Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Neurosurgeon and Pain Management Specialist
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
January 6, 2026
Who This Brain Tumors Page Is For
This brain tumors overview page is designed primarily for patients who have been diagnosed with a brain tumor (or told they may have one), as well as for family members seeking to understand imaging findings and treatment options.
It is especially intended for those who were told that the situation is “complex,” “high risk,” or “uncertain,”
and who want to understand what different tumor types mean, how diagnosis is established,
when surgery is indicated, and how modern treatment decisions are made using imaging, pathology, and molecular markers.
The page explains core concepts such as benign versus malignant tumors, infiltrative growth, brain edema and mass effect,
the role of MRI and advanced imaging, surgical strategies (maximum safe resection, biopsy, awake surgery),
and how radiation and chemotherapy are integrated into treatment plans.
If the information raises questions about diagnosis, operability, prognosis, or whether the proposed treatment strategy is optimal,
you may contact us to see how we provide an individualized
neurosurgery second opinion
tailored to your specific case.
When patients and families usually seek a neurosurgical second opinion for brain tumors
• The diagnosis feels complex or difficult to understand
• Surgery is described as high risk or “not recommended”
• Treatment options seem unclear or contradictory
• The tumor was found incidentally, and the current recommendation is “watch and monitor” (active surveillance)
• Imaging, pathology, or molecular findings raise new questions
In neuro-oncology, seeking an independent expert opinion is a common and responsible step.
If this reflects your situation, you can request an individualized neurosurgical review here:
Request Second Opinion
Contents
- Who This Page Is For
- 100+ Tumor Types
- Causes Overview
- WHO Grades
- Growth Patterns
- Key Symptoms
- Functional Status (Karnofsky Score)
- Diagnosis (MRI)
- Treatment Strategy
- Surgery Options
- Surgery vs Biopsy
- Surgery Outcomes
- Pathology & Markers
- Radiation Therapy
- Chemo & Targeted
- Complementary Methods
- Gliomas
- Meningiomas
- Schwannomas
- Pituitary Tumors
- Brain Metastases
- Pediatric Tumors
- Request Consultation
- Brain Tumor FAQs
- Patient Resources
- MAS (PubMed)
There Are More Than 100 Types of Tumors That Can Grow Inside the Skull
According to the World Health Organization (WHO 2021) classification and the CBTRUS (latest edition) report, there are over 100 distinct types of tumors that can develop inside the skull. These are broadly classified into two categories: Primary and Secondary (Metastatic) tumors.
In clinical practice, more than 90% of adult cases are represented by the following groups:
Primary Brain Tumors
These tumors originate from the brain tissue or its surrounding structures.
- Gliomas: This is the most critical group of primary tumors, including astrocytomas, oligodendrogliomas, and glioblastomas. Notably, glioblastoma is the most common and aggressive primary malignant brain tumor, accounting for more than 50% of malignant primary brain tumors, and approximately ~14% of all primary intracranial tumors when benign entities are included.
- Meningiomas: These arise from the protective membranes covering the brain. They are the most frequent primary brain tumors, representing between 35% and 41% of all primary cases.
- Pituitary Adenomas: These tumors grow in the pituitary gland at the base of the skull and account for approximately ~10–15% of primary brain tumors.
- Schwannomas (Neurinomas): These develop from nerve sheaths (most often the acoustic nerve) and make up roughly ~5–10% of primary intracranial tumors.
Secondary Brain Tumors (Metastases)
Secondary tumors, or metastases, are cancers that have spread to the brain from distant organs (such as the lungs, breast, or kidney).
- Incidence: In clinical practice, metastases are the most common tumors found inside the skull, accounting for approximately 50% of all intracranial tumors in adults.
Causes of Brain Tumors
Brain tumors, like other tumors in the body, arise as a consequence of changes (mutations) in specific genes of normal cells. During these changes, two primary types of genes are affected:
- Proto-oncogenes: In a healthy cell, these genes function only at strictly controlled levels. When they mutate into oncogenes, they become permanently active. This triggers accelerated cell division and allows tumor cells to become increasingly autonomous, meaning they no longer respond to the external regulatory signals that normally control cell growth. Functionally, this process resembles a “gas pedal” that is stuck in the pressed position.
- Tumor Suppressor Genes: Their role is to inhibit uncontrolled cell multiplication. When these genes become inactivated by mutation, the cell loses its natural “brakes.”
Such genetic changes occur constantly in the human body in a large number of cells, but in most cases, the immune system recognizes and neutralizes them. However, in situations where these cells escape immune control and continue to multiply uncontrollably, tumor formation occurs.
Initially, a tumor is often benign (non-cancerous), but over time, additional genetic mutations may accumulate, giving the tumor increasingly aggressive characteristics and allowing it to transform into a malignant form. The reasons why these additional genetic changes occur are not always fully known. However, it is important to note that some of the most aggressive tumors, such as Glioblastomas, are often malignant from the very beginning (known as de novo tumors) and do not pass through a detectable benign stage. While we understand the cellular mechanisms, the exact triggers that initiate these initial or cumulative mutations remain a subject of intensive research.
Heredity and Genetic Predisposition
In a small number of people, there are inherited syndromes (such as Neurofibromatosis) that increase the risk. However, it is important to clarify that while all individuals inherit normal proto-oncogenes and tumor suppressor genes, the vast majority of brain tumors arise from somatic mutations acquired during life and are not inherited.
Influence of External Factors on the Origin of Brain Tumors
The influence of external factors is still being intensively studied. Current scientific knowledge indicates the following:
- Ionizing Radiation: Exposure to high-dose radiation is a well-established risk factor for developing brain tumors.
- Infections and Inflammation: Researchers are investigating the role of prior viral infections and long-term inflammatory processes, though results are not yet conclusive for most tumor types.
- Chemicals: Exposure to certain pesticides and industrial chemicals continues to be monitored as a potential risk factor.
- Stress and Lifestyle: Patients frequently ask about stress, head injuries, overwork, or the use of mobile phones. At present, there is no scientific evidence that these factors directly cause brain tumors, but their possible long-term effects continue to be tracked in large-scale studies.
Classification of Brain Tumors by Malignancy
Based on how rapidly they progress and the percentage of cases in which they can be cured, these tumors are classified as benign (non-cancerous) or malignant (cancerous). This classification is further refined into WHO grades (I–IV), where higher grades indicate more aggressive growth and a greater tendency to invade healthy tissue.
Meningiomas, neurinomas, and pituitary adenomas are most often benign. Metastases are always the result of malignant disease, while gliomas are more often malignant. One type of glioma—glioblastoma—is the most common malignant brain tumor.
Classification by Growth Pattern of Brain Tumors
According to their growth behavior, tumors can be divided into those that, by their growth, only compress surrounding parts of the brain, and those that infiltrate (invade) surrounding brain tissue, as well as combined forms.
(For example, large malignant tumors infiltrate the brain and also exert pressure on it.). Additionally, many tumors cause brain edema (swelling) by leaking fluid into the surrounding area, which increases intracranial pressure and often intensifies neurological symptoms.
