Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
February 28, 2026
Who This Spinal Tumors Page Is For
This page is intended for patients who have been diagnosed with a spinal tumor or an unclear spinal lesion on MRI or CT imaging, as well as for family members seeking a clear and structured explanation of what such findings may mean and how treatment decisions are typically made.
Spinal tumors often raise urgent and complex questions — whether the finding represents a benign tumor, metastatic disease, or compression of the spinal cord requiring timely treatment. Many patients encounter conflicting medical opinions regarding surgery, radiotherapy, or observation. You are not expected to read this page from beginning to end. Instead, you may return to specific sections if new symptoms appear, neurological function changes, or treatment options are proposed.
If surgery has been recommended, radiotherapy is being considered, or imaging findings seem difficult to interpret, an individualized neurosurgical second opinion may help clarify diagnosis, urgency of treatment, and the safest therapeutic strategy based on tumor type, neurological status, and overall medical condition.
When patients seek a second opinion for spinal tumors
• A spinal tumor or suspicious lesion has been detected on MRI, but its nature or urgency remains unclear
• Surgery has been proposed without clear explanation of risks, expected recovery, or alternative treatments
• Radiotherapy or oncological treatment is recommended, but it is uncertain whether surgical decompression should be performed first
• Progressive weakness, walking difficulty, or bladder symptoms raise concern about spinal cord compression
• Different specialists recommend observation, surgery, or radiation therapy
• Symptoms persist or worsen after previous tumor treatment or spinal surgery
Not every spinal tumor requires immediate surgery, but delayed treatment in cases of spinal cord compression may lead to permanent neurological deficit.
When diagnosis, treatment sequence, or urgency remain uncertain, careful neurosurgical evaluation is essential.
If your situation involves uncertainty regarding diagnosis or treatment strategy, you may request an individualized neurosurgical review here:
Request Second Opinion
Spinal Tumors — Quick Summary (Read This First)
- Spinal tumors are abnormal growths located within or around the spinal cord, nerve roots, or vertebrae. Their clinical impact depends on location and size.
- Metastatic disease represents the most common spinal tumors in adults. Many cancers originating elsewhere in the body may spread to the spine, most commonly lung, breast, prostate, kidney, and thyroid cancers, which together account for the majority of spinal metastatic lesions.
- Symptoms usually develop gradually. Persistent back pain, radiating pain, numbness, weakness, or walking difficulty may appear as neural structures become compressed.
- Progressive neurological symptoms may indicate spinal cord compression. Weakness, balance problems, or bladder dysfunction require urgent medical evaluation.
- MRI with contrast is the key diagnostic examination. It determines tumor location, relationship to neural structures, and treatment planning.
- Not all spinal tumors require immediate surgery. Treatment may include observation, surgery, radiotherapy, systemic oncological therapy, or combined approaches.
- Treatment decisions are multidisciplinary. Neurosurgeons, oncologists, and radiation specialists jointly determine optimal timing and sequence of therapy.
- The spinal cord has limited tolerance to compression and radiation. Early decompression significantly improves chances of neurological recovery.
- Neurological outcome depends strongly on timing. Patients treated before severe weakness or loss of walking ability generally recover better.
- The primary goals of treatment are preservation of neurological function, spinal stability, and tumor control.
- This page provides a structured overview. Use the Contents section to navigate directly to diagnosis, treatment options, prognosis, or specific tumor types.
Most readers benefit from reviewing the Quick Summary together with the sections on Symptoms of Spinal Tumors, Diagnosis, and Treatment Strategy. Later sections provide deeper clinical detail for patients seeking a comprehensive understanding of spinal tumor management.
