Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author:
Dr. Zeljko Kojadinovic, MD, PhD
— Neurosurgeon and Pain Specialist
Specialized Experience:
30 years of clinical expertise in neurosurgery.
Last medically reviewed:
March 08, 2026
Who Should Read This Page
This page is intended for patients who have pain that increases during sitting, but do not clearly understand why this happens or how to reduce it. In many cases, patients notice that pain appears after a period of sitting, worsens in certain positions or environments, or improves when standing or changing position — yet the exact reason for this pattern remains unclear, even after medical evaluation.
The main problem is that sitting is often treated as a general cause of pain, while in reality it acts as a specific mechanical load on particular anatomical structures. Without identifying which structure is involved and what process is occurring within it, it is not possible to define an effective strategy — whether that involves posture, chair selection, or additional modifications. If you are trying to understand why sitting increases your pain and what exactly needs to be changed to reduce it, this page provides a structured explanation of those mechanisms.
Sitting and Pain — Quick Summary (Read This First)
- Sitting does not cause pain by itself. Pain develops because sitting increases load on specific anatomical structures and the processes occurring within them.
- The same sitting position can relieve pain in one patient and worsen it in another. This depends on which structure is involved and what mechanism is causing pain.
- Pain during sitting usually appears after prolonged exposure. It is related to cumulative load, reduced circulation, and gradual tissue sensitization.
- Multiple structures may be involved at the same time. Discs, facet joints, sacroiliac joints, coccyx, nerves, muscles, and fascia can all contribute to symptoms.
- The key problem is not posture alone, but the process within the affected structure. Microtrauma, inflammation, instability, muscle spasm, and nerve irritation are the actual causes of pain.
- Identifying the structure is not enough — the mechanism must be understood. The same anatomical region can produce pain through different processes that require different approaches.
- General sitting advice is often insufficient. Standard recommendations may not reduce load on the specific structure responsible for pain.
- Even within the same diagnosis, sitting must be individualized. Patients with the same condition may require completely different sitting strategies.
- Chair selection cannot be based on short testing. Pain often appears only after prolonged real-life sitting, so evaluation must be structured and time-based.
- Sitting is usually only one of several contributing factors. Mechanical load interacts with systemic and neurophysiological factors that influence pain persistence.
- Leg and pelvic pain during sitting is not always a disc problem. It may originate from joints, muscles, peripheral nerves, or load distribution in the pelvis.
- Effective treatment requires identifying the true pain generator and modifying load accordingly. The goal is not to sit “correctly,” but to reduce load on the specific structure driving the pain.
Most readers benefit from combining this summary with sections on how sitting-related pain develops, anatomical structures involved, pain mechanisms, and individualized sitting strategies. The following sections explain how these factors interact and how sitting can be modified based on the specific cause of pain.
Contents
- Who Should Read This Page
- Quick Summary
- Prolonged Sitting
- How Sitting Causes Pain
- Structures Affected
- Why Mechanism Matters
- Combination of Causes
- How Tissues Are Loaded
- Treatment Principles
- Why General Advice Fails
- Why It Must Be Individualized
- Chair Selection
- Clinical Principle
- Sciatica While Sitting
- Sacroiliac Pain
- Tailbone Pain
- Pudendal Neuralgia
- Other Pelvic Pain
- Leg Pain While Sitting
- Car and Truck Drivers
- Cycling and Motorcycle Riding
- Gaming Chairs
- Red Flags
- FAQS
- Common Questions
- Second Opinion
This page is not about general posture advice. It focuses on patients whose pain appears or worsens during sitting because sitting loads a specific structure — such as a disc, sacroiliac joint, coccyx, pudendal nerve, pelvic floor, gluteal region, or lumbar nerve root. The key question is not simply how to sit correctly, but which structure becomes overloaded, why pain appears after time, and what needs to be changed to reduce that load.
This includes lower back pain, buttock pain, pelvic pain, coccyx pain, pudendal-type pain, and leg pain that becomes worse while sitting.
To keep the analysis precise, the discussion is intentionally limited to this anatomical region. Sitting can affect other parts of the body, but here the mechanisms are the most complex and clinically relevant.
Although sitting is commonly presented as a general cause of pain, this is an oversimplification. In practice, pain does not arise from sitting itself, but from how sitting interacts with specific anatomical structures, the processes occurring in those structures, and the individual characteristics of the patient.

Image: Long sitting provokes pain in many different ways
What is considered prolonged sitting
In most clinical and research contexts, prolonged sitting is defined as more than 6–7 hours per day, particularly when it occurs without meaningful breaks. In certain populations such as office workers, drivers, and students, this threshold is frequently exceeded, and studies show a clear association with low back pain.
However, duration alone does not explain why some individuals develop pain while others do not. The key factors are position, type of load, variability of posture, and the specific structures being stressed.
How sitting-related pain develops in practice
Sitting-related pain has a very characteristic pattern that is often misunderstood.
