Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

(heart, lungs, breast, stomach, bladder, kidney, liver, etc.)
Author: Zeljko Kojadinovic, MD, PhD — neurosurgeon and chronic pain specialist
Last medically reviewed: June 10, 2026
Who this page is for
This page is for patients who have persistent pain that has been attributed to internal organ disease — for example, pain in the chest, abdomen, pelvis, or urinary tract — but repeated imaging and laboratory results have remained normal.
Pain often continues because the true cause is nerve or musculoskeletal irritation that “mimics” internal organ pain, and these sources have not been properly identified or treated. As a result, medications aimed at the wrong organ or general painkillers usually fail to provide relief. Once the true pain generators are recognized, most cases improve with a targeted combination of medications, sometimes supported by vitamin or supplement therapy.
A detailed telehealth consultation allows assessment of all contributing factors and guidance on the most effective diagnostic and treatment approach.
Contents
- Who This Page Is For
- General About Pain That Mimics Illness
- What Makes This Consultation Different?
- Breast Pain: Normal Tests
- Heart/Chest Pain: Normal Tests
- Stomach/Gallbladder Pain: Normal Tests
- Kidney/Flank Pain: Normal Tests
- Bladder/Pelvic Pain: Sterile Tests
- Why Are Organ Tests Normal?
- Pinpointing Pain Source in Video Visit
- Treatment After Cause Is Found
- Frequently Asked Questions
- When To Seek Urgent Care
- Start Telehealth Consultation Now
- Related Topics and Resources
General About the Pain that Mimics Illnesses
All organ tests are normal, yet the pain persists? Many patients report kidney, heart/chest, breast, stomach, or bladder pain despite normal labs and imaging (ultrasound/CT/MRI, ECG, endoscopy, urinalysis). In many such cases, the true source is irritation of a sensory nerve—not disease of the organ itself. Patients are then treated for months for a presumed organ problem while the real cause lies in the spinal canal, paraspinal region or in the chest/abdominal wall. Once the exact pain generator—often a 1–2 cm trigger point and its radiation—is located, treatment becomes straightforward.
Pain arising from irritation of a truncal sensory or sensorimotor nerve is often referred to as musculoskeletal pain (pain coming from muscles, bones, or joints), neuralgic pain (pain caused by nerve irritation), or neuropathic pain (pain due to nerve damage or dysfunction). Nerve irritation may be caused by inflammation (for example after herpes zoster or due to metabolic problems), inflammation and spasm of the surrounding muscle, pressure from a ligament, nerve entrapment (a nerve being pinched or compressed), inflammation of local bursae (small fluid-filled sacs near joints), and so on.
Any pain can only be treated effectively once the exact anatomical structure responsible has been identified, as well as contributing factors causing and maintaining irritation in them.
What Makes This Consultation Different?
Many patients are told their pain is due to an organ disorder, yet the true source is often missed. When labs and imaging are normal, my approach starts by looking for a focal nerve irritation—most commonly in the spinal canal, paraspinal region or in the chest/abdominal wall.
During the video consultation, I review your medical documentation, ask highly targeted questions, and guide you through simple motion and pressure tests that you perform yourself. This helps locate the exact anatomical source of your pain — by reproducing or relieving it through specific actions.
This functional evaluation has the same diagnostic value as an in-person physical exam. Effective treatment begins only after the true cause of pain is identified — and that starts with a conversation guided by a physician who understands pain anatomy and knows exactly what structures can generate pain in your case.
This approach can lead to improvement even in long-term, chronic pain that mimics organ disease.
Breast Pain with Normal Mammogram/Ultrasound — When Is It Nerve-Origin Pain
Breast pain with a normal mammogram or ultrasound is a common example of pain that mimics internal organ disease. With the rising incidence of breast cancer, this symptom creates particular anxiety for many women, who fear that an early cancer might be missed. Pain from irritated or sensitized trunk nerves (intercostal nerves or spinal roots) can feel identical to pain coming from the breast. Routine organ tests are then normal, and therapy aimed at the organ does not help. Similar can happen with postsurgical pain,
Heart/Chest Pain with Normal ECG/Echo — Typical Scenarios We See
– Intercostal neuralgia (reproducible with fingertip pressure between ribs; worse with trunk rotation or deep breath).
