Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Neurosurgeon and Pain Management Specialist
Specialized Experience:
30 years of clinical expertise in neurosurgery and neurocritical care.
Last medically reviewed:
June 03, 2026
What Acute Hydrocephalus Means (Simple Definition)
Acute hydrocephalus is a sudden buildup of cerebrospinal fluid (CSF) inside the brain’s ventricles.
Because the skull cannot expand, the enlarged ventricles increase pressure inside the head (ICP) and can quickly affect consciousness. In chronic hydrocephalus, where the ventricles enlarge gradually, the brain has time to partially accommodate at the beginning, so deterioration occurs over weeks or months. In acute hydrocephalus, there is no time for accommodation, so deterioration happens over minutes or hours and represents an emergency.
The condition is most often caused by situations that suddenly block the flow of cerebrospinal fluid (CSF) within the ventricles, such as intraventricular hemorrhage (IVH) and hemorrhages near the CSF pathways. These forms of CSF blockage are most frequent in traumatic brain injury (TBI) , subarachnoid hemorrhage (SAH) due to an aneurysmal rupture, or intracerebral hemorrhage (ICH).

Image: Comparison of normal and enlarged brain ventricles in hydrocephalus. Read more about the anatomy of brain ventricles.
Why Acute Hydrocephalus Is Dangerous
When CSF cannot circulate normally, it collects in the ventricles, making them enlarge. As they expand, they compress the surrounding brain tissue.
This can lead to:
- decreased alertness or sudden coma,
- irregular breathing,
- pupillary changes,
- rapid ICP elevation,
- risk of brain herniation.
Changes can happen within minutes to hours, so early recognition is essential.
How Doctors Diagnose Acute Hydrocephalus
Diagnosis is made by:
- CT scan — enlarged ventricles, blood blocking the CSF pathways, compressed brain tissue,
- Neurological exam: Worsening consciousness, progressing to breathing changes and pupillary abnormalities in the comatose patient.
- ICP monitoring in selected severe cases.
Repeat CT scans are often performed if the patient’s condition changes suddenly.
How Acute Hydrocephalus Is Treated (Simple Overview)
Treatment focuses on lowering pressure and restoring CSF flow.
The most common emergency treatment is:
External Ventricular Drain (EVD)
A thin sterile tube placed into the ventricle that:
- drains excess CSF,
- measures intracranial pressure (ICP),
- allows CSF sampling when needed.
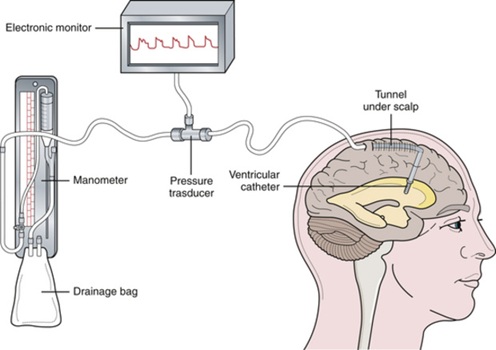
Image: External Ventricular Drain (EVD), which is used to drain excess Cerebrospinal Fluid (CSF) and monitor Intracranial Pressure (ICP).
EVD placement usually improves the patient’s condition within minutes to hours, depending on the severity.
A full explanation of how an EVD works is available here: External Ventricular Drain (EVD) — Simple Explanation
In rare cases where long-term CSF drainage is needed, a VP shunt may be placed after the acute phase stabilizes.
What Families Should Expect
Patients with acute hydrocephalus often experience:
- fluctuating wakefulness,
- rapid changes in responsiveness,
- improvement after CSF drainage, but sometimes gradual recovery.
The ICU team closely monitors:
- ICP trends,
- the amount of CSF drained,
- neurological exam changes,
- repeat CT scans to confirm improvement.
The first hours are often the most critical.
An online neurosurgical second opinion may help clarify how serious acute hydrocephalus is in this situation, whether CSF diversion is indicated, and what the usual next steps are.
Frequently Asked Questions about Acute Hydrocephalus
What does acute hydrocephalus mean?
Acute hydrocephalus means a sudden buildup of cerebrospinal fluid (CSF) inside the ventricles, the fluid spaces of the brain. Because the skull cannot expand, the enlarged ventricles can quickly increase intracranial pressure (ICP) and compress nearby brain tissue. Unlike chronic hydrocephalus, which develops slowly, acute hydrocephalus may worsen over minutes or hours. This is why doctors treat it as a neurocritical emergency, especially when consciousness, breathing, pupils, or CT findings are changing.
Why is acute hydrocephalus dangerous?
Acute hydrocephalus is dangerous because the sudden fluid buildup raises pressure inside the skull. High intracranial pressure (ICP) can reduce blood flow and oxygen delivery to the brain. As the ventricles enlarge, the patient may become sleepy, confused, unresponsive, or comatose. Breathing changes, pupil changes, worsening brain swelling, mass effect, or brain herniation may appear in severe cases. The danger is not only the size of the ventricles, but how quickly the patient is deteriorating.
How is acute hydrocephalus seen on CT scan?
Acute hydrocephalus is usually seen on CT scan as enlarged ventricles, sometimes with blood, tumor, swelling, or another blockage affecting the cerebrospinal fluid pathways. The CT may show that the ventricles are larger than expected, that CSF flow is blocked, or that surrounding brain tissue is compressed. Doctors compare CT findings with the neurological examination. A patient who is becoming more drowsy, has worsening pupils, or shows breathing changes may need urgent treatment even if the CT change seems subtle.
When does acute hydrocephalus require an external ventricular drain (EVD)?
Acute hydrocephalus may require an external ventricular drain (EVD) when enlarged ventricles are causing high intracranial pressure, reduced consciousness, worsening neurological signs, or blocked cerebrospinal fluid flow. An EVD is a thin sterile tube placed into the ventricle to drain excess CSF and measure ICP. It is commonly used when acute hydrocephalus follows intraventricular hemorrhage, subarachnoid hemorrhage, traumatic brain injury, infection, tumor obstruction, or postoperative swelling. The decision depends on CT findings and the patient’s clinical condition.
Can acute hydrocephalus improve after CSF drainage?
Acute hydrocephalus can improve after cerebrospinal fluid (CSF) drainage, especially when the main problem is pressure from blocked or trapped fluid. After an EVD starts draining, some patients become more awake, ICP may fall, and follow-up CT may show smaller ventricles. Improvement can happen within minutes to hours, but recovery is not always immediate. Outcome also depends on the cause of hydrocephalus, the severity of bleeding or swelling, brain injury, age, infection risk, and whether the brain can later maintain normal CSF circulation.
What is the difference between acute hydrocephalus and chronic hydrocephalus?
The main difference is speed. Acute hydrocephalus develops suddenly, often over minutes or hours, and can quickly raise intracranial pressure. It may cause rapid drowsiness, coma, breathing changes, pupil changes, or urgent CT findings. Chronic hydrocephalus develops more slowly, over weeks or months, so the brain may partially adapt at first. Chronic forms may cause gait problems, memory decline, urinary symptoms, or slowly progressive pressure effects. Acute hydrocephalus is usually treated as an emergency, while chronic hydrocephalus is evaluated more gradually.
If your family is dealing with one of these conditions, you may find these detailed guides helpful:
-
Traumatic Brain Injury (TBI) – diagnosis, treatment options, ICU phases, and recovery.
Read the full guide → -
Intracerebral Hemorrhage (ICH) – when surgery helps and what families should expect in the first days.
Family explanation → -
Ruptured Aneurysm & Subarachnoid Hemorrhage (SAH) – stabilization, treatment, ICU course, and prognosis.
Read more →