Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Persistent Nerve Pain After Shingles
Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 07, 2026
Who this page is for
This page is for patients with postherpetic neuralgia (PHN) who continue to have persistent pain despite multiple treatments or medications.
Pain often persists because only the nerve pain is treated, while the additional contributors — muscle spasm, trigger points, or low-grade inflammation — remain undetected. Effective treatment requires addressing both the sensitized nerve and these peripheral irritators. A carefully chosen combination of medications, adjusted over 4–8 weeks, usually brings significant improvement. Interventional procedures are used only when necessary.
If you need a structured plan and medication guidance, you can request a telehealth pain consultation.
If you are unsure whether an online consultation can help after all previous tests and treatment, read why this consultation is different.
When patients usually seek a second opinion for postherpetic neuralgia
- Burning, stabbing, or electric pain persists months after shingles
- Pain returns or worsens after temporary improvement
- The pain is thought to come from the heart, lungs, or another internal organ — but tests are normal
- The diagnosis or pain mechanism feels unclear
- You are considering stronger medications, injections, or other procedures
If this reflects your situation, a focused telehealth review can clarify the dominant pain mechanisms, treatment options, and what is and is not indicated in your case: Request Consultation
AUDIO: Learn why postherpetic neuralgia pain persists despite treatment.
AUDIO: Learn about the effective treatment strategy for persistent postherpetic pain.
Postherpetic Neuralgia — Quick Summary (Read This First)
- Postherpetic neuralgia is persistent nerve pain that continues or returns after shingles. The pain usually remains in the same skin region where the shingles rash occurred and is commonly defined as pain lasting three months or more after the rash has healed.
- The pain is usually burning, stabbing, electric, itching, numb, or extremely touch-sensitive. Even light clothing, bedsheets, a breeze, gentle touch, movement, or stress can trigger pain because the affected nerve and skin region remain hypersensitive.
- Postherpetic neuralgia can affect different body regions depending on which nerve was involved. It may appear as band-like chest or abdominal pain after thoracic shingles, facial pain after trigeminal involvement, or pain in the buttock, leg, or other dermatomal regions.
- The condition develops after varicella-zoster virus injures a sensory nerve or ganglion. After shingles, the rash may heal, but the affected nerve can continue sending abnormal pain signals because of peripheral nerve injury, dorsal root ganglion irritation, and central sensitization.
- Postherpetic neuralgia is diagnosed mainly from the clinical picture. A history of shingles in the same dermatome followed by persistent neuropathic pain is usually enough for diagnosis, while atypical, recurrent, or no-rash cases may require targeted testing for varicella-zoster virus activity.
- Postherpetic neuralgia can sometimes occur without a visible shingles rash. This is called zoster sine herpete, and it should be considered when one-sided burning, stabbing, or touch-sensitive pain follows a clear nerve distribution even though the skin looks normal.
- Antiviral treatment is useful mainly during acute shingles or early suspected reactivation. Antivirals such as acyclovir, valacyclovir, or famciclovir help most when started early, but they usually do not treat established postherpetic neuralgia once active viral replication has stopped.
- First-line treatment focuses on calming the sensitized nerve. Gabapentin, pregabalin, tricyclic antidepressants, topical lidocaine, and selected topical or systemic treatments are commonly used, often in carefully adjusted combinations rather than as one fixed medication.
- Postherpetic neuralgia treatment failure often means that only the nerve pain was treated while other pain-maintaining factors were missed. Muscle spasm, trigger points, local inflammation, skin hypersensitivity, sleep disturbance, metabolic factors, nutritional deficiencies, and central sensitization can all maintain pain after shingles.
- When postherpetic neuralgia persists, the next step is reassessment rather than simply repeating the same medication. The goal is to identify whether pain is driven mainly by nerve injury, local tissue irritation, allodynia, central sensitization, recurrent viral activity, or several mechanisms acting together.
- Nerve blocks, sympathetic blocks, botulinum toxin, pulsed radiofrequency, and neuromodulation are used only in selected cases of postherpetic neuralgia. These options may help when pain is focal, severe, resistant to medication, or associated with marked allodynia, but they should be chosen according to the exact pain location and mechanism.
- The prognosis of postherpetic neuralgia depends on age, pain severity, location, immune status, comorbidities, and how long symptoms have persisted. Many patients improve gradually over months, but older patients or those with severe long-lasting pain may require a structured multimodal plan for sustained pain control.
- A second opinion is especially useful when pain in PHN persists despite several medications, when the pain is mistaken for heart, lung, breast, abdominal, dental, or spinal disease, or when procedures are being considered. A structured review can clarify whether symptoms are due to postherpetic neuralgia alone, recurrent zoster, zoster sine herpete, local irritators, or another overlapping pain condition.
- Online consultation may still help when treatment has failed: read why this consultation is different.
Contents
- What is postherpetic neuralgia?
- Why PHN happens (Pathophysiology)
- Symptoms of PHN (shingles nerve pain)
- How PHN Is Diagnosed
- Treatment for postherpetic neuralgia
- Patient Summary
- Prognosis and Recovery in PHN
- Other Viral Causes of Focal Neuralgia (HSV-1 / HSV-2)
- Why pain persists despite treatment
- Treatment of Contributing Factors
- Telehealth: Managing PHN Remotely
- FAQ — Postherpetic Neuralgia
- Additional Patient Resources
What is postherpetic neuralgia?
Postherpetic neuralgia (PHN) is a type of nerve-related (neuropathic) pain that continues or returns in the same area of skin (dermatome) where a shingles (herpes zoster) rash occurred. It is usually defined as pain lasting three months or more after the rash has healed.
The condition develops when the varicella-zoster virus (VZV) becomes active again inside the sensory ganglia of a spinal or cranial nerve root (inside spinal canal), causing long-term irritation and injury of the affected nerve.
Depending on which nerve is involved, this pain can appear in the chest (intercostal neuralgia), face (trigeminal neuralgia), or lower body (sciatic distribution).

Image: Skin changes in herpes zoster
Why PHN happens (pathophysiology)
After the first infection in childhood — usually chickenpox (varicella) — the varicella-zoster virus (VZV) does not leave the body. It remains dormant (inactive) inside small clusters of nerve cells called spinal root ganglia (DRG), located near the spinal cord. They give rise to peripheral nerves such as the intercostal nerves and the sciatic nerve. The virus can also remain latent in specific cranial sensory ganglia (e.g., the trigeminal or Gasserian ganglion).