The onset of pain depends on several mechanical and situational factors, which are outlined below:
- after prolonged sitting, often several hours
- during specific activities, such as computer work or leaning forward
- in specific environments, such as office chairs, cars, or soft seating
- and often becomes more pronounced later in the day
Patients frequently report that pain is absent during short periods of sitting, but becomes evident only after sustained exposure. This is why it may not be reproducible during a short clinical examination.
Pain localisation and distribution vary depending on the anatomical structure involved and the underlying pathological process:
- disc-related pain may radiate toward the leg
- facet joint pain is usually localized or referred
- sacroiliac pain often spreads toward the buttock
- pudendal nerve irritation produces pain in the perineal or genital region, typically worsening during sitting
These are not mutually exclusive. In many patients, several of these patterns coexist.
Anatomical structures affected by sitting and related pain patterns
Sitting distributes load across multiple anatomical structures, and each of them can generate a specific type of pain.
At the spinal level, intervertebral discs are exposed to increased pressure, especially in flexed posture. This may lead to degeneration or herniation, with possible irritation of nerve roots and pain radiating into the leg
Facet joints, located posteriorly, are sensitive to changes in spinal curvature and load distribution. Their irritation typically causes localized low back pain or referred pain without clear neurological deficit.
Sacroiliac joints are subjected to prolonged and often asymmetrical loading. Pain originating from this region is commonly felt in the lower back, buttock, or upper leg.
The coccyx (tailbone) is directly exposed to pressure during sitting. Pain in this region is highly dependent on anatomical variation, joint mobility, and local inflammatory processes.
Nervous structures are particularly important. Sitting may irritate lumbar and sacral nerve roots, but also peripheral nerves such as the pudendal nerve, which can be compressed or stretched along its course, producing neuropathic pain in the perineal region
Muscles and fascia, including paraspinal muscles, gluteal muscles, and pelvic floor, are continuously active during sitting. This leads to fatigue, increased tone, and secondary pain syndromes with inflammation and spasm, which may further contribute to nerve irritation.
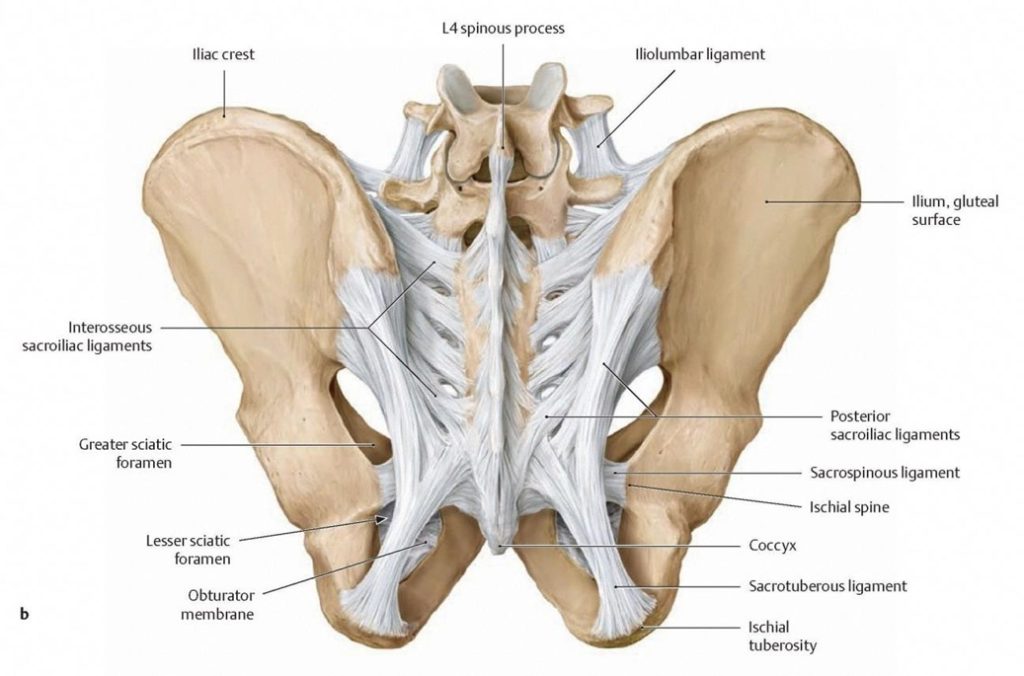
Image: These are just some of the lower back and pelvic structures that can be damaged by prolonged sitting and become sources of pain, such as the facet and sacroiliac joints, elements of the coccyx, and associated ligaments.
Why Identifying the Structure Is Not Enough — The Mechanism Matters
Identifying which anatomical structure is involved is only the first step. In clinical practice, pain cannot be understood or treated based on structure alone.
The same structure can generate pain through different mechanisms, and each of them requires a different approach to unloading and treatment.
For example, pain originating from the coccyx is not a single condition. It may result from:
- joint instability between coccygeal segments, with ligamentous stretching and local inflammation
- a coccyx that is straight or anteriorly curved, which changes how load is transmitted during sitting
- local inflammation or bursitis in surrounding soft tissues
- or a neuropathic component, involving structures such as the ganglion impar or coccygeal nerve
Each of these mechanisms produces pain through a different process, which is why the same sitting position may relieve pain in one patient but worsen it in another.
