Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Thoracic Outlet Syndrome — Compression of the Brachial Plexus and Subclavian Vessels
Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
May 08, 2026
Who This Thoracic Outlet Syndrome Page Is For
This page is intended for patients who experience pain, numbness, tingling, or weakness in the arm or hand, especially when thoracic outlet syndrome has been suspected or previously discussed during medical evaluation.
If symptoms appear during overhead arm activity, prolonged arm elevation, or certain shoulder positions — or if previous examinations have suggested possible compression of the brachial plexus nerves or nearby blood vessels between the neck and shoulder — understanding the potential causes, diagnostic process, and treatment options may help guide further medical decisions. In complex or persistent cases, an individualized neurosurgical second opinion may help clarify the diagnosis and determine the most appropriate management strategy.
When patients seek a second opinion for thoracic outlet syndrome
• Persistent pain, numbness, or tingling in the arm or hand
• Weakness of the hand or reduced grip strength during arm activity
• Symptoms worsen when the arm is elevated, during overhead activity, or after prolonged use of the arm
• It is unclear whether symptoms originate from thoracic outlet compression, cervical spine disorders, or another nerve compression syndrome
• Conservative treatment or physiotherapy has not improved symptoms over several months
• Uncertainty whether surgical decompression of the thoracic outlet should be considered
If your symptoms persist or the diagnosis and treatment options remain unclear, you may request an individualized neurosurgical review here:
Request Second Opinion
Contents
- Who this page is for
- Definition
- Thoracic outlet anatomy
- Causes of compression
- Symptoms
- Diagnosis
- Similar conditions
- Operate or not
- Conservative treatment
- Surgical treatment
- Surgical risks
- Symptoms after surgery
- Contributing factors
- Re-evaluation
- Prognosis and recovery
- Specialist evaluation
- Request second opinion
- FAQs
What Is Thoracic Outlet Syndrome
Thoracic outlet syndrome is a condition caused by compression of nerves or blood vessels in the region between the neck and shoulder.
This area, known as the thoracic outlet, is the passage through which the brachial plexus, subclavian artery, and subclavian vein travel from the neck into the arm. When these structures become compressed, patients may develop symptoms affecting the arm, shoulder, and hand.
The most common form is neurogenic thoracic outlet syndrome, which involves compression of the brachial plexus. Less common forms include venous thoracic outlet syndrome and arterial thoracic outlet syndrome, which involve compression of the subclavian vessels.
Thoracic outlet syndrome most commonly affects adults between 20 and 50 years of age, occurs more frequently in women.
Read more about nerve injuries and other nerve entrapments on this page: https://neurohirurgija.in.rs/en/peripheral-nerve-injury/
Anatomy of the Thoracic Outlet
The thoracic outlet is formed by several anatomical structures located between the neck and the shoulder, creating a passage through which important nerves and blood vessels travel toward the arm.
Important anatomical components include:
• the first rib, the clavicle (collarbone) and the costoclavicular space
• the scalene muscles
• the pectoralis minor muscle region
Through these relatively narrow spaces pass the brachial plexus nerves and the subclavian artery and vein, which supply the arm.
Compression may occur at several levels, including:
• between the scalene muscles (in the interscalene triangle)
• between the clavicle and the first rib (the costoclavicular space)
• beneath the pectoralis minor tendon
Because these anatomical corridors are naturally narrow, certain anatomical variations, muscular tightness, or repetitive overhead arm movements may increase pressure on the nerves or blood vessels and lead to symptoms of thoracic outlet syndrome.
More about nerve anatomy can be found on this page.
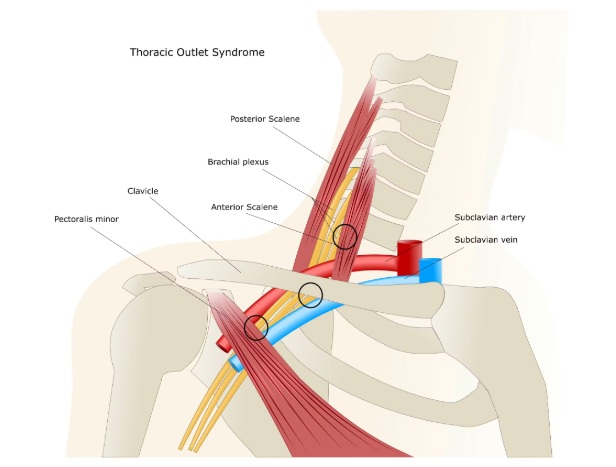
Image: The thoracic outlet consists of three distinct anatomical spaces (marked with circles on the image): the interscalene triangle between the scalene muscles, the costoclavicular space between the first rib and clavicle, and the sub-pectoralis minor space. Compression or irritation of the neurovascular bundle within any of these regions—often due to muscular abnormalities, a first rib anomaly, or a cervical rib—can lead to Thoracic Outlet Syndrome (TOS).
