Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery and pain management.
Last medically reviewed:
June 16, 2026
Neck Pain When Lying Down — Quick Summary (Read This First)
- Neck pain when lying down usually means that a sleeping position is stressing an already sensitive part of the neck. The important question is which structure becomes painful during sleep and why that position increases symptoms.
- Neck pain after sleeping can manifest in different ways. It may appear as local neck pain, morning stiffness, pain in the back of the head, shoulder pain, arm pain, tingling, numbness, or a “dead arm” sensation after waking.
- Morning neck pain may develop when the neck stays for hours in a position that overloads the affected structure. Depending on the cause, this may involve cervical joints, discs, ligaments, deep neck muscles, or an unstable cervical segment, so the same sleep position may relieve pain in one patient and worsen it in another.
- Pain in the back of the head when lying down may come from more than one source. Occipital nerves, upper cervical joints, suboccipital muscles, and cervicogenic headache mechanisms may all contribute to this pattern.
- Neck pain with arm tingling or numbness during sleep is not always a disc problem. It may come from cervical nerve-root irritation, shoulder compression, brachial plexus tension, thoracic-outlet-like positioning, or peripheral nerve compression.
- Sleeping on the stomach often worsens neck pain because it keeps the neck in a forced position for several hours. To breathe, the head must stay turned to one side, often with additional extension, which can overload cervical facet joints, deep ligaments, neck muscles, occipital nerves, or cervical nerve roots.
- Sleeping on the side may help some patients but worsen others because it changes how the neck and shoulder are supported. Pillow height, shoulder width, and mattress firmness can place the neck in a tolerable position in one patient, but overload cervical joints, discs, muscles, or ligaments in another.
- Sleeping on the back may reduce rotation, but it can still provoke pain. A pillow that is too high, too low, too firm under the back of the head, or poorly matched to the natural curve of the neck may increase symptoms.
- Cervical instability can make neck pain worse in different lying positions. When a cervical segment is already unstable, certain sleeping positions may increase abnormal movement or mechanical stress at that level, causing local neck pain, muscle spasm, or nerve irritation.
- Loss of cervical lordosis or cervical kyphosis changes what “neutral neck position” means. A rigid pillow that forces the neck into one fixed curve may help some patients but worsen others, especially older patients with degenerative cervical alignment changes.
- A pillow may contribute to neck pain if it holds the neck in the wrong position for several hours. Flexion, extension, side bending, rotation, or focal pressure under the back of the head can provoke pain in susceptible patients.
- The correct pillow is not the same for every patient. Pillow choice depends on the pain generator, sleep position, body shape, shoulder width, mattress firmness, cervical alignment, and symptom pattern.
- A fixed-shape “orthopedic” pillow is not always the best solution. Some patients need stable cervical support, while others need a pillow that can be adjusted or reshaped according to how pain behaves during real sleep.
- MRI findings do not always explain neck pain that appears when lying down. Facet joints, ligaments, occipital nerves, suboccipital muscles, and myofascial trigger points may be painful even when imaging findings are mild or nonspecific.
- Standard sleep advice is only a starting point. The goal is not to find a universally correct sleeping position, but to identify which structure is being overloaded and how to reduce load on that structure.
- The practical goal is to find the sleeping position and neck support that reduce load on the patient’s actual pain generator. This requires identifying which structure becomes painful, why symptoms increase in that position, and which pillow height, sleeping position, or support modification is most suitable for that individual patient.
- When standard pillow and sleep-position advice fails, the next step is not more guesswork but a focused medical evaluation. A focused medical evaluation should connect the pain pattern, sleep position, cervical alignment, imaging findings, movement tests, and pressure-point responses. Without identifying the actual pain generator, pillow and position changes remain guesswork.
Most readers benefit from reviewing this Quick Summary together with sections on why lying down can cause neck pain, standard sleep advice, when pillow and sleep-position advice must be individualized, pain in the back of the head, arm tingling or numbness during sleep, and when medical evaluation is needed.
Contents
- Who this page is for
- When patients seek second opinion
- Neck pain lying down summary
- Not just general sleep advice
- Why lying down causes neck pain
- Why pain appears after sleep
- Standard neck sleep advice
- When standard advice must change
- Why fixed-shape pillows may fail
- Pain generators during lying down
- How lying down loads tissues
- Neck pain when back sleeping
- Neck pain when side sleeping
- Neck pain when stomach sleeping
- Pain patterns during sleep
- Pain in back of head
- Neck pain with arm symptoms
- Why MRI may not explain
- Why general advice may fail
- Same diagnosis, different sleep position
- How to test pillow contribution
- When medical evaluation is needed
- What effective treatment requires
- How online consultation can help
- Start online neck pain consultation
- FAQ about neck pain lying down
This Page Is Not About General Sleep Advice
This page is for patients whose neck pain is position-dependent — pain that appears, worsens, or changes when the head, neck, shoulder, or arm is held in a certain position during sleep.
In these patients, pain usually comes from an already sensitive pain generator — such as a cervical joint, disc, ligament, muscle, nerve, or unstable segment — that may be painful during daily activities, appear only when lying down, or become more obvious after several hours of sleep.
When the neck stays in that position for several hours, the affected structure may be exposed to different types of load:
- compressed
- stretched
- rotated
- irritated
- kept under constant low-grade tension
- exposed to reduced movement and circulation
The main question is not only:
“How should I sleep?”
The more important question is:
“Which structure becomes painful when I lie down, and what position reduces load on that structure?”
