Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Headache is one of the most common neurological complaints.
In the vast majority of cases, headaches are benign and do not indicate a serious underlying condition. However, a small but important group of headaches are secondary, meaning they are caused by another medical problem that requires targeted evaluation and treatment.
Headaches can be acute or chronic (long-lasting). This page provides a clinical overview of chronic headache types, with particular attention to situations in which headache may signal an underlying neurological or neurosurgical condition.
Primary Headaches
Primary headaches are disorders in which headache itself is the disease, not a symptom of another condition. They are common, often recurrent, and usually diagnosed based on clinical features rather than imaging findings.
Tension-Type Headache
Tension-type headache is typically described as a dull, pressure-like pain, often bilateral, without focal neurological symptoms.
It is commonly associated with stress, muscle tension, and prolonged static posture. As with any other pain syndrome, there are numerous contributing factors that can trigger the onset, recurrence, and persistence of tension-type and other headaches, even despite treatment.
Migraine
Migraine headaches are usually episodic and often unilateral, with moderate to severe intensity.
They may be accompanied by nausea, sensitivity to light or sound, and sometimes visual or sensory aura, but are not caused by structural brain disease.
Menstrual Headache (Menstrual Migraine)
Menstrual headache represents a hormonally triggered form of migraine that typically occurs in temporal association with the menstrual cycle.
Pain characteristics are similar to migraine, often unilateral and pulsating, and may be more resistant than non-menstrual attacks.
Cluster Headache
Cluster headache is a rare but severe primary headache characterized by intense, unilateral pain around the eye or temple.
Attacks occur in clusters over weeks or months and are often accompanied by autonomic symptoms such as tearing or nasal congestion.
Neuralgias
Certain headache presentations are caused by irritation or dysfunction of specific cranial or peripheral nerves rather than by primary headache disorders.
The pain is typically sharp, stabbing, or electric in character and follows a specific nerve distribution.
Common neuralgias associated with head pain include:
- Trigeminal neuralgia and atypical trigeminal neuralgia
- Occipital neuralgia
- Postherpetic (zoster-related) neuralgia
Hemicrania Continua
Hemicrania continua is a primary headache disorder characterized by continuous, strictly unilateral head pain.
Pain intensity fluctuates over time and may be accompanied by autonomic symptoms, but unlike migraine, the headache is persistent rather than episodic.
Exertional Headache
Exertional headache is triggered by physical activity, including exercise, coughing, or straining.
It is usually short-lasting and bilateral, but new or severe exertional headache should prompt evaluation to exclude secondary causes.
Ice-Pick Headache (Primary Stabbing Headache)
Ice-pick headache consists of very brief, stabbing pains that occur spontaneously and last only seconds.
Despite their intensity, these headaches are benign and unrelated to peripheral nerve disorders such as occipital neuralgia.
Other Rare Primary Headaches
Some primary headache disorders are short-lasting and sharp, with abrupt onset and resolution.
They may be triggered by alcohol consumption, coughing, or sexual activity.
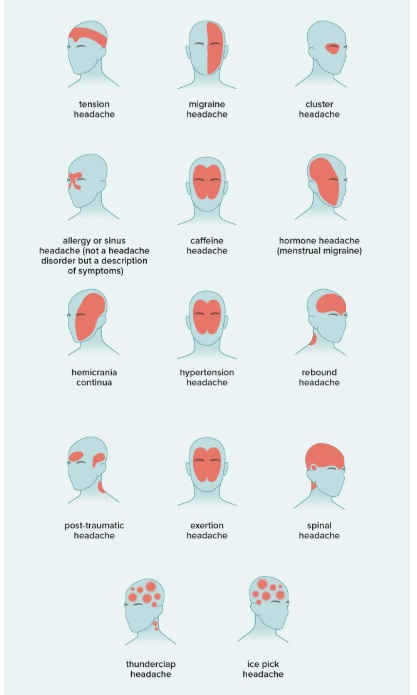
Image: Typical pain distribution in common primary headache disorders
Secondary Headaches
Secondary headaches occur as a consequence of another medical condition rather than being the primary disorder.