Contents
- Who This Spinal Tumors Page Is For
- Quick Summary
- Anatomy of the Spine
- Types of Spinal Tumors
- Causes of Spinal Tumor Development
- Biological Behavior and Growth Patterns
- Symptoms
- Diagnosis
- Surgical Treatment
- Radiation & Chemotherapy
- Prognosis
- Specific Types of Spinal Tumors
- Spinal Meningioma
- Spinal Schwannoma
- Intramedullary Gliomas
- Vertebral Tumors
- Spinal Metastases
- Request Second Opinion
- FAQs
Spinal tumors are usually classified according to their anatomical location:
• intramedullary tumors (inside the spinal cord)
•intradural-extramedullary tumors (inside the dura but outside the cord)
• extradural tumors (most commonly vertebral tumors or metastases)
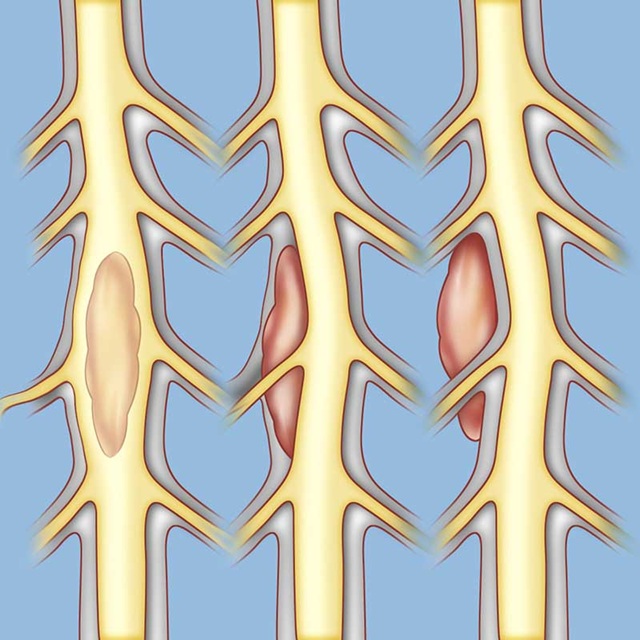
Image: Spinal tumors can be located in three different areas (from left to right): intramedullary (inside the spinal cord, e.g., ependymoma or astrocytoma), intradural-extramedullary (inside the spinal membrane but outside the cord, e.g., meningioma or schwannoma), or extradural (outside the spinal membrane, e.g., bone metastases or vertebral tumor).
Anatomy of the Spine
The spine consists of 5 main regions: cervical, thoracic and lumbar spine, sacrum and coccyx (tailbone)
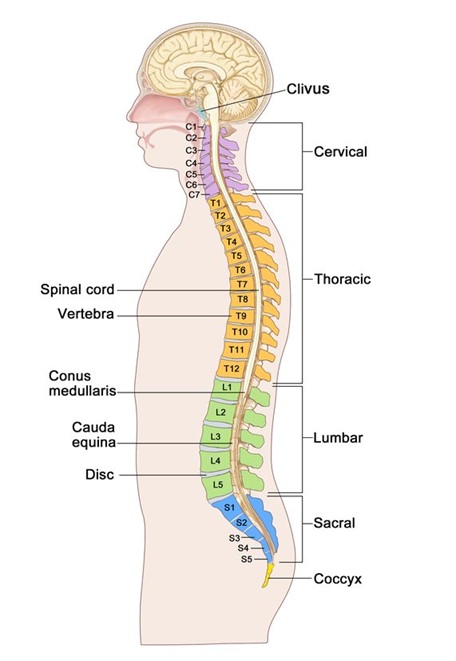
Image: Regions of the spine: cervical (neck), thoracic (mid-back), lumbar (lower back), sacral, and coccygeal (tailbone). Inside the spine is the spinal canal, which houses the spinal cord. The spinal cord ends at the level of the L1 vertebra, so the spinal canal of the lumbosacral region contains only nerve roots (either individually or as the cauda equina). Learn more on our Spine Anatomy page.
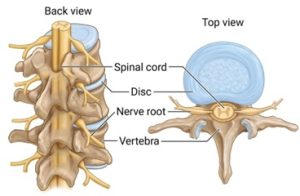
Image: The spine is composed of vertebrae stacked one on top of the other. Inside, these bones form the spinal canal, which acts as a protective tunnel. The spinal cord and the nerve roots that branch off from it pass through this canal.
