Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 12, 2026
Who is this page for?
This page is for patients whose neck or arm pain did not improve after several therapies, or who are unsure if surgery is really needed. The page explains how cervical disc herniation develops, what symptoms are truly caused by nerve or spinal cord compression, and when treatment or surgery may be needed. Reading it first will help you understand your MRI findings and treatment options before booking a consultation.
- Persistent neck pain or arm pain (radiculopathy) despite therapy — during a telehealth consultation, we help determine whether the disc is the true source of pain and discuss tailored conservative and surgical options.
- Surgery was already recommended? Request an online second opinion on anterior cervical discectomy and fusion (ACDF), disc arthroplasty, or decompression — with clear explanation of benefits, risks, and expected recovery.
When patients usually seek a second opinion for cervical disc herniation and radiculopathy
- Arm pain, numbness, tingling, or weakness persists despite medications or physical therapy
- Symptoms keep recurring after temporary improvement
- MRI shows a disc herniation, foraminal narrowing, or nerve root compression, but the picture feels unclear
- You are considering epidural injections, nerve root blocks, or surgery
If this reflects your situation, a focused telehealth review can clarify whether your symptoms truly match the imaging findings, what treatment options are reasonable, and what is — and is not — indicated in your case: Request Consultation
Cervical Disc Herniation & Radiculopathy — Quick Summary (Read This First)
- Cervical disc herniation occurs when disc material protrudes toward a cervical nerve root or the spinal cord. It may cause neck pain, arm pain, numbness, tingling, weakness, or, in more severe cases, signs of spinal cord compression.
- Cervical radiculopathy means irritation or compression of a cervical nerve root. Pain often radiates from the neck into the shoulder, arm, hand, or fingers, depending on the affected nerve root.
- MRI findings must match the symptoms before treatment decisions are made. A cervical disc herniation, bulging disc, or foraminal narrowing may be incidental if the pain pattern, neurological findings, and imaging level do not fit together. In that case, treatment for a herniated disc is not indicated, and especially not surgical intervention.
- Not every cervical disc herniation requires surgery. Many patients improve with structured conservative treatment, especially when inflammation around the nerve root is more important than fixed mechanical compression.
- Progressive weakness or spinal cord symptoms require urgent neurosurgical evaluation. Hand clumsiness, gait imbalance, leg stiffness, increasing weakness, or bladder symptoms may suggest cervical myelopathy or serious nerve compression.
- Soft cervical disc herniations and hard disc–osteophyte complexes behave differently. Soft fragments are more typical in younger adults and may shrink over time, while hard spondylotic discs are more common after age 50 and may cause more fixed narrowing.
- Neck and arm pain can mimic cervical disc radiculopathy. Shoulder disease, facet joint pain, thoracic outlet syndrome, brachial plexus irritation, myofascial trigger points, or peripheral nerve entrapments can produce similar symptoms.
- Conservative treatment is usually the first step when there is no progressive deficit. Medication, short-term activity modification, posture correction, physical therapy, cervical traction in selected cases, and sometimes selective injections may reduce pain and nerve irritation.
- Image-guided injections or nerve root blocks may help selected patients. They are most useful when symptoms suggest nerve-root inflammation and surgery is not clearly required, or when diagnosis needs confirmation before a major treatment decision.
- Surgery is considered when symptoms and imaging clearly match and conservative care fails. Common options include anterior cervical discectomy and fusion (ACDF), cervical disc arthroplasty, posterior foraminotomy, or decompression for spinal canal stenosis.
- A second opinion can clarify whether the disc is truly the pain source. This is especially important when surgery has been recommended, symptoms are mixed, or MRI findings do not fully explain neck and arm pain.
- This page explains cervical disc herniation, cervical radiculopathy, diagnosis, conservative treatment, surgery, recovery, and when telehealth second opinion may help.
Most readers benefit from reviewing the Quick Summary together with the sections on Symptoms of Cervical Disc Herniation, Diagnosis of Cervical Disc Herniation, Conservative Treatment, and When Do You Need Surgery?. Later sections provide deeper clinical detail for patients deciding between medication, injections, continued observation, or surgery for cervical disc herniation and radiculopathy.
Contents
- Who is this page for?
- What Is Disc Herniation?
- Types of Herniation
- Location of Herniation
- How Herniation Causes Symptoms
- Symptoms (Radiculopathy, Myelopathy)
- Diagnosis of Disc Herniation
- Detecting Neurological Deficits
- Diseases That Mimic Disc Pain
- Herniation vs Spondylosis/Stenosis
- Pain Contributing Factors
- Conservative (Non-Surgical) Treatment
- Why Neck Pain Persist Despite Treatment
- When Do You Need Surgery?
- Surgical Options Overview
- ACDF (Discectomy and Fusion)
- Posterior Foraminotomy
- Surgery for Myelopathy/Stenosis
- Potential Risks and Complications
- Chronic Pain After Surgery
- Role of Second Opinion/Online Consultation
- Prognosis and Recovery
- FAQs for Disc Herniation
- Additional Information
- Start Telehealth Consultation
What Is Cervical Disc Herniation?
The cervical spine consists of seven vertebrae (C1–C7) that support the neck, protect the spinal cord, and allow flexible motion of the head. Between each vertebra lies an intervertebral disc — a cushion-like structure that absorbs mechanical stress during movement and load-bearing.
Each disc has a soft central part, the nucleus pulposus, surrounded by a tough fibrous outer ring called the annulus fibrosus, which provides stability and limits excessive movement.