As a result, sitting strategy cannot be generalized, but must be adapted to the specific mechanism involved.
Pain is usually caused by a combination of mechanisms
In most patients, pain does not originate from a single structure. It results from a combination of interacting mechanisms.
For example, a patient may have:
- disc-related irritation combined with facet joint overload
- sacroiliac dysfunction combined with muscle imbalance
- nerve irritation combined with pelvic floor tension
The exact combination depends on individual characteristics such as body height, body weight, obesity, spinal curvature, pelvic anatomy, and daily mechanical load.
However, pain is not determined by mechanical factors alone. Systemic and neurophysiological factors — including metabolic state, inflammatory processes, nutritional status, and central sensitization — may significantly influence how pain develops and persists.
This explains why identical sitting conditions can produce completely different symptoms in different individuals.
How sitting loads tissues and what processes occur in them
A key point is that pain is not caused by the structure itself, but by processes occurring within that structure.
Sitting creates several types of load, each affecting tissues in a different way.
Mechanical load increases pressure on discs, joints, and soft tissues, particularly in flexed or asymmetrical positions.
Static load results from prolonged muscle activation without movement, leading to fatigue and overload.
Reduced movement decreases circulation, contributing to tissue hypoxia and increased sensitivity.
Neural load may occur through direct compression of nerves or indirectly through surrounding structures such as muscles or ligaments.
Over time, these loads lead to specific pathological processes, which often coexist and reinforce each other:
- Microtrauma due to repetitive mechanical stress
- Inflammation in joints, ligaments, or surrounding soft tissues
- Muscle spasm and increased tone, contributing to further mechanical overload
- Mechanical instability in joints or segments — for example, in facet joints, sacroiliac joints, or sacrococcygeal joints
- Nerve irritation, microcompression, and sensitization, which amplify pain perception
These processes are the actual cause of pain, not posture alone.
What effective treatment requires
Effective treatment requires a structured approach.
First, it is necessary to determine which structure is the primary source of pain.
Second, it is essential to understand which process is occurring within that structure.
Third, contributing factors must be identified. Sitting is often one of them, but rarely the only one.
This means that sitting is not treated as an isolated cause, but as one of the factors that must be modified to allow the affected structure to recover.
Why general sitting advice is insufficient
General recommendations such as sitting upright or keeping the knees at 90 degrees are often presented as universal solutions. In reality, they are not sufficient and may not apply to a specific condition.
Different structures require different unloading strategies.
For example:
- in disc-related pain, certain positions increase pressure on the disc
- in facet joint pain, extension may increase joint loading
- in sacroiliac dysfunction, asymmetrical loading is often critical
- in pudendal neuralgia, pressure on the perineal region must be avoided
Therefore, a single recommendation cannot be applied to all patients. These are only general principles; in fact, advice is always individualized and is never the same even for two patients who both suffer from coccydynia, for example.
Even within the same diagnosis, sitting must be individualized
A particularly important example is tailbone pain.
The appropriate sitting strategy depends on multiple factors, including:
- whether the coccyx is straight or curved forward
- whether there is joint instability
- whether the pain is mechanical or neuropathic
- whether inflammation or bursitis is present
The coccyx is used here as a clear and illustrative example, because it demonstrates particularly well how different mechanisms can exist within the same anatomical region. This means that even within the same diagnosis, different patients require different approaches to sitting and unloading.
Individualized unloading and chair selection
Once the pain mechanism is understood, sitting can be modified in a targeted way.
This includes adjusting posture, selecting an appropriate chair, and using additional supports or relaxation if necessary.
However, an important limitation must be emphasized.
A chair cannot be properly evaluated during a short trial. Pain often appears only after prolonged sitting under real-life conditions. For that reason, patients must be instructed how to test a chair in their usual environment, how long the testing should last, and what specific changes in symptoms they should observe. Without this structured approach, even a well-designed chair may seem comfortable initially but fail to prevent pain.
In addition, recommendations must consider what is available in the patient’s country. Different manufacturers design chairs with different priorities. Some focus on general ergonomics, while others provide better unloading of specific regions such as the lumbar spine or pelvis.
Final clinical principle
Sitting is a common contributing factor in the development of pain, but it is not the full explanation.
Effective treatment requires identifying the exact pain generator, the processes occurring within that structure, and the factors that maintain those processes. Only then can sitting be modified in a way that actually reduces load on the relevant structure.
The goal is not to sit ‘correctly,’ but to identify the specific structure involved, understand the pathological process within it, and adjust sitting in a way that directly reduces the mechanical load driving that process.
Sciatica (Leg Pain) While Sitting — Why It Happens
Pain radiating from the lower back into the leg while sitting is one of the most commonly searched symptoms. It is often attributed to a “pinched nerve,” but the mechanism is not always the same.
In many cases, this type of pain is related to irritation of a lumbar nerve root. This irritation may result from a disc herniation, but also from facet joint changes, ligament thickening, or muscle-related compression around the nerve.
Sitting increases pressure inside the intervertebral discs and may also change the alignment of the spine, which can increase tension on already irritated nerve roots. In addition, prolonged sitting leads to reduced movement and circulation, which may further increase nerve sensitivity.