– Thoracic dorsal root irritation (band-like chest pain; often with paraspinal tenderness).
– Costosternal/costochondral joint irritation (precise tender point near the sternum).
More about chest pain mimicking heart disease can be read on this page.
Stomach/Gallbladder-Like Pain with Normal Ultrasound/Endoscopy
When ultrasound and endoscopy are normal, a common cause is abdominal wall nerve entrapment (e.g., ACNES) or referral from thoracic/upper-lumbar roots. Clues include a precise 1–2 cm tender point along the costal margin or lateral edge of the rectus, pain that increases with localized pressure, and a positive Carnett sign (worse when tensing the abdominal wall). Symptoms are usually posture-dependent rather than meal-related. During a video visit we map the exact spot and radiation with guided pressure and small-movement maneuvers, then plan targeted therapy.
Kidney/Ureter or Flank Pain with Normal Imaging
If CT/ultrasound are normal and urine tests are clean, consider iliohypogastric, ilioinguinal, or genitofemoral nerves—or certain nerve roots—as the pain source. Typical features are a band or line of pain from the back toward the groin, worsening with turning in bed, hip extension, or bending. A small tender point above the iliac crest or near the inguinal canal is often present, and symptoms are not linked to urination. Guided self-exam during a video consult helps confirm a nerve-origin pattern and select focused treatment. Video consultation is also known as a virtual visit, video visit, online consultation, remote consultation or telehealth appointment.
Bladder/Pelvic Pain with Sterile Tests
With sterile urine and normal cystoscopy, pelvic nerves can mimic bladder disease (IC-like phenotype, pudendal or genitofemoral involvement). Pain often worsens with sitting or cycling and may radiate to the perineum, vulva, scrotum, or inner thigh; pelvic floor tenderness or tightness is common. We use a symptom map plus guided palpation and posture tests to differentiate patterns, then combine pelvic-floor relaxation, nerve-glide work, and targeted medication; nerve blocks are considered when appropriate.
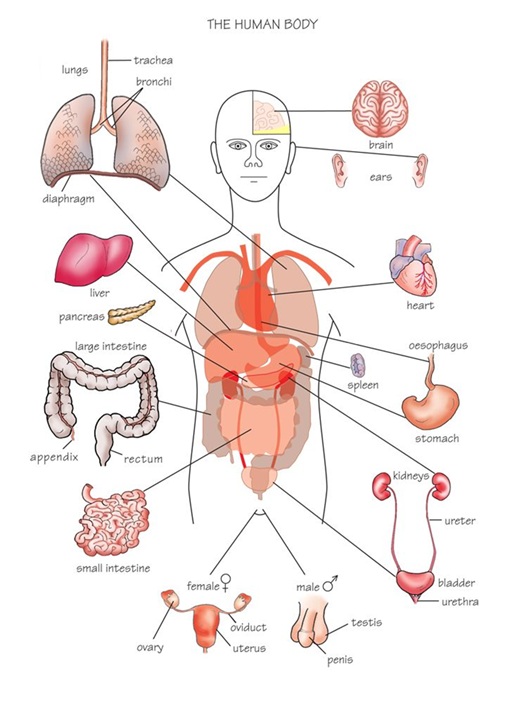
Illustration of trunk nerves and organs; identical chest/breast, stomach or bladder pain may be nerve-origin.
Organ Pain with Normal Endoscopy/CT — Why Are Tests Often Normal?
- Organ-focused diagnostics (labs, ultrasound, CT/MRI) do not detect or measure nerve pain.
- EMG is frequently normal in purely sensory nerve problems.
- Pain patterns, triggers, and movement/pressure tests are more informative than static images.
Pinpointing the Real Source of Mimicked Organ Pain in a Video Visit
Video visit is also known as a virtual visit, video consultation, online consultation, remote consultation or telehealth appointment.
- We start with a focused nerve hypothesis that there is a focal irritation—often in spinal canal, paraspinal or in the chest/abdominal wall.