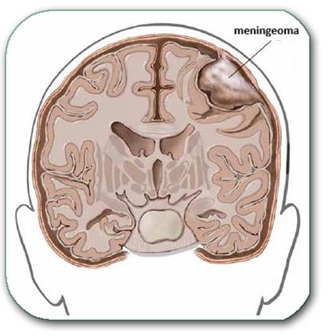
Image: A meningioma growing from the coverings of the brain and compressing surrounding parts of the brain, without infiltrating them.
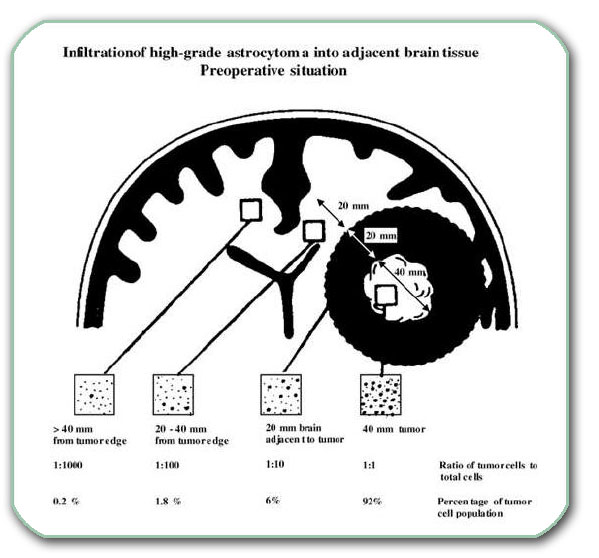
Image: A cross-section of the two cerebral hemispheres. In one hemisphere there is a large malignant glioma (approximately 4 centimeters in diameter). Tumor cells have already penetrated into the wider surrounding area (even into the opposite hemisphere) by infiltration.
Symptoms of Brain Tumors
When a tumor reaches a significant size, it exerts pressure on the surrounding brain tissue, causes brain swelling, disrupts blood circulation in nervous tissue, and may also lead to bleeding. The mechanisms by which a tumor damages nervous tissue are numerous and overlap with each other.
All of this results in symptoms such as headache, epilepsy (seizures), drowsiness, and various deficits in brain and cranial nerve function. The functional deficits depend on the tumor’s location and size. These may include disorders of vision, speech, hearing, smell, movement of the limbs, balance, sense of touch, and psychiatric disturbances, …
In benign tumors, one or several symptoms usually appear first, and then—for months or even years—no new symptoms develop despite continued tumor growth. Because of their slow growth, additional symptoms typically emerge only when the tumor becomes large enough to compress adjacent neural structures. A typical example is a vestibular schwannoma (acoustic neuroma), which often initially causes hearing loss and balance disturbances on one side. For a long time, these may remain the only symptoms. Additional neurological deficits usually appear only later, when the tumor grows sufficiently to compress neighboring cranial nerves or the brainstem.
Functional Status and the Karnofsky Performance Scale (KPS)
In patients with malignant brain tumors, symptoms alone are not sufficient to assess disease severity or to guide treatment decisions. Equally important is the patient’s functional status — how the tumor affects daily activity, independence, and overall physical condition.
One of the most widely used tools in neuro-oncology for this purpose is the Karnofsky Performance Status (KPS). KPS plays a central role in the evaluation of malignant brain tumors because it directly influences:
- assessment of overall disease severity and biological impact
- indications for surgical treatment and operability
- eligibility for radiation therapy and chemotherapy
- tolerance of aggressive treatment protocols
- interpretation of treatment results and prognosis
In high-grade gliomas and other malignant tumors, a lower Karnofsky score often reflects both tumor aggressiveness and the extent of functional brain involvement. For this reason, KPS is a key parameter in balancing surgical radicality with preservation of quality of life.
| Karnofsky Score | Functional Meaning |
|---|---|
| 90–100 | Normal activity or only minor symptoms |
| 70–80 | Independent, but unable to carry out normal work |
| 50–60 | Requires assistance and frequent medical care |
| < 50 | Severe disability, limited self-care |
It is important to note that the Karnofsky score does not define tumor malignancy by itself. Rather, it reflects the functional consequences of the disease and is interpreted together with imaging, pathohistological findings, and molecular markers to guide individualized treatment decisions.
Diagnosis of Brain Tumors
Because small tumors are significantly easier to treat than large ones, early diagnosis is critical. The gold standard and most important diagnostic method is Magnetic Resonance Imaging (MRI) of the brain.
With the widespread availability of MRI scanners today, this examination should be performed at the onset of any symptoms suggesting a potential tumor. This includes cases of sensorineural hearing loss, new-onset epilepsy, disorders of smell or vision, and unexplained psychiatric disturbances.
The procedure is painless and typically lasts between 15 and 45 minutes. It requires the patient to remain still in a confined space while being exposed to rhythmic noise. For patients with claustrophobia or severe anxiety, the imaging can be performed under sedation or light anesthesia to ensure comfort and image quality. For brain tumors, an MRI is typically performed both before and after the administration of a contrast agent. Therefore, kidney function is assessed and an intravenous (IV) line is placed prior to the scan.
The MRI scan reveals the tumor’s location, size, and probable type, its relationship with critical surrounding structures (e.g., functional centers, major white matter tracts, blood vessels, and nerves), as well as the presence of complications (mass effect, herniation, ischemia, hemorrhage, hydrocephalus, etc.). These tumor characteristics determine the neurosurgeon’s operative approach; this is why neurosurgeons often examine the imaging data through different eyes than radiologists. For this reason, unlike other medical specialties, a radiologist’s written report alone is never sufficient for a neurosurgeon.
Advanced and Additional Diagnostic Methods
Beyond standard MRI, specialized imaging techniques are often used to refine the diagnosis and plan surgical interventions:
- Functional MRI (fMRI): Maps the relationship between the tumor and vital brain centers (e.g., speech or motor functions).
- MRI Spectroscopy (MRS): Helps differentiate the tumor type and grade before surgery by analyzing chemical metabolites.
- MR Angiography (MRA): Visualizes the blood vessels surrounding or feeding the tumor.
- MR Tractography (DTI): Visualizes white matter pathways to help plan the safest surgical approach.
Other diagnostic tools may include Computed Tomography (CT), EEG, evoked potentials, endocrine (hormonal) evaluations, and specialized vision or hearing tests. In some cases, skeletal scintigraphy (bone scans) may be required to detect systemic involvement.
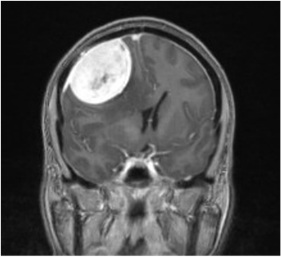
Image: Brain MRI showing a meningioma in the right parietal region, causing a significant mass effect on the brain due to its size and surrounding edema.
Comprehensive Medical Evaluation
It is essential to conduct a full oncologic evaluation (imaging of other organs) to determine if the brain tumor is primary or a metastasis from elsewhere in the body. Furthermore, assessing the patient’s overall health is vital for safe anesthesia and personalized treatment planning.
