Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 10, 2026
Who this page is for
This page is for patients with shoulder pain that persists beyond 6–12 weeks even after a proper initial treatment trial (rest, medication, physical therapy), and where imaging (X-ray/MRI/ultrasound) shows no clear structural cause or only mild-to-moderate degenerative changes that don’t fully match the symptoms.
If you’re in this situation and want a focused evaluation to identify the dominant pain source (rotator cuff/bursa, AC joint, long head of biceps, labrum, referred cervical pain, or myofascial trigger points), you can request an online consultation with our specialist.
When patients usually seek a second opinion for shoulder pain
- Your MRI shows a rotator cuff tear, but shoulder strength is relatively preserved
- Pain persists after steroid injections or physiotherapy
- You are being advised to undergo arthroscopic repair and want to understand the real benefit and risks
- You experience night pain, weakness, or radiating pain and the diagnosis remains unclear
A detailed symptom-based telehealth evaluation can help differentiate structural tears from tendon irritation, bursitis, or cervical spine referral — and clarify whether surgery is truly indicated.
Shoulder pain affects up to one in five adults at some point in their lives and is one of the most common musculoskeletal complaints seen in primary care.
It occurs slightly more often in women over 40 and in people with repetitive overhead activities, such as manual workers, athletes, and office employees who spend long hours at a computer.
Because the shoulder joint is the most mobile joint in the body, it depends on a complex system of muscles, tendons, and stabilizing structures. Pain may come from any of these local tissues — or be referred from the neck and upper thoracic region. Identifying the exact pain generator is therefore essential before planning treatment.
Common Causes of Shoulder Pain
Typical causes of shoulder pain include inflammation or irritation of:
- Long head of the biceps tendon — the most frequent source of anterior shoulder pain, responsible for 25–35% of chronic cases in outpatient settings.
Inflammation within the bicipital groove (tenosynovitis) often coexists with nearby bursal irritation and causes localized tenderness and pain during flexion or supination. - Subacromial / subdeltoid bursa (bursitis) — present in about 20–30% of patients. These bursae communicate with each other in most patients. It usually develops secondarily, as a reaction to mechanical overload or inflammation of the biceps or supraspinatus tendons.
It produces lateral shoulder pain and night pain, often relieved after ultrasound-guided corticosteroid injection. - Supraspinatus and rotator cuff tendinopathy — seen in roughly 15–25% of patients, frequently accompanying the biceps-bursa complex rather than existing alone.
In younger patients, shoulder pain usually results from an acute injury causing a partial or complete tear of the supraspinatus tendon. In older adults, pain is more often due to chronic tendon degeneration (tendinopathy or tendinitis), frequently accompanied by subacromial bursitis rather than a true tear. - Acromioclavicular (AC) joint degeneration or micro-instability — accounts for 10–15% of chronic shoulder pain, producing localized pain on top of the shoulder and discomfort on cross-arm adduction.
- Labral or capsular lesions — explain 5–10% of cases, mostly in younger or athletic individuals exposed to repetitive overhead activity.
Pain may also originate from the cervical spine or peripheral nerve irritation, which should always be considered when shoulder imaging appears inconclusive. For that reason, every case should be clinically evaluated to distinguish between true shoulder pathology and referred pain.