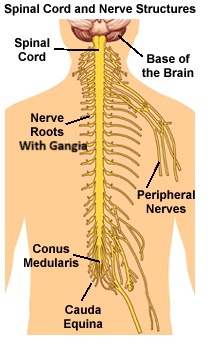
Image: Spinal nerve roots with ganglia. Learn more about nerve anatomy here.
Years or decades later, the virus can reactivate (for example with aging, illness, stress, or weakened immunity). When that happens, it travels along a sensory nerve toward the skin and produces the shingles (herpes zoster) rash. During this phase, the infection and your body’s inflammatory response can cause structural and functional injury to the affected nerves and to their connections within the nervous system. Depending on which nerve is involved, the pain and rash follow that nerve’s dermatome—for example, the trigeminal nerve (face), the intercostal nerves (chest wall or abdomen), the sciatic nerve distribution (buttock/leg), or other involved nerves.
After the skin rash heals, the nerve can stay irritated and keep sending pain signals even when nothing harmful is happening. This ongoing, nerve-related pain is called postherpetic neuralgia (PHN). The nerve becomes over-sensitive, so even small triggers like light touch, clothing, a breeze, or stress can hurt. Doctors call this sensitization. It can occur in the peripheral nerves and also in the brain and spinal cord, which is why the pain can last for months or even years after shingles.
Importantly, PHN is not only the result of leftover nerve injury. In many people, nearby muscles and soft tissues along the same nerve pathway go into spasm, develop tender trigger points, or show low-grade inflammation. These secondary irritators can further aggravate the already sensitive nerve and amplify pain—for example along the intercostal nerves after thoracic shingles, or in the face with trigeminal involvement. Because of this, effective care usually addresses both the nerve-related pain (medications and topical treatments) and these secondary drivers (adequate combination of medications, targeted physical therapy, desensitization, trigger-point treatment, and selected nerve or sympathetic blocks).
Can herpes zoster recur?
Yes. Even after a previous shingles episode, the virus can reactivate in the same or a different nerve — a condition known as recurrent herpes zoster. Each new episode can again cause acute nerve inflammation and sometimes a new phase of PHN in the same or a different area.
Can neuralgia occur without a visible rash? (Zoster sine herpete, ZSH)
Yes — sometimes the virus reactivates without producing any skin eruption. In these cases, the patient experiences burning or stabbing pain in one nerve region (dermatome), but the skin appears normal. This form, called zoster sine herpete, is more difficult to diagnose. When available, laboratory tests can confirm viral activity.
Symptoms of PHN (shingles nerve pain) — with location examples
Pain stays in the same band of skin (dermatome) where the shingles rash was. It may burn, stab, or feel like electric shocks, and it often worsens at night or during certain movements. Touch-sensitivity (allodynia) is common — even light clothing, bedsheets, a breeze, or gentle brushing can hurt. People may also notice hyperalgesia (stronger-than-expected pain from minor triggers), tingling/pins-and-needles, itching, or numb spots in that strip of skin. Pain triggers include stress, some movements, fatigue, temperature change, and friction. Ongoing pain often disrupts sleep, mood, daily activities, and overall quality of life.
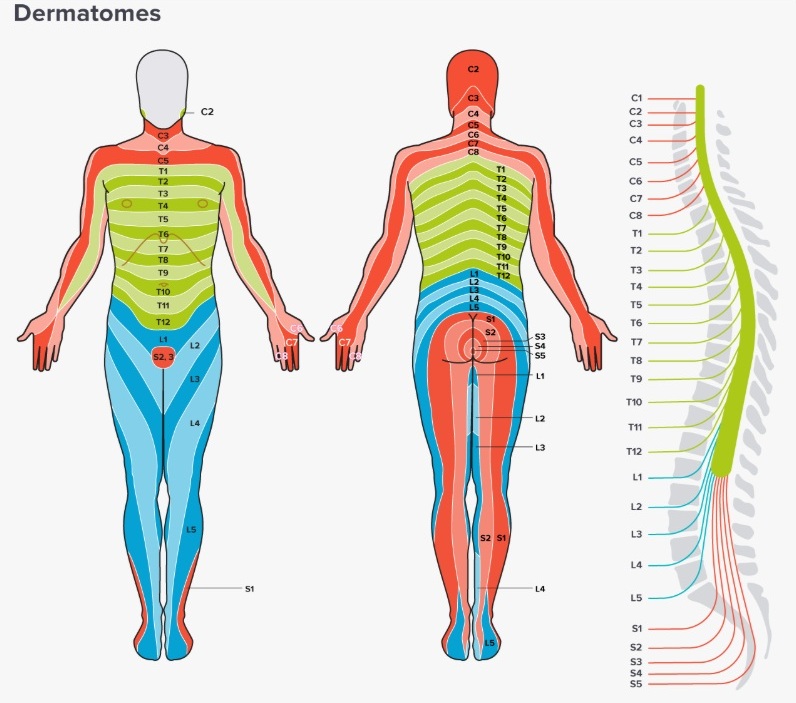
Image: Skin dermatomes
Where it shows up most often (examples + typical frequencies):
- Chest wall or abdomen/ intercostal nerves (thoracic dermatomes): band-like pain wrapping around one side of the chest; clothes, breathing or motion can aggravate it. Thoracic involvement is most common (~50–60% of zoster cases), and thoracic PHN is likewise the most frequent location.
- Face / trigeminal nerve (especially the ophthalmic V1 branch): pain, burning, or shocks on one side of the forehead/eye/upper face. Washing the face, shaving, or wearing glasses can hurt. Trigeminal involvement is ~10–20% of cases overall. You can read about the various forms of primary and secondary headaches on this page.
- Buttock/leg (“sciatic distribution”, lumbosacral dermatomes): pain down the buttock and back of the leg, sometimes with numbness in the foot. Sitting or clothing friction can trigger flares. Lumbosacral involvement is reported around ~10–14%.

Image: different locations of herpes zoster. When these skin changes resolve, pain may persist. Read more about the anatomy of the cranial nerves here.
Early neuralgia without a clear rash (general): Shingles-related nerve pain can begin before the rash appears—or there may be no rash at all (zoster sine herpete- ZSH). The pain usually stays in one nerve’s territory (a dermatome) on one side of the body and is often touch-sensitive (clothing or a light brush hurts). When this pattern occurs, shingles/PHN should be considered even if the skin looks normal.
Example of neuralgia without rash — intercostal nerves (chest wall): The pain may feel like a tight, burning band at the level of one or a few ribs, worse with movement, breathing, or friction from clothes. If zoster/PHN isn’t suspected, people often worry about the breast, heart, liver, or stomach, which can lead to extensive—but unrelated—testing. A unilateral, band-like, touch-sensitive pattern along the ribs should prompt consideration of intercostal neuralgia which can be intercostal zoster/PHN, even without a visible rash.
