Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Neurosurgeon and Pain Management Specialist
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
January 28, 2026
Who This Page Is For
This page is intended for patients and family members dealing with the combination of
gait disturbance, cognitive decline, and urinary problems, especially when brain MRI shows
enlarged ventricles together with brain atrophy or ischemic changes.
It explains how to distinguish age-related and degenerative brain changes from
normal pressure or chronic communicating hydrocephalus, why imaging alone is often insufficient,
and how clinicians assess whether hydrocephalus plays a meaningful and potentially reversible role in symptoms.
Readers may focus only on sections relevant to their situation.
If MRI findings are unclear, symptoms overlap with dementia, or it is uncertain whether surgical treatment could realistically help,
an experienced
neurosurgical second opinion
can help clarify whether hydrocephalus is a significant contributor and what outcomes can reasonably be expected.
When patients and families usually seek a second opinion
- MRI shows enlarged ventricles together with brain atrophy or ischemic changes, and it is unclear whether hydrocephalus is clinically relevant
- Walking difficulty, cognitive decline, and urinary problems progress despite medical treatment
- Doctors disagree on whether symptoms are due to dementia, vascular brain disease, hydrocephalus — or a combination
- Normal pressure hydrocephalus is mentioned, but no clear explanation is given about expected benefit from treatment
- A lumbar tap test or shunt surgery is proposed, but risks and realistic outcomes remain uncertain
- Medication effects (sedatives, antidepressants) may be worsening gait or cognition and confounding assessment
- Families are unsure whether further testing or surgery could meaningfully improve quality of life
In these situations, an experienced neurosurgical review can help determine whether hydrocephalus meaningfully contributes to symptoms, clarify the role of further testing, and define realistic expectations before any invasive intervention: Request a Second Opinion
Dementia, Gait Disorders and Urinary Incontinence — Quick Summary (Read This First)
- The combination of gait disturbance, cognitive decline, and urinary problems in older adults has multiple possible causes. Brain atrophy, small-vessel ischemic disease, neurodegenerative dementias, and hydrocephalus often coexist on MRI.
- Enlarged ventricles on MRI do not automatically mean treatable hydrocephalus. Ventricular enlargement may reflect aging, brain atrophy, vascular disease, hydrocephalus — or a combination of these processes.
- Normal pressure hydrocephalus (NPH) is caused by impaired cerebrospinal fluid absorption. Ventricles enlarge gradually due to excess CSF–related mechanical stress, often without sustained elevation of intracranial pressure, yet chronic stretching can still damage surrounding brain tissue.
- Gait disturbance is usually the earliest and most reliable symptom of NPH. Cognitive impairment typically reflects frontal–subcortical dysfunction rather than primary memory loss; urinary symptoms usually appear later.
- Degenerative and vascular brain changes are common with aging and are generally not reversible. When these processes predominate, surgical treatment (ventriculo-peritoneal or VP shunt) aimed at cerebrospinal fluid diversion is unlikely to provide meaningful clinical benefit.
- Most patients show mixed pathology. NPH frequently overlaps with brain atrophy, vascular disease, or Alzheimer-type degeneration, which explains why treatment outcomes are variable and probabilistic.
- No single test determines whether surgery (VP shunt) will help. Diagnosis relies on integrated assessment of clinical course, neurological examination, cognitive testing, MRI findings, medication effects, and dynamic tests such as temporary CSF removal.
- When hydrocephalus contributes meaningfully, gait improvement is the most consistent benefit of VP shunt. Cognitive and urinary improvements are less predictable and depend on coexisting brain disease.
- This page is structured so you can focus only on what matters to you. Use the Contents box to jump to sections on causes, diagnosis, testing, or when a neurosurgical second opinion may be useful.
Most readers benefit from the Quick Summary plus the sections on Normal Pressure Hydrocephalus, Integrated Diagnostic Evaluation, and Temporary CSF Reduction (Tap Test). Other sections provide deeper clinical context.
Contents
- Who This Page Is For
- When patients and families usually seek a second opinion
- Quick Summary (Read This First)
- A Real-World Clinical Scenario
- Brain Atrophy, Vascular Changes, and Dementia
- Alzheimer’s Disease and Other Neurodegenerative Dementias
- Normal Pressure Hydrocephalus (NPH)
- Communicating Chronic Hydrocephalus
- Overlap Between Hydrocephalus and Degenerative Dementias
- Clinical and Neurological Assessment
- Integrated Diagnostic Evaluation
- Brain MRI: What It Can (and Cannot) Tell Us
- Incidental finding of ventriculomegaly on MRI
- Temporary CSF Reduction (Lumbar Tap Test)
- Request a Neurosurgical Second Opinion
- When Surgical Treatment Is Considered
- Why Decision About Surgery Is Often Unclear
- VP Shunt With Programmable Valve
- Why Experience Matters
- When an Expert Neurosurgical Second Opinion Is Valuable
- FAQs
- Additional Resources for Patients & Caregivers
A Real-World Clinical Scenario
An 85-year-old woman gradually develops difficulty walking, frequent falls, loss of bladder control, and progressive cognitive decline with episodes of agitation and confusion. Over time, she is prescribed antidepressants and sedative medications, which further worsen gait instability and alertness.
Brain MRI shows generalized cerebral atrophy with ischemic white-matter changes, enlarged ventricles, and features suggestive of hydrocephalus. It remains unclear whether her symptoms are driven primarily by neurodegenerative disease, vascular brain injury, hydrocephalus, or a combination of all three.
The central question becomes: is hydrocephalus a meaningful contributor to her symptoms, and if so, is there a realistic chance that surgical intervention (VP shunt) could help?
Particularly in developed countries, with their growing elderly populations, these cases are becoming increasingly common. The most important question is not whether the ventricles are enlarged, but whether the symptoms are truly caused by NPH — because only then surgery can lead to meaningful improvement.
Brain Atrophy, Vascular Changes, and Dementia
Age-related brain atrophy and small vessel disease are common findings in older adults and are often part of the normal aging process. Brain MRI may show widened cortical sulci, reduced overall brain volume, and small ischemic lesions within the white matter. These findings reflect chronic degenerative changes of small cerebral blood vessels rather than an active or rapidly progressive disease. Over time, such microvascular changes—often related to hyaline-type degeneration of small arteries—can impair blood flow to deep brain structures and contribute to cognitive slowing and gait instability. Importantly, these age-related changes may coexist with hydrocephalus and partially overlap with its symptoms, which is why they should be interpreted as background findings unless clinical features and CSF dynamics suggest otherwise.
These processes alone can explain:
- slow cognitive decline,
- impaired executive function (difficulty planning, organizing, and managing everyday tasks)
- gait slowing,
- urinary urgency or incontinence.
Importantly, atrophy-related and vascular dementia are not reversible.