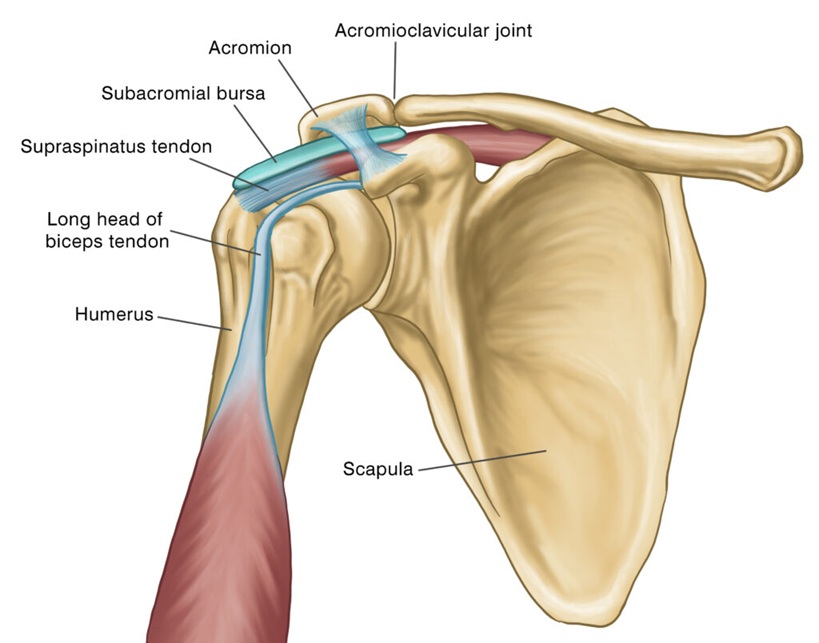
Image: Anatomical structures of shoulder which are the most usual cause of the shoulder pain.
The reported frequency of shoulder pain causes varies widely across studies — sometimes showing rotator cuff tendinopathy as the leading diagnosis, and in other reports highlighting biceps or bursal inflammation.
This variation reflects differences in study populations and clinical settings:
- Orthopedic surgical studies mostly include patients who failed conservative therapy or required surgery — therefore, they overrepresent rotator cuff tears and labral lesions.
- Primary care and pain-clinic studies include the full spectrum of patients — from mild overload and posture-related dysfunctions to chronic myofascial pain — where biceps tenosynovitis and subacromial bursitis are the most frequent findings.
- Imaging-based surveys (MRI or ultrasound screening) often report structural changes in asymptomatic individuals, which inflates the apparent prevalence of rotator cuff pathology.
Symptoms in Shoulder Pain
Symptoms depend on which structure around the shoulder is affected.
When the long head of the biceps tendon is inflamed, pain is usually felt at the front of the shoulder, sometimes radiating toward the upper arm. It worsens during lifting, carrying, or turning the palm upward (supination). Pressing on the bicipital groove often provokes sharp tenderness, and some patients report a sense of “clicking” in the front of the joint.
If the subacromial or subdeltoid bursa is inflamed (bursitis), pain typically appears on the outer side of the shoulder and increases when the arm is raised or during the night while lying on the affected side. It may feel like a dull ache spreading toward the deltoid region. Relief after a corticosteroid injection or rest is common.
In supraspinatus or rotator cuff tendinopathy, pain occurs with overhead activities, such as reaching for an object or dressing. Younger patients may recall a sudden injury, while older adults usually experience a gradual onset of aching and weakness. Movements like lifting the arm to the side or above the head become painful or limited.
When the acromioclavicular (AC) joint is affected, pain is most prominent on top of the shoulder, especially during cross-arm motion or when lying directly on that area. Swelling or tenderness at the AC joint may also be present.
Labral or capsular injuries cause deep, sharp pain inside the shoulder, sometimes accompanied by catching or clicking inside the joint, or a sense of instability, particularly in athletes or those performing repetitive overhead movements.
Finally, referred pain from the neck or peripheral nerves may mimic shoulder pathology. Such pain is often associated with neck stiffness, tingling, or radiating discomfort into the arm, while shoulder movements themselves remain relatively preserved.
Diagnostic Evaluation — Why Imaging Alone Is Not Enough
The first step in diagnosis is to identify which specific structure is responsible for the pain.
A common mistake is to rely too heavily on X-ray or MRI findings. In many patients, X-rays appear completely normal — or show degenerative changes that are unrelated to the actual pain source.
A correct diagnosis relies on:
• a detailed physical examination with specific shoulder function tests,
• ultrasound evaluation of soft tissues, tendons, and surrounding nerves and vessels,
• and, when necessary, small diagnostic injections that confirm the true pain generator.
Ultrasound is particularly valuable because it allows real-time visualization of tendon motion, inflammation, and local vascular changes — making it both a diagnostic and interventional tool.
Treatment of Shoulder Pain
Most shoulder pain can be effectively treated without surgery.