This is why advice must often be individualized. A patient with facet-joint pain, a patient with cervical radiculopathy, a patient with occipital neuralgia, and a patient with myofascial neck pain may all describe “neck pain in bed,” but the best sleeping strategy may be different in each case.
Since poor sleeping posture can increase irritation of an already sensitive pain generator, it may become one of the contributing factors that prevents effective treatment of neck pain.
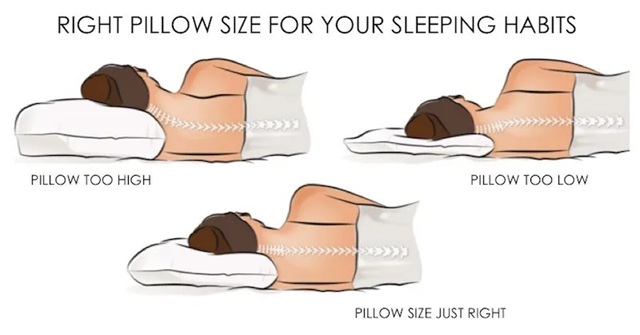
Image: General recommendations for pillow dimensions to keep the neck aligned during side sleeping. However, there are numerous other rules on how to relieve neck pain while lying down, and they depend on the underlying cause—the pain generator.
Why Lying Down Can Cause Neck Pain
During the day, the neck moves frequently. During sleep, however, the cervical spine may remain in one position for a long time. Lying down changes the relationship between the head, neck, shoulders, upper back, and arms.
Even a small positional mismatch can become painful when it lasts for several hours.
Pain may appear when lying down because the neck is held in:
- flexion — when the head is pushed too far forward, such as with a pillow that is too high while lying on the back
- extension — when the head drops backward, the chin points upward, or the upper neck is compressed by poor pillow support
- rotation — especially during stomach sleeping
- side bending — when the pillow is too high or too low during side sleeping
- combined positions — such as rotation with extension or side bending with shoulder compression
These positions can increase load on joints, discs, nerves, ligaments, muscles, and the shoulder–brachial plexus region.
In a healthy and non-sensitized neck, these loads may not cause symptoms. But if a structure is already irritated, inflamed, overloaded, unstable, compressed, or sensitized, lying down can become the trigger that makes pain appear.
This is why some patients feel better when lying down, while others feel worse. The difference is not the act of lying down itself, but the structure being loaded and the mechanism of pain within that structure.
Why Neck Pain May Not Start Immediately After Lying Down but Appears After Sleep
Many patients do not feel pain immediately when they lie down. They may fall asleep normally but wake up during the night or in the morning with pain, stiffness, or headache.
This pattern is important because it suggests that time and sustained loading are involved.
Several mechanisms can explain this delayed pain pattern:
- Prolonged static positioning reduces normal movement. Muscles, joints, and fascia are not designed to remain under the same load for many hours.
- Reduced local circulation may occur in compressed or overloaded areas. This can increase sensitivity in muscles, tendons, ligaments, or joint capsules.
- Protective muscle spasm may develop during sleep. If the nervous system detects irritation in a joint, disc, nerve, or ligament, surrounding muscles may tighten.
- Nerve sensitivity may increase after hours of compression, stretch, or reduced movement.
- Poor sleep increases pain sensitivity, while pain disrupts sleep. This creates a cycle in which neck pain and poor sleep reinforce each other.
This is why some patients wake with:
- morning neck stiffness
- pain at the base of the skull
- headache
- shoulder pain
- arm tingling or numbness
- burning or electric-like pain
- pain that improves only after moving around
Standard Advice for Lying Down and Neck Position
Standard advice for neck pain during lying down usually focuses on keeping the neck in a neutral position. This means that the head should not be pushed too far forward, dropped backward, bent to one side, or rotated for several hours.
In general, sleeping on the back or side is better tolerated than sleeping on the stomach. Stomach sleeping often forces the neck into prolonged rotation, which may aggravate joints, muscles, nerves, and ligaments.
For back sleeping, the pillow should:
- support the natural curve of the neck
- avoid pushing the head too far forward
- avoid allowing the head to drop backward
- reduce focal pressure under the back of the head
- keep the upper neck relaxed
If the pillow is too high, the neck may remain in flexion. If it is too low, the head may fall backward and increase upper-cervical extension.
For side sleeping, the pillow should:
- fill the space between the shoulder and the head
- prevent the neck from bending downward
- prevent the neck from bending upward
- reduce pressure on the lower shoulder
- avoid excessive rotation of the head
If the pillow is too low, the neck bends toward the mattress. If it is too high, the neck bends away from the mattress. Both situations can increase mechanical stress in the cervical spine.
The mattress also matters indirectly. A very soft mattress may allow the shoulder or upper back to sink too much, changing the position of the neck. A very firm mattress may increase pressure on the shoulder or occipital region.
These principles are useful as a starting point. However, they are not enough for every patient. Standard advice assumes that all neck pain behaves similarly, but clinical practice shows that this is not true.
Standard advice about a neutral neck position must also be interpreted carefully in patients with loss of cervical lordosis, cervical kyphosis, forward head posture, or cervical instability. In these patients, the neck may not tolerate the same pillow height or cervical curve support that works for a person with normal alignment. The goal is not to force the neck into an ideal shape, but to find a supported position that reduces pain and avoids end-range flexion, extension, rotation, or focal segmental stress.
