Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Author: Dr. Zeljko Kojadinovic, MD, PhD – Consultant Neurosurgeon and Pain Management Specialist
Last medically reviewed: June 3, 2026
Who this page is for
This page is for patients who have been diagnosed with Tarlov (perineural) cysts on MRI and are uncertain whether these cysts are causing their pain or are incidental findings.
It is also intended for those who have persistent low back, sacral, pelvic, or leg pain, numbness, or urinary symptoms without a clear explanation, where Tarlov cysts were noted in imaging reports.
A structured telehealth second opinion helps determine whether the cyst is clinically significant and provides guidance on the most appropriate management — conservative, image-guided, or surgical.
When patients usually seek a second opinion for Tarlov cyst pain
- Pain persists despite conservative treatment (physical therapy, medications)
- Symptoms keep recurring after temporary improvement
- MRI shows Tarlov cysts but uncertainty if they’re clinically relevant
- You are considering injections, procedures, or surgery
If this reflects your situation, a focused telehealth review can clarify the most likely pain generators, what treatments are reasonable, and what is — and is not — indicated in your case: Request Consultation
Tarlov Cysts — Quick Summary (Read This First)
- A Tarlov cyst seen on MRI is often incidental and should not automatically be assumed to be the cause of pain. Many sacral or perineural cysts are found by chance and do not require surgery.
- A Tarlov cyst should also not be ignored when symptoms fit its nerve-root location. Sacral, pelvic, buttock, tailbone, leg, urinary, bowel, or sexual symptoms may be relevant when they match the affected sacral nerve roots.
- The key question is whether the Tarlov cyst is incidental, a contributing factor, or the primary pain generator. MRI alone usually cannot answer this question.
- Before deciding that a Tarlov cyst causes pain, other pain generators must be actively excluded. Low back, sacral, pelvic, gluteal, coccygeal, and leg pain may come from discs, facet joints, sacroiliac joints, coccyx, pudendal nerve, pelvic floor muscles, gluteal muscles, ligaments, or peripheral nerve entrapment.
- Many important causes of pain are not clearly visible on standard MRI. Mechanical overload, instability, nerve irritation, pelvic floor spasm, ligament pain, myofascial pain, and sensitization may produce severe symptoms even when imaging findings seem mild.
- A decision about Tarlov cyst surgery should not be based only on seeing a cyst on MRI. Symptoms, neurological findings, cyst level, cyst anatomy, sitting intolerance, pelvic symptoms, and exclusion of other pain sources must fit together.
- Some surgical opinions may focus mainly on the visible cyst. In complex pain cases, this can be risky if other pain generators have not been systematically checked before surgery is proposed.
- Good assessment requires detailed knowledge of pain anatomy. The clinician must understand which structures can cause low back, sacral, pelvic, buttock, tailbone, or leg pain before deciding whether the Tarlov cyst is truly responsible.
- Treatment depends on clinical relevance, not size alone. Observation, conservative treatment, pain-source treatment, image-guided procedures, aspiration with fibrin sealant, or surgery may be considered only after structured evaluation.
- This page is for patients who have Tarlov cysts on MRI and need to know whether the cyst explains their pain or whether another hidden pain source should be considered first.
Most readers benefit from reviewing this summary together with the sections on When Can Tarlov Cysts Cause Pain?, Persistent Pain and Tarlov Cysts, Pain Contributing Factors That Should Also Be Diagnosed, and Indications for Surgery and Surgical Options in Tarlov Cysts. The main purpose is to clarify whether the cyst is a true pain generator, only a contributing factor, or an incidental MRI finding.
Learn how to determine if a Tarlov cyst is truly the cause of your symptoms and when its surgery is justified.
Contents
- Who this page is for
- What Are Tarlov Cysts?
- How Common Are Tarlov Cysts?
- Symptoms Linked to Cysts
- When Can Cysts Cause Pain?
- How Are Cysts Diagnosed?
- How We Assess Unexplained Pain
- What if Persistent Pain and Tarlov Cysts Coexist?
- Pain Contributing Factors That Should Also Be Diagnosed
- Treatment Options
- Conclusion: Is the Cyst the Cause or a Contributor?
