Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon and Pain Specialist
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
March 08, 2026
Who This Chronic Pain Page Is For
This page is intended for patients with chronic pain (such as low back pain, neuralgia, neck pain, or post-surgical pain) in whom symptoms have persisted despite treatment, and where the exact cause of pain has not been clearly identified. In many cases, the true source of pain lies in underlying processes within joints, ligaments, muscles, fascia, or nerves — such as inflammation, micro-injury, or nerve irritation — which are not visible on standard imaging. Even incidental or age-related findings seen on scans are often incorrectly assumed to be the cause of pain.
If you have received different diagnoses or treatments without a clear explanation of the underlying mechanism of pain, or if you are trying to understand how factors such as mechanical load, daily activities, obesity, metabolic or inflammatory disturbances, nutritional deficiencies, and nervous system changes contribute to the persistence of pain, an individualized second opinion consultation may help identify the true source of pain and all contributing factors, and define a structured and personalized treatment approach rather than relying on isolated or symptomatic therapies.
When patients with chronic pain seek a second opinion
• Pain has persisted despite medications, physical therapy, or procedures, without clear or lasting improvement
• A diagnosis was given (such as low back pain, neuralgia, or post-surgical pain), but the exact cause of pain was not clearly explained
• MRI or CT findings are present, but it is unclear whether they truly explain the symptoms or are incidental
• There is uncertainty about which structure is actually generating pain (joint, ligament, muscle, fascia, or nerve)
• Daily activities such as sitting, work, or movement may be maintaining pain, but it is unclear how to reduce load on the painful structures
• There is awareness that factors such as obesity, metabolic imbalance, inflammation, or nutritional deficiencies may contribute, but they have not been fully evaluated
• Pain has reduced physical activity, leading to deconditioning or weight gain, making recovery more difficult
• There is a need to understand whether all contributing factors have been identified and how to combine them into an effective treatment strategy
If your situation involves persistent pain, unclear cause, or insufficient response to treatment, a detailed analysis of the pain mechanism — including the true pain generator and all contributing factors described on this page — may help define a more effective and individualized treatment approach:
Request Second Opinion
Chronic Pain — Quick Summary (Read This First)
- Chronic pain usually has a specific local source. It most often originates from joints, ligaments, muscles, fascia, or peripheral nerves, even when imaging does not clearly show it.
- Imaging findings often do not explain the real cause of pain. Many changes seen on MRI or CT are incidental or age-related and may not be responsible for symptoms.
- Pain rarely persists because of a single problem. It is usually maintained by a combination of mechanical, metabolic, inflammatory, and nervous system factors.
- Mechanical overload is one of the most common reasons pain continues. Daily activities such as prolonged sitting, repetitive movements, poor posture, computer work, or asymmetrical loading may constantly irritate the same structure.
- Metabolic, hormonal, and inflammatory factors can significantly influence pain. Conditions such as insulin resistance, excess body weight, chronic low-grade inflammation, and thyroid disorders (including hypothyroidism) increase pain sensitivity and slow recovery.
- Nutritional deficiencies — but also excess intake — may contribute to persistent symptoms. Deficiencies in vitamin B12, vitamin D, magnesium, or iron can affect nerves and muscles, while excessive intake of vitamin B6 may itself cause or worsen neuropathic symptoms.
- Certain medications and previous treatments may maintain or worsen pain. Statins may cause muscle pain, long-term use of analgesics can increase pain sensitivity, corticosteroids affect tissue quality, and sedatives may reduce activity and indirectly worsen the condition.
- Other medical conditions often contribute to persistent pain. Diabetes, anemia, autoimmune and inflammatory diseases, sleep disorders, and hormonal imbalances may reduce the effectiveness of treatment.
- Over time, in chronic pain, the nervous system may become more sensitive. This process (central sensitization) can cause pain to persist even when the original tissue problem is reduced.
- Reduced activity and weight gain often create a cycle that maintains pain. Pain limits movement, leading to deconditioning and increased mechanical and metabolic load.
- Treatment often fails because it is not directed at the true pain mechanism. The problem is usually not that nothing works, but that therapy is not targeted correctly.
- Effective treatment requires a combined and individualized approach. It must address the local pain generator together with all contributing factors at the same time.
Most readers benefit from reviewing this Quick Summary together with the sections on Diagnosis of the True Cause of Pain, Mechanical Factors, Metabolic and Nutritional Factors, and Treatment Approach. The following sections provide a detailed explanation of how these factors interact and how they can be addressed in a structured and individualized way.
Contents
- Who This Page Is For
- Quick Summary
- Local Source of Pain
- Central Sensitization
- Diagnosis
- Why Pain Persists
- Mechanical Overload
- Metabolic Factors
- Nutritional Deficiencies
- Diet
- Obesity
- Tissue Quality
- Sleep and Hormonal Regulation
- Autonomic Nervous System
- Gut–Brain Axis
- Psychological Factors
- Allostatic Load
- Second Opinion
- Comprehensive Treatment
- Anti-Inflammatory Diet
- Osteopathic Approaches
- Key Takeaway
- FAQ
Why Treatment Fails in Chronic Pain — What Is Actually Missed in Diagnosis and Treatment
In many patients, treatment fails not because the condition is untreatable, but because the pain is not precisely analyzed at three critical levels.
First, the exact anatomical structure responsible for the pain is often not identified. Pain may be attributed to findings seen on imaging, while the true source — such as joints, ligaments, muscles, fascia, or nerves — remains unrecognized.
Second, even when the correct structure is suspected, the specific pathological process within that structure is not clearly defined. Inflammation, mechanical irritation, instability, micro-injury, or nerve sensitization require different treatments, yet therapy is often applied without this distinction.