When they represent the dominant process, surgical treatment aimed at cerebrospinal fluid (CSF) diversion is unlikely to produce meaningful benefit. Read more about brain anatomy on this page.
Alzheimer’s Disease and Other Neurodegenerative Dementias
Alzheimer’s disease and other neurodegenerative dementias represent a fundamentally different disease process from hydrocephalus. They are characterized by progressive neuronal loss, synaptic degeneration, and accumulation of abnormal proteins within the brain, leading to irreversible cognitive decline.
In Alzheimer’s disease, MRI typically shows predominant hippocampal and medial temporal lobe atrophy rather than ventricular enlargement out of proportion to cortical atrophy. Gait and urinary symptoms usually appear late in the disease course and are secondary to advanced cognitive impairment rather than a primary neurological mechanism.
Other degenerative dementias—such as dementia with Lewy bodies, frontotemporal dementia, or Parkinson-related dementia—have distinct clinical patterns and imaging features and do not improve with cerebrospinal fluid diversion procedures.
Importantly, neurodegenerative dementias may coexist with vascular changes or hydrocephalus in older patients, creating diagnostic overlap. However, their presence significantly reduces the likelihood of meaningful improvement after shunt surgery and must be carefully considered before any invasive intervention.
Normal Pressure Hydrocephalus (NPH)
Normal pressure hydrocephalus is a chronic disorder of cerebrospinal fluid (CSF) circulation characterized by progressive enlargement of the brain ventricles without sustained elevation of intracranial pressure on routine measurement. It primarily affects older adults and develops slowly over months to years.
How NPH Develops and Damages the Brain
In NPH, cerebrospinal fluid is produced normally but is inadequately absorbed, leading to gradual ventricular expansion. Because this process evolves slowly, the brain adapts to the increasing ventricular size without triggering the acute warning signs typically associated with raised intracranial pressure, such as severe headache, vomiting, or visual disturbances.
Despite “normal” measured pressure, ventricular enlargement exerts chronic mechanical stress on surrounding brain tissue. The expanding ventricles stretch and compress the periventricular white matter, disrupt long neural pathways, and impair microcirculation. This results in reduced signal transmission between deep brain structures and the frontal lobes, particularly affecting motor planning, executive function, and bladder control.
Importantly, the absence of sustained pressure elevation does not mean absence of brain injury. In NPH, damage occurs through long-term distortion and shear stress, combined with impaired clearance of interstitial fluid around the ventricles.
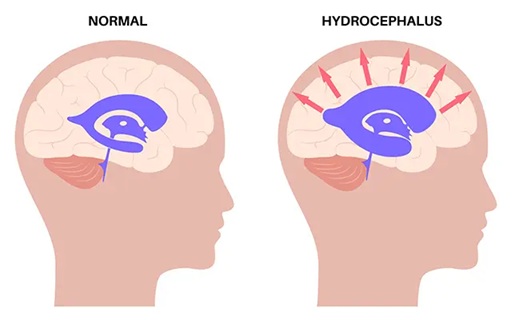
Image: In NPH, there is a gradual and slow enlargement of the ventricles due to the inadequate resorption of CSF, which is constantly being produced. Thanks to intracranial adaptive mechanisms, there is no increase in ICP. However, the accumulation of CSF leads to brain tissue damage due to the stretching of the ventricular walls and the penetration of CSF into the periventricular areas. Read more about the anatomy of the ventricles on this page.
Why Intracranial Pressure Is Often Normal
In normal pressure hydrocephalus, excess cerebrospinal fluid builds up slowly over time. Because this process is gradual, the brain has time to adapt instead of reacting with a sudden rise in pressure. As part of this adaptation, the brain makes room for the expanding ventricles by gradually redistributing fluids within the skull. As a result, the fluid-filled spaces in the brain can enlarge without causing persistently high intracranial pressure, and routine lumbar puncture measurements often appear normal. Even so, abnormal fluid accumulation continues, and the gradual stretching of surrounding brain tissue can still lead to progressive neurological symptoms, such as difficulty walking and memory loss.
In clinical practice, the term normal pressure hydrocephalus is often used as a broad descriptive label. From a diagnostic and therapeutic perspective, however, the majority of older patients evaluated for this condition fall within the category of idiopathic normal pressure hydrocephalus (iNPH), which develops gradually without a clearly identifiable precipitating event such as acute subarachnoid hemorrhage, meningitis, traumatic brain injury, or prior neurosurgical intervention. Secondary forms of NPH may occur after such insults to cerebrospinal fluid absorption pathways, but in elderly patients the distinction between idiopathic and secondary NPH is frequently blurred, particularly when potential causative events occurred many years earlier. For this reason, real-world clinical decision-making relies primarily on the clinical presentation, imaging characteristics, and response to cerebrospinal fluid drainage tests, rather than on strict etiological classification alone.
Clinical Manifestations
The characteristic clinical picture of NPH reflects the specific brain regions affected by ventricular enlargement:
- Gait disturbance is usually the earliest and most prominent symptom. Patients develop a broad-based, short-stepped, shuffling gait with difficulty initiating movement and turning.
- Cognitive impairment typically follows and reflects frontal–subcortical dysfunction, with slowed thinking, impaired attention, reduced executive function, and apathy rather than primary memory loss.
- Urinary dysfunction appears later and ranges from urgency and frequency to loss of bladder control.
This symptom combination—gait disturbance, cognitive decline, and urinary dysfunction—forms the classic clinical triad of NPH, although not all patients present with all three features simultaneously.
A diagnostic challenge arises when NPH (Normal Pressure Hydrocephalus) or communicating hydrocephalus occurs alongside conditions that can themselves cause hydrocephalus, such as Chiari malformation.
Communicating Chronic Hydrocephalus
Communicating hydrocephalus refers to a broader category in which cerebrospinal fluid circulates freely through the ventricular system but is inadequately absorbed. Reduced CSF absorption may develop secondary to identifiable conditions, such as prior subarachnoid hemorrhage, meningitis or other central nervous system infections, inflammatory processes, previous neurosurgical procedures, or diffuse leptomeningeal disease. In these situations, scarring, fibrosis, or obstruction of resorptive surfaces interferes with normal CSF outflow.
In other patients, particularly older adults, no single triggering event is identified. Instead, impaired absorption appears to result from gradual age-related degeneration of the CSF resorption system, including reduced efficiency of arachnoid granulations and altered venous compliance. This slow degenerative process may progress over years, leading to ventricular enlargement without an acute rise in intracranial pressure.
Because both mechanisms can produce similar imaging and clinical features, communicating hydrocephalus represents a heterogeneous group rather than a single disease entity.
In contrast to NPH, communicating hydrocephalus may be associated with:
- persistently elevated intracranial pressure,
- pressure-related symptoms such as headache,
- earlier clinical recognition.