- Indications for Surgery and Surgical Options
- FAQ – Tarlov Cysts
- Additional Information
- Start Telehealth Consultation
What Are Tarlov Cysts?
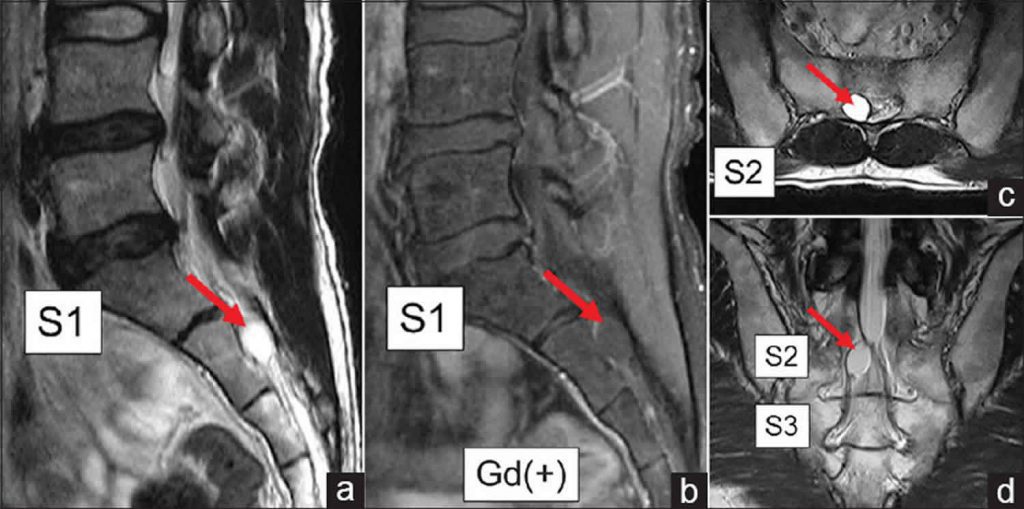
Tarlov cysts are perineural (periradicular) dilatations of the nerve root sheath filled with cerebrospinal fluid (CSF). They are usually diagnosed on MRI scans and are located predominantly in the sacral region (S1–S5), most commonly around the S2–S3 nerve roots.
Approximately 80–90% of reported Tarlov cysts are found in the sacral region, which is also the area where symptomatic cysts and surgical treatment are most commonly discussed. Because sacral nerves contribute to pelvic sensation, bladder, bowel, and sexual function, symptomatic cysts in this region may produce a broad spectrum of symptoms.
Although much less common, Tarlov cysts can also occur in the lumbar, thoracic, and cervical spine. These non-sacral cysts are often smaller and are less commonly responsible for clinically significant symptoms.
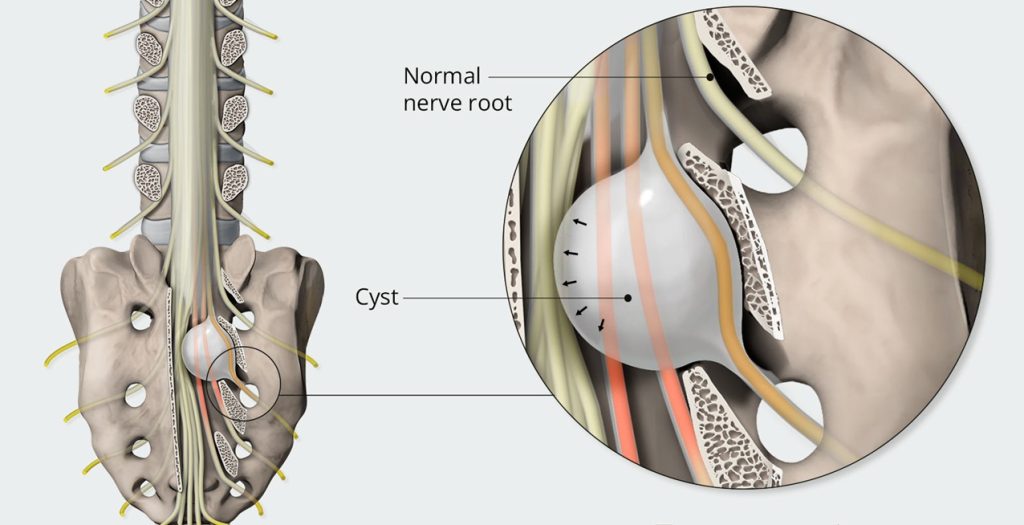
Image – the arrow points to a Tarlov cyst in sacral canal. Learn more on our Pain Anatomy page.