Third, contributing factors that continue to provoke and maintain pain are frequently overlooked. These include mechanical overload, repetitive strain, asymmetrical loading, and poor movement patterns, but also chronic low-grade inflammation, metabolic factors (such as insulin resistance), nutritional influences, and altered tissue recovery capacity. Because these processes remain active, they can continuously trigger pain even when the primary condition is being treated.
Because of this, treatment may appear correct but remains incomplete, which is why pain persists or returns.
For this reason, when treatment does not work, the key step is not repeating the same approach, but performing a structured reassessment — identifying the exact structure involved, the process within it, and all relevant contributing factors that sustain the pain.
This is why chronic pain is often misunderstood and incorrectly treated in everyday clinical practice. It may appear as low back pain, nerve pain (neuralgia), post-surgical pain, or widespread pain syndromes such as fibromyalgia. Although these conditions seem different, they are often driven by similar underlying mechanisms.
Most patients are given a “diagnosis” that is often just the name of a syndrome (such as trigeminal neuralgia or low back pain). This describes where the pain is or how it behaves, but does not explain its true cause. A true diagnosis would identify the underlying problem — for example, not just low back pain, but inflammation at the attachment of specific posterior ligaments of the sacroiliac joint. At the same time, imaging findings are often presented as the cause, even though many of these changes are incidental and not responsible for the patient’s symptoms. In the same patient with low back pain, if imaging shows degenerative disc changes, these are often assumed to be the cause without detailed clinical evaluation, even though they may simply be age-related findings, especially in older patients. Even when a specific ligament inflammation is identified as the source of pain, it is essential to detect the systemic contributing factors that promote the onset and persistence of the pain syndrome (e.g., improper sitting posture, pro-inflammatory diet, metabolic disturbances, etc.).
Identifying which of these factors are dominant in an individual patient is often not straightforward and usually requires structured clinical analysis, as multiple factors frequently coexist and interact. This applies to most chronic pain syndromes, including conditions such as interstitial cystitis, occipital neuralgia, pudendal neuralgia, intercostal neuralgia, postherpetic neuralgia, low back pain, Tarlov cyst and neck pain where different mechanisms may overlap and lead to incomplete or ineffective treatment.
This page explains the local and contributing mechanisms that can cause pain to persist and lead to unsuccessful treatment when they are not properly identified.
Organizational and system-related reasons why pain treatment may fail — such as limited consultation time, protocol-based therapy, or lack of follow-up — are explained here: Understanding why pain treatment may fail in real clinical practice
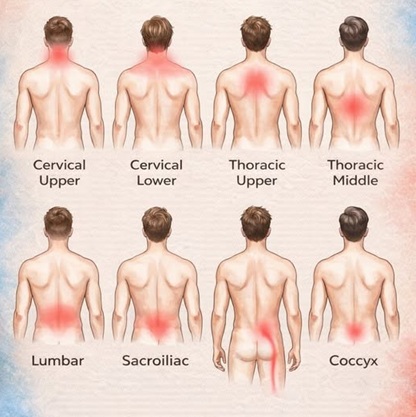
Image: Different types of back pain
Chronic Pain Has a Local Source — Even When It Is Not Visible on Images
In most cases, pain begins in a specific structure such as:
- joint
- ligament
- muscle
- fascia
- peripheral nerve
This structure is called the pain generator.
What Is Actually Happening in These Tissues
Pain is rarely caused by a single process.
In most cases, it develops through a combination of:
- inflammation
- micro-injury / repetitive strain
- muscle spasm
- fascial tension
- nerve irritation or micro-compression
Here are 2 examples of the combination of different processes developing in tissues.
1) Fascia — the invisible source of pain
Fascia (connective tissue) is one of the most common sources of chronic pain.
It can:
- become tight
- lose elasticity
- develop trigger points
And importantly, it is not visible on standard imaging.
2) Nerve irritation without clear damage
Nerves may be affected in very small compression zones:
- without major structural compression
- without clear MRI findings
This leads to persistent pain signals despite “normal” imaging.
Central Sensitization — Why Pain Becomes Persistent
Over time, continuous pain signals lead to changes in the nervous system. This process is called central sensitization, often described as the “wind-up” phenomenon.
With repeated stimulation, the nervous system becomes increasingly reactive:
- minor stimuli produce stronger pain
- normally non-painful sensations may become painful
- pain persists even after the initial cause is reduced
This is one of the key reasons why chronic pain behaves differently from acute pain. A similar mechanism of central sensitization is often seen in conditions such as fibromyalgia.
Treatment may include:
- explanation of pain mechanisms
- appropriate medication when needed
- gradual exposure to movement
- reduction of fear and avoidance patterns
This is particularly important in long-lasting pain.
Diagnosis of the True Cause of Pain
In many patients, the true pain generator is not clearly visible on MRI or CT scans. At the same time, imaging may show abnormalities that are incidental, age-related, and not responsible for symptoms.
Because of this, establishing a correct diagnosis requires a detailed understanding of pain anatomy—that is, knowing which specific structures can produce pain in a given syndrome (such as low back pain, atypical trigeminal neuralgia, or neck pain) and how to confirm their involvement.
In clinical practice, physical examination is often more important than imaging. The key is to analyze:
- the characteristics of pain
- what triggers it
- what reduces or worsens it
and to perform targeted tests that increase or decrease pain, helping to identify the true source.
These assessments can be performed not only in person, but also during video consultations. In many cases, the relevant information is already present in the medical documentation patients provide, or can be recognized through guided testing during the consultation—although patients are often not aware of its importance.
This is one of the main reasons why pain can persist for a long time despite treatment: the underlying cause has not been precisely identified, and therapy is therefore not directed at the true pain generator.
Treatment Begins With Identifying the True Source of Pain
Once the pain generator is identified, treatment becomes significantly more effective.
Medication strategy
Treatment usually starts with carefully selected combinations of medications, adjusted gradually over time.