However, communicating hydrocephalus can also evolve slowly, particularly when pressure elevation is mild or fluctuating. In such cases, patients may experience long-term gait impairment and cognitive decline over years.
Normal pressure hydrocephalus and other forms of chronic communicating hydrocephalus are most likely caused by impaired cerebrospinal fluid (CSF) resorption. CSF is continuously produced and absorbed, with the entire CSF volume being renewed several times per day. When CSF resorption is significantly reduced, ventricular enlargement is typically accompanied by an increase in intracranial pressure, as seen in communicating hydrocephalus with elevated pressure. When the reduction in resorption is more gradual or less severe, compensatory intracranial mechanisms may be sufficient to maintain intracranial pressure within the normal range, as in normal pressure hydrocephalus (NPH). In this setting, brain ventricles progressively enlarge despite normal measured pressure, and chronic mechanical stress with periventricular tissue injury develops over time. As a result, neurological damage may occur even in the absence of sustained intracranial pressure elevation.
Overlap Between Normal Pressure Hydrocephalus and Degenerative Dementias (Atrophic, Alzheimer’s, and Others)
Neuropathological, imaging, and biomarker studies show that normal pressure hydrocephalus frequently coexists with other degenerative brain processes, most commonly age-related cerebral atrophy and neurodegenerative dementias, rather than representing an isolated disease entity.
Reported rates of combined pathology vary depending on diagnostic methods and patient selection:
- Degenerative or atrophic brain changes are present in the majority of older patients diagnosed with NPH,
- Alzheimer-type pathology is identified in approximately 20–40% of patients undergoing shunt surgery,
- higher rates are reported when CSF biomarkers, amyloid PET, or postmortem analysis are used.
This overlap explains several well-known clinical observations regarding shunt treatment:
- Gait disturbance improves more reliably than cognition after shunt treatment,
- Cognitive improvement is often partial, delayed, or absent, particularly when significant cortical atrophy is present,
- Treatment outcomes are inherently probabilistic, reflecting the combined contribution of hydrocephalus-related and degenerative brain injury.
Importantly, the presence of atrophic or degenerative dementia does not automatically exclude a contribution from hydrocephalus, but it significantly influences the magnitude, durability, and domains of potential improvement.
Clinical and Neurological Assessment of Normal Pressure Hydrocephalus (NPH)
The clinical evaluation aims to create a clear picture of how cerebrospinal fluid buildup affects daily function. Assessment focuses on four key domains:
1. Walking and Balance (Gait)
Walking is carefully observed, including how movement is initiated, step length, walking speed, and turning. A typical finding in NPH is a wide-based gait or the sensation that the feet are “stuck” to the floor. Balance and postural stability are also assessed to estimate the risk of falls.
2. Physical Movement and Strength
Muscle tone, movement speed, coordination, and reflexes are examined. Particular attention is paid to whether abnormalities are symmetric, which helps distinguish NPH from conditions such as stroke or Parkinson’s disease.
3. Cognitive Function and Mental Processing Speed
Cognitive changes in NPH are often characterized by mental slowing rather than prominent memory loss. Testing focuses on attention, processing speed, planning, and the ability to manage multiple tasks. This pattern differs from typical neurodegenerative dementias (such as Alzheimer’s disease), as NPH primarily affects frontal–subcortical networks rather than memory storage systems.
4. Bladder Control
Urinary symptoms are evaluated, ranging from increased urgency and frequency to loss of bladder control in more advanced stages.
Severity of Clinical Involvement in Normal Pressure Hydrocephalus
| Clinical stage | Gait and balance | Cognitive function | Urinary function |
|---|---|---|---|
| Mild | Subtle gait instability, slowed walking, difficulty with turns | Mental slowing, reduced attention or executive function | Urinary urgency or increased frequency |
| Moderate | Gait requiring support or walking aids | Difficulty managing daily activities, reduced independence | Urge incontinence or frequent accidents |
| Advanced | Inability to walk independently or severe postural instability | Marked cognitive impairment with dependence on caregivers | Frequent or persistent incontinence |
Different centers use different grading scales; the goal is to document baseline function consistently.
Why Formal Testing Is Used (MMSE, MoCA, Timed Tasks)
Formal cognitive and gait tests complement the neurological examination by providing standardized, repeatable measurements. Together, the clinical findings and test results establish a functional baseline for monitoring disease progression and for meaningful comparison before and after diagnostic procedures (such as a lumbar tap test) or surgical treatment (shunt placement), helping determine whether intervention has produced true clinical improvement.
Integrated Diagnostic Evaluation
No single test can determine whether hydrocephalus is clinically relevant. Accurate assessment requires integrated interpretation of multiple factors, including:
- brain imaging findings,
- medical history and coexisting illnesses,
- medication effects, particularly sedatives and psychoactive drugs,
- clinical response to trial medications that reduce cerebrospinal fluid (CSF) production,
- laboratory studies to exclude metabolic contributors,
- eye examination to assess for findings that may suggest increased intracranial pressure,
- prior neurological events such as trauma or intracranial bleeding,
- In selected cases, cerebrospinal fluid biomarkers may be helpful to clarify diagnostic overlap with neurodegenerative diseases, particularly Alzheimer’s disease. These tests are not performed routinely in all patients with suspected iNPH but may be considered when cognitive impairment is prominent or atypical; typical examples include amyloid beta (Aβ42), tau proteins, and neurofilament light chain, which can support differential diagnosis and help estimate the likelihood of benefit from shunt surgery..
No individual factor is sufficient on its own. Rather, the interaction between clinical findings, imaging features, cognitive profile, eye examination, medication adjustments, response to trial therapies, and the tempo of symptom progression determines whether hydrocephalus is likely contributing meaningfully to a patient’s condition.
Accurately integrating these elements requires substantial clinical experience, particularly when determining whether a patient’s symptoms are driven primarily by potentially reversible hydrocephalus-related dysfunction or by coexisting degenerative or vascular brain disease, both of which can present with ventricular enlargement. In practice, this level of judgment typically requires a neurologist or neurosurgeon familiar with the full spectrum of hydrocephalus presentations.
When symptoms and imaging suggest a potentially reversible component, cautious further evaluation—such as lumbar puncture—may be appropriate. When degenerative disease clearly predominates, aggressive intervention is unlikely to provide meaningful benefit and may carry unnecessary risk.
Brain MRI: What It Can (and Cannot) Tell Us
Brain MRI is an essential part of the evaluation, but it rarely provides a single definitive answer. Distinct imaging patterns exist for ischemic brain disease, age-related atrophy, and hydrocephalus, yet these findings often coexist in older patients.
