Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Consultant Neurosurgeon
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
February 28, 2026
Who This Astrocytoma Page Is For
This page is intended for patients diagnosed with astrocytoma, as well as for family members and caregivers who are seeking a clear, structured explanation of the disease, its biological behavior, and treatment options.
Readers are not expected to read this page from start to finish. Instead, you may return to specific sections over time — when MRI findings change, seizures occur, treatment decisions arise, or new questions appear during follow-up.
If treatment recommendations differ, it is unclear whether surgery, radiotherapy, or chemotherapy is needed, or if you want to better understand the long-term strategy and prognosis in your specific situation, an individualized neurosurgical second opinion can help clarify options and define a realistic, long-term treatment plan.
When patients and families seek a second opinion for astrocytoma
• It is uncertain whether surgery, biopsy, or observation is the safest next step
• There is doubt about the need for radiotherapy or chemotherapy (Temozolomide)
• Seizures are difficult to control, worsening, or it is unclear whether surgery could help
• MRI follow-up suggests that the tumor may be growing again, coming back, or that changes may be treatment-related
• The tumor may be growing again, and doctors are discussing another surgery, repeat biopsy, further treatment, or clinical trials
• Different specialists provide different or conflicting recommendations
• A clear long-term strategy, recurrence plan, and realistic prognosis are not well explained
In astrocytoma, decisions often depend on tumor grade, IDH status, MRI changes, seizure control, and whether the tumor may be growing again. An independent neurosurgical opinion can help clarify the safest next step.
If this reflects your situation, you may request an individualized neurosurgical review here:
Request Second Opinion
Astrocytoma — Quick Summary (Read This First)
- Astrocytoma is a diffuse infiltrative brain tumor (glioma). Tumor cells extend microscopically beyond what is visible on MRI, which means it cannot be completely separated from normal brain tissue.
- In adults, astrocytoma is defined by IDH mutation. To be classified as a diffuse astrocytoma of any grade (2–4), the tumor must carry an IDH mutation. IDH-wildtype diffuse tumors are generally classified as glioblastoma, even when they appear less aggressive on histology.
- In adults, it exists as a spectrum of grades (2–4), not separate diseases. Grade 2 tumors usually grow more slowly, grade 3 tumors show more active biological behavior, and grade 4 represents the most aggressive stage within the same disease continuum.
- Surgery is usually the first and most important treatment step, especially for Grade 2 tumors. Resection is not based on a clear boundary, but on removing all MRI-visible abnormal tissue (T2/FLAIR), often including an entire anatomical region when safe. In higher grades (3–4), surgery is still essential but is typically followed by additional oncologic treatment.
- MRI with contrast is the key diagnostic and follow-up tool. Grade 2 tumors often show little or no contrast enhancement, while grade 3 and especially grade 4 tumors more commonly enhance and may show necrosis and edema. However, MRI always underestimates the full microscopic extent of disease.
- Additional treatment depends strongly on tumor grade. Some patients with low-risk grade 2 astrocytoma may be observed after surgery. In grade 3 and grade 4 tumors, postoperative treatment is usually required and includes radiotherapy and Temozolomide.
- Radiotherapy and chemotherapy follow specific protocols. Grade 2 tumors are typically treated with approximately 50–54 Gy when indicated, while grade 3 and grade 4 tumors usually receive higher doses (~59–60 Gy) combined with Temozolomide (concurrent and adjuvant).
- The disease course varies widely depending on grade. Grade 2 astrocytomas often have a long course (commonly around 8–15+ years), grade 3 astrocytomas typically remain a long-survival disease compared with glioblastoma (often around 5–10 years), while grade 4 IDH-mutant astrocytoma is a serious malignant disease, although survival often extends to several years (commonly around 2–4 years).
- Seizures are common, especially in lower grades. They may be the first symptom and often improve after surgery, but may require long-term management. If epilepsy is the only indication for surgery in a stable MRI lesion suspected to be an astrocytoma, it is essential to confirm that the lesion is truly the source of seizures before proceeding.
- Long-term follow-up is essential. Even after treatment, astrocytoma can recur or progress over time, and regular MRI monitoring is required.
- This page is structured so you can read only what matters to you. Use the Contents box to navigate to sections on diagnosis, surgery, treatment, recurrence, and prognosis.
Most readers benefit from the Quick Summary plus the sections on Treatment, When Surgery Is Not Recommended, and Prognosis. The remaining sections provide deeper understanding.
Contents
- Who this is for
- Quick summary
- Definition
- Types of astrocytoma
- Not one disease
- Why IDH matters
- Why age matters
- Astrocytomas in children
- Diffuse astrocytoma in adults
- Grade 2
- Grade 3
- Grade 4
- Grade 4 vs glioblastoma
- How it develops
- Possible causes
- How astrocytoma damages the brain
- Functional status (KPS)
- How malignancy progresses over time
- Symptoms
- Seizures
- Diagnosis
- Differential diagnosis
- Histopathology and Molecular Analysis
- Treatment overview
- Symptomatic treatment
- Surgery
- When biopsy is preferred
- Radiotherapy & chemotherapy
- Grade 2 adjuvant therapy
- Grade 3 adjuvant therapy
- Grade 4 adjuvant therapy
- Observation only
- Prognosis
- MRI follow-up
- Recurrence
- Experimental treatments
- Why Do Experts Sometimes Disagree?
- FAQs
- Second opinion
This page focuses mainly on adult brain astrocytoma, especially IDH-mutant diffuse astrocytoma grades 2–4. Its main purpose is to help patients and families understand treatment decisions over time: when surgery is recommended, when biopsy or observation may be safer, when radiotherapy and Temozolomide are used, how MRI follow-up is interpreted, what recurrence or progression may mean, and how grade, molecular markers, seizures, functional status, and prior treatment shape prognosis.
What Is Astrocytoma?
Astrocytoma is a tumor that arises from astrocytic glial cells, a type of supportive cell in the brain. Glial cells normally help protect, nourish, and stabilize neurons (nerve cells). When astrocytic cells start to grow uncontrollably, they may form tumors with very different biological behaviors. Astrocytomas are one of the most common types of gliomas, a term frequently used in searches for brain tumors.
Astrocytomas can develop both in the brain and the spinal cord. For detailed information about spinal (intramedullary) astrocytomas, see: Intramedullary Spinal Cord Tumors.
From the patient’s perspective, the word astrocytoma can be misleading because it sounds like one diagnosis. In reality, it includes tumors that differ profoundly in:
- age group
- growth speed
- MRI appearance
- surgical strategy
- need for further treatment
- long-term prognosis
Some astrocytomas are relatively well circumscribed and behave in a more benign way. Others are diffuse gliomas, meaning they do not remain confined to a sharply defined mass, but infiltrate healthy brain tissue microscopically.
The classification used on this page follows the WHO CNS classification (World Health Organization Classification of Tumors of the Central Nervous System), an internationally accepted system that defines brain tumors based on both their microscopic appearance and molecular characteristics.
That is why a patient with a pilocytic astrocytoma and a patient with an astrocytoma, IDH-mutant, grade 4 do not in practice have the same disease, even though both tumors belong to the broad astrocytic family.
Gliomas as a group occur in approximately 4–6 cases per 100,000 people per year, with astrocytic tumors representing a substantial proportion of these cases.
This page focuses primarily on astrocytomas in adults. Pediatric astrocytomas represent a different group of diseases with distinct behavior and treatment principles.
How Many Types of Astrocytoma Exist?
According to the WHO classification, there are many distinct astrocytic tumor entities, reflecting different biological mechanisms, genetic alterations, and clinical behaviors.
In total, modern classifications recognize more than 20 different astrocytic and related tumor types, particularly when pediatric and rare tumors are included.
However, in adult clinical practice, most patients fall into a much smaller number of categories:
- Astrocytoma, IDH-mutant (grades 2–4)
- Glioblastoma, IDH-wildtype
This is why, although the classification appears complex, the majority of real-world treatment decisions are based on only a few key tumor types.
Why Astrocytomas Are Not a Single Disease
This is the single most important thing patients and families need to understand — astrocytoma is not one disease, but a group of biologically distinct tumors.
Older classifications focused mainly on how the tumor looked under the microscope and whether it was called low-grade, anaplastic, or glioblastoma. Modern classification goes further and combines:
- histology
- molecular markers
- clinical behavior
The most important molecular distinction in adult diffuse astrocytic tumors is IDH mutation status.
Why IDH Matters in Astrocytoma
Most genetic alterations make a tumor behave more aggressively. Interestingly, IDH mutation is one of the rare examples in oncology where a mutation may actually work partly in the patient’s favor. Tumors with IDH mutation usually grow more slowly and have a more favorable prognosis than comparable IDH-wildtype tumors (with a non-mutated IDH gene). To be classified as a diffuse astrocytoma in adults, regardless of grade (2–4), a tumor must have an IDH mutation.
For example:
- The highest grade 4 IDH-mutant astrocytoma is not the same disease as glioblastoma
- IDH-wildtype diffuse astrocytic tumors in adults are not classified as lower-grade astrocytomas. Even when classical high-grade histological features are absent, the presence of specific molecular alterations leads to their classification as glioblastoma (WHO grade 4).
Why Age Matters in Astrocytoma
Astrocytomas in children are often very different from astrocytomas in adults.
For example:
- many pediatric grade 1 astrocytomas may remain stable for years or be cured surgically
- adult diffuse astrocytomas usually infiltrate surrounding brain tissue and require a very different long-term strategy
For patients, the practical meaning is simple:
- the name on the pathology report
- the IDH status
- the MRI pattern
- and the clinical context
must always be interpreted together when making treatment decisions.
Astrocytomas in Children (Different Disease Group — Brief Context)
Astrocytic tumors in children represent a separate biological group and should not be directly compared with astrocytomas discussed later on this page.