At a minimum, the following preoperative assessments are required: comprehensive blood and urine laboratory tests, ECG, chest X-ray, and an abdominal ultrasound. Depending on the patient’s medical history, additional specialist consultations—such as cardiologic, urologic, or gynecologic evaluations—may be performed.
Treatment of Brain Tumors
Once a brain tumor is diagnosed, a multidisciplinary team of specialists (often referred to as a Neuro-Oncology Board) evaluates the case to determine the most effective treatment plan. The available options generally fall into three categories: symptomatic treatment, surgical intervention, and adjuvant therapy (such as radiation or chemotherapy).
The treatment strategy is based on the latest neuro-oncological clinical guidelines and the patient’s overall health.
In specific situations—most often in elderly patients or in those with significant comorbidities—a brain tumor may be stable and not currently impairing brain function. In such cases, immediate active treatment is not always necessary. In everyday neuro-oncological practice, approximately one quarter of newly diagnosed intracranial tumors are initially managed with active surveillance rather than surgery or adjuvant therapy. This approach is especially common for tumors that are small, slow-growing, and not causing relevant mass effect or neurological deficits.
Typical examples include:
- small vestibular schwannomas, particularly when hearing is still preserved
- calcified or minimally growing meningiomas, especially in older patients
- non-functioning pituitary adenomas that show no progression on follow-up imaging
- selected low-grade or diffuse gliotic infiltrations, particularly in pediatric patients
Active surveillance involves structured follow-up with periodic MRI examinations and clinical assessment. The goal is not to avoid treatment, but to postpone invasive interventions until there is clear evidence of tumor growth, new symptoms, or functional compromise.
Symptomatic Treatment of Brain Tumors
Symptomatic treatment is administered to manage complications caused by the tumor’s presence, such as brain swelling, headaches, seizures (epilepsy), and vomiting.
To manage brain edema (swelling), corticosteroids (most commonly Dexamethasone/Dexason) are prescribed. These medications are typically administered via injection or in tablet form. Because long-term corticosteroid use can affect the digestive system, medications to protect the stomach lining are often prescribed concurrently. Additionally, patients experiencing seizures are treated with anti-epileptic drugs (AEDs) to stabilize electrical activity in the brain.
In certain situations, symptomatic (palliative) treatment represents the only appropriate therapeutic approach. This most often applies to patients with very aggressive malignant brain tumors who have a severely reduced Karnofsky Performance Status (KPS), indicating profound functional impairment. In such cases, the risks of surgery, radiation, or chemotherapy clearly outweigh any potential benefit, and active oncological treatment would not improve survival or quality of life. A similar approach is taken in patients with advanced systemic malignancies with brain involvement, where the overall prognosis is poor and neurological symptoms are part of a widespread disease process. In these circumstances, treatment is focused exclusively on symptom control and comfort — reducing brain edema, relieving pain, controlling seizures, managing agitation or confusion, and supporting basic neurological function. The primary goal is to preserve dignity, minimize suffering, and maintain the best possible quality of life for the remaining time.
Surgical Treatment of Brain Tumors
Surgical treatment involves opening the skull (craniotomy), reaching the tumor, and removing it. During the procedure, vital surrounding structures—such as healthy brain tissue, cranial nerves, and blood vessels—must be carefully separated from the tumor.
Total removal is often impossible if the tumor grows infiltratively, which is common in most gliomas and aggressive malignant variants of other tumor types. Furthermore, if a benign tumor becomes very large, it may thin and adhere to surrounding structures so strongly that separating them without causing functional damage becomes impossible. This highlights the critical importance of early diagnosis while the tumor is still small.
Depending on the tumor’s relationship with the surrounding brain, the surgeon performs either:
- Complete removal (ablation): Total excision of the tumor mass.
- Partial removal (reduction/debulking): This involves removing the majority of the tumor to relieve pressure while leaving small remnants or infiltrative parts to protect vital functions. Thanks to advanced techniques such as stereotactic radiation, these small remnants of benign tumors can be effectively controlled to prevent further growth or even be significantly reduced in size. For infiltrative and malignant forms, adjuvant therapy (radiation and/or chemotherapy) must be performed according to the specific treatment protocol for that tumor type.
In high-risk cases where surgery is too dangerous or diagnosis is uncertain, only tumor samples (biopsy) are taken to determine the exact type of tumor. This is often performed stereotactically, using precision guidance systems. The procedure involves inserting a specialized biopsy needle through a small burr hole in the skull, guided with sub-millimeter accuracy by a stereotactic frame or neuronavigation (frameless stereotaxy).
Modern Surgical Technologies in Brain Tumor Surgery
To ensure the best possible outcome, surgery should be performed by a specialist with extensive microsurgical experience. Surgical plan depends mostly on: the tumor’s location, size, and probable type, its relationship with critical surrounding structures (e.g., functional centers, major white matter tracts, blood vessels, and nerves), as well as the presence of complications (mass effect, herniation, ischemia, hemorrhage, hydrocephalus, etc.).
Modern neurosurgery utilizes advanced technologies to make procedures more precise and safer:
- Neuronavigation (Intraoperative GPS): Using MRI/CT data and ultrasound to navigate precisely to deep-seated tumors.
- Fluorescence-guided surgery: Using special dyes (like 5-ALA) that make tumor cells „glow“ under the microscope to distinguish them from healthy brain tissue.
- Intraoperative Neurophysiological Monitoring (IONM): Continuous monitoring of nerve functions during surgery to prevent paralysis or sensory loss.
- Ultrasonic Aspirator (CUSA): A tool that uses ultrasonic vibrations to fragment and remove tumors while sparing blood vessels and nerves.
- Awake Craniotomy: Performed on tumors near the speech or motor centers. This allows the surgeon to interact with the patient during the procedure to ensure vital functions remain intact.
Read more about potential complications following craniotomy and open brain surgery on this page.

Image: The image illustrates a craniotomy. Both the skin incision and the skull opening are performed within the hair-bearing area of the scalp. The dura is opened to expose the brain as part of the surgical approach to the tumor. After the procedure, the bone flap is secured and the scalp is reconstructed, ensuring no cosmetic defect remains after healing.
Surgery vs Biopsy: clinical indications and limitations
The decision between surgical resection and biopsy in brain tumors is based on tumor extent, surgical risk, expected benefit of non-surgical therapy, and the need for precise biological diagnosis. Surgery is not automatically the best option and, in many cases, is intentionally avoided or postponed for well-defined medical reasons.
When surgery is not indicated because of tumor extent
Surgical resection is not indicated when the tumor is extensive or diffusely infiltrative, making meaningful cytoreduction impossible. Typical examples include:
- Butterfly glioblastoma crossing the corpus callosum
- diffuse high-grade gliomas with bilateral hemispheric involvement
- tumors with widespread deep white-matter or subependymal spread
In these situations, surgery does not improve survival or functional outcome and exposes the patient to significant neurological risk. Biopsy is required to establish histopathological and molecular diagnosis necessary for adjuvant treatment planning.