MRI may show:
- changes suggestive of chronic small vessel ischemia,
- features consistent with generalized brain atrophy,
- or ventricular enlargement compatible with hydrocephalus, with or without signs associated with elevated intracranial pressure.
Importantly, similar MRI appearances can reflect different underlying mechanisms, and ventricular enlargement alone does not establish the diagnosis. MRI findings must therefore be interpreted in combination with clinical presentation, cognitive profile, disease progression, and other diagnostic indicators to determine whether hydrocephalus plays a meaningful role in the patient’s symptoms.
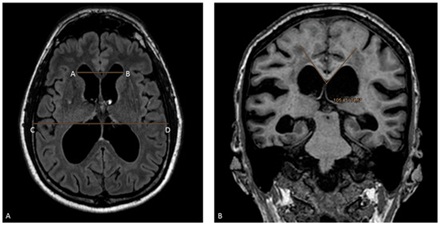
Image: Brain MRI in elderly patients often shows cerebral atrophy combined with enlarged ventricles. Specialized evaluation is required to determine whether these enlarged ventricles represent active hydrocephalus or are simply enlarged due to brain atrophy (compensatory enlargement).
Incidental Ventriculomegaly on Brain MRI: When to Monitor and What to Track
Ventricular enlargement is sometimes discovered incidentally on MR brain imaging performed for unrelated reasons, before clear clinical symptoms of normal pressure hydrocephalus are present. In such cases, immediate intervention is usually not indicated, but structured clinical follow-up is important.
Patients should be monitored for early changes in gait, cognition, and urinary function. Subtle gait instability, slowed walking, difficulty with turns, reduced attention, executive dysfunction, or new urinary urgency may represent the earliest clinical signals of progression. In the absence of symptoms, clinical reassessment is typically reasonable at intervals of 6 to 12 months, or earlier if new neurological or functional complaints emerge. Repeat imaging is not routinely required unless clinical status changes.
Establishing a formal baseline assessment of gait and cognitive function can be particularly useful when ventricular enlargement is pronounced or when the clinical picture is borderline. Objective baseline measurements allow earlier detection of progression and support timely decision-making if symptoms begin to evolve.
Temporary CSF Reduction (Lumbar Tap Test): Indications, Procedure, and Interpretation
A temporary reduction of cerebrospinal fluid (CSF) volume (30-50 ml) via lumbar puncture is not intended as a general screening tool and should not be performed as a routine procedure. It is indicated only after a structured clinical evaluation suggests that hydrocephalus—normal pressure or chronic communicating—contributes meaningfully to the patient’s neurological deficits, rather than representing an incidental imaging finding.
When the Test Is Considered
A cerebrospinal fluid (CSF) tap test is considered only after potentially reversible or confounding factors have been addressed. This includes careful review and optimization of centrally acting medications, such as sedatives, antidepressants, and antipsychotics. It also includes exclusion of acute or subacute neurological or medical complications, for example chronic subdural hematoma, infection, or metabolic disturbances.
A documented baseline is then established through neurological examination and objective assessment of gait, balance, and cognitive function. Brain imaging, medical history, eye examination findings, prior neurological events, response to medication adjustments or trial therapies, and the tempo of symptom progression are considered together as part of this integrated evaluation.
The purpose of the tap test is not to confirm a diagnosis, but to assess whether symptoms show signs of physiological reversibility. No single finding is decisive on its own. Instead, the likelihood that hydrocephalus is meaningfully contributing to a patient’s symptoms depends on the combined interpretation of clinical findings, brain imaging, and functional assessment. A lack of improvement after a tap test does not rule out potential benefit from shunt surgery. Rather, a positive response to the test provides supportive evidence—alongside clinical and imaging features—that cerebrospinal fluid diversion may lead to symptom improvement.
How the Procedure Is Performed
The test consists of a controlled lumbar puncture, during which the opening pressure is measured at the start of the procedure to document whether intracranial pressure appears elevated, followed by the removal of approximately 30–50 mL of CSF under sterile conditions.
Before CSF removal, the following are documented:
- baseline gait performance, including walking speed over a 10-meter distance, step length, turning, and balance; video recording is particularly useful when the patient is unable to walk independently, as it allows objective comparison with post–tap test performance.
- baseline cognitive and attentional function (structured bedside or formal tests),
- baseline functional status as reported by patient and caregivers.
After CSF removal, the same parameters are reassessed, typically:
- within 2-4 hours, and
- again over the following 24–72 hours, depending on the clinical protocol.
- Improvements in gait are often detected early, while changes in cognitive function and urinary symptoms may appear later and are therefore monitored for up to 7 days.
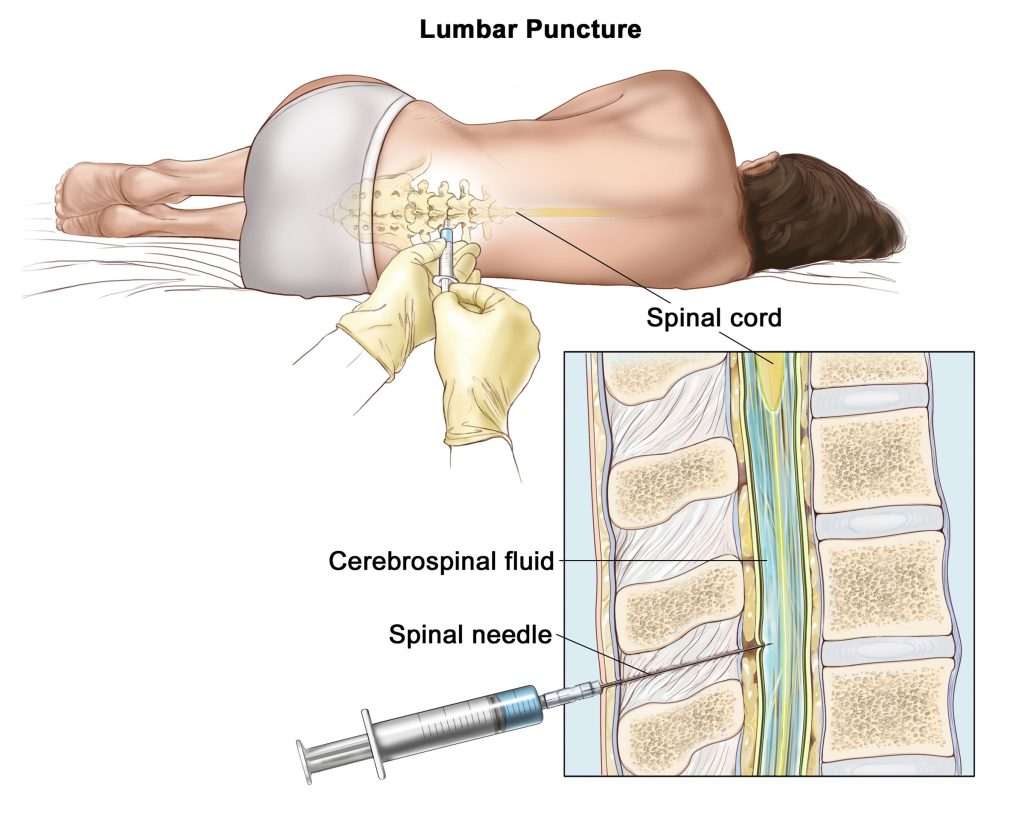
Image: Performing a lumbar puncture for a CSF tap test, involving measuring initial ICP, and the evacuation of 30–50 mL of cerebrospinal fluid.