In the current WHO CNS classification, pediatric gliomas are divided into several categories that include multiple distinct tumor entities, not a single disease.
These include:
- Pediatric-type diffuse low-grade gliomas
→ multiple tumor types (approximately 6–8 entities)
→ usually WHO grade 1–2 - Pediatric-type diffuse high-grade gliomas
→ several distinct tumor entities (around 4–6 types)
→ WHO grade 3–4 - Circumscribed astrocytic gliomas
→ 6 defined tumor types
→ most often WHO grade 1, but may include higher-grade variants
What This Means in Practice
- Pediatric astrocytic tumors include more than a dozen different tumor types overall
- They cover the full spectrum of WHO grades (1–4)
- They differ significantly in:
- growth pattern
- molecular biology
- clinical behavior
- treatment approach
Diffuse Astrocytoma in Adults (IDH-mutant, WHO Grades 2–4)
From this point onward, the discussion refers to astrocytomas in adults, which are predominantly diffuse infiltrative tumors with a different biology and clinical course compared to pediatric tumors.
In adults, the most clinically important astrocytic diffuse glioma group is Astrocytoma, IDH-mutant.
This is a biologically distinct family that includes:
- Grade 2 astrocytomas are often diagnosed in younger adults, commonly between 20–40 years
- Grade 3 astrocytomas tend to occur somewhat later, often in 30–50 years
- Grade 4 astrocytomas (IDH-mutant) are usually seen in adults between 30–60 years, although variability exists
These tumors usually arise through a pathway that is different from glioblastoma. They tend to occur in younger adults and often have a longer clinical course.
What “Diffuse” Means — Why These Tumors Grow Infiltratively
From a clinical perspective, diffuse astrocytomas do not grow as neatly encapsulated masses with sharp borders. Instead, they infiltrate the surrounding brain microscopically. In practical terms, this means that the visible tumor on MRI is not the entire disease.
Like a fog extending beyond the visible core, tumor cells may spread into surrounding tissue that appears only mildly abnormal or even normal on standard imaging.
This infiltrative behavior explains why surgery alone often cannot eradicate the disease completely, even when the visible lesion is removed very extensively.
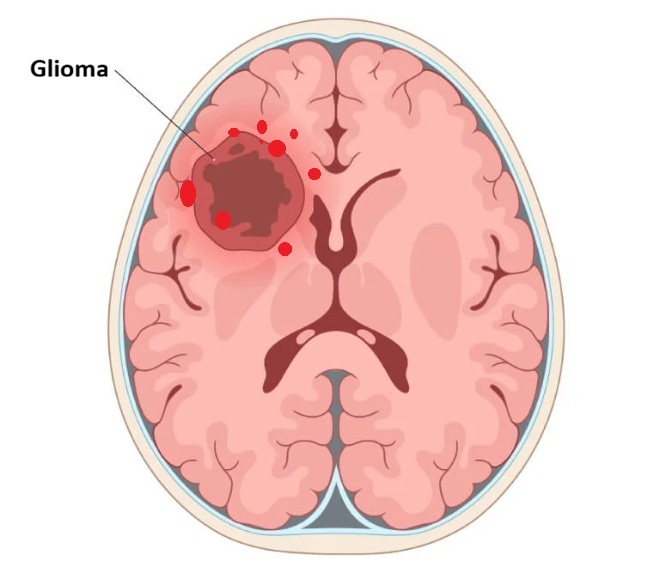
Image: Illustrating diffuse brain infiltration by an astrocytoma. This microscopic spread makes it impossible to define a precise boundary between the tumor and healthy tissue during surgical resection.
Grade 2 IDH-mutant Astrocytoma in Adults
Grade 2 tumors usually have a slower growth rate, but they are still diffuse gliomas and are not benign in the practical surgical sense.
Patients may present with:
These tumors may remain clinically stable for prolonged periods, but recurrence after surgery or progression over time is common.
Grade 3 IDH-mutant Astrocytoma
Grade 3 disease generally reflects a more active and biologically aggressive phase of the same tumor family.
Compared with grade 2, grade 3 tumors typically show:
- higher proliferative activity (meaning the tumor cells are dividing and growing more rapidly)
- faster growth
- greater likelihood of progression
- greater need for postoperative oncologic treatment
For patients, the key point is that grade 2 and grade 3 do not represent two unrelated diseases, but rather different levels of aggressiveness within the same IDH-mutant astrocytoma spectrum.
Grade 4 IDH-mutant Astrocytoma
Grade 4 astrocytoma with IDH mutation represents the most aggressive end of this same spectrum, but it still remains biologically distinct from glioblastoma.
This distinction is not just academic. It has real consequences for:
- expected survival
- treatment interpretation
- counseling
Grade 4 Astrocytoma: IDH-mutant vs Glioblastoma
This distinction is one of the most important modern concepts in neuro-oncology.
Astrocytoma, IDH-mutant, grade 4 is not the same disease as glioblastoma, IDH-wildtype. Glioblastoma refers specifically to a highly aggressive IDH-wildtype diffuse astrocytic tumor with grade 4 biology.
Although both are grade 4 tumors, the biology is different. In general IDH-mutant grade 4 astrocytoma usually has a better prognosis.
IDH-wildtype diffuse astrocytic tumors in adults are not classified as lower-grade astrocytomas. When specific molecular features associated with glioblastoma are present, they are classified as glioblastoma (WHO grade 4), even in the absence of classic high-grade histological features. In some cases, a tumor may be IDH-wildtype but not yet meet full criteria for glioblastoma on initial analysis. Further molecular testing and follow-up are then required to establish the final diagnosis.
Bottom Line
- Grade 4 IDH-mutant astrocytoma = an astrocytoma, biologically distinct from GBM
- Glioblastoma = usually IDH-wildtype, highly aggressive diffuse astrocytic tumor
How Astrocytoma Develops: Genetic Mutations and Tumor Biology
Astrocytoma develops as a consequence of acquired (mutations that occur during a person’s lifetime, not inherited from parents) genetic mutations that disrupt the normal regulation of cell growth, differentiation, and survival. As these mutations accumulate over time, tumor cells gradually lose normal control mechanisms and begin to behave independently of surrounding brain tissue.
These gene mutations involve two fundamental biological processes:
- activation of oncogenic pathways (driving uncontrolled proliferation)
- loss of tumor suppressor function (removing normal growth inhibition)
In astrocytoma, this process is not uniform. The biological behavior of the tumor depends strongly on its molecular profile, rather than on histological appearance alone.
The most important molecular distinction is:
- IDH-mutant astrocytoma
- versus IDH-wildtype diffuse astrocytic tumors
IDH-mutant astrocytomas typically arise through a slower evolutionary pathway. Tumor cells accumulate mutations gradually, and the disease often follows a prolonged clinical course over years.
In contrast, IDH-wildtype tumors (which are usually classified as glioblastoma when aggressive features are present) tend to follow a more rapid and biologically aggressive trajectory.
In addition to IDH, other molecular alterations may be identified (ATRX loss, TP53 mutations, proliferation indices such as Ki-67), but their clinical relevance varies. Some markers are used primarily to confirm the tumor type, while others help estimate growth potential.
It is important for patients to understand:
- these mutations are not inherited in the vast majority of cases
- they occur spontaneously during life
- they reflect errors in DNA replication or repair
Astrocytoma is therefore not caused by a single event, but by a progressive accumulation of molecular changes that gradually shift cells from normal regulation toward uncontrolled, malignant growth.
In rare cases, astrocytomas may develop as part of inherited genetic conditions. These include disorders such as neurofibromatosis type 1 (NF1), Li-Fraumeni syndrome, and tuberous sclerosis complex, which are associated with an increased risk of certain brain tumors. However, this situation is uncommon, and the vast majority of astrocytomas occur sporadically, without any inherited predisposition.
Influence of External Factors on Astrocytoma
The role of external factors in the development of astrocytoma is often misunderstood.
Current scientific evidence indicates:
- High-dose ionizing radiation (for example, previous radiation therapy to the head) is the only well-established environmental risk factor
- most astrocytomas arise sporadically, without an identifiable external trigger
Several commonly discussed factors are not supported by consistent evidence:
- mobile phone use
- psychological stress
- head trauma
- lifestyle factors
These are frequently mentioned by patients but have not been proven to directly cause astrocytoma.
Other factors are under investigation:
- long-term inflammation
- viral influences
- occupational exposures
However, their role remains uncertain and is not considered causative in routine clinical practice.
From a practical standpoint, the key message is:
- astrocytoma is primarily driven by internal genetic alterations, not by lifestyle or daily habits
This distinction is important because many patients incorrectly assume that something they did caused the disease.
Mechanisms of Brain Damage in Astrocytoma
Astrocytoma affects brain function through several mechanisms, which often occur simultaneously:
Tumor Infiltration of Functional Brain Tissue
Diffuse astrocytomas infiltrate areas responsible for movement, speech, vision, and cognition. As tumor cells invade these networks, neurological deficits develop.
These deficits depend on tumor location and may include:
- weakness in the opposite side extremities
- speech impairment
- visual disturbances
- cognitive decline
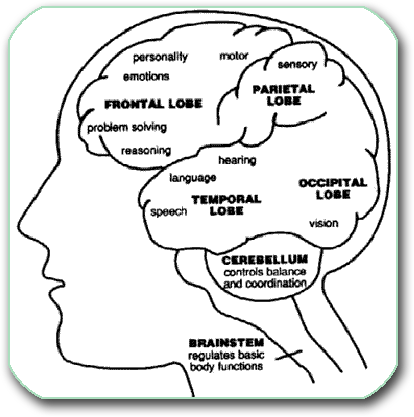
Image: Functional centers in the brain cortex. Explanations regarding the anatomy of various brain regions can be found on this page.
Peritumoral Edema and Increased Intracranial Pressure
Tumor-associated swelling (edema) is a major contributor to symptoms.
