Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Neurosurgeon and Pain Management Specialist
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
June 05, 2026
Who This Page Is For
This page is intended for patients and family members who have been told that MRI shows a
syrinx within the spinal cord, often in association with
Chiari malformation, prior spinal injury, or unclear cerebrospinal fluid flow disturbance.
It explains when syringomyelia requires only observation, when it may cause progressive neurological symptoms,
and how doctors decide whether surgical treatment is reasonable or unlikely to help.
If MRI findings and symptoms do not clearly match, opinions differ, or surgery has been proposed with uncertainty,
an experienced
neurosurgical second opinion
can help clarify the situation and define realistic expectations.
When patients and families usually seek a second opinion
- MRI shows a syrinx within the spinal cord, but it is unclear whether it is clinically relevant or incidental
- Neurological symptoms progress while MRI findings appear stable, or vice versa
- Syringomyelia is associated with Chiari malformation, but opinions differ on whether surgery is necessary
- Surgery has been proposed despite mild or slowly progressive symptoms
- Different specialists provide conflicting explanations or recommendations
- It is unclear whether symptoms are caused by the syrinx itself, altered CSF flow, or another spinal condition
- Patients and families are unsure whether observation, further testing, or surgical intervention could realistically help
In these situations, an experienced neurosurgical review can help determine whether syringomyelia is likely stable or progressive, clarify the role of Chiari malformation or other causes, and define realistic expectations before any invasive intervention: Request a Neurosurgical Second Opinion
Syringomyelia — Quick Summary (Read This First)
- Syringomyelia means that a fluid-filled cavity, called a syrinx, has formed inside the spinal cord. It most often develops due to disturbed cerebrospinal fluid (CSF) circulation rather than a primary disease of the spinal cord itself.
- The presence of a syrinx on MRI does not automatically mean treatment is required. Many syrinxes remain stable for years and do not cause progressive neurological damage.
- Chiari malformation type I is the most common associated condition in adults. Altered CSF flow at the cranio-cervical junction plays a central role in syrinx formation and progression.
- Symptoms depend more on syrinx location and functional impact than on size. Small syrinxes may be symptomatic, while larger cavities can remain clinically silent.
- Only a minority of adult patients require surgery. Approximately 20–30% eventually need operative treatment, usually directed at correcting the underlying CSF flow disturbance. The majority of syrinxes are treated surgically by addressing the underlying Chiari malformation rather than operating on the syrinx itself.
- Direct shunting of the syrinx is rarely the first option. It is reserved for selected cases when correction of the underlying cause is not feasible or has failed.
- The main goal of treatment is to prevent neurological progression. Symptom improvement may be partial and gradual, especially in long-standing cases.
- This page is structured so you can focus only on what matters to you. Use the Contents box to jump to sections on causes, MRI interpretation, treatment decisions, or when a neurosurgical second opinion may be helpful.
Most readers benefit from the Quick Summary plus the sections on Chiari Malformation, MRI Interpretation, and When Syringomyelia Requires Treatment. Other sections provide additional clinical context.
Contents
- Who This Page Is For
- When patients seek second opinion
- Syringomyelia quick summary
- What is syringomyelia
- How syringomyelia develops
- Common causes
- Chiari type I
- Location and segments
- Symptoms
- MRI appearance
- Treatment vs observation
- Surgical treatment why-opinions-differ
- Why Specialist Opinion Differ
- Syringomyelia and Chiari
- Monitoring and follow-up
- When second opinion helps
- Request a second opinion
- FAQs
- Additional information
What is syringomyelia and What Is a Syrinx in the Spinal Cord?
Syringomyelia refers to the presence of an abnormal, fluid-filled cavity (syrinx) within the spinal cord. This cavity is filled with cerebrospinal fluid (CSF) and can slowly expand over time.
Unlike tumors or infections, a syrinx does not destroy tissue directly. Instead, symptoms arise because the expanding cavity causes mechanical compression, disrupting the function of the spinal cord and its neural pathways. In its early stages, the damage caused by a syrinx is functional and potentially reversible. However, if the compression persists over time, it can lead to permanent organic damage and irreversible neurological deficits.
Importantly, the presence of a syrinx alone does not automatically mean that treatment is required.