Types of Spinal Tumors
According to localization, spinal tumors may be divided into:
- tumors originating from the vertebra (anterior or posterior parts of the vertebra) — most commonly chondroma, osteoma, osteoid osteoma, and chordoma
- tumors growing within the dural sac but outside the spinal cord — most commonly schwannoma or neurinoma (arising from a spinal nerve root) and meningioma (arising from the dura mater)
- tumors growing within the spinal cord — most commonly astrocytomas and ependymomas
Many malignant tumors originating from other organs may metastasize to the spine. Metastatic disease accounts for approximately 70–80% of all tumors involving the spine in adults, making spinal metastases the most common spinal tumors overall. Vertebral metastases are frequently detected on skeletal scintigraphy (bone scan).
Causes of Spinal Tumor Development
Spinal tumors, like other tumors in the body, arise as a result of genetic alterations occurring within normal cells. Some genes become activated (proto-oncogenes transforming into oncogenes), while others become inactivated (tumor suppressor genes).
Such changes occur continuously in many cells. Immune surveillance mechanisms normally recognize and eliminate many abnormal cells, but occasionally altered cells escape this control and continue to proliferate, leading to tumor formation. Some tumors remain benign, while others may acquire additional genetic alterations associated with more aggressive biological behavior.
The precise causes of these genetic changes are not always known. They may occur spontaneously or be associated with exposure to ionizing radiation, certain environmental factors, or prior medical treatments. For most spinal tumors, however, no single identifiable cause can be established.
Most spinal tumors are not inherited. Nevertheless, certain rare genetic syndromes (such as neurofibromatosis) may increase susceptibility to tumor development. In the general population, a family history of malignant disease may reflect shared genetic or environmental risk factors rather than direct inheritance.
Biological Behavior and Growth Patterns of Spinal Tumors
Spinal tumors may be broadly classified as benign or malignant based on their biological behavior and growth characteristics.
According to their pattern of growth, tumors may:
- compress surrounding neural structures, as seen in meningiomas, schwannomas, and many metastatic lesions
- infiltrate neural tissue, which is typical of intramedullary tumors such as astrocytomas and ependymomas
- demonstrate combined growth characteristics, with both compression and infiltration
Symptoms of Spinal Tumors
When a spinal tumor reaches sufficient size, it may compress the spinal cord and nerve roots, leading to swelling, impaired blood circulation, and occasionally hemorrhage within neural tissue. Spinal tumors — particularly metastatic lesions — may also weaken vertebral bone and cause pathological fractures. These fractures can result in spinal instability and additional compression of neural structures within the spinal canal.
Symptoms typically develop gradually and may include:
Local spinal symptoms
- persistent back or neck pain, often worsening at night or during rest
Radicular symptoms
- pain radiating into the arms, chest, abdomen, or legs
- numbness or sensory disturbances
Spinal cord compression symptoms
- weakness of the arms and/or legs
- difficulty walking or loss of coordination
- bladder or bowel dysfunction
Rarely, tumors affecting the upper cervical spine may lead to breathing difficulties.
Benign tumors often produce mild symptoms that remain stable for months or even years despite slow growth. Additional neurological deficits usually appear only after significant tumor enlargement.
Diagnosis of Spinal Tumors
Because small tumors are generally easier to treat than advanced lesions, early diagnosis is essential.
Spinal tumors are usually suspected based on progressive neurological symptoms or persistent spinal pain that cannot be explained by degenerative disease.
Magnetic resonance imaging (MRI) with contrast enhancement is the most important diagnostic method and represents the standard examination when a spinal tumor is suspected. MRI allows precise visualization of tumor location, its relationship to the spinal cord and nerve roots, and the degree of neural compression.
The examination is painless and typically lasts 15–45 minutes. Some patients may require sedation due to discomfort or claustrophobia.
Additional diagnostic methods may include:
- spinal X-ray
- computed tomography (CT)
- electromyography (EMG)
- somatosensory evoked potentials (SSEP)
- skeletal scintigraphy (bone scan)
Once a spinal tumor is identified, evaluation of other organs is required to determine whether the lesion represents a primary tumor or metastatic disease. Preoperative assessment typically includes laboratory testing, ECG, chest imaging, abdominal ultrasound, and internal medicine evaluation.