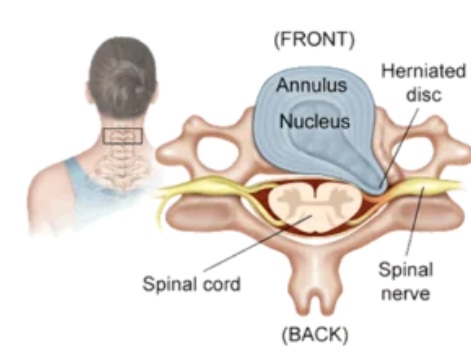
Image: A cervical vertebra showing an intervertebral disc with a herniation. The nucleus pulposus (the soft inner part) has penetrated the annulus fibrosus (the tough outer ring) and is compressing the nerve root.
When part of the nucleus pushes outward through a tear in the annulus, it is called a cervical disc herniation. If the herniated fragment compresses or irritates a nerve root, this results in cervical radiculopathy — pain, numbness, or weakness radiating from the neck into the shoulder, arm, or hand.
Unlike the lumbar region, where “soft” disc herniations are more frequent, cervical disc herniations often occur after age 50 and are typically associated with spondylotic (degenerative) changes, where bony ridges (osteophytes) accompany the disc protrusion.
This combined “disc–osteophyte complex” is sometimes referred to as a “hard disc”. This is in contrast to the “soft disc” cervical herniations, which are typically seen in younger adults (often between the ages of 40 and 50 and are slightly more common in women).
Cervical herniations tend to be more central or paramedian and can compress the spinal cord (cervical myelopathy) in addition to producing arm pain from nerve root irritation.

Image: Anatomy of the cervical spine showing seven vertebrae (C1–C7), eight nerve roots, and the intervertebral discs that act as flexible shock absorbers. Also presented is a disc herniation at level C6-C7 compressing a cervical nerve root C7.

Image: The posterior longitudinal ligament (PLL) covers the back of the vertebral bodies and discs inside the spinal canal. The image also displays different ways of spinal canal narrowing and compression of the spinal cord and nerve roots, such as disc herniation, spondylotic osteophytes, PLL thickening, PLL calcification, thickening of the ligamentum flavum (the ligament between the posterior arches of the cervical vertebrae), facet hypertrophy (the posterior joints between two vertebrae), and instability (spondylolisthesis between the cervical vertebrae).
Types of Cervical Disc Herniation
Bulging disc
A broad-based, circumferential extension of the disc beyond its normal margin.
The annulus and posterior longitudinal ligament (PLL) remain intact.
This degenerative finding is often accompanied by small anterior or marginal osteophytes, representing age-related remodeling rather than nerve compression.
It is common with aging and usually not a true herniation or cause of pain.
Disc protrusion
A focal displacement of nucleus material where the annulus is partially ruptured but the PLL remains intact.
This is the most frequent symptomatic type in the cervical spine and may cause neck and arm pain (radiculopathy) if it contacts a nerve root.
In patients typically over the age of 50, a protrusion often coexists with bony ridges (osteophytes) and thickening of the PLL, forming a “hard disc” or disc–osteophyte complex that can narrow the spinal canal more significantly.

Image: Cervical disc herniation accompanied by bone spurs (osteophytes). These spondylotic changes and the disc material work together to compress the nerve root (a condition often referred to as a „hard disc“).
Disc extrusion
The nucleus material extends through the annulus, and the PLL becomes thinned or displaced.
Disc extrusions are relatively less frequent in the cervical spine, and they occur most often in younger adults. They can sometimes resolve spontaneously without surgery as the extruded material is reabsorbed by the body.
Disc sequestration (free fragment)
A complete rupture of the PLL with separation of a disc fragment.
This is rare in the cervical spine due to the tight canal and limited space for fragment migration.
If present, it may mimic a tumor or epidural mass on imaging.
Several case reports have documented spontaneous resorption of cervical disc extrusions, although this phenomenon is less frequently observed than in lumbar herniations.
Clinical Relevance of the Types of Herniation
Not every cervical disc herniation causes pain. MRI studies have shown that many symptom-free individuals have protrusions or extrusions.

Image: Illustrations showing types of cervical disc herniation — bulging, protrusion, extrusion (contained and uncontained), and sequestration.
Location of Cervical Disc Herniation
Cervical disc herniations most often occur at C5–C6, C6–C7, and less frequently at C4–C5 levels. Other levels are less frequent and only level C1-C2 has no intervertebral disc.
Soft disc herniation (most common in those younger than 45) can be lateral, foraminal (compressing the nerve root), or central (compressing the spinal cord). In older patients — typically over 50 — the disc is no longer soft and gelatinous but rather fibrotic and calcified, often associated with osteophytes and spondylotic ridges. These spondylotic changes make the herniation more rigid and frequently central or paramedian, which increases the likelihood of spinal cord compression (cervical myelopathy) rather than isolated nerve root irritation.
Common locations and effects:
- Paracentral (paramedian) — the most common type in younger patients; compresses the nerve root and sometimes partially narrows the central canal.
- Foraminal or extraforaminal (lateral) — compresses the exiting nerve root within or just beyond the neural foramen, producing radicular pain and numbness along the arm.
- Central (dorsomedial) — more typical in older (>50) patients with spondylotic discs; can press on the spinal cord itself, leading to weakness or stiffness in both arms or even legs (cervical myelopathy).

Image: Typical locations of cervical disc herniation within the spinal canal — A-central (compressed spinal cord), B-paramedian (compressed nerve root and less spinal cord), and C-foraminal (compressed nerve root).