Why Thoracic Outlet Syndrome Develops
Several factors may contribute to compression of the brachial plexus or the subclavian vessels in the thoracic outlet region.
Common causes include:
• Congenital anatomical variations, such as a cervical rib
• Hypertrophy or tightness of the scalene muscles
• Repetitive overhead arm activity (sports, manual work)
• Previous trauma to the neck or shoulder
• Poor posture with forward shoulder position
• Fibrous bands compressing the brachial plexus
• Clavicle fractures or structural abnormalities
In many patients, symptoms develop due to a combination of anatomical predisposition and repetitive mechanical stress.
Symptoms of Thoracic Outlet Syndrome
Symptoms depend on whether nerves or blood vessels are primarily affected.
Common symptoms include:
• Pain in the neck, shoulder, or arm
• Numbness or tingling in the arm or hand
• Weakness of the hand or reduced grip strength
• Arm fatigue during overhead activity
• Coldness or color changes in the hand (in vascular forms)
• Swelling of the arm in venous compression
In neurogenic thoracic outlet syndrome, symptoms usually follow the distribution of the lower brachial plexus nerves. Compression affecting different parts of the brachial plexus may produce different symptom patterns. Upper plexus involvement may cause pain in the neck, shoulder, or upper arm, while lower plexus compression more commonly affects the forearm, hand, and fourth or fifth fingers.
Venous thoracic outlet syndrome may present with sudden swelling, heaviness, cyanosis, or visible superficial veins of the arm due to compression or thrombosis of the subclavian vein, particularly after repetitive overhead arm activity. Arterial thoracic outlet syndrome is the least common but potentially most serious form, because compression of the subclavian artery may lead to reduced blood flow, embolization, or ischemic complications affecting the arm or hand.
How Thoracic Outlet Syndrome Is Diagnosed
Diagnosis begins with clinical examination and careful evaluation of symptoms.
During examination, the doctor may identify:
• Reproduction of symptoms during arm elevation
• Weakness of hand muscles
• Sensory changes in the arm or hand
• Postural abnormalities affecting the shoulder girdle
• Changes in the radial pulse during certain arm positions
• Reduced or asymmetric pulses suggesting possible vascular compression
Additional tests may include:
• Nerve conduction studies (EMG) to evaluate the function of the brachial plexus and help distinguish thoracic outlet syndrome from other nerve compression disorders
• Chest or cervical spine X-rays to identify anatomical abnormalities, including cervical ribs or clavicle abnormalities, that may contribute to thoracic outlet compression
• Doppler ultrasound to assess blood flow in the subclavian artery and vein and detect possible vascular compression during certain arm positions
• Ultrasound examination to visualize vascular structures and identify dynamic compression of the vessels or surrounding soft tissues
• MRI of the cervical spine and brachial plexus to evaluate possible nerve compression and exclude other conditions such as cervical disc disease or structural abnormalities
• CT angiography or MR angiography and venography, in suspected vascular forms of thoracic outlet syndrome to provide detailed imaging of the arteries and veins and confirm the exact location of compression
These investigations help confirm the diagnosis and exclude other conditions. Some patients develop objective neurological abnormalities detectable on EMG studies (“true” neurogenic thoracic outlet syndrome), while others may experience typical symptoms despite less clear electrophysiological findings.
Thoracic outlet syndrome remains a clinically complex diagnosis because symptoms may overlap with cervical spine disorders, peripheral nerve entrapments, or shoulder pathology, and no universally accepted diagnostic standard currently exists.
Conditions That Can Mimic Thoracic Outlet Syndrome
Several disorders may produce symptoms similar to thoracic outlet syndrome.
