Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 02, 2026
Who this page is for
This page is for patients with foot pain that persists beyond 6–12 weeks despite an initial trial of care (activity modification, medication, physiotherapy), and where imaging (X-ray/MRI/ultrasound) shows no major deformity or fracture and only mild-to-moderate changes that do not fully match the symptoms.
We focus on non-traumatic, non-deformity pain syndromes such as plantar fasciitis, Morton’s neuroma/metatarsalgia, Achilles tendinopathy, and tarsal tunnel syndrome (and other peri-tendinous or nerve-related causes). If you want a targeted evaluation to identify the dominant pain source and create a precise treatment plan, you can request an online consultation with our specialist.
Note: This page does not cover foot deformities (e.g., bunions, flatfoot) or acute injuries (e.g., fractures, sprains).
When patients usually seek a second opinion for chronic foot pain
- Plantar fasciitis has not improved despite months of conservative therapy
- You suspect Morton’s neuroma or nerve entrapment, but imaging is inconclusive
- You still have pain after foot surgery or steroid injections
- You are being advised surgery and want to understand whether less invasive options exist
A focused online consultation can help localize the true pain generator — tendon, joint, fascia, or nerve — and determine whether surgery, guided injections, or conservative management is the appropriate next step.
Contents
- Overview
- Distribution of Pain Sources
- Common Causes of Foot Pain
- Plantar Fasciitis
- Morton’s Neuroma and Metatarsalgia
- Achilles Tendinopathy
- Tarsal Tunnel Syndrome
- Other Extra-articular Causes
- Diagnostic Approach
- Treatment of Foot Pain
- Treatment of Contributing Factors in Foot Pain
- Prognosis and Long-Term Outlook
- FAQ — Foot Pain
- Additional Patient Resources
Overview
Foot pain affects one in five adults at some point in life and accounts for up to 10% of primary care musculoskeletal visits.
It can arise from tendons, fascia, nerves, or small joints — and often several structures coexist in the same patient.
Because the foot bears body weight and absorbs repetitive impact, local overload and micro-injuries are frequent even without visible damage on imaging.
Distribution of Pain Sources
In real-world outpatient studies:
- Plantar heel pain (plantar fasciitis) — accounts for 30–40% of all chronic foot-pain cases.
- Forefoot pain (Morton’s neuroma / metatarsalgia) — seen in 20–25% of patients.
- Posterior heel pain (Achilles tendinopathy) — about 15–20%.
- Neuropathic pain (tarsal tunnel, entrapment) — 5–10%.
- Other causes (fat-pad atrophy, bursitis, referred lumbar pain) — <10%.
Common Causes of Foot Pain
Plantar Fasciitis
- Plantar fasciitis is the most frequent source of heel pain in adults aged 40–60 years.
- It is caused by micro-tears and degenerative changes at the origin of the plantar fascia on the calcaneal tuberosity (heel bone).
- Pain is typically sharpest with the first steps in the morning or after rest and may ease with gentle walking.
- Clinical examination is the key to diagnosis. Ultrasound shows a thickened and hypoechoic fascia, while MRI is rarely needed.
- Plain X-rays often reveal a heel spur (calcaneal spur), which many patients mistakenly believe is the cause of pain; however, it is actually a reactive bony change secondary to chronic inflammation, not the source of pain itself.

Image: Plantar fasciitis
Morton’s Neuroma and Metatarsalgia
- Morton’s neuroma is a perineural fibrosis of the common interdigital nerve, most often located between the 3rd and 4th metatarsal heads at the base of the corresponding toes.
- Metatarsalgia refers to mechanical overload and inflammation of the metatarsal heads and supporting ligaments, without nerve thickening.
- Both conditions cause burning or tingling pain under the forefoot, often radiating into the involved toes.
- Symptoms are typically worsened by tight footwear, prolonged standing, or high-impact activity.
- Clinical examination remains the key to diagnosis.
- Most patients respond to activity modification, orthotics (custom insoles with metatarsal off-loading pads)
- Ultrasound can visualize the neuroma and guide precise corticosteroid or alcohol (sclerosing) injections, which often provide long-term relief without the need for surgery.