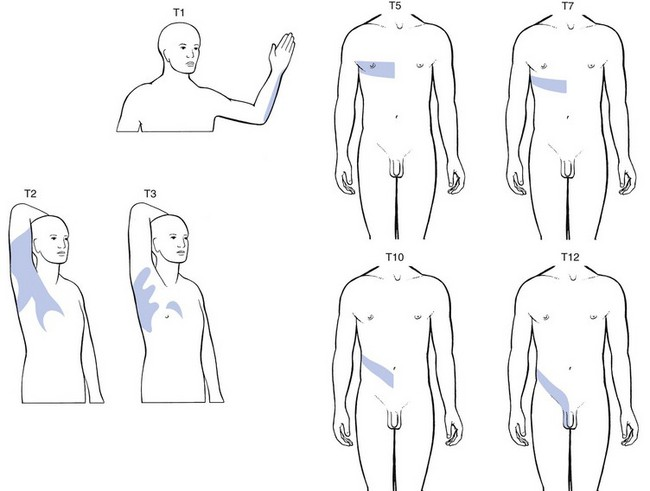
Image: Pain locations with intercostal neuralgia at different levels. If this isn’t suspected, patients may think the pain is coming from the breast, heart, liver, stomach, or other organs — which often leads to extensive testing of those organs.

Image: Intercostal neuralgia mimicking chest pain
How PHN Is Diagnosed
Typical PHN is a clinical diagnosis based on previous shingles in the same dermatome and persistent neuropathic pain. It is important to be examined in person or during a video consultation by a specialist who understands the pain anatomy of this region and knows how to check a large but defined group of possible pain-maintaining mechanisms — often around 15 different nerve, muscle, viral, inflammatory, or sensitization-related factors. Such a specialist will not only diagnose postherpetic neuralgia, but will also determine which ongoing processes are leading to nerve irritation after the infection.
For atypical/recurrent/no-rash cases, confirm Varicella-Zoster Virus (VZV) with labs when possible:
- A test that directly detects the chickenpox/shingles virus in the sample (PCR test for VZV DNA) is the preferred method to confirm varicella/zoster; lesion material (the base of a fresh vesicle or a scab) works best. If there is no lesion, PCR can be tried on other samples (e.g., CSF; sometimes saliva or blood), but these are less sensitive.
- Serology:
- IgM antibodies is not recommended for confirming acute disease due to its poor specificity. A positive IgM test result without a compatible illness is not reliable evidence of an acute infection.
- IgG antibodies indicate that you have had a prior exposure to the virus and have long-term immunity. They are a sign of a past infection, not necessarily a new one. To confirm that your current symptoms are caused by a recent infection, doctors rely on a special test: the four-fold rise in paired IgG. This test requires two blood samples to be drawn from you, usually two to four weeks apart. If the second sample shows a level of IgG that is four times higher than the first, it strongly supports a diagnosis of an active or recent infection.
In suspected zoster sine herpete (dermatomal neuralgia without a rash), clinicians try to document recent VZV reactivation with targeted PCR when a suitable specimen is available, or with a combined approach using PCR plus paired serology. If the clinical picture strongly suggests an acute reactivation (zoster or ZSH) but PCR is negative and serology is inconclusive, a short course of empiric antiviral therapy may be reasonable while tests are repeated or confirmed. However, antivirals are not effective for established PHN when there is no evidence of active viral replication.
Treatment for postherpetic neuralgia
Goals: reduce neuropathic pain and, where present, address ongoing peripheral irritators along the involved nerve (see “secondary drivers” below). Multimodal, stepwise plans are standard. PHN does not have a single mechanism — peripheral nerve injury, sensitization of the dorsal root ganglion, and central sensitization may all contribute. Because of this, no single treatment works for every patient and different approaches may help different individuals.
First-line pharmacologic options (evidence-based):
Gabapentin/pregabalin, tricyclic antidepressants (e.g., amitriptyline/nortriptyline), and topical 5% lidocaine patches. Capsaicin 8% patch is effective in selected patients; opioids/tramadol are reserve options. Combination therapy is common.
Adjunctive Therapy for Residual Local Nerve Irritation
PHN is not solely the result of residual nerve damage. In some patients, myofascial spasm/trigger points and low-grade muscle or soft-tissue inflammation along the same nerve pathway can maintain or amplify pain (e.g., intercostal muscles after thoracic zoster; jaw/face with trigeminal involvement). Therapy should begin with evidence-based neuropathic treatments (such as gabapentin/pregabalin, TCAs, or topical lidocaine; 8% capsaicin may also be considered). It is essential to screen for myofascial or other local contributors during this initial phase. Supporting measures include physical therapy, desensitization techniques, and specific home strategies. Where appropriate, a short, closely monitored trial of an anti-inflammatory medication (NSAID) or a muscle relaxant can be added. Adequate combination of all these medications is essential, as well as their reassessment and dose adjustments, which are performed throughout the 4- to 8-week period. If pain remains focal (localized) and refractory (unresponsive to initial therapy), treatment is escalated. This escalation may involve considering short-term corticosteroids and focused local treatments. Local treatments include specialized procedures such as trigger-point injections or selected nerve/sympathetic blocks, all while the neuropathic regimen is continued. This dual-track approach treats both the sensitized nerve and the additional pain generators — inflammatory and muscular factors — maintaining the pain.
Treating Zoster Itself (acute/recurrent):
When an acute Shingles rash (Zoster) is present—or strongly suspected in the early stages—oral antivirals (like acyclovir, valacyclovir, or famciclovir) should be started ideally within 72 hours (benefit for preventing PHN beyond 72 hours is limited). Starting this medication quickly can help shorten the acute pain and is known to reduce the risk of developing long-term Postherpetic Neuralgia (PHN). This rapid treatment strategy is also beneficial in specific, related conditions where the nerve is affected but the typical rash is not visible (Zoster sine herpete, or ZSH). Early treatment in these cases has been linked to better overall outcomes, particularly in conditions like acute facial paralysis caused by the virus. Antiviral therapy (acyclovir, valacyclovir, famciclovir) rarely affects outcomes more than 7–10 days after the onset of the rash—or the onset of nerve pain in Zoster sine herpete cases. This is because viral replication has already stopped, and the remaining pain stems from nerve damage, not active infection.