However, not all leg pain while sitting is caused by a disc. In some patients, similar symptoms may originate from muscular or fascial structures, or even from sacroiliac dysfunction.
This is why identifying the exact mechanism is essential before deciding how sitting should be modified.
Sacroiliac Joint Pain While Sitting
Pain originating from the sacroiliac joints is often overlooked, especially in patients who have been told that their problem is “disc-related.”
The sacroiliac joints connect the spine and pelvis and are exposed to continuous load during sitting, particularly when weight distribution is asymmetrical. This type of pain is typically felt in the lower back and buttock, sometimes radiating toward the thigh. It may worsen during prolonged sitting, especially in positions that shift load to one side.
Sacroiliac pain is more common in women, partly due to anatomical and hormonal factors that influence joint stability.
Unlike disc-related pain, sacroiliac pain is more strongly influenced by asymmetrical loading and load distribution across the pelvis. During sitting, this is affected not only by spinal position, but also by how weight is transmitted through the pelvis — including direct loading of the coccyx, which can alter load transfer toward the sacroiliac joints.
Tailbone (Coccyx) Pain While Sitting — Why Sitting Strategy Must Be Individual
Tailbone pain is one of the clearest examples of why sitting recommendations cannot be universal.
The coccyx is directly exposed to pressure during sitting, but the effect of that pressure depends on several individual factors. In some patients, the coccyx is relatively straight, while in others it is curved forward. In some cases, the joints between coccygeal segments are stable, while in others there is increased mobility or instability.
Pain may arise from purely mechanical irritation, but it may also involve inflammation of surrounding soft tissues, such as bursitis, or even neuropathic mechanisms involving local nerves. Because of this, two patients with the same diagnosis of coccyx pain may require completely different sitting strategies. In some cases, reducing direct pressure is sufficient. In others, the position of the pelvis and distribution of load must be modified more precisely. This is why simple advice such as using a cushion is often not enough unless it is adapted to the specific anatomical and mechanical characteristics of the patient.
Pudendal Neuralgia and Sitting — A Key but Often Missed Mechanism
Pudendal neuralgia represents one of the most specific and often overlooked causes of sitting-related pain.
The pudendal nerve travels through narrow anatomical spaces in the pelvis, including regions where it may be compressed between ligaments or within the pudendal canal. Sitting increases pressure in these regions and may directly irritate the nerve or increase tension along its course.
The pain is typically located in the perineal or genital region and is often described as burning, sharp, or electric. A characteristic feature is that pain worsens while sitting and improves when standing or sitting on a toilet seat, where pressure is redistributed.
In many patients, multiple mechanisms coexist. Mechanical compression, muscle tension in the pelvic floor, and nerve sensitization may all contribute to symptoms.
Because imaging often does not show the problem clearly, this condition is frequently misdiagnosed or attributed to other causes. Understanding how sitting affects the pudendal nerve is essential for both diagnosis and treatment.
Other Pelvic Pain Syndromes Related to Sitting
Similar mechanisms may also contribute to other types of pain in the same anatomical region.
Compression, tension, or sensitization of neural and surrounding structures during sitting may affect not only the pudendal nerve, but also other nerves and tissues within the pelvic region.
In addition to the pudendal nerve, sitting-related mechanisms may involve:
- the posterior femoral cutaneous nerve, contributing to pain in the lower buttock and posterior thigh
- the inferior cluneal nerves, associated with gluteal pain
- the ilioinguinal and genitofemoral nerves, which may contribute to groin or anterior pelvic pain
- branches of the sacral plexus, affected indirectly through surrounding muscles and connective tissues
These nerves may be affected either directly by pressure during sitting or indirectly through muscle tension and altered load distribution.
In addition to neural structures, similar mechanisms may contribute to symptoms in other pelvic conditions.
For example:
- in hemorrhoidal disease, prolonged sitting may increase venous pressure and congestion
- in prostate-related pain syndromes, sitting may contribute to pelvic tension and discomfort
- in vaginal or vulvar pain, neural sensitivity and pelvic floor dysfunction may play a role
- pelvic floor muscle spasm and increased tone, which may contribute to pain directly and also lead to secondary nerve irritation or compression
- interstitial cystitis (IC/BPS)
- Tarlov cyst
Although these conditions differ, they often share a common feature: increased pressure and altered load distribution within the pelvic region during sitting. This is why sitting-related pain in the pelvic region is often multifactorial and cannot be attributed to a single structure alone.
Leg Pain While Sitting — Not Always a Disc Problem
Leg pain during sitting is commonly attributed to sciatica, but this is not always correct.
Similar symptoms may arise from:
- Sacroiliac joint dysfunction — pain increases when sitting unevenly, leaning to one side, or when getting up from a chair
- Muscle-related compression — prolonged sitting on a hard surface or on the chair edge compresses gluteal muscles and sensitized tissues
- Peripheral nerve irritation — chair edge pressure or an inappropriate seat angle may compress the sciatic or pudendal nerve, especially with posterior pelvic tilt or asymmetrical loading
- Vascular or positional factors — crossing legs, pressure under the thigh, or restricted blood flow may cause numbness, tingling, or deep aching
The key is to determine whether the pain follows a nerve distribution, whether it changes with position, and whether it is influenced by mechanical load.