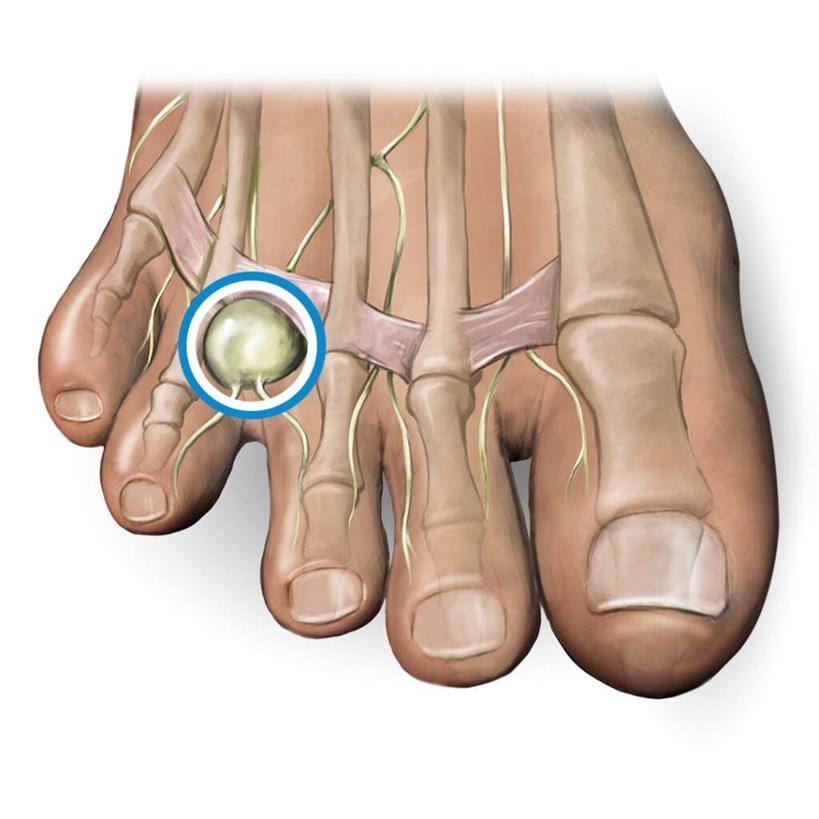
Image: Morton’s neuroma between the 3rd and 4th metatarsal heads
Achilles Tendinopathy
- Achilles tendinopathy — degenerative or insertional tendinopathy caused by repetitive loading, calf tightness, or altered biomechanics.
- In most patients, degenerative changes coexist with peritendinitis, and the pain arises from inflammatory irritation of surrounding tissues and nearby sensory nerves rather than from the degenerated tendon itself.
- Symptoms include morning stiffness and pain after activity, localized along the tendon or its insertion.
- The exam is the most important part of the diagnosis. Ultrasound identifies thickening and peritendinous fluid; MRI is used if a partial tear or rupture is suspected.
- Most patients improve with eccentric strengthening, stretching, load modification, and precisely targeted peritendinous (not intratendinous) ultrasound-guided injections of corticosteroids or PRP, while surgery is reserved for refractory cases.
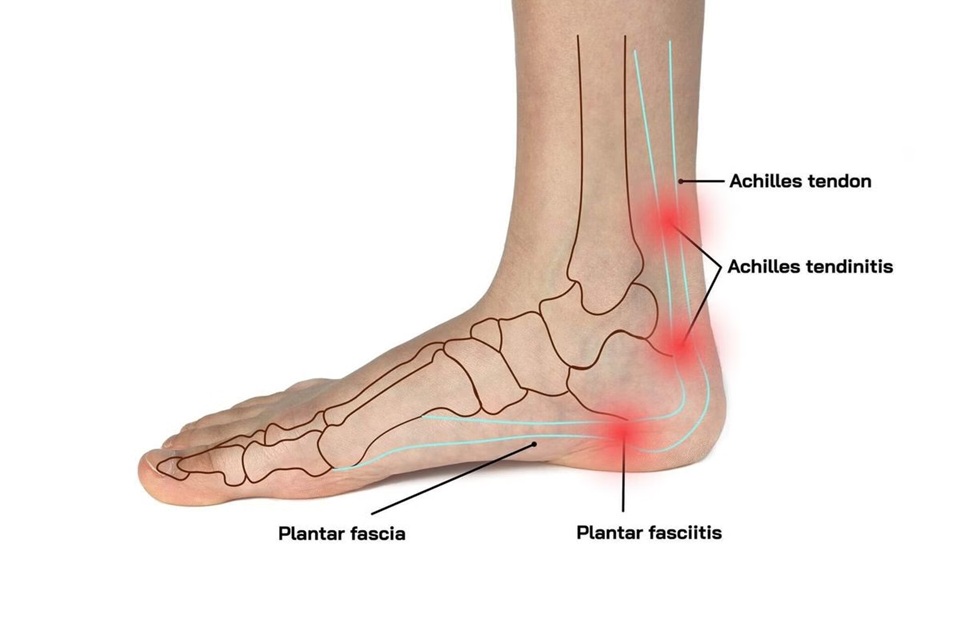
Image: Achilles tendinitis and plantar fasciitis
Tarsal Tunnel Syndrome
Tarsal tunnel syndrome — compression of the posterior tibial nerve beneath the fibrous band (flexor retinaculum) behind the inner (medial) ankle.
• Produces burning pain, tingling, or numbness in the sole, sometimes radiating to the toes.