Image: Spinal MRI shows a spinal cord tumor (ependymoma – red arrow) which causes cysts to form within the cord both above and below the tumor (yellow arrow).
Surgical Treatment of Spinal Tumors
The decision to perform surgery depends on several factors, including tumor type, location, rate of progression, neurological impairment, and overall patient condition. The primary goals of surgery are decompression of neural structures, preservation or restoration of neurological function, and, whenever possible, complete tumor removal.
If the tumor is non-malignant and non-infiltrative, the goal is complete surgical excision.
When tumors infiltrate vertebrae or surrounding tissues, adjacent tissues may also require removal. Tumors infiltrating the spinal cord itself cannot usually be completely excised without unacceptable neurological damage, and treatment strategies must balance tumor control with functional preservation.
Surgical approaches may be anterior or posterior, depending on tumor location.
Two main procedures include:
- laminectomy — removal of the posterior vertebral elements
- corpectomy — partial or complete removal of the vertebral body
If tumor removal results in spinal instability, stabilization procedures are performed.
In cases of metastatic vertebral collapse causing pathological fracture, minimally invasive vertebroplasty may be performed. Bone cement is injected into the vertebral body to restore stability and reduce pain without removing the tumor.
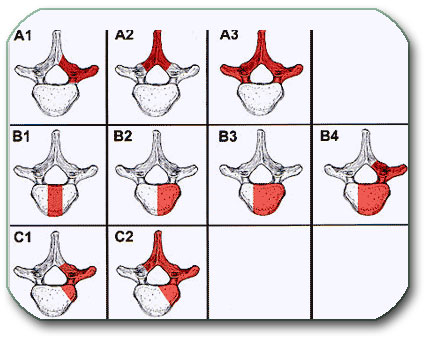
Image: Figures A1–3 show different degrees of vertebral lamina removal (laminectomy); figures B show various degrees of vertebral body removal (corpectomy). Figures C represent a combination of both surgical procedures.
Radiation Therapy and Chemotherapy
Adjuvant treatment of spinal tumors may include radiotherapy and systemic oncological therapy, depending on tumor type and biological behavior.
Treatment decisions are typically made within a multidisciplinary oncology team, involving neurosurgeons, oncologists, radiation oncologists, and other specialists. In metastatic disease, therapy largely depends on the characteristics of the primary tumor and its sensitivity to radiation or systemic treatment.
Modern radiation devices deliver high-precision doses measured in Gray (Gy). Radiosurgical techniques such as Gamma Knife or LINAC systems may effectively control tumor growth when lesions are relatively small (approximately 2.5–3 cm) and safely distant from radiation-sensitive neural structures. The spinal cord has a limited tolerance to radiation exposure, which must always be carefully considered during treatment planning. For this reason, surgical decompression is often required before radiotherapy when significant spinal cord compression is present.
Radiotherapy is commonly used after surgery to control residual tumor tissue or to prevent further progression when complete removal is not possible.
Systemic therapies, including chemotherapy, targeted therapy, or immunotherapy, are selected according to the primary malignancy rather than the spinal location itself.
Why Treatment Recommendations for Spinal Tumors Often Differ — What Actually Determines the Decision
Different treatment recommendations for spinal tumors do not occur because one opinion is right and another is wrong, but because the decision depends on several critical factors that may be interpreted differently depending on clinical perspective.
The key issue is not only what the tumor is, but how it behaves, what it is doing to the spinal cord, and how urgent the situation is.
Is The Tumor Causing Spinal Cord Compression Or Is It An Incidental Finding
A tumor that compresses the spinal cord and causes weakness, walking difficulty, or bladder dysfunction usually requires urgent decompression. In contrast, a tumor discovered incidentally on MRI without neurological deficit may be safely observed. This is one of the most common reasons why one specialist recommends surgery while another suggests monitoring.