- Review of your records and imaging, then a targeted interview to map the exact irritation point and its radiation.
- Guided self-exam: brief pressure, posture, and small-movement maneuvers that reproduce or switch off the pain. This functional exam has the diagnostic value of an in-person visit.
- Decision point: do we need any additional test, or can we begin treatment right away?
- Once the true pain generator is identified, treatment becomes straightforward—often with faster improvement.
(Our method relies on anatomy of pain; many patients improve quickly once the true source is identified.)
When to Seek Urgent In-Person Care (Safety First)
Call emergency services for: new crushing chest pain with shortness of breath, fainting, severe sudden abdominal pain with fever, new neurological deficits, progressive weakness, unexplained weight loss, or any rapidly worsening condition. Video consultations are not a substitute for emergency evaluation.
Treatment After the Cause of Breast, Heart, Stomach, or Kidney Is Found
- Tailored medication plan (short, targeted, with clear goals).
- Local measures, posture/nerve-glide instructions, activity adjustments.
- Coordination with your local physician for targeted nerve blocks when needed.
- Escalation only if necessary.
- Follow-up to fine-tune the plan.
Expectation: when the true source is identified, improvement is typically felt within about 10 days; persistent cases are re-checked and the plan adjusted. (This reflects my clinical practice.)
Frequently Asked Questions about Pain that Mimics Internal-Organ Disease
All organ tests are normal but pain persists — could it still be nerve pain?
Yes. Pain can persist even when organ-focused tests are normal because many tests are designed to detect organ disease, not nerve irritation or small musculoskeletal pain generators. Ultrasound, CT, MRI, ECG, endoscopy, cystoscopy, and blood tests may all be normal if the pain comes from a sensory nerve, spinal root, chest wall, abdominal wall, rib joint, pelvic floor, or a small focal trigger point. The key clue is often pain that follows a line, worsens with posture, movement, pressure, breathing, sitting, or twisting, and can be reproduced from a precise painful spot.
Why can CT, MRI, ultrasound, ECG, endoscopy, cystoscopy, and labs be normal in nerve-related pain?
These tests are excellent for many serious diseases, but they do not measure pain signals directly. A normal ECG or echocardiogram can reduce concern about heart disease, and normal CT, ultrasound, endoscopy, cystoscopy, or blood tests can reduce concern about organ damage, infection, tumor, stones, or inflammation. However, irritated sensory nerves, intercostal neuralgia, abdominal wall nerve entrapment, pelvic nerve irritation, muscle spasm, or small tender pain generators may not appear on standard imaging. That is why pain behavior, exact location, radiation, pressure sensitivity, and movement triggers can be more informative than another scan.
Chest pain with normal ECG and echocardiogram — could it be intercostal neuralgia?
Yes. Chest pain with normal ECG and echocardiogram can sometimes come from intercostal neuralgia, thoracic spinal root irritation, costosternal joint irritation, rib dysfunction, or chest wall muscle and nerve irritation. This pain may feel alarming because it appears in the heart or lung region. Clues include pain that worsens with trunk rotation, deep breathing, coughing, pressure between the ribs, or a specific posture. New, crushing, severe, or unexplained chest pain must first be assessed urgently. But when cardiac and pulmonary causes are excluded, nerve or chest wall sources should be considered.
Can chest wall or rib pain mimic heart or lung pain?
Yes. Chest wall and rib pain can closely mimic heart or lung pain because the brain receives pain signals from the chest wall, ribs, intercostal nerves, thoracic spine, and internal organs in overlapping regions. Intercostal nerve irritation may create a band-like pain around the chest. Costochondral or costosternal irritation can produce a sharp tender point near the sternum. Rib and muscle pain can worsen with breathing, twisting, coughing, or direct pressure. The important step is first to exclude urgent heart and lung causes, then to identify whether the remaining pain behaves like nerve or musculoskeletal pain.
Breast pain with normal mammogram and ultrasound — can it come from chest wall nerves?