• Symptoms often worsen with prolonged standing or walking and may improve with rest or ankle inversion.
• Clinical examination is the key to diagnosis — sensory testing and a positive Tinel’s sign behind the medial malleolus are characteristic.
• Nerve conduction studies (NCS/EMG) confirm slowed conduction of the posterior tibial nerve.
• Ultrasound or MRI help identify space-occupying lesions (ganglion cysts, varicose veins, tenosynovitis) compressing the nerve.
• Most patients respond to activity modification, foot orthoses that support the medial arch and correct over-pronation, and ultrasound-guided perineural corticosteroid or hydrodissection around the tibial nerve; surgery (tarsal tunnel release) is reserved for refractory compression. Outcomes are generally less predictable than in carpal tunnel release and depend on etiology and symptom duration.
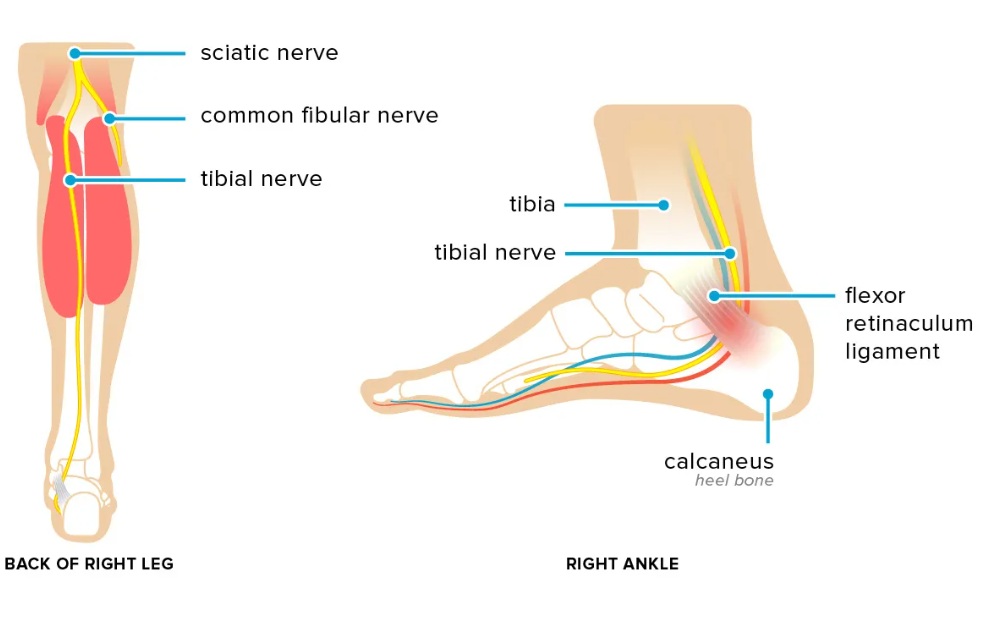
Image- Tarsal tunnel syndrome — compression of the posterior tibial nerve beneath the fibrous bend (flexor retinaculum) behind the inner (medial) ankle.
Other Extra-articular Causes
- Fat-pad atrophy — loss of cushioning beneath the heel.
- Retrocalcaneal bursitis — inflamed bursa between the Achilles tendon and heel (calcaneus).
- Referred pain — from lumbar radiculopathy or peripheral neuropathy (diabetic, small-fiber).
Diagnostic Approach
Imaging alone often fails to identify the true pain generator.
A comprehensive evaluation combines:
- Focused physical exam — localization by palpation, gait assessment.
- Dynamic ultrasound — real-time view of fascia, tendons, bursae, and nerves.
- MRI — for intra-tendinous or neuropathic lesions when ultrasound is inconclusive.
- Diagnostic injections — local anesthetic or corticosteroid injections confirm the symptomatic structure.
Treatment of Foot Pain
Most patients achieve significant relief with structured, stepwise management:
Medication & local therapy — short courses of NSAIDs; precisely targeted ultrasound-guided injestions (corticosteroid, PRP, or dextrose) around the affected fascia, tendon, or nerve.
Physiotherapy — stretching of the plantar fascia and Achilles tendon, eccentric calf strengthening, metatarsal padding, and orthotic correction of load imbalance.
Shockwave therapy (ESWT) — a non-invasive treatment that delivers high-energy acoustic pressure waves into the affected tissue to stimulate healing, improve circulation, and reduce pain. This is effective for chronic plantar fasciitis or Achilles tendinopathy unresponsive to standard care.
Procedure-level care — ultrasound-guided nerve hydrodissection, alcohol ablation for Morton’s neuroma, or lavage for chronic bursitis.
Surgery — rarely required. Indicated for:
- Refractory plantar fasciitis (>9–12 months conservative care).
- Confirmed Morton’s neuroma nonresponsive to injections.