These include:
• Cervical radiculopathy caused by cervical disc disease
• Cubital tunnel syndrome and Guyon canal syndrome
• Carpal tunnel syndrome
• Peripheral neuropathy
• Shoulder joint disorders
• Brachial plexus injury
• Tumors or other structural lesions near the thoracic outlet that may compress the brachial plexus or nearby vessels and mimic thoracic outlet syndrome symptoms
Careful clinical evaluation usually allows these conditions to be distinguished.
When Is Surgery Necessary in Thoracic Outlet Syndrome — Continue Conservative Treatment or Operate?
In many patients, the key question is whether symptoms will improve with continued conservative treatment, particularly physiotherapy and postural correction, or whether surgical decompression of the thoracic outlet is needed.
When symptoms are mild or improving, especially when pain, numbness, or weakness decrease with structured physiotherapy, continued non-surgical treatment is usually appropriate.
Surgery becomes more likely when symptoms are persistent over time, when neurological deficits such as weakness or reduced hand function progress, or when findings suggest ongoing compression of the brachial plexus or subclavian vessels.
The most important factor is timing — performing surgery too early may not be necessary in milder cases, while delaying surgery in more severe or prolonged compression may reduce the chance of functional recovery and symptom resolution.
Because this decision depends on symptom progression, severity, and clinical findings, different specialists may reasonably recommend either continued conservative treatment or surgical decompression based on how these factors are interpreted in an individual case.
Conservative Treatment
Many patients improve with non-surgical treatment.
Common approaches include:
• Postural correction
• Physiotherapy focused on shoulder girdle stabilization
• Stretching of the scalene and pectoralis muscles
• Activity modification
• Pain medications
• Medications for neuropathic pain
• Injection therapy involving local anesthetics, corticosteroids, or botulinum toxin in selected patients, which may provide temporary symptom relief and occasionally help clarify whether muscular compression contributes to symptoms
• Anticoagulation therapy, thrombolysis, or vascular surgical management in vascular forms of thoracic outlet syndrome associated with thrombosis, in addition to decompression procedures
In many patients, conservative treatment including physiotherapy and postural correction is continued for several months before surgical decompression is considered.
Surgical Treatment in Persistent Cases
Surgery may be considered when symptoms remain severe or progressive despite conservative treatment.
The most common procedures include:
• First rib resection
• Scalenectomy (removal of the scalene muscles)
• Removal of fibrous bands compressing the brachial plexus
Surgical treatment is usually recommended when there is:
• persistent neurological deficit
• severe vascular compression
• failure of prolonged conservative therapy
Possible Complications and Surgical Risks
Surgical decompression for thoracic outlet syndrome is generally reserved for selected patients with persistent neurological deficits or significant vascular compression. Although surgery may improve symptoms in appropriately selected cases, it is a technically demanding procedure performed near important nerves and blood vessels, and certain complications may occur.
These may include:
Wound healing problems (dehiscence)
In some patients, healing of the surgical incision may be delayed or incomplete, particularly after extensive dissection around the shoulder girdle or first rib.
Infection
Postoperative infection is uncommon but may require additional treatment if it occurs.
Injury to the brachial plexus or surrounding nerves
Because surgery is performed close to the brachial plexus and nearby peripheral nerves, temporary or persistent neurological symptoms may occasionally occur, including numbness, weakness, or neuropathic pain.
Residual or persistent symptoms
In some patients, pain, numbness, or weakness may persist despite technically successful decompression. This may occur when long-standing nerve irritation, overlapping diagnoses, or additional pain mechanisms are present.
Vascular complications
In vascular forms of thoracic outlet syndrome, surgical procedures performed near the subclavian artery or vein may rarely lead to bleeding, thrombosis, or vascular injury.
Scar-related discomfort and shoulder stiffness
Some patients may experience discomfort around the surgical site, shoulder stiffness, or limited mobility during postoperative recovery.
Although most complications are uncommon, it is important to distinguish true surgical complications from more frequent causes of persistent symptoms, such as prolonged nerve compression before surgery, incomplete functional recovery of the brachial plexus, or coexisting cervical spine disorders.