This distinction is essential because treatment and sitting modification depend on the underlying mechanism.
Sitting in Car and Truck Drivers — Prolonged Load in a Fixed Seating Environment
Sitting while driving represents a specific and often underestimated form of mechanical stress. It differs significantly from sitting in an office environment because it combines prolonged static posture, axial loading, and continuous micro-vibrations.
Drivers are exposed to sustained spinal loading without the possibility of frequent posture changes. In addition, the seated position is often slightly flexed, increasing pressure within the intervertebral discs.
A key factor is vibration. Even low-level, continuous vibration transmitted through the seat can contribute to accelerated disc degeneration and increased mechanical stress on spinal structures. This effect is well documented in populations such as professional drivers.
At the same time, muscle activity is reduced, particularly in stabilizing muscles, while passive structures such as ligaments and discs take over the load. This leads to fatigue, overload, and eventually pain.
In drivers, pain may present as:
- low back pain after prolonged driving
- stiffness and reduced mobility after getting out of the vehicle
- radiating pain into the leg
- worsening of pre-existing conditions such as disc herniation or sacroiliac dysfunction
Another important factor is limited ability to adjust position. Unlike office settings, where posture can be modified, drivers are constrained by the vehicle seat and controls.
Because of this, the same sitting recommendations used for office work cannot be directly applied to driving. The strategy must consider vibration, seat design, duration of driving, and individual biomechanics.
Cycling and Motorcycle Riding — Focal Perineal Load and Vibration
Cycling and motorcycle riding represent a specific form of sitting in which body weight is concentrated on a relatively small contact surface, often directly over the perineal and posterior pelvic region. This leads to focal pressure on soft tissues and neural structures, which differs from the broader load distribution seen in typical seating.
In both activities, this effect may be further increased by repetitive microtrauma and vibration, contributing to tissue irritation, inflammation, and nerve sensitivity.
Because of these factors, attempts to reduce symptoms often focus on modifying the contact interface, including different saddle or seat designs and the use of inserts in cycling shorts or riding pants. These modifications aim to redistribute pressure and reduce direct loading of sensitive structures.
However, their effectiveness depends on how well they address the specific mechanism responsible for pain, as not all forms of load can be sufficiently altered through these adjustments alone.
Prolonged Sitting in Gaming Chairs — Static Load and Postural Fatigue
Gaming-related sitting introduces a different pattern of load, characterized by prolonged static posture and reduced movement.
Although gaming chairs are often marketed as ergonomic, their design frequently prioritizes appearance and adjustability over actual load distribution. In many cases, multiple adjustable components — such as backrest angle, lumbar support, and seat tilt — create configurations that may appear supportive but do not necessarily reduce load on the relevant anatomical structures. However, the fundamental relationships between key elements — including seat shape, backrest geometry, and pressure distribution — are usually fixed and cannot be substantially modified. Because of this, a chair may appear highly adjustable, yet remain unable to adapt to the specific biomechanical requirements of a given condition, limiting its ability to effectively unload the structures responsible for pain.
Over time, this leads to:
- sustained muscle activation and fatigue
- increased load on passive structures such as ligaments and discs
- reduced circulation and tissue sensitivity
In addition, attention during gaming is focused on the screen, which reduces awareness of posture and delays natural position changes.
This combination of static load, reduced variability, and prolonged duration may contribute to the development or worsening of:
- low back pain
- neck and shoulder pain
- pelvic discomfort
For this reason, the key issue is not the chair itself, but the lack of movement and sustained loading over time.
When Sitting-Related Pain Requires Medical Evaluation (Red Flags)
Most sitting-related pain is mechanical and not dangerous. However, certain symptoms indicate that further medical evaluation is necessary.
These warning signs are important because they may suggest serious underlying conditions that should not be attributed to posture or sitting alone.
Medical evaluation should be considered if pain is associated with:
- progressive weakness in the leg
- numbness in the genital or perineal region
- loss of bladder or bowel control
- severe, constant pain that does not change with position
- pain following trauma
- unexplained weight loss or systemic symptoms
- history of cancer or infection
These features may indicate conditions such as significant nerve compression, spinal cord involvement, infection, or tumor. In such cases, focusing only on sitting position or ergonomics may delay appropriate diagnosis and treatment. Recognizing these signs is an essential part of any comprehensive discussion of sitting-related pain.
Questions Patients Commonly Ask About Sitting and Pain
Patients rarely ask about sitting in general terms. Instead, they come with specific questions that reflect uncertainty about the cause of their symptoms or why previous treatment has not worked.
Does sitting actually cause my pain, or is something else wrong?
In most cases, sitting is not the primary cause, but a trigger that increases load on an already sensitive structure. The key is to identify which structure is involved and how sitting affects it.
Why does my pain appear only after prolonged sitting?
Pain usually depends on duration, cumulative load, and reduced circulation, rather than on position alone. This is why symptoms often appear only after several hours.