- Severe tarsal tunnel compression with EMG-proven neuropathy.
➤ Less than 10–15% of all chronic foot-pain cases require surgical intervention.
Why Foot Pain Often Persists Despite Treatment
Persistent foot pain is a frequent problem, even after treatment with medication, orthotics, physiotherapy, or injections.
This often occurs not because treatment options are insufficient, but because the exact source of pain has not been accurately identified. Imaging findings such as plantar fasciitis, heel spurs, or degenerative changes may be present, but they do not always represent the true cause of symptoms.
In addition, ongoing mechanical stress — such as abnormal foot loading, gait disturbances, improper footwear, or muscle imbalance — may continue to provoke pain even when the primary condition is partially treated. Without addressing both the main pain generator and these contributing factors, symptoms often persist or recur.
Treatment of Contributing Factors in Foot Pain
Effective treatment of foot pain always begins with identifying the primary pain generator — the specific structure responsible for symptoms (such as plantar fascia, interdigital nerve in Morton’s neuroma, Achilles tendon, small joints, or tibial nerve in tarsal tunnel syndrome).
However, in many patients, pain persists not only because of the local problem, but because additional contributing factors are not recognized or adequately addressed. These factors rarely act as the sole cause of pain, but they can maintain irritation, delay recovery, and reduce the effectiveness of otherwise appropriate treatment.
For that reason, successful management of foot pain requires not only treating the primary structure, but also understanding the broader mechanical and systemic context.
What contributing factors may play a role in foot pain?
- Repetitive loading and impact stress — Walking, running, prolonged standing, or hard surfaces continuously stress the plantar fascia, tendons, and metatarsal heads.
- Foot biomechanics and load distribution — Flatfoot, high arch, or altered weight distribution increase stress on specific regions of the foot.
- Footwear factors — Tight shoes, poor cushioning, high heels, or inadequate support significantly contribute to plantar fasciitis, metatarsalgia, and nerve compression.
- Muscle tightness and imbalance — Tight calf muscles (gastrocnemius/soleus) increase tension on the plantar fascia and Achilles tendon.
- Reduced ankle mobility — Limited dorsiflexion shifts load toward the forefoot and plantar structures.
- Metabolic factors, pro-inflammatory diet and low-grade inflammation — Obesity, insulin resistance, and systemic inflammation increase load and impair tissue recovery.
- Nutritional deficiencies — Low vitamin D, B12, or other micronutrients may slow healing and prolong symptoms.
- Peripheral nerve sensitivity — Nerve irritation or entrapment (e.g., tarsal tunnel, interdigital nerves) increases pain sensitivity even with minimal structural change.
- Reduced activity and compensatory patterns — Altered walking due to pain leads to overload of other foot regions and persistence of symptoms.
- Medications and previous treatments — Certain medications such as statins, long-term use of pain medications, corticosteroids, or medications that cause excessive sedation may contribute to muscle or tendon-related pain, reduce tissue quality, or alter pain perception. Previous treatments, including repeated injections or incomplete rehabilitation, may also maintain symptoms if the underlying mechanism was not fully addressed.
- Other medical conditions and comorbidities — Conditions such as autoimmune diseases, thyroid disorders, diabetes, or chronic inflammatory states may increase pain sensitivity, affect tendon and joint structures, and reduce the response to otherwise appropriate treatment.
- Vitamin-related factors — Both deficiencies and excesses of certain vitamins (particularly vitamin B6) may contribute to nerve-related symptoms, burning pain, or altered sensitivity around the foot.
- Tissue quality and degeneration — Age-related changes, reduced blood supply, or repeated micro-injuries may impair tendon healing and increase vulnerability to persistent pain, even when mechanical factors are partially corrected.
Why this matters in practice
In many cases, treatment fails because the primary pain generator is not correctly identified, and therapy is directed only at contributing factors such as footwear changes, exercises, or orthotics. Conversely, even when the main structural cause is treated, failure to recognize and address contributing factors often leads to only partial or temporary improvement.
The most effective approach is a carefully selected combination of treatment that addresses both the primary pain generator and the contributing mechanical, functional, and systemic factors. In contrast, an inadequate or incomplete combination — even when it includes individually effective methods — is a common reason for suboptimal or short-lasting results.
This approach significantly increases the likelihood of long-term improvement and reduces the need for repeated injections or surgery.
In practice, many patients try to address contributing factors on their own — for example by changing footwear, using insoles or orthotics, performing stretching and strengthening exercises, following an anti-inflammatory diet, using supplements (vitamin D, magnesium, glucosamine, chondroitin), or applying various local treatments.
While these approaches can be helpful, they rarely lead to lasting improvement if the primary pain generator is not clearly identified and treated. On the other hand, even well-targeted medical treatment may fail if all contributing factors are not recognized and corrected.