Why Symptoms May Persist After Thoracic Outlet Surgery
In some patients, pain, numbness, weakness, or arm fatigue may persist even after technically successful thoracic outlet decompression. This does not necessarily mean that surgery was unsuccessful. In many cases, decompression adequately relieves pressure on the brachial plexus or subclavian vessels, but pain and other symptoms continue because the dominant mechanism responsible for symptoms has not been fully resolved or because additional contributing factors remain active.
Successful recovery depends not only on decompression itself, but also on determining whether long-standing nerve irritation, cervical spine pathology, muscular dysfunction, or chronic pain mechanisms continue to influence symptoms after surgery.
Unrecognized Alternative or Overlapping Diagnoses
Several disorders may mimic thoracic outlet syndrome or coexist with it. These conditions are outlined in the section “Conditions That Can Mimic Thoracic Outlet Syndrome.”
If another neurological or orthopedic condition is also present — such as cervical radiculopathy, peripheral nerve entrapment, or shoulder pathology — decompression of the thoracic outlet alone may not fully resolve symptoms.
Double Crush Syndrome and Multi-Level Nerve Involvement
In some patients, the same nerve pathway may be affected at more than one anatomical level. For example, cervical nerve root compression may coexist with brachial plexus compression within the thoracic outlet.
If only one site of compression is treated, symptoms may improve only partially despite technically successful surgery.
Pre-existing Nerve Damage and Recovery Limitations
When compression of the brachial plexus has been present for a prolonged period, chronic structural and functional changes of the nerves may already have developed.
In such cases, improvement after decompression may remain slow or incomplete because recovery potential becomes limited over time.
Scar Tissue and Local Postoperative Factors
In some patients, postoperative fibrosis or scar tissue may develop around the brachial plexus or surrounding structures. This may contribute to persistent irritation, altered nerve mobility, or discomfort during shoulder movement and arm elevation.
Although less common, postoperative muscular tension or altered shoulder mechanics may also contribute to persistent symptoms.
Technical Factors Related to Surgical Outcome
In selected cases, persistent symptoms may be related to technical aspects of the decompression procedure itself.
Residual fibrous bands, incomplete decompression of the thoracic outlet, or persistent mechanical narrowing during certain arm positions may continue to affect the brachial plexus or vascular structures even after surgery.
Although these situations are less common than overlapping diagnoses or chronic nerve damage, they should still be considered when recovery does not progress as expected.
Contributing Factors That May Maintain Symptoms After Surgery
Persistent symptoms are often influenced not only by the original compression, but also by additional factors that continue to maintain nerve irritation or abnormal pain processing.
These factors may include:
- Cervical spine disorders affecting nerve roots
- Persistent postural abnormalities and shoulder girdle dysfunction
- Muscular imbalance involving the scalene or pectoralis muscles
- Central sensitization and chronic neuropathic pain mechanisms
- Delayed rehabilitation or persistent movement compensation patterns
- Chronic pain-related muscle guarding and altered biomechanics
Although these factors are rarely the primary cause, they may significantly influence long-term recovery and treatment response.
What Should Be Re-evaluated When Symptoms Persist
When symptoms continue after surgery, the most important step is not to repeat treatment blindly, but to reassess the underlying mechanism responsible for symptoms.
This includes determining:
- whether brachial plexus compression remains present
- whether cervical spine pathology or another peripheral nerve disorder is involved
- whether postoperative scar tissue or altered shoulder mechanics contribute to symptoms
- whether chronic pain mechanisms or muscular dysfunction continue to maintain symptoms
In many patients, different aspects of the condition have already been treated individually. However, lasting improvement often requires a comprehensive strategy based on a clearly defined mechanism of symptoms.
Online pain consultation for pain after surgery in detail
How the video consultation works — step by step
Answers to questions about the process and success of video consultations for pain after urgery
See the page “Possible Reasons for Poor Pain Treatment Effectiveness of Pain After Nerve Surgery” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
Prognosis and Recovery
The prognosis depends mainly on the severity and duration of compression.
When the condition is diagnosed early, many patients improve with physiotherapy and conservative treatment.
After surgical decompression improvement usually occurs gradually over several months.
Long-standing compression may result in partial residual symptoms.
Long-standing symptoms, severe nerve compression, obesity, previous trauma, or persistent postural abnormalities may reduce the likelihood of complete recovery and contribute to prolonged symptoms.