What Constitutes a Meaningful Response
Improvement after CSF removal is often subtle rather than dramatic and must be evaluated objectively.
A positive response may include:
- measurable improvement in gait initiation, speed, or stability,
- clearer attention, improved responsiveness, or reduced psychomotor slowing,
- improved ability to perform daily activities noted by caregivers.
Crucially, gait improvement following a tap test tends to be more immediate and robust than changes in cognition or urinary control. This discrepancy occurs for two main reasons: first, neurological recovery of cognitive function requires more time to manifest post-drainage; and second, while gait is directly linked to CSF dynamics, cognition and bladder control are often concurrently compromised by pre-existing vascular brain atrophy—a condition present in the majority of these elderly patients.
How Results Are Interpreted
Interpretation requires caution:
- Improvement supports—but does not guarantee—benefit from permanent CSF diversion.
- Absence of improvement does not automatically exclude benefit, particularly in patients with advanced disease, mixed pathology, or delayed response patterns.
- Responses may be influenced by placebo effects, medication adjustments, fatigue, or day-to-day variability, which is why objective comparison to baseline is essential.
The test therefore provides probabilistic guidance, not certainty. It helps estimate whether reducing CSF volume is likely to alleviate symptoms, but it does not replace clinical judgment.
Clinical Meaning of the Test
A favorable response suggests that hydrocephalus-related mechanisms are functionally relevant and that the patient may benefit from further consideration of CSF diversion strategies. Conversely, a negative or equivocal response highlights the need for caution and reinforces the importance of integrating all clinical, imaging, and functional data before proceeding.
What to Do If the Tap Test Is Inconclusive
If a single large-volume lumbar tap test does not result in clear clinical improvement, this does not rule out idiopathic normal pressure hydrocephalus. In such cases, additional diagnostic steps may be considered.
Repeating the tap test under standardized conditions can sometimes reveal subtle or delayed changes, particularly in gait. If the clinical response remains unclear, extended lumbar cerebrospinal fluid drainage is often the next step. This involves continuous CSF drainage through a lumbar catheter over several days, typically 2 to 3 days, during which the patient is encouraged to mobilize and walk under supervision. Repeated assessment of gait, balance, and functional performance during this period often provides stronger prognostic information than a single tap test.
In selected centers, a CSF infusion test may also be used to assess cerebrospinal fluid outflow resistance. However, because patients must remain supine during the procedure and functional improvement cannot be assessed, this test is not routinely used and rarely changes clinical decision-making.
Request a Neurosurgical Second Opinion — Normal Pressure Hydrocephalus vs Other Causes.
24-Hour Review or Priority Option (Usually Within 3 Hours)
Families dealing with gait decline, cognitive impairment, and urinary problems are often told that
MRI shows brain atrophy, ischemic changes, enlarged ventricles — or all of them at once.
The key question is usually not whether abnormalities exist, but
whether hydrocephalus meaningfully contributes to symptoms and whether any surgical intervention could realistically help.
An independent neurosurgical second opinion can help clarify how imaging, clinical findings, medications,
and test results fit together, and whether further diagnostic steps or surgical treatment are reasonable — or unlikely to help.
- ✔ Send a short message describing current symptoms (walking, cognition, bladder control) and what the MRI report says
- ✔ You’ll receive a reply within 24 hours explaining whether and how a second opinion could help in your specific situation
- ✔ Time-sensitive cases: if symptoms are rapidly worsening, falls are frequent, or surgery is being proposed with uncertainty — write PRIORITY in your first message
- ✔ Brain MRI (DICOM images) and available medical documentation can be reviewed once initial contact is established
- ✔ During the consultation, we discuss whether hydrocephalus is likely contributing to symptoms, the role of lumbar tap testing or other evaluations, and realistic expectations regarding VP shunt surgery — with up to 10 days of follow-up for brief questions
Consultation fees typically range from $180–250, depending on case complexity.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth second opinions in neurosurgery.
When Surgical Treatment Is Considered
Surgical diversion of cerebrospinal fluid may be considered when:
- symptoms significantly impair function,
- hydrocephalus appears to contribute meaningfully,
- overall health permits intervention,
- expectations are realistic.
Outcomes vary widely. Improvement is most likely in gait, less predictable in bladder function, and often limited for cognition. Surgery is most beneficial in patients where clinical symptoms, imaging findings, and functional testing all point in the same direction — otherwise, the chance of improvement is significantly lower.
Why the Decision About Surgery Is Often Unclear
Uncertainty arises because:
- MRI findings are not self-explanatory,
- pressure measurements capture only a moment in time,
- symptom overlap with dementia is substantial,
- treatment benefits are probabilistic rather than guaranteed.
This complexity explains why answers to important questions may differ. The reasons are outlined below.
Why MRI Findings Alone Are Not Sufficient?
MRI often shows enlarged ventricles together with brain atrophy or vascular changes, but these findings can have different causes. Ventricular enlargement may reflect hydrocephalus, age-related atrophy, or both, and imaging alone cannot determine which process is actually responsible for the patient’s symptoms.
Why Symptoms Overlap Between Hydrocephalus And Dementia?
Gait disturbance, cognitive decline, and urinary problems can be caused by normal pressure hydrocephalus, vascular brain disease, or neurodegenerative dementia. Because these conditions frequently coexist, it is often unclear which one is the dominant driver of symptoms.
Why No Single Test Can Confirm The Diagnosis?
Tests such as the lumbar tap test or CSF drainage can suggest reversibility, but they are not definitive. A positive response increases the likelihood of benefit, while a negative result does not exclude potential improvement, making interpretation inherently uncertain.
Why Treatment Outcomes Are Not Predictable?
Even when hydrocephalus contributes to symptoms, outcomes after shunt surgery vary because most patients have mixed pathology. Improvement is usually most visible in gait, while cognitive and urinary changes are less predictable, depending on the degree of coexisting brain damage.
Why Do Some Specialists Recommend Surgery While Others Do Not?