Identifying these headaches is clinically crucial, as treatment must address the underlying cause.
Sinus-Related Headache
Sinus-related headache usually presents as facial or frontal pain associated with nasal congestion or infection.
Pain often worsens with head movement or changes in position.
Ear, Jaw, and Temporomandibular Disorders
Disorders of the middle ear, mastoid, or temporomandibular joint can produce pain perceived as headache.
This pain is frequently misinterpreted as a primary headache disorder.
Cervical Spine and Musculoskeletal Causes
Degenerative or functional disorders of the cervical spine can lead to referred head pain.
Such headache is often localized to the occipital or suboccipital region and aggravated by neck movement or posture.
Hypertension-Related Headache
Headache associated with hypertension typically occurs during acute elevations of blood pressure rather than in chronic, well-controlled hypertension.
It is usually diffuse and pressure-like and should raise concern for hypertensive crisis or secondary intracranial pathology.
Infectious Causes
Intracranial infections may cause secondary headache due to inflammation, mass effect, or increased intracranial pressure.
Headache is often progressive and may be accompanied by fever, altered mental status, or focal neurological signs.
These include:
- Intracranial empyema
- Brain abscess
Trauma-Related Headache
Headache following head injury may result from the concussion itself or from delayed structural intracranial complications.
A key cause is traumatic chronic subdural hematoma, in which headache may develop days or weeks after injury and progressively worsen.
Brain Tumors and Other Space-Occupying Lesions
Headache caused by intracranial mass lesions is typically progressive and differs from primary headache disorders.
It may be worse in the morning, exacerbated by coughing or straining, and associated with nausea, vomiting, seizures, or focal neurological deficits.
Common space-occupying causes of secondary headache include:
- Gliomas (including glioblastoma, astrocytoma, oligodendroglioma)
- Meningiomas (olfactory, convexity, parasagittal, sphenoid)
- Brain metastases
- Pituitary adenomas
- Chronic subdural hematomas
- Other brain tumors
- Other intracranial mass lesions
Vascular Causes of Headache
Vascular headaches often present acutely or subacutely and may be unusually severe.
They can be associated with neurological deficits, altered consciousness, or rapid clinical deterioration.
Vascular causes of secondary headache include:
- Arteriovenous malformations (AVM)
- Cavernous malformations (cavernomas)
- Intracranial aneurysms (particularly when ruptured or enlarging)
- Cerebral venous sinus thrombosis
- Intracranial hemorrhage (parenchymal or subarachnoid)
Red Flags: When Headache Requires Further Evaluation
A headache should not be dismissed when it shows any of the following features:
- New-onset headache after the age of 40–50
- Progressive worsening over time
- Headache associated with seizures
- Headache accompanied by neurological deficits
- Morning headache with nausea or vomiting
- Headache following head injury
- Headache resistant to previously effective treatment
In such cases, neuroimaging and specialist evaluation are often necessary.
Thunderclap Headache
Thunderclap headache describes a sudden-onset, severe headache reaching maximal intensity within seconds to minutes.
This pattern represents a medical emergency, as it may indicate serious vascular conditions such as subarachnoid hemorrhage or other acute intracranial events such as spontaneous intracerebral hemorrhage.
Headache in the Context of Chronic Pain and Neurosurgical Conditions
While most headaches are managed conservatively, some are part of broader neurological or neurosurgical conditions, including neuralgias, epilepsy-related lesions, chronic subdural hematomas, or brain tumors.
Understanding when headache is a symptom rather than the primary disorder is essential for appropriate decision-making.
When to Seek a Specialist Opinion
If headache patterns change, become progressive, or are associated with seizures or other neurological symptoms, a focused neurological or neurosurgical assessment may be helpful—particularly when prior evaluations have not provided clear answers.