Why does sitting hurt even when I try to sit properly?
General ergonomic advice does not address the specific mechanism of pain. A position that reduces load for one structure may increase it for another.
What should I change — posture, chair, or something else?
The answer depends on the interaction between the structure involved, the process within it, and the type of load. In many cases, changing posture alone is not sufficient.
How do I know which chair is right for me?
A chair cannot be selected based on general features. It must be evaluated based on whether it reduces load on the specific structure involved, which usually requires testing under real conditions.
Why didn’t previous treatment solve the problem?
In many cases, treatment focuses on imaging findings or general diagnoses, while the actual pain mechanism remains unrecognized and therefore not properly addressed.
Sitting-Related Pain — Second Opinion (Why Sitting Causes Your Pain and What Needs to Be Changed)
Patients whose pain increases during sitting often notice a very specific pattern:
pain appears after a period of sitting, worsens in certain positions or environments, and improves when standing or changing position.
They often face the same unanswered questions:
Why does sitting trigger my pain?
Which structure is actually affected?
Why does pain appear only after some time?
Why didn’t previous treatments help?
Should I change posture, chair, or something else?
In most cases, the problem is not sitting itself, but how sitting loads a specific structure and what process is occurring within it.
Without identifying this mechanism, recommendations remain general and often ineffective.
A medical second opinion focuses on identifying the true pain generator and the exact mechanism —
including discs, joints, nerves, pelvic structures, muscles, and load distribution during sitting.
The goal is to explain why pain appears in your specific case and what exactly needs to be changed to reduce it.
In most cases, this type of analysis is performed as part of a general medical second opinion about your pain condition.
However, when sitting is a major trigger, a more detailed and focused analysis of sitting mechanics may be required.
- ✔ Describe when pain appears (duration of sitting, positions, activities such as computer work or driving)
- ✔ Send available reports (MRI, CT, previous diagnoses) — but focus is on symptom pattern and load response
- ✔ You will receive a reply within 24 hours explaining whether consultation is appropriate and what additional information is needed
- ✔ During consultation, we analyze how sitting affects your body and identify the structure and mechanism responsible for pain
- ✔ You receive clear guidance on what to change — posture, chair, load distribution, or other factors — based on your specific case
Consultation fees typically range from $180–250 depending on case complexity.
Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Frequently Asked Questions About Sitting-Related Pain
Why does pain appear only after prolonged sitting?
Pain that appears only after prolonged sitting usually reflects cumulative load rather than a single bad position. During sitting, discs, facet joints, sacroiliac joints, coccyx, pelvic nerves, muscles, and fascia are exposed to sustained mechanical and static load. At first, the tissue may tolerate this load, but after one or two hours circulation decreases, muscles fatigue, ligaments remain stretched, and sensitized nerves become more reactive. This is why a short clinical examination or brief chair test may not reproduce the pain. The key is to identify which anatomical structure becomes overloaded over time and what process inside it — inflammation, instability, muscle spasm, nerve irritation, or sensitization — produces the symptoms.
Why does sitting increase pain even when MRI findings seem mild?
Mild MRI findings do not always mean that pain is mild, and normal or near-normal imaging does not exclude sitting-related pain. MRI shows anatomy, but it may not show functional overload, local inflammation, muscle spasm, ligament strain, pelvic floor tension, peripheral nerve irritation, or central sensitization. Sitting can increase pressure on a mildly degenerated disc, shift load toward facet or sacroiliac joints, compress the coccyx, or irritate pelvic nerves such as the pudendal nerve. A specialist must understand the anatomy of pain in the lower back, pelvis, and legs and determine whether the MRI finding is truly responsible or whether another structure is the real pain generator.
Does sitting itself cause pain or only aggravate an existing problem?
Sitting rarely acts as the only cause of pain. More often, it is a mechanical trigger that increases load on an already sensitive anatomical structure. The affected structure may be an intervertebral disc, facet joint, sacroiliac joint, coccyx, nerve root, pudendal nerve, pelvic floor muscle, fascia, or ligament. Sitting then modifies pressure, circulation, nerve tension, and load distribution in a way that activates symptoms. This is why the same sitting posture can be harmless for one person and painful for another. Effective treatment requires identifying the primary pain generator, understanding the pathological process within it, and recognizing contributing factors that keep it sensitive over time.
Why can the same sitting position help one patient but worsen pain in another?
The same sitting position can have opposite effects because different patients have different pain generators and mechanisms. A posture that reduces disc pressure may increase facet joint load. A cushion that unloads the coccyx may shift pressure toward the sacroiliac joints or perineal region. A forward-leaning position may help one type of tailbone pain but worsen disc-related or pelvic floor-related pain. This is why sitting advice cannot be generalized. The specialist must know which structures in the lower back, pelvis, and legs can cause pain, how sitting loads each of them, and which contributing factors maintain sensitivity. Only then can posture or chair strategy be individualized.
Why is identifying the pain structure not enough without understanding the mechanism?