When Standard Sleep Advice Must Be Modified According to the Type of Neck Pain
Standard sleep advice must be modified when neck pain is not caused by a general posture problem, but by a specific pain generator.
A position that seems neutral in general may still overload the wrong structure in a particular patient — which is why some patients feel worse despite following standard advice. The goal is therefore not to force every patient into the same correct position, but to modify sleep advice according to the actual pain generator.
Sleep advice should change according to the dominant pain pattern:
- In facet joint-related neck pain, excessive extension or rotation may increase pain. Even a pillow that appears to support the neck well may provoke symptoms if it keeps the upper cervical spine too extended or the head turned for a long time.
- In disc-related neck pain or cervical radiculopathy, the important question is whether the position increases arm pain, tingling, numbness, or weakness. The neck may feel comfortable at first, but if the position narrows the nerve-root space or increases neural tension, symptoms may appear during the night.
- In occipital neuralgia or pain in the back of the head, the problem may be pressure on the occipital region, irritation of the occipital nerves, upper-cervical joint dysfunction, or suboccipital muscle tension. In this situation, the pillow must not only support the neck; it must also avoid provoking the painful occipital pathway.
- In myofascial neck pain, the problem may be prolonged strain in the trapezius, levator scapulae, scalene, sternocleidomastoid, or suboccipital muscles. These patients may wake with stiffness, deep aching, or trigger-point pain even if the sleep position looks acceptable from the outside.
- In neck pain with arm numbness during sleep, the source may be outside the cervical spine. It can be irritation of the brachial plexus, thoracic outlet region, ulnar nerve at the elbow, median nerve at the wrist, or other peripheral nerve. Shoulder position, arm position, elbow flexion, wrist compression, brachial plexus tension, or thoracic-outlet-like loading may contribute, even when the neck itself appears to be in a standard supported position.
This means that sleep position should be guided by the type of pain, not only by general rules. A recommended sleeping position is useful only if it reduces load on the patient’s actual pain generator.
Why a Fixed-Shape Pillow Is Not Always the Best Solution for Neck Pain
Many pillows marketed for neck pain have a fixed anatomical shape. Some of them can help by supporting the cervical curve and preventing the head from falling into a poor position. However, a fixed-shape pillow is not always the best solution for every patient. This does not mean that fixed-shape pillows are wrong. It means that their effect depends on whether their shape matches the patient’s pain generator, cervical alignment, shoulder anatomy, mattress, and sleep position.
A pillow that feels comfortable during a short test may become painful after several hours. This happens because sleep is not static in a simple way. The head, neck, shoulders, and upper back change position during the night.
The pillow must support the neck, but it must also allow enough adaptation to avoid:
- prolonged pressure
- forced alignment
- excessive extension
- excessive flexion
- side bending
- occipital pressure
- shoulder compression
Some patients need firmer and more stable support. Others need a pillow that can be adjusted, compressed, reshaped, or modified depending on which position reduces pain.
The important issue is not whether a pillow is called:
- orthopedic
- anatomical
- memory foam
- cervical
- soft
- firm
The real question is:
Does this pillow unload the specific pain generator?
For one patient, the goal may be to reduce cervical extension.
For another, it may be to avoid pressure over the occipital nerves.
For another, it may be to prevent side bending during side sleeping.
For another, it may be to reduce shoulder compression and arm numbness.
This is why a pillow should not force every neck into one universal “correct” shape. In patients with persistent or position-dependent neck pain, the pillow must help reduce load on the painful structure.
Sometimes the patient becomes aware of the best support only after observing symptoms over several nights. In other cases, this becomes clearer after analysis of the pain pattern, imaging, sleep position, and clinical testing during specialist consultation.
Anatomical Structures Affected by Lying Down and Sleep Position
Several anatomical structures can become painful during lying down. The same symptom — neck pain in bed — may come from different sources. In many patients, more than one structure is involved at the same time, which is why treating only one pain generator often leads to incomplete relief.
Important pain generators include:
- Cervical facet joints
These small joints at the back of the cervical spine can become painful when the neck is kept in extension, rotation, or side bending. Facet-related pain may remain local or refer toward the shoulder blade, upper back, or back of the head. - Intervertebral discs
Discs can contribute to pain when certain neck positions increase pressure inside the disc or change the relationship between the disc and nearby nerve roots. - Cervical nerve roots
Nerve roots may be irritated by foraminal narrowing, disc herniation, inflammation, or positional narrowing. Symptoms may include pain, tingling, numbness, or weakness in the shoulder, arm, or hand. - Occipital nerves
These nerves can be irritated by pressure, muscle tension, fascial compression, or upper-cervical dysfunction. Pain may be felt in the back of the head, scalp, behind the ear, or sometimes behind the eye. - Deep cervical ligaments and joint capsules
These structures may produce pain when stretched or compressed during prolonged positioning. - Suboccipital muscles, trapezius, levator scapulae, scalene muscles, and sternocleidomastoid muscles
These muscles may develop spasm, trigger points, or local inflammation. They can refer pain to the head, shoulder, upper back, or arm. - Shoulder and brachial plexus region
During side sleeping, pressure on the shoulder or tension across the neck-shoulder region may contribute to arm numbness, tingling, or pain that is mistakenly attributed only to the cervical spine. - Cervical alignment and segmental stability
Loss of lordosis, cervical kyphosis, degenerative spondylolisthesis, retrolisthesis, or segmental instability can change how load is distributed during lying down. In these patients, a pillow or sleep position may provoke pain by stressing one cervical level, increasing muscle guarding, or narrowing the space around sensitive neural structures.