How a Cervical Disc Herniation Causes Symptoms
A herniated disc (paramedian or foraminal) can irritate a nerve root by mechanical compression, inflammatory reaction, or both. If inflammation predominates, pain may improve with conservative treatment alone. If mechanical pressure is stronger, symptoms can persist longer or require surgery.
Central cervical herniation may affect the spinal cord itself, leading to gait imbalance, hand clumsiness, or leg stiffness in addition to arm pain.
Symptoms of Cervical Disc Herniation (Neck Pain, Radiculopathy and Myelopathy)
The symptoms are commonly associated with cervical radiculopathy (nerve root compression/irritation) and, in severe cases, cervical myelopathy (spinal cord compression). However, it is important to note that the overall neck pain is often a result of multiple factors, including local causes (such as muscle spasm or joint pain) that frequently occur alongside radiculopathy.
Typical symptoms may include:
- Neck pain radiating into the shoulder or down one arm (mostly due to nerve root irritation or compression).
- Tingling, numbness, or burning sensations in the fingers or hand (a key sign of nerve root compression, known as cervical radiculopathy).
- Muscle weakness in the arm or hand (usually a sign of radiculopathy, but may also indicate spinal cord involvement).
- Pain worsening with neck movement or sustained posture (a common indicator of radiculopathy).
- In severe cases (myelopathy), patients may experience unsteady gait and leg weakness.
Pain distribution depends on the affected root:
- C5 Root: Shoulder pain and weakness of the deltoid muscle (shoulder weakness);
- C6 Root: Pain radiating to the thumb, accompanied by weakness in the biceps (affecting elbow bending) and wrist extensors;
- C7 Root: Pain radiating to the middle finger, along with triceps weakness (affecting elbow extension); and
- C8 Root: Pain along the inner forearm to the ring and little fingers, characterized by hand grip weakness.

Image: Dermatomal distribution of cervical nerve roots (C5–C8) showing typical areas of pain and sensory loss.
How Doctors Detect Neurological Deficits (Nerve and Spinal Cord Damage)
Deficits are primarily signs of radiculopathy and may include:
- Sensory changes: Numbness or tingling in a dermatomal pattern (C5–C8).
- Motor weakness: Decreased strength in muscles innervated by the affected root.
- Reflex loss: Biceps (C5–C6), brachioradialis (C6), triceps (C7).
When spinal cord compression (myelopathy) develops, additional, more serious signs will appear:
- Clumsy hands and difficulty fastening buttons.
- Gait imbalance or leg stiffness.
- Urinary urgency or retention (in advanced cases).
- Increased reflexes on the legs (patellar, Achilles reflex) + Babinski’s sign
These require urgent neurosurgical evaluation.
Diseases of the Neck That Mimic Cervical Disc Pain
Several conditions can cause pain similar to cervical radiculopathy. In that situation even when MRI shows a disc herniation it does not have to be the main problem. Examples include:
- Shoulder joint disease (rotator cuff tear, adhesive capsulitis)
- Peripheral nerve entrapment (carpal tunnel, ulnar neuropathy)
- Myofascial trigger points in neck or shoulder muscles
- Facet joint arthropathy
- Thoracic outlet syndrome
This overlap explains why some patients do not improve after surgery — the disc was not the true pain generator or it was not the only one.
Diagnosis of Cervical Disc Herniation
MRI of the cervical spine is the gold standard. It clearly shows the disc, spinal cord, and nerve roots.
CT scans may be used to assess bone spurs (osteophytes) and foraminal stenosis. Additionally, a cervical spine X-ray (taken in neutral and different neck positions) can help evaluate for vertebral instability.
Electromyography (EMG) and nerve conduction studies can confirm nerve involvement when symptoms and imaging do not clearly match.
However, finding a herniated disc on MRI does not always mean it is the source of pain. Many people have asymptomatic herniations. A neurosurgeon must always interpret imaging in the context of clinical findings. If MRI does not explain the type of pain in the neck and arm a specialist who is familiar with pain anatomy should examine the patient. This is an expert who knows all possible reasons for neck and arm pain and how to diagnose and treat them.

Image: MRI of the cervical spine, sagittal and axial views, arrow showing a C6–C7 disc herniation compressing the exiting C7 root.
Cervical Disc Herniation vs Cervical Spondylosis and Spinal Canal Stenosis
Spondylosis refers to age-related degeneration of vertebrae and discs, often producing spinal canal stenosis (narrowing). Cervical stenosis is more likely in older adults (>50) and develops gradually.
Symptoms often include neck stiffness, numbness in hands, loss of balance, or leg weakness (myelopathy), rather than isolated arm pain. Surgical treatment for stenosis focuses on decompression of the spinal cord, not just removing a single disc fragment. (usually surgeries like laminectomy, laminotomy, corpectomy).
Pain Contributing Factors That Should Also Be Diagnosed in Neck Pain and Cervical Spine Disorders
In patients with persistent neck pain, shoulder discomfort, or radiating arm pain (cervical radiculopathy), treatment should not focus only on the primary anatomical pain generator. It is also important to identify additional factors that can maintain pain, increase sensitivity, delay recovery, or reduce the effectiveness of otherwise appropriate treatment. Many patients with cervical disc herniation continue to have pain even when the disc itself is correctly treated.