Identifying the painful structure is only the first step. The same structure can cause pain through different mechanisms, and each mechanism requires a different sitting strategy and treatment plan. Coccyx pain, for example, may result from instability between coccygeal segments, a straight or anteriorly curved coccyx, soft-tissue inflammation, bursitis, or neuropathic irritation involving local nerves. These mechanisms do not respond to the same cushion, posture, or procedure. Similarly, disc-related pain, sacroiliac pain, and pudendal neuralgia can each have multiple sub-mechanisms. Successful treatment requires knowing the structure, the process occurring inside it, and the contributing factors that continue to maintain irritation during sitting.
Which anatomical structures can cause pain during sitting?
Sitting-related pain can come from several anatomical structures in the lower back, pelvis, and legs. Intervertebral discs may be overloaded, especially in flexed posture, and may irritate nerve roots. Facet joints can become painful when spinal curvature and load distribution change. Sacroiliac joints may hurt when pelvic loading is asymmetrical. The coccyx is directly compressed during sitting and may be affected by instability, shape, inflammation, or neuropathic irritation. Peripheral nerves, including the pudendal nerve, posterior femoral cutaneous nerve, inferior cluneal nerves, ilioinguinal and genitofemoral nerves, may also be irritated. Muscles and fascia can fatigue, tighten, and contribute to secondary pain and nerve irritation.
Can several pain generators be active at the same time during sitting?
Yes. In many patients, sitting-related pain is not caused by one structure alone. Disc irritation may coexist with facet overload, sacroiliac dysfunction may coexist with muscle imbalance, and pudendal nerve irritation may coexist with pelvic floor tension. Mechanical factors also interact with systemic and neurophysiological contributors such as inflammation, metabolic state, nutritional status, sleep disturbance, stress, and central sensitization. This explains why identical sitting conditions can produce different symptoms in different people. A successful evaluation must identify the dominant pain generator, but also recognize secondary mechanisms that amplify symptoms. Treating only one part of the pain system often leads to partial or temporary improvement.
Why does leg pain while sitting not always mean a disc herniation?
Leg pain while sitting is often called sciatica, but it is not always caused by a disc herniation. Sitting can irritate a lumbar nerve root, but similar pain may come from sacroiliac dysfunction, gluteal muscle compression, piriformis-related irritation, peripheral nerve compression, pelvic load imbalance, or pressure under the thigh. Vascular or positional factors, such as crossing the legs or compressing the back of the thigh, may also cause numbness, tingling, or aching. The key is to determine whether pain follows a true nerve distribution, whether it changes with position, and whether it is influenced by mechanical load. Treatment depends on this mechanism, not the word “sciatica” alone.
How can sitting irritate lumbar nerves and produce sciatica-like pain?
Sitting can irritate lumbar nerves by increasing pressure inside the intervertebral discs, changing spinal alignment, and increasing tension around already sensitive nerve roots. In a flexed sitting posture, disc pressure may rise and aggravate a disc-related or degenerative process. Prolonged sitting also reduces movement and circulation, which can increase nerve sensitivity over time. However, sciatica-like pain may also come from facet-related changes, ligament thickening, muscle-related compression, or sacroiliac dysfunction. This is why a specialist must compare the pain pathway, neurological findings, imaging, and mechanical triggers. The goal is to identify whether the lumbar nerve root is truly involved or whether another structure is imitating sciatica.
Why is sacroiliac joint pain often mistaken for disc-related pain?
Sacroiliac joint pain is often mistaken for disc-related pain because it may produce lower back, buttock, and upper leg pain. Patients may be told that their symptoms are disc-related, especially if MRI shows degenerative disc changes, but the real pain generator may be the sacroiliac joint or its surrounding ligaments. Sitting can worsen sacroiliac pain when pelvic loading is asymmetrical, when weight shifts to one side, or when the coccyx changes force transfer through the pelvis. Unlike disc pain, sacroiliac pain is strongly influenced by load distribution. Accurate diagnosis requires understanding pelvic pain anatomy, clinical pattern, and sometimes diagnostic SI joint blocks rather than relying only on lumbar MRI.
Why does coccyx pain require individualized sitting strategy?
Coccyx pain is one of the clearest examples of why sitting advice must be individualized. The coccyx is directly exposed to pressure during sitting, but the effect of that pressure depends on anatomy and mechanism. In one patient, the coccyx may be straight or anteriorly curved; in another, joint instability between coccygeal segments may be present. Pain may come from mechanical irritation, local inflammation, bursitis, ligament stretching, or neuropathic irritation involving local nerves such as the ganglion impar or coccygeal nerve. A simple cushion may help one mechanism and fail in another. Sitting strategy must therefore reduce load on the specific mechanism, not just the region.
How does pudendal neuralgia become worse during sitting?
Pudendal neuralgia often worsens during sitting because the pudendal nerve travels through narrow pelvic spaces where it may be compressed or stretched. Sitting increases pressure in the perineal region and can directly irritate the nerve or increase tension along its course. The pain is usually felt in the perineal or genital region and may be burning, sharp, or electric. A characteristic feature is that pain improves when standing or when sitting on a toilet seat, where pressure is redistributed. In many patients, mechanical compression, pelvic floor muscle tension, and nerve sensitization coexist. Imaging often does not show the problem clearly, so understanding pelvic nerve anatomy is essential for diagnosis.