Disruption of the blood–brain barrier leads to fluid leakage into surrounding tissue, resulting in:
- increased intracranial pressure
- headache
- nausea
- neurological deterioration
Corticosteroids (such as Dexamethasone) may temporarily improve symptoms by reducing this edema. Before corticosteroids are given, it is important to consider whether primary CNS lymphoma is a possibility, as steroids can rapidly reduce or even obscure the lesion and complicate diagnosis.
Mass Effect and Secondary Complications
As tumor volume and edema increase, pressure effects develop:
- compression of brain structures
- displacement of midline structures
- obstruction of cerebrospinal fluid flow (hydrocephalus)
In severe cases, this may lead to life-threatening brain shifts (herniation).
Functional Network Disruption
Even without massive tumor growth, infiltration of neural networks can lead to:
- cognitive slowing
- personality change
- loss of executive function
This explains why some patients deteriorate even when imaging does not show dramatic enlargement.
Functional Status and Karnofsky Performance Scale (KPS)
In astrocytoma, symptoms alone are not sufficient to guide treatment decisions. Equally important is the patient’s functional status, which reflects the ability to perform daily activities.
The most widely used tool is the Karnofsky Performance Status (KPS).
It plays a central role, especially in patients with grade 4 astrocytoma, in determining:
- suitability for surgery
- tolerance of radiotherapy and chemotherapy
- expected recovery
- overall prognosis
Karnofsky Scale (Simplified)
- 90–100 → normal or near normal function
- 70–80 → independent but limited
- 50–60 → requires assistance
- <50 → severe disability
A higher KPS generally indicates:
- better tolerance of treatment
- better functional recovery potential
- more favorable prognosis
It is important to understand:
- KPS does not measure tumor biology directly
- it reflects the impact of the tumor on the patient
In many cases, improvement after corticosteroids suggests that symptoms are driven by edema rather than irreversible damage, which may influence surgical decisions.
How Astrocytoma Behaves Over Time
Unlike glioblastoma, which often progresses rapidly, many astrocytomas — especially IDH-mutant tumors — follow a prolonged clinical course.
However, progression over time is expected, not exceptional.
The disease typically evolves through phases:
- initial diagnosis (often slower-growing stage)
- period of relative stability
- gradual progression
- possible transformation to higher-grade disease
Progression may present as:
- growth on MRI
- worsening neurological symptoms
- increased contrast enhancement
- new or worsening edema
It is important to understand:
- stability does not mean cure
- progression may occur after years of apparent control
- long-term follow-up is essential
The key clinical challenge is not only detecting progression, but determining when intervention is beneficial.
Symptoms of Astrocytoma in Adults
Symptoms depend mainly on:
- tumor location
- tumor growth speed
- degree of infiltration
- presence of edema
- intracranial pressure
- and whether seizures occur
Common Symptoms
- headache
- seizures
- focal neurological deficits
- speech problems
- weakness in the opposite side extremities
- visual symptoms
- cognitive decline
- personality or behavioral changes
- gait instability
How Astrocytoma in Adults Is Diagnosed
MRI Is the Key Imaging Study
Magnetic resonance imaging (MRI) of the brain, performed with and without contrast, is the central diagnostic test when astrocytoma is suspected.
MRI helps define:
- tumor location
- size
- growth pattern
- involvement of eloquent brain regions
- heterogeneous contrast enhancement
- central necrotic change
- edema
- mass effect (compression on the brain)
- ventricular compression
- hemorrhage
- and overall surgical accessibility
Different astrocytomas have different imaging appearances. A crucial principle for patients to understand is this the visible lesion on MRI is not always the whole disease. In diffuse astrocytomas, microscopic tumor cells extend beyond the obvious borders.
In addition to defining anatomy and surgical accessibility, MRI findings must always be interpreted in the context of tumor biology. In IDH-mutant astrocytomas, imaging appearance often reflects the underlying grade, although not with absolute certainty. Grade 2 tumors typically show more subtle changes, often without significant contrast enhancement and with relatively limited compressive effect, reflecting slower growth. Grade 3 tumors more often demonstrate increased signal abnormality, greater infiltrative extent, and may begin to show contrast enhancement, indicating higher biological activity. Grade 4 IDH-mutant astrocytomas usually display more aggressive imaging features, such as heterogeneous contrast enhancement, areas of necrosis, and more pronounced edema and mass effect, although their overall behavior still differs from glioblastoma. Grade 4 IDH-mutant astrocytomas most commonly involve the cerebral hemispheres, particularly the frontal lobes, but they do not show a specific predilection for a particular subregion. Compared to glioblastoma (IDH-wildtype), they are less likely to present with classic “butterfly” growth across the corpus callosum, reflecting differences in biological behavior and patterns of infiltration.
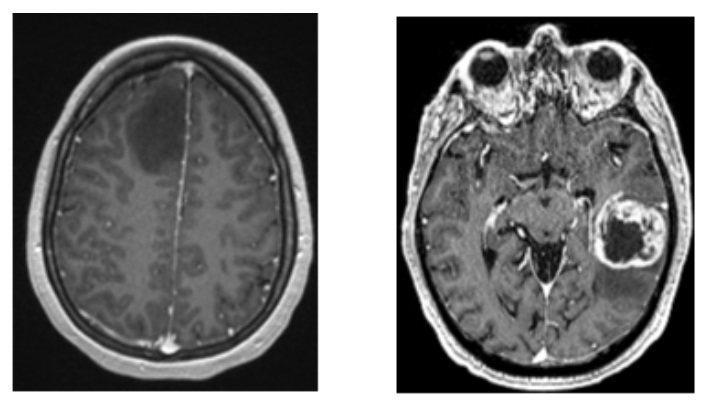
Image: Left: A Grade 2 astrocytoma (no contrast uptake). Right: A more aggressive Grade 4 tumor, which appears bright white after contrast injection and shows a dark area of necrosis in the middle.
It is important to understand that these imaging differences represent a spectrum rather than strict categories, and MRI alone cannot definitively determine tumor grade. The same lesion may appear relatively indolent at one stage and more aggressive later, reflecting biological progression over time. For this reason, MRI findings must always be interpreted together with histopathological and molecular analysis, rather than used in isolation.
Advanced MRI Techniques
Depending on location and surgical planning, advanced imaging may be used:
- functional MRI (fMRI) to identify speech and motor cortex
- MR tractography (DTI) to map critical white matter tracts
- MR spectroscopy (MRS) to assess metabolic behavior
- MR perfusion to help characterize aggressiveness
- MR angiography (MRA) to assess vascular relationships
These tools refine the map, but they do not replace tissue diagnosis.
Differential Diagnosis
Depending on MRI appearance, astrocytoma may need to be distinguished from:
- oligodendroglioma
- glioblastoma
- primary CNS lymphoma
- metastases
- abscess
- tumefactive demyelinating lesions (such as multiple sclerosis)
- radiation necrosis or treatment-related changes
For that reason, no important management decision should rely on a radiology report alone. The images themselves must be reviewed directly by an experienced neurosurgeon and correlated with the pathology and molecular data.
In many cases, MRI already provides a reasonable orientation as to whether a lesion is likely an astrocytoma and even suggests its approximate grade. However, even at the time of surgery, the exact diagnosis is often not fully certain until definitive histopathology is available. Intraoperative (extemporaneous) pathology can help guide the procedure, mainly by indicating tumor type or level of malignancy, but it is typically only an orientation and not a final diagnosis. For that reason, no important management decision should rely on a radiology report alone—the images must be reviewed directly and correlated with pathology and molecular findings.
Why Histopathology Remains the Gold Standard
Imaging can strongly suggest astrocytoma, but definitive diagnosis requires tissue obtained through:
- surgical resection
- or biopsy
The pathology report evaluates:
- Cellular atypia: Abnormal cell structure
- Mitotic activity: Rate of cell division
- Cellular density: Concentration of tumor cells
- Necrosis: Areas of tissue death
- Microvascular proliferation: New blood vessel growth
- Immunohistochemical markers: Genetic and protein profiling
Markers such as:
- GFAP
- OLIG2
- ATRX
- p53
- Ki-67
help define the tumor’s astrocytic nature and biological activity.
Molecular Diagnosis Is Essential
Modern diagnosis does not stop at microscopy.
The final integrated diagnosis requires molecular analysis, especially:
- IDH mutation status
- In many treatment contexts, MGMT promoter methylation is also assessed. This does not define the tumor type, but it helps predict how well chemotherapy may work. If the MGMT gene is “switched off” (methylated), tumor cells are less able to repair damage caused by chemotherapy such as temozolomide, and treatment is more likely to be effective. If the MGMT gene remains active (unmethylated), tumor cells can better repair this damage, and the response to treatment may be weaker.
These findings do not merely decorate the report. They explain why some astrocytomas behave more indolently, why others progress more rapidly, and how treatment expectations should be framed.
Astrocytoma and Headache — Is the Tumor Always the Cause?
Headache is a common symptom in the general population and does not automatically indicate that a brain tumor is the cause.
In patients with astrocytoma, headache is more likely to be related to the tumor when there is:
- significant tumor size
- surrounding edema
- increased intracranial pressure
- mass effect
However, in patients with small, non-enhancing, or diffuse lesions without mass effect, headache is often unrelated to the tumor.
Many patients have primary headache disorders such as:
- tension-type headache
- migraine
- cervicogenic headache
These conditions are very common and may coexist with an incidental brain tumor.
For this reason, the presence of headache alone is usually not a sufficient indication for surgical treatment of an otherwise stable astrocytoma.
Careful clinical evaluation is required to determine whether the tumor is actually responsible for the symptoms.
Astrocytoma and Seizures — When Is the Tumor the Cause?
Seizures may be the first symptom of an astrocytoma, particularly when the tumor involves or is close to the cerebral cortex. However, it is important to understand that not every seizure in a patient with astrocytoma is necessarily caused by the tumor. Epilepsy can occur independently, and a brain lesion may be an incidental finding.