Management typically progresses through several stages:
• Medication and local therapy — short courses of anti-inflammatory drugs, combined with targeted local injections into or around the painful structure (usually long-acting corticosteroid suspensions that release gradually over 2-3 weeks and reduce inflammation).
• Physiotherapy — once pain is controlled, guided exercises help restore motion and strengthen the rotator cuff and scapular muscles.
• Ultrasound-guided interventions — such as lavage of calcium deposits or hydrodistension for frozen shoulder, often provide rapid relief and help avoid surgery.
• Arthroscopic and surgical procedures — indicated when pain persists despite full conservative care, including: arthroscopic decompression, tendon repair, removal of calcium deposits, or capsular release. Shoulder replacement (arthroplasty) is rarely required except in advanced degenerative disease.
Online pain consultation for regional pain in detail
Schematic explanation of the video consultation for regional pain
Answers to questions about the process and success of video consultations for regional pain
There are several common reasons for poor therapeutic outcomes in the treatment of chronic pain, which are often seen in patients with regional pain.
Artificial intelligence can also support the process by analyzing complex pain syndromes in regional pain syndrome, but clinical expertise remains essential.
Why Shoulder Pain May Persist Despite Treatment
This is a common question among patients who have already tried medication, injections, or physiotherapy — but continue to experience pain.
In many cases, treatment does not fail because the methods themselves are ineffective, but because the true pain generator has not been precisely identified. Imaging findings may show structural changes such as tendon degeneration or partial tears, yet these do not always correspond to the actual source of pain.
Even when the primary cause is correctly treated, pain can persist if additional contributing factors — such as mechanical overload, poor shoulder mechanics, muscle imbalance, or systemic influences — are not recognized and addressed. These factors can maintain irritation and prevent full recovery despite otherwise appropriate therapy.
Treatment of Contributing Factors in Shoulder Pain
Effective treatment of shoulder pain always begins with identifying the primary pain generator — the specific structure responsible for symptoms (such as the long head of the biceps tendon, subacromial bursa, rotator cuff, or AC joint).
However, in many patients, pain persists not only because of the local problem, but because additional contributing factors are not recognized or adequately addressed. These factors rarely act as the sole cause of pain, but they can maintain irritation, delay recovery, and reduce the effectiveness of otherwise appropriate treatment.
For that reason, successful management of shoulder pain requires not only treating the primary structure, but also understanding the broader mechanical and systemic context.
What contributing factors may play a role in shoulder pain?
- Repetitive overhead activity and mechanical overload — Frequent reaching, lifting, sports, or prolonged work with the arms elevated can continuously irritate the same tendon or bursa. This is usually recognized through patient history and movement testing, and improved by correcting activity patterns and load.
- Posture and scapular mechanics — Forward shoulder position and poor coordination of scapular stabilizing muscles alter shoulder biomechanics and increase stress on the rotator cuff and biceps tendon. Clinical examination typically reveals these patterns, and targeted physiotherapy helps restore balance.
- Muscle imbalance and reduced shoulder stability — Weakness of the rotator cuff or scapular muscles leads to inefficient movement and overload of specific structures. Functional testing helps identify this, and guided exercises are a key part of recovery.
- Metabolic factors, pro-inflammatory diet and low-grade inflammation — Obesity, insulin resistance, and chronic inflammation can increase pain sensitivity and slow tissue healing. These factors are often identified through clinical context and basic laboratory testing.
- Nutritional deficiencies — Low levels of vitamin D, vitamin B12, or other micronutrients may impair recovery and contribute to persistent pain. When suspected, simple blood tests can confirm the diagnosis and guide correction.
- Sleep disturbances and night pain cycle — Shoulder pain often worsens at night, and poor sleep further increases pain sensitivity. Addressing sleep quality and nighttime positioning can be an important part of treatment.
- Central sensitization — In some patients, the nervous system becomes more sensitive over time, amplifying pain even when local tissue irritation is relatively mild. This is recognized clinically and requires a broader, multimodal treatment approach.
- Stress and reduced activity due to pain — Pain often leads to avoidance of movement, resulting in loss of strength and further instability of the shoulder. Gradual return to controlled movement is essential to break this cycle.