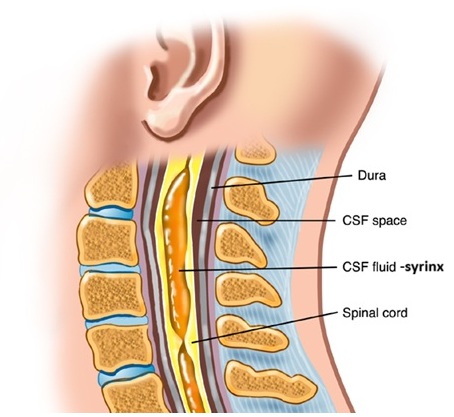
Image: A syrinx filled with cerebrospinal fluid (CSF) within the cervical spinal cord.
How and why syringomyelia develops
The most widely accepted explanation is that syringomyelia develops due to disturbed CSF circulation around the spinal cord.
When the normal pulsatile flow of cerebrospinal fluid is partially blocked or altered, pressure differences can force fluid into the spinal cord tissue, gradually forming a cavity. Over time, this cavity may enlarge or remain stable, depending on the underlying cause.
This explains why syringomyelia is often associated with structural abnormalities that disturb CSF circulation rather than primary spinal cord disease.
Common causes of syringomyelia
Chiari malformation type I
The most frequent cause in adults. Downward displacement of the cerebellar tonsils interferes with CSF flow at the cranio-cervical junction. In some patients, associated craniocervical junction abnormalities — such as basilar impression — may further exacerbate CSF flow obstruction.

Image: Due to the descent of the tonsils into the spinal canal, the flow of cerebrospinal fluid is disrupted. As a result, a collection of fluid forms inside the spinal cord (syrinx). As this syrinx grows, it can compress the spinal cord from the inside out.
Post-traumatic syringomyelia
May develop months or years after spinal cord injury due to scarring and altered CSF dynamics.
Spinal cord tumors
Both intramedullary and, less often, extramedullary tumors can obstruct CSF flow and lead to syrinx formation. Because some spinal cord tumors may be subtle or poorly visible on non-contrast MRI, at least one contrast-enhanced MRI study of the spinal cord is essential during the diagnostic evaluation of syringomyelia, in order to reliably exclude neoplastic causes. In intramedullary spinal cord tumors, the syrinx most commonly involves the central canal or the adjacent spinal cord tissue, and despite not always being confined to the central canal, it is still classified as syringomyelia.
Arachnoid adhesions and inflammation
Scarring after infection, surgery, or hemorrhage may disrupt CSF circulation.
Idiopathic syringomyelia
In some patients, no clear cause is identified despite detailed imaging.
Location, size, and number of involved spinal segments
Syringomyelia most commonly affects the cervical spinal cord, but its location, length, and extent vary significantly between patients.
- Cervical syringomyelia is the most frequent form, present in approximately 60–70% of adult cases, often associated with Chiari malformation type I.
- Cervicothoracic syringomyelia accounts for about 20–30% of cases and may extend over multiple vertebral levels.
- Isolated thoracic syringomyelia is less common, occurring in approximately 5–10% of patients, often related to trauma, tumors, or arachnoid pathology.
- Holocord syringomyelia, extending through most of the spinal cord, is rare and typically associated with long-standing cerebrospinal fluid flow obstruction.
Size and length of the syrinx
The absolute diameter of the syrinx does not reliably predict symptom severity.
Small syrinxes may be symptomatic if strategically located, while larger cavities may remain clinically silent.
In terms of length:
- many syrinxes span 3–5 vertebral segments,
- others may extend over more than 10 segments, especially in long-standing or post-traumatic cases.
Clinical relevance depends more on progression over time than on size at a single MRI examination.
Number of syrinx cavities
In most patients, syringomyelia presents as a single continuous cavity.
However:
- multiple syrinx cavities or segmental syringomyelia can occur, particularly in post-traumatic cases or in the presence of arachnoid adhesions,
- these cavities may be separated by segments of apparently normal spinal cord.
The presence of more than one syrinx does not automatically indicate a more severe condition, but it does require careful imaging review and follow-up.
Symptoms of syringomyelia
Symptoms depend more on functional impact than on the absolute size of the syrinx.
Common symptoms include:
- chronic or neuropathic pain, often described as burning, stabbing, or electric, which may involve the neck, shoulders, arms, trunk, or legs depending on syrinx location
- Cape-like loss of pain and temperature sensation, affecting the neck, shoulders, upper back, and proximal upper limbs, typically seen with cervical syrinx involvement.