Recommendations differ because the decision depends on how each specialist weighs the potential reversibility of symptoms against the risks of surgery. Some consider intervention justified when there is a reasonable chance that hydrocephalus contributes to symptoms, particularly when gait impairment is prominent and potentially reversible. Others recommend a more conservative approach when degenerative or vascular brain changes appear to dominate, or when the expected benefit is uncertain relative to the procedural risk.
Ventriculoperitoneal (VP) Shunt With Programmable Valve: What It Means in Practice
When permanent cerebrospinal fluid (CSF) diversion is considered, the most commonly used procedure is ventriculoperitoneal (VP) shunt placement. The operation involves creating a small opening in the skull to place a thin catheter into a brain ventricle. This catheter is connected to a valve system and a soft tube that runs under the skin, usually behind the ear and along the neck and chest, directing excess CSF into the abdominal cavity, where it is safely absorbed.
In some centers, lumboperitoneal (LP) shunts are frequently utilized, which divert cerebrospinal fluid from the lumbar subarachnoid space to the peritoneal cavity. Additionally, ventriculoatrial (VA) shunts are reserved for specific, selected cases where traditional drainage routes are not feasible.
Why a Programmable Valve Is Essential
In older patients with suspected normal pressure or chronic communicating hydrocephalus, programmable valves are strongly preferred. Programmable is preferred when available; in some settings fixed-pressure valves are used with acceptable outcomes when chosen carefully and monitored properly.
A programmable valve allows:
- non-invasive adjustment of CSF drainage pressure,
- gradual and individualized regulation of CSF outflow over time,
- avoidance of abrupt overdrainage, which can be harmful.
Rather than choosing a single fixed pressure at surgery, treatment becomes a stepwise process.
How Pressure Adjustment Works
After shunt implantation:
- the valve is initially set to a relatively higher opening pressure,
- the patient is observed clinically over days to weeks,
- pressure is then gradually lowered in controlled steps if symptoms persist and no complications occur.
Adjustments are performed externally, using a magnetic programming device placed over the scalp. No surgery, puncture, or anesthesia is required.
This gradual strategy allows the brain to adapt to changing CSF dynamics and helps identify the lowest effective pressure that provides benefit without causing harm.
What Is Monitored After Shunt Placement
Follow-up focuses on clinical function, not imaging alone.
Key parameters include:
- gait stability and walking confidence,
- balance and fall frequency,
- cognitive clarity and responsiveness,
- urinary control,
- overall functional independence.
Imaging may be used selectively to exclude complications, but clinical response is the primary guide for valve adjustment.
Expected Benefits and Realistic Outcomes
When hydrocephalus is a significant contributor to symptoms, clinical improvement after shunt surgery is common but variable. Reported improvement rates vary widely across studies and depend strongly on diagnostic criteria, patient selection, comorbidities, and follow-up protocols. Across published studies, improvement rates of approximately 40–80% within the first 3–6 months and 60–70% at 1–2 years have been reported in appropriately selected patients, with outcomes depending strongly on diagnostic criteria and patient selection. The degree of improvement varies across different clinical deficits:
- gait improvement is usually the earliest and most reliable response,
- cognitive changes, if present, are often modest and gradual,
- urinary symptoms may improve variably.
Improvement reflects reversal of hydrocephalus-related dysfunction, not treatment of underlying neurodegenerative disease. In carefully selected patients, shunt surgery can significantly improve walking and quality of life, but in others it may bring little benefit — which is why proper preoperative evaluation is critical.
Potential Complications (What Patients Should Know)
VP shunt surgery is a standard neurosurgical procedure, but it is not risk-free.
Possible complications include:
- overdrainage, which may cause headaches, dizziness, or subdural fluid collections,
- underdrainage, resulting in limited or absent symptom improvement,
- shunt malfunction or blockage,
- infection,
- abdominal complications (rare).
The use of a programmable valve significantly reduces the risk of long-term complications by allowing pressure correction without repeated surgery.
Why Experience Matters
Determining:
- when to implant a shunt,
- which valve to use,
- how quickly to adjust pressure,
- and how to interpret partial or delayed responses
requires substantial clinical experience. VP shunt treatment is not a single event but a dynamic, long-term management process tailored to each patient’s physiology and symptom profile.
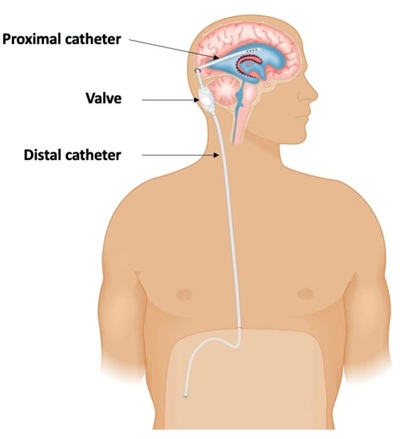
Image: The illustration shows a ventriculoperitoneal (VP) shunt placed for hydrocephalus, which drains excess cerebrospinal fluid (CSF) into the abdominal cavity. The components of the shunt include a ventricular catheter, a programmable valve—designed to precisely regulate CSF drainage to prevent both under-drainage and over-drainage—and a distal catheter that routes the fluid from the valve into the abdomen.
Read about how hydrocephalus can be associated with the occurrence of spontaneous CSF leaks.
When an Expert Neurosurgical Second Opinion Is Valuable
A neurosurgical second opinion is most helpful when diagnostic findings are mixed, test results are inconclusive, or treatment decisions carry meaningful risk. In these situations, an experienced review can help determine whether hydrocephalus is a major driver of symptoms, clarify the role and limitations of further testing, and define realistic expectations regarding VP shunt surgery, valve adjustment, and long-term follow-up.
Frequently Asked Questions About Normal Pressure Hydrocephalus and Similar Conditions
What is normal pressure hydrocephalus (NPH)?
Normal pressure hydrocephalus is a chronic disorder of cerebrospinal fluid circulation in which the brain ventricles gradually enlarge, usually in older adults, without sustained high intracranial pressure on routine measurement. The term “normal pressure” can be misleading, because normal measured pressure does not mean that the brain is unharmed. The problem is usually impaired absorption of cerebrospinal fluid, causing slow ventricular expansion and long-term mechanical stress on the surrounding brain tissue. This may affect pathways involved in walking, attention, executive function, and bladder control. The typical clinical picture includes gait disturbance, cognitive slowing, and urinary urgency or incontinence. Diagnosis is not made from MRI alone; symptoms, examination, imaging, medication effects, and CSF drainage tests must be interpreted together.
Do enlarged ventricles on brain MRI always mean normal pressure hydrocephalus?