For this reason, it is essential to evaluate whether the tumor is truly responsible for seizure activity.
This assessment typically includes:
- correlation between tumor location and cortical areas involved in seizures
- EEG findings and their spatial relation to the lesion
- presence of surrounding edema or cortical irritation
- clinical seizure pattern
When seizures are clearly related to the tumor:
- surgical treatment may significantly reduce seizure frequency
- in some patients, seizures may stop completely
However, when seizures are well controlled with medication and the tumor shows no signs of progression, immediate surgery may not always be necessary.
Treatment of Astrocytoma in Adults
Once a brain tumor is diagnosed, treatment decisions are ideally made in a multidisciplinary neuro-oncology setting, integrating:
- MRI findings
- pathology
- molecular markers
- neurological function
- functional status
- age
- and realistic surgical benefit
The Main Treatment Categories
Treatment may include:
- observation
- symptomatic treatment
- surgery
- radiotherapy
- chemotherapy
The correct combination depends entirely on the specific astrocytoma subtype and clinical context. The treatment strategy is based on the latest neuro-oncological clinical guidelines and the patient’s overall health.
After evaluation by a multidisciplinary neuro-oncology team (tumor board), the treatment decision may be one of the following:
• Surgical resection followed by radiotherapy and chemotherapy (Temozolomide), which is the most common approach when surgery is feasible
• Biopsy followed by radiotherapy and chemotherapy when safe resection is not possible or would not provide meaningful benefit
• Structured observation (active surveillance) in carefully selected cases, when the lesion is stable on serial MRI, symptoms are minimal or well controlled, and there is no urgent need for immediate intervention, with the understanding that diagnosis cannot be definitively confirmed without tissue analysis and that treatment may become necessary if progression occurs
• Symptomatic (palliative) treatment only in patients with poor functional status or extensive disease where active treatment would not improve quality of life
Treatment of Astrocytoma According to Grade (IDH-mutant)
Although general treatment principles apply to all astrocytomas, the actual strategy differs significantly between grade 2, 3, and 4 tumors. These are not separate diseases, but different stages of biological aggressiveness within the same spectrum.
Grade 2 IDH-mutant Astrocytoma Treatment
In grade 2 astrocytoma, surgery is often the first and most important step when it is safely feasible.
These tumors infiltrate surrounding brain tissue, which means that surgical removal is not based on finding a cleavage plane, but on removing as much MRI-visible abnormal tissue (on T2/FLAIR sequences) as safely possible. As a result, surgery in grade 2 astrocytoma may involve resection may extend to resection of an entire anatomical region or lobe when functionally safe, guided by neuronavigation and functional mapping.
However, surgery is not always appropriate. It may be avoided or limited when:
- the tumor involves eloquent cortex (speech, motor, vision)
- the expected neurological deficit would outweigh benefit
- the lesion is diffuse and not surgically accessible
- functional status is already compromised
In such cases, biopsy may be the more appropriate initial step.
After surgery, further management depends on the overall risk profile. Lower-risk patients — typically younger individuals, those with more complete tumor removal, preserved neurological function, and stable imaging — may be managed with observation and regular MRI follow-up. In contrast, patients with higher-risk features such as residual tumor, tumor growth over time, or the development of symptoms (including seizures or neurological decline) are more likely to require active treatment, most often with radiotherapy, with or without chemotherapy, depending on the clinical context.
In selected patients, particularly those with higher-risk features, Temozolomide (Temodar) is often used. It can be given concurrently with radiotherapy as a radiosensitizer, and/or as adjuvant chemotherapy after completion of radiation, in cyclic regimens. The exact use of Temozolomide depends on factors such as patient age, extent of resection, tumor behavior over time, and overall clinical context.
The goal of this combined approach is not to eliminate the disease completely, but to control residual microscopic tumor, delay progression, and preserve neurological function for as long as possible.
The key principle is that grade 2 astrocytoma often follows a long clinical course, but is not biologically benign. Treatment decisions are therefore based on timing, risk, and functional impact, not on the diagnosis alone.
Grade 3 IDH-mutant Astrocytoma Treatment
In the absence of contraindications, surgical resection is the primary approach; otherwise, a biopsy is performed. In both cases, adjuvant therapy is subsequently indicated.
The goal of surgery is to remove as much of the tumor as safely possible, while protecting the normal function of the brain. On an MRI scan, the tumor is typically visible in two ways: as a bright spot on the contrast-enhanced scan (representing the most active part of the tumor) and as a white area on the T2/FLAIR scan (representing the zone where tumor cells have spread into the surrounding brain tissue).
The surgeon always aims to remove the contrast-enhancing part first, as this is the most biologically aggressive portion of the tumor. However, in some patients with this type of tumor, there may be little or no contrast enhancement at all — meaning the tumor does not show up clearly on the contrast scan. In those cases, the white area on the T2/FLAIR scan becomes the main guide for surgery, similar to how lower-grade brain tumors are approached.
When it is safe to do so, the surgeon will also attempt to remove as much of the surrounding abnormal tissue as possible — the area that appears white on T2/FLAIR. How far this resection extends depends not on the scan alone, but on how close the tumor is to areas of the brain responsible for movement, speech, or other vital functions.
It is important to understand that this type of tumor does not have sharp edges. Tumor cells spread diffusely into the surrounding brain, which means complete removal of every tumor cell is not possible. The goal of surgery is therefore not to achieve a perfect anatomical removal, but to reduce the tumor burden as much as safely possible — which makes subsequent treatments such as radiation and chemotherapy more effective, and helps the patient maintain their quality of life.
Grade 3 astrocytoma represents a more active phase of the disease and usually requires postoperative oncologic treatment.
After surgery (or biopsy if resection is not feasible), treatment most often includes:
- radiotherapy
- Temozolomide chemotherapy (concurrent and/or adjuvant)
This combined approach is conceptually similar to the treatment used in grade 4 tumors, but the overall strategy, timing, and expected disease course differ, reflecting the distinct biology of grade 3 astrocytoma.
Grade 4 IDH-mutant Astrocytoma
In the absence of contraindications, surgical resection is the primary approach; otherwise, a biopsy is performed. In both cases, adjuvant therapy is subsequently indicated.
Grade 4 IDH-mutant astrocytoma represents the most aggressive end of this spectrum and is treated more similarly to high-grade gliomas, although it remains biologically distinct from glioblastoma.
In most patients, treatment includes:
- maximal safe surgical resection (when feasible)
- followed by radiotherapy combined with Temozolomide
- and adjuvant Temozolomide
The rationale is the same as in other high-grade diffuse gliomas:
The goal of surgery is to remove as much of the tumor as safely possible, while protecting the normal function of the brain.
In grade 4 IDH-mutant astrocytoma, the tumor typically shows a clearly visible bright area on the contrast-enhanced MRI scan, representing the most active and aggressive part of the tumor. Unlike glioblastoma, however, this tumor carries a specific genetic change — the IDH mutation — which makes it biologically less aggressive than glioblastoma, despite sharing the same grade 4 classification. This distinction matters, because these patients tend to be younger and have a longer life expectancy, which makes preserving brain function an especially important part of the surgical plan.
The surgeon always aims to remove the contrast-enhancing tumor as completely as possible. When it is safe to do so, surgery may also extend into the surrounding white area visible on the T2/FLAIR scan, where tumor cells have infiltrated the surrounding brain tissue beyond the visible tumor core.
How far this resection extends depends not on the scan alone, but on how close the tumor is to areas responsible for movement, speech, memory, or other vital functions. In some locations, a more extensive removal is safely achievable. In others, preserving function takes priority.
As with all diffuse gliomas, this tumor does not have sharp edges. Tumor cells spread into the surrounding brain in a way that cannot be fully captured on any scan, and complete removal of every tumor cell is not possible. The goal of surgery is therefore not a perfect anatomical removal, but maximal safe cytoreduction — reducing the tumor burden as much as possible to make subsequent radiation and chemotherapy more effective, and to help the patient maintain their quality of life for as long as possible.
At this stage, more frequently than in Grade 2 or 3 cases, contraindications may render surgical resection non-indicated. In such instances, the protocol shifts to biopsy followed by adjuvant therapy. In the most advanced clinical presentations, where even biopsy is unfeasible, the focus remains solely on symptomatic palliative care—a management strategy similar to that employed for Glioblastoma (GBM).
Key Clinical Principle
The presence of a tumor does not automatically define the treatment.
Treatment intensity increases with:
- tumor grade
- growth behavior
- clinical symptoms
- and risk of progression
Two patients with “astrocytoma” may receive completely different treatments depending on these factors.
Symptomatic Treatment in Brain Astrocytoma
Symptomatic treatment addresses the effects of the tumor on the brain rather than the tumor biology itself.
This may include:
- Dexamethasone to reduce edema
- anti-epileptic drugs for seizure control
- analgesics
- anti-nausea medication
- supportive treatment for confusion or agitation
Improvement after steroids usually reflects reduction of edema and mass effect, not elimination of the tumor.
Surgical Management of Astrocytoma in Adults
Surgery plays several possible roles:
- obtaining tissue for diagnosis
- reducing tumor burden
- relieving mass effect
- improving or stabilizing neurological function
- creating the best conditions for further treatment
The principle is not maximal removal at any cost, but maximal safe resection.
The most important question is not simply whether surgery is technically possible, but what is realistically gained by surgery in this specific patient?