Many patients reading this recognize that they have already tried one part of this approach — but not the complete strategy. This is one of the most common reasons why otherwise well-treated foot pain becomes chronic.
Prognosis and Long-Term Outlook
Once the dominant pain source is identified and appropriately treated, over 80% of patients achieve durable pain relief and restored function. Most cases improve with conservative, image-guided, or telehealth-supervised treatment — surgery is needed only for selected patients.
Recurrence is uncommon when mechanical overload and footwear factors are corrected.
Persistent pain after standard care often signals overlooked combined sources (e.g., fascia + nerve or tendon + bursa).
Request Persistent Foot Pain Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Persistent foot pain despite orthotics, physiotherapy, medication, injections, shockwave therapy, or previous surgery
often raises important questions:
Is the pain really coming from the plantar fascia, tendon, joint, or nerve?
Do X-ray, MRI, or ultrasound findings truly explain the symptoms?
Is a heel spur, Morton’s neuroma, Achilles tendinopathy, tarsal tunnel syndrome, or metatarsalgia actually the main pain source?
Could the pain come from abnormal loading, footwear, small sensory nerves, peripheral neuropathy, or referred pain from the lumbar spine?
An independent specialist second opinion may help clarify whether the dominant pain source is
fascia, tendon, joint, nerve-related, or referred, whether the proposed procedure is medically justified,
and whether more targeted treatment — such as medication adjustment, correction of contributing mechanical and systemic factors,
ultrasound-guided evaluation, diagnostic injections, nerve hydrodissection, focused rehabilitation, orthotic correction, or image-guided treatment — may be more appropriate before surgery or repeated injections.
- ✔ Send a brief message describing your foot pain location, how long it has lasted, what makes it worse, and which treatments have already been tried
- ✔ You will receive a reply within 24 hours explaining whether an online consultation is appropriate and which documentation is required
- ✔ Priority cases: severe burning or electric foot pain, progressive numbness, weakness, pain after foot surgery or injection, suspected nerve entrapment, conflicting specialist recommendations, or uncertainty before proposed surgery — write PRIORITY in your first message
- ✔ X-ray, MRI, ultrasound, EMG/NCS reports, injection history, shockwave therapy history, operative notes, orthotic history, and physiotherapy summaries can be reviewed
- ✔ During consultation we analyze whether the dominant pain generator is plantar fascia, Achilles tendon, interdigital nerve, tibial nerve, small joint, bursa, fat pad, local overload, peripheral neuropathy, or referred lumbar nerve pain
- ✔ We explain which treatment direction best matches the suspected dominant pain generator — including medication adjustment, correction of contributing factors, footwear and load modification, targeted rehabilitation, diagnostic injections, ultrasound-guided treatment, or nerve-directed procedures. If surgery for plantar fasciitis, Morton’s neuroma, tarsal tunnel syndrome, or Achilles pathology is being considered, we clarify whether the pain pattern supports that decision before discussing it with your local treating team — with up to 10 days of follow-up clarification.
Consultation fees typically range from $180–250 depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Based on our medical report, reimbursement may be possible if your insurance plan allows it.
This corresponds to typical international specialist telehealth second-opinion services for complex pain and treatment-decision review.
FAQ About Persistent Foot Pain
How can a doctor identify whether foot pain comes from fascia, tendon, joint or nerve?
Identifying the true source of foot pain requires more than reading an X-ray or MRI report. The doctor must map the exact pain location, the timing of pain, walking pattern, footwear triggers, local tenderness, sensory symptoms, and response to previous treatment. Heel pain with first steps in the morning may suggest plantar fascia involvement. Burning or tingling into the sole or toes may suggest nerve irritation, such as tarsal tunnel syndrome or interdigital nerve compression. Pain behind the heel may involve the Achilles tendon or surrounding tissues. Forefoot pain may come from Morton’s neuroma, metatarsalgia, small joints, or load imbalance. Dynamic ultrasound, MRI when needed, nerve testing, and diagnostic injections can help confirm the dominant pain generator.
Can foot X-ray, MRI or ultrasound show changes that are not the true cause of pain?
Yes. Imaging can show heel spurs, mild degenerative changes, tendon thickening, bursitis, or neuroma-like findings that do not always explain the patient’s symptoms. A heel spur is a common example: many patients believe the spur itself is the cause of pain, but it is often a reactive bony change related to chronic plantar fascia traction rather than the pain generator itself. MRI and ultrasound are useful, especially when ultrasound shows fascia thickening, tendon changes, peritendinous fluid, bursitis, or nerve compression. However, imaging must match the clinical pattern. If the location, timing, palpation findings, gait pattern, and treatment response do not fit the imaging abnormality, another structure may be responsible.
Can heel pain be caused by a pinched nerve instead of plantar fasciitis?
