Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
February 28, 2026
Who This Vestibular Schwannoma Page Is For
This page is intended for patients diagnosed with vestibular schwannoma (acoustic neuroma) and for family members seeking a clear, medically accurate explanation of what this diagnosis means in real clinical practice.
It is particularly relevant for individuals deciding between observation, stereotactic radiosurgery, or microsurgical removal, as well as for those concerned about hearing preservation, facial nerve outcomes, tumor growth, or long-term prognosis.
If tumor size is increasing, hearing is declining, treatment recommendations differ between centers, surgery has been proposed or delayed, or uncertainty exists about whether to continue observation — an individualized
neurosurgical second opinion
can help clarify risks, expected functional outcomes, and the most appropriate strategy based on tumor size, growth behavior, and personal priorities.
When patients usually seek a second opinion for vestibular schwannoma
- Surgery is being proposed for a tumor under 3 cm, and you are unsure whether observation or radiosurgery could be reasonable alternatives
- Radiosurgery has been recommended, but there is concern about long-term tumor control or gradual hearing decline
- The tumor is measuring between 2 and 3 cm, and you are unsure whether this represents a critical decision window
- The tumor is growing, yet the pace of growth and urgency of intervention remain unclear
- Two specialists recommend different strategies (observation vs radiosurgery vs microsurgery) for the same MRI findings
- Hearing is still serviceable, and you want to understand how realistic hearing preservation may be in your specific case
- The tumor exceeds 3 cm and there is uncertainty about surgical risk versus expected neurological outcome
- Facial nerve weakness, worsening imbalance, or hydrocephalus has developed and the next step is unclear
- You have NF2 or bilateral tumors and long-term hearing preservation requires individualized planning
These situations often represent genuine clinical gray zones rather than simple “right or wrong” decisions. An expert neurosurgical review can help clarify whether continued observation is safe, whether intervention should be timed strategically, and what realistic functional outcomes (hearing and facial nerve) can be expected in your specific anatomical situation: Request Consultation
Vestibular Schwannoma (Acoustic Neuroma) — Quick Summary (Read This First)
- Vestibular schwannoma is a benign (WHO grade 1) tumor. It arises from the Schwann cells of the eighth cranial nerve (the vestibulocochlear nerve), which is responsible for transmitting hearing and balance information from the inner ear to the brain. The tumor is extracerebral, meaning it is located outside the brain tissue itself, situated within a narrow space at the base of the skull known as the cerebellopontine angle.
- It is uncommon but not rare. Modern MRI-based data show an incidence of approximately 2–5 per 100,000 persons per year, higher than older registries due to improved detection.
- Most tumors are unilateral and sporadic. Bilateral tumors are strongly associated with Neurofibromatosis Type 2 (NF2), a rare genetic condition.
- The most frequent early persistent symptom is unilateral hearing loss. Brief balance disturbance may occur early and then improve due to central compensation, which can delay diagnosis.
- About 30–50% of tumors demonstrate measurable growth during follow-up. Average growth for growing tumors is roughly 1–2 mm per year, though behavior is variable.
- Observation alone is initially chosen in approximately 40–60% of patients, particularly when tumors are small (typically under 1.5–2 cm), symptoms are minimal, growth has not been documented, or patient-specific factors (age, comorbidities) favor a conservative approach.
- Management options include observation, stereotactic radiosurgery, and microsurgery. The optimal choice depends on tumor size, growth rate, hearing status, age, symptoms, and patient preference.
- Radiosurgery is typically most suitable for small- to medium-sized tumors (generally up to about 2.5–3 cm) without significant brainstem compression. Larger tumors more often require microsurgical treatment.
- Functional outcomes depend strongly on tumor size and surgical expertise. Smaller tumors offer higher chances of preserving facial nerve function and, in selected cases, hearing.
- Different specialists may reasonably recommend different strategies. Variability often reflects differences in tumor size, hearing status, growth behavior, patient age, and institutional philosophy rather than medical error.
- This page is structured so you can read only what matters to you. Use the Contents section to navigate directly to symptoms, diagnosis, treatment options, outcomes, or when a neurosurgical second opinion may be helpful.
Most readers benefit from reviewing the Quick Summary together with the sections on Early Symptoms, Treatment Strategies, and Facial Nerve & Hearing Outcomes. Other sections provide deeper clinical context and decision-making insight.
Contents
- Who this page is for
- When to seek consult
- Quick summary
- Definition
- How common
- Which side
- Is it hereditary
- Tumor growth
- Early symptoms
- Initial dizziness
- Hearing phase
- Advanced signs
- Diagnosis
- Audiometry
- MRI
- CT
- Differential
- Treatment overview
- Observation
- Radiosurgery
- Microsurgery
- Outcomes
- Special situations
- Very Small Tumor
- Tumor 1-2 cm
- Tumor 2-3 cm
- Large Tumor > 3 cm
- Bilateral NF2
- Cystic tumors
- Hydrocephalus
- Tumor Recurrence
- Pathology
- Prognosis
- Why opinions differ
- Request consultation
- FAQs
Definition of Vestibular Schwannoma
Vestibular schwannoma (historically called acoustic neuroma) is a benign tumor that develops from the Schwann cells covering the vestibular portion of the eighth cranial nerve (the nerve responsible for balance and hearing). In a smaller proportion of cases, estimated at up to about 20%, the tumor may arise from the cochlear (hearing) portion of the nerve. It most commonly arises within the internal auditory canal and may extend into the cerebellopontine angle, the space between the cerebellum and the brainstem.
In simple terms, this tumor develops from the eighth cranial nerve connecting the inner ear with the brain, which explains both its historical name (“acoustic neuroma”) and its effects on hearing and balance.
Although benign, its location makes early recognition important — not because it spreads through the body, but because progressive growth can affect hearing, facial function, balance, and in advanced cases the brainstem.
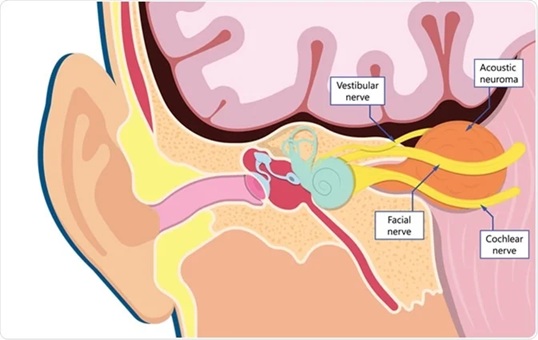
Image: Vestibular schwannoma growing from the internal auditory canal and extending into the space between the cerebellum and the brainstem. The internal auditory canal runs from the middle ear and houses the facial nerve and the 8th cranial nerve. The 8th nerve consists of an acoustic part and a vestibular part responsible for balance. A schwannoma most commonly grows on the vestibular portion.
You can read more about other brain tumors on our Brain Tumors page.
How Common Is Vestibular Schwannoma?