Interventional Options for Refractory Cases: Nerve and Sympathetic Blocks
Previous medication failure does not always mean medication cannot help; in many persistent cases, the problem is that the right combination of mechanisms was not treated together. In most cases, you don’t need a special intervention to reduce pain. When medications and topical treatments don’t fully relieve the pain, specialized injections—called nerve blocks—can be used to calm the irritated nerve pathway directly:
- Peripheral nerve blocks — injections near the irritated nerve (e.g., intercostal or paravertebral blocks for chest-wall pain, or trigeminal branch blocks for facial pain).
- Sympathetic blocks — injections that calm the autonomic nervous system when pain includes signs like cold skin, color change, or burning sensitivity (stellate ganglion block for facial/arm pain; thoracic sympathetic block for chest/trunk).
- Epidural injection — anesthetic ± steroid placed near the affected spinal level to reduce inflammation and pain transmission.
- Botulinum toxin injections (intradermal, in the affected dermatomal area) have shown benefit in some PHN patients, especially when allodynia is present. These are not muscle injections, but very superficial injections targeting the sensitized skin nerves.
These procedures are used selectively for focal, resistant pain, often together with medications and treatment of local tissue-related factors such as muscle spasm, inflammation, and trigger points. Many other interventional options exist, but no single technique is universally accepted as superior. Centers may offer different options depending on expertise. In many pain centers, these procedures are part of a broader treatment protocol — a structured sequence that combines medication optimization, physical or postural therapy, and targeted interventions. Within such protocols, results are often better, because all potential pain generators are systematically identified and treated rather than focusing only on the nerve.
Interventional Options for PHN (RF & Neuromodulation)
Used rarely and only in selected, refractory cases.
Pulsed Radiofrequency (PRF) Treatment — This is a modern technique that uses short, controlled electrical pulses to gently warm the nerve to a low temperature (typically around 42°C / 108°F). Unlike older thermal radiofrequency procedures that intentionally heat the nerve to destroy it, PRF keeps the temperature low enough to avoid permanent nerve injury. The goal is to calm and normalize the nerve’s electrical activity. PRF is commonly performed near the dorsal root ganglion (DRG) — the control center of that nerve segment — especially for highly localized pain in the chest (intercostal nerves), head, or limbs.
Thermal RF (neurotomy). Less common due to risk of neuritis/worsened dysesthesia. It is reserved for carefully selected focal neuralgias when PRF fails.
Spinal cord stimulation (SCS). Option for refractory PHN after meds/topicals and blocks. Today, dorsal root ganglion (DRG) stimulation is used more frequently in patients with PHN.
Dorsal Root Ganglion Stimulation (DRG-S). This is a highly advanced neuromodulation technique that targets the Dorsal Root Ganglion (DRG)—the specific control center for the painful nerve. Usually about 3% of patients with resistant PHN require this level of intervention. This allows for much greater precision than older stimulation methods (spinal cord stimulation) and fewer unwanted paresthesia side effects. This focused approach is reserved for patients with severe, chronic, and highly localized pain (focal pain) who have not responded to earlier treatments. It often focuses on one to three affected ganglia. Before the final, permanent implantation, a temporary trial period (usually lasting several days) is performed using temporary leads. This trial period is essential to confirm that the stimulation provides adequate pain relief and to ensure complete patient satisfaction with the stimulation effects.
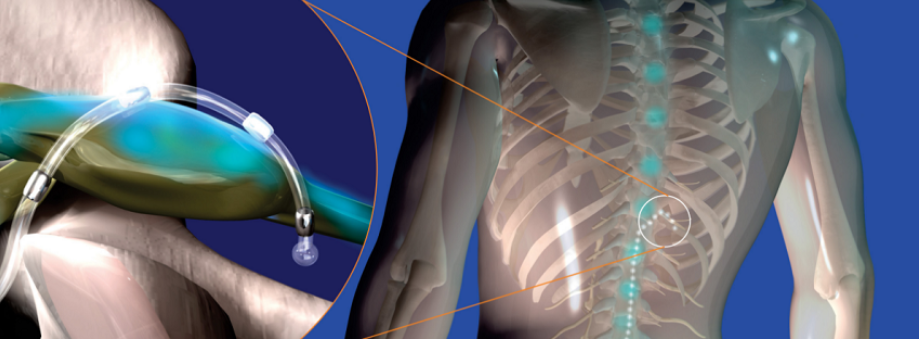
Image: A micro-lead wire for stimulation is positioned around the Dorsal Root Ganglion (DRG), which is the specific control center for the painful nerve. This wire connects to a small electrical device with a battery (the pulse generator), which is implanted under the skin, usually on the side of the abdomen or the upper trunk.
Before contacting us, please read our Privacy Policy and Terms of Use.
Online pain consultation in detail for postherpetic neuralgia
Schematic explanation of the video consultation in PHN
Answers to questions about the process and success of video consultations for PHN
See the page “Possible Reasons for Poor Pain Treatment Effectiveness in PHN ” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
Why Postherpetic Neuralgia Pain May Persist Despite Treatment
In many patients, postherpetic neuralgia persists even after appropriate treatment with medications, topical therapies, or nerve blocks. In addition, failure to determine which anatomical structure is primarily responsible for the pain, what pathological process is occurring within that structure, and which contributing factors are maintaining the pain is a key reason why symptoms persist despite treatment. This usually does not mean that the condition is untreatable, but rather that the pain mechanism has not been fully addressed.
PHN is not driven by a single process. While the initial trigger is nerve injury caused by the virus, ongoing pain often reflects a combination of persistent nerve sensitization and additional factors that continue to amplify pain signals.
A common reason for incomplete improvement is that treatment focuses only on suppressing nerve pain, without identifying what is maintaining that sensitivity over time. In other cases, the dominant pain mechanism may be misinterpreted — for example, when central sensitization or local tissue factors play a larger role than expected.
As a result, patients may receive multiple treatments that provide temporary or partial relief, but do not lead to stable improvement.
A structured reassessment of the pain mechanisms is often the key step in determining why previous treatments were not effective and what needs to be addressed next.
Pain Contributing Factors in Postherpetic Neuralgia
Effective treatment of postherpetic neuralgia (PHN) begins with identifying the primary mechanism of pain — persistent nerve damage and altered nerve signaling following herpes zoster infection.
However, in many patients, pain persists not only because of the initial viral nerve injury, but because additional contributing factors are not recognized or adequately addressed. These factors rarely represent the main cause of pain, but they can maintain nerve hypersensitivity, increase pain intensity, delay recovery, and reduce the effectiveness of otherwise appropriate treatment.
For that reason, successful management requires not only targeting the damaged nerve, but also understanding the broader neurological and systemic context in which pain persists.
What contributing factors may play a role in postherpetic neuralgia?