This is particularly important in patients who:
- already had procedures
- underwent surgery
- did not improve with standard therapy
Very often, the problem is not that “nothing works,” but that the treatment was not targeted to the real source of pain
Advanced options
If needed, additional methods may be used:
- nerve blocks
- radiofrequency ablation
- neuromodulation
- surgery
Chronic Pain Is Not Only a Local Problem
One of the most important facts is that chronic pain is almost never caused by a single factor
Instead, it persists because multiple systems interact at the same time, including:
- mechanical load and daily habits
- muscle and fascial tension
- nerve sensitivity and autonomic nervous system activity
- metabolic and inflammatory factors
- nutritional status and pro-inflammatory diet
- tissue quality and regeneration capacity
- sleep, circadian rhythm, and hormonal regulation
- gut–brain interactions
- psychological and emotional factors
- cumulative stress on the body over time
These factors do not act independently — they often reinforce each other, creating a persistent pain cycle.
Mechanical Overload and Daily Habits as Contributing Factors to Chronic Pain
Chronic pain is very often maintained by continuous mechanical stress. Common examples include:
- prolonged sitting — most often affecting the lumbosacral region and neck
- long periods in fixed positions (standing or sitting without movement)
- repetitive lifting or carrying loads (especially with poor technique)
- repetitive movements (typing, using a mouse, manual work, sports which can cause irritation of the ulnar nerve at the wrist, or elbow, or the median nerve)
- prolonged computer or smartphone use (forward head posture, shoulder strain)
- asymmetrical postures (leaning to one side, crossing legs compressing the perineal nerve, carrying a bag on one shoulder, or a tight belt in meralgia )
- sleeping in poor positions (improper pillow or mattress support)
- sudden increase in physical activity (unprepared tissues exposed to higher load)
- Altered gait patterns due to anomalies (leg length discrepancy) or joint diseases, such as those affecting the hip, knee, or ankle.
High-risk groups
Certain professions are particularly exposed:
- working at a computer for many hours daily
- professional musicians (neck, shoulder, wrist overload)
- office workers
- manual laborers
- athletes with repetitive movements
Over time, this leads to:
- chronic overload of fascia, ligaments, muscles, and joints
- micro-injuries from repeated strain
- local inflammation
- slower tissue recovery
- muscle fatigue and persistent muscle spasm
- reduced flexibility of soft tissues
- joint irritation
- nerve irritation, micro-compression, and sensitization- Thoracic outlet syndrome, or pain after nerve injury
Importantly, these factors can be corrected only after identifying which specific structure is generating pain, what process is occurring within it, and how to reduce or relieve the load on that exact tissue. Once this is identified, it is necessary to carefully analyze the situations in which mechanical load occurs, in order to understand how to relieve stress on the painful structures. Different patients with low back pain do not require the same type of unloading.
For example:
- if pain comes from posterior ligaments of the sacroiliac joint, prolonged sitting and certain movements may need to be modified, sometimes with the use of cushions, new chair or positional adjustments
- if the problem is cervical muscle and fascial overload, computer posture and head position need to be corrected
- if pain is related to repetitive wrist or forearm strain, hand positioning and activity patterns must be adjusted
- if a peripheral nerve is irritated, even small positional changes may significantly reduce symptoms
Metabolic and Inflammatory Factors as Contributing Factors to Chronic Pain
Certain systemic conditions can significantly influence pain:
- insulin resistance
- excess visceral fat and adipokine activity
- elevated uric acid
- chronic low-grade inflammation
- excess body weight (increased mechanical and inflammatory load)
- hormonal imbalance (especially thyroid dysfunction and altered cortisol regulation)
These factors:
- increase pain sensitivity
- slow tissue recovery
- reduce treatment effectiveness
Because of this, in chronic pain, basic laboratory evaluation is often necessary, including:
- fasting glucose
- fasting insulin
- HbA1c
- glucose and insulin response after a glucose load (when indicated)
- lipid profile
- thyroid function tests
- inflammatory markers
- uric acid levels
When these abnormalities are identified, targeted correction can significantly improve pain control, especially when combined with treatment directed at the actual pain source.
Nutritional Deficiencies as Contributing Factors to Chronic Pain
Deficiencies in key nutrients can directly affect pain:
- vitamin B12 — nerve dysfunction and neuropathic pain
- vitamin D — musculoskeletal pain, weakness, and reduced recovery
- magnesium — muscle tension, cramps, and increased excitability
- iron — fatigue and reduced muscle performance
- vitamin B1 (thiamine) — nerve dysfunction, especially in metabolic and alcohol-related conditions
- vitamin B6 — both deficiency and excess may contribute to neuropathic symptoms
Even mild deficiencies may contribute to persistent symptoms. In many patients, these deficiencies are not recognized without appropriate testing.
Evaluation may include:
- vitamin B12 levels
- vitamin D levels
- magnesium levels
- iron status
- selected B vitamins when clinically indicated
Correction may include:
- targeted supplementation
- dietary adjustments
- follow-up monitoring
However, supplementation alone is usually not sufficient unless the underlying cause of pain is also identified and treated.
These deficiencies do not act in isolation — they often coexist with metabolic and inflammatory factors, further increasing pain sensitivity and slowing recovery.
Diet and Its Role in Chronic Pain
Diet does not only affect nutrient levels — it also directly influences inflammation, metabolism, and pain sensitivity.
In many patients, dietary habits contribute to the persistence of pain, especially when metabolic disturbances such as insulin resistance or chronic low-grade inflammation are already present.