When surgery is avoided because it is neurologically dangerous
Surgery may be avoided or intentionally limited when the tumor is located in critical or eloquent brain regions, where resection carries a high risk of permanent neurological deficit, including:
- the brainstem
- deep basal ganglia or thalamus
- eloquent cortex responsible for speech, movement, or vision
Here, the limitation is surgical risk, not lack of treatment intent. Biopsy enables diagnostic certainty while preserving neurological function.
When adjuvant therapy offers greater benefit than immediate surgery
In certain tumors, primary non-surgical treatment provides superior outcomes, and surgical resection would not alter management. Examples include:
- primary CNS lymphoma
- tumors with high radiosensitivity or chemosensitivity
- cases where molecular profiling primarily determines therapy
In such cases, surgery is not avoided because it is impossible, but because it does not add therapeutic value beyond diagnosis. Biopsy is essential to guide definitive treatment.
When biopsy is necessary as preparation for surgery
Biopsy is not limited to non-surgical cases. In selected situations, it represents a necessary preparatory step even when surgery is being considered.
Histopathological and molecular analysis may be required to:
- confirm tumor type and grade
- identify molecular markers with prognostic and therapeutic relevance
- determine whether surgery is indicated at all
- define the timing and safe extent of resection
Biopsy results may support delayed surgery, limited resection, or initiation of preoperative therapy before any operative intervention.
When surgery provides clear therapeutic benefit
Surgical resection is indicated when it is expected to:
- significantly reduce tumor burden
- relieve mass effect or intracranial hypertension
- improve neurological symptoms
- enhance the effectiveness of adjuvant radiotherapy or chemotherapy
In these situations, surgery remains a central component of multimodal treatment.
Final clinical perspective
Biopsy is not a lesser option but a necessary step in cases where resection is not indicated.
When surgical removal is unsafe, unlikely to provide benefit, or would not change the therapeutic strategy, biopsy represents the most responsible and medically correct decision.
Histopathological and molecular analysis obtained through biopsy directly guides adjuvant therapy and has clear prognostic and therapeutic implications.
Modern neuro-oncology is no longer defined solely by what can be surgically removed, but by precise biological characterization of the tumor, which determines treatment selection, survival, and quality of life.
Choosing biopsy in these situations reflects clinical judgment and experience, not therapeutic limitation, and forms the foundation of individualized, evidence-based care.
Results of Surgical Treatment of Brain Tumors
The outcomes of surgical treatment depend primarily on the type, malignancy, size, and location of the tumor.
- Surgical Mortality: In modern neurosurgery, mortality related directly to the procedure is generally less than 1%. When it occurs, it is usually due to the complications of pre-existing medical conditions.
- Neurological Deficits: The risk of postoperative deficits depends on the tumor’s size and its proximity to vital brain areas. In most cases, severe neurological deficits occur in less than 1% of patients. For tumors in complex or „eloquent“ locations, the risk can increase up to 20%.
- Temporary vs. Permanent: It is important to distinguish between temporary deficits, which may occur due to post-operative brain swelling and resolve as the brain heals, and permanent deficits, which occur if vital structures are directly affected by the tumor or its removal.
It is essential that all potential risks associated with the specific type of surgery—whether complete removal or tumor reduction—are thoroughly explained in advance to the patient and their family. This ensures informed consent and prepares everyone for the recovery and rehabilitation process.
Pathohistological Analysis (PH Analysis)
The definitive nature of a tumor is determined 4–7 days after surgery through a comprehensive analysis of the removed tissue. While traditional pathohistological analysis (PH analysis) uses special staining techniques and microscopic examination to determine the tumor type and grade, modern diagnostics go much further.
Today, this process is significantly enhanced by:
- Immunohistochemistry (IHC): Used to detect specific proteins and markers within the cells to confirm the tumor’s origin.
- Chromosomal and Genetic Analysis: Identifies specific genetic alterations. For example, the presence of an IDH mutation in astrocytoma or 1p/19q co-deletion in oligodendroglioma can mean a significantly better prognosis and a different response to therapy than tumors without these markers.
- Molecular Grading: We are increasingly identifying specific genes (such as MGMT promoter methylation) that predict how well a tumor will respond to chemotherapy and help determine the biological aggressiveness of the tumor, beyond what is seen under the microscope.
Modern diagnostics are moving closer to the root cause of malignancy. In the near future, a „true diagnosis“ will likely transcend simple naming; it will involve identifying the exact cell of origin and a complete map of mutated genes. This will allow for Targeted Therapy, where specific drugs are designed to attack only the mutated proteins or genes, minimizing damage to healthy brain tissue.
Based on this integrated molecular and PH profile, the multidisciplinary board decides on the necessity and type of adjuvant treatment, such as radiation or personalized chemotherapy.
Radiation Therapy and Chemotherapy for Brain Tumors
Adjuvant treatment methods, which include radiation therapy and chemotherapy, are used to eliminate remaining tumor cells and prevent recurrence after surgical intervention.
Radiation Therapy
is most often delivered using sophisticated devices designed to target the tumor with high-energy beams. The goal is to deliver the highest radiation dose (measured in Gray—Gy) to the tumor while minimizing exposure to the surrounding healthy brain tissue.
The highest level of precision is achieved through radiosurgical methods (such as Gamma Knife, LINAC, and Proton Therapy). These technologies allow for extremely targeted treatment:
- They are highly effective at stopping tumor growth for masses no larger than 2.5–3.5 cm in diameter.
- They are ideal for treating small tumor remnants that were strategically left behind during surgery to protect vital functions.
- However, their use is limited if the tumor is located too close to critical structures (like the optic nerves or brainstem) that cannot tolerate high doses of radiation.
Chemotherapy and Targeted Treatment
Chemotherapy involves the use of specialized drugs (cytostatics) to kill tumor cells or stop them from dividing. Unlike many other cancers that require intravenous therapy, the primary treatment for many brain tumors (e.g., astrocytoma, GBM) is Temozolomide (Temodar), an oral chemotherapy agent administered in capsule form.
Other Agents: For recurrent tumors or specific types like lymphomas or medulloblastomas, other protocols (such as PCV or Bevacizumab/Avastin) may be used to target the tumor’s blood supply or different cellular mechanisms.
Temozolomide (Temodar): This is an oral chemotherapy agent (taken in capsule form) that is uniquely effective because it can cross the blood-brain barrier—the protective shield that prevents many other drugs from entering brain tissue.
The MGMT Connection: The effectiveness of Temodar is closely linked to the MGMT promoter methylation status. If the MGMT gene is „silenced“ (methylated), the tumor cells cannot repair the damage caused by Temodar, making the treatment significantly more effective.
Radiochemotherapy: In many aggressive cases, Temodar is administered daily alongside radiation therapy. This combination acts as a „radio-sensitizer,“ making the radiation more lethal to tumor cells. After radiation is complete, the patient usually continues with maintenance cycles of Temodar.
Alternative Treatment Methods in Brain Tumors
Standard medical treatment modalities are not necessarily in contradiction with most alternative or complementary methods. However, it is essential that patients discuss any such methods with their medical specialists before implementation. The purpose of these discussions is not to discourage patients from exploring alternative therapies, but to prevent situations where such advice might interfere with the efficacy of evidence-based medical treatment. Complementary approaches must not delay evidence-based treatment decisions.