That depends on:
- tumor grade
- tumor location
- proximity to eloquent cortex
- depth
- infiltrative extent
- preoperative neurological status
- Karnofsky Performance Status (KPS)
- response to steroids
- age and overall condition
Surgical treatment involves a craniotomy (the surgical opening of the skull). The surgeon then navigates through the brain tissue to access the tumor, often using neuronavigation to guide the path. Once reached, the goal is to remove as much of the tumor as safely possible—a process known as maximal safe resection. The surgical goal for resection is defined by the tumor grade, following the criteria described in the chapters above. The primary goal is to maximize tumor removal while safeguarding neurological function. This balance is critical, as the preservation of a high Karnofsky Performance Status (KPS) is just as vital for the patient’s prognosis as the extent of the resection itself. A stable KPS not only ensures functional independence but also determines the patient’s eligibility for essential post-operative therapies like radiation and chemotherapy.

Image: The image illustrates a craniotomy. Both the skin incision and the skull opening are performed within the hair-bearing area of the scalp. The dura is opened to expose the brain as part of the surgical approach to the tumor. After the procedure, the dura is closed with stitches, the bone flap is secured, and the scalp is reconstructed, ensuring no cosmetic defect remains after healing.
Modern Surgical Technologies in Brain Astrocytoma Surgery
The goal of modern neurosurgery is to maximize tumor removal while leaving healthy brain tissue untouched. To achieve this, several advanced technologies are used to guide the surgeon in real-time.
Neuronavigation and Intraoperative Imaging
Think of neuronavigation as „GPS for the brain.“ By synchronizing the patient’s head with their MRI scans, this system allows the surgeon to see the exact position of their instruments inside the brain with sub-millimeter precision. This is especially vital for reaching deep-seated tumors or defining the irregular edges of a astrocytoma. In some centers, intraoperative MRI or Ultrasound is used to update these „maps“ during surgery as the brain shifts.

Image: Preoperative preparation for brain tumor surgery using MRI-guided neuronavigation in the operating room.
Fluorescence-Guided Surgery (5-ALA)
Astrocytoma cells often blend in with healthy brain tissue, making them hard to see under standard white light. With this technology, the patient drinks a special liquid (5-ALA) a few hours before surgery. Under a specific blue light on the surgical microscope, the tumor cells glow a bright pink/violet color. This „glow-in-the-dark“ effect helps the surgeon identify and remove hidden tumor clusters that would otherwise be invisible, significantly increasing the likelihood of a complete resection.
Intraoperative Neurophysiological Monitoring (IONM)
This acts as a continuous „early warning system“ for the brain’s function. While the patient is asleep, specialized technicians monitor electrical signals passing through the brain. If the surgeon’s instruments get too close to a vital pathway—such as the nerves controlling movement or sensation—the system provides an immediate alert. This allows the surgeon to stop or change direction before any permanent neurological damage occurs.
Awake Craniotomy in Eloquent Cortex
For tumors located in „eloquent“ areas (the centers for speech, language, or complex movement), an awake craniotomy is the safest option. Although the patient is awake for part of the procedure, they feel no pain because the brain itself has no pain receptors and local anesthesia is used for the scalp. By having the patient talk, count, or move their fingers during the resection, the surgeon can map the brain in real-time. This ensures the tumor is removed as aggressively as possible without damaging the patient’s ability to communicate or move.
Note to Patients: Not every surgery requires all of these technologies. Your neurosurgical team will select the specific tools that are most appropriate for the size and location of your tumor to ensure the safest and most effective outcome.
Read more about potential complications following craniotomy and open brain surgery on this page.
Not every operation requires all of these tools. The goal is always to maximize safe tumor removal while preserving meaningful neurological function.
When Biopsy Is Preferred Over Surgery
Biopsy is medically appropriate when resection would be too risky or would not provide meaningful benefit.
This may apply when there is:
- grade 4 and sometimes 3
- deep-seated location
- eloquent cortex involvement
- diffuse bilateral infiltration
- poor functional status
- or a situation where surgery would not improve the overall therapeutic path
Biopsy is not a “lesser” treatment. It is often the correct step needed to establish diagnosis and plan the proper oncologic strategy.
Types of Brain Biopsy and What Patients Should Expect
In most cases, biopsy is performed as a stereotactic (needle) biopsy, which is a minimally invasive procedure.
This can be done using either:
- a frame-based system (a rigid frame attached to the head for maximum precision), or
- a frameless (neuronavigation-guided) system, which uses advanced imaging and tracking without a fixed frame
Both approaches are widely used today and provide high accuracy, with the choice depending on the tumor location, institutional preference, and surgical planning.
The procedure is usually performed:
- under general anesthesia (the patient is asleep), or
- in selected cases under local anesthesia with sedation, especially with frame-based systems
Open biopsy (during a craniotomy) is less commonly performed as a separate procedure, because if open surgery is undertaken, surgeons typically aim for maximal safe resection rather than biopsy alone.
From a patient’s perspective, stereotactic biopsy is generally:
- shorter and less invasive than tumor removal surgery
- associated with faster recovery
- focused on diagnosis rather than immediate treatment
Radiotherapy and Chemotherapy for Astrocytoma in Adults (Grade 2-4)
Adjuvant therapy (radiotherapy and chemotherapy) is used to control residual microscopic disease that cannot be removed surgically. Its role and intensity increase with tumor grade.
Radiotherapy does not target only the visible tumor. In most cases, the treatment area includes the tumor itself and a surrounding zone of brain tissue that may contain microscopic tumor infiltration, often corresponding to MRI changes (such as FLAIR). This surrounding margin is usually on the order of up to about 1–2 cm, although the exact extent is individualized based on tumor type, location, and planning protocols. External beam radiotherapy is the standard approach, delivered in multiple sessions (fractions) over several weeks. Modern techniques (such as IMRT or stereotactic radiotherapy) allow precise targeting of the tumor while reducing exposure to surrounding healthy brain tissue.
Grade 2 (IDH-mutant)
Adjuvant therapy is not always required immediately after surgery.
It is typically recommended when there is:
- residual tumor with high-risk features
- documented growth on follow-up MRI
- or development of symptoms
When indicated, treatment usually includes:
- radiotherapy, most commonly delivered as external beam radiation to a total dose of 50–54 Gy over approximately 5–6 weeks
- Temozolomide (Temodar) may be added in selected higher-risk patients, either concurrently with radiotherapy and/or as adjuvant therapy
Grade 3 (IDH-mutant)
In grade 3 astrocytoma, adjuvant therapy is most often recommended after surgery or biopsy.
Treatment typically includes:
- radiotherapy, delivered to a total dose of 60 Gy in standard daily fractions over approximately 6 weeks
- Temozolomide chemotherapy, given concurrently with radiotherapy and/or as adjuvant treatment
This approach reflects the more aggressive biological behavior compared to grade 2 disease.
Grade 4 (IDH-mutant)
In grade 4 astrocytoma, adjuvant therapy is considered standard and is usually initiated after surgery or biopsy.
Treatment most commonly follows a combined protocol similar in structure to the Stupp regimen:
- radiotherapy to a total dose of 60 Gy (2 Gy per fraction over 6 weeks)
- concurrent Temozolomide administered daily during radiotherapy (typically 75 mg/m²)
- followed by adjuvant Temozolomide, given in cycles (commonly 150–200 mg/m² for 5 days every 28 days, for 6 or more cycles depending on tolerance and response)
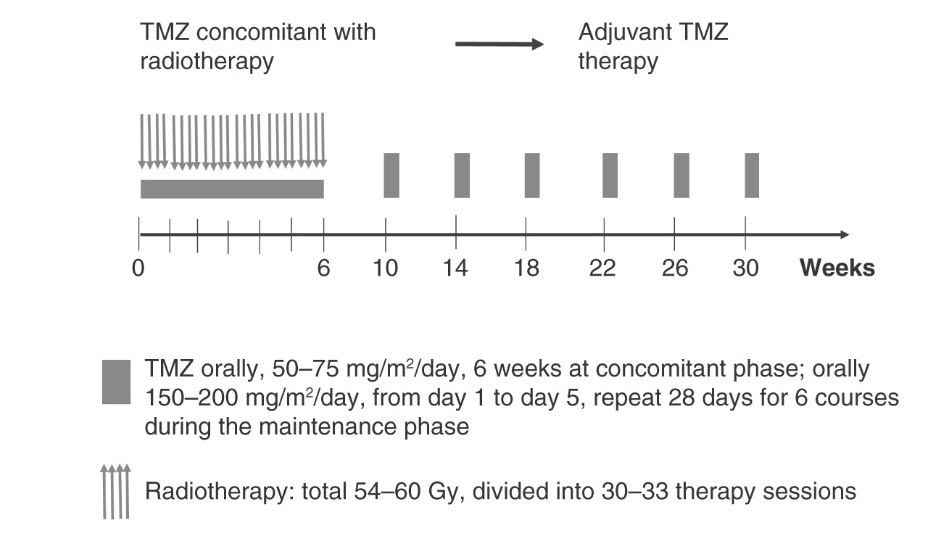
Image: Combined radiotherapy and Temozolomide (TMZ) treatment schedule used in high-grade astrocytoma. During the first 6 weeks, radiotherapy is delivered together with daily Temozolomide (concurrent phase), followed by cyclic adjuvant Temozolomide treatment. Although this approach is structurally similar to glioblastoma protocols, astrocytoma, IDH-mutant, grade 4 represents a biologically distinct disease with generally more favorable outcomes.
In some treatment strategies, especially in selected higher-risk patients, PCV chemotherapy (a combination of procarbazine, lomustine, and vincristine) may be used instead of or in addition to Temozolomide.
Observation in Adult Astrocytoma (Selected Cases Only)
In rare situations, a lesion that appears stable over a long period of time — for example, when prior imaging suggests that it has been present for many years without significant change — may be managed with careful follow-up rather than immediate intervention.
However, it is important to understand that in adults, a diagnosis of astrocytoma cannot be confirmed without tissue analysis. Imaging alone may strongly suggest a diffuse glioma, but it cannot definitively determine tumor type or biological behavior.