Incidence varies depending on the era and availability of MRI.
Older population-based registries reported approximately 0.5–1.0 cases per 100,000 persons per year.
More recent epidemiologic data, reflecting widespread MRI use, show higher detection rates — commonly 2–5 per 100,000 per year, with some modern datasets approaching 6–7 per 100,000 per year.
This isn’t a real increase in cases; rather, modern MRI scans have made it possible to detect small neuromas that often don’t cause any symptoms.
Laterality: On Which Side Does It Occur?
In the vast majority of patients, vestibular schwannoma is unilateral (one side only).
Bilateral tumors are strongly associated with Neurofibromatosis Type 2 (NF2). NF2 is a rare genetic disorder that causes tumors to grow on nerves.
Is Vestibular Schwannoma Hereditary?
Sporadic Cases
Most vestibular schwannomas are sporadic, meaning they are not inherited and occur without a family history. Most vestibular schwannomas develop because of changes in a gene called NF2 occurring only within the tumor tissue. This does not mean the patient has the genetic disease Neurofibromatosis Type 2, which is rare and inherited.
Neurofibromatosis Type 2 (NF2)
NF2 is a rare genetic condition characterized by the development of bilateral vestibular schwannomas. Unlike typical sporadic cases, NF2 is often diagnosed at a younger age and requires a different long-term management strategy.
In addition to vestibular schwannomas, patients with NF2 may also develop other tumors of the nervous system, most commonly schwannomas affecting other cranial or spinal nerves, meningiomas, and spinal tumors such as ependymomas. Because multiple tumors may appear over time, lifelong monitoring is required.
- Lifetime risk of bilateral vestibular schwannoma in NF2: approaches 90–95%
- NF2 prevalence: approximately 1 in 25,000–40,000
Neurofibromatosis Type 1 (NF1)
NF1 is much more common (about 1 in 3,000), but it is not typically associated with vestibular schwannomas. Bilateral vestibular schwannomas are not characteristic of NF1.
How Does the Vestibular Schwannoma Grow?
Growth behavior is variable.
Studies show:
- Approximately 30–50% of tumors demonstrate measurable growth during follow-up.
- Average growth rate for growing tumors: approximately 1–2 mm per year.
- Some tumors may grow faster (3–4 mm/year), especially if early progression is observed.
- Approximately 40–60% of small, sporadic vestibular schwannomas remain stable long-term without measurable growth.
Importantly, tumors may grow for several years and then stabilize permanently, which supports careful observation strategies in selected patients. Long-term studies show that if a vestibular schwannoma remains stable for approximately five years or longer, the likelihood of later significant growth becomes considerably lower. Therefore, older patients with longstanding stable hearing loss and unchanged tumor size over many years can often be reassured that immediate intervention is unlikely to be necessary, although periodic MRI follow-up is still recommended.
Early Symptoms of Vestibular Schwannoma: Why Diagnosis During the “Hearing Phase” Matters
Vestibular schwannoma does not follow a rigid “stage-by-stage” symptom pattern.
However, certain clinical tendencies are commonly observed.
Initial Vestibular Disturbance (Often Transient)
Because the tumor grows from the vestibular branch of the eighth cranial nerve (the nerve responsible for balance), some patients initially experience:
- Brief episodes of imbalance
- Mild vertigo
- Nausea
- A feeling of unsteadiness
In many cases, these symptoms improve within weeks due to central vestibular compensation.
As a result, early balance disturbance may disappear and not remain the dominant complaint.
The “Hearing Phase” — The Most Common Early Presentation
In clinical practice, the most frequent persistent early symptom is:
- Progressive unilateral hearing loss
- Sometimes sudden hearing loss
- Tinnitus (ringing in one ear)
Vestibular schwannomas typically grow slowly and may remain asymptomatic for many years. The tumor often begins to enlarge silently, without causing noticeable problems.
If symptoms develop, progressive unilateral hearing loss is usually the first manifestation. Importantly, this hearing impairment often appears only after months or even years of tumor growth. There is no strict millimeter threshold at which hearing becomes impaired. Even small intracanalicular tumors may significantly affect hearing.
At that stage, the tumor may remain stable indefinitely if no further enlargement occurs. However, if the tumor continues to grow significantly over time, additional neurological symptoms — such as imbalance, facial numbness, or, in large tumors, brainstem-related signs — usually develop only after several years.
Advanced Neurological Compression
With larger tumors (often >2–3 cm), additional cranial nerve and brainstem involvement may occur:
- Facial nerve compression → facial weakness
- Trigeminal nerve compression → facial numbness, trigeminal neuralgia
- Brainstem compression → gait disturbance
- Very large tumors → obstructive hydrocephalus (fluid buildup in the brain because the exit is blocked)
This clinical pattern explains why an MRI performed during isolated unilateral hearing loss allows for earlier diagnosis and broader treatment options. For example, smaller tumors can often be treated with radiosurgery to avoid invasive surgery. Early detection also improves functional preservation, as surgical results are generally worse for very large tumors
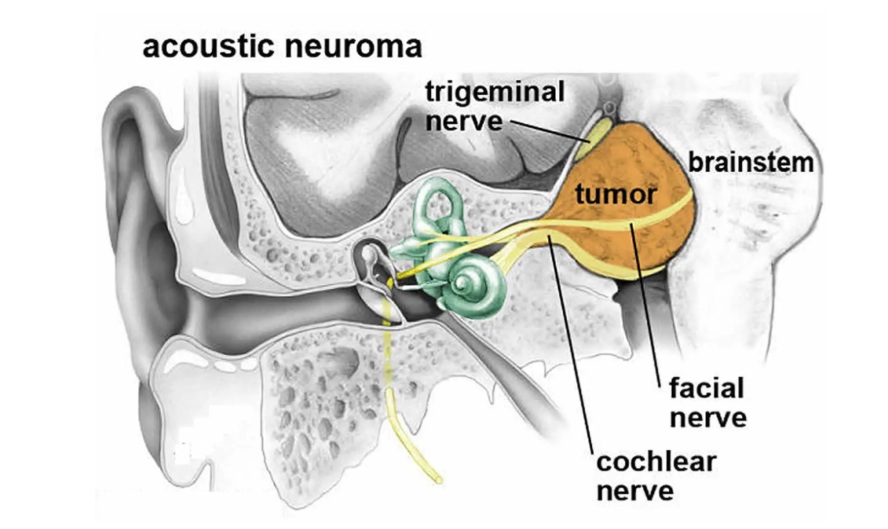
Image: Large vestibular schwannoma (>3 cm) extending from the internal auditory canal into the cerebellopontine angle. At this size, the tumor may compress the facial nerve, trigeminal nerve, and brainstem. Radiosurgery is typically more suitable for smaller tumors, while larger lesions often require microsurgical removal. As tumor size increases, surgical complexity and the risk of incomplete functional recovery may also increase.