- neuropathic pain or burning sensations in the arms or legs, depending on syrinx level
- muscle weakness or stiffness, most often affecting the hands and arms in cervical syringomyelia
- hand clumsiness or gait instability
- sensory asymmetry between the left and right side of the body
- in advanced cases, bladder or bowel dysfunction
Some patients remain completely asymptomatic for years, even with a visible syrinx.
Important clinical note
Not all neurological symptoms in patients with syringomyelia are necessarily caused by the syrinx itself.
Coexisting spinal, neurological, or peripheral nerve disorders are common and must be carefully evaluated to avoid attributing symptoms to syringomyelia when another condition is the primary cause.
Conditions that may produce similar or overlapping symptoms include:
- Chiari malformation
- degenerative cervical or lumbar spine disease (disc herniation, spinal canal stenosis, foraminal stenosis)
- cervical or lumbar radiculopathy
- peripheral nerve entrapment syndromes (e.g., carpal tunnel syndrome, ulnar neuropathy)
- spinal cord compression from other causes (degenerative, inflammatory, or neoplastic)
- central neuropathic conditions unrelated to syrinx progression
- musculoskeletal and myofascial disorders affecting posture, gait, or limb function
- other neurological diseases that may coexist and influence symptoms
For this reason, clinical decision-making should be based on integrated assessment of symptoms, neurological examination, and imaging findings, rather than on the presence of a syrinx alone.
What syringomyelia looks like on MRI — Syrinx MRI Findings
MRI is the key diagnostic tool. A syrinx appears as a fluid-filled cavity within the spinal cord, usually visible on T2-weighted images. The spinal cord normally contains a central canal, a narrow CSF-filled channel that is a remnant of normal embryological development. A central canal diameter up to 1–2 mm is usually regarded as a benign persistent central canal, whereas cavities exceeding 2–3 mm are more likely to represent true syringomyelia, especially when symptomatic or progressive. While many syrinx cavities involve the central canal, extracanalicular (paracentral) intramedullary syrinxes can also occur. These are most commonly seen after spinal cord trauma, spinal cord infarction, or myelomalacia, and may also develop in association with intramedullary pathologies such as spinal cord tumors.
When syringomyelia is present without an obvious Chiari malformation on standard MRI, further evaluation of cerebrospinal fluid dynamics may be helpful. Cine (phase-contrast) MRI can assess CSF flow at the craniocervical junction and may reveal functional obstruction not apparent on conventional imaging.
However, MRI interpretation requires experience:
- a long but narrow syrinx may be clinically insignificant,
- a small syrinx may cause symptoms if strategically located,
- stability over time is often more important than size at one moment.
For this reason, MRI findings should always be interpreted together with symptoms and neurological examination.

Image: MRI of the cervical spine. The arrow points to a syrinx within the spinal cord.
When syringomyelia requires treatment
Not all cases require active treatment. In adults, only a minority of patients with syringomyelia—approximately 20–30%—ultimately require surgical intervention, while the majority can be managed conservatively with careful clinical and imaging follow-up.
Observation with periodic MRI is usually appropriate when:
- symptoms are absent or mild,
- neurological status is stable,
- the syrinx does not enlarge over time.
Treatment should be considered when:
- neurological symptoms are progressive,
- imaging shows syrinx enlargement,
- an identifiable and treatable cause is present.
The key question is not “Is there a syrinx?” but rather “Is it causing ongoing neurological damage?” For many patients, understanding why surgery is not recommended is just as important as understanding when it is.
Surgical treatment of syringomyelia
Surgery is not aimed at draining the syrinx itself, but at correcting the underlying cause of disturbed CSF flow.
Examples include:
- posterior fossa decompression in Chiari malformation,
- removal of obstructing tumors,
- release of arachnoid adhesions in selected cases.
Direct shunting of the syrinx is rarely the first option and is reserved for specific situations. In contemporary adult series, syrinx shunting is performed in approximately 5–10% of surgically treated cases, typically when correction of the underlying cerebrospinal fluid flow disturbance is not feasible or has failed. When indicated, this approach involves controlled opening of the syrinx cavity, with fenestration of internal septations in wide or multiloculated syrinxes when necessary, followed by placement of a syrinx shunt. The most commonly used option is a syringosubarachnoid shunt, which diverts fluid from the syrinx into the surrounding subarachnoid space and restores communication with normal cerebrospinal fluid pathways. Syringopleural or syringoperitoneal shunts are generally reserved for cases in which the subarachnoid space is obliterated by scarring or adhesions, or when a syringosubarachnoid shunt has failed, with the specific configuration tailored to individual anatomy and pathology.