What Is The Biological Nature Of The Tumor — Benign, Malignant, Or Metastatic
Treatment strategy differs significantly depending on tumor type.
Benign tumors such as meningioma or schwannoma are often treated surgically with curative intent.
Intramedullary tumors may not be fully resectable without neurological risk.
Metastatic tumors are often treated with a combination of surgery, radiotherapy, and systemic therapy.
The same MRI finding may lead to completely different recommendations depending on tumor biology.
Are Neurological Symptoms Stable Or Progressively Worsening
Stable symptoms may allow time for additional evaluation or conservative management. However, progressive weakness, loss of walking ability, or new bladder dysfunction indicate an evolving spinal cord injury, where delay may result in permanent deficit. This is why surgeons often recommend earlier intervention compared to other specialists.
Should Treatment Begin With Surgery Radiotherapy Or Systemic Therapy
In some cases, surgery is required first to relieve spinal cord compression. In others, particularly in metastatic disease, radiotherapy or systemic oncological treatment may be the initial step. Different specialists may prioritize different treatment sequences based on their perspective.
What Is The Balance Between Tumor Control And Preservation Of Neurological Function
Aggressive tumor removal may increase the chance of oncological control, but also carries risk of neurological damage. More conservative approaches may preserve function but leave residual tumor. This balance is often interpreted differently, especially in complex or borderline cases.
How Urgent Is The Situation Immediate Intervention Or Careful Observation
The same tumor may be an emergency in a patient with rapid neurological decline, or a condition that can be monitored in a patient with stable symptoms. The perceived urgency is one of the key reasons why treatment recommendations differ.
Prognosis After Treatment of Spinal Tumors
Prognosis after treatment of spinal tumors should be considered from several perspectives.
Oncological prognosis (overall survival) primarily depends on the biological behavior of the tumor and, in metastatic disease, on the characteristics and stage of the primary malignancy.
Neurological prognosis depends largely on the degree and duration of spinal cord or nerve root compression before treatment. Patients treated before severe or prolonged neurological impairment generally achieve significantly better functional recovery.
Risk of tumor recurrence is influenced by tumor type, completeness of surgical removal, and the need for adjuvant therapies such as radiotherapy or systemic oncological treatment.
MRI findings, residual tumor presence, and response to treatment are important factors during long-term follow-up.
Specific Types of Spinal Tumors
Spinal tumors represent a heterogeneous group of lesions that differ significantly according to their anatomical location and biological behavior. The following overview summarizes the most common tumor types discussed in greater detail on dedicated pages.
Spinal Meningioma
Arises from the dura mater within the spinal canal. Symptoms include pain, weakness, and numbness below tumor level. Surgical removal is usually complete with excellent recovery when diagnosed early.
Spinal Schwannoma (Neurinoma)
Originates from spinal nerve roots. Surgical removal is typically complete with favorable prognosis.
Intramedullary Gliomas (Astrocytoma, Ependymoma)
Located within the spinal cord and often associated with syringomyelia. Some tumors infiltrate neural tissue and cannot be fully removed. Malignant variants occur more frequently than in meningiomas or neurinomas but less often than in brain gliomas.
Vertebral Tumors
May involve anterior or posterior vertebral structures and cause spinal instability or pathological fractures. Treatment is primarily surgical with stabilization when necessary.
Spinal Metastases
Spinal metastases represent the most common tumors affecting the spine in adults, accounting for approximately 60–70% of all spinal tumor cases. They occur when cancer originating in another organ — most commonly the lung, breast, prostate, kidney, or thyroid — spreads to the vertebrae or spinal canal.
Patients typically present with progressive back pain, pathological vertebral fractures, spinal instability, or signs of spinal cord or nerve root compression. Treatment usually requires a multidisciplinary approach involving neurosurgery, oncology, and radiation therapy, depending on neurological status and the biological behavior of the primary tumor.
Request Spinal Tumor Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Being told that a spinal tumor or a suspicious spinal lesion is present on MRI or CT can raise urgent, high-stakes questions:
Is this likely a benign tumor or metastatic disease? Is there spinal cord compression that requires timely treatment?