Diagnosis of Vestibular Schwannoma
Audiometric Red Flags
Audiometry is a non-invasive hearing test that measures your ability to hear sounds of varying intensities and pitches across both ears. Asymmetric sensorineural hearing loss—where one ear performs significantly worse than the other due to nerve involvement—is the primary „red flag“ that triggers the need for an MRI to rule out a tumor.
Common MRI referral threshold:
A hearing difference of 15 dB or more between your ears at the 3 kHz frequency (a specific high-pitched tone, known as the ‘Rule 3000’).
MRI
The gold standard is MRI with and without gadolinium contrast.
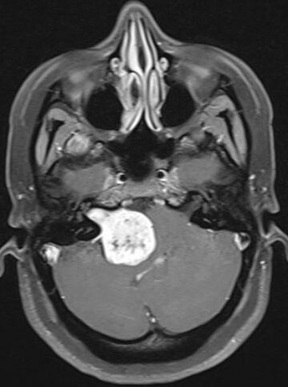
Image: MRI scan (T1-weighted with contrast) showing a bright vestibular schwannoma with a characteristic ‘ice cream cone’ appearance. The narrow portion (the cone) is located within the internal auditory canal, while the wider portion (the scoop) extends into the cerebellopontine angle between the brainstem and the cerebellum.
CT
CT is useful for:
- Preoperative bone anatomy assessment
- Surgical planning
- Differentiation of certain skull base lesions
Differential Diagnosis of Vestibular Schwannoma
- Meningioma of cerebellopontine angle
- Epidermoid cyst
- Metastasis
- Other cranial nerve schwannomas
Radiologic pattern usually distinguishes vestibular schwannoma clearly.
Treatment Strategies for Vestibular Schwannoma
Management depends on:
- Tumor size
- Growth pattern
- Hearing status
- Age
- Patient preference
- Genetic background (NF2 vs sporadic)
Therapeutic options are: observation, stereotactic radiosurgery or surgery.
1. Observation (Wait-and-Scan)
Common initial strategy for:
- Small tumors (<1.5–2 cm)
- Minimal symptoms
- Elderly patients
- Already poor hearing
Approximately 40–60% of small, sporadic vestibular schwannomas remain stable long-term and may require no active treatment. About 30–50% demonstrate measurable growth during follow-up. Even in growing tumors, intervention is considered only if progression is clinically significant.
Importantly, not all measurable growth automatically requires treatment. Some tumors show minimal enlargement over time and may later stabilize again during follow-up. In such cases, continued observation without active intervention remains appropriate, provided there are no clinically significant symptoms or rapid progression.
MRI follow-up is recommended both after initial diagnosis during observation and after active treatment (microsurgery or radiosurgery). Imaging is typically performed annually during the first five years, as most tumor growth or treatment-related changes occur within this period. If stability is confirmed, follow-up intervals may be extended, commonly with additional MRI scans at approximately 7–10 years and periodically thereafter. Earlier imaging should be arranged if new neurological symptoms develop.
Overall, long-term studies suggest that roughly one-third of patients initially managed with observation eventually require active treatment (surgery or radiation), while the majority can be safely monitored without intervention.
2. Stereotactic Radiosurgery (SRS)
Observation remains appropriate for small tumors without consistent documented growth.
Radiosurgery is typically considered when some of the following factors are present:
- Documented, sustained tumor growth on serial MRI (consistent enlargement over time rather than minor 1–2 mm variation on a single scan).
- Small to medium-sized tumors (generally up to 2.5–3 cm) when the goal is long-term tumor control rather than decompression; mild to moderate radiological brainstem contact without neurological deficits may still be compatible with radiosurgery, whereas significant mass effect usually favors surgery.
- Progressive symptoms during observation, particularly hearing decline.
- Patients who prefer a non-surgical approach or who are not optimal surgical candidates.
The goal of radiosurgery is long-term tumor control rather than immediate tumor removal.
Typical marginal dose: 12–13 Gy (single fraction).
Tumor control rates:
- 5-year control: 90–99%
- Facial nerve preservation: >95%
- Serviceable hearing preservation: ~40–60% (varies by baseline hearing)
Radiosurgery is generally most appropriate for small- to medium-sized tumors without significant brainstem compression. When the tumor exceeds approximately 3 cm, particularly in the presence of brainstem compression, progressive neurological symptoms, cystic enlargement, or hydrocephalus, microsurgical treatment is more commonly recommended.
In selected cases of very large tumors, a planned subtotal (debulking) resection may be performed to relieve brainstem compression, followed by staged radiosurgery for the residual tumor.
3. Microsurgical Removal
Indications
Microsurgical treatment is typically indicated in the following situations:
- Large tumors (generally >3 cm in maximal diameter)
- Brainstem compression or significant mass effect
- Progressive tumor growth on serial imaging
- Hydrocephalus
- Patient preference for definitive removal, even with small tumors
General Principles
Microsurgical removal is performed under general anesthesia with continuous intraoperative neurophysiological monitoring, particularly facial nerve monitoring and, in selected cases, auditory brainstem evoked potentials. These procedures are typically carried out in specialized centers with dedicated skull base experience.
Surgery is performed by a neurosurgeon, often in collaboration with a neuro-otologic (skull base) surgeon, depending on institutional practice.
Patient positioning depends on the selected approach:
- Supine with head rotation (most common overall): The patient lies flat on their back with their head turned to the side (giving the surgeon easy access to the ear area).
- Lateral / park-bench position (frequently used for retrosigmoid approach): The patient lies on their side (like sleeping) with the bottom arm safely tucked away, allowing the surgeon to reach the back of the head more easily.
- Semi-sitting position in selected centers, most commonly only for the retrosigmoid approach
The skin incision and surgical corridor vary according to the chosen approach.
Middle Fossa Approach
Primarily indicated for small intracanalicular tumors when hearing preservation is a major goal.
- Patient positioned supine with the head turned
- Temporal craniotomy performed above the ear
- Access to the internal auditory canal from a superior direction
- Designed to preserve hearing and facial nerve function
Retrosigmoid (Retromastoid) Approach
Commonly used for tumors extending into the cerebellopontine angle.
- Patient positioned lateral (park-bench) or supine with head rotation (lying flat on the back with the head turned to the side)
- Semi-sitting position may be used in selected centers
- Craniotomy performed behind the ear, posterior to the mastoid
- Cerebellum gently mobilized to expose the tumor
- Suitable for small, medium, and selected large tumors
- Hearing preservation may be possible depending on tumor size and preoperative hearing status
Translabyrinthine Approach
Preferred when hearing is already non-serviceable and hearing preservation is not possible.
- Most commonly performed by ENT (neuro-otologic/skull base) surgeons, often in collaboration with a neurosurgeon
- Patient positioned supine with head rotation (lying flat on the back with the head turned to the side)
- Incision made behind the ear
- The surgeon reaches the tumor by removing the inner ear structures located behind the ear. This gives the best access to safely separate the tumor from the facial nerve, but it means that any remaining hearing in that ear will be permanently lost.