- Medications and previous treatments — Certain medications such as statins, long-term use of pain medications, corticosteroids, or medications that cause excessive sedation may contribute to muscle or tendon-related pain, reduce tissue quality, or alter pain perception. Previous treatments, including repeated injections or incomplete rehabilitation, may also maintain symptoms if the underlying mechanism was not fully addressed.
- Other medical conditions and comorbidities — Conditions such as autoimmune diseases, thyroid disorders, diabetes, or chronic inflammatory states may increase pain sensitivity, affect tendon and joint structures, and reduce the response to otherwise appropriate treatment.
- Vitamin-related factors — Both deficiencies and excesses of certain vitamins (particularly vitamin B6) may contribute to nerve-related symptoms, burning pain, or altered sensitivity around the shoulder.
- Tissue quality and degeneration — Age-related changes, reduced blood supply, or repeated micro-injuries may impair tendon healing and increase vulnerability to persistent pain, even when mechanical factors are partially corrected.
Why this matters in practice
In many cases, treatment fails because the primary pain generator is not correctly identified, and therapy is directed only at contributing factors such as posture correction, exercise, or dietary changes. Conversely, even when the main structural cause (for example, a tendon or bursa) is treated, failure to recognize and address contributing factors often leads to only partial or temporary improvement. The most effective approach is a carefully selected combination of treatment that addresses both the primary pain generator and the contributing mechanical, functional, and systemic factors. In contrast, an inadequate or incomplete combination — even when it includes individually effective methods — is a common reason for suboptimal or short-lasting results. This approach significantly increases the likelihood of long-term improvement and reduces the need for repeated injections or surgery.
In practice, many patients try to address these contributing factors on their own — for example by improving posture, starting exercise programs, following an anti-inflammatory diet, using supplements such as vitamin D, magnesium, or joint-support products like glucosamine and chondroitin, or applying methods such as kinesio taping.
While these approaches can be helpful in selected cases, they rarely lead to lasting improvement if the primary pain generator is not clearly identified and treated. On the other hand, even well-targeted medical treatment may fail if all contributing factors are not recognized and corrected.
Many patients reading this recognize that they have already tried one part of this approach — but not the complete strategy. This is one of the most common reasons why otherwise well-treated shoulder pain becomes chronic.
Prognosis and Long-Term Outlook for Shoulder Pain
The majority of patients with persistent shoulder pain experience significant or complete relief once the true pain source is identified and treated with a combination of targeted medication and image-guided therapy.
In many cases, surgery can be completely avoided.
Even in chronic conditions, maintaining pain control for six consecutive weeks strongly predicts long-term improvement and stable shoulder function.
Request Persistent Shoulder Pain Second Opinion — 24-Hour Review (Priority Option Available Within Hours)
Persistent shoulder pain despite physiotherapy, injections, medication, arthroscopy, or previous treatment
often raises important questions:
Is the pain really coming from the shoulder joint itself?
Do MRI, X-ray, or ultrasound findings truly explain the symptoms?
Is arthroscopic repair, decompression, capsular release, or another procedure actually the right next step?
Could the pain come from the biceps tendon, subacromial bursa, rotator cuff, AC joint, labrum, cervical spine, peripheral nerves, or myofascial trigger points?
An independent specialist second opinion may help clarify whether the dominant pain source is
inside the shoulder joint, around the shoulder joint, or referred from the neck,
whether the proposed procedure is medically justified,
and whether more targeted treatment — such as medication adjustment, correction of contributing mechanical and systemic factors,
ultrasound-guided evaluation, diagnostic injections, focused rehabilitation, or image-guided treatment — may be more appropriate before arthroscopy or surgery.