Realistic expectations are essential: surgery primarily aims to halt disease progression and restore cerebrospinal fluid flow rather than guarantee full neurological recovery. In adults with Chiari malformation–associated syringomyelia, long-term stabilization is achieved in approximately 85–95% of cases.
Follow-up MRI demonstrates significant reduction or collapse of the syrinx in 70–85% of patients, which often correlates with gradual clinical improvement. Complete radiological resolution, however, is not required for meaningful symptomatic benefit.
Clinical improvement is observed in approximately 60–80% of patients, while recovery of sensory or motor function depends largely on the extent and duration of pre-existing spinal cord damage rather than on complete disappearance of the syrinx itself.
Why Do Medical Opinions Differ in Syringomyelia?
Differences in medical opinion are common because decisions depend on how symptoms, MRI findings, and CSF flow disturbance are interpreted together, and not on a single parameter.
Is the syrinx truly causing the symptoms?
Some specialists attribute symptoms directly to the syrinx, while others consider it incidental unless there is clear clinical and anatomical correlation, especially when other spinal or neurological conditions may better explain the findings.
When is surgery actually necessary?
There is no strict threshold, as some recommend surgery based on MRI or presence of a syrinx, while others reserve it only for progressive neurological deficit, syrinx enlargement, or clear evidence of ongoing spinal cord damage.
Should treatment target the syrinx or the underlying cause?
Some approaches focus on draining the syrinx, but most specialists prioritize treating the underlying CSF flow disturbance, with direct shunting used only in selected cases.
Can Chiari malformation be present without requiring surgery?
Some recommend decompression based on imaging, while others consider surgery only when there is clear symptom progression or clinically significant CSF flow obstruction, even if Chiari is present.
Should the condition be monitored or treated early?
Many syrinxes remain stable, so some recommend observation, while others consider earlier treatment when there is concern about future progression or unclear symptom correlation.
Syringomyelia and Chiari malformation
Chiari malformation and syringomyelia frequently coexist, but they are not the same condition.
Key points:
- not every patient with Chiari develops a syrinx,
- not every syrinx in Chiari requires surgery,
- the decision to operate depends on symptoms, progression, and CSF flow disturbance.
This is one of the most common scenarios where second opinions differ — and where careful individualized assessment matters.
Living with syringomyelia and long-term monitoring
Many patients live for years with a stable syrinx and minimal symptoms.
Follow-up usually includes:
- periodic neurological examinations,
- repeat MRI at appropriate intervals,
- attention to new or changing symptoms.
Most adult patients show a stable syrinx on long-term follow-up, while spontaneous resolution is uncommon.
There is no evidence that normal daily activities worsen syringomyelia in stable cases. While most everyday activities are safe in stable cases, certain types of physical strain may worsen symptoms in some patients. Activities that involve repeated straining, heavy lifting, or breath-holding can temporarily increase pressure around the spinal cord. Contact sports and activities with a high risk of falls or spinal impact may also pose a risk, especially when the syrinx is large or when neurological symptoms such as weakness, numbness, or pain are already present.
When a second opinion is useful
Since numerous factors influence the decision of whether or not to operate on syringomyelia, the neurosurgeon’s experience in this field is vital. However, differences of opinion are common even among highly experienced specialists.
A second opinion can be especially helpful if:
- surgery has been recommended but symptoms are mild,
- it remains unclear whether the symptoms are caused by syringomyelia or by other coexisting conditions,
- MRI findings and clinical symptoms do not clearly match,
- different specialists have offered conflicting advice,
- you want to understand long-term risks and alternatives.
Careful review of imaging and clinical history often clarifies whether intervention is truly necessary.
Request a Neurosurgical Second Opinion — Syringomyelia and Chiari-Related Conditions.
24-Hour Review or Priority Option (Usually Within 3 Hours)
Patients diagnosed with syringomyelia are often told that MRI shows a spinal cord cavity,
a Chiari malformation, post-traumatic changes, or scarring affecting cerebrospinal fluid flow.
The most important question is usually not whether a syrinx exists, but
whether it is causing ongoing neurological damage and whether any form of surgical treatment is likely to help.
An independent neurosurgical second opinion can help clarify how MRI findings, symptoms,
and disease progression fit together — and whether observation, further testing,
or surgical intervention is reasonable, unnecessary, or unlikely to be beneficial.