How Lying Down Loads Cervical Tissues
Lying down creates several types of load on cervical tissues.
- Sustained flexion occurs when the pillow pushes the head forward. This can increase strain in the posterior neck and may aggravate disc-related or muscle-related pain in some patients.
- Sustained extension occurs when the head drops backward or when the pillow supports the head poorly. This can increase compression in upper cervical joints and may aggravate facet-related or occipital pain.
- Rotation occurs most often during stomach sleeping, but it can also occur when the head turns to one side on the pillow. Prolonged rotation may irritate facet joints, muscles, ligaments, and nerve structures.
- Side bending occurs when the pillow is too high or too low during side sleeping. This may overload one side of the neck and stretch or compress muscles and nerves.
- Direct pressure occurs when the occipital region, ear, jaw, shoulder, or side of the neck is compressed against the pillow or mattress. In sensitized patients, this can provoke local pain, headache, neuralgia, or numbness.
- Reduced movement is also important. During sleep, normal movement is limited. If the neck remains in a painful position for several hours, the tissue response may be much stronger than during a short examination.
These mechanisms may coexist. A patient may have facet irritation, muscle spasm, and occipital nerve sensitivity at the same time. In that situation, changing only one element may not be enough.
Neck Pain When Sleeping on the Back
Sleeping on the back is often recommended for neck pain because it avoids prolonged rotation. However, it is not automatically the best position for every patient.
When sleeping on the back, the main issue is the relationship between the:
- head
- neck
- pillow
- upper back
- occipital region
If the pillow is too high, the head is pushed forward and the neck remains in flexion. This may increase strain in posterior muscles and ligaments and may contribute to morning stiffness.
If the pillow is too low, the head may fall backward. This can increase extension in the upper cervical spine and may aggravate facet joints, suboccipital muscles, or occipital nerve-related pain.
Some patients need support under the neck rather than under the head. Others need less pressure under the occipital region. In occipital pain, even a pillow that seems anatomically correct may provoke symptoms if it creates focal pressure at the back of the head.
Back sleeping may be useful, but it must be adjusted according to symptoms. The patient should observe whether this position produces:
- local neck pain
- pain in the back of the head
- headache
- shoulder symptoms
- arm tingling or numbness
Neck Pain When Sleeping on the Side
Side sleeping can be comfortable for many patients, but it can also provoke neck pain if the pillow height does not match the shoulder width, mattress firmness, and head position.
If the pillow is too low, the head falls downward and the neck bends toward the mattress. If the pillow is too high, the head is pushed upward and the neck bends away from the mattress. Both situations create side bending that may overload cervical joints, muscles, ligaments, and nerves.
Side sleeping can also affect the shoulder. Pressure on the lower shoulder may irritate shoulder structures or increase tension in the brachial plexus region.
Arm position is also important. Symptoms may worsen if the patient sleeps:
- with the arm under the head
- with the arm under the pillow
- with the shoulder compressed
- with the elbow sharply flexed
- with the wrist bent
- with the neck and shoulder pulled in opposite directions
Side sleeping is not wrong, but it must be individualized. The best side-sleeping position is the one that keeps the neck close to neutral while also avoiding shoulder compression and nerve tension.
Neck Pain When Sleeping on the Stomach
Sleeping on the stomach is often the most problematic position for neck pain. The reason is simple: the head must be turned to one side in order to breathe. This keeps the cervical spine in rotation for a long time.
Prolonged rotation can irritate:
- cervical facet joints
- deep cervical ligaments
- suboccipital muscles
- trapezius and scalene muscles
- occipital nerves
- cervical nerve roots
If the head is also extended or supported by a high pillow, the mechanical load becomes even greater.
Stomach sleeping may be especially problematic for patients with:
- facet-related neck pain
- occipital pain
- myofascial pain
- cervical radiculopathy
- morning neck stiffness
- headache after sleep
Some patients cannot immediately stop sleeping on the stomach. In that case, gradual modification is often more realistic than a sudden change. The goal is to reduce the degree of neck rotation, avoid excessive extension, and transition toward side or back sleeping if possible.
Pain in the Back of the Head When Lying Down
Pain in the back of the head when lying down may come from several different mechanisms. It is often described as:
- pressure
- burning
- stabbing pain
- electric-like pain
- deep aching
- pain at the base of the skull
- pain spreading toward the scalp or behind the eye
One possible source is irritation of the occipital nerves. These nerves pass through muscles and fascia at the back of the upper neck and scalp. Direct pressure from the pillow, sustained muscle tension, or upper-cervical mechanical stress may provoke symptoms.
Another possible source is the C2–C3 region or upper cervical facet joints. These structures can refer pain toward the back of the head and may be sensitive to extension, rotation, or certain head positions.
Suboccipital muscles can also generate pain. If these muscles remain contracted during sleep, the patient may wake with tightness at the base of the skull, headache, or pain radiating upward.
This type of pain should not automatically be labeled as migraine, tension headache, or “bad pillow pain.” The location, triggers, tenderness, response to pressure, relation to neck movement, and associated symptoms must be analyzed.