Vascular Warning Signs
Sudden arm swelling, cyanosis, coldness of the hand, significant pulse asymmetry, or major differences in blood pressure between the arms may suggest vascular involvement and require urgent medical evaluation.
When to Seek Specialist Evaluation
Medical evaluation is recommended if:
• Symptoms persist for several months
• Weakness of the hand develops
• Arm pain or numbness interferes with daily activities
• Symptoms worsen during overhead activity
• The diagnosis remains uncertain
Early specialist evaluation may help prevent permanent nerve damage.
Request Thoracic Outlet Syndrome Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Persistent pain, numbness, tingling, or weakness in the arm or hand may raise several important questions:
Is this really thoracic outlet syndrome?
Could the symptoms come from cervical spine disorders or peripheral nerve compression elsewhere?
Could vascular compression be involved?
Should treatment remain conservative with physiotherapy and posture correction, or should surgical decompression be considered?
Why are the symptoms lasting longer than expected?
An independent neurosurgical second opinion may help clarify the cause of nerve or vascular compression within the thoracic outlet,
confirm whether the symptoms correspond to thoracic outlet syndrome or another neurological or orthopedic condition,
and determine whether physiotherapy, activity modification, pain management, or surgical decompression
offers the most appropriate treatment strategy based on the duration of symptoms, neurological findings, and previous evaluations.
- ✔ Send a brief message describing your symptoms, when they began, and whether you notice arm pain, numbness, weakness, or symptoms during overhead activity
- ✔ You will receive a reply within 24 hours explaining whether an online consultation is appropriate and which documentation is required
- ✔ Priority cases: progressive arm weakness, severe neurological symptoms, or vascular symptoms such as swelling or color changes in the hand — write PRIORITY in your first message
- ✔ Previous medical reports, EMG studies, cervical spine imaging, brachial plexus MRI, or vascular imaging can be reviewed
- ✔ During consultation we explain whether physiotherapy, posture correction, activity modification, pain management, or surgical decompression may be appropriate — including expected recovery timelines and up to 10 days of follow-up clarification
Consultation fees typically range from $180–250 depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This corresponds to typical international specialist telehealth neurosurgical second-opinion services.
Frequently Asked Questions About Thoracic Outlet Syndrome
What is thoracic outlet syndrome?
Thoracic outlet syndrome is a condition caused by compression of nerves or blood vessels in the region between the neck and shoulder. This area, called the thoracic outlet, contains the brachial plexus nerves, subclavian artery, and subclavian vein as they pass toward the arm. When these structures are compressed, symptoms may affect the neck, shoulder, arm, hand, or circulation. The most common form is neurogenic thoracic outlet syndrome, involving the brachial plexus. Less common forms involve venous or arterial compression. The condition may develop from anatomical narrowing, cervical rib, scalene muscle tightness, first rib or clavicle abnormalities, fibrous bands, trauma, poor posture, or repetitive overhead arm activity.
What are the most common symptoms of thoracic outlet syndrome?
The most common symptoms of thoracic outlet syndrome depend on whether nerves or blood vessels are primarily compressed. Neurogenic thoracic outlet syndrome may cause pain in the neck, shoulder, arm, or hand, numbness or tingling, hand weakness, reduced grip strength, arm fatigue, and symptoms that worsen with overhead activity or prolonged arm elevation. Lower brachial plexus involvement may affect the forearm, hand, and fourth or fifth fingers, while upper plexus irritation may produce more neck, shoulder, or upper arm pain. Venous thoracic outlet syndrome can cause arm swelling, heaviness, cyanosis, or visible superficial veins. Arterial thoracic outlet syndrome may cause coldness, color changes, pulse changes, or ischemic symptoms in the hand.
What causes thoracic outlet syndrome?
Thoracic outlet syndrome develops when anatomical narrowing or mechanical stress compresses the brachial plexus or subclavian vessels. Compression may occur between the scalene muscles in the interscalene triangle, between the clavicle and first rib in the costoclavicular space, or beneath the pectoralis minor tendon. Causes include congenital anatomical variations such as a cervical rib, tight or hypertrophied scalene muscles, fibrous bands, repetitive overhead activity, poor posture with forward shoulders, previous trauma to the neck or shoulder, clavicle fractures, and structural abnormalities around the first rib. In many patients, symptoms result from a combination of predisposition and repeated mechanical loading. This is why diagnosis and treatment must be individualized, not based only on one anatomical finding.
