, insurance review, or legal clarification after the acute hospital phase.
How can a second opinion help in managing a penetrating brain injury?
A second opinion can help families understand a penetrating brain injury when CT findings, ICU strategy, surgical decisions, or prognosis are unclear. An independent neurosurgical review can explain the projectile path, swelling, hematomas, retained fragments, ventricular involvement, infection risk, sedation, ICP management, and likely recovery scenarios. It can also clarify why surgery was performed, why some fragments were left in place, or why the patient is not waking up as expected. A second opinion does not replace emergency care or the local ICU team, but it can help families ask better questions and understand realistic next steps.
Patient-Friendly Resources on Gunshot and Penetrating Head Injuries
The following resources are written for patients and families. They explain gunshot and penetrating head injuries in clear, non-technical language and are provided by well-recognised medical institutions or educational services.
-
AANS — Gunshot Wound Head Trauma
Educational patient resource on head gunshot trauma from the American Association of Neurological Surgeons, including causes, imaging, treatment decisions, and outcomes. :contentReference[oaicite:4]{index=4} -
NCBI / StatPearls — Penetrating Head Trauma
Overview of penetrating head injuries, their evaluation, management principles, and why these are among the most lethal forms of traumatic brain injury. :contentReference[oaicite:5]{index=5} -
UCLA Health — Cranial Gunshot Wounds
Patient-oriented information from a neurosurgery department that treats cranial gunshot injuries, explaining presentation, CT usage, surgical considerations, and outcomes. :contentReference[oaicite:6]{index=6}