Neck Pain With Arm Pain, Tingling or Numbness During Sleep
Neck pain with arm symptoms during sleep is a common and important pattern. Patients may wake with pain radiating into the:
- shoulder
- upper arm
- forearm
- hand
- fingers
Others notice:
- tingling
- numbness
- burning
- weakness
- a “dead arm” feeling
- symptoms that improve after changing position
Cervical radiculopathy is one possible cause. In that situation, a cervical nerve root is irritated or compressed, and certain neck positions may increase symptoms. The pain may follow a nerve-root distribution and may be associated with numbness or weakness.
However, not all arm symptoms during sleep come from the cervical spine.
Other possible mechanisms include:
- shoulder compression during side sleeping
- brachial plexus tension
- thoracic-outlet-like positioning
- sleeping with the arm under the head
- ulnar nerve compression at the elbow
- median nerve compression at the wrist
- combined cervical and peripheral nerve irritation
Symptoms that improve immediately after moving the arm may suggest positional compression. Symptoms that change with neck movement may suggest a cervical component.
A careful analysis is needed before assuming that the MRI finding in the neck is the only explanation.
Why MRI May Not Explain Neck Pain That Appears When Lying Down
MRI is very useful when there is suspicion of:
- disc herniation
- nerve-root compression
- spinal stenosis
- tumor
- infection
- instability
- myelopathy
- structural cervical disease
However, MRI does not always explain pain that appears only in certain positions, especially when lying down.
Many patients have:
- disc bulges
- degenerative changes
- spondylosis
- mild foraminal narrowing
- straightening or reversal of cervical lordosis
These findings may be relevant in some cases, but they may also be incidental. At the same time, the true pain generator may be small and difficult to see on routine imaging.
Pain may come from:
- facet joint capsule
- small ligament
- occipital nerve
- suboccipital muscle
- trapezius attachment
- scalene trigger point
- local fascial irritation
- position-dependent nerve compression
These structures may produce significant pain even when MRI does not show a dramatic abnormality.
This does not mean that the pain is psychological. It means that the pain generator may be functional, mechanical, inflammatory, or neurophysiological rather than clearly visible as a large structural lesion.
For this reason, MRI must be interpreted together with the pain pattern. The key question is whether the imaging finding matches:
- symptoms
- triggers
- sleep position
- neurological findings
- movement tests
- pressure-point responses
- arm or head pain distribution
Why General Sleep and Pillow Advice Is Often Insufficient
General advice such as “sleep on your back,” “use a firm pillow,” “keep your neck straight,” or “avoid stomach sleeping” may help when neck pain is mainly caused by simple positional strain. However, persistent neck pain during lying down usually means that a specific structure is being overloaded.
In that situation, the problem is not only whether the pillow is good or bad. The problem is whether the pillow and sleep position reduce load on the dominant pain generator.
A standard recommendation may fail when it does not consider:
- which structure is painful
- whether the pain mechanism is compression, stretch, inflammation, instability, spasm, or nerve sensitization
- whether the patient has loss of lordosis, cervical kyphosis, or segmental instability
- whether symptoms spread to the head, shoulder, arm, or hand
- whether the pain appears immediately or only after several hours
- whether the pillow forces the neck into a position the patient cannot tolerate
For this reason, sleep advice should be treated as a clinical test, not as a universal rule. The goal is not to follow a standard position perfectly, but to find the position that reduces mechanical and neural load in that individual patient.
Even Within the Same Diagnosis, Sleep Position Must Be Individualized
Even patients with the same diagnosis may need different sleep strategies because the mechanism of pain may not be the same.
Two patients with occipital neuralgia may both have pain in the back of the head, but one may be sensitive to direct occipital pressure, while another may be more sensitive to upper-cervical extension or suboccipital muscle tension.
Two patients with cervical radiculopathy may both have arm pain, but one may worsen with neck extension, while another may worsen with side bending, shoulder compression, or arm position during sleep.
Two patients with loss of lordosis or cervical kyphosis may both struggle with pillow support, but one may need gentle support under the neck, while another may worsen when a rigid pillow tries to force the cervical spine into an artificial curve.
This is why the diagnosis alone is not enough. Sleep position must be adjusted according to pain distribution, mechanism, cervical alignment, segmental stability, and response to position changes.
How to Test Whether Sleep Position or Pillow Is Contributing to Pain
Testing a pillow or sleep position should be structured. A short test in a store or a single night of use is often not enough. Neck pain related to lying down may appear only after several hours or after repeated nights of the same mechanical load.
The patient should change only one factor at a time. Changing the pillow, mattress topper, sleep position, and arm position at the same time makes it impossible to know what helped or worsened symptoms.
Useful observations include:
- whether pain appears immediately after lying down or only in the morning
- whether pain wakes the patient during the night
- whether pain is local in the neck or spreads to the head, shoulder, arm, or hand
- whether numbness or tingling appears during sleep
- whether symptoms improve after changing position
- whether the problem occurs only on one side
- whether a lower, higher, softer, firmer, or more adjustable pillow changes symptoms
- whether the same symptoms occur during daytime neck movement
- whether arm position changes the symptoms
- whether pressure on the back of the head provokes pain
A reasonable test usually requires several nights. The goal is not to prove that the pillow is the only cause, but to determine whether sleep position is one of the factors maintaining pain.
If symptoms are severe, progressive, neurological, or associated with warning signs, pillow testing should not delay medical evaluation.
When Neck Pain When Lying Down Requires Medical Evaluation
Most neck pain related to sleep position is mechanical and not dangerous. However, certain symptoms require medical evaluation because they may indicate a more serious condition.