In some cases, alternative practitioners may inappropriately suggest modifications to the primary treatment or prescribe supplements that the patient is already receiving in a different form. Furthermore, emphasis is often placed on substances that have not been scientifically proven to be effective or, in some instances, may even be harmful or counteract the effects of chemotherapy and radiation. Transparency with the neuro-oncology team is vital to ensure that any complementary therapy supports, rather than undermines, the patient’s recovery.
The specific characteristics of individual types of brain tumors are explained below.
Gliomas of the Brain
Gliomas are the most common primary brain tumors, originating from the glial (supportive) cells of the brain. The latest WHO Classification of Tumours of the Central Nervous System (5th Edition) identifies more than 100 distinct types and subtypes of gliomas and related tumors, highlighting the immense diversity and complexity of these diseases.
They are broadly categorized into several families, with the most clinical relevance for adults being:
- Adult-type Diffuse Gliomas: This is the most frequent group, consisting of Astrocytomas (IDH-mutant), Oligodendrogliomas (IDH-mutant and 1p/19q-codeleted), and Glioblastomas (IDH-wildtype).
- Pediatric-type Gliomas: A distinct group of tumors found in children, further divided into low-grade and high-grade types based on specific genetic mutations.
- Ependymal Tumors (Ependymomas): These also belong to the glioma family; they arise from the ependymal cells lining the brain’s ventricles and the central canal of the spinal cord.
- Circumscribed Astrocytic Gliomas: These include types like Pilocytic Astrocytoma, which grow in a more localized manner compared to diffuse gliomas.
Distribution of Adult-Type Gliomas
Approximately 90% of all gliomas in adults belong to the group of diffuse gliomas, which include both lower-grade infiltrative tumors and highly malignant disease.
Their approximate distribution is:
Oligodendroglioma (IDH-mutant, 1p/19q-codeleted)
• Accounts for ~5–10% of adult diffuse gliomas
• Classified as WHO grade 2 or grade 3
• Grade 3 oligodendrogliomas are malignant tumors requiring combined surgical and adjuvant treatment
Glioblastoma (IDH-wildtype)
• Most frequent and most aggressive adult glioma
• Accounts for ~60–70% of adult diffuse gliomas
• Defined as WHO grade 4 by definition
The most common „imitators“ of glioblastoma include: brain lymphoma, brain metastases, and abscess
Astrocytoma (IDH-mutant)
• Represents ~15–20% of adult diffuse gliomas
• Includes WHO grade 2, grade 3, and grade 4 tumors
• Higher-grade forms (grades 3 and 4) are malignant and often clinically aggressive
Gliomas most often, during their growth, infiltrate surrounding brain structures. They have a high potential to become malignant. According to the degree of malignancy (WHO classification), they are classified into four grades:
- Grade I: A complete cure is very likely after successful surgical removal.
- Grade II: These are slower-growing but infiltrative; survival longer than five years is present in 50–75% of cases.
- Grades III and IV: These represent more aggressive, malignant forms where the survival period is significantly shorter.
Surgical Treatment of Brain Gliomas: Goals and Philosophy
The primary objective of surgery for brain gliomas is the maximum safe resection of the tumor tissue. However, the surgical strategy differs significantly depending on the tumor’s malignancy and growth pattern.
1. Surgery for Malignant Gliomas (High-Grade)
In malignant cases, the main goal is to remove as much of the contrast-enhancing portion of the tumor as seen on the MRI.
- Extent of Resection: Clinical data suggests that the goal should be a decompression or the removal of more than 76% of the tumor mass to significantly impact survival.
- Preserving Quality of Life: The surgeon must carefully avoid causing new neurological deficits. If a radical resection results in a decreased Karnofsky Performance Status (KPS)—leaving the patient unable to care for themselves—the surgery will not achieve its goal of prolonging life. Functional survival is as important as surgical radicality.
2. Surgery for Low-Grade (Infiltrative) Astrocytomas
Because these tumors often do not enhance on contrast, the surgical approach is different:
- Signal Abnormality: The goal is to remove everything that appears as an altered signal on the MRI (FLAIR/T2 sequences).
- Surgical Technique: Since there is often no clear boundary (cleavage plane) between the tumor and healthy brain tissue, surgeons use neuronavigation to follow anatomical landmarks like brain sulci.
- Supratotal Resection: Instead of searching for a margin that is hard to detect, the strategy involves safe removing the specific brain segments containing the tumor while monitoring functional integrity.
Adjuvant Treatment of Gliomas
After surgery, radiation therapy is almost always performed, and chemotherapy is often indicated. The choice of therapy depends on the tumor subtype:
- Ependymomas: These tumors generally respond more effectively to radiation therapy, which is often the primary adjuvant treatment to ensure local control.
- Oligodendrogliomas: This subtype tends to respond better to chemotherapy, particularly when specific molecular markers are present, allowing for a more tailored drug-based approach.
Exceptions to Adjuvant Treatment of Gliomas
In certain scenarios, adjuvant therapy (radiation and chemotherapy) is not required, and the medical team may opt for clinical monitoring. This typically occurs in the following cases:
- Completely Removed Low-Grade Gliomas: If a low-grade glioma (WHO Grade 1 or specific Grade 2 cases) has been fully resected (total removal), the risk of immediate recurrence is low enough that further treatment may be deferred in favor of regular MRI follow-ups.
- Grade 1 Tumors in Children: Pediatric tumors, such as pilocytic astrocytomas, which have the radiological and biological characteristics of Grade 1 tumors, often have an excellent prognosis. If these are surgically removed or remain stable, adjuvant therapy is avoided to protect the developing brain from the side effects of radiation.
- Stable Non-Progressive Lesions: In cases of certain gliozises or very slow-growing benign tumors where the surgical risk outweighs the benefits, and the lesion is not causing neurological deficits, „active surveillance“ is the preferred strategy.
Scoring System for Malignant Brain Gliomas (The MAS Method)
To provide a more accurate assessment of illness severity and prognosis, we utilize the Malignant Astrocytoma Score (MAS). Developed by the author of this website and published in international medical literature (including PubMed/NIH and ResearchGate), this system allows for a highly individualized approach to treatment planning.
The MAS method calculates a prognosis based on four key clinical factors:
- Age: The patient’s age at the time of diagnosis.
- Karnofsky Performance Status (KPS): An assessment of the patient’s functional abilities and quality of life.
- Histopathological Grade (PH): The specific malignancy of the tumor cells as determined by a pathologist.
- Preoperative Seizures: Whether the patient experienced seizures for at least six months prior to diagnosis, which often indicates a specific biological behavior of the tumor.
This research has been validated and published in international medical literature. You can access the original study here: The Evaluation of Malignant Astrocytoma Score (MAS) – PubMed.
Integration with Modern Molecular Markers
While the MAS score remains a robust clinical tool, it is most effective when used in conjunction with other modern prognostic parameters. Research and clinical practice show that the MAS score correlates excellently with molecular markers, particularly the IDH mutation status.