How Common Are Tarlov Cysts?
Tarlov cysts are a relatively common finding. Epidemiological studies estimate that these cysts are detected in approximately 4% to 9% of the general population undergoing spinal Magnetic Resonance Imaging (MRI). Given this high prevalence, the vast majority of cysts are considered asymptomatic findings (incidental findings) that require no treatment.
When Can Tarlov Cysts Cause Pain?
While most cysts are incidental, some should not be overlooked. Alone or in combination with other pathologic changes, they can compress or irritate nerve roots and thereby cause or sustain back or leg pain and neurologic symptoms. In such cases, they should not be dismissed as incidental. It is estimated that only 1% to 15% of patients with Tarlov cysts experience symptoms caused by the cyst. Symptomatic cysts are also diagnosed more frequently in women.
Symptoms Linked to Tarlov Cysts
Most Tarlov cysts do not produce significant compression or irritation of the nerve roots and are considered incidental findings. However, in certain cases, they may contribute to the development or persistence of symptoms.
Reported issues in the literature include:
- Low back and sacral pain
- Buttock, pelvic, tailbone or perineal pain
- Leg pain (sciatica-like symptoms)
- Pain aggravated by prolonged sitting or sitting intolerance
- Sensory deficits (numbness, tingling, or burning sensations)
- Weakness in the legs
- Urinary symptoms (urgency, hesitancy, retention, or incomplete emptying)
- Bowel dysfunction
- Sexual dysfunction or altered genital sensation.
How Are Tarlov Cysts Diagnosed?
Tarlov cysts are most often seen on MRI scans as fluid-filled formations. It is important to recognize which cysts are incidental findings and which may have a role in producing pain. It is also necessary to distinguish Tarlov cysts from other types of spinal cysts, since some of those more frequently require surgical treatment. The final judgment should be made by an experienced neurosurgeon.
Persistent Pain and Tarlov Cysts — Does Finding a Cyst on MRI Mean It Needs Treatment?
In many patients, the presence of a Tarlov cyst on MRI leads to the assumption that the cyst is automatically responsible for pain. However, persistent pain often reflects a more complex problem.
The first challenge is that the true pain-generating structure is frequently not identified. While MRI may show a Tarlov cyst, pain may originate from other structures in the lumbar, sacral, or pelvic region, including ligaments, facet joints, sacroiliac joint, muscles, nerve entrapment, or combinations of several pain generators.
The second problem is that the pathological process within these structures is often not clearly defined. Pain may result from inflammation, mechanical overload, instability, nerve irritation, or nervous system sensitization. These mechanisms do not behave the same way and therefore do not respond to the same treatment.
The third and often overlooked issue involves contributing factors that continue to trigger or maintain pain. These may include prolonged sitting, mechanical load, posture, movement patterns, pelvic mechanics, metabolic influences, low-grade inflammation, or persistent nervous system sensitization.
Because of this, pain may persist not simply because a Tarlov cyst exists, but because the diagnostic process remains incomplete. Successful treatment usually requires knowledge of pain anatomy — understanding which structures in this region may generate pain, what process is occurring within them, and which contributing factors must be diagnosed or excluded in order to design effective treatment.