For this reason, observation is typically considered only when:
- the lesion shows no signs of progression on serial MRI
- symptoms are minimal or well controlled
- surgical intervention carries a meaningful functional risk
- and there is no urgent need for immediate histological confirmation
In such cases, management is based on close monitoring, with the understanding that intervention may become necessary if the lesion changes over time.
Prognosis and Survival for Astrocytoma in Adults
Prognosis in astrocytoma varies widely because astrocytoma is not one disease.
The most important prognostic factors include:
- exact diagnosis
- IDH status
- grade
- age
- functional status
- extent of safe resection
- tumor location
- response to treatment
- and overall biological behavior over time
General Principle
The more favorable end of the spectrum includes:
- pediatric grade 1 tumors
- circumscribed lesions
- IDH-mutant diffuse astrocytomas with slower behavior
- younger, functionally independent patients
- and tumors that can be safely resected extensively
The less favorable end includes:
- rapidly progressive tumors
- grade 4 disease
- poor functional status
- limited resectability
- and aggressive biological behavior
Broad Survival Orientation for IDH-mutant Astrocytoma
Because patients almost always ask for numbers, it is reasonable to discuss broad ranges honestly, while emphasizing that these are not personal predictions.
For many adult IDH-mutant astrocytomas:
- Grade 2 often has a long course, and median survival in modern series may extend roughly into the 8–15+ year range in favorable settings
- Grade 3 often remains a long-survival disease compared with glioblastoma, with median survival often in the 5–10 year range
- Grade 4 IDH-mutant astrocytoma generally has a better prognosis than glioblastoma, although it remains a serious, life-limiting malignant disease. Median survival in glioblastoma is typically around 12–15 months, whereas in grade 4 IDH-mutant astrocytoma it often extends to several years, commonly in the range of approximately 2–4 years depending on clinical and molecular factors.
These are broad, context-dependent ranges. Real outcome varies substantially with age, surgery, molecular profile, and treatment response.
Functional Prognosis Matters Too
In astrocytoma, survival should not be understood only in calendar terms. Patients care about:
- independence
- speech
- mobility
- cognition
- self-care
- and quality of life
A treatment strategy should therefore be judged not only by whether it extends life, but whether it preserves meaningful function.
Bottom Line
- some astrocytomas have a very long course
- recurrence and progression over time remain common
- prognosis depends on biology, not just grade
- IDH-mutant tumors usually do better than IDH-wildtype glioblastoma
- honest counseling requires numbers, context, and limits
Request Astrocytoma Neurosurgery Consultation — 24-Hour Review or Priority Option (Usually Within 3 Hours)
When an MRI or pathology report suggests astrocytoma (glioma), patients and families are often faced with important questions:
what the diagnosis really means, whether surgery is needed, how much tumor can realistically be removed, whether observation may be appropriate, and when radiotherapy or Temozolomide should be considered depending on tumor grade.
An independent neurosurgical second opinion can help you understand the situation clearly, assess whether the proposed treatment plan is appropriate, and explain what outcomes are realistic based on tumor grade, molecular profile, MRI features, seizure burden, and overall functional condition.
- ✔ Send a short message describing the astrocytoma diagnosis or suspicion, current symptoms (especially seizures, weakness, speech problems, headache, or cognitive changes), and what your MRI or pathology report says
- ✔ You’ll receive a reply within 24 hours explaining if and how we can help in your specific astrocytoma situation
- ✔ Time-sensitive cases: if seizures are worsening, neurological status is declining, or doctors are urgently recommending surgery or biopsy, consultations can often be arranged within a few hours — write PRIORITY in your first message
- ✔ Radiology and other medical reports can be reviewed once initial contact is established
- ✔ During the consultation, we explain operability and surgical goals (maximal safe resection vs biopsy vs observation), expected recovery, long-term treatment strategy, and when radiotherapy or chemotherapy may or may not be needed — with up to 10 days of follow-up for brief questions
Consultation fees typically range from $180–250, depending on case complexity and MRI / pathology findings.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth second opinions in neurosurgery.
MRI Follow-Up Protocol by Grade
The frequency of follow-up MRI scans depends on tumor grade, biological behavior, the type of treatment given, and the clinical course. Lower-grade tumors usually require long-term surveillance because late progression or transformation to a higher grade remains possible, while higher-grade tumors require closer follow-up because of the greater risk of early recurrence.
Grade 2 — IDH-mutant Astrocytoma
Slower growth. These tumors require long-term follow-up because progression or transformation to a higher grade may still occur even after many years of apparent stability.
- Postoperative MRI: within 24–72 hours after surgery
- Purpose: baseline assessment of residual tumor
- First 2 years: MRI every 3–6 months
- Protocol: T2/FLAIR (sequences showing tumor infiltration) plus gadolinium contrast (contrast dye that highlights more active tumor areas); lack of contrast enhancement is often expected
- After 2 years if stable: MRI every 6–12 months
- Follow-up: lifelong, because transformation to a higher grade may occur years or even decades later
Warning signs: new contrast enhancement (newly visible areas after contrast injection), rapid change in FLAIR volume, or new neurological symptoms. In that situation, biopsy or reoperation should be considered to exclude malignant transformation.
Grade 3 — Anaplastic Astrocytoma
Intermediate to high recurrence risk. These tumors require closer surveillance, especially during the first few years after surgery and adjuvant treatment.
- Postoperative MRI: within 24–72 hours
- During radiotherapy ± chemotherapy: MRI at the end of radiotherapy, or earlier if symptoms worsen
- Pseudoprogression: treatment-related changes that can mimic tumor growth on MRI, especially during the first 3 months after radiotherapy
- First 2–3 years: MRI every 3 months
- After that: every 4–6 months, then every 6 months if stable
- If PCV or Temozolomide is given: MRI between cycles, usually after every 2–3 cycles
This is the critical period for detecting recurrence early, but also for distinguishing true progression from treatment-related imaging changes.
Grade 4 — Glioblastoma (GBM)
High risk of early recurrence. MRI surveillance must be more frequent and closely linked to the phases of the Stupp protocol (standard treatment combining radiotherapy and Temozolomide).
- Postoperative MRI: within 24–72 hours — mandatory
- Purpose: assessment of residual tumor and baseline imaging for follow-up during the Stupp protocol
- After radiotherapy: MRI approximately 4 weeks after completion of radiotherapy
- Pseudoprogression: common, especially in MGMT-methylated tumors (a molecular feature influencing response to chemotherapy)
- During adjuvant Temozolomide: MRI every 2 cycles, approximately every 8 weeks
- After completion of treatment: MRI every 2–3 months
Urgent MRI is needed earlier if there is clinical deterioration.
Early warning signs: new enhancement outside the radiotherapy field, multifocal disease, or leptomeningeal spread (spread of tumor cells into the fluid spaces around the brain).
Note on RANO Criteria
RANO criteria (standard rules used by doctors to define tumor progression on MRI) are used to assess treatment response and progression in gliomas. In higher-grade tumors, progression is usually defined as at least a 25% increase in the size of enhancing tumor (based on standardized measurements), the appearance of a new lesion, or clear clinical deterioration. In lower-grade tumors, progression may occur without contrast enhancement and is often detected as gradual expansion of T2/FLAIR abnormalities, which is why principles similar to RANO-LGG criteria are used.
Management of Recurrence in Astrocytoma (Grades 2–4)
Recurrence in astrocytoma is expected over time, but it does not represent a single situation. Management depends on tumor grade, time to progression, imaging pattern, and functional status.
The key clinical challenge is not only detecting recurrence, but determining:
- whether the lesion represents true tumor progression or treatment-related change
- whether surgery will provide meaningful benefit
- and whether further oncologic treatment is justified
True Tumor Recurrence vs Radiation Necrosis
After radiotherapy, new or increasing MRI changes do not automatically mean tumor recurrence.
Three possibilities must always be considered:
- True tumor progression
- Pseudoprogression (early treatment effect)
- Radiation necrosis (late treatment-related injury)
These conditions may appear similar on MRI:
- contrast enhancement
- surrounding edema
- mass effect
- clinical deterioration
How to Distinguish Recurrence from Radiation Necrosis
No single test is definitive. Diagnosis is based on a combination of:
- MRI evolution over time (progressive vs stable or fluctuating changes)
- advanced imaging (perfusion MRI, MR spectroscopy, sometimes PET)
- clinical course (speed of deterioration, steroid response)
Typical patterns:
- Tumor recurrence → progressive growth, increasing enhancement, worsening symptoms
- Radiation necrosis → may fluctuate, often steroid-responsive, may appear months to years after RT
However, in many cases, imaging remains inconclusive, and decision-making must rely on overall clinical context.
When Reoperation Is Indicated
Reoperation is not automatic and is only considered when it is expected to provide real clinical benefit.
Reoperation is most appropriate when:
- the patient has good functional status (KPS ≥70)
- the lesion is well localized and surgically accessible
- there is significant mass effect causing symptoms
- a meaningful volume of tumor can be removed
- the patient is expected to tolerate recovery and further therapy
In this setting, surgery may:
- reduce tumor burden
- relieve intracranial pressure
- improve or stabilize neurological function
- provide tissue for updated diagnosis (progression vs transformation)
When Reoperation Is Not Appropriate
Surgery is usually avoided when:
- low functional status (KPS <60)
- diffuse or bilateral disease
- deep or eloquent location with high risk of deficit
- limited expected benefit from cytoreduction
In these cases, surgery may worsen quality of life without improving outcome.
Reoperation in Radiation Necrosis
Radiation necrosis is not a tumor, but it can produce significant mass effect and neurological deterioration.
Surgery may be indicated when:
- symptoms are severe and progressive
- steroids are ineffective or not tolerated
- imaging cannot exclude tumor recurrence
- removal would significantly reduce mass effect
In this situation, surgery is performed:
- to relieve pressure
- to improve neurological function
- to confirm diagnosis
Importantly, functional improvement after surgery is often more pronounced in radiation necrosis than in tumor recurrence, because no active tumor remains.