Is thoracic outlet syndrome dangerous?
Thoracic outlet syndrome is not always dangerous, but some forms require urgent attention. Neurogenic thoracic outlet syndrome can become functionally serious when brachial plexus compression causes persistent pain, numbness, weakness, reduced grip strength, or progressive hand dysfunction. Long-standing nerve compression may lead to slower or incomplete recovery. Venous thoracic outlet syndrome can be more urgent if it causes thrombosis of the subclavian vein, with sudden arm swelling, heaviness, cyanosis, or prominent superficial veins. Arterial thoracic outlet syndrome is the least common but potentially serious because compression of the subclavian artery can reduce blood flow or cause embolic complications. Sudden swelling, coldness, color change, or major pulse asymmetry should prompt urgent medical evaluation.
Can thoracic outlet syndrome improve without surgery?
Yes. Many patients with thoracic outlet syndrome improve without surgery, especially when symptoms are mild, intermittent, posture-related, or improving with physiotherapy. Conservative treatment often includes postural correction, shoulder girdle stabilization, stretching of the scalene and pectoralis muscles, activity modification, pain medication, neuropathic pain medication, and avoidance of positions that provoke symptoms. Injection therapy with local anesthetic, corticosteroid, or botulinum toxin may be used in selected cases to reduce symptoms or clarify whether muscular compression contributes. Conservative treatment is usually continued for several months before surgery is considered. However, progressive neurological deficit, persistent functional limitation, severe vascular compression, thrombosis, or failure of prolonged structured treatment may shift the decision toward surgical decompression.
How is thoracic outlet syndrome diagnosed?
Thoracic outlet syndrome is diagnosed by combining symptom pattern, clinical examination, positional testing, and targeted investigations. The doctor looks for symptoms reproduced by arm elevation, sensory changes, hand weakness, postural abnormalities, and possible pulse or color changes during certain arm positions. EMG and nerve conduction studies may help evaluate brachial plexus function and distinguish thoracic outlet syndrome from cervical radiculopathy or peripheral nerve entrapments. X-rays can identify cervical ribs or clavicle abnormalities. Doppler ultrasound, CT angiography, MR angiography, or venography may be used when vascular compression is suspected. MRI of the cervical spine or brachial plexus can exclude other causes. Diagnosis is complex because symptoms overlap with spine, shoulder, and peripheral nerve disorders.
What treatments are available for thoracic outlet syndrome?
Treatment for thoracic outlet syndrome depends on the type of compression, severity of symptoms, and whether nerves or blood vessels are involved. Many neurogenic cases start with conservative treatment, including physiotherapy, postural correction, shoulder girdle stabilization, scalene and pectoralis stretching, activity modification, pain medication, and medication for neuropathic pain. Selected patients may benefit from local anesthetic, corticosteroid, or botulinum toxin injections, which may also help confirm a muscular component. Vascular thoracic outlet syndrome may require anticoagulation, thrombolysis, vascular surgical management, and decompression when thrombosis or major vessel compression is present. Surgery may include first rib resection, scalenectomy, or removal of fibrous bands compressing the brachial plexus or vessels.
When is surgery recommended for thoracic outlet syndrome?
Surgery for thoracic outlet syndrome is considered when symptoms remain severe, persistent, or progressive despite structured conservative treatment, or when there is significant neurological or vascular compromise. In neurogenic thoracic outlet syndrome, surgery becomes more likely if hand weakness, reduced grip strength, sensory symptoms, or functional impairment persist or worsen over time. In vascular forms, severe compression, thrombosis, swelling, ischemic symptoms, or arterial complications may require more urgent evaluation and treatment. The timing is important. Surgery too early may be unnecessary in milder cases, while delaying decompression too long in more severe compression may reduce recovery potential. The decision depends on symptom progression, examination, imaging, vascular findings, EMG results, and response to physiotherapy.
Can thoracic outlet syndrome cause permanent nerve damage?