Pain Contributing Factors That Should Also Be Diagnosed in Tarlov Cyst
In patients with persistent back and pelvic pain it is first necessary to determine which structure or combination of structures is responsible for pain. Even when a Tarlov cyst is present, pain may also arise from or be maintained by facet joints, sacroiliac joint dysfunction, ligaments, muscular spasm or inflammation, nerve irritation or entrapment, pelvic floor dysfunction, or combinations of several pain generators. It is equally important to identify additional factors that may maintain pain, increase sensitivity, delay recovery, or reduce the effectiveness of otherwise appropriate treatment. There factors are:
- Mechanical overload and daily habits — prolonged sitting, poor posture, repetitive bending, lifting, or asymmetrical loading may continue to irritate already sensitized structures
- Reduced physical activity and deconditioning — loss of strength, endurance, and spinal stability often develops after long-lasting pain and makes recovery more difficult
- Metabolic factors, pro-inflammatory diet and low-grade inflammation — obesity, insulin resistance, chronic inflammation, and processed/high-sugar diet increase pain sensitivity and impair recovery
- Nutritional deficiencies — low levels of vitamin D, vitamin B12, magnesium, or iron may contribute to nerve dysfunction and slower healing
- Vitamin-related factors — both deficiency and excess of vitamin B6 may contribute to burning pain, tingling, or hypersensitivity
- Sleep disturbance and pain cycle — poor sleep increases pain perception and reduces recovery capacity
- Stress and increased muscle tone — stress does not cause the pain, but increases muscle tension and nervous system reactivity, helping maintain symptoms
- Central sensitization — in long-standing pain, the nervous system may become more reactive, amplifying pain signals even when the original irritation is reduced
- Medications and long-term drug effects — certain medications and treatment patterns may contribute to persistent symptoms or altered pain processing. For example, statins may be associated with muscle pain in some patients; prolonged use of analgesics, especially opioids, may lead to increased pain sensitivity (opioid-induced hyperalgesia); repeated corticosteroid exposure may affect tissue balance and recovery; and polypharmacy can alter symptom perception without addressing the underlying mechanism.
- Other medical conditions and comorbidities — diabetes, thyroid disorders, autoimmune diseases, fibromyalgia, osteoporosis, and chronic inflammatory conditions may increase pain sensitivity and reduce treatment response
These factors should be identified and treated, but they should not replace the central task: the primary anatomical source of pain must still be correctly diagnosed and treated. In most patients, meaningful improvement requires addressing both.
Start Your Telehealth Consultation with a Pain Specialist
If you have Tarlov cyst and your back pain treatment has failed or you’re unsure what to do next — don’t wait. A detailed telehealth consultation can help identify the exact cause of your pain, even if previous therapies didn’t work.
- ✔ First, send a short message describing your problem
- ✔ You’ll receive a reply within 24 hours if and how we can help — including the consultation cost and a suggested time
- ✔ Only then, you can send your medical documentation
- ✔ The video consultation is followed by a written report and follow-up questions (up to 10 days)
- ✔ Secure payment by credit card, PayPal invoice (USD), or bank transfer.
Consultation fees typically range from $180–250, depending on the complexity of your case.
Based on our medical report, reimbursement can often be obtained (if your insurance plan allows it).
This is within the usual range for specialist telehealth consultations worldwide. Thousands of patients worldwide already use telehealth consultations for second opinions — it’s safe, accepted, and effective.
Treatment Options for Tarlov Cysts
Treatment options for Tarlov cysts depend primarily on whether the cyst is truly responsible for symptoms and how strongly symptoms correlate with imaging and clinical findings.
Management may range from observation and conservative treatment to image-guided procedures and, in carefully selected patients, microsurgical treatment.
The goal is not simply to treat an MRI finding, but to determine which treatment is appropriate for the actual pain mechanism and the individual patient.
Conclusion: Is Your Tarlov Cyst the Primary Cause or a Contributing Factor?
Only an experienced neurosurgeon can determine whether a Tarlov cyst is the actual cause of symptoms, a contributing factor, or completely asymptomatic—and based on this, decide on the appropriate treatment (observation, medication, or rarely surgery).
Indications for Surgery and Surgical Options in Tarlov Cysts
Once a Tarlov cyst is suspected to be clinically relevant, a structured evaluation is required before any treatment decision is made.
Only after careful clinical correlation — and when symptoms clearly match the affected nerve root — further steps may be discussed.