Role of Adjuvant Treatment at Recurrence
Further treatment depends on tumor biology and prior therapy.
Options may include:
- repeat radiotherapy (selected cases only)
- chemotherapy (Temozolomide rechallenge or alternative protocols)
- targeted or antiangiogenic therapy (e.g., Bevacizumab)
- clinical trials
Key principles:
- treatment is individualized
- prior treatments and response matter
- benefit must be balanced against toxicity and functional decline
Grade-Specific Considerations
Although principles overlap, recurrence behaves differently across grades:
- Grade 2 (IDH-mutant)
- progression may be slow
- reoperation often considered for growth or malignant transformation
- long-term strategy is critical
- Grade 3 (IDH-mutant)
- higher likelihood of progression
- reoperation considered when localized recurrence and functional reserve exist
- systemic therapy often required
- Grade 4 (IDH-mutant astrocytoma / glioblastoma)
- recurrence is expected
- reoperation only in selected cases
- treatment often focuses on disease control and function preservation
Core Clinical Principle
Management of recurrence is not based on imaging alone.
It requires integration of:
- MRI dynamics over time
- neurological status
- tumor location and resectability
- prior treatment
- expected benefit vs risk
Two patients with “recurrence” may require completely different decisions. Both called “astrocytoma” may require completely different decisions.
Experimental and Emerging Therapies in Astrocytoma
Many patients investigate new or experimental treatment options, especially in cases of progression.
These may include:
- clinical trials (novel drugs, targeted therapies)
- immunotherapy approaches
- vaccine-based treatments
- experimental drug combinations
While these strategies are scientifically important, it is essential to understand:
- most remain investigational
- individual benefit is uncertain
- they do not replace standard treatment
The main risks include:
- loss of time
- treatment-related toxicity
- unrealistic expectations
A balanced approach is required:
- exploration of new options is reasonable
- but decisions must remain grounded in clinical reality
If you are considering an experimental treatment within a clinical trial or an ‘off-label’ therapy, you may request an independent second opinion to evaluate the potential benefits and risks of such an approach.
Why Do Experts Sometimes Disagree About the Best Treatment?
It is not uncommon for different specialists to recommend different strategies for the same astrocytoma. This does not mean that someone is wrong — it reflects the complexity of the disease and the fact that in many situations there is no single correct treatment.
Tumors can behave differently in each patient, even with the same diagnosis. Specialists may prioritize different goals — maximal tumor removal, preservation of neurological function, or quality of life. In addition, guidelines are not always identical, and medical knowledge is evolving, especially with the growing role of molecular markers. Finally, patient preferences play an important role in every decision.
These differences become most visible in key treatment decisions:
Surgery vs Biopsy — When Is Tumor Removal Recommended
When the tumor can be removed with acceptable neurological risk, many specialists recommend maximal safe resection. However, if the tumor involves deep or critical brain areas, the risk of surgery may outweigh the benefit, and a biopsy followed by oncological treatment may be preferred.
When It May Be Safer Not to Operate Immediately
Not all astrocytomas require immediate surgery. In selected cases, especially with slower growth or mild symptoms, some specialists recommend observation or delayed intervention, while others favor earlier treatment to reduce the risk of progression.
Extent of Resection — How Much Tumor Should Be Removed
Even when surgery is indicated, opinions may differ. Some aim for maximal safe resection, while others take a more conservative approach near critical brain structures. The key question is how much can be safely removed, not simply how much can be removed.
Risks of Surgery vs Risks of Tumor Progression
Decisions often involve balancing immediate surgical risk against the risk of tumor progression. Some prioritize avoiding neurological deficits, while others emphasize early tumor control.
Role of Molecular Factors in Treatment Decisions
Molecular markers such as IDH status increasingly influence strategy. In some cases they support a more aggressive approach, while in others they justify a more conservative plan.
When a Second Opinion May Be Helpful
If you have received different recommendations — or if you are unsure which path is best — seeking an additional expert opinion can be valuable.
A second opinion may help you:
- understand why recommendations differ
- confirm whether the proposed treatment is appropriate
- explore alternative strategies that may not have been discussed
- make a more confident and informed decision
If you would like an independent review of your case, you can request a detailed evaluation here:
https://neurohirurgija.in.rs/en/second-opinion-in-neurosurgery-trusted-insight/
Frequently Asked Questions About Brain Astrocytoma
What is brain astrocytoma?
Brain astrocytoma is a glioma that arises from astrocytic glial cells in the brain. In adults, the most clinically important form is usually a diffuse astrocytoma, meaning that tumor cells infiltrate surrounding brain tissue microscopically. This makes astrocytoma different from many sharply bordered tumors. The visible abnormality on MRI does not always represent the full extent of disease. Brain astrocytoma may behave slowly or aggressively depending on grade, IDH mutation status, MRI appearance, tumor location, and functional impact. For patients, the key point is that the word “astrocytoma” is not enough by itself. Treatment decisions require MRI review, tissue diagnosis when needed, molecular markers, neurological status, and realistic surgical risk assessment.
Is brain astrocytoma a single disease?
Brain astrocytoma is not a single uniform disease. It includes tumors with different biological behavior, growth speed, treatment needs, and prognosis. In adults, diffuse astrocytoma is now understood mainly through molecular classification, especially IDH mutation status. Grade 2 tumors usually grow more slowly, grade 3 tumors show more active biological behavior, and grade 4 IDH-mutant astrocytoma represents the most aggressive stage within this tumor family. Pediatric astrocytomas are often biologically different and should not be directly compared with adult diffuse astrocytomas. This is why two patients with the same general word “astrocytoma” may receive very different recommendations regarding observation, surgery, biopsy, radiotherapy, chemotherapy, and follow-up.
What does IDH mutation mean in adult brain astrocytoma?
IDH mutation is one of the most important molecular markers in adult brain astrocytoma. In modern classification, adult diffuse astrocytoma is generally defined by the presence of an IDH mutation. This mutation is associated with a different biological pathway and usually a more favorable prognosis compared with IDH-wildtype diffuse tumors. IDH-wildtype diffuse astrocytic tumors in adults are often classified as glioblastoma when specific molecular or histological features are present, even if the tumor initially appears less aggressive under the microscope. For patients, IDH status helps explain expected growth pattern, treatment strategy, prognosis, and how doctors interpret grade 2, grade 3, and grade 4 disease.
What does diffuse brain astrocytoma mean?
Diffuse brain astrocytoma means that tumor cells spread microscopically into surrounding brain tissue instead of forming a completely separate, well-defined mass. On MRI, the visible abnormality may show the main tumor region, but tumor cells can extend beyond the visible border. This is why surgery cannot remove every tumor cell in an absolute sense, even when all visible abnormal tissue is removed. The surgical goal is maximal safe resection: removing as much tumor as possible while preserving speech, movement, vision, memory, and other important brain functions. Diffuse growth also explains why long-term MRI follow-up is necessary and why radiotherapy or chemotherapy may be recommended after surgery in selected patients.
What is the difference between grade 2, grade 3, and grade 4 brain astrocytoma?
Grade 2, grade 3, and grade 4 brain astrocytomas represent different levels of biological aggressiveness. Grade 2 IDH-mutant astrocytoma usually grows more slowly and may present with seizures or subtle symptoms, but it is still infiltrative and not truly benign. Grade 3 astrocytoma shows more active tumor behavior, higher proliferation, and usually requires postoperative oncological treatment. Grade 4 IDH-mutant astrocytoma is the most aggressive form within this astrocytoma spectrum and is commonly treated with maximal safe surgery or biopsy followed by radiotherapy and Temozolomide. Grade affects urgency, treatment intensity, recurrence risk, MRI follow-up frequency, and prognosis, but individual outcome also depends on age, function, tumor location, and resectability.
Is grade 4 IDH-mutant brain astrocytoma the same as glioblastoma?
Grade 4 IDH-mutant brain astrocytoma is not the same disease as glioblastoma, although both are high-grade malignant gliomas. Glioblastoma usually refers to an IDH-wildtype diffuse astrocytic tumor with grade 4 biology. Astrocytoma, IDH-mutant, grade 4 belongs to the IDH-mutant astrocytoma spectrum and often has a different clinical course. It is still a serious malignant disease and is usually treated aggressively, often with surgery or biopsy followed by radiotherapy and Temozolomide. However, its prognosis is generally better than typical IDH-wildtype glioblastoma. This distinction is important because the word “grade 4” can sound identical to patients, while the underlying biology and expected disease course may differ significantly.
How is brain astrocytoma diagnosed?
Brain astrocytoma is suspected based on MRI findings, symptoms, tumor location, and growth pattern, but definitive diagnosis usually requires tissue analysis. MRI with and without contrast is the key imaging test. It helps define tumor size, location, edema, enhancement, mass effect, and relationship to functional brain areas. Advanced MRI methods such as perfusion, spectroscopy, tractography, or functional MRI may help surgical planning. However, imaging alone cannot reliably determine the final tumor type or grade. Histopathology and molecular testing are essential. The final integrated diagnosis usually includes microscopic appearance and markers such as IDH mutation, ATRX, p53, Ki-67, and sometimes MGMT promoter methylation, depending on treatment context.
What does brain astrocytoma look like on MRI?
Brain astrocytoma can look different on MRI depending on grade and biological behavior. Grade 2 IDH-mutant astrocytomas often appear as T2/FLAIR hyperintense lesions with little or no contrast enhancement. Grade 3 tumors may show greater infiltrative extent, more active growth, and sometimes contrast enhancement. Grade 4 IDH-mutant astrocytomas more often show aggressive features such as heterogeneous enhancement, necrosis, edema, and mass effect. However, MRI appearance is not absolute. A tumor can progress over time, and microscopic tumor spread may extend beyond visible borders. For this reason, MRI must be interpreted together with clinical symptoms, previous scans, surgical feasibility, and final histopathological and molecular diagnosis.