Thoracic outlet syndrome can cause long-lasting or permanent nerve-related symptoms if brachial plexus compression is severe or prolonged. Neurogenic thoracic outlet syndrome may initially cause intermittent pain, numbness, tingling, weakness, or arm fatigue during overhead activity. If compression continues, nerves may develop chronic irritation, reduced function, and slower recovery. The risk is higher when weakness progresses, hand function declines, or symptoms persist for many months without improvement. However, not every patient with thoracic outlet syndrome develops permanent nerve damage. Many improve with physiotherapy and postural correction. The challenge is identifying which patients are improving safely and which patients have ongoing compression that may reduce the chance of complete recovery if treatment is delayed too long.
Can symptoms persist after thoracic outlet surgery?
Yes. Symptoms can persist after thoracic outlet surgery, even when decompression was technically successful. This may happen when long-standing brachial plexus irritation has already caused nerve recovery limitations, or when another condition was contributing to symptoms. Cervical radiculopathy, peripheral nerve entrapment, shoulder pathology, double crush syndrome, muscular dysfunction, or chronic pain mechanisms may coexist with thoracic outlet compression. Scar tissue, altered shoulder mechanics, postoperative muscular tension, residual fibrous bands, or incomplete decompression may also contribute. Persistent symptoms do not automatically mean the wrong operation was performed, but they do require reassessment. The important question is whether brachial plexus or vascular compression remains, or whether another neurological, orthopedic, vascular, or pain mechanism is now dominant.
What are possible complications of thoracic outlet surgery?
Thoracic outlet surgery is performed near important nerves and blood vessels, so careful patient selection is essential. Possible complications include wound healing problems, infection, scar discomfort, shoulder stiffness, persistent pain, temporary or persistent numbness, weakness, or neuropathic symptoms from irritation of the brachial plexus or nearby nerves. In vascular forms, bleeding, thrombosis, or vascular injury can rarely occur because surgery is close to the subclavian artery and vein. Some patients continue to have symptoms because nerve irritation was long-standing, because another diagnosis was present, or because recovery of the brachial plexus is incomplete. It is important to distinguish true surgical complications from persistent symptoms caused by overlapping cervical spine disease, peripheral nerve entrapment, muscular dysfunction, or chronic pain sensitization.
What should be re-evaluated if symptoms continue after thoracic outlet surgery?
If symptoms continue after thoracic outlet surgery, the mechanism should be reassessed rather than repeating treatment blindly. The evaluation should determine whether brachial plexus compression remains, whether vascular compression persists, whether residual fibrous bands or incomplete decompression are present, and whether scar tissue or altered shoulder mechanics contribute to symptoms. Other diagnoses must also be reconsidered, including cervical radiculopathy, peripheral nerve entrapments such as carpal tunnel or cubital tunnel syndrome, shoulder disorders, brachial plexus injury, or other structural lesions near the thoracic outlet. Double crush syndrome is also possible, where cervical nerve root compression coexists with thoracic outlet compression. Chronic neuropathic pain, central sensitization, muscular imbalance, and delayed rehabilitation may also maintain symptoms.
Can I obtain an online consultation for thoracic outlet syndrome?
Yes. An online consultation can help when thoracic outlet syndrome is suspected, symptoms persist, or treatment decisions remain unclear. Medical reports, EMG studies, cervical spine imaging, brachial plexus MRI, Doppler ultrasound, CT angiography, MR angiography, or venous studies can be reviewed. The consultation can clarify whether symptoms are more consistent with neurogenic thoracic outlet syndrome, vascular compression, cervical radiculopathy, shoulder pathology, or another peripheral nerve entrapment. It can also help determine whether continued physiotherapy, posture correction, activity modification, pain management, injection therapy, vascular evaluation, or surgical decompression should be discussed with the local team. Progressive weakness or vascular symptoms such as arm swelling, cyanosis, coldness, or color change require urgent local care.
What is the difference between neurogenic, venous and arterial thoracic outlet syndrome?
Neurogenic, venous, and arterial thoracic outlet syndrome differ by which structure is compressed. Neurogenic thoracic outlet syndrome is the most common form and involves the brachial plexus nerves. It typically causes pain, numbness, tingling, weakness, reduced grip strength, and arm fatigue, often worse during overhead activity. Venous thoracic outlet syndrome involves compression of the subclavian vein and may cause sudden arm swelling, heaviness, cyanosis, visible superficial veins, or thrombosis after repetitive arm use. Arterial thoracic outlet syndrome is the least common but potentially serious because subclavian artery compression may reduce blood flow or cause embolic complications. Differentiating these forms matters because diagnosis, urgency, imaging, treatment, and surgical planning can be very different.