In selected cases, diagnostic image-guided procedures — such as temporary cyst aspiration or local anesthetic testing — may be used to confirm whether symptom relief occurs when pressure within the cyst is reduced. Even partial or temporary improvement can help clarify whether the cyst plays a meaningful role in the patient’s pain.
Based on:
- the clinical response,
- the anatomy and characteristics of the cyst,
- and the presence or absence of communication with the cerebrospinal fluid space,
a decision may then be made between minimally invasive image-guided treatments (such as aspiration with fibrin sealant) or, in rare and carefully selected cases, surgical procedures aimed at reducing the cyst and nerve irritation.
Patients may encounter many different names and descriptions of these procedures in medical or patient-focused literature. Terms such as cyst aspiration, fibrin sealant injection, decompression, cyst reduction, or microsurgical repair may sound confusing at first. During a professional consultation, these options are explained in clear and practical terms — focusing primarily on indications, expected benefit, and potential risks. The following sections briefly explain how some of these procedures are performed.
How Is Tarlov Cyst Aspiration Performed?
Temporary cyst aspiration is usually performed as an image-guided procedure, most commonly under CT or fluoroscopic guidance. A needle is carefully advanced into the cyst and a portion of the cerebrospinal fluid is removed to reduce internal pressure.
This procedure may serve two purposes. First, it can temporarily reduce pressure and symptoms in selected patients. Second, and often more importantly, it may provide diagnostic confirmation. If symptoms improve after decompression, even partially or temporarily, this supports the possibility that the cyst contributes to pain or neurological symptoms.
However, aspiration alone often provides only temporary benefit because fluid may gradually reaccumulate.
How Is Aspiration with Fibrin Sealant Performed?
In selected patients, aspiration may be followed by injection of fibrin sealant (fibrin glue) into the cyst cavity.
The principle is relatively straightforward: after cyst decompression, fibrin material is introduced with the goal of limiting refilling with CSF and reducing repeated pressure on adjacent nerve structures.
This is considered a minimally invasive image-guided procedure and is increasingly discussed in specialized centers managing symptomatic Tarlov cysts.
Not all cysts are suitable for this approach. Results depend on several factors, including cyst anatomy, the width of communication (neck) between the cyst and the cerebrospinal fluid space, and how strongly symptoms correlate with the cyst location.
How Is Microsurgical Tarlov Cyst Surgery Performed?
Modern Tarlov surgery is usually nerve-root preserving microsurgery rather than simple cyst removal. The main goal is to reduce cyst size and thereby decrease nerve compression and other forms of mechanical or fluid-related nerve irritation while preserving neurological function.
In the most common sacral procedures, the surgical approach is performed from the posterior aspect of the sacrum. Access to the cyst may require removal of part of the posterior sacral bone (sacral roof) in order to expose the involved region safely.
Once the cyst is identified, a particularly important step is careful recognition of the nerve root located within or attached to the cyst wall. Preservation of this nerve root is a central principle of modern surgery.
Rather than simply removing the cyst, treatment usually focuses on cyst reduction. This may involve controlled excision of part of the cyst wall combined with microsurgical suturing and reinforcement of the remaining wall, allowing the cyst to become smaller and reducing repeated pressure and irritation affecting the nerve.
Because these procedures involve delicate sacral nerve anatomy, they are technically demanding and generally reserved for carefully selected patients in whom symptoms clearly correlate with the cyst and alternative pain generators have been systematically excluded.
🎯 How We Assess Tarlov Cysts When Pain Is Still Unexplained
Many patients with Tarlov cysts are told that the cyst is either definitely responsible for their symptoms — or completely incidental. In reality, this decision is often more complex, and MRI findings alone may not explain whether the cyst is truly causing pain or whether another pain generator is involved.
Tarlov cysts are common MRI findings and in most cases are considered incidental. Yet in some patients, they may contribute to pain or neurological symptoms by irritating or compressing a nerve root. This consultation often reveals whether your cyst is a contributing factor or a completely incidental finding — something MRI alone cannot determine.
Before the consultation, the doctor reviews your MRI and records. During a video consultation, we correlate symptoms with imaging and use functional testing to pinpoint the pain source.