- Provides direct exposure of the facial nerve along its course
- Often selected for larger tumors when facial nerve preservation is prioritized
Surgical Goals in Vestibular Schwannoma
The primary objectives of microsurgery are:
- Adequate tumor removal (complete when safely achievable)
- Relief of brainstem compression
- Preservation of facial nerve function
- Hearing preservation when anatomically and functionally feasible
In selected cases of very large tumors or when the lesion is densely adherent to critical neurovascular structures, a planned subtotal (debulking) resection may be performed to decompress the brainstem and preserve facial nerve function, followed by staged radiosurgery for the residual tumor.
Possible Complications of Microsurgical Removal of Vestibular Schwannoma
Microsurgical removal of vestibular schwannoma is a well-established procedure, but as with any cranial surgery, it carries potential risks. The type and likelihood of complications depend on tumor size, location, surgical approach, and preoperative nerve function.
• Facial nerve weakness or paralysis – temporary in many cases, but permanent weakness may occur, particularly with larger tumors. In rare cases of complete anatomical nerve disruption, early reconstructive procedures (such as hypoglossal–facial nerve anastomosis) may be considered to restore facial tone and function.
• Hearing loss – hearing preservation is not always possible and depends on tumor size, location, and preoperative hearing status.
• Balance disturbance – usually temporary due to central vestibular compensation.
• Cerebrospinal fluid (CSF) leak – may require additional treatment or, rarely, reoperation.
• Infection or meningitis – uncommon but possible.
• Bleeding or hematoma formation – rare but potentially serious.
• Hydrocephalus – may require temporary or permanent CSF diversion in selected cases.
• Very rarely, serious neurological deterioration or life-threatening complications.
Headache, after retrosigmoid approach, is usually related to muscle dissection in the suboccipital region, dural manipulation, and occipital nerve irritation. In most patients it gradually improves over time. If headache persists beyond the early recovery period, it is often managed according to the principles used for occipital neuralgia, including targeted physical therapy, medication for neuropathic pain, and, in selected cases, occipital nerve blocks.
In experienced skull base centers, permanent severe complications are uncommon, particularly for small to medium-sized tumors.
Request Vestibular Schwannoma (Acoustic Neuroma) Neurosurgery Consultation — 24-Hour Review or Priority Option (Usually Within 3 Hours)
When MRI confirms vestibular schwannoma (acoustic neuroma), patients often face complex decisions:
whether observation is still safe, when stereotactic radiosurgery (SRS) is appropriate, when microsurgery is recommended,
and how likely hearing and facial nerve function can be preserved in their specific case.
An independent neurosurgical second opinion can help you understand the situation clearly, confirm whether the proposed strategy is reasonable,
and explain what outcomes are realistic based on tumor size, growth behavior, hearing status, brainstem contact/mass effect, and your personal priorities.
- ✔ Send a short message describing your vestibular schwannoma diagnosis, symptoms (hearing loss, tinnitus, imbalance/vertigo, facial numbness), and what the MRI report says about tumor size and location (intracanalicular vs CPA extension)
- ✔ You’ll receive a reply within 24 hours explaining if and how we can help in your specific vestibular schwannoma situation
- ✔ Time-sensitive cases: if new neurological deficits develop, rapid tumor growth is reported, hydrocephalus is suspected, or doctors are urgently recommending surgery or radiation — write PRIORITY in your first message
- ✔ If available, MRI images (DICOM) and audiometry + ENT/neurosurgery notes can be reviewed once initial contact is established
- ✔ During the consultation, we clarify observation vs SRS vs microsurgery, expected hearing and facial nerve outcomes, timing, key risks, and realistic next steps — with up to 10 days of follow-up for brief questions
Consultation fees typically range from $180–250, depending on case complexity and imaging findings.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth second opinions in neurosurgery.
Facial Nerve and Hearing Outcomes After Surgery
Tumor size is the most important factor influencing facial nerve function and hearing outcomes after treatment. Outcomes also depend on baseline hearing, tumor anatomy, and treatment method (microsurgery or radiosurgery).
Tumors Under 2 cm
Microsurgery
- Facial nerve preservation is excellent. In experienced centers, more than 90–95% of patients maintain normal or near-normal facial movement (House–Brackmann Grade I–II).
- Hearing preservation is possible in selected patients with good preoperative hearing, typically ranging between approximately 40–70%, depending on tumor size, surgical approach, and baseline hearing quality.
Radiosurgery
- Long-term tumor control rates exceed 90–95%.
- Facial nerve injury is rare.
- Serviceable hearing may be preserved in roughly 40–70% of patients, although gradual hearing decline may occur over time despite tumor control.
Tumors 2–3 cm
As tumor size increases, preservation of hearing becomes significantly more difficult regardless of treatment method.
Microsurgery
- Facial nerve preservation remains achievable in most patients but surgical complexity increases.
- Hearing preservation rates decline substantially and are often limited, particularly as tumors approach 3 cm.
Radiosurgery
- May still be considered in selected tumors with minimal brainstem compression.
- Facial nerve preservation remains high, but hearing preservation becomes less predictable.
Specific Recommendations by Vestibular Schwannoma Size and Clinical Situation
Intracanalicular Tumors (Confined to the Internal Auditory Canal)
Tumors limited to the internal auditory canal are frequently detected during evaluation of unilateral hearing loss, but they may also be discovered incidentally on MRI performed for unrelated reasons such as headache, dizziness, or trauma assessment.
If no documented growth exists and hearing is stable, observation with serial MRI is usually appropriate.
If sustained growth is documented, stereotactic radiosurgery is most commonly recommended as the primary active treatment option because it provides high long-term tumor control with minimal facial nerve risk.
Microsurgery — typically via a middle fossa approach — may be considered in carefully selected younger patients with excellent baseline hearing when anatomical tumor removal and long-term durability are prioritized. However, this represents a more selective indication.
Hearing preservation rates are highest in this size category.
Small Tumors (Up to ~1.5–2 cm)
Small tumors extending into the cerebellopontine angle without significant brainstem displacement are frequently managed initially with observation if growth has not been documented.
When consistent growth is confirmed, stereotactic radiosurgery is generally the most common active treatment strategy because it offers high long-term tumor control, excellent facial nerve preservation rates, and a reasonable probability of maintaining serviceable hearing in selected patients with good baseline hearing.
Microsurgery may be considered in younger patients with good hearing when long-term anatomical removal is preferred, but it is not routinely required in all cases. Facial nerve preservation rates remain excellent. Hearing preservation is possible but depends strongly on baseline function and surgical expertise.
Medium Tumors (~2–3 cm)
Tumors measuring between approximately 2 and 3 cm represent a transitional decision zone.
Management depends primarily on:
- Degree of brainstem contact or displacement
- Documented growth pattern
- Hearing status
- Patient age
For tumors closer to 2 cm with minimal brainstem compression, radiosurgery may still be appropriate, particularly if growth is documented but neurological symptoms are limited. In this setting, tumor control rates are high, facial nerve preservation is excellent, and hearing may be preserved in a subset of patients, although gradual decline remains possible over time.