Yes. Heel pain is often caused by plantar fasciitis, but not every heel pain comes from the plantar fascia. Nerve-related heel pain may occur when sensory branches around the heel or the tibial nerve region are irritated. Baxter’s nerve entrapment, tarsal tunnel syndrome, sural nerve irritation, or lumbar radicular pain can mimic plantar fasciitis. Plantar fasciitis usually causes sharp pain with the first steps in the morning or after rest and local tenderness at the plantar fascia origin. Nerve-related pain is more likely to feel burning, tingling, electric, numb, or radiating into the sole or toes. If standard plantar fasciitis treatment fails, the diagnosis should be reassessed and nerve entrapment or referred pain should be considered.
Can a heel spur be present but not be the true cause of heel pain?
Yes. A heel spur can be present on X-ray without being the real cause of heel pain. In many patients, the spur is a reactive bony change that develops near the origin of the plantar fascia after long-term traction and inflammation. The painful structure is often the plantar fascia itself, surrounding soft tissue, fat pad, bursa, or a nearby nerve branch, not the spur as a sharp object pressing into the foot. This distinction matters because treating only the X-ray finding may lead to poor results. The decision should be based on pain location, tenderness, morning first-step pain, ultrasound findings, gait, footwear, and response to targeted treatment. Removing or focusing on the spur is rarely the first solution.
Why can plantar fasciitis persist despite stretching, orthotics or injections?
Plantar fasciitis can persist when treatment reduces symptoms temporarily but does not correct the dominant mechanical and biological factors maintaining irritation. Stretching, orthotics, NSAIDs, and injections may help, but pain can return if repetitive loading, hard surfaces, tight calf muscles, reduced ankle mobility, poor footwear, obesity, or abnormal foot biomechanics continue to stress the plantar fascia. In some patients, the diagnosis is also incomplete: heel pain may come from fat-pad atrophy, nerve entrapment, tarsal tunnel syndrome, referred lumbar pain, or combined fascia and nerve irritation. Ultrasound can show plantar fascia thickening, but clinical examination remains essential. Persistent heel pain after months of care should prompt reassessment of the primary pain generator and contributing factors.
What is the difference between Morton’s neuroma and metatarsalgia?
Morton’s neuroma and metatarsalgia can both cause forefoot pain, but they are not the same condition. Morton’s neuroma is irritation and perineural fibrosis of a common interdigital nerve, most often between the third and fourth metatarsal heads. It often causes burning, tingling, numbness, or radiating pain into the toes, and patients may feel as if they are walking on a pebble or folded sock. Metatarsalgia is mechanical overload and inflammation around the metatarsal heads and supporting ligaments without a true nerve thickening. It is usually related to pressure, footwear, load distribution, or forefoot mechanics. Correct distinction matters because treatment may involve metatarsal pads, orthotics, footwear changes, ultrasound-guided injections, alcohol ablation, or nerve-directed treatment.
Why does it feel like I am walking on a pebble or a folded sock?
A feeling of walking on a pebble, lump, or folded sock under the forefoot is typical of irritation near the metatarsal heads. Morton’s neuroma is one important cause, especially when the sensation is associated with burning, tingling, numbness, or radiation into the toes. Metatarsalgia can produce a similar feeling when mechanical overload inflames the tissues under the metatarsal heads without a true nerve thickening. Tight shoes, high heels, prolonged standing, running, or poor forefoot load distribution often worsen symptoms. Clinical examination is still central, because ultrasound may show a neuroma but the finding must match the exact pain pattern. Targeted treatment depends on whether the dominant generator is nerve compression, metatarsal overload, joint irritation, or a combination.
Why do I feel burning, tingling or numbness that radiates into my toes?
Burning, tingling, numbness, or radiating pain into the toes usually suggests nerve irritation rather than simple joint or tendon pain. The source may be Morton’s neuroma, tarsal tunnel syndrome, interdigital nerve compression, sural nerve irritation, tibial nerve compression, peripheral neuropathy, small-fiber neuropathy, or referred pain from the lumbar spine. Local nerve entrapment often produces symptoms in a specific anatomical distribution and may worsen with footwear, standing, walking, or pressure over the nerve. Peripheral neuropathy is more often bilateral, diffuse, and associated with diabetes, metabolic factors, vitamin problems, or systemic disease. Clinical examination, sensory testing, Tinel’s sign, ultrasound, MRI, and sometimes EMG/NCS help determine whether the dominant problem is local entrapment or more generalized neuropathy.
How can I tell if foot pain is peripheral neuropathy or a local nerve entrapment?