During the video consultation we:
- ask targeted questions about pain characteristics, sensory symptoms, and triggers,
- guide you to perform specific movements and to apply gentle pressure over mapped points,
- observe whether symptoms increase or decrease to identify the most likely level and structure involved,
- compare your responses with MRI-visible cysts to judge whether a cyst is relevant or incidental.
This approach has diagnostic value comparable to an in-person exam and often allows us to create a focused treatment plan. When a cyst is clinically relevant, we discuss conservative options and, in rare cases, surgical indications—always providing a clear written summary and the possibility to ask follow-up questions for up to 10 days.
The goal is simple: verify whether your Tarlov cyst is the pain generator or a bystander, and provide a precise treatment path.
FAQ – Tarlov Cysts
These are the most common questions patients ask after discovering Tarlov cysts on MRI — especially when symptoms persist or diagnosis is unclear.
What are Tarlov cysts?
Tarlov cysts are perineural or periradicular cysts filled with cerebrospinal fluid (CSF). They arise from the nerve root sheath and are most often found in the sacral spinal canal, especially around the S2–S3 nerve roots. Many are discovered incidentally on MRI performed for low back, sacral, pelvic, or leg symptoms. Although they can also occur in the cervical, thoracic, or lumbar spine, symptomatic Tarlov cysts are most commonly discussed in the sacral region because sacral nerves contribute to pelvic sensation, bladder, bowel, and sexual function.
Do Tarlov cysts always cause pain?
No. Most Tarlov cysts are incidental MRI findings and do not cause significant nerve compression or symptoms. This is important because many patients become worried as soon as the word “cyst” appears in an MRI report. The key question is not simply whether a Tarlov cyst exists, but whether the patient’s symptoms match the involved nerve root and whether other pain generators have been excluded. In selected patients, however, a cyst may irritate or compress a nerve root and contribute to persistent sacral, pelvic, buttock, or leg pain. Therefore, Tarlov cysts should not be automatically blamed, but they should not be automatically dismissed either.
What symptoms can Tarlov cysts cause?
Most Tarlov cysts cause no symptoms. When they are clinically relevant, symptoms may include low back pain, sacral pain, buttock pain, pelvic or perineal pain, tailbone discomfort, sciatica-like leg pain, numbness, tingling, burning sensations, or leg weakness. Some patients report sitting intolerance, pain aggravated by pressure, or symptoms that fluctuate with posture and activity. Because sacral nerve roots are involved in bladder, bowel, and sexual function, selected patients may also have urinary urgency, hesitancy, retention, bowel dysfunction, altered genital sensation, or sexual dysfunction. These symptoms are not specific to Tarlov cysts, so correlation with MRI anatomy and clinical findings is essential.
How are Tarlov cysts diagnosed?
Tarlov cysts are usually diagnosed on spinal MRI as CSF-filled formations related to the nerve root sheath. MRI helps show the cyst location, size, relation to the sacral canal, and whether the cyst is near nerve roots that could explain the patient’s symptoms. However, diagnosis does not end with seeing the cyst on MRI. The more important clinical task is deciding whether the cyst is incidental, contributory, or the main pain generator. This requires correlation between symptoms, neurological findings, pain distribution, sitting intolerance, bladder or pelvic symptoms, and the exact level of the cyst. Other spinal or pelvic causes of pain must also be considered.
When can a Tarlov cyst be the source of pain?
A Tarlov cyst can be considered a possible source of pain when symptoms match the involved nerve root and when the cyst appears capable of irritating or compressing neural structures. This may be more likely when pain is located in the sacrum, buttock, pelvis, perineal region, or leg, especially if symptoms worsen with sitting, pressure, straining, or certain movements. Still, the cyst may be only one part of the problem. Sacroiliac dysfunction, ligament pain, muscular spasm, pelvic floor dysfunction, pudendal irritation, lumbar disc disease, or central sensitization may produce similar symptoms. A careful clinical correlation is needed before labeling the cyst as the primary pain generator.
What does an S2 or S3 Tarlov cyst mean?