- Posture, screen use and daily habits — prolonged sitting, forward head posture, frequent smartphone use (“text neck”), and working at a computer without proper ergonomics can continuously overload cervical structures and maintain irritation
- Muscle imbalance and cervical instability — weakness of deep neck flexors and overactivity of superficial muscles (trapezius, levator scapulae) may lead to poor stabilization and persistent pain
- Reduced physical activity and deconditioning — long-lasting pain often leads to reduced movement, loss of strength and endurance, and increased vulnerability to further irritation
- Metabolic factors, pro-inflammatory diet and low-grade inflammation — obesity, insulin resistance, and chronic inflammation may increase pain sensitivity and slow recovery
- Nutritional deficiencies — low levels of vitamin D, vitamin B12, magnesium, or iron may contribute to nerve dysfunction, muscle fatigue, and slower healing
- Vitamin-related factors — both deficiency and excess of vitamin B6 may contribute to burning sensations, tingling, or hypersensitivity in the neck, shoulder, or arms
- Sleep position and sleep disturbance — inadequate pillow support, poor sleep posture, and fragmented sleep may aggravate neck pain and reduce recovery capacity
- Stress and increased muscle tension — stress increases muscle tone in the neck and shoulder region and enhances nervous system reactivity, contributing to persistent symptoms
- Central sensitization — in long-standing pain, the nervous system may become more reactive, amplifying pain signals even when the original structural problem is less pronounced
- Medications and long-term drug effects — certain medications and treatment patterns may influence symptom persistence or pain perception. For example, statins may be associated with muscle pain in some patients; prolonged use of analgesics, especially opioids, may increase pain sensitivity; repeated corticosteroid use may affect tissue balance; and polypharmacy can alter symptom perception without addressing the underlying mechanism
- Other medical conditions and comorbidities — diabetes, thyroid disorders, autoimmune diseases, fibromyalgia, and chronic inflammatory conditions may increase pain sensitivity and reduce treatment response
These factors should be identified and treated, but they should not replace the central task: the primary anatomical source of pain (disc pathology, nerve root compression, facet joint pain, or muscular dysfunction) must still be correctly diagnosed and treated. In most patients, meaningful improvement requires addressing both.
Conservative (Non-Surgical) Treatment for Cervical Disc Herniation
Around 85–90% of patients recover without surgery.
Treatment options include:
- Medication: nonsteroidal anti-inflammatory drugs (NSAIDs), standard pain relievers, short-term corticosteroids, and muscle relaxants. When radicular pain is prominent, neuropathic pain medications (pregabalin, gabapentin) or low-dose antidepressants (amitriptyline, duloxetine) may also be used.
- Physical therapy: usually started after the first 5–7 days, when acute pain settles. Includes exercises to strengthen neck and shoulder muscles, improve posture, and reduce nerve irritation.
- Cervical traction may be used selectively.
- Cervical manipulations are not recommended, especially techniques that involve sudden or forceful neck movements.
- Lifestyle measures: ergonomics at work, avoiding prolonged neck flexion (smartphone/computer), posture correction, and good sleep posture. A short period (5–7 days) of cervical collar use can help during severe pain. The correction of head and neck alignment during sleep is also important in treatment.
- Interventional options: selective nerve root blocks or epidural steroid injections when radicular symptoms persist despite structured conservative therapy.
If symptoms improve within 6–8 weeks, surgery is not needed. Reasons for pain relief without surgery are many herniations move from the nerve root and shrink spontaneously or their prevalent type of irritation on the nerve was not compression but inflammation (together with herniation of part of the disk, there is excretion and accumulation of inflammatory products around the nerve).

Image: Irritation of the cervical nerve root during disc herniation caused by mechanical compression and chemical inflammation from proteins released from the disc.
Why Conservative Treatment of Neck Pain and Cervical Disc Herniation Often Fails — What Is Commonly Missed
In many patients, treatment does not fail because the condition is severe, but because the pain is not precisely analyzed at three critical levels.
First, the exact anatomical structure responsible for the pain is not clearly identified. Neck and arm pain are often attributed to MRI findings such as disc herniation or spondylosis, while the true source — facet joints, ligaments, muscles, fascia, or peripheral nerves — may remain unrecognized.
Second, even when the correct structure is suspected, the specific pathological process within that structure is not defined. Inflammation, mechanical irritation, instability, micro-injury, or nerve sensitization require different treatments, yet therapy is often applied without this distinction.
Third, contributing factors that maintain and reactivate pain are frequently overlooked. These include posture-related overload, repetitive strain, muscle imbalance, and reduced physical conditioning, but also chronic low-grade inflammation, metabolic factors (such as insulin resistance), nutritional deficiencies, and impaired tissue recovery.
Because these mechanisms remain active, pain may persist even when the primary condition appears to be treated correctly (after discectomy).
For this reason, when treatment does not lead to improvement, the key step is not repeating the same approach, but performing a structured reassessment — identifying the exact structure, the underlying process, and all contributing factors that sustain the pain.
When Do You Need Surgery for a Cervical Disc Herniation?
Most cervical disc herniations do not require surgery. Around 80–90% of patients improve with structured conservative treatment, especially when inflammation (rather than strong mechanical compression) is the main cause of pain.
Surgery is indicated only when:
- There is progressive muscle weakness or paralysis (due to radiculopathy and/or myelopathy).
- Pain remains disabling after 6–12 weeks of proper therapy
- MRI shows spinal cord compression (myelopathy)
Surgical Options for Cervical Disc Herniation
The goal is to remove the herniated material and relieve pressure on the nerve root or spinal cord.
Anterior Cervical Discectomy and Fusion (ACDF):
The most common and reliable procedure — the disc is removed through a small incision in the front of the neck, followed by placement of a bone graft or cage to fuse the vertebrae.