Should treatment start with surgery, radiation therapy, systemic oncology treatment, or careful observation?
An independent neurosurgical second opinion can help clarify the most likely diagnosis, the urgency of treatment,
and the safest therapeutic strategy based on imaging findings, neurological status, spinal stability, and overall medical condition.
- ✔ Send a brief message describing your main symptoms (pain, weakness, walking difficulty, numbness, bladder/bowel symptoms) and what your MRI/CT report states
- ✔ You’ll receive a reply within 24 hours explaining whether we can help with an online consultation and what documentation is needed
- ✔ Priority cases: progressive weakness, new walking difficulty, bladder/bowel dysfunction, suspected spinal cord compression, or rapidly worsening pain — write PRIORITY in your first message
- ✔ MRI images (DICOM) and radiology reports can be reviewed once initial contact is established (CT and PET/CT reports are also helpful when metastases are suspected)
- ✔ During the consultation, we explain the likely tumor compartment (intramedullary vs. intradural-extramedullary vs. extradural), treatment sequence (surgery vs. radiation vs. systemic therapy vs. observation), expected neurological recovery, risks, and realistic next steps — with up to 10 days of follow-up for clarification questions
Consultation fees typically range from $180–250, depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth neurosurgical second opinions.
Frequently Asked Questions About Spinal Tumors
What is a spinal tumor?
A spinal tumor is an abnormal growth located within or around the spinal cord, nerve roots, spinal membranes, or vertebrae. Some spinal tumors grow inside the spinal cord, some develop inside the spinal canal but outside the cord, and others arise from the vertebral bones or spread there from cancer elsewhere in the body. The clinical importance of a spinal tumor depends less on the name alone and more on its location, biological behavior, size, growth rate, and effect on the spinal cord or nerve roots. Even a benign spinal tumor can become serious if it causes compression, weakness, walking difficulty, bladder dysfunction, or spinal instability.
Are most spinal tumors cancerous or metastatic?
In adults, many spinal tumors are metastatic, meaning that cancer from another organ has spread to the spine, most often from lung, breast, prostate, kidney, or thyroid cancer. However, not every spinal tumor is cancerous. Benign tumors such as spinal meningiomas and schwannomas are also common inside the spinal canal, and some spinal cord tumors are low grade or slow growing. The distinction is important because treatment differs greatly. A benign compressive tumor may be treated surgically with curative intent, while metastatic spinal disease often requires a combination of surgery, radiotherapy, and systemic oncological treatment. MRI appearance, medical history, CT/PET findings, and sometimes biopsy help clarify the diagnosis.
What are the main types of spinal tumors by location?
Spinal tumors are mainly classified by where they are located, because location determines symptoms, urgency, treatment options, and prognosis. Intramedullary tumors grow inside the spinal cord itself and include ependymomas and astrocytomas. Intradural-extramedullary tumors grow inside the spinal membrane but outside the spinal cord, commonly meningiomas or schwannomas. Extradural tumors are located outside the dura, most often in the vertebrae or epidural space; these are frequently metastatic tumors in adults. A tumor inside the cord, around the nerve roots, or in the vertebral body creates different surgical risks and treatment priorities. This is why MRI localization is one of the first steps in spinal tumor evaluation.
What symptoms can spinal tumors cause?
Spinal tumors can cause persistent back or neck pain, pain radiating into the arms, chest, abdomen, or legs, numbness, tingling, weakness, walking difficulty, balance problems, or bladder and bowel dysfunction. The exact symptom pattern depends on tumor location and whether the spinal cord, nerve roots, vertebral bone, or spinal stability is affected. Tumors in the cervical spine may affect arms and legs, thoracic tumors may cause band-like trunk pain or walking difficulty, and lumbar or sacral tumors may produce leg pain or pelvic symptoms. Symptoms often develop gradually, but progressive weakness, new walking difficulty, or bladder changes may indicate spinal cord compression and require urgent medical assessment.
Is back pain alone a sign of a spinal tumor?