- Central sensitization — the nervous system may amplify pain signals over time, so that even mild stimuli produce significant discomfort
- Sleep disturbance and pain cycle — poor sleep increases pain perception and reduces the nervous system’s ability to regulate pain
- Stress and increased nervous system reactivity — stress does not cause the pain, but increases sensitivity and helps maintain symptoms
- Metabolic factors, pro-inflammatory state and low-grade inflammation — obesity, insulin resistance, and chronic inflammation increase nerve sensitivity and impair recovery
- Nutritional deficiencies — low levels of vitamin B12, vitamin D, magnesium, or iron may contribute to impaired nerve function and slower healing
- Vitamin-related factors — both deficiency and excess of vitamin B6 may contribute to burning sensations, tingling, or hypersensitivity
- Medications and previous treatments — long-term or inappropriate use of certain medications may alter pain perception without addressing the underlying mechanism
- Other medical conditions and comorbidities — diabetes, immune dysfunction, thyroid disorders, and chronic inflammatory diseases may increase nerve vulnerability and prolong symptoms
- Physical inactivity and deconditioning — reduced activity due to pain may increase overall sensitivity and decrease pain tolerance over time
Why this matters in practice
In many cases, treatment fails because therapy focuses only on suppressing pain (for example with medications), without addressing the mechanisms that maintain nerve hypersensitivity and central sensitization. Conversely, even when the primary nerve damage is recognized, failure to address contributing factors often leads to only partial or temporary improvement.
The most effective approach combines treatment of neuropathic pain with identification and correction of contributing factors that maintain pain sensitivity. An incomplete approach — even when it includes individually effective methods — is one of the most common reasons why postherpetic neuralgia becomes persistent.
In practice, many patients try to address parts of this problem on their own — through topical treatments, supplements, or different medications. While these approaches may provide partial relief, they rarely lead to lasting improvement if the full mechanism of pain is not clearly understood and treated.
Many patients recognize that they have already tried one part of this approach — but not the complete strategy. This is one of the most common reasons why postherpetic neuralgia becomes chronic.
Prognosis and Recovery in PHN
How long until it’s called PHN?
Most guidelines define PHN as pain that lasts ≥90 days after the shingles rash began (or healed).
How often does pain persist? (varies by age and study)
- About 10–20% of people with shingles report ongoing pain at 3 months; in some datasets it’s nearer ~5% overall, but higher with older age.
- By 12 months after shingles onset, only about 3–8% of all patients still report pain
- Severity declines over time; e.g., an Icelandic cohort found severe pain in those >60 yr was 6% at 1 month and 4% at 3 months, while no one <50 yr reported severe pain.
- In older adults with long-lasting PHN, pain can be prolonged: one study (>65 yr) reported mean duration ~3.3 years (range 3 months to >10 years).
Who is at higher risk of prolonged PHN?
Older age; more severe acute rash/pain and prodromal pain; ophthalmic (trigeminal) involvement; and immunosuppression are consistent risks. In addition, several studies/meta-analyses link diabetes and other comorbidities (e.g., COPD, hypertension) with higher PHN risk; and some sources note risk in conditions requiring immunosuppressive therapy (e.g., certain autoimmune diseases). An underlying peripheral polyneuropathy has also been proposed as a co-factor in persistent pain.
Preventive vaccination against herpes zoster — recommended for adults aged 50 and older — significantly reduces the risk of shingles and therefore lowers the chance of developing postherpetic neuralgia. It is especially advised for individuals with weakened immunity, chronic medical conditions, high stress levels, or those who have already had a herpes zoster episode.
What to Expect with Treatment (Patient Summary)
Most people improve over months with evidence-based nerve-pain therapy (gabapentin/pregabalin, TCAs, topical 5% lidocaine cream or patch; 8% capsaicin for some). Using combination therapy, careful dose titration, and treating nearby local tissue irritators (e.g., myofascial spasm, compression, inflammation, trigger points) often reduces pain and allodynia. Antivirals help acute shingles if started early but do not treat established PHN. If pain lasts 3 months after shingles, it meets criteria for PHN. Many patients improve gradually; a smaller group—especially older adults—may have pain for a year or longer, and a minority for several years.
Other Viral Causes of Focal Neuralgia (HSV-1 / HSV-2)
Although postherpetic neuralgia is caused by Varicella-Zoster (Shingles), herpes simplex viruses — HSV-1 (oral) and HSV-2 (genital) — can also produce focal neuralgia. The rash, when present, appears as small grouped blisters on reddened skin or mucosa, but nerve pain may also occur without visible lesions when the virus irritates a sensory ganglion. HSV-1 most often affects branches of the trigeminal nerve and can mimic trigeminal neuralgia or irritation of one of its branches (burning, electric facial pain). HSV-2 tends to reactivate in the sacral ganglia (S2–S4) and may cause pelvic or pudendal-type neuralgia with localized burning, hypersensitivity, or sharp pain in the genital or perineal region. The pain mechanism is neuropathic, so treatment follows the same principles as postherpetic neuralgia (neuropathic medications, topical agents, and interventional options when needed). However, if symptoms clearly follow recurrent herpes outbreaks or recur in the same dermatome, suppressive antiviral therapy (acyclovir or valacyclovir) may be considered, the same way it is used for preventing herpes recurrences.
Treatment of complex cases of pain in PHN can be analyzed by artificial intelligence (AI)
Why an Online Consultation Can Help When Postherpetic Neuralgia Pain Persists
A video consultation for postherpetic neuralgia can help identify the exact source of your shingles-related nerve pain — one or more pain generators — as well as the factors that trigger and maintain it. This is achieved through a detailed conversation and review of your medical records, previous treatments, and imaging when available. During the session, you are instructed to perform specific skin-sensitivity, movement, posture, or finger-pressure tests to see what increases, reduces, or changes your pain. This helps identify which pain source is active. Many of these pain generators and sustaining factors cannot be seen on MRI or CT.
This may sound like examinations you have already had. It is not — because what matters most is not the test itself, but who interprets it. Only a specialist with deep knowledge of nerve pain anatomy knows which questions to ask, how to map the painful dermatome, where to check for allodynia or hypersensitivity, which movements or pressure points to test, and how to confirm which pain source is active. This is not just another opinion.
You will also receive advice on which additional factors that trigger and sustain pain should be investigated — such as vitamin deficiencies, side effects of other medications, inadequate diet, metabolic disorders, sleep disturbance, low-grade inflammation, physical strain during daily activities or work, skin hypersensitivity, muscle spasm around the painful region, and other overlooked contributors. In many patients who have already visited several specialists, these factors have still not been fully investigated.