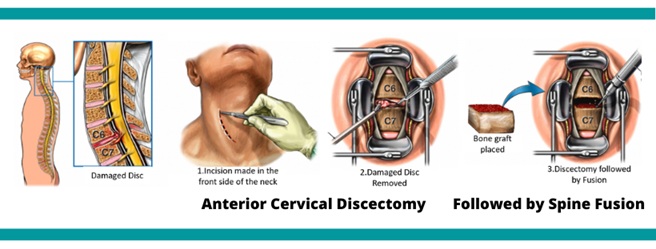
Image: Surgical illustration of anterior cervical discectomy and fusion (ACDF), showing removal of the disc and placement of an interbody cage or bone graft.

Image: Anterior spinal plate fixation after removal of cervical disc and its replacement with a cage.
Artificial Disc Replacement (Cervical Arthroplasty) After Removal of The Disc:
An alternative that preserves some motions at the operated level, suitable for selected patients without severe degeneration.
Posterior Foraminotomy
This surgical procedure is used for lateral disc herniations to decompress the nerve root from the back, without requiring spinal fusion. Today, this is typically performed as a microscopic or endoscopic discectomy.
Surgeries for multilevel spinal canal stenosis (compression of the spinal cord)
Typically employ one of two main approaches:
Posterior (Back) Approach: Involves the removal or repositioning of the posterior vertebral arches (laminectomy or laminoplasty) to create more space for the spinal cord.
Anterior (Front) Approach: Involves the removal of one or two vertebral bodies (corpectomy) and replacement with a prosthesis or bone graft.

Image: Cervical spine x-ray shows that artificial cervical disc replacement maintains some motions between vertebrae.
Start Your Telehealth Consultation for Cervical Disc Herniation & Radiculopathy
If neck and arm pain persist or you’re unsure what to do next — don’t wait. A telehealth consultation can clarify whether the cervical disc is the true pain source, review your MRI, and outline the best next steps.
✔ Send a short message describing your symptoms (neck/arm pain, numbness, weakness) and attach prior reports
✔ You’ll receive a reply within 24 hours confirming if we can help, consultation cost, and available time slots
✔ After confirmation, send your medical files securely (MRI/CT, EMG) by email or WhatsApp
✔ A written summary is provided when appropriate, and you may send free follow-up questions for 10 days.
✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
✔ You’ll receive a reply within 24 hours confirming if we can help, consultation cost, and available time slots
✔ After confirmation, send your medical files securely (MRI/CT, EMG) by email or WhatsApp
✔ A written summary is provided when appropriate, and you may send free follow-up questions for 10 days.
✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Typical consultation fee: 180 – 250 USD, depending on case complexity.
Many patients use telehealth second opinions to confirm or avoid surgery (ACDF, disc arthroplasty, decompression).
It’s safe, accepted, and effective.
Before contacting us, please read our Privacy Policy and Terms of Use.
Online pain consultation for neck pain and cervical radiculopathy in detail
Schematic explanation of the video consultation for neck pain and cervical radiculopathy
Answers to questions about the process and success of video consultations for neck pain and cervical radiculopathy
Possible Reasons Why Chronic Pain Treatment Fails
Potential Risks and Complications of Cervical Discectomy
Even with experienced surgeons, spine surgery carries risks:
- Infection, bleeding, or cerebrospinal fluid leak
- Nerve or spinal cord injury (rare)
- Persistent or recurrent pain if another pain generator exists
- Recurrence of herniation at the same or different level (≈10%)
- Adjacent segment disease — accelerated degeneration above or below the fusion level
Chronic Pain After Cervical Disc Surgery
Most patients experience rapid relief of arm pain after surgery.
However, about one in five may continue to have neck discomfort, often due to:
- Pre-existing facet joint or muscle pain
- Scar tissue around the nerve root
- Adjacent level degeneration
- Wrong pain generator targeted before surgery
Persistent or recurrent symptoms should be reassessed to identify the true cause.
A detailed telehealth or in-person review by a spine specialist helps determine if the pain is mechanical, neuropathic, or muscular in origin.
Persistent or recurrent pain after cervical discectomy can have more possible causes than mentioned above.
Several mechanisms described on the page about chronic pain after lumbar discectomy — including residual nerve irritation, epidural fibrosis, facet joint overload, and secondary muscular pain — may also occur in the cervical spine. Proper diagnostic reevaluation and targeted treatment can often improve symptoms.
Prognosis and Recovery After Treatment of Cervical Disc Herniation
With proper diagnosis and a personalized treatment plan, the majority of patients recover completely or nearly completely.
The natural course is generally favorable — most patients improve within 6 to 12 weeks of conservative management, although recovery may be slower in older adults with spondylotic (“hard-disc”) changes.
Studies show that:
- 75–90% of patients improve without surgery, particularly when pain results mainly from inflammation rather than severe mechanical compression.
- Pain reduction and functional recovery follow a gradual pattern — acute radicular pain typically subsides within several weeks, followed by improvement in strength and sensory symptoms.
- Spontaneous resorption of herniated or extruded disc material has been documented on follow-up MRI in both lumbar and cervical cases, especially when there is a soft, non-calcified fragment.
- Surgery provides faster pain relief and neurologic recovery when there is significant or persistent nerve root or spinal cord compression, but long-term outcomes (after 1–2 years) are comparable between surgical and conservative groups in most studies.
- Regarding neurological recovery, outcomes are generally better in cervical radiculopathy than in cervical myelopathy. Surgical series report motor recovery in about 85–95% of patients with cervical radiculopathy and preoperative weakness, while cervical myelopathy improves less predictably; one prospective study reported neurological improvement in 71% after decompression, with lower recovery of gait and sphincter function. Recovery depends strongly on the duration and severity of preoperative compression.