Medical evaluation is important if neck pain is associated with:
- progressive weakness in the arm or hand
- difficulty walking
- loss of coordination
- numbness in both hands
- electric-shock sensations down the spine
- bladder or bowel dysfunction
- fever
- unexplained weight loss
- history of cancer
- recent trauma
- infection risk
- severe constant night pain that does not change with position
- rapidly worsening neurological symptoms
Pain that is rapidly worsening, pain associated with neurological deficit, or pain that does not behave mechanically should not be attributed only to posture, sleep position, or pillow choice.
In these situations, imaging, neurological examination, laboratory tests, or urgent medical assessment may be necessary.
What Effective Treatment Requires
Effective treatment of neck pain when lying down requires more than changing the pillow. The first step is to identify both the dominant pain generator and the mechanical context in which that pain generator becomes overloaded during sleep. Second, the mechanism of pain must be understood. Third, pain contributing factors must be recognized.
The pain generator is the structure that directly produces pain. This may include:
- cervical facet joint
- intervertebral disc
- cervical nerve root
- occipital nerve
- deep cervical ligament
- joint capsule
- suboccipital muscle
- trapezius, scalene, or levator scapulae muscle
- fascia or myofascial trigger point
- shoulder structure
- brachial plexus region
- peripheral nerve
The mechanical context explains why that pain generator becomes overloaded in a certain position. This may include:
- loss of cervical lordosis
- straightened cervical spine
- cervical kyphosis
- forward head posture
- degenerative cervical spondylosis
- segmental instability
- degenerative spondylolisthesis or retrolisthesis
- previous cervical trauma
- previous cervical surgery
- muscle imbalance or poor cervical support
- mismatch between pillow shape, mattress firmness, shoulder width, and cervical alignment
Second, the mechanism of pain must be understood. Pain may come from:
- compression
- stretch
- inflammation
- instability
- muscle spasm
- nerve sensitization
- central pain amplification
- a combination of several mechanisms
Third, contributing factors must be recognized. These may include:
- sleep position
- pillow height and shape
- mattress firmness
- daytime posture
- computer work
- phone use
- reduced physical activity
- stress
- sleep disturbance
- metabolic inflammation
- vitamin deficiencies
- medication effects
- central sensitization
Treatment may include:
- sleep-position modification
- pillow adjustment
- targeted medication
- physical therapy
- ergonomic changes
- treatment of contributing factors
- image-guided diagnostic or therapeutic procedures when indicated
In most patients, the best results come when all three levels are considered together: the pain generator, the mechanical context, and the mechanism that maintains pain during lying down or sleep. Treating only one part of the problem often leads to temporary or incomplete improvement.
Why an Online Consultation Can Help When Neck Pain Appears During Lying Down or Sleep
A focused online medical consultation can help when neck pain persists despite changing pillows, sleep position, mattress, physical therapy, or medication.
The consultation begins with a detailed analysis of the pain pattern:
- where the pain starts
- where it spreads
- when it appears
- what position triggers it
- whether it is worse at night or in the morning
- whether there are symptoms in the back of the head
- whether there are shoulder, arm, or hand symptoms
- whether numbness or tingling appears during sleep
Medical records and MRI or CT findings are reviewed, but imaging is not interpreted in isolation. The key question is whether the imaging findings match the symptoms and mechanical triggers.
During a video consultation, the patient may be guided through:
- specific neck movements
- posture tests
- gentle pressure-point testing
- pain mapping
- symptom comparison between positions
- review of sleep setup and pillow position
The sleep setup can also be discussed, including:
- sleeping position
- pillow height
- pillow shape
- mattress firmness
- arm position
- morning symptoms
- whether pain changes after modifying one element
For many patients with persistent position-dependent neck pain, it can clarify why previous advice failed and what should be changed next. This type of evaluation does not replace emergency care or in-person examination when red flags are present.
The goal of this online consultation is not simply to recommend a pillow. The goal is to identify the true pain generator, understand the mechanism that makes lying down painful, and create a targeted strategy to reduce load on the structure responsible for the pain.
Start Your Online Consultation for Neck Pain When Lying Down
If neck pain persists despite changing pillows, sleep position, mattress, physical therapy, or medication, the next step is not more guesswork. A focused online medical consultation can help clarify whether symptoms are coming from a cervical joint, disc, nerve root, occipital nerve, muscle, unstable segment, or shoulder–brachial plexus region.
The goal is not simply to recommend another pillow. The goal is to connect the pain pattern, sleep position, cervical alignment, MRI or CT findings, movement triggers, and pressure-point responses to identify the most likely pain generator and the most reasonable next step.
- ✔ First, send a short message describing your neck pain and when it appears during lying down or sleep
- ✔ You will receive a reply within 24 hours explaining whether we may be able to help, the consultation cost, and a suggested time
- ✔ Only then, you can send your medical documentation, MRI or CT reports, and relevant images if available
- ✔ The consultation can review your pain pattern, sleep position, pillow setup, imaging findings, and possible pain generators
- ✔ When needed, the video consultation is followed by a written medical report and follow-up questions for up to 10 days
- ✔ Secure payment is available by credit card, PayPal invoice, or bank transfer
Consultation fees usually range from $180–250, depending on the complexity of the case.
Online consultation is most useful when symptoms persist despite standard pillow or sleep-position advice, when MRI findings do not fully explain the pain, or when the source of pain remains unclear.