Common contributing patterns include:
- high intake of processed foods and refined carbohydrates
- excessive sugar consumption
- frequent spikes in blood glucose and insulin levels
- imbalance between pro-inflammatory and anti-inflammatory nutrients
- irregular eating patterns and long periods without proper meals
These factors may:
- increase systemic inflammation
- worsen metabolic imbalance
- increase pain sensitivity
- slow tissue recovery
Importantly, even foods generally considered healthy may have negative effects when consumed in inappropriate amounts or in the wrong metabolic context. For example, fruit contains important nutrients and antioxidants, but high intake of sugars may worsen glucose regulation in patients with insulin resistance, indirectly contributing to inflammation and persistence of pain.
Similarly, diets that appear “balanced” may still promote inflammation if they:
- contain excessive refined carbohydrates
- lack sufficient protein
- include poor-quality fats
Because of this, evaluating diet is not about following a universal plan, but about understanding how specific eating patterns affect the individual patient.
Dietary changes can significantly improve pain control, but only when they are aligned with:
- the patient’s metabolic state
- the underlying pain mechanism
- other contributing factors such as mechanical load and nervous system sensitization
For this reason, diet should always be considered as part of a comprehensive approach to chronic pain, rather than as an isolated solution.
Obesity and Its Role in Chronic Pain
Obesity influences chronic pain through multiple interacting mechanisms.
On a mechanical level, excess body weight increases load on joints, ligaments, and the spine, particularly in:
This leads to:
- faster tissue overload
- joint irritation
- earlier muscle fatigue
However, obesity is not only a mechanical problem.
Adipose tissue is metabolically active and produces substances (adipokines) that contribute to:
- chronic low-grade inflammation
- increased pain sensitivity
- slower tissue healing
Because of this, obesity is closely linked with:
- insulin resistance
- metabolic imbalance
Another important factor is reduced physical conditioning.
Many patients with chronic pain decrease their activity over time, which leads to:
- loss of muscle strength
- reduced endurance
- decreased joint and spine stability
This creates a cycle:
pain → reduced activity → deconditioning → more pain
For these reasons, obesity should be understood as a combined mechanical, metabolic, and functional factor in chronic pain. Obesity can contribute to the development and persistence of chronic pain. At the same time, chronic pain often reduces mobility and physical activity, which can lead to weight gain.
This creates a cycle:
pain → reduced movement → weight gain → increased load and inflammation → more pain
Because of this, simply advising patients to lose weight, without first reducing pain and enabling movement, is often not realistic or effective.
A combined approach is usually necessary, where pain is addressed first to allow gradual return to activity, which then supports sustainable weight reduction.
Tissue Quality and Regeneration
Not all tissues recover equally.
Factors such as:
- reduced blood flow
- degeneration
- repeated micro-injuries
lead to:
- slower healing
- increased vulnerability to pain
In many patients, additional factors further impair tissue recovery, such as:
- persistent mechanical overload
- age-related changes in tissue structure
- chronic low-grade inflammation
- inadequate nutrition (e.g., vitamin D deficiency)
When these factors are present, treatment directed only at symptoms is often not sufficient.
Medications may temporarily reduce pain, but they usually cannot provide significant or lasting improvement unless the underlying conditions affecting tissue recovery are also addressed.
Sleep, Circadian Rhythm, and Hormonal Regulation
Sleep quality and circadian rhythm play an important role in how pain is processed.
Poor or disrupted sleep can:
- increase pain sensitivity
- reduce pain tolerance
- impair tissue recovery
Hormonal regulation, particularly cortisol rhythm, also influences inflammation and pain perception.
Because of this, sleep is not usually the primary cause of pain, but it can significantly amplify existing pain and slow recovery.
Autonomic Nervous System as a Contributing Factor to Chronic Pain
The autonomic nervous system plays a major role in chronic pain. In some patients, increased sympathetic activity maintains pain.
This may lead to:
- temperature changes
- altered circulation
- increased sensitivity
This mechanism is especially important in:
- sympathetically maintained pain
- CRPS (complex regional pain syndrome)
Gut–Brain Axis as a Contributing Factor to Chronic Pain
The gastrointestinal system can influence pain through several mechanisms, particularly in patients with metabolic or inflammatory disturbances.
Relevant factors include:
- altered gut motility (constipation, irregular bowel function)
- changes in gut microbiota composition (dysbiosis)
- increased intestinal permeability
- chronic low-grade inflammation originating from the gut
These changes may:
- contribute to systemic inflammation
- affect nervous system sensitivity
- influence how pain is perceived and maintained
In clinical practice, this is more relevant in patients who also have:
- bloating or abdominal discomfort
- irregular bowel movements
- food intolerances
- symptoms consistent with irritable bowel syndrome
Addressing these factors may support overall pain management, but they are rarely the primary cause of chronic pain.
Treatment approaches may include:
- dietary adjustments
- correction of nutritional deficiencies
- management of bowel function
- in selected cases, modulation of gut microbiota (e.g., probiotics or prebiotics), although evidence remains variable
The goal is not to “treat the gut instead of pain,” but to reduce contributing systemic factors that may amplify pain.
Psychological and Emotional Factors as Contributing Factors to Chronic Pain
Psychological factors do not mean that pain is imaginary. Pain is a real biological process, but it is also influenced by how the nervous system processes and amplifies signals.
In many patients, persistent pain leads to changes in the nervous system, a process known as central sensitization.
Over time, this may result in:
- increased sensitivity to pain
- stronger response to minor stimuli
- persistence of pain even when the original cause is reduced
Emotional and psychological factors interact with this process.
Important factors include:
- chronic stress
- anxiety
- depression
It is often assumed that depression causes pain. In reality, the opposite is frequently true — long-lasting pain leads to psychological distress, which then further amplifies pain and makes treatment more difficult.
These factors can:
- lower pain threshold
- increase muscle tension
- maintain a cycle of pain → stress → more pain
Because of this, psychological factors are not the primary cause of pain, but they can significantly influence its intensity, persistence, and response to treatment.