Peripheral neuropathy and local nerve entrapment can both cause burning, tingling, numbness, and altered sensitivity in the feet, but their patterns are different. Peripheral neuropathy often affects both feet, may be symmetrical, and may involve the soles, toes, or lower legs in a stocking-like pattern. It can be related to diabetes, insulin resistance, thyroid disease, vitamin deficiency or excess, autoimmune disease, medications, or other systemic factors. Local nerve entrapment usually follows the territory of one nerve, such as the tibial nerve in tarsal tunnel syndrome or an interdigital nerve in Morton’s neuroma. Symptoms may worsen with specific footwear, standing, walking, or local pressure. Examination, Tinel’s sign, ultrasound, MRI, and EMG/NCS can help separate these mechanisms.
What is tarsal tunnel syndrome and when can it cause persistent foot pain?
Tarsal tunnel syndrome is compression of the posterior tibial nerve beneath the flexor retinaculum behind the inner ankle. It can cause burning pain, tingling, numbness, or altered sensation in the sole, sometimes radiating into the toes. Symptoms often worsen with prolonged standing or walking and may improve with rest or certain ankle positions. A positive Tinel’s sign behind the medial malleolus and sensory changes support the diagnosis. EMG/NCS can show slowed tibial nerve conduction, while ultrasound or MRI may identify ganglion cysts, varicose veins, tenosynovitis, or other space-occupying lesions compressing the nerve. Treatment may include activity modification, arch support, perineural injections, hydrodissection, or surgery when compression is severe and refractory.
Why can Achilles tendon pain persist even when MRI only shows tendinopathy?
Achilles tendon pain can persist because the painful mechanism is often more complex than tendon degeneration seen on MRI. In many patients, degenerative tendon changes coexist with peritendinitis, inflammatory irritation of surrounding tissues, altered loading, calf tightness, reduced ankle mobility, footwear problems, or nearby sensory nerve irritation. Pain may arise from tissues around the tendon rather than only from the degenerated tendon fibers. This is why ultrasound examination and clinical testing are important. Ultrasound can show tendon thickening, peritendinous fluid, and local changes that guide treatment. Most patients improve with eccentric strengthening, stretching, load modification, and precisely targeted peritendinous treatment when needed. Injections should not be placed inside the tendon because that may increase risk.
Are steroid injections safe for Achilles tendon or chronic foot pain?
Steroid injections can be useful in selected chronic foot pain conditions, but safety depends on the target structure and technique. Around the plantar fascia, bursae, nerve entrapments, or inflamed peri-tendinous tissues, ultrasound guidance can improve precision and reduce unnecessary tissue injury. For Achilles tendinopathy, corticosteroid should not be injected into the tendon itself, because intratendinous injection may weaken tendon fibers and increase rupture risk. When used, treatment is placed peritendinously — around the tendon — and only when inflammation of surrounding tissues is a major contributor. The decision should depend on the exact pain generator, previous injections, tendon quality, activity level, and whether conservative measures such as load modification, stretching, eccentric strengthening, footwear correction, and orthotics have been properly tried.
When does shockwave therapy (ESWT) help chronic foot pain?
Shockwave therapy, or ESWT, may help selected patients with chronic plantar fasciitis or Achilles tendinopathy when standard care such as stretching, footwear correction, orthotics, medication, and physiotherapy has not provided enough relief. It uses acoustic pressure waves to stimulate tissue healing, improve local circulation, and reduce pain sensitivity in chronically irritated tissues. However, ESWT is not a universal treatment for all foot pain. It is less likely to help if the dominant pain generator is Morton’s neuroma, tarsal tunnel syndrome, peripheral neuropathy, small joint disease, fat-pad atrophy, or referred lumbar nerve pain. Before choosing ESWT, the key question is whether the pain truly comes from plantar fascia or Achilles tendon overload, and whether contributing factors such as footwear, calf tightness, gait, and load distribution have been corrected.
When are diagnostic injections useful in persistent foot pain?
Diagnostic injections are useful when persistent foot pain has several possible sources or when imaging does not clearly explain the symptoms. A small amount of local anesthetic can be placed around a suspected pain generator, such as the plantar fascia, interdigital nerve, Achilles peritendinous tissues, tarsal tunnel region, bursa, or small joint. If the patient’s typical pain temporarily improves, the injected structure is more likely to be clinically relevant. This is especially helpful when plantar fasciitis, heel spur, Baxter’s nerve, tarsal tunnel syndrome, Morton’s neuroma, metatarsalgia, bursitis, and referred pain may overlap. Diagnostic injections are not a complete treatment plan by themselves, but they can prevent poorly targeted surgery, repeated ineffective injections, or generic orthotic treatment.
Why can foot pain persist despite orthotics, physiotherapy, injections or medication?
Foot pain can persist despite orthotics, physiotherapy, injections, or medication when the dominant pain generator has not been precisely identified or when contributing factors continue to irritate the same structure. Treatment may focus on footwear, insoles, or exercises while the true source is plantar fascia, interdigital nerve, Achilles peritendinous tissue, tarsal tunnel compression, small joint irritation, fat-pad atrophy, bursitis, or referred lumbar pain. Even when the main structure is treated, symptoms may continue if repetitive loading, hard surfaces, poor footwear, abnormal gait, calf tightness, reduced ankle mobility, metabolic factors, inflammation, neuropathy, or central sensitization are not corrected. Persistent pain usually means the entire mechanical, neurological, and systemic context needs reassessment.