As tumor size approaches 2.5–3 cm, especially if there is clear brainstem displacement or progressive symptoms, the balance increasingly shifts toward microsurgical decompression. Hearing preservation rates decline significantly as tumor size approaches 3 cm, and surgical complexity increases.
Tumors measuring around 2.8 cm (28 mm) often represent a true decision window. At this size, management depends mainly on brainstem compression, documented growth, and current hearing status. Clear brainstem displacement or progressive symptoms more often favor microsurgery, while minimal compression and moderate growth may still allow consideration of radiosurgery in selected cases.
Large Tumors (>3 cm)
Tumors exceeding approximately 3 cm commonly produce brainstem compression and may affect facial or trigeminal nerve function.
In this size category, microsurgical removal is typically recommended because:
- Immediate decompression is required
- Radiosurgery does not relieve mass effect
- The risk of neurological deterioration increases
In large tumors, surgeons traditionally aim to remove the entire tumor when this can be done safely. However, if parts of the tumor are tightly attached to critical nerves or the brainstem, attempting complete removal may increase the risk of permanent neurological deficits. For this reason, some centers intentionally leave a small residual portion of tumor in these high-risk areas to protect neurological function, with radiosurgery later used to control the remaining tissue.
Hydrocephalus may develop in very large tumors and requires urgent evaluation and management.
Bilateral Tumors (Neurofibromatosis Type 2 – NF2)
In Neurofibromatosis Type 2 (NF2), vestibular schwannomas usually develop on both sides and often appear at a younger age than sporadic tumors.
Management differs fundamentally from typical unilateral vestibular schwannoma. Because tumors tend to grow throughout life and frequently become large enough to affect the brainstem, treatment planning focuses on long-term neurological function and preservation of usable hearing in at least one ear.
Unlike sporadic tumors, observation periods are often shorter in NF2. Tumors are commonly larger at the time of diagnosis or demonstrate continued growth, meaning that active treatment — most often surgery — eventually becomes necessary in many patients.
Microsurgical treatment is therefore performed more frequently than radiosurgery, particularly when tumors begin to compress the brainstem or threaten neurological function.
In many cases, the surgical goal is not complete tumor removal but safe reduction of tumor volume in order to:
- relieve brainstem compression
- preserve facial and lower cranial nerve function
- maintain hearing for as long as possible
After partial tumor removal, the remaining tumor may later be treated with stereotactic radiosurgery to achieve long-term control while minimizing neurological risk.
Because NF2 is a lifelong condition with repeated tumor growth, treatment is often staged over many years rather than performed as a single definitive procedure.
In selected patients, targeted medical therapy such as bevacizumab (a medication that blocks tumor blood vessel growth) may be used to slow tumor enlargement or help stabilize hearing, especially when surgery or radiation are not immediately suitable options.
Treatment timing is individualized and may prioritize intervention on the side with better hearing in order to prolong functional hearing, even if that tumor is not the largest.
Cystic Vestibular Schwannoma
Cystic tumors may show more rapid changes in size due to cyst expansion and can produce earlier mass effect compared with purely solid tumors.
During surgery, cystic components can make resection technically more complex. The cyst wall may be thin or irregular and may adhere to surrounding cranial nerves or vascular structures. This does not automatically imply worse outcomes, but it can increase operative difficulty.
Radiosurgery is sometimes less predictable in predominantly cystic tumors, as cyst volume may fluctuate. For this reason, microsurgical treatment is often favored when significant cystic features and mass effect are present.
Tumor with Hydrocephalus
Hydrocephalus may develop in larger tumors due to compression of the fourth ventricle or obstruction of cerebrospinal fluid pathways.
When hydrocephalus is symptomatic, urgent treatment is required. In many cases, removal of the tumor itself restores normal cerebrospinal fluid circulation and resolves the hydrocephalus.
If immediate pressure relief is necessary before definitive tumor surgery, a temporary external ventricular drain (EVD) may be placed.
Permanent ventriculoperitoneal (VP) shunting is less commonly required and is usually reserved for cases in which hydrocephalus persists after adequate tumor removal. A VP shunt is a surgically implanted drainage system (tubes) that diverts excess cerebrospinal fluid from the brain’s ventricles into the abdominal cavity, where it can be absorbed. In selected situations, a VP shunt may also be placed before tumor surgery if hydrocephalus is severe and definitive tumor removal cannot be performed promptly in a specialized center. However, when timely microsurgical treatment is feasible, tumor removal alone often restores normal cerebrospinal fluid circulation and eliminates the need for permanent shunting.
Vestibular Schwannoma Recurrence and Follow-Up After Treatment
After treatment of vestibular schwannoma — whether by observation, radiosurgery, or microsurgery — long-term follow-up with MRI is necessary.
Vestibular schwannoma may remain stable for many years, but in some patients tumor growth or regrowth can occur.
The meaning of “recurrence” depends on the type of previous treatment:
After observation, tumor growth may eventually be detected during follow-up imaging and does not represent treatment failure, but rather natural tumor behavior.
After radiosurgery, the tumor usually does not disappear. The goal of treatment is growth control. Mild enlargement during the first 1–2 years may represent temporary treatment-related swelling rather than true progression. True regrowth requiring further treatment occurs in a small percentage of patients over long-term follow-up.
After microsurgical removal, recurrence risk depends on how much tumor was safely removed. Complete removal carries a low but not zero risk of recurrence, while intentionally leaving a small residual portion to protect critical nerves may require later monitoring or additional treatment.
Management of regrowth depends on:
- tumor growth rate
- size of residual tumor
- brainstem compression
- hearing and facial nerve function
- previous treatment strategy
In many cases, small regrowth can be effectively controlled with stereotactic radiosurgery, avoiding repeat open surgery. When tumor progression occurs several years after previous radiosurgery (commonly delivered with a marginal dose around 12 Gy), repeat radiosurgery may be considered in carefully selected patients if the tumor remains relatively small and does not cause significant brainstem compression. During repeat treatment, radiation planning takes into account the previously delivered dose, tumor location, and proximity to critical nerves and the brainstem. A second radiosurgical procedure is typically performed using adjusted dosing in order to maintain tumor control while minimizing the cumulative risk to surrounding neural structures.
Repeat microsurgery is usually reserved for larger or symptomatic recurrences causing compression or neurological deterioration.
Because vestibular schwannoma typically grows slowly, treatment decisions after recurrence are usually planned carefully rather than performed urgently, unless brainstem compression or progressive neurological symptoms develop.
Histopathology of Vestibular Schwannoma
Classic benign histology includes:
- Antoni A and Antoni B patterns
- Verocay bodies
Vestibular schwannoma is classified as a WHO grade 1 tumor in the vast majority of cases. Malignant transformation is extremely rare.