- ✔ Send a brief message describing your symptoms (pain, sensory changes, weakness, gait issues) and what the MRI report states
- ✔ You will receive a reply within 24 hours explaining whether and how a second opinion may help in your specific case
- ✔ Time-sensitive situations: if neurological symptoms are progressing, surgery has been proposed with uncertainty, or opinions differ — write PRIORITY in your first message
- ✔ Spine and brain MRI (DICOM images) and available medical documentation can be reviewed once initial contact is established
- ✔ During the consultation, we discuss whether syringomyelia is likely stable or progressive, the role of Chiari malformation or other causes, and realistic expectations regarding observation, decompression surgery, or — in selected cases — syrinx shunting, with up to 10 days of follow-up for brief questions
Consultation fees typically range from $180–250, depending on case complexity.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
This is within the usual range for international specialist telehealth second opinions in neurosurgery.
Frequently Asked Questions About Syringomyelia
What is syringomyelia?
Syringomyelia means that a fluid-filled cavity, called a syrinx, has formed inside the spinal cord. The cavity is usually filled with cerebrospinal fluid (CSF). A syrinx does not behave like a tumor or infection; it usually causes symptoms by gradually expanding and compressing spinal cord pathways from the inside. In many adults, syringomyelia develops because normal CSF circulation around the spinal cord is disturbed. The most important question is not only whether a syrinx is visible on MRI, but whether it is stable, progressive, and truly responsible for the patient’s symptoms.
What is a syrinx in the spinal cord?
A syrinx is a fluid-filled cavity within the spinal cord. It may be located in the cervical, thoracic, or cervicothoracic spinal cord, and it may be short, long, narrow, or wide. Some syrinx cavities remain unchanged for years and never cause progressive neurological damage. Others may enlarge slowly if the underlying CSF flow disturbance continues. A syrinx becomes clinically important when it matches the patient’s symptoms, causes neurological signs, enlarges over time, or is associated with an underlying condition such as Chiari malformation, spinal trauma, arachnoid adhesions, or a spinal cord tumor.
Does the presence of a syrinx always require treatment?
No. The presence of a syrinx on MRI does not automatically mean that treatment or surgery is required. Many syrinxes remain stable for years, especially when symptoms are absent, mild, or not clearly related to the MRI finding. Observation with neurological follow-up and repeat MRI is often appropriate when the syrinx is not enlarging and neurological function is stable. Treatment is considered when symptoms are progressive, MRI shows enlargement, or there is an identifiable cause that can be corrected. The key clinical question is whether the syrinx is causing ongoing spinal cord damage, not simply whether it exists.
What is the difference between a persistent central canal and syringomyelia?
The spinal cord normally contains a very narrow central canal, which is a remnant of normal development. On MRI, a persistent or prominent central canal may appear as a thin CSF-like line within the cord. A canal measuring about 1–2 mm is often considered a benign persistent central canal, especially if symptoms are absent and the finding is stable. True syringomyelia is more likely when the cavity is wider, enlarges over time, extends through multiple segments, or correlates with neurological symptoms. The distinction depends on MRI appearance, size, progression, symptoms, and clinical examination.
What does syringomyelia look like on MRI?
On MRI, syringomyelia appears as a fluid-filled cavity inside the spinal cord, usually best seen on T2-weighted images. The syrinx often has the same signal as cerebrospinal fluid. MRI helps define the level, length, width, and shape of the cavity, and whether it involves the cervical, thoracic, or cervicothoracic spinal cord. It also helps identify possible causes, such as Chiari malformation, prior trauma, arachnoid adhesions, spinal cord tumor, or myelomalacia. MRI interpretation should not focus only on size; stability over time and correlation with symptoms are often more important than a single measurement.
What do syringomyelia MRI findings mean?
MRI findings in syringomyelia must be interpreted in clinical context. A report may describe a syrinx, hydromyelia, syringohydromyelia, persistent central canal, cervical syrinx, thoracic syrinx, or long-segment syrinx. These terms do not all carry the same clinical meaning. A narrow stable cavity may be insignificant, while a smaller syrinx can be important if it affects a sensitive part of the spinal cord or is enlarging. MRI should also look for the cause of altered CSF flow. In unexplained cases, contrast-enhanced MRI and sometimes cine MRI may be helpful to exclude tumor or assess CSF dynamics.
What symptoms are most typical of syringomyelia?