Yes. Breast pain with normal mammogram and ultrasound can come from chest wall nerves, intercostal neuralgia, thoracic spinal roots, rib joints, pectoral muscles, or postsurgical nerve irritation. The pain may feel as if it is inside the breast, even when breast imaging is normal. Clues include a small tender point along a rib, pain near the sternum or under the breast, burning or stabbing pain, pain that worsens with pressure or arm movement, and radiation around the chest wall. Breast disease must be excluded appropriately, but persistent pain after normal breast evaluation may need pain-source assessment.
Can intercostal nerve irritation cause breast pain without breast disease?
Yes. Intercostal nerve irritation can cause pain that is perceived in the breast even when the breast itself is healthy. Intercostal nerves run between the ribs and supply sensation to the chest wall and breast region. When one of these nerves is irritated by muscle spasm, rib joint irritation, thoracic root irritation, surgery, trauma, shingles, or prolonged posture strain, the pain can be felt as burning, stabbing, aching, or hypersensitivity in the breast area. A normal mammogram or ultrasound does not exclude intercostal neuralgia because routine breast imaging does not test nerve pain.
Stomach pain with normal endoscopy and ultrasound — could it be abdominal wall nerve entrapment?
Yes. Stomach or upper-abdominal pain with normal endoscopy and ultrasound can sometimes come from the abdominal wall rather than the stomach, gallbladder, liver, or pancreas. Abdominal wall nerve entrapment, including ACNES, may cause a precise painful spot along the rectus muscle border, costal margin, or abdominal wall. Pain may worsen with local pressure, sitting up, twisting, coughing, or tightening the abdominal muscles. A positive Carnett-type pattern, where pain increases when the abdominal wall is tensed, supports an abdominal wall source. This pain is often posture-dependent rather than meal-dependent.
What is ACNES and how can it mimic stomach, gallbladder, or abdominal organ pain?
ACNES means anterior cutaneous nerve entrapment syndrome. It occurs when a small sensory nerve branch becomes irritated or trapped as it passes through the abdominal wall. The pain can mimic stomach, gallbladder, liver, intestinal, or pelvic organ pain because it is felt in the same abdominal region. Patients often have normal endoscopy, ultrasound, CT, and laboratory tests. A typical clue is a very small tender point, often one to two centimeters wide, with pain that increases when pressing on the spot or tightening the abdominal muscles. Treatment is different from organ-directed therapy.
Right upper abdominal or liver-area pain with normal ultrasound and blood tests — could it be nerve or muscle pain?
Yes. Right upper abdominal pain or liver-area pain with normal ultrasound and blood tests may come from the abdominal wall, lower ribs, thoracic spinal roots, intercostal nerves, costal margin irritation, or myofascial trigger points. Patients may feel pain under the ribs and assume it is liver or gallbladder pain, especially if the discomfort is deep or persistent. Clues suggesting a nerve or muscle source include pain that worsens with twisting, bending, pressure along the ribs, deep breathing, prolonged sitting, or a precise tender point. Organ disease must be excluded first, but normal tests shift attention to pain generators outside the organ.
Kidney or flank pain with normal CT, ultrasound, and urine tests — could it be nerve-related?
Yes. Kidney or flank pain with normal CT, ultrasound, and urine tests can be nerve-related. Possible sources include thoracolumbar spinal roots, iliohypogastric nerve irritation, ilioinguinal nerve irritation, genitofemoral nerve irritation, abdominal wall trigger points, quadratus lumborum muscle pain, or pain from the lower ribs and paraspinal region. Clues include pain that travels from the back toward the groin, pain worsened by turning in bed, hip extension, bending, prolonged sitting, or pressure above the iliac crest. If urine is clean and imaging shows no stone, obstruction, or kidney disease, nerve and musculoskeletal causes become more likely.
Can iliohypogastric, ilioinguinal, or genitofemoral nerves mimic kidney, ureter, or groin pain?
Yes. Iliohypogastric, ilioinguinal, and genitofemoral nerves can produce pain in the flank, lower abdomen, groin, upper inner thigh, labial, scrotal, or inguinal region. Because this distribution overlaps with kidney, ureter, pelvic, and groin symptoms, patients may undergo repeated urine tests, CT scans, ultrasound, or urology evaluations before a nerve source is considered. Pain may be sharp, burning, pulling, electric, or pressure-like. It may worsen with hip movement, abdominal wall pressure, standing, walking, coughing, or certain positions. A precise tender point near the inguinal canal or iliac crest can be an important clue.