Can thoracic outlet syndrome be confused with cervical radiculopathy or peripheral nerve entrapment?
Yes. Thoracic outlet syndrome can be confused with cervical radiculopathy, carpal tunnel syndrome, cubital tunnel syndrome, Guyon canal syndrome, peripheral neuropathy, shoulder disorders, brachial plexus injury, and structural lesions near the thoracic outlet. Symptoms overlap because many of these conditions can produce arm pain, numbness, tingling, weakness, or reduced grip strength. Cervical spine disease may affect nerve roots before they enter the brachial plexus, while peripheral entrapments affect nerves farther down the arm. Thoracic outlet syndrome often worsens with arm elevation or shoulder position, but this is not enough for diagnosis by itself. Clinical examination, EMG, cervical imaging, brachial plexus imaging, vascular studies, and careful symptom analysis help separate these conditions.
Why do thoracic outlet syndrome symptoms worsen during overhead arm activity?
Thoracic outlet syndrome symptoms often worsen during overhead arm activity because arm elevation changes the position and tension of the shoulder girdle, clavicle, first rib, scalene muscles, pectoralis minor region, brachial plexus, and subclavian vessels. These movements can narrow the interscalene triangle, costoclavicular space, or sub-pectoralis minor space. When the brachial plexus is compressed, the patient may feel pain, tingling, numbness, weakness, or arm fatigue. When the subclavian vein or artery is compressed, swelling, heaviness, color change, coldness, or pulse changes may occur. Repetitive overhead work, sports, or prolonged arm elevation can repeatedly irritate already narrow anatomical corridors. This positional worsening is one reason TOS diagnosis requires functional and dynamic assessment, not only static imaging.
What vascular warning signs in thoracic outlet syndrome require urgent evaluation?
Vascular warning signs in thoracic outlet syndrome include sudden arm swelling, cyanosis, coldness of the hand, major color change, prominent superficial veins, significant pulse asymmetry, or a large difference in blood pressure between the arms. These symptoms may suggest venous or arterial thoracic outlet syndrome rather than purely neurogenic compression. Venous compression can lead to subclavian vein thrombosis, especially after repetitive overhead activity. Arterial compression may reduce blood flow, cause embolization, or produce ischemic symptoms in the hand. These situations require urgent in-person medical evaluation because vascular complications can progress and may need imaging, anticoagulation, thrombolysis, vascular surgery, or decompression. Telehealth second opinion may help in stable cases, but acute vascular signs should not be delayed.
What is the difference between first rib resection, scalenectomy and fibrous band removal in thoracic outlet syndrome surgery?
First rib resection, scalenectomy, and fibrous band removal are different decompression techniques used in thoracic outlet syndrome surgery. First rib resection removes part or all of the first rib to enlarge the costoclavicular space and reduce compression of the brachial plexus or subclavian vessels. Scalenectomy removes or releases scalene muscle tissue that contributes to narrowing of the interscalene triangle. Fibrous band removal addresses abnormal bands that directly compress the brachial plexus or vessels. These procedures may be combined depending on the anatomy and compression site. The choice is not identical for every patient. It depends on whether compression is neurogenic, venous, or arterial, where the narrowing occurs, and what imaging, examination, and operative findings suggest.
Why can recovery after thoracic outlet syndrome surgery take several months?
Recovery after thoracic outlet syndrome surgery can take several months because decompression removes mechanical pressure, but nerves, muscles, posture, and movement patterns need time to recover. If brachial plexus compression was present for a long time, nerve irritation or functional changes may improve slowly or incompletely. Postoperative scar tissue, shoulder stiffness, muscular imbalance, altered biomechanics, pain guarding, and delayed rehabilitation can prolong symptoms. Some patients also have overlapping cervical spine disease, peripheral nerve entrapment, or chronic neuropathic pain mechanisms that continue after decompression. Improvement is therefore not always immediate. Follow-up should evaluate whether symptoms are gradually decreasing, whether rehabilitation is restoring shoulder mechanics, and whether another diagnosis or residual compression needs to be reconsidered.