Symptoms of syringomyelia depend on the level and functional impact of the syrinx. Typical symptoms may include burning, stabbing, or electric pain; loss of pain and temperature sensation; numbness; weakness; stiffness; hand clumsiness; gait instability; or sensory differences between the two sides of the body. Cervical syringomyelia often affects the neck, shoulders, arms, and hands. Thoracic syringomyelia may affect the trunk or legs. In advanced cases, bladder or bowel symptoms may occur. However, not every symptom in a patient with a syrinx is caused by the syrinx, because degenerative spine disease, radiculopathy, neuropathy, and musculoskeletal disorders may coexist.
What is cape-like loss of pain and temperature in syringomyelia?
Cape-like loss of pain and temperature is a classic sensory pattern associated with cervical syringomyelia. It usually affects the neck, shoulders, upper back, and upper arms, similar to the distribution of a cape. This happens because a syrinx can disrupt crossing pain and temperature fibers inside the spinal cord. Patients may notice reduced ability to feel heat, cold, or painful stimuli in these areas, while other sensations may be relatively preserved. This pattern is clinically useful, but it is not present in every patient. Symptoms still need to be correlated with MRI level, neurological examination, and other possible causes of sensory disturbance.
Can a cervical syrinx cause arm or hand symptoms?
Yes. A cervical syrinx can affect spinal cord pathways related to the arms and hands. Symptoms may include hand weakness, clumsiness, numbness, burning pain, altered temperature sensation, stiffness, or difficulty with fine movements. Some patients notice that one hand becomes weaker or less coordinated. However, arm and hand symptoms can also come from cervical disc disease, foraminal stenosis, radiculopathy, carpal tunnel syndrome, ulnar neuropathy, or other peripheral nerve problems. This is why the MRI finding must be interpreted together with neurological examination and symptom distribution. A cervical syrinx is important only if it plausibly explains the clinical picture.
Can a thoracic syrinx cause symptoms?
Yes. A thoracic syrinx can cause symptoms when it affects spinal cord pathways at the thoracic level. Possible symptoms include trunk sensory changes, band-like pain, neuropathic pain, stiffness, leg weakness, gait imbalance, or, in more advanced cases, bladder or bowel dysfunction. Isolated thoracic syringomyelia is less common than cervical syringomyelia and may be related to trauma, arachnoid adhesions, tumors, or other causes of CSF flow disturbance. Because thoracic symptoms can overlap with degenerative spine disease, peripheral neuropathy, or musculoskeletal pain, careful clinical correlation is essential before attributing symptoms to the syrinx.
Why do symptoms not always match the size of the syrinx?
Symptoms do not always match syrinx size because location, pressure effect, progression, and affected spinal cord pathways are more important than diameter alone. A small syrinx may cause symptoms if it affects critical sensory or motor pathways. A long but narrow syrinx may remain clinically silent if it is stable and does not disrupt important function. Some symptoms may also come from another condition, such as cervical stenosis, radiculopathy, peripheral nerve entrapment, neuropathy, or musculoskeletal pain. This is why treatment decisions should not be based only on the MRI measurement. Clinical examination, symptom pattern, and MRI follow-up are essential.
What size syrinx requires surgery?
There is no single syrinx size that automatically requires surgery. Surgery is not decided by a size chart alone. A small syrinx may require attention if it is enlarging or causing progressive neurological symptoms, while a larger syrinx may be observed if it is stable and clinically silent. Doctors consider the cause of the syrinx, whether symptoms are worsening, whether neurological deficits are present, whether MRI shows enlargement, and whether a treatable CSF flow obstruction exists. The real question is whether the syrinx is causing ongoing spinal cord injury and whether surgery can realistically stop progression with acceptable risk.
Is a syrinx serious or dangerous?
A syrinx can be serious, but many syrinxes are stable and do not cause progressive neurological damage. The seriousness depends on symptoms, progression, location, size change over time, and the underlying cause. A stable incidental syrinx or persistent central canal may require only observation. A syrinx that enlarges, causes weakness, sensory loss, gait problems, or bladder symptoms is more concerning. Syringomyelia is most important when it reflects disturbed CSF flow from Chiari malformation, trauma, tumor, arachnoid adhesions, or another treatable cause. The diagnosis should therefore be interpreted individually rather than assumed to be harmless or dangerous in every case.
What does syringomyelia life expectancy depend on?