Histopathological findings generally confirm the diagnosis but do not usually alter primary treatment strategy, which is determined mainly by tumor size, growth behavior, symptoms, and anatomical relationships. However, in rare atypical or malignant variants, more aggressive management and closer follow-up may be required.
Long-term Outcomes and Prognosis of Vestibular Schwannoma
Observation:
- ~30–50% require later intervention.
Radiosurgery:
- 90–99% tumor control at 5 years.
Microsurgery:
- Excellent tumor control.
- Functional outcome depends strongly on size and center experience.
Why Specialist Opinions May Differ in Vestibular Schwannoma Management
Differences in specialist recommendations do not necessarily indicate that one opinion is wrong. In vestibular schwannoma management, treatment strategy may vary depending on how a physician weighs tumor size (for example, tumors measuring 2–3 cm), documented growth rate, baseline hearing quality, patient age, surgical philosophy, institutional experience, and the balance between hearing preservation and long-term tumor control.
In many patients, the diagnosis itself is clear, but the decision about treatment is not. When recommendations differ regarding observation versus intervention, timing of surgery, suitability for radiosurgery, or the likelihood of preserving hearing or facial nerve function, an independent neurosurgical second opinion can help clarify which strategy best fits the specific anatomical situation, risk profile, and long-term priorities.
These differences become most visible in specific clinical decisions that patients frequently face:
Is It Safe to Wait or Should Treatment Be Started?
In small or slowly growing tumors, observation may be a reasonable strategy. However, some specialists recommend earlier intervention to prevent future growth or hearing decline. The same MRI finding may therefore lead to different recommendations depending on how risk is interpreted and how much importance is given to potential long-term changes.
Should I Choose Radiosurgery or Microsurgery?
Radiosurgery is often preferred for smaller tumors without significant brainstem compression, while microsurgery is more commonly recommended for larger lesions or those causing neurological symptoms. In intermediate cases, both options may be considered acceptable, and differences in experience and institutional preference may influence the recommendation.
What Should Be Done When the Tumor Is 2–3 cm?
Tumors in the 2–3 cm range often represent a true decision boundary. Some specialists favor radiosurgery if brainstem compression is minimal, while others recommend surgery before further growth increases technical complexity and the risk of functional impairment.
Can Hearing Be Preserved or Is Tumor Control More Important?
When hearing is still functional, treatment decisions become more complex. Some specialists prioritize preserving hearing for as long as possible, while others emphasize long-term tumor control, even if hearing preservation becomes less likely over time.
Is It Riskier to Operate Now or to Wait?
Decisions often involve balancing the immediate risks of surgery against the long-term risks of tumor growth. Some specialists prioritize avoiding neurological deficits, while others recommend earlier intervention to reduce the chance of future complications or more complex treatment.
Frequently Asked Questions About Vestibular Schwannoma
Is vestibular schwannoma cancer or a benign tumor?
Vestibular schwannoma is usually a benign WHO grade 1 tumor, not cancer in the usual sense. It arises from Schwann cells of the eighth cranial nerve, most often the vestibular part responsible for balance. It does not spread through the body like malignant cancer. However, “benign” does not always mean harmless. Its importance comes from its location in the internal auditory canal and cerebellopontine angle, close to the hearing nerve, facial nerve, trigeminal nerve, cerebellum, brainstem, and cerebrospinal fluid pathways. If it grows, it may cause hearing loss, tinnitus, imbalance, facial numbness, facial weakness, brainstem compression, or hydrocephalus. Treatment decisions therefore depend on size, growth, hearing, symptoms, and anatomical risk.
What is usually the first symptom of vestibular schwannoma?
The most common persistent early symptom of vestibular schwannoma is unilateral hearing loss, meaning hearing decline on one side. Tinnitus, or ringing in one ear, may also occur. Some patients initially experience imbalance, mild vertigo, nausea, or unsteadiness because the tumor usually arises from the vestibular branch of the eighth cranial nerve. However, balance symptoms may improve within weeks because the brain can compensate for the gradually reduced vestibular signal. This can delay diagnosis. Hearing loss may appear slowly over months or years, and even small intracanalicular tumors can affect hearing. For this reason, asymmetric sensorineural hearing loss is an important red flag that often leads to MRI with contrast.
Can dizziness from vestibular schwannoma disappear even while the tumor continues to grow?
Yes. Dizziness or imbalance from vestibular schwannoma can improve even if the tumor remains present or continues to grow slowly. This happens because the tumor often affects the vestibular nerve gradually, and the brain may adapt through central vestibular compensation. A patient may have early vertigo, nausea, unsteadiness, or imbalance, and then feel better after several weeks. This improvement can create the false impression that the problem has resolved. Meanwhile, hearing loss or tinnitus may persist and become the dominant symptom. If the tumor later becomes larger, additional problems such as worsening imbalance, facial numbness, facial weakness, brainstem compression, or hydrocephalus may appear. This is why unilateral hearing symptoms should not be ignored.
Why is unilateral hearing loss considered an important warning sign for vestibular schwannoma?
Unilateral hearing loss is an important warning sign for vestibular schwannoma because the tumor develops from the eighth cranial nerve, which carries hearing and balance information from the inner ear to the brain. The hearing loss is usually sensorineural and asymmetric, meaning one ear performs worse than the other because the nerve pathway is affected. Audiometry may show a significant difference between ears, and one commonly used MRI referral threshold is a 15 dB difference at 3 kHz. Vestibular schwannoma may also cause unilateral tinnitus. Because balance symptoms may improve through compensation, hearing loss may be the most reliable persistent early clue. MRI with and without gadolinium contrast is the gold standard for confirming the diagnosis.
Do all vestibular schwannomas grow over time?
No. Not all vestibular schwannomas grow over time. Many small, sporadic tumors remain stable for years and may never require active treatment. Studies show that approximately 40–60% of small sporadic vestibular schwannomas remain stable long-term, while about 30–50% demonstrate measurable growth during follow-up. Even when growth occurs, it may be slow, often around 1–2 mm per year, and some tumors may later stabilize again. This is why observation, or wait-and-scan management, is often appropriate for small tumors with minimal symptoms and no documented growth. Treatment is usually considered when growth is sustained, clinically significant, associated with worsening symptoms, or when tumor size begins to threaten hearing, facial nerve function, or the brainstem.
How fast does vestibular schwannoma usually grow?
Vestibular schwannoma growth is variable. In tumors that grow, the average growth rate is often around 1–2 mm per year, but some tumors may grow faster, approximately 3–4 mm per year, especially if early progression is documented. Other tumors remain stable for many years or stop growing after an initial period of enlargement. Small differences of 1–2 mm on a single MRI may sometimes reflect measurement variation rather than true progression, so doctors usually look for consistent growth across serial scans. If a vestibular schwannoma remains stable for about five years or longer, the likelihood of later significant growth becomes lower. Growth rate is important because it influences whether observation, radiosurgery, or microsurgery is recommended.