Treatment of depressive and anxiety-related factors in chronic pain involves a combination of pharmacological and non-pharmacological approaches. In clinical practice, antidepressants are often used, as they can reduce the perception of pain by acting on central pain-processing mechanisms, in addition to improving mood. Psychotherapy plays an important role, helping patients better understand and manage their responses to pain.
Support from family and close social environment is also a significant factor, as it reduces the feeling of isolation and improves motivation for treatment. In some individuals, spiritual aspects (such as religion) may have a positive effect, as well as relaxation techniques, including breathing exercises and gradual return to daily activities.
However, this approach is often overemphasized in practice, especially when the true anatomical source of pain has not been clearly identified. In such cases, treatment may remain incomplete, as it addresses the consequences rather than the underlying cause.
Cumulative Stress on the Body (Allostatic Load)
Chronic pain is rarely caused by a single event.
It often develops after years of:
- physical strain
- poor sleep
- metabolic imbalance
- psychological stress
This cumulative burden is called allostatic load.
It reduces the body’s ability to regulate pain effectively.
Medications and Previous Treatments That May Contribute to Pain
Chronic pain may sometimes be influenced or maintained by medications or previous treatments. This is often overlooked.
Certain drugs can affect:
- muscle function
- nerve sensitivity
- metabolic balance
- inflammatory processes
Common examples include:
- statins — may contribute to muscle pain, weakness, or increased muscle sensitivity
- some antidepressants — may alter pain perception or cause fatigue
- long-term use of certain pain medications — may lead to reduced effectiveness or increased sensitivity (medication overuse or hyperalgesia)
- corticosteroids — may affect metabolism, muscle tissue, and recovery
- sedative medications — may reduce physical activity and worsen deconditioning
- vitamin B6 (pyridoxine) excess — prolonged high intake (often through supplements) may lead to sensory neuropathy, tingling, or burning pain; both deficiency and excess can affect nerve function
Previous treatments may also play a role:
- surgery (scar tissue, altered biomechanics, nerve irritation), similar to postdiscectomy pain, pain after surgery of internal organs, pain after lumbar or cervical spine surgery
- repeated injections
- incomplete or misdirected rehabilitation programs
In many patients, these factors do not directly cause pain, but they may:
- maintain or amplify existing pain
- interfere with recovery
- reduce the effectiveness of otherwise appropriate treatment
Because of this, a detailed review of all medications and previous treatments is an important part of evaluation.
In some cases, modifying or adjusting therapy may significantly improve symptoms.
Other Medical Conditions That May Contribute to Pain
Chronic pain is sometimes influenced by other medical conditions that are not directly related to the primary pain source.
These conditions may:
- increase pain sensitivity
- slow recovery
- reduce treatment effectiveness
Common contributing conditions include:
- diabetes and insulin resistance — affecting nerve function and healing
- thyroid disorders — influencing metabolism and muscle function
- chronic inflammatory conditions
- autoimmune diseases
- anemia and chronic fatigue states
- hormonal imbalances
- sleep disorders
In some patients, these conditions are already diagnosed but not considered relevant to pain.
In others, they remain unrecognized.
These factors rarely act as the sole cause of pain, but they often:
- maintain symptoms
- make pain more persistent
- reduce response to treatment
Because of this, identifying and addressing these conditions is an important part of a comprehensive approach to chronic pain.
How the Cause of Pain Is Identified
Effective diagnosis requires identifying:
- which structure generates pain (joint, disc, muscle, fascia, ligament, nerve)
- why that structure remains irritated (mechanical overload, posture, repetitive strain, poor movement patterns)
- which systemic factors prevent recovery (metabolic imbalance, inflammation, hormonal factors)
- whether nutritional deficiencies are present
- how the nervous system has adapted (central sensitization)
- which additional factors contribute (sleep, stress, obesity, medications, comorbidities)
This type of analysis is based on knowledge of pain anatomy, functional examination (in person or via telehealth), and interpretation of imaging in clinical context.
Request Chronic Pain Second Opinion — Identify the Cause and Contributing Factors (24-Hour Review, Priority Within Hours)
Patients with chronic pain and unsuccessful treatment often face the same unanswered questions:
What is actually causing the pain?
Is the diagnosis correct?
Why does pain persist despite therapy?
Are all contributing factors identified — including posture, work habits, weight, metabolism, and nervous system sensitivity?
Is treatment addressing the real pain generator or only symptoms?
An independent medical second opinion focuses on identifying the true source of pain and all contributing factors,
including mechanical overload, muscle and fascial dysfunction, nerve irritation, metabolic influences, body weight, daily activity patterns, and possible central sensitization.
The goal is to explain why previous treatments did not work and what can realistically be improved.
- ✔ Describe your pain (location, duration, triggers, previous treatments) and send available medical documentation
- ✔ You will receive a reply within 24 hours explaining whether an online consultation is appropriate and what additional information is needed
- ✔ Priority cases: severe persistent pain, rapidly worsening symptoms, inability to function normally, or multiple failed treatments — write PRIORITY in your first message
- ✔ Imaging (MRI/CT), previous reports, therapy history, and daily activity patterns are reviewed to identify the true pain generator and contributing factors
- ✔ During consultation we explain the mechanisms maintaining your pain and which factors can be modified — including posture, workload, movement patterns, weight, and metabolic influences — with realistic expectations and up to 10 days of follow-up clarification
Consultation fees typically range from $180–250 depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This corresponds to typical international specialist telehealth second-opinion services.
Why Treatments Do Not Work the Same for Everyone
Not all patients respond equally to the same therapy.
One important reason is genetic variability in drug metabolism.
This explains why some patients feel that “nothing helps” despite appropriate treatment
How Chronic Pain Is Actually Treated
Effective treatment of chronic pain is not possible unless both are identified and addressed:
- the primary pain generator
- the factors that contribute to and maintain the pain
Treatment must target both levels simultaneously.