Earlier intervention is associated with better functional recovery, while chronic cord compression or long-standing motor weakness may lead to only partial improvement even after technically successful surgery.
After recovery, recurrence at the same or another level is possible but relatively uncommon (estimated 5–10% over several years). Maintaining neck mobility, posture correction, and strengthening of stabilizing muscles reduces the risk of relapse.
In summary, cervical disc herniation—particularly “soft disc” types—has an excellent prognosis with modern conservative care. Surgery remains reserved for patients with clear cord or root compression, progressive deficits, or persistent pain that limits daily life.
The Role of Second Opinion and Online Consultation
A second opinion can often prevent unnecessary surgery — or confirm that an operation is truly needed if you are uncertain. For cervical disc herniation and radiculopathy, where symptoms may overlap with muscle, joint, or peripheral nerve disorders, a specialist online consultation helps patients to:
- Clarify whether the disc seen on MRI is the true cause of symptoms
- Determine whether conservative treatment is still reasonable or if surgery should be considered
- Understand the risks, benefits, and expected results of surgical versus non-surgical options
- Plan long-term strategies for pain control, posture correction, and rehabilitation
Online second-opinion services are now widely used in the United States, Europe, and other developed regions. They are especially valuable for patients who already have imaging results but wish to discuss them with a neurosurgeon experienced in spinal disorders before deciding on surgery.
In international terminology, this service may also appear under different names — video consultation, virtual consultation, teleconsultation, telehealth consultation, telemedicine consultation, remote consultation, online doctor visit, virtual doctor appointment, online medical advice, doctor chat online, or online second opinion.
A telehealth consultation can help identify whether your pain truly originates from the cervical disc, which treatment options are most appropriate, and when — if ever — surgery should be performed.
FAQs for Cervical Disc Herniation & Radiculopathy
What is a cervical disc herniation and how does it cause arm pain?
Cervical disc herniation occurs when disc material in the neck moves beyond its normal boundary and irritates or compresses a cervical nerve root or, in more severe cases, the spinal cord. When a cervical nerve root is affected, pain can travel from the neck into the shoulder, arm, forearm, or hand. This is called cervical radiculopathy. The pain may be caused by direct mechanical pressure, local inflammation around the nerve root, or both. The exact arm pain pattern often depends on which cervical nerve root is involved, such as C6, C7, or C8.
What is the difference between a soft cervical disc herniation and a hard disc–osteophyte complex?
A soft cervical disc herniation usually refers to disc material that is softer, more recent, and less calcified. It is more common in younger adults and may irritate or compress a nerve root, causing cervical radiculopathy. A hard disc–osteophyte complex is different: the disc is usually more degenerated, fibrotic, or calcified and is often accompanied by bony spurs called osteophytes. This pattern is more common after age 50 and may narrow the spinal canal or neural foramen more rigidly. Hard-disc cervical disease is more likely to coexist with cervical spondylosis, foraminal stenosis, or spinal cord compression.
Which cervical disc levels are most commonly affected by cervical disc herniation?
Cervical disc herniation most often affects the C5–C6 and C6–C7 levels, followed by C4–C5. These levels carry significant motion and mechanical load, which makes them more vulnerable to disc degeneration, protrusion, and nerve root irritation. A C5–C6 disc herniation often affects the C6 nerve root, while a C6–C7 disc herniation often affects the C7 nerve root. Symptoms may include pain, numbness, tingling, or weakness in a pattern that follows the involved nerve. The level seen on MRI must always be compared with the patient’s symptoms and neurological examination.
What symptoms suggest cervical radiculopathy?
Cervical radiculopathy usually causes pain, numbness, tingling, burning, or weakness that travels from the neck into the shoulder, arm, forearm, or hand. The symptoms often follow a nerve-root pattern. C6 radiculopathy may radiate toward the thumb, C7 radiculopathy toward the middle finger, and C8 radiculopathy toward the ring and little fingers. Arm pain may worsen with neck movement, coughing, posture, or prolonged sitting. Weakness, reduced reflexes, or sensory loss can indicate more significant nerve root involvement. Cervical radiculopathy should not be diagnosed from MRI alone; symptoms, examination, and imaging must match.
What symptoms suggest spinal cord compression from cervical myelopathy?
Cervical myelopathy means that the spinal cord is compressed in the neck. Symptoms are usually more serious than isolated cervical radiculopathy. Warning signs include clumsy hands, difficulty buttoning clothes, dropping objects, unsteady walking, leg stiffness, balance problems, frequent falls, increased reflexes, Babinski sign, or urinary urgency in advanced cases. Arm pain may or may not be present. Cervical myelopathy requires prompt specialist evaluation because long-standing spinal cord compression can leave permanent neurological deficits. When MRI shows cervical spinal cord compression and symptoms suggest myelopathy, treatment decisions should not be delayed or based only on pain intensity.
Can neck and arm pain come from something other than cervical disc herniation?
Yes. Neck and arm pain can come from several conditions other than cervical disc herniation, even when MRI shows a disc abnormality. Shoulder disease, rotator cuff problems, carpal tunnel syndrome, ulnar neuropathy, thoracic outlet syndrome, facet joint pain, myofascial trigger points, and muscle spasm can all mimic cervical radiculopathy. Sometimes more than one pain generator is present at the same time. This is a common reason why patients do not improve after treatment that focuses only on the disc. A good evaluation must determine whether the cervical disc herniation truly matches the pain pattern, neurological signs, and imaging findings.
Can MRI show cervical disc herniation even when the disc is not the true pain source?