Life expectancy in syringomyelia depends on the cause, severity, progression, neurological deficits, and whether treatment is needed and effective. Many adults with a stable syrinx live for years with minimal or no symptoms and do not require surgery. The main concern is not the diagnosis itself, but progressive spinal cord dysfunction. Syringomyelia related to Chiari malformation may stabilize after appropriate decompression when surgery is truly indicated. Post-traumatic, tumor-related, or arachnoid adhesion-related syringomyelia may be more complex. Prognosis is best when progression is recognized early, the cause is correctly identified, and expectations are realistic.
Can a syrinx kill you?
Most syrinxes do not directly threaten life, especially when they are small, stable, and not causing progressive neurological deficits. The main risk of syringomyelia is usually long-term neurological deterioration rather than sudden death. However, certain causes or associated conditions may be more serious, such as Chiari malformation with significant brainstem compression, spinal cord tumor, severe trauma-related scarring, or progressive neurological decline. A patient should seek urgent medical evaluation if there is rapidly worsening weakness, walking difficulty, bladder or bowel dysfunction, new severe neurological symptoms, or signs suggesting spinal cord compression. The seriousness depends on the full clinical and MRI picture.
What causes a syrinx to form?
A syrinx usually forms because normal cerebrospinal fluid circulation around the spinal cord is disturbed. Pressure differences may force fluid into the spinal cord tissue, gradually creating a cavity. In adults, the most common associated condition is Chiari malformation type I, where the cerebellar tonsils disturb CSF flow at the craniocervical junction. Other causes include spinal cord injury, arachnoid adhesions, inflammation, prior surgery, hemorrhage, or spinal cord tumors. In some patients, no clear cause is found despite detailed imaging, and the syringomyelia is described as idiopathic. Identifying the cause is crucial because treatment usually targets the underlying CSF flow problem.
How are Chiari malformation and syringomyelia related?
Chiari malformation type I is the most common associated condition in adults with syringomyelia. In Chiari malformation, the cerebellar tonsils descend toward or below the foramen magnum and may disturb cerebrospinal fluid flow at the craniocervical junction. This altered CSF circulation can contribute to syrinx formation and progression. However, not every patient with Chiari malformation develops a syrinx, and not every syrinx in a patient with Chiari requires surgery. The decision depends on symptoms, neurological progression, syrinx behavior on MRI, and evidence of clinically significant CSF flow obstruction.
Can syringomyelia be monitored instead of treated surgically?
Yes. Many adults with syringomyelia are monitored rather than treated surgically. Observation is usually appropriate when symptoms are absent or mild, neurological status is stable, and MRI does not show enlargement. Monitoring often includes neurological examinations and repeat MRI at intervals chosen according to the cause, size, location, and symptoms. Monitoring is not passive neglect; it is an active strategy used when surgery is unlikely to improve the situation or when procedural risk outweighs expected benefit. Treatment is reconsidered if symptoms progress, neurological deficits appear, or imaging shows syrinx enlargement or a treatable underlying cause.
How often does syringomyelia require surgery?
Only a minority of adults with syringomyelia ultimately require surgery. Many cases remain stable and are managed with observation and MRI follow-up. Surgery is considered when there is progressive neurological deficit, syrinx enlargement, or a clear underlying cause that can be corrected. In adult practice, the main goal is usually to treat the cause of disturbed CSF flow rather than simply drain the syrinx. For Chiari-related syringomyelia, this often means posterior fossa decompression when symptoms, progression, and imaging support surgery. Direct syrinx shunting is reserved for selected cases and is not usually the first option.
What is the goal of surgery for syringomyelia?
The main goal of surgery for syringomyelia is to stop progression by correcting the underlying cause of disturbed cerebrospinal fluid flow. Surgery is not primarily performed to “empty” the syrinx in every case. For Chiari malformation, treatment may involve posterior fossa decompression to restore CSF flow at the craniocervical junction. For tumors, surgery targets the obstructing lesion. For arachnoid adhesions, selected cases may require restoration of CSF pathways. Improvement may be gradual and incomplete, especially if symptoms have been present for a long time. Stabilization and prevention of further neurological decline are often the most realistic goals.
When is direct shunting of the syrinx considered?