Anti-Inflammatory Diet and Nutritional Strategy
In many patients, diet directly contributes to the persistence of pain, especially when metabolic disturbances are present.
Treatment includes:
- implementation of an anti-inflammatory diet
- reduction of refined carbohydrates and sugars
- stabilization of glucose and insulin levels
- adequate protein intake
- improvement of fat quality
- individualized adjustment based on metabolic status
An anti-inflammatory diet is not a universal plan, but a structured approach adapted to:
- insulin sensitivity
- level of inflammation
- body composition
- type of pain
Even foods considered healthy, such as fruit, may contribute to metabolic imbalance when consumed in excess, particularly in patients with insulin resistance.
Dietary intervention can significantly improve pain control, but only when combined with treatment of the underlying pain mechanism.
Manual Therapy and Osteopathic Approaches
Manual therapy techniques, including osteopathic treatment, are often used in patients with chronic pain, particularly when dysfunction involves muscles, fascia, joints, or movement patterns.
These approaches may include:
- mobilization of joints
- soft tissue and fascial techniques
- muscle relaxation methods
- correction of movement patterns
In selected patients, such techniques can reduce local tissue tension, improve mobility, and temporarily decrease pain.
However, their effectiveness depends on whether the actual pain generator has been correctly identified.
Limitations of Osteopathic and Manual Therapy Approaches
In many patients with chronic pain, manual therapy alone is not sufficient.
This is particularly true when:
- the primary pain source is not correctly identified
- mechanical overload persists in daily activities
- metabolic or inflammatory factors are present
- central sensitization has developed
In such cases, manual therapy may provide only temporary relief without addressing the underlying mechanism of pain.
Because of this, these methods should be considered as part of a broader, individualized treatment strategy, rather than a standalone solution.
What Effective Treatment Usually Requires
In patients with chronic pain, treatment usually requires a combination of:
- treatment of the local pain generator (medications, injections, interventions, neuromodulation, or surgery when indicated)
- reduction of mechanical overload (posture, activity modification, ergonomic adjustments)
- correction of metabolic, inflammatory, and hormonal factors
- nutritional optimization and an anti-inflammatory diet
- weight reduction when needed, but only together with pain control and gradual return to movement
- carefully adapted physical rehabilitation that does not irritate the actual pain source
- addressing central sensitization and abnormal pain amplification
- improving sleep, recovery, and autonomic regulation
- recognizing the role of medications, previous treatments, and other medical conditions
- psychological support and stress reduction when these factors amplify pain
Effective treatment is usually not based on one method, but on combining several approaches in the right order, according to the patient’s specific pain mechanism and contributing factors.
In clinical practice, priority should be given to identifying and treating the primary pain-generating structure, while other contributing factors are addressed as supportive elements. These factors are not present in all patients, and even when they are, they rarely lead to meaningful improvement unless the underlying source of pain is properly treated.
Key Takeaway
Chronic pain is not caused by a single problem.
It is the result of interaction between:
- a local pain source
- mechanical stress and daily habits
- metabolic, nutritional, and inflammatory factors
- nervous system changes (including central sensitization)
- psychological and functional factors
Effective treatment begins only when all of these are identified and addressed together, in a coordinated and individualized way. However, in clinical practice, there is often an excessive focus on a single contributing factor. These factors are not present in all patients, and even when they are, addressing them alone is usually insufficient without first identifying and treating the primary pain-generating structure.
Frequently Asked Questions About Chronic Pain and Its Causes
Why does chronic pain persist despite treatment?
Chronic pain often persists because treatment is directed at symptoms rather than at the true pain mechanism. In many patients, the exact pain generator — such as a joint, ligament, muscle, fascia, or peripheral nerve — has not been clearly identified. Even when a painful structure is suspected, the actual process inside it may be unclear: inflammation, mechanical irritation, micro-injury, instability, spasm, or nerve sensitization require different approaches. Treatment may also fail because contributing factors remain active, including prolonged sitting, repetitive strain, obesity, insulin resistance, poor sleep, nutritional deficiencies, or central sensitization. In that situation, medication or procedures may reduce pain temporarily, but the same mechanism continues to provoke symptoms.
Can chronic pain exist even if MRI or CT findings are minimal?
Yes. Chronic pain can be real and severe even when MRI or CT findings are minimal, because many important pain sources are not clearly visible on standard imaging. Fascia, ligaments, small joint structures, muscle attachments, minor nerve irritation, and functional overload may produce significant pain without showing a dramatic abnormality on scans. At the same time, MRI may show age-related disc changes, arthritis, or other findings that are incidental and not responsible for symptoms. This is why imaging must be interpreted together with pain location, triggers, relieving factors, neurological findings, and targeted clinical testing. A normal or mild scan does not prove that pain is psychological; it often means that the true pain generator requires more precise clinical analysis.
What is meant by the pain generator in chronic pain?
The pain generator is the specific anatomical structure that is producing the pain signal. In chronic pain, this may be a joint, ligament, muscle, fascia, disc-related structure, peripheral nerve, scar tissue, or a small compression zone. Identifying the pain generator is essential because treatment cannot be properly targeted if the source is only described in general terms such as “low back pain,” “neck pain,” or “neuralgia.” Those labels describe the region or pattern of pain, but they do not explain why the pain persists. A true diagnosis should identify both the structure involved and the process within it, such as inflammation, overload, instability, micro-injury, nerve irritation, or sensitization. Without that step, treatment often remains incomplete.
How do daily activities affect chronic pain?