Can vestibular schwannoma remain stable for many years without treatment?
Yes. Vestibular schwannoma can remain stable for many years without active treatment, especially when it is small, sporadic, and discovered during evaluation of hearing loss or incidentally on MRI. Observation is commonly used because a substantial proportion of tumors do not grow or grow only minimally. Long-term studies suggest that if a vestibular schwannoma remains stable for five years or longer, later significant growth becomes less likely. This is particularly reassuring in older patients with longstanding stable hearing loss and unchanged tumor size. However, stability does not mean follow-up can be abandoned completely. Periodic MRI is still recommended, and earlier imaging is needed if new symptoms appear, such as worsening imbalance, facial numbness, facial weakness, or hydrocephalus signs.
When is observation (wait-and-scan) appropriate for vestibular schwannoma?
Observation is appropriate for vestibular schwannoma when the tumor is small, usually under about 1.5–2 cm, symptoms are minimal, growth has not been documented, hearing is already poor or stable, or patient factors such as age and medical condition favor a conservative approach. Observation is also reasonable when slight MRI change is not clearly progressive or clinically important. Follow-up MRI is usually performed annually during the first five years, because most growth or treatment-related decisions occur during that period. If the tumor remains stable, intervals may later be extended. Observation is not passive neglect. It is an active strategy that monitors tumor growth, hearing status, neurological symptoms, and the need for later radiosurgery or microsurgery.
How do doctors decide between observation, radiosurgery, and microsurgery for vestibular schwannoma?
Doctors decide between observation, radiosurgery, and microsurgery for vestibular schwannoma by considering tumor size, documented growth, hearing status, age, symptoms, brainstem contact, hydrocephalus, NF2 status, and patient priorities. Small stable tumors with minimal symptoms are often monitored. Small to medium-sized growing tumors, generally up to about 2.5–3 cm without significant brainstem compression, may be suitable for stereotactic radiosurgery. Larger tumors, especially above 3 cm, tumors causing brainstem compression, hydrocephalus, cystic enlargement, progressive neurological symptoms, or significant mass effect more often require microsurgical removal. The decision becomes especially difficult in the 2–3 cm range, where both radiosurgery and surgery may be considered depending on compression, growth, and hearing.
When is stereotactic radiosurgery recommended for vestibular schwannoma?
Stereotactic radiosurgery is usually recommended for vestibular schwannoma when the tumor is small to medium-sized, shows sustained documented growth, and does not cause significant brainstem compression or hydrocephalus. It is commonly considered for tumors up to about 2.5–3 cm when the goal is long-term tumor control rather than immediate removal. Radiosurgery may also be appropriate when hearing is declining during observation, when the patient prefers a non-surgical approach, or when surgery carries increased risk. The usual marginal dose is around 12–13 Gy. Tumor control rates are high, often above 90% at five years, and facial nerve preservation is usually excellent. However, radiosurgery does not decompress large tumors and does not remove the mass.
Can radiosurgery for vestibular schwannoma preserve hearing?
Radiosurgery for vestibular schwannoma can preserve serviceable hearing in some patients, but hearing preservation is not guaranteed. Outcomes depend strongly on baseline hearing, tumor size, tumor location, radiation dose planning, and follow-up duration. In small tumors, serviceable hearing preservation after radiosurgery is often reported around 40–70%, but gradual hearing decline can still occur over time despite tumor control. Radiosurgery is very effective at stopping or slowing tumor growth, but it does not reverse nerve damage that has already occurred. Hearing preservation is most realistic when the tumor is small, baseline hearing is good, and there is no major brainstem compression. In larger tumors, hearing preservation becomes less predictable regardless of treatment method.
When does vestibular schwannoma usually require microsurgery?
Vestibular schwannoma usually requires microsurgery when the tumor is large, generally above about 3 cm, causes brainstem compression, produces significant mass effect, leads to hydrocephalus, grows progressively, or causes neurological symptoms that require decompression. Microsurgery may also be chosen when the patient prefers definitive removal, even for smaller tumors, after understanding the risks and alternatives. The main goals are adequate tumor removal, relief of brainstem compression, preservation of facial nerve function, and hearing preservation when feasible. Surgery is performed in specialized skull base centers with facial nerve monitoring and, in selected cases, auditory brainstem monitoring. For very large tumors adherent to critical nerves or brainstem, planned subtotal resection may be safer than aggressive complete removal.
What happens if vestibular schwannoma becomes larger than 3 cm?
When vestibular schwannoma becomes larger than about 3 cm, the risk profile changes. Large tumors commonly extend from the internal auditory canal into the cerebellopontine angle and may compress the brainstem, facial nerve, trigeminal nerve, cerebellum, and cerebrospinal fluid pathways. Symptoms may include worsening imbalance, facial numbness, facial weakness, gait disturbance, hydrocephalus, or signs of brainstem compression. Radiosurgery is usually less suitable for large tumors because it does not provide immediate decompression and swelling after radiation could worsen mass effect. Microsurgical removal is more commonly recommended. In selected very large tumors, surgeons may intentionally leave a small residual portion attached to critical nerves or brainstem to preserve function, followed later by staged radiosurgery if needed.
Can vestibular schwannoma cause facial weakness or trigeminal symptoms?
Yes. Vestibular schwannoma can cause facial weakness or trigeminal symptoms when it becomes large enough to compress nearby cranial nerves in the cerebellopontine angle. The facial nerve runs very close to the tumor, especially in the internal auditory canal, and may be stretched or compressed as the tumor enlarges. This can lead to facial weakness, although this is more common in larger tumors or after treatment than as an early symptom. Trigeminal nerve compression may cause facial numbness, altered facial sensation, or sometimes trigeminal neuralgia-like pain. These symptoms suggest that the tumor is no longer affecting only hearing and balance pathways. Their presence often increases concern about tumor size, brainstem contact, and the need for active treatment.
Is hearing preservation realistic after vestibular schwannoma treatment?
Hearing preservation after vestibular schwannoma treatment is realistic only in selected patients. The best chances occur when the tumor is small, hearing is still serviceable before treatment, and the anatomy is favorable. In tumors under 2 cm, hearing preservation may be possible with either microsurgery or radiosurgery, but results vary widely and gradual decline may still occur. As tumors approach 2.5–3 cm, hearing preservation becomes much less predictable. If hearing is already non-serviceable, approaches such as translabyrinthine surgery may be used because preserving hearing is no longer possible, while facial nerve preservation becomes the main functional goal. Patients should understand that tumor control, facial nerve function, and hearing preservation may compete with one another in treatment planning.
Why may specialists recommend different treatments for the same vestibular schwannoma?
Specialists may recommend different treatments for the same vestibular schwannoma because management depends on how tumor size, growth, hearing, age, brainstem contact, symptoms, and patient priorities are weighted. A small stable tumor may be observed by one team, while another may recommend early radiosurgery if growth risk or hearing decline is emphasized. In tumors measuring 2–3 cm, one specialist may favor radiosurgery if compression is minimal, while another may recommend surgery before further growth increases risk. If hearing is still serviceable, decisions become even more complex because hearing preservation and long-term tumor control may pull treatment in different directions. These differences usually reflect genuine clinical gray zones, not simple right-versus-wrong recommendations.