Why can foot pain persist after steroid injections or foot surgery?
Foot pain can persist after steroid injections or surgery when the treated structure was not the dominant pain generator, when several pain sources coexist, or when contributing factors continue to overload the foot. For example, a patient treated for plantar fasciitis may also have nerve entrapment, fat-pad atrophy, calf tightness, abnormal gait, or referred lumbar pain. A patient treated for Morton’s neuroma may also have metatarsalgia or small joint overload. After surgery, true complications such as infection, scar-related pain, nerve irritation, incomplete decompression, persistent mechanical overload, or recurrent symptoms must be considered. If these are excluded, reassessment should focus on fascia, tendon, nerve, joint, footwear, gait, systemic factors, and whether the original diagnosis was complete.
Will I need surgery if I have chronic foot pain?
Most patients with chronic foot pain do not need surgery. Many cases improve when the dominant pain generator is identified and treated with a structured combination of medication, load modification, footwear changes, orthotics, physiotherapy, stretching, image-guided injections, shockwave therapy, or nerve-directed procedures. Surgery is reserved for selected cases, such as plantar fasciitis that remains disabling after many months of well-performed conservative care, Morton’s neuroma that does not respond to targeted injections, or severe tarsal tunnel compression with objective nerve involvement. The decision should not be based only on imaging or persistent symptoms. It should depend on the exact structure causing pain, duration of symptoms, previous treatment quality, neurological findings, mechanical factors, and realistic expected benefit.
Can foot pain come from the lower back or a referred nerve source?
Yes. Foot pain can sometimes come from the lower back, especially when lumbar nerve root irritation produces radiating pain, numbness, tingling, burning, or weakness into the leg or foot. This may mimic local foot disorders such as tarsal tunnel syndrome, Morton’s neuroma, plantar fasciitis, or peripheral neuropathy. Referred lumbar pain is more likely when symptoms are associated with back pain, leg pain, position-dependent symptoms, sensory changes, or pain that does not match local foot examination. However, local foot pathology and lumbar referral can also coexist. A proper evaluation compares the foot pain location, neurological pattern, walking triggers, back symptoms, imaging, EMG/NCS when needed, and response to local diagnostic injections before deciding on treatment.
Can metabolic or systemic factors make persistent foot pain harder to treat?
Yes. Metabolic and systemic factors can make persistent foot pain harder to treat, even when a local diagnosis is present. Obesity increases load on the plantar fascia, metatarsal heads, and Achilles tendon. Insulin resistance, diabetes, thyroid disease, autoimmune conditions, chronic inflammatory states, poor sleep, and pro-inflammatory diet may increase pain sensitivity and reduce tissue recovery. Low vitamin D or B12 may impair healing, while excessive vitamin B6 can contribute to nerve-related sensory symptoms in some patients. Peripheral neuropathy, small-fiber neuropathy, medication effects, repeated injections, incomplete rehabilitation, and chronic pain cycles may also maintain symptoms. These factors rarely act as the only cause, but they can reduce the effect of otherwise appropriate local treatment.
Can an online video consultation help identify the source of persistent foot pain?
An online video consultation can help identify the likely source of persistent foot pain when the case is non-emergent and the patient already has imaging, treatment history, or conflicting recommendations. Reports from X-ray, MRI, ultrasound, EMG/NCS, previous injections, surgery, orthotics, or physiotherapy can be reviewed together with the exact pain location and symptom pattern. Video assessment can help evaluate gait, pain during standing or walking, footwear factors, heel versus forefoot pain, burning or tingling, first-step pain, and whether symptoms suggest fascia, tendon, joint, nerve, or referred lumbar involvement. It cannot replace urgent in-person care or every physical test, but it can clarify what should be checked locally next and whether surgery, guided injections, or conservative care is most reasonable.
Additional Patient Resources — Foot Pain
-
NHS — Foot pain overview
Patient-friendly guide to common foot pain locations, self-care, and when to seek medical help. -
AAOS OrthoInfo — Plantar Fasciitis & Bone Spurs
Symptoms, causes, and non-surgical/surgical options for heel pain. -
AAOS OrthoInfo — Morton’s Neuroma
What it is, typical symptoms (burning/tingling), and treatment choices. -
AAOS OrthoInfo — Achilles Tendinitis
Causes of mid-portion vs insertional pain, rehab basics, and when imaging is needed. -
Cleveland Clinic — Tarsal Tunnel Syndrome
Symptoms, diagnosis (NCS/EMG, imaging), and conservative vs surgical care.