Daily activities can maintain chronic pain by repeatedly irritating the same painful structure. Prolonged sitting, fixed posture, computer work, smartphone use, repetitive lifting, asymmetrical loading, poor sleeping position, or sudden increases in activity may overload joints, ligaments, fascia, muscles, or peripheral nerves. The patient may receive correct medication, injections, or rehabilitation, but if the same mechanical stress continues every day, the irritated tissue does not recover. This is why activity analysis is not just general advice about posture or exercise. The key is to identify which structure is painful and then determine which positions or movements increase load on that exact tissue. Different patients with similar pain locations may need very different unloading strategies.
Can obesity and metabolism influence chronic pain?
Yes. Obesity and metabolic factors can influence chronic pain through both mechanical and biological mechanisms. Excess body weight increases load on the spine, joints, ligaments, hips, knees, and feet, which can worsen tissue irritation and slow recovery. However, obesity is not only a mechanical issue. Visceral fat is metabolically active and may contribute to chronic low-grade inflammation, insulin resistance, altered adipokine activity, and increased pain sensitivity. Metabolic disturbances such as elevated insulin, glucose dysregulation, thyroid dysfunction, elevated uric acid, or inflammatory imbalance can make treatment less effective. These factors rarely explain pain alone, but they can strongly maintain it. Chronic pain treatment is often more successful when local pain mechanisms and metabolic contributors are addressed together.
What is central sensitization in chronic pain?
Central sensitization means that the nervous system becomes more reactive after repeated or prolonged pain signals. Over time, the spinal cord and brain may amplify incoming signals, so minor stimuli feel more painful and normally non-painful sensations may become unpleasant. This does not mean that pain is imaginary. It means that the nervous system has adapted to persistent stimulation and now processes pain differently. Central sensitization is one reason chronic pain may continue even after the original tissue problem has partly improved. Treatment must therefore address both levels: the original pain generator and the amplified nervous system response. Medication, education, gradual movement, sleep improvement, and reduction of fear-avoidance patterns may all be needed.
Can an online second opinion help identify why chronic pain treatment failed?
Yes. An online second opinion can help when chronic pain persists despite medication, physical therapy, injections, procedures, or surgery and the cause remains unclear. The goal is not to repeat the same diagnosis, but to reassess the pain mechanism: where the pain is generated, what process is occurring in that structure, and which factors keep it active. Medical reports, MRI or CT findings, previous treatments, medication history, activity patterns, triggers, weight, metabolic issues, and symptoms can be reviewed together. In many cases, guided video assessment can also clarify which movements or positions reproduce pain. A second opinion is especially useful when imaging findings do not match symptoms, treatments have failed, or different doctors have given different explanations.
What is needed to successfully treat chronic pain?
Successful chronic pain treatment requires much more than prescribing pain medication or reading an MRI report. The doctor must understand all possible pain sources in the painful region. In some areas, there may be 10, 20, or more possible pain generators, including joints, ligaments, muscles, fascia, discs, peripheral nerves, scar tissue, or small zones of nerve irritation. Each possible source must be clinically considered, provoked, confirmed, or excluded through pain history, targeted examination, imaging interpretation, and functional testing. After that, provoking and maintaining factors must be identified, such as sitting, posture, repetitive load, obesity, metabolic imbalance, poor sleep, nutritional deficiency, or central sensitization. Without this structured process, treatment often remains incomplete or random.
How many possible pain generators can exist in one chronic pain region?
In one painful region, there may be many possible pain generators. Depending on the location, 10 to 30 or more structures may potentially produce similar symptoms. For example, low back or pelvic pain may come from discs, facet joints, sacroiliac ligaments, muscles, fascia, peripheral nerves, hip joints, scar tissue, or small zones of mechanical irritation. Neck and head pain may involve cervical joints, muscles, fascia, occipital nerves, trigeminal pathways, or intracranial conditions. This is why chronic pain cannot be understood only by naming the painful area. The diagnostic task is to know the full anatomical list of possible sources, then systematically confirm or exclude them using history, examination, imaging, provocative maneuvers, and response to treatment.
Why do different doctors give different diagnoses or treatments for chronic pain?
Different doctors may give different diagnoses for chronic pain because they often focus on different parts of the problem. One specialist may emphasize MRI findings, another may focus on nerve symptoms, another on muscles or posture, and another on systemic conditions such as inflammation or metabolic imbalance. Chronic pain is frequently maintained by several interacting mechanisms, so a partial assessment can lead to a partial explanation. For example, an MRI finding may be real but incidental, while the true pain generator is a ligament, fascia, joint, or small nerve irritation. Treatment also differs when one doctor focuses on pain relief and another tries to identify why pain is being maintained. A structured reassessment can help separate the primary pain source from contributing factors.
Can prolonged sitting or poor posture keep chronic pain persistent?
Yes. Prolonged sitting and poor posture can keep chronic pain persistent when they repeatedly load the same sensitive structure. Sitting may irritate the lumbosacral region, sacroiliac ligaments, pelvic nerves, hip structures, or painful scars, while computer posture may overload cervical muscles, fascia, joints, and nerves. The problem is not simply that posture is “bad,” but that a specific tissue is being exposed to the same mechanical stress for many hours. If that structure is already inflamed, irritated, or sensitized, treatment may fail unless the load is reduced. Correcting posture therefore requires knowing the actual pain generator. The same chair, cushion, exercise, or ergonomic advice may help one patient and worsen another.
Should weight reduction be the first step in chronic pain treatment?
Weight reduction may be important in chronic pain, but it is not always realistic or effective as the first isolated step. Many patients gain weight because pain limits movement, reduces activity, and causes deconditioning. Simply telling the patient to lose weight may fail if pain remains uncontrolled and normal activity is impossible. In these cases, treatment should first identify and reduce the primary pain generator enough to allow gradual movement. Weight reduction then becomes more achievable and can reduce mechanical load and inflammation. The most effective approach is usually combined: pain control, careful activity restoration, nutritional changes, metabolic correction, and progressive conditioning. Weight matters, but it should be addressed in a strategy that the patient can actually follow.