Back pain alone is rarely enough to diagnose a spinal tumor, because most back pain is caused by degenerative spine disease, muscle strain, disc problems, or joint-related pain. However, certain patterns raise concern. Persistent pain that worsens at night or at rest, pain that progressively increases, pain associated with cancer history, unexplained weight loss, fever, neurological symptoms, or new weakness should be evaluated carefully. A spinal tumor may also cause pain that does not behave like ordinary mechanical back pain. The key is not to assume every back pain is dangerous, but also not to ignore pain that is persistent, unexplained, progressive, or accompanied by neurological change.
When do spinal tumor symptoms suggest spinal cord compression?
Spinal tumor symptoms suggest spinal cord compression when pain is accompanied by progressive weakness, walking difficulty, balance problems, stiffness in the legs, numbness below a certain level, loss of coordination, or bladder and bowel dysfunction. These symptoms mean that the spinal cord or nerve pathways may be under pressure or losing function. In metastatic disease, vertebral collapse or epidural tumor extension may compress the spinal cord quickly. In benign tumors, compression may develop more slowly but still become serious if treatment is delayed. New or worsening neurological symptoms should not be managed as ordinary back pain. They require prompt MRI assessment and neurosurgical or oncological evaluation.
What is the best imaging test for diagnosing spinal tumors?
Contrast-enhanced MRI is the most important imaging test for diagnosing spinal tumors. MRI shows the tumor’s exact level, whether it is inside the spinal cord, around the nerve roots, inside the dura, in the epidural space, or in the vertebrae. It also shows spinal cord compression, nerve-root involvement, edema, cysts, syringomyelia, and relationship to nearby structures. CT is useful when bone destruction, vertebral collapse, calcification, or surgical stabilization must be assessed. PET/CT, bone scan, or systemic imaging may be needed when metastasis is suspected. In some cases, imaging suggests the likely diagnosis, but tissue biopsy or surgical pathology is needed to confirm tumor type.
How does MRI show where a spinal tumor is located?
MRI helps determine whether a spinal tumor is intramedullary, intradural-extramedullary, or extradural. An intramedullary tumor expands the spinal cord from within and may be associated with cord swelling, cysts, syrinx formation, or abnormal enhancement. An intradural-extramedullary tumor lies inside the spinal membrane but outside the cord, usually displacing the spinal cord or nerve roots from the outside. An extradural tumor is outside the dura, often involving vertebral bone, epidural space, or metastatic disease. This distinction matters because treatment strategy is different in each group. MRI localization helps decide whether observation, surgery, decompression, radiotherapy, systemic therapy, biopsy, or stabilization is most appropriate.
Do all spinal tumors require surgery?
No. Not all spinal tumors require surgery. Some benign or incidentally detected spinal tumors may be monitored with periodic MRI if neurological function is preserved, symptoms are mild, and there is no dangerous spinal cord compression or instability. Other tumors may be treated primarily with radiotherapy, systemic oncological therapy, or combined treatment. Surgery becomes more important when the tumor causes progressive neurological symptoms, spinal cord or nerve-root compression, vertebral instability, pathological fracture, severe pain, or uncertain diagnosis requiring tissue confirmation. The decision depends on tumor location, biological behavior, patient condition, expected recovery, and whether surgery would improve neurological function, stability, diagnosis, or tumor control.
When is spinal tumor surgery urgent?
Spinal tumor surgery is urgent when a tumor causes progressive spinal cord compression, rapidly worsening weakness, new walking difficulty, loss of balance, bladder or bowel dysfunction, or spinal instability from vertebral collapse. These symptoms may indicate that the spinal cord is being injured and that delay could lead to permanent neurological deficit. In metastatic disease, surgery may be needed before radiotherapy if the spinal cord is significantly compressed or if the spine is unstable. In benign tumors, urgency depends on symptom progression and degree of compression. The goal of urgent surgery is usually decompression, preservation of walking ability, pain control, stabilization, and prevention of irreversible spinal cord injury.
Can spinal tumors be treated with radiation instead of surgery?