Bladder pain with sterile urine and normal cystoscopy — could pelvic nerves mimic bladder disease?
Yes. Bladder pain with sterile urine and normal cystoscopy can sometimes be produced or amplified by pelvic nerve irritation, pelvic floor muscle spasm, pudendal nerve sensitivity, genitofemoral neuralgia, ilioinguinal neuralgia, or lumbar and sacral referral. The pain may feel like pressure, burning, urgency, or a bladder flare even when infection is absent and cystoscopy does not show a clear bladder cause. Clues include pain that worsens with sitting, cycling, intercourse, bowel activity, pelvic floor tension, or pressure in the perineum, groin, genitals, or inner thigh. This pattern needs pelvic pain-source analysis.
Can pelvic floor muscle spasm or pudendal nerve irritation mimic bladder pain?
Yes. Pelvic floor muscle spasm and pudendal nerve irritation can mimic bladder pain because they can create urinary urgency-like sensations, burning, pressure, perineal pain, genital pain, rectal discomfort, and sitting-related pelvic pain. The bladder may feel involved even when urine tests are sterile and cystoscopy is normal or inconclusive. Tight pelvic muscles can irritate nerves and maintain a pain cycle. Pudendal irritation often worsens with sitting and improves when pressure is reduced. In many patients, bladder, nerve, and muscle mechanisms overlap, so treatment must identify the dominant generator rather than treating every symptom as bladder inflammation.
Why does organ-like pain often worsen with posture, movement, pressure, or deep breathing?
Organ-like pain that worsens with posture, movement, pressure, twisting, sitting, standing, coughing, or deep breathing often suggests that the pain may come from nerves, muscles, joints, ribs, abdominal wall, pelvic floor, or spinal roots rather than from the organ itself. Internal organ pain is usually less dependent on precise pressure points or small body movements, although exceptions exist. When pain can be reproduced by pressing a small area, stretching a nerve path, rotating the trunk, tensing the abdominal wall, or changing sitting pressure, the pattern becomes more compatible with a mechanical or nerve-related pain generator.
What does a 1–2 cm tender point suggest when organ tests are normal?
A small one to two centimeter tender point can be an important clue when organ tests are normal. It may suggest a focal nerve irritation, abdominal wall nerve entrapment, intercostal neuralgia, costochondral irritation, muscle trigger point, ligament irritation, or a local pain generator near the chest wall, abdominal wall, flank, groin, or pelvis. The tender point matters especially if pressing it reproduces the patient’s typical pain and radiation. This does not automatically prove the diagnosis, but it shifts attention from broad organ disease toward a specific anatomical source that can be tested and treated more directly.
Can EMG be normal in nerve pain that mimics internal-organ disease?
Yes. EMG can be normal in nerve pain that mimics internal-organ disease because many of these conditions involve small sensory nerves, superficial cutaneous branches, intercostal nerves, pelvic nerves, or pain pathways that are not well tested by routine EMG and nerve conduction studies. EMG is more useful for selected large-fiber neuropathies, radiculopathies, or motor nerve problems. A normal EMG does not exclude intercostal neuralgia, ACNES, pudendal neuralgia, ilioinguinal or genitofemoral irritation, or sensory nerve pain. Diagnosis often depends more on pain distribution, triggers, pressure response, and functional examination.
How can a video consultation identify pain that mimics organ disease?
A video consultation can help identify pain that mimics organ disease by combining record review, symptom mapping, pain behavior analysis, and guided self-examination. The consultation looks at where the pain starts, where it radiates, what provokes it, what reduces it, whether it follows a nerve path, and whether pressure, posture, breathing, trunk movement, abdominal wall tension, or sitting changes the symptoms. In many cases, this functional information is more useful than repeating tests that already excluded major organ disease. The goal is to decide whether pain is organ-related, nerve-related, musculoskeletal, spine-referred, pelvic, or mixed.