No. Enlarged ventricles on brain MRI do not automatically mean treatable normal pressure hydrocephalus. Ventricles may enlarge because of true hydrocephalus, but they may also appear enlarged because of brain atrophy, vascular brain disease, neurodegenerative dementia, or a combination of these processes. In older patients, MRI often shows cerebral atrophy, ischemic white-matter changes, and enlarged ventricles at the same time. The key question is whether ventricular enlargement is actively contributing to gait decline, cognitive slowing, and urinary symptoms, or whether it mainly reflects loss of brain volume. This distinction cannot be made from ventricle size alone. Clinical course, neurological examination, cognitive profile, MRI pattern, medication review, and response to CSF removal all matter.
Why is intracranial pressure often normal in normal pressure hydrocephalus?
Intracranial pressure is often normal in NPH because the cerebrospinal fluid problem develops slowly. As ventricles enlarge over months or years, the brain and intracranial compartments partly adapt instead of reacting with an acute pressure crisis. Routine lumbar puncture pressure may therefore be within the normal range. However, this does not mean that the condition is harmless. Gradual ventricular enlargement can still stretch periventricular white matter, disturb long neural pathways, impair microcirculation, and interfere with communication between deep brain structures and the frontal lobes. This chronic mechanical stress can produce gait disturbance, slowed thinking, impaired attention, and bladder dysfunction. In NPH, the injury is often due to long-term distortion and CSF-related tissue stress, not necessarily sustained high pressure.
How is normal pressure hydrocephalus different from Alzheimer’s disease or vascular dementia?
Normal pressure hydrocephalus differs from Alzheimer’s disease and vascular dementia mainly in mechanism, symptom pattern, and potential reversibility. In NPH, impaired cerebrospinal fluid absorption causes ventricular enlargement and dysfunction of frontal-subcortical pathways. Gait disturbance is usually the earliest and most reliable symptom, followed by cognitive slowing and urinary problems. In Alzheimer’s disease, the dominant problem is progressive neurodegeneration with neuronal loss and protein accumulation, often beginning with memory impairment and medial temporal or hippocampal atrophy. Vascular dementia results from chronic small-vessel disease or ischemic brain injury and may cause cognitive slowing, gait impairment, and executive dysfunction. These conditions may overlap with NPH in older patients. This overlap is why shunt benefit is variable and must be judged carefully.
Can normal pressure hydrocephalus coexist with Alzheimer’s disease, brain atrophy or vascular dementia?
Yes. Normal pressure hydrocephalus often coexists with brain atrophy, vascular brain disease, or Alzheimer-type degeneration, especially in older patients. This mixed pathology is one of the main reasons why diagnosis and treatment decisions are difficult. Ventricular enlargement may be partly due to hydrocephalus and partly due to loss of brain volume. Symptoms may also overlap: gait slowing, cognitive decline, and urinary problems can be caused by hydrocephalus, vascular disease, neurodegeneration, medication effects, or several of these together. The presence of degenerative or vascular changes does not automatically exclude a hydrocephalus contribution, but it reduces the chance of broad improvement after shunt surgery. In such patients, gait improvement is usually more likely than major cognitive recovery.
Which symptoms are most likely to improve after treatment for normal pressure hydrocephalus?
Gait disturbance is the symptom most likely to improve after successful treatment for normal pressure hydrocephalus. Patients may walk faster, initiate steps more easily, turn more safely, or have fewer falls. This is because gait dysfunction in NPH is closely related to frontal-subcortical pathway disruption caused by ventricular enlargement. Cognitive and urinary symptoms may improve, but they are less predictable. Cognitive recovery may be partial, delayed, or absent, especially when Alzheimer-type degeneration, brain atrophy, or vascular disease is significant. Urinary urgency may improve in some patients, but longstanding incontinence is less reliable. The most realistic expectation is therefore not “reversal of dementia,” but possible improvement in walking and function if hydrocephalus is a meaningful contributor.
What is the large-volume lumbar puncture or lumbar tap test and why is it performed in suspected NPH?
The lumbar tap test is a controlled lumbar puncture in which a relatively large volume of cerebrospinal fluid, usually about 30–50 mL, is removed to see whether symptoms improve temporarily. It is not meant to be a routine screening test for every patient with enlarged ventricles. It is considered after clinical evaluation suggests that hydrocephalus may meaningfully contribute to gait, cognitive, or urinary symptoms. Before the test, baseline walking, balance, cognitive function, and functional status should be documented. After CSF removal, the same functions are reassessed over hours to days. Gait response is usually the most useful and earliest sign. A positive response supports possible benefit from shunt surgery, but does not guarantee it.
Is normal pressure hydrocephalus a form of dementia?
Normal pressure hydrocephalus is not a degenerative dementia in the same sense as Alzheimer’s disease, frontotemporal dementia, or vascular dementia. However, NPH can cause dementia-like cognitive symptoms because enlarged ventricles affect frontal-subcortical brain networks involved in attention, processing speed, planning, motivation, and daily function. This is why some patients with NPH appear forgetful, slow, apathetic, confused, or less able to manage routine activities. The important difference is that part of this dysfunction may be reversible if hydrocephalus is a meaningful contributor and the patient is appropriately selected for treatment. In older patients, NPH may also coexist with true neurodegenerative or vascular dementia, which makes improvement after shunt surgery less predictable, especially for cognition.
Does lack of improvement after a lumbar tap test exclude benefit from shunt surgery?
No. Lack of improvement after a single lumbar tap test does not completely exclude benefit from shunt surgery. The tap test provides probabilistic guidance, not certainty. Some patients have delayed or subtle improvement that may be missed if gait and function are not measured objectively. Others may have mixed pathology, fatigue, medication effects, advanced disease, or day-to-day variability that makes the response difficult to interpret. A clearly positive tap test strengthens the case for CSF diversion, but a negative or equivocal result requires careful reassessment rather than an automatic conclusion. In selected cases, repeating the tap test, using standardized gait measurements, or considering extended lumbar drainage over several days may provide better information before deciding about a permanent shunt.
What is communicating hydrocephalus and how does it differ from normal pressure hydrocephalus?
Communicating hydrocephalus is a broader condition in which cerebrospinal fluid can circulate through the ventricles but is not absorbed adequately. It may occur after subarachnoid hemorrhage, meningitis, inflammation, previous neurosurgery, leptomeningeal disease, or gradual age-related decline in CSF absorption. When impaired absorption causes ventricular enlargement with persistently or intermittently elevated pressure, symptoms may include headache or other pressure-related complaints. Normal pressure hydrocephalus is usually a slowly developing form in older adults where measured pressure is often normal, but chronic ventricular enlargement still damages periventricular brain pathways. In practice, the distinction can be blurred, especially in elderly patients. Treatment decisions depend less on terminology and more on symptoms, imaging pattern, CSF dynamics, and reversibility testing.
When is VP shunt surgery considered for normal pressure or chronic communicating hydrocephalus?