Once the main pain mechanism behind postherpetic neuralgia symptoms is identified, treatment follows: a targeted combination of medications covering all identified mechanisms, carefully introduced and adjusted over 6–8 weeks, with regular communication during the treatment period, especially when you need it. The aim is to achieve early pain reduction during the first 10 days, then stabilize the result over the following weeks for a longer-lasting effect. When selecting medications, we take into account whether patients are older or have other health conditions, and we prescribe them in a safe combination for the shortest possible duration to avoid medication overload. All recommendations are explained during the conversation and are also given in a written medical report.
Many patients assume that because medications have already failed, a specific procedure is now needed. In most cases, this is not true — previous medications often did not cover the right combination of mechanisms, were not individualized, or were not adjusted over a sufficient period of time. In the minority of patients where medication alone is not sufficient, we recommend the exact intervention or procedure — such as a targeted nerve block, sympathetic block, pulsed radiofrequency, or neuromodulation option — chosen based on the confirmed pain generator, not assumptions.
Postherpetic Neuralgia (PHN) — Start Your Telehealth Consultation
If you have nerve pain after shingles (or suspected zoster sine herpete) that persists despite treatment, a detailed telehealth consultation can help identify all sources of pain and plan a tailored therapy covering both the neuropathic pain (sensitized nerve) and any peripheral irritators (e.g., muscle spasm/trigger points). In most patients, pain persists because these irritators are not discovered or adequately treated.
- ✔ Send a short message describing your symptoms, location of pain (dermatome), and prior treatments
- ✔ You’ll receive a reply within 24 hours with info on whether and how we can help, including consultation cost and scheduling
- ✔ Only then, you can send medical documentation (reports, prior imaging/labs)
- ✔ The video visit is followed by a written plan and free follow-up questions for 10 days
- ✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Consultation fees typically range from $180–250, depending on case complexity.
Based on our medical report, reimbursement can often be obtained (if your insurance plan allows it).
This reflects the usual international range for specialist telehealth. A session helps clarify whether the pain is due to
PHN alone or also to local irritators, and whether optimized medication, physical therapy/desensitization,
nerve/sympathetic blocks, or (rarely) RF/neuromodulation are appropriate.
FAQ — Postherpetic Neuralgia: Causes, Diagnosis & Treatment
What is postherpetic neuralgia (PHN)?
Postherpetic neuralgia, or PHN, is persistent nerve pain after shingles. It usually remains in the same dermatome, meaning the same strip of skin supplied by the affected nerve where the shingles rash appeared. PHN is commonly defined as pain lasting three months or more after the rash has healed. The pain may feel burning, stabbing, electric, itchy, numb, or hypersensitive to touch. It occurs because the varicella-zoster virus injures sensory nerves and their ganglia. Even after the skin heals, the nerve may remain irritated and over-sensitive, sending pain signals when nothing harmful is happening.
Why does postherpetic neuralgia pain persist after the shingles rash heals?
Postherpetic neuralgia pain may persist because the shingles virus can injure the affected sensory nerve and make it over-reactive. After the rash disappears, the nerve may continue sending abnormal pain signals. This is called sensitization and can occur in peripheral nerves, the dorsal root ganglion, spinal cord, and brain. Light touch, clothing, wind, or stress may then become painful. In many patients, pain is not maintained by nerve injury alone. Nearby muscles and soft tissues along the same nerve pathway may develop spasm, trigger points, or low-grade inflammation. These secondary irritators can amplify the already sensitized nerve and explain why pain continues despite apparently correct treatment.
What does postherpetic neuralgia feel like?
Postherpetic neuralgia may feel like burning, stabbing, electric shocks, itching, tingling, numbness, or deep skin sensitivity after shingles. Many patients describe pain from clothing, bedsheets, a light breeze, or gentle touch. This touch sensitivity is called allodynia. Some patients also have hyperalgesia, meaning that a mildly painful stimulus feels much stronger than expected. The pain usually follows one nerve territory on one side of the body, such as the chest wall, abdomen, face, arm, or leg. The skin may look healed, but the nerve remains irritated and hypersensitive. This is why PHN can continue long after the shingles rash disappears.
I tried several medicines — why do I still have postherpetic neuralgia pain?
Postherpetic neuralgia may persist despite several medicines when treatment focuses only on suppressing nerve pain but does not identify all mechanisms maintaining the pain. Gabapentin, pregabalin, antidepressant-type pain modulators, lidocaine, or capsaicin may reduce nerve sensitivity, but they may not fully help if local irritators remain active. Muscle spasm, trigger points, low-grade inflammation, friction sensitivity, poor sleep, diabetes, nutritional deficiencies, or central sensitization may keep the pain cycle going. In such cases, medication is not necessarily wrong, but incomplete. Treatment often needs careful dose adjustment over several weeks plus targeted management of local and systemic contributors that continue to irritate the sensitized nerve.
Can postherpetic neuralgia happen without a shingles rash?
Yes. Shingles-related nerve pain can sometimes occur without a visible skin rash. This condition is called zoster sine herpete. The patient may feel burning, stabbing, electric, or touch-sensitive pain in one nerve territory, but the skin looks normal. This makes diagnosis more difficult because the pain can be mistaken for heart, lung, abdominal, dental, spinal, or musculoskeletal disease depending on the affected dermatome. When available, doctors may use VZV PCR testing and paired IgG blood tests to support recent varicella-zoster reactivation. If the clinical picture strongly suggests acute reactivation, antiviral therapy may sometimes be started early, but antivirals do not treat established PHN without active viral replication.
How is postherpetic neuralgia diagnosed?
Typical postherpetic neuralgia is usually diagnosed clinically. The key pattern is prior shingles in a specific dermatome followed by persistent neuropathic pain in the same area. The pain may burn, stab, itch, shock, or become very sensitive to touch. In atypical cases, recurrent cases, or suspected zoster sine herpete without rash, laboratory confirmation may be considered. VZV PCR is preferred when a suitable sample exists, especially from fresh vesicles or scabs. If no skin lesion is present, PCR from other samples may be less sensitive. IgM alone is not reliable. Paired IgG testing may help if a four-fold rise supports recent infection.
What is the best treatment for postherpetic neuralgia?
Postherpetic neuralgia treatment usually works best when it is multimodal and adjusted gradually. First-line options include gabapentin or pregabalin, tricyclic antidepressants such as amitriptyline or nortriptyline, topical lidocaine, and selected use of an 8% capsaicin patch. Combination therapy is common because PHN does not have only one mechanism. The plan should also check whether local tissue irritators are maintaining the pain. Physical therapy, desensitization, trigger-point treatment, and carefully monitored short trials of anti-inflammatory medication or muscle relaxants may help selected patients. If pain remains focal and resistant, nerve blocks, sympathetic blocks, botulinum toxin, pulsed radiofrequency, or neuromodulation may be considered.