Yes. Cervical MRI can show disc bulging, protrusion, foraminal narrowing, or degenerative changes in people who do not have symptoms from that disc. This is why cervical disc herniation should not be treated based on MRI alone. The disc is more likely to be the true pain source when the MRI level matches the patient’s arm pain distribution, numbness, weakness, reflex changes, and neurological examination. If symptoms do not match the MRI, another cause may be responsible, such as shoulder disease, peripheral nerve entrapment, facet joint pain, muscle trigger points, or central pain sensitization.
Does every cervical disc herniation require surgery?
No. Most cervical disc herniations do not require surgery. Many patients improve with conservative treatment because nerve irritation can settle, inflammation can decrease, and some soft disc fragments may shrink over time. Surgery is usually considered when there is progressive weakness, clear spinal cord compression, disabling arm pain that persists despite proper treatment for 6–12 weeks, or worsening neurological signs. A cervical disc herniation seen on MRI is not enough by itself to justify surgery. The decision depends on symptoms, examination, MRI findings, severity of compression, duration of symptoms, and whether the clinical picture truly matches the disc level.
What is the difference between cervical disc bulging, protrusion, extrusion, and sequestration?
Cervical disc bulging is a broad extension of the disc beyond its normal margin and is often age-related. Cervical disc protrusion is more focal and may contact or compress a nerve root. Cervical disc extrusion means that disc material has pushed farther through the outer disc layer, often forming a larger fragment. Cervical disc sequestration means that a free disc fragment has separated from the main disc. These terms describe shape and anatomy, but they do not automatically determine symptoms. A small protrusion in the wrong place can cause severe radiculopathy, while a larger bulge may be painless if it does not compress a nerve or spinal cord.
Can a cervical disc herniation shrink or heal without surgery?
Yes. A cervical disc herniation can sometimes shrink or become less symptomatic without surgery, especially when it is a soft, non-calcified disc fragment and the main problem is inflammation rather than fixed mechanical compression. Symptoms often improve over 6–12 weeks with medication, physical therapy, posture correction, activity modification, and time. Extruded disc material may be gradually resorbed by the body in selected cases. However, healing is less predictable when the disc is calcified, associated with osteophytes, or causing significant spinal cord compression. Progressive weakness, myelopathy, or severe persistent pain requires specialist reassessment rather than waiting indefinitely.
What conservative treatments are used first for cervical disc herniation with radiculopathy?
Conservative treatment for cervical disc herniation with radiculopathy usually begins with pain control, reduction of inflammation, and protection of the irritated nerve root. Treatment may include anti-inflammatory medication, short corticosteroid courses in selected cases, muscle relaxants, neuropathic pain medication such as gabapentin or pregabalin, and physical therapy after the acute pain settles. Posture correction, ergonomic changes, avoiding prolonged neck flexion, and careful neck and shoulder strengthening are important. Cervical traction may help selected patients. Forceful neck manipulation is generally avoided. If radicular pain persists despite structured conservative care, selective nerve root blocks or epidural steroid injections may be considered.
Why does cervical disc herniation treatment sometimes fail despite medication, physical therapy, or injections?
Cervical disc herniation treatment may fail when the true pain generator is not correctly identified or when several mechanisms are active at the same time. Pain may persist if the dominant cause is not only nerve root compression, but also facet joint pain, muscle spasm, myofascial trigger points, shoulder disease, peripheral nerve entrapment, posture-related overload, central sensitization, or metabolic and inflammatory contributors. Treatment can also fail when the MRI finding does not match the symptoms. In persistent neck and arm pain, the next step is usually structured reassessment, not simply repeating the same medication, therapy, or injection.
When are block injections considered in cervical disc herniation?
Block injections in cervical disc herniation are considered when arm pain from cervical radiculopathy persists despite structured conservative treatment, or when doctors need to clarify whether a specific nerve root is the main pain source. A selective nerve root block or epidural steroid injection may reduce inflammation around the irritated nerve and provide temporary or sometimes longer-lasting relief. Injections are not a cure for every cervical disc herniation and should be used carefully, especially when there are neurological deficits or spinal cord compression. If weakness or myelopathy is present, surgery may be more appropriate than repeated injections.
How is cervical disc herniation diagnosed?
Cervical disc herniation is diagnosed by combining symptoms, neurological examination, and imaging. MRI is the main test because it shows discs, nerve roots, spinal cord compression, foraminal narrowing, and the degree of canal stenosis. CT may help when bone spurs or calcified hard-disc changes are suspected. X-rays can show alignment or instability in selected cases. EMG and nerve conduction studies may help when symptoms and MRI do not clearly match. The most important point is that cervical disc herniation is not diagnosed by MRI alone. The imaging finding must explain the patient’s neck pain, arm pain, numbness, weakness, or myelopathy signs.
What surgical options for cervical disc herniation exist?
Surgical options for cervical disc herniation depend on the location of compression, the number of levels involved, spinal alignment, degeneration, and whether the nerve root or spinal cord is compressed. The most common operation is anterior cervical discectomy and fusion, or ACDF, where the disc is removed from the front and the level is fused. Cervical disc arthroplasty may be used in selected patients to preserve motion. Posterior foraminotomy may help lateral or foraminal disc herniations without fusion. Multilevel stenosis or myelopathy may require laminectomy, laminoplasty, or corpectomy. Surgery should match the exact anatomy and symptoms.
Which is better for cervical disc herniation — ACDF or cervical disc arthroplasty?