When is surgery recommended for brain astrocytoma?
Surgery is recommended for brain astrocytoma when it is expected to provide meaningful benefit with acceptable neurological risk. The goals may include obtaining tissue for diagnosis, reducing tumor burden, improving seizure control, relieving mass effect, or preparing the patient for radiotherapy and chemotherapy. Surgery is most strongly considered when the tumor is accessible, growing, symptomatic, causing seizures or neurological deficits, or suspected to be higher grade. In grade 2 astrocytoma, early maximal safe resection is often important when feasible. In grade 3 and grade 4 tumors, surgery or biopsy is usually needed to establish diagnosis and guide further treatment. The decision depends on location, eloquent cortex involvement, functional status, MRI features, and expected risk.
What is maximal safe resection in brain astrocytoma surgery?
Maximal safe resection means removing as much brain astrocytoma as possible while protecting important neurological functions. Because diffuse astrocytoma does not have a clean border, the surgeon cannot simply peel it away from normal brain tissue. The goal is to remove visible tumor on MRI, often including abnormal T2/FLAIR tissue when safe, while avoiding damage to areas responsible for movement, speech, vision, memory, and cognition. Techniques such as neuronavigation, functional MRI, tractography, intraoperative monitoring, awake mapping, ultrasound, intraoperative MRI, and fluorescence guidance may be used depending on the case. The word “safe” is essential: preserving a good functional status may be as important as the extent of resection.
When is biopsy preferred instead of brain astrocytoma surgery?
Biopsy may be preferred instead of tumor removal when resection would carry high neurological risk or would not meaningfully improve the treatment path. This may apply to deep-seated tumors, diffuse bilateral lesions, tumors involving eloquent cortex, poor functional status, advanced disease, or cases where safe cytoreduction is not realistic. A stereotactic needle biopsy can provide tissue for histopathology and molecular diagnosis with less surgical trauma than open resection. Biopsy is not a “lesser” decision when the main goal is to establish diagnosis and plan radiotherapy, chemotherapy, or palliative treatment. The choice between resection and biopsy depends on expected benefit, surgical accessibility, neurological risk, and the patient’s overall condition.
What is the treatment for brain astrocytoma by grade?
Treatment for brain astrocytoma depends strongly on grade. Grade 2 IDH-mutant astrocytoma is often treated first with maximal safe resection when feasible. After surgery, selected lower-risk patients may be observed with regular MRI, while higher-risk patients may need radiotherapy and sometimes chemotherapy. Grade 3 astrocytoma usually requires surgery or biopsy followed by radiotherapy and Temozolomide. Grade 4 IDH-mutant astrocytoma is treated more like a high-grade glioma, usually with maximal safe resection or biopsy followed by radiotherapy with concurrent and adjuvant Temozolomide. Treatment is individualized according to MRI findings, residual tumor, molecular markers, age, neurological status, Karnofsky performance status, and patient goals.
When are radiotherapy and Temozolomide used for brain astrocytoma?
Radiotherapy and Temozolomide are used when brain astrocytoma has higher-risk features, more aggressive grade, residual disease, progression, or a need for postoperative tumor control. In grade 2 astrocytoma, adjuvant treatment is not always immediate, but may be recommended if there is residual tumor, growth, symptoms, or other high-risk factors. In grade 3 astrocytoma, radiotherapy and Temozolomide are commonly used after surgery or biopsy. In grade 4 IDH-mutant astrocytoma, combined radiotherapy and Temozolomide is usually standard when the patient can tolerate treatment. Temozolomide is an oral chemotherapy drug, and MGMT promoter methylation may help estimate how likely the tumor is to respond.
Can brain astrocytoma cause seizures?
Brain astrocytoma can cause seizures, especially when the tumor involves or irritates the cerebral cortex. Seizures are often the first symptom in lower-grade diffuse astrocytomas and may occur even before major neurological deficits appear. Tumor-related seizures depend on location, cortical involvement, edema, and the electrical irritability of surrounding brain tissue. Surgery may improve seizure control when the tumor is truly the seizure source, especially if resection can be performed safely. However, not every seizure in a patient with an MRI lesion is automatically caused by the tumor. Clinical seizure pattern, EEG findings, tumor location, medication response, and MRI evolution all help determine the relationship between the tumor and epilepsy.
How are seizures from brain astrocytoma treated?
Seizures from brain astrocytoma are usually treated first with anti-seizure medication, most commonly drugs such as levetiracetam or other antiepileptic medicines chosen by the treating neurologist. Treatment depends on seizure type, tumor location, MRI findings, edema, medication tolerance, and whether seizures are controlled. Corticosteroids may help temporarily if seizures worsen because of tumor-related edema, but they do not treat the tumor itself. If seizures remain frequent despite medication, or if they are clearly linked to a surgically accessible tumor, surgery may become part of seizure control strategy. The key question is whether the astrocytoma is truly the epileptic focus and whether tumor removal can be performed safely without causing neurological deficit.
Can brain astrocytoma surgery stop seizures?
Brain astrocytoma surgery can sometimes stop seizures or significantly reduce their frequency, especially when seizures are caused by a cortical tumor that can be safely removed. Seizure improvement is more likely when the epileptic focus corresponds to the tumor location and when maximal safe resection is possible. However, surgery does not guarantee seizure freedom. Some patients still need long-term anti-seizure medication after tumor removal, especially if seizures were present for a long time, if tumor tissue remains, or if the surrounding cortex remains irritated. Before recommending surgery mainly for epilepsy, doctors should confirm that the lesion is truly responsible for the seizures and that the expected benefit outweighs surgical risk.
What is the prognosis for brain astrocytoma?
Prognosis for brain astrocytoma varies widely because astrocytoma is not one disease. The most important factors include grade, IDH status, patient age, functional status, tumor location, extent of safe resection, molecular profile, and response to treatment. Many grade 2 IDH-mutant astrocytomas follow a long clinical course, often measured in many years. Grade 3 astrocytoma has a more active course but may still have longer survival than glioblastoma. Grade 4 IDH-mutant astrocytoma is a serious malignant disease, often with survival measured in several years rather than months in favorable cases. These ranges are not individual predictions. Personal prognosis requires direct review of MRI, pathology, molecular findings, and clinical status.
Can brain astrocytoma recur or progress after treatment?
Brain astrocytoma can recur or progress after treatment because diffuse tumor cells often remain beyond the visible MRI abnormality. Recurrence may appear as slow enlargement of T2/FLAIR abnormality, new contrast enhancement, increasing edema, neurological decline, or seizure worsening. In grade 2 tumors, progression may occur after years of stability and may sometimes involve transformation to a higher grade. In grade 3 and grade 4 tumors, recurrence risk is higher and follow-up is closer. New MRI changes after radiotherapy do not always mean tumor progression; pseudoprogression and radiation necrosis may mimic recurrence. Management may include observation, reoperation, biopsy, repeat oncological treatment, clinical trials, or supportive care depending on the situation.
How is brain astrocytoma recurrence or progression diagnosed?
Brain astrocytoma recurrence or progression is diagnosed by combining MRI changes, clinical symptoms, treatment history, and sometimes advanced imaging or repeat tissue diagnosis. Warning signs may include enlargement of T2/FLAIR abnormality, new or increasing contrast enhancement, increasing edema, mass effect, worsening seizures, neurological decline, or steroid-dependent symptoms. After radiotherapy, new MRI changes do not always mean active tumor; pseudoprogression and radiation necrosis can mimic recurrence. Perfusion MRI, MR spectroscopy, PET imaging, serial MRI comparison, and clinical evolution may help distinguish these possibilities. In uncertain or surgically relevant cases, biopsy or reoperation may be needed to confirm whether the change represents tumor progression, treatment effect, or malignant transformation.
How is recurrent brain astrocytoma treated?
Recurrent brain astrocytoma is treated according to tumor grade, MRI pattern, prior treatment, functional status, location, and whether the recurrence is localized or diffuse. Options may include careful observation, reoperation, biopsy, repeat radiotherapy in selected cases, Temozolomide rechallenge, PCV chemotherapy, Bevacizumab for edema or radiation necrosis, clinical trials, or supportive treatment. Reoperation is most useful when the recurrent tumor is localized, surgically accessible, causing mass effect or symptoms, and the patient has good functional status. If disease is diffuse, deep, multifocal, or the patient’s condition is poor, surgery may not help and may worsen quality of life. The goal is to balance tumor control, neurological function, treatment burden, and realistic prognosis.
How often is MRI follow-up needed after brain astrocytoma treatment?
MRI follow-up after brain astrocytoma treatment depends on tumor grade, treatment type, residual tumor, and clinical course. A postoperative MRI is often performed within 24–72 hours after resection to assess residual visible tumor and establish a baseline. Grade 2 tumors usually require long-term surveillance, often every 3–6 months initially and then less frequently if stable, but follow-up may continue for many years. Grade 3 tumors usually need closer MRI monitoring, especially during the first several years. Grade 4 tumors require frequent follow-up, often every 2–3 months depending on treatment phase. Any new neurological decline, seizure change, or steroid-dependent worsening may require earlier imaging.
Can patients receive an online neurosurgical second opinion for brain astrocytoma?
Yes. An online neurosurgical second opinion for brain astrocytoma can be useful when diagnosis, surgical strategy, biopsy, radiotherapy, Temozolomide, prognosis, or MRI follow-up is unclear. Review is especially helpful when different doctors recommend different approaches, when the tumor is near eloquent brain areas, when surgery has been proposed but risks are not well explained, or when MRI suggests recurrence or progression. A meaningful second opinion usually requires MRI images, radiology reports, pathology and molecular results if available, operative reports, treatment history, and current neurological symptoms. The goal is not to replace the treating team, but to clarify options, risks, timing, and realistic expectations.