Some spinal tumors can be treated with radiotherapy instead of surgery, but this depends on tumor type, spinal cord compression, neurological status, and spinal stability. Radiotherapy may be appropriate for radiosensitive tumors, residual tumor after surgery, recurrent disease, or metastatic lesions without severe mechanical compression or instability. However, if a tumor is already compressing the spinal cord and causing neurological decline, surgery may be needed first to decompress neural structures before radiation. The spinal cord has limited tolerance to radiation, so treatment planning must be precise. Radiation is not simply interchangeable with surgery; the correct sequence depends on whether the main problem is tumor control, compression, instability, pain, or systemic cancer treatment.
How do doctors decide between spinal tumor surgery, radiotherapy, systemic therapy, and observation?
Doctors decide between spinal tumor surgery, radiotherapy, systemic therapy, and observation by assessing several factors together. These include tumor location, suspected tumor type, degree of spinal cord or nerve-root compression, neurological symptoms, spinal stability, tumor growth, cancer history, general health, and treatment goals. A stable benign tumor may be observed. A compressive benign tumor may be removed surgically. A metastatic vertebral tumor may require surgery, radiotherapy, systemic therapy, or a staged combination. If the spine is unstable, stabilization may be necessary. If the diagnosis is uncertain, biopsy or surgery may be needed. Different specialists may emphasize different risks, which is why treatment recommendations sometimes differ.
What determines prognosis after spinal tumor treatment?
Prognosis after spinal tumor treatment depends on tumor type, biological behavior, location, extent of removal, response to radiotherapy or systemic treatment, and neurological condition before treatment. In metastatic spinal tumors, overall survival depends mainly on the primary cancer type, stage, systemic disease control, and response to oncology treatment. In benign spinal tumors, prognosis is often favorable when the tumor can be removed safely before severe neurological damage develops. Neurological prognosis depends strongly on how long the spinal cord or nerve roots were compressed before treatment. Patients treated before loss of walking ability, severe weakness, or bladder dysfunction usually have better functional recovery than patients treated after advanced deficits develop.
Can neurological function recover after spinal tumor compression of the spinal cord?
Neurological function can recover after spinal tumor compression of the spinal cord, but recovery depends on severity and duration of compression, tumor type, speed of symptom progression, and neurological status before treatment. If compression is treated before permanent spinal cord damage develops, weakness, walking difficulty, numbness, or coordination problems may improve substantially. Recovery may occur over weeks or months. However, long-standing severe weakness, loss of walking ability, marked spasticity, or bladder dysfunction may recover only partially or may become permanent. This is why timing is important. The goal is not only tumor treatment, but also preservation of neurological independence before spinal cord reserve is exhausted.
Can a spinal tumor recur after treatment?
Yes. A spinal tumor can recur after treatment, but recurrence risk depends on tumor type, biology, completeness of removal, and whether radiotherapy or systemic treatment was needed. Benign tumors such as meningiomas or schwannomas have lower recurrence risk after complete removal, although recurrence can still occur after subtotal resection or in complex locations. Intramedullary tumors may recur depending on tumor grade and extent of safe removal. Metastatic spinal tumors may progress because systemic cancer remains active. Follow-up MRI is important to distinguish stable postoperative change from residual or recurrent tumor. Recurrence may be managed with observation, repeat surgery, radiotherapy, systemic therapy, or combined treatment depending on the situation.
Can I obtain an online neurosurgical second opinion for a spinal tumor?
Yes. An online neurosurgical second opinion may be useful when MRI or CT shows a spinal tumor, spinal lesion, vertebral metastasis, spinal cord compression, intramedullary tumor, meningioma, schwannoma, or unclear finding. A review can help clarify the likely tumor compartment, urgency, need for surgery, role of radiotherapy, spinal stability, expected neurological recovery, and whether observation is safe. It is especially helpful when different specialists recommend different treatment sequences or when surgery, radiation, or systemic therapy has been proposed without clear explanation. The most useful documents include MRI images in DICOM format, radiology reports, CT or PET/CT reports when available, cancer history, symptoms, and neurological status.