By combining clinical data from the MAS system with genetic insights (such as IDH status and MGMT methylation), we can achieve a truly comprehensive „Integrated Diagnosis.“ This synergy allows us to predict the tumor’s behavior more accurately and customize the therapy to achieve the best possible outcome for the patient.
Meningiomas
Meningiomas are, in most cases, benign (non-cancerous) tumors. They grow from the coverings of the brain (meninges), compressing surrounding parts of the brain, nerves, and blood vessels.
Usually, they are not firmly adherent to surrounding structures so that they can be completely removed.
Meningiomas can grow in different parts of the skull:
- above the cerebral hemispheres
- above the cerebellum
- in various regions of the skull base, …
The symptoms and neurological deficits they cause depend on the size and location of the meningioma.
(A large number of very different clinical presentations is possible.)
For information on tumor development, growth, diagnosis, and treatment, see the introductory section.
It is important that the diagnosis is made while the tumors are still small.
There are also malignant variants, such as atypical meningioma and meningosarcoma.
When a tumor inside the skull is diagnosed, there are many indicators suggesting that it is a meningioma. At that point, experience is required to decide whether the patient should undergo surgery or whether the tumor should only be monitored. Monitoring is most often chosen when we believe that the tumor does not cause significant pressure on surrounding structures and that it has stopped growing or is growing very slowly. This is particularly the case in elderly patients or patients who are severely ill due to other diseases.
Fortunately, with good surgical technique, it is possible to completely remove the vast majority of meningiomas without major neurological deficits, especially if the tumor is not large and has a favorable location.
Meningiomas: Classification by Location
Meningiomas are typically named after the specific anatomical site where they originate. Understanding the location is critical because it determines the surgical approach and the potential impact on surrounding neurological structures.
Common locations for meningiomas include:
• Tentorial Meningioma: Found on the fold of tissue that separates the cerebrum from the cerebellum.
• Olfactory Groove Meningioma: Located at the anterior base of the skull, above the nose, near the nerves responsible for the sense of smell.
• Sphenoid Wing Meningioma (Medial or Lateral): Positioned along the sphenoid bone behind the eyes.
• Suprasellar / Tuberculum Sellae Meningioma: Found near the optic nerves and the pituitary gland.
• Cavernous Sinus Meningioma: Located in a complex area involving critical veins and cranial nerves behind the eye.
• Clival and Petroclival Meningioma: Deep-seated tumors located at the base of the skull near the brainstem.
• Foramen Magnum Meningioma: Situated where the brain joins the spinal cord.
• Cerebellopontine Angle (CPA) Meningioma: Found in the area between the cerebellum and the pons, often affecting hearing and balance.
• Convexity Meningioma: Located on the outer surface of the brain, directly under the skull.
• Parasagittal and Sagittal Sinus Meningioma: These involve or are adjacent to the large vein (superior sagittal sinus) that runs along the top of the brain.
• Posterior Fossa Meningioma: Located in the back of the skull near the cerebellum.
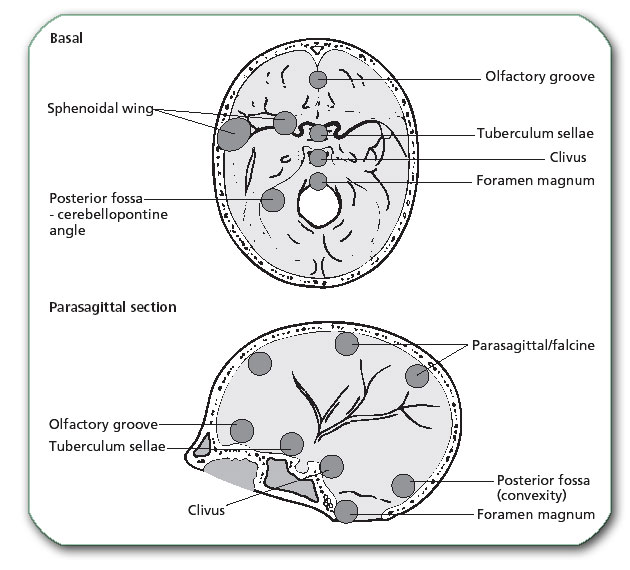
Image: Common locations of meningiomas
Neurinomas (Schwannomas)
Neurinomas arise from Schwann cells of peripheral nerves. They are most commonly localized on the hearing and balance nerve. Because of this, they usually begin with hearing loss and dizziness. This symptom may remain the only symptom for years.
Later, they may cause:
- facial numbness or pain due to trigeminal nerve compression (secondary trigeminal neuralgia)
- facial asymmetry due to facial nerve damage
- weakness of the limbs due to pressure on the brainstem
- hydrocephalus (accumulation of cerebrospinal fluid in the brain ventricles), …
For information on tumor development, growth, diagnosis, and treatment, see the introductory section.
It is important that the diagnosis is made while the tumors are still small.
When a tumor inside the skull is diagnosed, many indicators suggest that it is a neurinoma. Experience is then required to decide whether the patient should undergo surgery or whether the tumor should only be only monitored.
Clinical Surveillance is most often chosen when we believe that the tumor does not cause significant pressure on surrounding structures (brainstem, nearby nerves, cerebrospinal fluid pathways, …) and that it has stopped growing or is growing very slowly. This is particularly the case in elderly patients or patients who are severely ill due to other diseases.
Treatment Strategies for Acoustic Neuromas (Vestibular Schwannomas)
Modern diagnostic tools, particularly high-resolution MRI, now allow acoustic neuromas (vestibular schwannomas) to be detected much earlier than in the past. Today, the majority of these tumors are diagnosed while they are still small—most often below 2.5–3 cm in diameter. This shift toward early detection has fundamentally changed treatment strategy.
Because most newly diagnosed acoustic neuromas are small and do not yet cause significant brainstem compression, stereotactic radiosurgery (such as Gamma Knife or LINAC-based systems) has become the preferred primary treatment in many cases. The goal of radiosurgery is not immediate tumor removal, but long-term growth control while preserving neurological function, particularly hearing and facial nerve function.
Surgical resection is reserved for selected situations—most commonly for larger tumors, tumors causing significant mass effect on the brainstem, progressive neurological deficits, or when radiosurgery is not appropriate. Modern surgery for acoustic neuromas is highly specialized and should be performed only in experienced centers with advanced intraoperative neurophysiological monitoring, including continuous monitoring of brainstem function, the facial nerve, and the cochlear (acoustic) nerve. The goal of surgery, when indicated, is maximal safe removal while minimizing permanent neurological deficits.
Pituitary Tumors
These are tumors that grow from an endocrine gland located below the center of the brain and above the nose (the pituitary gland).
These tumors may produce excessive amounts of hormones and are therefore usually diagnosed earlier, while still small. Depending on which hormones are produced, the patient may develop:
- High Prolactin levels
- Cushing’s disease
- acromegaly
- or, more rarely, other hormonal disorders
If the tumor does not produce hormones, it usually grows significantly before causing the first symptoms. Large adenomas most often initially present with visual disturbances – loss of peripheral vision (bitemporal hemianopsia)
Later symptoms may include:
- decreased pituitary hormone production
- eye misalignment
- double vision
- frequent urination
- difficulty walking
- psychological disturbances
- signs of hydrocephalus
Some smaller tumors (most commonly prolactinomas) are treated with medications.