What is Neurofibromatosis Type 2 (NF2) and how does it change vestibular schwannoma treatment?
Neurofibromatosis Type 2, or NF2, is a rare genetic condition strongly associated with bilateral vestibular schwannomas, meaning tumors on both sides. NF2 is different from typical sporadic vestibular schwannoma. Patients are often younger and may develop multiple nervous system tumors, including schwannomas, meningiomas, and spinal tumors. Treatment planning focuses on lifelong function, especially preserving useful hearing in at least one ear for as long as possible. Observation periods may be shorter because tumors often continue to grow over time. Surgery is commonly needed when brainstem compression or neurological risk appears, but the goal may be planned partial reduction rather than complete removal. In selected patients, bevacizumab may help slow tumor growth or stabilize hearing.
Are cystic vestibular schwannomas more difficult to treat?
Cystic vestibular schwannomas can be more difficult to treat in some patients because their size may change more rapidly due to cyst expansion. This can produce earlier mass effect than a similarly sized solid tumor. During surgery, cystic components may make the dissection more complex because the cyst wall can be thin, irregular, and adherent to surrounding cranial nerves or vessels. This does not automatically mean the outcome will be worse, but it may increase technical difficulty. Radiosurgery may also be less predictable in predominantly cystic tumors because cyst volume can fluctuate. For that reason, microsurgical treatment is often favored when cystic vestibular schwannoma produces significant mass effect, brainstem compression, or progressive symptoms.
Can vestibular schwannoma cause hydrocephalus and require urgent treatment?
Yes. A large vestibular schwannoma can cause hydrocephalus by compressing the fourth ventricle or blocking cerebrospinal fluid pathways. When fluid cannot circulate normally, pressure may build inside the brain’s ventricles. Symptoms can include worsening headache, vomiting, drowsiness, gait disturbance, confusion, or neurological deterioration. Symptomatic hydrocephalus requires urgent evaluation. In many cases, removing the tumor restores cerebrospinal fluid circulation and resolves the hydrocephalus. If pressure relief is needed before definitive tumor surgery, an external ventricular drain may be placed temporarily. A permanent ventriculoperitoneal shunt is less commonly required and is usually reserved for cases where hydrocephalus persists after adequate tumor removal or when surgery cannot be performed promptly.
Can vestibular schwannoma treatment improve tinnitus or make it worse?
Tinnitus outcomes after vestibular schwannoma treatment are variable and depend on tumor size, baseline hearing, nerve function, and treatment type. Some patients experience improvement or reduced intensity of tinnitus after microsurgery or stereotactic radiosurgery, particularly if the symptom was directly related to tumor-related nerve irritation. However, tinnitus may also remain unchanged despite successful tumor control, and in some cases it can worsen or newly appear after treatment. This is because treatment aims primarily to control the tumor and preserve neurological function rather than directly eliminate tinnitus. Hearing preservation is an important factor, as tinnitus often correlates with hearing loss. Patients considering treatment should therefore understand that tumor control, facial nerve preservation, and hearing outcomes are usually more predictable than tinnitus response itself.
What are the specific risks and complications of the retrosigmoid approach for vestibular schwannoma?
The retrosigmoid approach provides access to tumors extending into the cerebellopontine angle and may offer a possibility of hearing preservation in selected patients. Its specific risks include hearing deterioration or complete hearing loss, facial nerve weakness, balance disturbance, cerebrospinal fluid leakage, infection, bleeding, cerebellar swelling or injury, and, particularly in large tumors, injury to the brainstem or lower cranial nerves responsible for swallowing and voice function.
Postoperative suboccipital headache and occipital neuralgia are especially relevant to this approach. Pain may result from suboccipital muscle dissection, dural scarring, or irritation or injury of the greater or lesser occipital nerves. Occipital neuralgia typically causes sharp, burning, or electric-shock-like pain extending from the back of the head toward the scalp or behind the ear. Persistent pain may require medication for neuropathic pain, targeted physical therapy, an occipital nerve block, or rarely further intervention. When surgery is performed in the semi-sitting position, there is also a specific risk of venous air embolism. More information is available on our occipital neuralgia and occipital headache page.
What are the specific risks and complications of the translabyrinthine approach for vestibular schwannoma?
The translabyrinthine approach passes through the inner-ear structures and therefore results in complete and permanent loss of any remaining hearing in the operated ear. It is generally selected when hearing is already non-serviceable or when direct exposure of the facial nerve is considered more important than attempting hearing preservation.
Other possible complications include temporary or permanent facial nerve weakness, imbalance while the brain adapts to loss of vestibular function on the operated side, cerebrospinal fluid leakage through the wound, mastoid air cells, middle ear, or nose, meningitis, wound infection, bleeding, and rarely injury to the sigmoid sinus or jugular bulb. Some patients may also experience persistent tinnitus or altered sensation around the ear. The likelihood of complications depends on tumor size, facial nerve adherence, previous hearing and balance function, and the experience of the skull-base surgical team.
What are the specific risks and complications of the middle fossa approach for vestibular schwannoma?
The middle fossa approach is mainly used for small intracanalicular tumors when preservation of useful hearing is an important goal. However, hearing may still deteriorate or be completely lost because of injury to the cochlear nerve, labyrinthine artery, or delicate blood supply of the inner ear. Temporary or permanent facial nerve weakness may also occur because the facial nerve lies close to the operative corridor within the internal auditory canal.
This approach requires elevation of the temporal lobe and therefore carries specific risks of temporal lobe swelling, contusion, venous injury, postoperative hematoma, or seizures. When performed on the dominant side, rare complications may include speech, memory, or other cognitive disturbances. Cerebrospinal fluid leakage, infection, meningitis, balance disturbance, and headache are also possible. The suitability of this approach depends on tumor size, its position within the internal auditory canal, preoperative hearing quality, patient age, and the surgeon’s experience with hearing-preservation surgery.
Can an online second opinion help clarify vestibular schwannoma treatment decisions?
Yes. An online second opinion can help clarify vestibular schwannoma treatment decisions when observation, radiosurgery, or microsurgery are all being considered, or when specialists give different recommendations. It is especially useful when the tumor is growing, hearing is still serviceable, tumor size is between 2 and 3 cm, radiosurgery has been proposed, surgery has been recommended, or brainstem contact, facial nerve risk, hydrocephalus, cystic features, NF2, or bilateral tumors make planning more complex. MRI images, audiometry, ENT and neurosurgery notes, and symptom history can be reviewed to assess tumor size, growth behavior, hearing status, brainstem compression, facial nerve risk, and realistic outcomes. The goal is to clarify timing, treatment choice, and expected functional results.