- ✔ Send a brief message describing your shoulder pain location, how long it has lasted, what movements make it worse, and which treatments have already been tried
- ✔ You will receive a reply within 24 hours explaining whether an online consultation is appropriate and which documentation is required
- ✔ Priority cases: severe persistent night pain, progressive weakness, pain after shoulder arthroscopy or injection, conflicting specialist recommendations, or uncertainty before proposed shoulder surgery — write PRIORITY in your first message
- ✔ MRI, X-ray, ultrasound reports, operative notes, injection history, physiotherapy summaries, and previous specialist opinions can be reviewed
- ✔ During consultation we analyze whether the dominant pain generator is inside the shoulder joint, around the shoulder joint, or referred from the cervical spine, and which specific structures are most likely responsible
- ✔ We explain which treatment direction best matches the suspected dominant pain generator — including medication adjustment, correction of contributing factors, targeted rehabilitation, or diagnostic injections when the responsible structure is uncertain. If arthroscopy, tendon repair, decompression, capsular release, or other surgery is being considered, we clarify whether the pain pattern supports that decision before discussing it with your local treating team — with up to 10 days of follow-up clarification.
Consultation fees typically range from $180–250 depending on case complexity and documentation volume.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Based on our medical report, reimbursement may be possible if your insurance plan allows it.
This corresponds to typical international specialist telehealth second-opinion services for complex pain and treatment-decision review.
FAQ About Persistent Shoulder Pain
Why can persistent shoulder pain come from around the joint rather than inside the shoulder joint?
Persistent shoulder pain does not always come from the joint surface, labrum, or arthritis inside the shoulder joint. The shoulder is the most mobile joint in the body and depends on a complex system of tendons, bursae, muscles, capsule, biceps tendon, AC joint, and stabilizing structures. Pain may come from the long head of the biceps tendon, subacromial or subdeltoid bursa, rotator cuff tendinopathy, AC joint irritation, or myofascial overload. These structures can produce strong pain even when X-ray or MRI shows only mild degenerative changes. This is why the exact pain location, movement triggers, night pain, tenderness, strength, and response to diagnostic injections are essential before deciding that surgery is needed.
What is the difference between intra-articular, periarticular and referred shoulder pain?
Intra-articular shoulder pain comes from inside the joint, such as the labrum, capsule, cartilage, or deeper joint structures. It may feel deep, sharp, unstable, or associated with clicking, catching, or a sense that the shoulder may give way. Periarticular shoulder pain comes from structures around the joint, such as the long head of the biceps tendon, subacromial bursa, rotator cuff tendons, AC joint, or surrounding muscles. It is often more localized and movement-related. Referred shoulder pain comes from outside the shoulder, especially the cervical spine, upper thoracic region, or peripheral nerves. In referred pain, shoulder movement may be relatively preserved, while neck stiffness, tingling, radiating arm pain, or neurological symptoms may be present.
Can shoulder MRI or X-ray show degenerative changes that are not the true cause of pain?
Yes. Shoulder X-ray or MRI can show degenerative changes, tendon degeneration, partial rotator cuff tears, AC joint arthritis, or labral changes that do not fully explain the patient’s symptoms. Imaging is important, but structural abnormalities are also common in people without severe pain. A rotator cuff tear on MRI does not automatically mean that the tear is the dominant pain generator, especially if strength is preserved or the pain pattern does not match the finding. X-rays may be normal or may show changes unrelated to the real pain source. Correct diagnosis requires matching imaging with physical examination, specific shoulder tests, ultrasound evaluation, pain location, movement triggers, and sometimes diagnostic injections that confirm which structure is actually painful.
How can a doctor identify the real pain generator in persistent shoulder pain?
The real pain generator in persistent shoulder pain is identified by combining symptom mapping, examination, imaging, movement testing, and anatomical reasoning. The doctor must determine whether the pain is anterior, lateral, superior, deep, radiating, or related to the neck. Pain in the front of the shoulder may suggest the long head of the biceps tendon; lateral pain and night pain may suggest subacromial bursitis or rotator cuff involvement; pain on top of the shoulder may suggest AC joint disease. Ultrasound is especially useful because it can show tendon movement, bursitis, fluid, local vascular changes, and guide precise injections. When several possible sources exist, small diagnostic injections can help confirm which structure is truly responsible.
Can shoulder pain come from the long head of the biceps tendon rather than the rotator cuff?