ACDF and cervical disc arthroplasty can both be effective for cervical disc herniation, but they are used in different situations. ACDF is the most established option and is often preferred when there is significant degeneration, instability, hard-disc osteophytes, deformity, or multilevel disease. Cervical disc arthroplasty may be considered in selected patients with a soft disc herniation, preserved motion, no major facet arthritis, and no severe spondylosis. Arthroplasty preserves some motion at the operated level, while ACDF fuses the level. The best option depends on age, anatomy, disc type, spinal alignment, symptoms, and surgeon experience.
How soon does cervical disc herniation surgery help when it is indicated?
Cervical disc herniation surgery often relieves arm pain quickly when the pain is truly caused by nerve root compression and the correct level is decompressed. Many patients notice improvement in radicular arm pain within days or weeks. Numbness, tingling, and weakness may recover more slowly because the nerve needs time to heal. Recovery is less predictable when nerve compression has lasted a long time, when weakness is severe, or when spinal cord compression has caused myelopathy. Neck pain may not improve as dramatically as arm pain if it comes from muscles, facet joints, posture, or another pain generator.
What is the typical recovery timeline for cervical disc herniation without surgery?
The typical recovery timeline for cervical disc herniation without surgery is about 6–12 weeks for many patients, especially when the main problem is inflammation around the nerve root rather than fixed severe compression. Acute arm pain often improves first, followed by gradual improvement in tingling, numbness, and function. Physical therapy is usually introduced after the most severe pain settles. Some patients need several months for full recovery, especially with older hard-disc changes or longer-lasting symptoms. Recovery should be reassessed if pain remains disabling, weakness progresses, or signs of cervical myelopathy appear. Conservative treatment should improve the trend, not just mask symptoms.
What are the risks of cervical disc herniation surgery?
Cervical disc herniation surgery is usually safe in experienced hands, but it carries risks like any spine operation. Possible risks include infection, bleeding, hoarseness, swallowing difficulty, cerebrospinal fluid leak, nerve root injury, spinal cord injury, persistent pain, recurrent symptoms, nonunion after fusion, adjacent segment degeneration, or need for further surgery. The risk profile depends on the procedure, number of levels, degree of degeneration, prior surgery, general health, and whether spinal cord compression is present. Surgery should be considered when the expected benefit clearly outweighs these risks. A second opinion can help when the indication for surgery is uncertain.
Why do some patients still have neck pain after cervical disc herniation surgery?
Some patients still have neck pain after cervical disc herniation surgery because the operation may successfully decompress the nerve root but not treat every pain generator. Arm pain from radiculopathy often improves faster than axial neck pain. Persistent neck pain may come from facet joints, muscle spasm, myofascial trigger points, adjacent level degeneration, scar-related nerve irritation, posture-related overload, or central sensitization. In some cases, the original disc was not the main source of pain. Persistent or recurrent pain after cervical surgery should be reassessed carefully before assuming that another operation is needed. The exact anatomical source of pain must be identified again.
How do cervical hard-disc spondylotic cases differ from soft cervical disc herniations?
Cervical hard-disc spondylotic cases differ from soft cervical disc herniations because they involve chronic degeneration, calcified or fibrotic disc material, osteophytes, and often narrowing of the spinal canal or neural foramen. Soft cervical disc herniations are usually more focal and may improve as inflammation settles or the fragment shrinks. Hard-disc disease is more rigid and less likely to disappear spontaneously. It may cause persistent foraminal stenosis, nerve root compression, or spinal cord compression. Treatment decisions are different because hard-disc cases may require more formal decompression, and symptoms may reflect spondylosis or myelopathy rather than only a fresh disc fragment.
When is cervical disc herniation urgent?
Cervical disc herniation is urgent when there is progressive arm or hand weakness, signs of cervical myelopathy, severe spinal cord compression, gait imbalance, clumsy hands, new bladder problems, rapidly worsening neurological deficits, or severe pain with concerning neurological findings. Sudden loss of function should not be managed only with home care or repeated medication. Cervical myelopathy is especially important because delayed treatment can leave permanent spinal cord damage. Severe pain alone is not always a surgical emergency, but worsening weakness or spinal cord signs require prompt neurosurgical evaluation. The urgency depends on neurological status, MRI findings, and symptom progression.
Can a second opinion via telehealth help in cervical disc herniation with radiculopathy?
A telehealth second opinion can help in cervical disc herniation with radiculopathy when symptoms persist, MRI findings are unclear, surgery has been recommended, or treatment has not worked as expected. During an online review, a specialist can compare the MRI level with the patient’s arm pain pattern, numbness, weakness, reflex changes, and possible myelopathy signs. The consultation can clarify whether conservative treatment is still reasonable, whether injections are appropriate, whether ACDF or disc arthroplasty is being considered for the right reason, and whether another pain generator may explain persistent neck or arm pain. It can also help patients avoid unnecessary or poorly targeted surgery.
Artificial intelligence can also support the process by analyzing complex data, but clinical expertise remains essential.
Additional Information for Cervical Disc Herniation & Radiculopathy
-
AAOS OrthoInfo — Cervical Radiculopathy (Pinched Nerve)
Patient-friendly guide to cervical nerve root impingement — causes, symptoms, and treatment. -
Spine-Health — Cervical Herniated Disc: Symptoms & Treatment
Detailed overview of cervical herniation, MRI findings, and conservative vs. surgical treatment paths. -
Mass General — Cervical Radiculopathy
Academic center resource describing clinical presentation and management of cervical disc disorders. -
NHS — Cervical Spondylosis
UK NHS guidance on age-related neck degeneration commonly associated with “hard-disc” herniation. -
AAFP — Cervical Radiculopathy (Patient Information)
Official patient handout explaining symptoms, diagnostic tests, and treatment approaches.