VP shunt surgery is considered when symptoms significantly impair function, hydrocephalus appears to contribute meaningfully, the patient’s overall health permits intervention, and expectations are realistic. The strongest situation is when gait disturbance is prominent, MRI findings support hydrocephalus, degenerative or vascular disease does not clearly dominate, and functional testing after CSF removal suggests reversibility. Surgery is less likely to help when symptoms are mainly due to advanced dementia, severe brain atrophy, vascular brain injury, medication effects, or other irreversible conditions. The decision should not be based only on enlarged ventricles. It requires integrated interpretation of clinical course, neurological examination, cognitive testing, MRI, medication review, tap test or drainage response, and surgical risk.
Why are programmable shunt valves preferred in older patients with suspected NPH?
Programmable shunt valves are preferred because they allow non-invasive adjustment of cerebrospinal fluid drainage after surgery. In older patients with suspected normal pressure or chronic communicating hydrocephalus, the ideal drainage level is often not obvious at the time of surgery. If drainage is too low, symptoms may not improve; if drainage is too strong, overdrainage can cause headaches, dizziness, or subdural fluid collections. A programmable valve allows the surgeon to start at a safer higher pressure and then gradually lower the setting if symptoms persist and no complications occur. Adjustments are made externally with a programming device, without another operation. This turns treatment into a controlled, stepwise process guided by gait, cognition, urinary symptoms, and imaging when needed.
What complications can occur after VP shunt surgery for NPH?
VP shunt surgery is a standard neurosurgical procedure, but it is not risk-free. Possible complications include overdrainage, underdrainage, shunt blockage, infection, subdural fluid collections or bleeding, abdominal catheter problems, and the need for later revision. Overdrainage may cause headaches, dizziness, or subdural collections because too much CSF is drained. Underdrainage may result in limited or absent improvement. Infection or blockage may require treatment or additional surgery. Programmable valves reduce some risks by allowing pressure adjustment without another operation, but they do not eliminate complications. This is why patient selection is crucial. Surgery should be considered only when the probability of meaningful benefit, especially gait improvement, justifies the procedural and long-term management risks.
Why do doctors sometimes disagree about diagnosis or shunt surgery in suspected NPH?
Doctors may disagree because suspected NPH is rarely a simple yes-or-no diagnosis. MRI findings are not self-explanatory, symptoms overlap with dementia and vascular brain disease, and no single test can prove that shunt surgery will help. One specialist may focus on enlarged ventricles and gait impairment and consider hydrocephalus potentially reversible. Another may focus on severe brain atrophy, Alzheimer-type features, vascular changes, medication effects, frailty, or limited tap test response and recommend caution. Both perspectives may be reasonable because treatment benefit is probabilistic. The decision depends on how clinical symptoms, imaging, cognitive profile, medication effects, functional testing, and surgical risk are weighed together. This is why experienced integrated review is often valuable.
When is a neurosurgical second opinion useful in suspected normal pressure hydrocephalus?
A neurosurgical second opinion is useful when MRI shows enlarged ventricles together with brain atrophy or ischemic changes, when symptoms overlap with dementia, or when doctors disagree about whether hydrocephalus is clinically relevant. It is especially helpful if a lumbar tap test is proposed, if the result is inconclusive, or if VP shunt surgery is being considered but expected benefit remains unclear. Review can also help when medications such as sedatives, antidepressants, or antipsychotics may be worsening gait or cognition and confusing the assessment. The goal is not simply to label the MRI as NPH, but to estimate whether hydrocephalus meaningfully contributes to symptoms, whether further testing is justified, and what improvement can realistically be expected.
How can doctors tell whether enlarged ventricles are caused by brain atrophy or hydrocephalus?
Doctors cannot reliably distinguish brain atrophy from clinically relevant hydrocephalus by ventricle size alone. In older patients, MRI often shows both enlarged ventricles and widened cortical spaces, together with ischemic white-matter changes. Ventricles may enlarge because cerebrospinal fluid absorption is impaired, but they may also enlarge passively when brain volume is lost through atrophy. The distinction depends on whether symptoms match a hydrocephalus pattern, especially early gait disturbance, frontal-subcortical cognitive slowing, and urinary urgency. MRI signs are interpreted together with neurological examination, cognitive profile, medication effects, disease progression, and response to temporary CSF removal. The key question is not whether ventricles are enlarged, but whether hydrocephalus is a meaningful and potentially reversible contributor to symptoms.
When should incidental ventriculomegaly on brain MRI be monitored rather than treated?
Incidental ventriculomegaly is usually monitored rather than treated when enlarged ventricles are found on MRI but the patient has no clear gait disturbance, cognitive decline, or urinary dysfunction consistent with normal pressure hydrocephalus. In this situation, immediate lumbar puncture or shunt surgery is usually not appropriate. Instead, clinicians track early changes in walking, balance, turning, attention, executive function, and urinary urgency. A baseline gait and cognitive assessment can be useful, especially when ventricular enlargement is pronounced or borderline symptoms exist. Follow-up is often clinical, with repeat imaging only if symptoms change. Treatment becomes relevant only if the clinical picture begins to suggest that hydrocephalus is contributing to functional decline.
What should be done if the lumbar tap test for suspected NPH is inconclusive?
If a lumbar tap test is inconclusive, the result should not be interpreted in isolation. First, the test conditions should be reviewed: whether baseline gait and cognition were measured objectively, whether reassessment occurred at the right time, and whether fatigue, medication effects, pain, infection, or day-to-day variability may have influenced the result. In some patients, repeating the tap test under standardized conditions can reveal subtle or delayed improvement. If uncertainty remains and the clinical suspicion is still meaningful, extended lumbar CSF drainage over several days may provide stronger prognostic information because walking and function can be observed repeatedly during drainage. The decision should still integrate imaging, clinical pattern, comorbidities, and surgical risk.
Public awareness note: Public attention to normal pressure hydrocephalus increased in 2025 after musician Billy Joel publicly disclosed an NPH diagnosis. Celebrity cases can help families recognize that NPH is a real and often misunderstood condition, but diagnosis and treatment decisions should always depend on the patient’s own symptoms, MRI findings, neurological examination, response to CSF drainage testing, and overall medical condition.
Additional Resources for Patients & Caregivers
For more detailed information on Normal Pressure Hydrocephalus, brain atrophy, and dementia, we recommend exploring the following reputable sources:
- Hydrocephalus Association: Understanding Normal Pressure Hydrocephalus (NPH)
- Mayo Clinic: Hydrocephalus Symptoms, Causes, and Diagnosis
- Johns Hopkins Medicine: Normal Pressure Hydrocephalus: An Overview
- Alzheimer’s Association: Comparing NPH and Other Types of Dementia
- National Institute of Neurological Disorders and Stroke (NIH): Hydrocephalus Information Page