Can pelvic floor tension and muscle spasm maintain sitting pain?
Yes. Pelvic floor tension and muscle spasm can maintain or amplify sitting-related pain, especially when pelvic nerves are already sensitive. During prolonged sitting, pelvic and gluteal muscles may remain under static load, fatigue, and develop increased tone. This can indirectly irritate nerves such as the pudendal nerve, posterior femoral cutaneous nerve, inferior cluneal nerves, or branches of the sacral plexus. Muscle spasm may also change pelvic load distribution and increase pressure on joints, fascia, and soft tissues. In these cases, pain is not explained by one anatomical lesion alone. Treatment must address both the nerve or joint source and the muscular contributors that maintain irritation.
Why do posture corrections and general ergonomic advice often fail?
General ergonomic advice often fails because it treats sitting as one problem, while sitting-related pain depends on the specific structure and mechanism involved. Advice such as sitting upright or keeping the knees at 90 degrees may reduce load for one structure but increase it for another. Disc pain, facet joint pain, sacroiliac dysfunction, coccyx pain, and pudendal neuralgia require different unloading strategies. Even patients with the same diagnosis may need different adjustments. The goal is not to sit “correctly” in a universal sense, but to reduce mechanical load on the exact pain-generating structure. Without identifying that structure and mechanism, posture advice becomes generic and often ineffective.
How should a chair be tested if pain appears only after prolonged sitting?
A chair cannot be judged during a short trial if pain usually appears only after prolonged sitting. Many chairs feel comfortable at first but fail after one or two hours because they do not change the load on the painful structure. Testing should be done in real-life conditions, during the activity that usually provokes pain, such as desk work, driving, or gaming. The patient should observe when pain begins, whether the pattern changes, and whether symptoms are delayed, reduced, or shifted. A useful chair is not simply the one that feels soft or comfortable initially, but the one that reduces load on the specific pain generator over time.
Can car driving and vibration worsen sitting-related pain differently than office work?
Yes. Driving creates a different type of sitting-related load than office work. It combines prolonged static posture, axial loading, limited ability to change position, and continuous micro-vibrations transmitted through the seat. The seated position is often slightly flexed, which can increase disc pressure and aggravate pre-existing disc or nerve-root problems. Vibration may further stress spinal structures and worsen pain in professional drivers or people who spend long hours in vehicles. Muscles also become less active, while passive structures such as discs and ligaments carry more load. For this reason, the same sitting recommendations used for office chairs cannot be directly applied to cars or trucks.
Why do gaming chairs and prolonged gaming often aggravate pain?
Gaming-related sitting often aggravates pain because it combines prolonged static posture, reduced movement, and high attention to the screen. Although gaming chairs are often marketed as ergonomic, many are designed more for appearance and adjustability than for true load redistribution. Adjustable backrest angle, lumbar support, or seat tilt may look helpful, but the basic seat shape and pressure distribution may still fail to unload the painful structure. Over time, sustained muscle activation, reduced circulation, ligament and disc loading, and delayed position changes can worsen low back, pelvic, or leg pain. The issue is not only the chair, but prolonged load without sufficient movement variability.
Which red-flag symptoms during sitting pain require medical evaluation?
Most sitting-related pain is mechanical and not dangerous, but some symptoms require medical evaluation. Progressive leg weakness, numbness in the genital or perineal region, loss of bladder or bowel control, severe constant pain that does not change with position, pain after trauma, unexplained weight loss, systemic symptoms, history of cancer, or signs of infection should not be attributed to posture or chair problems. These features may indicate significant nerve compression, spinal cord involvement, tumor, infection, or another serious condition. In such cases, focusing only on ergonomics can delay diagnosis. Red flags must be excluded before sitting-related pain is treated as a purely mechanical or postural issue.
Why did previous treatment fail to solve sitting-related pain?
Previous treatment often fails because it targets a general diagnosis rather than the real pain mechanism. A patient may receive treatment for a disc finding on MRI while the dominant pain generator is the sacroiliac joint, coccyx, pudendal nerve, pelvic floor muscle, or peripheral nerve irritation. In other cases, the correct structure is recognized, but the process inside it is misunderstood: inflammation, instability, muscle spasm, nerve sensitization, or microcompression may require different treatment. Sitting is often only one contributing factor among several. Meaningful improvement usually requires identifying the pain generator, defining the mechanism, and modifying the load that keeps the painful process active.
How can understanding the anatomy of pain change treatment and chair selection?
Understanding the anatomy of pain changes treatment because it shifts the focus from general posture advice to the exact structure and mechanism causing symptoms. If pain comes from a disc, the sitting strategy must reduce disc pressure. If it comes from the sacroiliac joint, symmetrical pelvic loading becomes more important. If the coccyx is involved, direct pressure and coccygeal mechanics must be considered. If pudendal neuralgia is present, perineal pressure must be reduced. Chair selection also becomes mechanism-based rather than brand-based. The goal is not to find a universally “best” chair, but to reduce load on the specific pain generator while treating the factors that maintain sensitivity.