Direct shunting of the syrinx is rarely the first treatment option. It is usually reserved for selected cases when the underlying cause of CSF flow disturbance cannot be corrected, when previous surgery has failed, or when scarring and adhesions prevent normal communication with the subarachnoid space. A syringosubarachnoid shunt diverts fluid from the syrinx into the surrounding subarachnoid space. Syringopleural or syringoperitoneal shunts may be considered when the subarachnoid space is not usable. Shunting can be useful in selected patients, but it carries risks such as blockage, infection, neurological injury, or recurrence, so indications must be strict.
Can syringomyelia improve without surgery?
Syringomyelia can remain stable without surgery, and in uncommon cases a syrinx may partially decrease or resolve spontaneously. However, spontaneous resolution is not the usual expectation in adults. Many patients do well with observation when the syrinx is stable and neurological function is not worsening. Improvement without surgery is more likely when symptoms are not caused by the syrinx or when the finding represents a benign persistent central canal. The important point is careful monitoring. If symptoms progress or MRI shows enlargement, the treatment plan may need to change. Stability over time is often more important than a single MRI result.
How often should MRI follow-up be performed?
MRI follow-up intervals depend on symptoms, syrinx size, location, cause, and whether the finding is stable. A newly discovered syrinx often requires comparison imaging to determine whether it is changing. Stable incidental syrinxes may be monitored less frequently, while symptomatic, enlarging, Chiari-related, post-traumatic, tumor-related, or arachnoid adhesion-related syringomyelia may require closer follow-up. MRI should usually be interpreted together with neurological examination because symptoms and imaging do not always change at the same pace. If new weakness, sensory loss, gait problems, or bladder symptoms develop, earlier reassessment is usually appropriate rather than waiting for a routine interval.
What is the recovery process after syrinx or Chiari-related surgery?
Recovery depends on the underlying cause, the type of surgery, the duration of symptoms, and the degree of pre-existing spinal cord injury. In Chiari-related syringomyelia, posterior fossa decompression aims to restore CSF flow and stop progression. MRI reduction of the syrinx may occur gradually over months, and complete disappearance is not always necessary for meaningful improvement. Pain and sensory symptoms may improve slowly or partially, while long-standing weakness, numbness, or spinal cord damage may not fully recover. After surgery, follow-up includes neurological assessment and repeat MRI to confirm that the syrinx is stable or decreasing and that CSF flow has improved.
What activities should patients with a stable syrinx avoid?
There is no universal activity ban for every patient with a stable syrinx. Many patients can continue ordinary daily activity, walking, light exercise, and normal work if neurological status is stable. However, some patients may notice symptom worsening with repeated straining, heavy lifting, breath-holding, or activities that increase pressure around the spinal cord. Contact sports or activities with a high risk of falls or spinal impact may be discouraged, especially if the syrinx is large or symptoms such as weakness, numbness, pain, or gait problems are present. Activity advice should be individualized according to symptoms, MRI findings, and neurological examination.
Why do doctors sometimes disagree about syringomyelia treatment?
Doctors may disagree because syringomyelia treatment depends on how symptoms, MRI findings, progression, and CSF flow disturbance are interpreted together. One specialist may consider the syrinx responsible for symptoms, while another may suspect that symptoms are caused by cervical stenosis, radiculopathy, neuropathy, or another condition. Some doctors recommend surgery when Chiari malformation and a syrinx are present, while others reserve surgery for progressive neurological deficit or clear CSF flow obstruction. Differences also occur over whether the syrinx itself should be shunted or whether treatment should focus on the underlying cause. Careful individualized review often clarifies the decision.
When is a neurosurgical second opinion useful for syringomyelia?
A neurosurgical second opinion is useful when MRI shows a syrinx but it is unclear whether it is clinically relevant, when symptoms and MRI findings do not match, when surgery has been recommended despite mild or stable symptoms, or when different specialists give different explanations. It is also helpful when Chiari malformation, prior spinal trauma, arachnoid adhesions, or spinal cord tumor are part of the differential diagnosis. The goal is to determine whether the syrinx is stable or progressive, whether another condition better explains the symptoms, and whether observation, further testing, decompression surgery, or selected shunting is realistic and medically justified.
Additional Information for Patients
For those who wish to explore syringomyelia and its causes further, we have selected four highly reliable, patient-oriented resources from leading medical institutions:
-
National Institute of Neurological Disorders and Stroke (NINDS)
A comprehensive fact sheet covering symptoms, causes, and ongoing research.
Visit NINDS Syringomyelia Guide -
Mayo Clinic – Patient Information
A clear overview of diagnosis and treatment options from a world-leading medical center.
View Mayo Clinic Overview