What is the first-line treatment for postherpetic neuralgia?
First-line treatment for postherpetic neuralgia usually includes medications that reduce nerve excitability and topical treatments that calm the affected skin. Common options include gabapentin, pregabalin, amitriptyline or nortriptyline, and topical lidocaine. An 8% capsaicin patch may be useful in selected patients. The best choice depends on age, other medical conditions, pain intensity, sleep disturbance, drug tolerance, and whether the pain is focal or widespread. Many patients need combination therapy rather than one drug alone. Treatment should be adjusted gradually over several weeks, because too low a dose may not help, while increasing too quickly may cause side effects.
Do antivirals treat postherpetic neuralgia?
Antiviral medication helps acute shingles when started early, ideally within the first 72 hours after rash onset. Acyclovir, valacyclovir, or famciclovir can shorten acute viral activity and may reduce the risk of developing long-term nerve pain. They may also be useful in early suspected zoster sine herpete when active reactivation is strongly suspected. However, antivirals usually do not treat established postherpetic neuralgia once viral replication has stopped. At that stage, the remaining pain is usually driven by nerve injury, sensitization, local tissue irritators, and central pain processing rather than active virus. Treatment then shifts toward neuropathic pain control and correction of contributing factors.
How long does postherpetic neuralgia last?
Postherpetic neuralgia duration varies widely. Many patients improve gradually over months, especially when pain mechanisms are treated early and systematically. PHN is commonly defined as pain that persists for at least 90 days after shingles. A smaller percentage of patients still report pain after one year, and older adults are at higher risk of prolonged symptoms. In some people, especially those with severe initial rash or pain, ophthalmic trigeminal involvement, diabetes, immunosuppression, or other comorbidities, pain may last for years. Long duration does not mean that improvement is impossible, but treatment usually needs a structured approach that addresses both nerve sensitization and contributing factors.
Can postherpetic neuralgia come and go?
Yes. Postherpetic neuralgia can fluctuate. Some patients have constant burning pain, while others have periods of improvement followed by flares. Pain may come and go because the sensitized nerve remains vulnerable and can be reactivated by friction, clothing, cold air, stress, fatigue, poor sleep, inflammation, muscle spasm, or another shingles episode. A flare does not always mean active viral replication. In established PHN, pain often fluctuates because the nervous system remains hypersensitive. When symptoms return after improvement, the active drivers should be reassessed: nerve sensitization, local irritators, systemic contributors, sleep, stress, and whether the medication plan is still adequate.
What aggravates postherpetic neuralgia?
Postherpetic neuralgia may be aggravated by light touch, tight clothing, bedsheets, cold air, heat, friction, movement, poor sleep, stress, fatigue, and local muscle tension. Some patients notice worsening with pressure over the affected dermatome or with movements that stretch the irritated nerve pathway. In thoracic PHN, breathing, twisting, or rubbing from clothing may worsen rib-band pain. In facial PHN, washing the face, shaving, glasses, or wind may trigger pain. These triggers do not mean the pain is psychological. They reflect sensitized skin nerves, dorsal root ganglion irritation, and sometimes local tissue factors that keep the painful area over-reactive.
Who is at higher risk for prolonged postherpetic neuralgia?
The risk of prolonged postherpetic neuralgia is higher in older adults, especially after age 50. Severe acute shingles pain, severe rash, prodromal pain before the rash, and ophthalmic trigeminal involvement are also important risk factors. Immunosuppression increases risk because viral injury and inflammation may be more intense or prolonged. Diabetes and other chronic medical conditions can make nerves more vulnerable and slow recovery. Some patients may also have underlying peripheral polyneuropathy or metabolic factors that amplify nerve sensitivity. Sleep disturbance, stress, inflammatory states, nutritional deficiencies, and reduced activity may not be the primary cause, but they can help maintain pain once PHN has become chronic.
Can postherpetic neuralgia affect the face or trigeminal nerve?
Yes. Postherpetic neuralgia can affect the face when shingles involves the trigeminal nerve, especially the ophthalmic V1 branch around the forehead and eye. Patients may have burning, electric, stabbing, or touch-sensitive pain on one side of the forehead, eye region, cheek, jaw, or scalp, depending on the involved trigeminal branch. Eye involvement requires prompt medical evaluation because shingles in the ophthalmic branch can threaten vision. Facial PHN may be confused with trigeminal neuralgia, dental pain, sinus pain, migraine, or TMJ-related pain. The diagnosis depends on shingles history, dermatome distribution, pain quality, skin sensitivity, and clinical examination.
Can postherpetic neuralgia mimic pain from the heart, lungs, breast, or internal organs?
Yes. Postherpetic neuralgia can mimic internal organ pain when it affects thoracic or abdominal dermatomes. Intercostal PHN may feel like a burning, tight, stabbing, or electric band around one side of the chest or abdomen. Patients may fear pain from the heart, breast, lung, liver, stomach, or gallbladder, especially when no obvious rash remains. A key clue is that shingles-related pain usually follows one nerve territory on one side of the body and is often touch-sensitive. Clothing, bedsheets, movement, breathing, or skin brushing may trigger pain. Internal organ tests may be normal because the pain source is the irritated intercostal nerve rather than the organ itself.
When should postherpetic neuralgia symptoms be checked in person urgently?
Postherpetic neuralgia symptoms should be checked urgently in person when there are eye symptoms, vision changes, severe eye pain, facial weakness, widespread rash, fever, confusion, immune suppression, or worsening neurological signs. Shingles affecting the ophthalmic branch of the trigeminal nerve can threaten the eye and requires prompt medical evaluation. New weakness, bladder problems, severe headache, or spreading neurological symptoms should not be managed only through telehealth. A remote consultation can help with chronic PHN and treatment planning, but emergency symptoms need direct examination, appropriate testing, and sometimes urgent antiviral or specialist treatment. The goal is to avoid missing active infection, eye involvement, or another serious neurological condition.
Why does postherpetic neuralgia pain persist despite treatment?
Postherpetic neuralgia often persists despite treatment because therapy may address only one part of the pain mechanism. The original trigger is viral injury to the sensory nerve, but chronic pain may also involve peripheral sensitization, dorsal root ganglion irritation, central sensitization, local muscle spasm, trigger points, low-grade inflammation, sleep disturbance, and systemic factors such as diabetes or nutritional deficiencies. If only one medication is used without identifying these contributors, pain may improve temporarily but return or remain only partially controlled. Persistent PHN usually requires reassessment of which anatomical structure is generating the pain, what process keeps it active, and which factors maintain nerve hypersensitivity.