Yes. The long head of the biceps tendon is a frequent source of anterior shoulder pain and may be more clinically important than a mild rotator cuff finding on MRI. Biceps tendon inflammation or tenosynovitis often causes pain in the front of the shoulder, tenderness in the bicipital groove, discomfort during lifting or carrying, and pain when turning the palm upward. It may coexist with subacromial bursitis or supraspinatus irritation, which can make diagnosis more difficult. Patients may also describe clicking or sharp pain in the front of the joint. If treatment is directed only at a rotator cuff finding while the biceps tendon is the dominant pain generator, symptoms may persist. Ultrasound evaluation and targeted injections can help clarify this.
Can lateral shoulder pain come from the subacromial bursa or rotator cuff tendinopathy?
Yes. Pain on the outer side of the shoulder commonly comes from the subacromial or subdeltoid bursa, supraspinatus tendon, or broader rotator cuff tendinopathy. Bursitis often produces lateral shoulder pain, pain when raising the arm, and night pain, especially when lying on the affected side. Rotator cuff tendinopathy may cause pain with overhead activity, dressing, reaching, or lifting the arm to the side. In many patients, these problems occur together rather than as isolated diagnoses. The bursa can become inflamed secondarily because of tendon overload or poor shoulder mechanics. Treatment should therefore address the painful structure, but also the mechanical factors that keep irritating it, including scapular control, rotator cuff strength, posture, and repetitive overhead loading.
Can pain on top of the shoulder come from the AC joint rather than the rotator cuff?
Yes. Pain on top of the shoulder may come from the acromioclavicular joint rather than the rotator cuff. AC joint degeneration, micro-instability, or inflammation typically causes localized tenderness directly over the top of the shoulder. Pain often increases with cross-arm movement, reaching across the body, lying on that side, or loading the shoulder in certain positions. This pattern is different from classic rotator cuff or subacromial pain, which is usually more lateral and often worse with overhead activity. MRI or X-ray may show AC joint degeneration, but the finding must match the patient’s symptoms. A focused examination and, when necessary, a diagnostic AC joint injection can help confirm whether this joint is the dominant pain generator.
Can deep shoulder pain with clicking come from the labrum or capsule?
Yes. Deep shoulder pain with catching, clicking, sharp internal pain, or a feeling of instability may come from the labrum or capsule. Labral and capsular lesions are more common in younger or athletic patients, especially those exposed to repetitive overhead activity, throwing, lifting, or previous dislocation. These lesions can produce mechanical symptoms that feel different from superficial tendon or bursal pain. However, labral findings on MRI are not always the true cause of pain, especially if symptoms do not match. Some patients have coexisting biceps tendon irritation, rotator cuff overload, AC joint pain, cervical referral, or myofascial dysfunction. Before arthroscopy is considered, the clinical picture, mechanical symptoms, imaging, and response to targeted diagnostic injections should be interpreted together.
Can shoulder pain come from the neck or cervical nerves rather than the shoulder itself?
Yes. Pain felt in the shoulder may come from the cervical spine, upper thoracic region, or peripheral nerve irritation. This is especially important when shoulder imaging appears inconclusive, when shoulder movement is relatively preserved, or when symptoms include neck stiffness, tingling, numbness, burning, or radiating pain down the arm. Cervical radicular pain can mimic rotator cuff or shoulder joint disease, while peripheral nerve irritation may create pain, weakness, or sensory symptoms around the shoulder and arm. Treating the shoulder alone may fail if the dominant pain source is actually referred from the neck. A correct evaluation must compare shoulder function, neck movement, neurological signs, imaging findings, and the distribution of pain before deciding on injections, physiotherapy, or surgery.
Can shoulder pain cause a dull ache or throbbing pain in the entire arm?
Shoulder disorders can cause pain that spreads toward the upper arm, especially when the biceps tendon, rotator cuff, or subacromial bursa is irritated. Biceps tendon pain may radiate down the front of the upper arm, while subacromial bursitis or rotator cuff tendinopathy often produces a dull ache over the outer shoulder and deltoid region. However, pain that travels far down the arm, especially with tingling, numbness, burning, electric sensations, or neck stiffness, should raise suspicion for cervical nerve involvement or peripheral nerve irritation. The distinction matters because shoulder injections or arthroscopy will not solve pain that is primarily nerve-related. Careful examination of shoulder motion, neck movement, sensory symptoms, strength, and imaging helps separate local shoulder pain from referred neurological pain.