Online pain consultation for chronic neck pain
Schematic explanation of the video consultation for chronic neck pain
Answers to questions about the process and success of video consultations for chronic neck pain
See the page “Possible Reasons for Poor Pain Treatment Effectiveness of Chronic Neck Pain” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
Treatment of complex cases of chronic neck pain can be analyzed by artificial intelligence (AI)
Frequently Asked Questions About Neck Pain When Lying Down
Why does neck pain appear when lying down or sleeping?
Neck pain when lying down usually appears when a sleeping position increases load on an already sensitive pain generator. The problem is not simply the act of lying down, but the position in which the head, neck, shoulder, or arm is held for several hours. The painful structure may be a cervical facet joint, disc, ligament, deep neck muscle, nerve root, occipital nerve, unstable segment, or shoulder–brachial plexus region. A position that feels comfortable at first may become painful later if it compresses, stretches, rotates, or irritates the affected structure. This is why the same pillow or sleeping position can help one patient and worsen another.
Why can neck pain appear only after several hours of sleep?
Neck pain may not start immediately after lying down because the affected structure can often tolerate a position for a short time. Pain appears later when the same position is maintained for several hours. During sleep, the neck may remain in flexion, extension, rotation, side bending, compression, or constant low-grade tension. Reduced movement and local circulation may also increase tissue sensitivity. This delayed pattern explains why some patients fall asleep without significant pain but wake during the night or in the morning with stiffness, headache, pain at the base of the skull, shoulder pain, or arm tingling. The timing of symptoms is important because it suggests sustained loading, not only the initial sleeping position.
Can a pillow cause neck pain when lying down?
A pillow can contribute to neck pain when it holds the neck in a position that the patient’s pain generator cannot tolerate. A pillow that is too high may push the head forward. A pillow that is too low may allow the head to drop backward. During side sleeping, the wrong pillow height may bend the neck toward or away from the mattress. A firm pillow may also create focal pressure under the back of the head and irritate the occipital region. The pillow is usually not the only cause, but it can expose an already sensitive cervical joint, disc, ligament, muscle, nerve, or unstable segment to prolonged mechanical stress during sleep.
Why can an orthopedic pillow make neck pain worse?
An orthopedic pillow can make neck pain worse if its fixed shape does not match the patient’s pain generator, cervical alignment, shoulder width, mattress firmness, or sleep position. Some pillows force the neck into one curve that may be useful for one patient but poorly tolerated by another. This is especially important in patients with loss of cervical lordosis, cervical kyphosis, cervical instability, occipital pain, or arm symptoms during sleep. A pillow may feel comfortable during a short test but become painful after several hours. The question is not whether the pillow is called orthopedic, anatomical, or cervical. The question is whether it reduces load on the actual painful structure.
What is the best sleeping position for neck pain?
There is no single best sleeping position for every patient with neck pain. Back sleeping and side sleeping are usually better tolerated than stomach sleeping, but the correct position depends on the pain generator and symptom pattern. A patient with facet-joint pain may need to avoid prolonged extension or rotation. A patient with cervical radiculopathy must avoid positions that increase arm pain, tingling, numbness, or weakness. A patient with occipital neuralgia may need to reduce pressure at the back of the head. A patient with shoulder or brachial plexus involvement may need arm-position correction. The best position is the one that reduces load on the structure causing symptoms.
Why does sleeping on the stomach often worsen neck pain?
Sleeping on the stomach often worsens neck pain because the head must remain turned to one side in order to breathe. This keeps the cervical spine in rotation for several hours and often adds extension, especially if the pillow is high or the head is tilted backward. Prolonged rotation and extension may overload cervical facet joints, deep ligaments, suboccipital muscles, trapezius or scalene muscles, occipital nerves, and cervical nerve roots. Stomach sleeping can therefore aggravate morning neck stiffness, pain in the back of the head, headache after sleep, myofascial pain, or cervical radiculopathy. Some patients need gradual modification rather than an abrupt change, but the goal is to reduce prolonged neck rotation.
Why can side sleeping cause neck pain or shoulder pressure?
Side sleeping can cause neck pain when pillow height does not match shoulder width, mattress firmness, and head position. If the pillow is too low, the neck bends toward the mattress. If the pillow is too high, the neck bends away from the mattress. Both positions may overload cervical joints, discs, ligaments, muscles, or nerves. Side sleeping can also increase pressure on the lower shoulder or create tension across the neck–shoulder region. Arm position matters as well. Sleeping with the arm under the head, elbow sharply flexed, wrist bent, or shoulder compressed may contribute to tingling, numbness, or a “dead arm” sensation. Side sleeping is useful only when neck and shoulder load are controlled together.
Why can sleeping on the back still cause neck pain?
Sleeping on the back reduces prolonged neck rotation, but it can still provoke pain if the pillow does not support the neck correctly. A pillow that is too high may push the head forward and keep the neck in flexion. A pillow that is too low may allow the head to drop backward and increase upper-cervical extension. A pillow that is too firm under the back of the head may create focal occipital pressure. Back sleeping may worsen facet-related pain, suboccipital muscle tension, occipital nerve irritation, or morning stiffness if the support is poorly matched. Some patients need more support under the neck, while others need less pressure under the occipital region.
Why do I wake up with neck stiffness in the morning?
Morning neck stiffness often develops when the neck remains for several hours in a position that overloads the affected structure. Depending on the cause, this may involve cervical facet joints, discs, ligaments, deep neck muscles, fascia, or an unstable cervical segment. The same sleep position may relieve pain in one patient and worsen it in another because the sensitive structure is not the same. Stiffness can also reflect protective muscle spasm. If a joint, disc, ligament, nerve, or muscle becomes irritated during sleep, surrounding muscles may tighten to protect the area. This can make the neck feel stiff, heavy, painful, or difficult to move after waking.