Why do some postherpetic neuralgia patients improve only temporarily with medication?
Temporary improvement with medication often means that nerve excitability was reduced, but the deeper pain-maintaining factors were not fully treated. Gabapentin, pregabalin, lidocaine, or antidepressant-type pain modulators can calm the sensitized nerve, but pain may return if trigger points, muscle spasm, local inflammation, friction sensitivity, central sensitization, or poor sleep continue to reactivate the pain pathway. In other patients, the dose may not yet be optimized, or side effects may prevent adequate titration. PHN treatment often needs 4–8 weeks of adjustment, not a single fixed prescription. When relief is partial, the next step is usually mechanism-based refinement rather than simply declaring treatment failure.
Can muscle spasm or trigger points maintain postherpetic neuralgia pain?
Yes. In many patients, postherpetic neuralgia is not only residual nerve injury. Muscles and soft tissues along the affected nerve pathway may become irritated, tense, or inflamed after weeks or months of protective posture and pain. In thoracic PHN, intercostal muscles may develop spasm or trigger points around the painful rib band. In facial PHN, jaw, facial, or cervical muscles may contribute to pain amplification. These local irritators can repeatedly stimulate an already sensitized nerve and make allodynia or burning pain worse. This is why treatment may include desensitization, physical therapy, trigger-point treatment, selected nerve blocks, and carefully monitored medication combinations alongside standard neuropathic pain therapy.
What contributing factors may keep postherpetic neuralgia active?
Several contributing factors can keep postherpetic neuralgia active even when the initial viral injury is no longer present. Central sensitization can make the nervous system amplify even mild signals. Poor sleep increases pain perception and reduces pain tolerance. Stress does not cause PHN, but it increases nervous system reactivity. Diabetes, thyroid disease, immune dysfunction, chronic inflammation, obesity, insulin resistance, and other comorbidities can increase nerve vulnerability. Low vitamin B12, vitamin D, magnesium, iron, or abnormal vitamin B6 levels may contribute to burning, tingling, or hypersensitivity. Physical inactivity and deconditioning may also reduce pain tolerance. These factors rarely act alone, but they can prevent stable recovery.
Are nerve blocks or sympathetic blocks necessary for postherpetic neuralgia?
Nerve blocks or sympathetic blocks are not necessary for every patient with postherpetic neuralgia. They are considered when pain remains focal, severe, and resistant despite optimized medication, topical therapy, desensitization, and treatment of local irritators. Peripheral nerve blocks may target intercostal nerves, paravertebral regions, or trigeminal branches depending on pain location. Sympathetic blocks may help selected patients when burning sensitivity is accompanied by autonomic features such as color change, cold skin, or marked hypersensitivity. Epidural injections or botulinum toxin may also be considered in specific cases. These procedures work best as part of a broader protocol, not as isolated procedures without medication optimization.
When are radiofrequency or neuromodulation procedures considered for postherpetic neuralgia?
Radiofrequency and neuromodulation procedures are reserved for selected, refractory postherpetic neuralgia cases. Pulsed radiofrequency may be used near the dorsal root ganglion to calm nerve activity without intentionally destroying the nerve. Thermal radiofrequency is used less often because it carries a higher risk of worsening dysesthesia or neuritis. Neuromodulation, especially dorsal root ganglion stimulation, is considered for severe, chronic, highly localized pain that has not responded to medication, topical treatment, blocks, or rehabilitation. A temporary trial is usually performed before permanent implantation to confirm meaningful relief. These treatments are not first-line options; they are advanced steps when structured conservative and interventional care has failed.
What should I do at home to reduce postherpetic neuralgia pain and nerve sensitivity?
Home care for postherpetic neuralgia should focus on reducing nerve irritation while supporting the medical plan. Protect the sensitive skin from friction, tight clothing, extreme temperature, and repeated scratching. Gentle desensitization may help when done carefully and gradually, but it should not be forced if it sharply increases pain. A simple pain diary can help identify triggers such as sleep loss, stress, clothing, movement, cold air, or specific activities. Follow medication titration exactly, because many PHN drugs require gradual adjustment. Good sleep, controlled blood sugar, correction of nutritional deficiencies, and gentle activity may also reduce overall nerve sensitivity. Home measures help most when combined with mechanism-based treatment.
How can telehealth help manage persistent postherpetic neuralgia?
Telehealth can help manage persistent postherpetic neuralgia by allowing a specialist to review the pain history, dermatome location, previous shingles episode, medication response, triggers, and possible local irritators. During an online consultation, the patient can describe or show the painful area, identify touch-sensitive zones, and explain which movements, clothing, or pressure worsen pain. This helps determine whether symptoms are caused mainly by nerve injury, central sensitization, muscle spasm, trigger points, or another contributor. The treatment plan can then combine neuropathic medication, topical therapy, desensitization, physical measures, and selected procedures when needed. Follow-up contact is especially useful during the first weeks while medication doses are adjusted.
Can postherpetic neuralgia consultation be reimbursed by health insurance?
Reimbursement depends on your individual insurance plan and whether it includes out-of-network or international specialist consultation benefits. We do not bill insurance companies directly. After the consultation, we can provide a formal medical report and a detailed invoice containing the clinical information usually needed for reimbursement claims. Many patients use this documentation when submitting a claim to their insurer, but approval is never guaranteed and should be checked with the insurance provider in advance. The consultation is paid directly by the patient. The report may then serve as supporting documentation for possible reimbursement, especially when the consultation addresses persistent postherpetic neuralgia despite previous treatment.
Additional Patient Resources
Clear, trustworthy information for patients and families about shingles and postherpetic neuralgia (PHN):
-
NHS — Post-herpetic neuralgia
Symptoms, treatment options, and when to seek urgent care. -
CDC — About Shingles
Overview of shingles, complications, and prevention. -
CDC — Shingles Symptoms & Complications
What to expect, including PHN as the most common complication. -
Mayo Clinic — Postherpetic neuralgia: Symptoms & Causes
Patient-friendly explanation of PHN and risk factors. -
Mayo Clinic — Postherpetic neuralgia: Diagnosis & Treatment
Medications, topicals, and procedures explained. -
Cleveland Clinic — Postherpetic Neuralgia
Overview of symptoms, diagnosis, and treatment options. -
Patient.info — Postherpetic Neuralgia (Leaflet)
Practical patient leaflet with FAQs and self-care advice.