Why can shoulder pain persist despite physiotherapy, injections or medication?
Shoulder pain can persist despite physiotherapy, injections, or medication when the dominant pain generator has not been identified precisely. Treatment may focus on a rotator cuff finding while the main source is the biceps tendon, subacromial bursa, AC joint, labrum, cervical referral, peripheral nerve irritation, or myofascial trigger points. Even when the primary structure is treated correctly, pain may continue if contributing factors are not addressed. These include repetitive overhead activity, poor scapular mechanics, weak rotator cuff or scapular stabilizers, posture, mechanical overload, sleep disturbance, metabolic factors, nutritional deficiencies, chronic inflammation, or central sensitization. Medication and injections can reduce inflammation, but lasting improvement usually requires matching treatment to both the true pain source and the factors maintaining irritation.
Why can shoulder pain persist after arthroscopy or previous shoulder surgery?
Shoulder pain can persist after arthroscopy or previous surgery when the operation treated a visible structural problem but not the dominant pain generator. Arthroscopy may address a tendon tear, decompression, labral lesion, calcium deposit, or capsular stiffness, but pain may continue if the main source is biceps tendon irritation, subacromial bursitis, AC joint disease, cervical referral, peripheral nerve irritation, myofascial overload, or central sensitization. Pain can also persist if rehabilitation does not restore scapular control, rotator cuff strength, shoulder mechanics, and gradual load tolerance. True surgical complications must be excluded when symptoms are severe or worsening. If no clear complication explains the pain, the wider shoulder-neck pain generator and contributing factors should be reassessed before repeat procedures are considered.
Why is shoulder arthroscopy not always useful for chronic shoulder pain?
Shoulder arthroscopy is not always useful for chronic shoulder pain because not every MRI finding is the true source of symptoms. Arthroscopy may help when there is a clearly symptomatic structural lesion, such as a clinically relevant tendon tear, labral lesion, calcific deposit, mechanical impingement, or frozen shoulder requiring capsular release after conservative therapy has failed. However, it is less likely to help if pain mainly comes from biceps tenosynovitis, bursitis without a surgical lesion, poor scapular mechanics, cervical referral, peripheral nerve irritation, myofascial pain, systemic contributing factors, or central sensitization. Before surgery, the key question is whether the imaging finding matches the pain pattern, weakness, functional limitation, examination findings, and response to targeted treatment.
Does every rotator cuff tear on MRI require surgery?
No. Not every rotator cuff tear seen on MRI requires surgery. In younger patients, an acute traumatic tear with significant weakness may require more urgent orthopedic assessment. In older adults, many rotator cuff findings are degenerative and may coexist with bursitis, biceps tendon irritation, AC joint pain, or altered shoulder mechanics. Some partial tears and tendinopathic changes improve with medication, targeted injections, and structured rehabilitation. Surgery is considered when symptoms, weakness, functional limitation, examination findings, and imaging all point to a clinically important tear that has not improved with appropriate non-surgical care. If shoulder strength is relatively preserved or the pain pattern does not match the MRI, the tear may not be the dominant pain generator.
Can frozen shoulder cause persistent pain and stiffness even when imaging is not dramatic?
Yes. Frozen shoulder, or adhesive capsulitis, can cause persistent pain and marked stiffness even when X-ray or MRI does not show dramatic structural damage. The main problem is capsular inflammation and tightening, which limits shoulder motion and causes pain with daily activities, dressing, reaching, or sleeping. It may develop gradually and can be confused with rotator cuff disease or bursitis. Hydrodistension, targeted injections, pain control, and careful physiotherapy may help restore motion, but forcing exercises too aggressively during the painful phase can worsen symptoms. The diagnosis depends more on the pattern of restricted passive and active movement than on imaging alone. In resistant cases, capsular release may be considered, but only after careful confirmation of the pain generator.
Can central sensitization make shoulder pain persist even when structural damage is limited?