Most pituitary adenomas today can be removed by surgery through the nose, without opening the skull. In tumors that grow aggressively, radiation therapy may also be considered.
Most transnasal operations today are performed using an endoscope– Endoscopic Endonasal Approach (EEA). With these methods, a large number of skull base tumors can be removed “through the nose,” without opening the skull. These tumors often cannot be treated using other surgical methods. To perform these operations, in addition to endoscopy, extensive additional equipment is required, such as navigation systems and neurophysiological monitoring. The significant experience required for successful performance of these operations, as well as all necessary equipment, exists only in the largest centers.
The lack of these resources often leads to a practice where only smaller pituitary tumors are successfully removed, while larger and more adherent tumors are not completely excised.
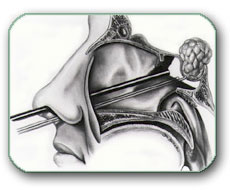
Image: Endoscopic Endonasal Approach (EEA) for pituitary tumor surgery
Brain Metastases
If a malignant tumor exists elsewhere in the body, malignant cells continuously detach from it and travel through the bloodstream. They may stop in various organs—most commonly the lungs, liver, and brain—where they multiply and form distant tumors (metastases).
The most common brain metastases originate from:
- lung cancer (about 50% of all brain metastases)
- breast cancer
- melanoma
- kidney cancer
- gastrointestinal cancers
- prostate cancer, …
Brain metastases can usually be completely removed surgically. Their removal should be pursued even when multiple metastases are present, especially when the prognosis for life expectancy and quality of life is favorable (for example, melanoma metastases).
If metastases are multiple, distant from one another, deeply located, and/or small in diameter, radiation therapy and/or chemotherapy may be used.
If the patient is in very poor general condition and in the terminal stage of malignant disease, only symptomatic treatment is indicated.
Personalized Surgical Strategy
Today, we take a much more aggressive and nuanced approach to surgery. The decision to operate is no longer based solely on the presence of a brain tumor, but on the overall clinical prognosis provided by the oncologist.
- Aggressive Resection: We often pursue the complete surgical removal of metastases even when multiple lesions are present, provided the patient’s systemic disease is under control. For example, melanoma or testicular seminoma metastases are often operated on aggressively because these patients can have a favorable long-term survival with modern immunotherapy and surgery.
- The „Hybrid“ Approach: In cases with multiple metastases, we frequently choose to surgically remove the largest, symptomatic lesions (to relieve pressure) while treating the remaining, smaller, or deeper lesions with Gamma Knife (stereotactic radiosurgery).
- When Surgery is Avoided: Certain tumors, such as small cell lung cancer (SCLC), are highly sensitive to radiation and chemotherapy but tend to be very diffuse. In these cases, surgery is rarely the primary choice unless it is necessary to save the patient’s life from acute pressure.
Prognosis and Quality of Life
If a patient is in a terminal stage with a very poor general condition, we prioritize symptomatic treatment to ensure comfort. However, for many, removing a brain metastasis is the key to maintaining the Karnofsky Performance Status (KPS), allowing them to continue their systemic cancer treatments (chemotherapy/immunotherapy).

Image: Contrast-enhanced brain MRI showing multiple, well-circumscribed metastatic brain tumors in both hemispheres, appearing as bright lesions with surrounding edema.
Brain Tumors in Children
After leukemia, brain tumors are the most common tumors in children, accounting for approximately 20% of all childhood cancers.
The most frequently encountered tumor types in the pediatric population include:
- Gliomas: Especially astrocytomas of the optic nerve, brainstem, and cerebellum.
- Medulloblastomas: And other embryonal tumors (formerly classified as PNET).
- Pineal Region Tumors.
- Craniopharyngiomas.
- Choroid Plexus Papillomas.
- Teratomas.
A key distinction in pediatric neuro-oncology is that tumors of the cerebellum (posterior fossa) are much more common in children than in adults, occurring in 42–74% of cases, depending on the child’s age. Due to the critical nature of these locations, early diagnosis and specialized microsurgical techniques are essential for a favorable long-term outcome. In contrast to the pediatric population, cerebellar tumors in adults are considered metastatic until proven otherwise.
Request a Neurosurgery Second Opinion for Brain Tumors — Standard 24-Hour Review or Priority Option (Usually Within 3 Hours)
A diagnosis of a brain tumor often raises complex and unsettling questions — about tumor type, operability, prognosis,
and whether the proposed treatment strategy is truly optimal. This is especially true when opinions differ,
surgery is described as “high risk,” or molecular and pathological findings are difficult to interpret.
An independent neurosurgical second opinion helps place imaging (MRI/CT), pathology, and molecular markers
into a clear clinical context. We review whether the diagnosis and treatment plan follow modern neuro-oncology principles,
and explain what options realistically exist — including surgery, radiation, chemotherapy, active surveillance,
or combined (hybrid) approaches.
- ✔ Send a short message describing the brain tumor diagnosis and your main questions
- ✔ You will receive a reply within 24 hours confirming if and how we can help — including consultation cost and timing
- ✔ In urgent or time-sensitive cases (rapid deterioration, upcoming surgery, unclear operability), a priority consultation can usually be arranged within a few hours. If needed, write PRIORITY in your initial message.
- ✔ After the initial reply, you may send relevant documentation (MRI/CT images, pathology reports, molecular findings)
- ✔ During the video consultation, we explain the findings in clear language and answer all practical questions
Consultation fees typically range from $180–250, depending on case complexity.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This fee range is consistent with international specialist telehealth second opinions in neurosurgery.
Families and patients often seek a second opinion to clarify diagnosis, confirm treatment strategy,
or better understand risks, benefits, and realistic outcomes.
Frequently Asked Questions About Brain Tumors
What is a brain tumor?
A brain tumor is an abnormal growth of cells inside the skull. Some tumors arise from brain tissue or surrounding structures (primary tumors),
while others spread to the brain from cancers elsewhere in the body (secondary tumors, also called brain metastases).
What is the difference between a primary brain tumor and a brain metastasis?
Primary brain tumors start inside the brain or its coverings (for example, gliomas or meningiomas). Brain metastases are tumors that originate in another organ
(such as lung, breast, melanoma, kidney) and then spread to the brain through the bloodstream. In adults, metastases are very common and must always be considered.
Are most brain tumors cancer?
No. Many intracranial tumors are benign (non-cancerous), such as most meningiomas, pituitary adenomas, and schwannomas.
However, some tumors are malignant (cancerous) and may infiltrate brain tissue (for example, many diffuse gliomas).
Even benign tumors can be dangerous if they compress critical brain structures or cause swelling.
What are the most common brain tumor types in adults?
In everyday clinical practice, the most common adult intracranial tumor groups include meningiomas, gliomas (including glioblastoma),
pituitary adenomas, schwannomas (vestibular schwannomas/acoustic neuromas), and brain metastases.
The exact frequency varies between registries and depends on whether benign tumors are included in the statistics.
What symptoms can a brain tumor cause?