An S2 or S3 Tarlov cyst means that the cyst is located around the second or third sacral nerve root. This is a common location for sacral Tarlov cysts. These nerve roots contribute to pelvic sensation and may be related to symptoms in the sacrum, buttock, perineal region, genital area, bladder, bowel, or legs. However, the level alone does not prove that the cyst is symptomatic. A small S2 or S3 cyst may be incidental, while another cyst in the same region may be clinically relevant if symptoms, MRI anatomy, and functional findings match. The meaning of the finding depends on correlation, not on the label alone.
Can a Tarlov cyst cause hip, pelvic, buttock, or leg pain?
Yes, in selected patients a symptomatic Tarlov cyst may contribute to hip-region pain, buttock pain, pelvic discomfort, sacral pain, perineal symptoms, or sciatica-like leg pain. This happens when the cyst irritates, stretches, or compresses sacral nerve roots. However, these symptoms are not specific to Tarlov cysts. Hip disorders, sacroiliac joint dysfunction, piriformis or gluteal muscle pain, lumbar disc disease, pudendal neuralgia, pelvic floor dysfunction, and ligament pain may produce similar complaints. This is why MRI alone is not enough. The question is whether the pain pattern, neurological symptoms, sitting intolerance, and cyst location form a consistent clinical picture.
Why does sitting worsen my pain — could a sacral Tarlov cyst be the reason?
Sitting may worsen symptoms in some patients with sacral Tarlov cysts because prolonged pressure and altered pelvic mechanics can increase irritation of nearby sacral nerve roots. This may lead to pain in the lower back, sacrum, buttock, perineal region, or legs, and sometimes to numbness or sitting intolerance. However, sitting pain is not specific to Tarlov cysts. Similar symptoms may arise from sacroiliac dysfunction, coccygeal disorders, pelvic floor tension, ligament pain, pudendal irritation, or combinations of several pain generators. For this reason, sitting-related symptoms should not automatically be attributed to the cyst itself. Correlating symptom patterns with MRI findings and clinical assessment helps determine whether the cyst is clinically relevant.
Can a Tarlov cyst mimic pudendal neuralgia or tailbone pain?
Yes. Because Tarlov cysts commonly involve sacral nerve roots responsible for pelvic sensation, they may sometimes produce symptoms that resemble pudendal neuralgia or coccyx-related pain. Patients may report burning, perineal discomfort, sitting intolerance, genital symptoms, rectal pressure, or pain around the tailbone and pelvic floor. However, symptom overlap creates diagnostic difficulty. Pudendal neuralgia, pelvic floor dysfunction, sacroiliac disorders, coccygeal pathology, muscular spasm, and other pelvic pain conditions may produce similar complaints. A Tarlov cyst may therefore be the primary cause, a contributing factor, or an incidental MRI finding. Distinguishing these possibilities requires careful analysis of pain anatomy and symptom distribution.
Can a Tarlov cyst cause urinary urgency, retention, or sexual dysfunction?
It can, particularly when cysts involve sacral nerve roots responsible for bladder, bowel, and sexual function, most commonly S2–S4. Patients may report urinary urgency, hesitancy, incomplete emptying, retention, altered genital sensation, painful intercourse, or sexual dysfunction. However, these symptoms are often multifactorial and do not automatically prove that a Tarlov cyst is responsible. Similar problems may also result from pelvic floor dysfunction, gynecological or urological conditions, medication effects, autonomic dysfunction, or other neurological disorders. Evaluation focuses on symptom correlation rather than MRI appearance alone. The goal is to determine whether the cyst directly irritates relevant nerve roots, contributes alongside other factors, or represents an incidental finding.
What does Tarlov cyst size on MRI mean?
Tarlov cyst size on MRI is important, but it does not determine treatment by itself. A larger cyst may have a greater chance of affecting nearby nerve roots or remodeling the sacral canal, but a small cyst can still be relevant if symptoms clearly match its location. Conversely, a larger cyst may be incidental if there is no clinical correlation. MRI should be used to understand cyst level, size, shape, relation to nerve roots, and possible communication with the CSF space. The clinical meaning of size depends on symptoms, neurological findings, pain distribution, and whether other pain generators have been excluded.