Yes. Central sensitization can make shoulder pain persist or feel disproportionate even when structural damage is limited. In this situation, the nervous system becomes more sensitive and amplifies pain signals from the shoulder, neck, muscles, tendons, or surrounding tissues. The pain is real, but the intensity may no longer reflect only the visible tissue change on MRI or ultrasound. Central sensitization is more likely when pain has lasted for months, sleep is poor, multiple treatments have failed, symptoms spread into the arm or neck, or ordinary movements become painful. Treatment must still identify and reduce the primary pain generator, but it also needs to address sleep, graded activity, medication strategy, mechanical overload, and contributing systemic factors.
Can metabolic or systemic factors make persistent shoulder pain harder to treat?
Yes. Metabolic and systemic factors can make persistent shoulder pain harder to treat, even when a local shoulder diagnosis is present. Obesity, insulin resistance, diabetes, thyroid disorders, autoimmune disease, chronic inflammatory states, poor sleep, and pro-inflammatory diet may increase pain sensitivity and slow tissue recovery. Low vitamin D or B12 may impair healing, while excessive vitamin B6 can contribute to nerve-related sensory symptoms in some patients. Certain medications, repeated corticosteroid injections, incomplete rehabilitation, deconditioning, and chronic pain cycles may also maintain symptoms. These factors rarely act as the only cause of shoulder pain, but they can reduce the effect of otherwise appropriate treatment. Durable improvement often requires addressing both the primary pain generator and the broader contributing context.
When are diagnostic injections useful in persistent shoulder pain?
Diagnostic injections are useful when persistent shoulder pain has several possible sources or when imaging findings do not clearly match the symptoms. A small amount of local anesthetic can be injected around a suspected pain generator, such as the biceps tendon sheath, subacromial bursa, AC joint, glenohumeral joint, or another targeted structure. If the patient’s typical pain improves temporarily, that structure is more likely to be clinically important. This can help distinguish biceps tendon pain from bursitis, rotator cuff-related pain, AC joint disease, intra-articular shoulder pain, or referred cervical pain. Diagnostic injections are not a full treatment plan by themselves, but they can prevent poorly targeted procedures and clarify whether rehabilitation, image-guided treatment, or surgery is reasonable.
Can an online video consultation help identify the source of persistent shoulder pain?
An online video consultation can help identify the likely source of persistent shoulder pain when the situation is non-emergent and the patient already has imaging, treatment history, or conflicting recommendations. MRI, X-ray, ultrasound, injection, physiotherapy, or surgical reports can be reviewed together with the exact pain location and symptom pattern. Video assessment can evaluate painful arm elevation, night pain, weakness, movement limitation, neck-related symptoms, scapular mechanics, and whether pain appears local shoulder-related or referred from the cervical spine. It cannot replace urgent in-person care or every physical test, but it can often clarify whether the dominant pain generator is tendon, bursa, AC joint, labrum, frozen shoulder, cervical referral, peripheral nerve irritation, or contributing factors.
Additional Patient Resources — Shoulder Pain
-
NHS — Shoulder Pain
Self-care advice, when to seek medical help, and red flag symptoms. -
AAOS OrthoInfo — Shoulder Pain & Common Shoulder Problems
Overview of common causes (rotator cuff, impingement, arthritis, instability). -
AAPM&R KnowledgeNow — Adhesive Capsulitis (Frozen Shoulder)
Definition, disease stages, and treatment options (hydrodilatation, exercises, injections). -
AAPM&R — Rotator Cuff & Shoulder Tendon Injuries
Information on tendon injuries, degeneration, and tears. -
AAOS OrthoInfo — Shoulder Impingement / Rotator Cuff Tendinitis
Symptoms, diagnosis, and non-surgical treatment options. -
RSNA RadiologyInfo — Musculoskeletal Ultrasound
What to expect from ultrasound imaging and guided procedures. -
RSNA RadiologyInfo — MRI of the Shoulder
The role of MRI in evaluating tendons, bursa, labrum, and joint structures. -
AAOS — Rotator Cuff & Shoulder Conditioning Program
Safe exercises to restore strength and flexibility after pain improves.