Symptoms depend on tumor size, location, swelling (edema), and whether there is bleeding or hydrocephalus.
Common symptoms include headaches, seizures, progressive weakness or numbness, speech or vision problems, balance issues,
personality or cognitive changes, and cranial nerve symptoms (hearing loss, double vision, facial numbness).
Some slow-growing tumors may cause very subtle symptoms for months or years.
Does a normal neurological exam rule out a brain tumor?
No. A patient can have a normal neurological exam and still have a tumor, especially if the lesion is small, slow-growing,
or located in a region that does not produce early focal deficits. If symptoms are concerning (new seizures, progressive deficits,
unexplained cognitive changes), imaging is still needed.
What is the best test to diagnose a brain tumor?
MRI of the brain is the gold standard. It shows tumor anatomy, edema, mass effect, and contrast enhancement patterns.
CT is useful in emergencies (for example, acute bleeding, hydrocephalus, severe mass effect) but MRI provides the most complete evaluation.
What does “contrast enhancement” mean on MRI?
Contrast enhancement means that a region becomes brighter after gadolinium contrast is given.
It often reflects abnormal blood-brain barrier and tumor vascularity. Enhancement can suggest higher-grade tumor activity,
but it is not a perfect marker of malignancy—some aggressive tumors may enhance minimally, and some benign tumors may enhance strongly.
What is brain edema and why does it matter?
Brain edema is swelling around a tumor caused by fluid leakage into surrounding tissue.
It increases intracranial pressure and can worsen symptoms quickly (headache, drowsiness, neurological deficits).
Steroids such as dexamethasone are often used to reduce tumor-related edema and stabilize the patient before definitive treatment.
What does “midline shift” mean on CT or MRI?
Midline shift means the tumor and swelling have pushed the brain away from its normal central position.
Larger shift suggests higher intracranial pressure and higher risk of herniation, and it often indicates the need for urgent neurosurgical assessment.
When is surgery necessary for a brain tumor?
Surgery is considered when a tumor causes significant mass effect, progressive neurological deficits, seizures that are difficult to control,
uncertain diagnosis requiring tissue confirmation, or when maximal safe removal is expected to improve survival or quality of life.
In some situations (small stable tumors, high surgical risk, or tumors in critical locations), active surveillance or biopsy may be recommended instead.
Is complete removal always possible?
Not always. Many tumors (especially diffuse gliomas) infiltrate normal brain tissue and have no clear boundary,
which makes total removal impossible without causing major neurological injury. In these cases, the goal is “maximum safe resection”
or decompression, followed by guideline-based adjuvant therapy.
In contrast, many benign tumors or metastases may have clearer margins and can often be removed completely.
What is a stereotactic biopsy and when is it used?
A stereotactic biopsy is a minimally invasive procedure that obtains a small tissue sample using a precise navigation system.
It is used when the tumor is deep, located in a high-risk area, or when removal would be too dangerous.
The goal is to obtain a diagnosis so that radiation, chemotherapy, or other targeted treatments can be planned.
What is the role of modern technologies like neuronavigation, 5-ALA, and awake craniotomy?
Neuronavigation helps the surgeon reach deep lesions accurately using MRI/CT-based guidance. 5-ALA fluorescence can highlight tumor tissue
under the microscope in selected gliomas, improving the extent of resection. Awake craniotomy is used for tumors near speech or motor areas,
allowing real-time functional testing to maximize safe tumor removal while protecting critical function.
How is the final tumor diagnosis confirmed?
The definitive diagnosis comes from tissue analysis after biopsy or surgery. Modern pathology integrates classic histology with immunohistochemistry (IHC)
and molecular/genetic markers (for example, IDH mutation, 1p/19q co-deletion, MGMT promoter methylation). This “integrated diagnosis” strongly influences
prognosis and treatment decisions.
What is MGMT methylation and why is it important in glioblastoma?
MGMT is a DNA-repair gene. If the MGMT promoter is methylated (“silenced”), tumor cells are less able to repair chemotherapy-induced DNA damage.
In practice, MGMT promoter methylation is associated with a better response to temozolomide (Temodar) and improved outcomes in many patients.
When are radiation therapy and chemotherapy used?
Radiation and/or chemotherapy are used when microscopic tumor cells may remain after surgery, when tumors are malignant,
or when surgery is not possible. For many aggressive gliomas, combined radiochemotherapy (radiation with temozolomide)
is a standard approach. For selected benign remnants, stereotactic radiosurgery (Gamma Knife/LINAC) may control growth without open surgery.
Can brain metastases be treated surgically?
Yes. Many brain metastases are well-circumscribed and can often be removed completely, especially if one lesion is dominant or causing mass effect.
A common modern strategy is a “hybrid approach”: removing the largest symptomatic metastasis and treating smaller/deeper lesions with stereotactic radiosurgery.
The decision depends on systemic cancer control, expected survival, and functional status (KPS).
Is it safe to use alternative or “natural” treatments instead of standard therapy?
Complementary approaches may help with well-being, but they must not delay evidence-based treatment.
Some supplements can interfere with chemotherapy, radiation, seizure medications, or blood clot prevention.
Any alternative therapy should be discussed with the neuro-oncology team to avoid harmful interactions and lost time.
When should families seek an urgent neurosurgical second opinion?
Consider an urgent second opinion when: the diagnosis is unclear; imaging shows significant edema or midline shift;
neurological status is worsening; surgery is labeled “too risky” without clear explanation; there are conflicting recommendations;
or the family needs a structured plan (what is urgent now, what can wait, and which treatment options exist).
Can we get a telehealth neurosurgery second opinion for brain tumors, including priority review?
Yes. Families can request a telehealth neurosurgery second opinion for brain tumors.
Priority review is available in urgent cases.
Learn more about our neurosurgery second opinion
.
Patient-Friendly Resources on Brain Tumors (Trusted Institutions)
The links below are written for patients and families in clear, non-technical language. I manually re-checked the URLs while preparing this list.
- National Cancer Institute (NCI) — Brain Tumors (Patient Version) — reliable overview + links to tumor types and treatments.
- NCI PDQ — Adult Central Nervous System Tumors Treatment — more detailed (still patient-facing) treatment pathways.
- Mayo Clinic — Brain tumor (Symptoms & Causes) — practical symptom explanations and “what it means.”
- Mayo Clinic — Brain tumor (Diagnosis & Treatment) — MRI/biopsy basics and major treatment options.
- NHS — Brain tumours (overview) — plain-language overview + when to seek help.
- Cancer Research UK — Brain tumour symptoms — symptom patterns and “raised intracranial pressure” explained.
- Macmillan Cancer Support — Signs & symptoms of a brain tumour — patient support + symptom guidance and next steps.
- American Brain Tumor Association (ABTA) — Educational Resources — excellent patient education + caregiver materials.
- The Brain Tumour Charity — Symptoms by tumor location — easy “where in the brain → what symptoms” explanation.
Scientific Resource: MAS Scoring System (Malignant Astrocytomas)
For readers who want a more technical (research) reference, here is the original publication of the Malignant Astrocytoma Score (MAS): PubMed: A new scoring system for malignant astrocytomas (MAS) .