Why does pain in the back of the head appear when lying down?
Pain in the back of the head when lying down may come from several sources. Occipital nerves can be irritated by pillow pressure, suboccipital muscle tension, fascial compression, or upper-cervical mechanical stress. Upper cervical facet joints, especially the C2–C3 region, can also refer pain toward the base of the skull, scalp, behind the ear, or sometimes behind the eye. Suboccipital muscles may generate deep aching, tightness, or headache after sleep. This pattern should not automatically be labeled as migraine, tension headache, or simple pillow pain. The location, trigger, tenderness, response to pressure, relation to neck movement, and sleep position must be analyzed to identify the most likely generator.
Can neck pain during sleep cause arm tingling or numbness?
Neck pain during sleep can be associated with arm tingling or numbness when a cervical nerve root is irritated or compressed. Certain neck positions may narrow the nerve-root space, increase neural tension, or provoke inflammation around a sensitive root. Symptoms may spread into the shoulder, upper arm, forearm, hand, or fingers and may be associated with burning, electric-like pain, numbness, weakness, or a “dead arm” feeling. However, arm symptoms during sleep are not always caused by a cervical disc. Shoulder compression, brachial plexus tension, thoracic-outlet-like positioning, elbow flexion, wrist compression, or peripheral nerve irritation may also contribute. The pattern of symptoms is more important than MRI alone.
Can arm numbness during sleep come from something other than a cervical disc?
Yes. Arm numbness during sleep can come from nerve irritation or compression at different levels, not only from a cervical disc. The source may be a cervical nerve root, but it may also involve the brachial plexus near the shoulder, thoracic-outlet region, ulnar nerve at the elbow, median nerve at the wrist, or another peripheral nerve. Sleeping with the arm under the head, shoulder compressed, elbow sharply flexed, or wrist bent can provoke symptoms even if the neck MRI shows only mild changes. The finger pattern matters. Tingling or numbness in different fingers may help distinguish whether the problem is more likely cervical, plexus-related, median-nerve-related, ulnar-nerve-related, or mixed.
Why may MRI not explain neck pain that appears when lying down?
MRI is useful for detecting disc herniation, nerve-root compression, stenosis, tumor, infection, myelopathy, and other structural disease. However, MRI does not always explain neck pain that appears only in certain positions or after several hours of sleep. The active pain generator may be small, functional, inflammatory, or position-dependent. Pain may come from a facet joint capsule, small ligament, occipital nerve, suboccipital muscle, trapezius attachment, scalene trigger point, fascia, or positional nerve irritation. These structures may produce significant pain even when MRI findings are mild or nonspecific. MRI must therefore be interpreted together with pain distribution, sleep triggers, movement response, neurological findings, and pressure-point sensitivity.
How do loss of cervical lordosis or cervical kyphosis affect pillow choice?
Loss of cervical lordosis or cervical kyphosis changes what a neutral neck position means for that patient. A pillow designed to support a normal cervical curve may not be tolerated by someone whose neck is straightened, reversed, rigid, or degenerative. In older patients or patients with degenerative alignment changes, a fixed-shape pillow may force the neck toward a curve that looks correct in theory but increases pain in practice. The goal is not to force the cervical spine into an ideal textbook shape. The goal is to find a supported position that reduces symptoms, avoids end-range flexion or extension, and does not increase focal stress on a sensitive cervical level.
Can cervical instability make neck pain worse in different lying positions?
Cervical instability can make neck pain worse in different lying positions because an unstable segment may allow or provoke abnormal movement during sleep. Some positions may increase mechanical stress at that level, causing local neck pain, muscle spasm, or nerve irritation. The problem is not only pillow height. The important issue is whether the sleep position reduces or increases stress on the unstable cervical segment. A position that appears neutral from the outside may still be poorly tolerated if it allows extra movement, extension, rotation, side bending, or focal stress at the unstable level. In these patients, sleep advice must be individualized according to symptoms, imaging, alignment, and response to position changes.
When does neck pain when lying down need medical evaluation?
Neck pain when lying down needs medical evaluation if it is associated with progressive arm or hand weakness, difficulty walking, loss of coordination, numbness in both hands, electric-shock sensations down the spine, bladder or bowel dysfunction, fever, unexplained weight loss, recent trauma, history of cancer, infection risk, or severe constant night pain that does not change with position. Medical evaluation is also important when symptoms persist despite pillow changes, sleep-position changes, physical therapy, or medication. A focused medical evaluation can connect the pain pattern, sleep position, cervical alignment, imaging findings, movement tests, and pressure-point responses. Without identifying the actual pain generator, pillow and position changes remain guesswork.
Can an online medical consultation help identify why neck pain worsens during sleep?
An online medical consultation can help when neck pain persists despite changing pillows, sleep position, mattress, physical therapy, or medication. The goal is not simply to recommend another pillow, but to identify the most likely pain generator and the mechanism that makes lying down painful. During consultation, the pain pattern, sleep position, pillow setup, cervical alignment, MRI or CT findings, movement triggers, pressure-point responses, and symptoms in the back of the head, shoulder, arm, or hand can be reviewed together. This type of evaluation may clarify why standard advice failed and what should be modified next. It does not replace emergency care or in-person examination when red flags are present.