Can a video consultation really replace a physical exam for this type of pain?
A video consultation cannot replace every type of physical examination, and it is not appropriate for emergencies. However, for many chronic organ-mimicking pain patterns, a structured video assessment can provide strong diagnostic direction. The patient can show the exact pain location, mark the painful area, apply guided pressure, change posture, perform small movements, tense the abdominal wall, rotate the trunk, or test sitting-related triggers. When these maneuvers reproduce or reduce the typical pain, they can help localize the pain generator. If the pattern is unclear or concerning, in-person evaluation is recommended.
Do I need an EMG, MRI, CT, or another test before booking a second opinion?
Not always. Many patients already have enough information from previous organ-focused tests, imaging, specialist reports, and treatment history to begin a pain-source review. A second opinion first analyzes the symptom pattern, test results, pain location, radiation, triggers, and previous treatment response. Additional EMG, MRI, CT, ultrasound, endoscopy, cystoscopy, or laboratory tests are useful only when they could change management, exclude red flags, or clarify a suspected diagnosis. Repeating tests without a clear question may delay treatment. The goal is to decide what is missing, not to repeat everything automatically.
How quickly can pain improve once the true source is identified?
When the true pain source is identified and treatment is targeted correctly, some patients feel meaningful improvement within days to about ten days. This depends on the cause, chronicity, nerve sensitization, inflammation, muscle spasm, posture factors, previous treatments, and whether the pain is purely local or mixed. Improvement does not always mean complete disappearance of pain immediately. A realistic early goal is reduction in intensity, fewer flares, better movement tolerance, clearer triggers, and a treatment plan that finally matches the pain generator. If there is no progress, the diagnosis and plan should be reviewed instead of waiting passively.
Is a video visit only for simple or minor organ-mimicking pain cases?
No. A video visit is often most useful when pain is persistent, confusing, or has not responded to standard treatment. Many patients with organ-mimicking pain have already seen several specialists, repeated tests, and tried medications aimed at the wrong organ. The value of the consultation is not that the case is simple, but that the assessment is structured around pain anatomy, nerve pathways, trigger points, radiation patterns, and functional testing. Complex cases may still need local examination, procedures, or further tests, but telehealth can often clarify the most likely direction and avoid repeating ineffective treatment.
When should organ-like pain be treated as urgent and not managed by telehealth?
Organ-like pain should be treated as urgent when it is new, severe, rapidly worsening, or associated with warning signs. Seek emergency care for crushing chest pain, shortness of breath, fainting, severe sudden abdominal pain, fever, vomiting blood, black stools, visible blood in urine, inability to urinate, new weakness, numbness in the saddle area, loss of bladder or bowel control, unexplained weight loss, or progressive neurological symptoms. Telehealth is useful for chronic or previously investigated pain patterns, but it must not replace emergency evaluation when serious heart, lung, abdominal, urinary, neurological, or infectious disease is possible.
Start Your Telehealth Consultation with a Pain Specialist
If your pain treatment has failed or you’re unsure what to do next — don’t wait. A detailed telehealth consultation can help identify the exact cause of your pain, even if previous therapies didn’t work.
- ✔ First, send a short message describing your problem
- ✔ You’ll receive a reply within 24 hours if and how we can help — including the consultation cost and a suggested time
- ✔ Only then, you can send your medical documentation
- ✔ The video consultation is followed by a written report and follow-up questions (up to 10 days)
- ✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Consultation fees typically range from $180–250, depending on the complexity of your case.
This is within the usual range for specialist telehealth consultations worldwide. Thousands of patients worldwide already use telehealth consultations for second opinions — it’s safe, accepted, and effective.
Related Topics About Pain in Internal Organs — Neurosurgery and Pain Treatment
Online pain consultation in detail for pain nerve pain mimicking organ disease
Schematic explanation of the video consultation in nerve pain mimicking organ disease
See the page “Possible Reasons for Poor Pain Treatment Effectiveness in Nerve Pain Mimicking Organ Disease” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
Treatment of complex cases of pain in pain-mimicking organ disease can be analyzed by artificial intelligence (AI)
Similar neuropathic pains is trigeminal neuralgia