Can diet and nutritional deficiencies affect chronic pain?
Diet and nutritional deficiencies can affect chronic pain because nerves, muscles, connective tissue, inflammation, and metabolism all depend on adequate biological support. Vitamin B12 deficiency may worsen neuropathic symptoms, vitamin D deficiency may contribute to musculoskeletal pain and weakness, magnesium deficiency can increase muscle excitability, and iron deficiency may reduce performance and recovery. Vitamin B6 is important because both deficiency and excessive supplementation may contribute to neuropathic symptoms. Diet also influences insulin regulation, inflammation, body weight, and tissue healing. However, supplements or diet alone usually do not solve chronic pain if the local pain generator remains untreated. Nutritional correction works best as part of a broader plan that also addresses mechanical, neurological, and metabolic contributors.
Can insulin resistance and chronic inflammation make chronic pain harder to treat?
Yes. Insulin resistance and chronic low-grade inflammation can make chronic pain harder to treat because they influence pain sensitivity, tissue recovery, and treatment response. When insulin levels remain elevated or glucose regulation is unstable, inflammation and metabolic stress may increase. Excess visceral fat can also produce inflammatory signals that affect muscles, joints, connective tissue, and nerves. These factors do not usually create a precise pain location by themselves, but they can make an existing pain generator more reactive and slower to heal. This is why chronic pain assessment may include fasting glucose, fasting insulin, HbA1c, lipid profile, thyroid function, inflammatory markers, and uric acid. Correcting these abnormalities can improve results when combined with local pain treatment.
Why does chronic pain limit activity and make recovery harder?
Chronic pain often creates a cycle in which pain reduces activity, reduced activity causes deconditioning, and deconditioning makes pain easier to trigger. Muscles lose strength and endurance, joints become less supported, posture worsens, and daily activities require more effort. At the same time, fear of movement may develop because patients expect activity to worsen symptoms. This can be protective in the short term but harmful over months or years. Recovery becomes harder when the painful structure is still irritated, but the body is also weaker and more sensitive. The solution is not simply forcing exercise. Activity must be reintroduced gradually, after identifying the pain generator and reducing the specific mechanical or neurological triggers that keep pain active.
Why do some chronic pain patients feel that nothing helps?
Some chronic pain patients feel that nothing helps because treatment has often been incomplete, misdirected, or stopped before the real mechanism was understood. Medication may be chosen without identifying the pain generator. Physical therapy may strengthen the wrong structures or irritate the painful one. Injections may target imaging findings that are not actually responsible for symptoms. Surgery may change anatomy but leave nerve irritation, scar tissue, altered biomechanics, or central sensitization unresolved. Systemic contributors such as insulin resistance, obesity, poor sleep, vitamin deficiencies, medication effects, or inflammation may also reduce treatment response. In many cases, the problem is not that the pain is untreatable, but that the plan has not addressed all dominant mechanisms together.
Can medications or previous treatments contribute to chronic pain?
Yes. Medications and previous treatments can sometimes maintain or worsen chronic pain, although they are not always the primary cause. Statins may contribute to muscle pain or weakness in selected patients. Long-term use of some pain medications may reduce effectiveness or increase pain sensitivity. Corticosteroids can affect tissue quality, metabolism, and recovery. Sedative medications may reduce activity and worsen deconditioning. Excess vitamin B6 from supplements can cause or aggravate sensory neuropathic symptoms. Previous surgery, repeated injections, scar tissue, altered biomechanics, or poorly directed rehabilitation may also contribute. This is why chronic pain evaluation should include a detailed review of medication history, procedures, surgery, rehabilitation, and supplements, not only the current pain complaint.
Can chronic pain be treated if several contributing factors are present?
Yes, but treatment usually has to be structured and individualized. Chronic pain often persists because several factors act together: a local pain generator, mechanical overload, nervous system sensitization, metabolic imbalance, poor sleep, nutritional problems, stress, obesity, medication effects, or previous procedures. Treating only one factor may provide temporary or incomplete relief. The first priority is usually to identify the dominant pain generator and reduce irritation of that structure. Contributing factors are then corrected in parallel, according to their importance in that patient. For example, posture modification, medication adjustment, metabolic correction, anti-inflammatory nutrition, gradual rehabilitation, and treatment of neuropathic mechanisms may all be needed. Improvement is more realistic when the plan matches the actual pain mechanism.
Why is identifying the true pain generator in chronic pain more important than repeating the same treatment?
Identifying the true pain generator is more important than repeating the same treatment because chronic pain often persists when therapy is aimed at the wrong target. If pain is caused by a ligament, fascia, joint, peripheral nerve, scar, or small compression zone, treatment directed only at an incidental MRI finding may fail. Repeating the same medication, injection, or rehabilitation program may give temporary relief or no benefit if the structure producing pain has not been identified. The same applies when the process inside the tissue is misunderstood: inflammation, instability, nerve irritation, muscle spasm, and central sensitization require different strategies. Treatment becomes more rational only when the source, mechanism, and maintaining factors are clarified together.
When should chronic pain be reassessed instead of continuing the same therapy?
Chronic pain should be reassessed when symptoms persist despite reasonable treatment, when improvement is short-lasting, when different doctors give different explanations, or when imaging findings do not match the patient’s symptoms. Reassessment is also important if pain worsens with specific positions, sitting, walking, work activity, or movement patterns that have not been analyzed. Continuing the same therapy may be unhelpful if the pain generator, mechanical load, metabolic factors, medication effects, nutritional deficiencies, or central sensitization were never evaluated. Reassessment does not mean starting from zero. It means reviewing the diagnosis at several levels: which structure hurts, what process is active, what provokes it, what maintains it, and which parts of previous treatment were incomplete or misdirected.