Do Tarlov cysts grow over time — should I repeat MRI?
Most Tarlov cysts remain stable over time, but a minority may enlarge, fluctuate, or become more clinically relevant if symptoms change. Repeat MRI is usually considered when pain becomes worse, new neurological symptoms appear, bladder or bowel symptoms develop, or the previous MRI did not clearly show the cyst anatomy. Routine rescanning is not always necessary for every incidental cyst. The interval should be individualized rather than based only on a calendar rule. If symptoms are stable and the cyst appears incidental, observation may be enough. If symptoms progress, repeat MRI can help reassess cyst size, nerve root relation, and possible alternative causes of pain.
Why doesn’t MRI alone explain my Tarlov cyst pain?
MRI shows anatomy, but it does not directly show pain generation. A scan may reveal a Tarlov cyst, degenerative changes, disc findings, or several abnormalities at the same time, while the true pain source may be another structure or a combination of structures. Pain may arise from nerve irritation, inflammation, mechanical overload, sacroiliac dysfunction, ligament pain, muscular spasm, pelvic floor dysfunction, or nervous system sensitization. This is why the presence of a Tarlov cyst on MRI does not automatically prove that it is responsible for symptoms. The cyst must be interpreted together with pain distribution, functional assessment, neurological symptoms, sitting tolerance, and clinical reasoning.
Do all Tarlov cysts need surgery?
No. Most Tarlov cysts do not require surgery because many are incidental MRI findings and are not the true cause of symptoms. The key question is not simply whether a cyst exists, but whether symptoms clearly correlate with the involved sacral nerve root and whether the cyst behaves as the primary pain generator, a contributing factor, or merely an unrelated finding. Before surgery is considered, it is important to exclude other potential pain sources such as sacroiliac dysfunction, ligament pain, muscular spasm or inflammation, pudendal irritation, or combined pain mechanisms. Surgical treatment is reserved for carefully selected patients in whom clinical findings, MRI anatomy, and symptom correlation consistently support cyst-related nerve irritation.
How is treatment decided for a symptomatic Tarlov cyst?
Treatment is not determined solely by MRI appearance or cyst size. The decision process begins by establishing whether the Tarlov cyst is truly related to symptoms and whether additional pain generators or contributing factors are present. This usually requires correlating pain distribution, neurological symptoms, MRI findings, and the anatomy of the involved sacral nerve roots. In some patients, conservative treatment targeting inflammation, muscular spasm, pelvic mechanics, or nerve sensitization may be appropriate. In selected cases, image-guided procedures such as aspiration or aspiration combined with fibrin sealant may help clarify or reduce symptoms. Microsurgical treatment is considered only when symptoms strongly correlate with cyst anatomy and other explanations have been carefully evaluated.
When is aspiration or surgery considered for a Tarlov cyst?
Aspiration or surgery is considered only in selected patients, not simply because a Tarlov cyst appears on MRI. Image-guided aspiration may sometimes be used diagnostically to see whether reducing cyst pressure improves symptoms, even temporarily. Aspiration with fibrin sealant may be considered in carefully selected cysts when anatomy is suitable. Microsurgical treatment is usually reserved for patients with persistent disabling symptoms, strong correlation between cyst level and symptoms, and insufficient response to conservative or less invasive approaches. The decision depends on cyst anatomy, communication with the CSF space, nerve root involvement, symptom pattern, and exclusion of other pain generators.
Are epidural or nerve injections safe if I have a Tarlov cyst?
Image-guided injections may sometimes be used in patients with Tarlov cysts, but careful planning is important. The presence of sacral cysts can change local anatomy and may increase the importance of avoiding poorly targeted or blind procedures near involved nerve roots. Depending on symptoms and cyst location, a specialist may recommend alternative approaches or targeted image-guided techniques designed to minimize risk and improve diagnostic value. In some cases, injections help clarify whether pain originates from sacral nerve irritation or from associated pain generators such as sacroiliac joint dysfunction, ligament pain, or muscular inflammation. Decisions are individualized and based on anatomy, symptom correlation, and procedural safety.
What activities or exercises should patients avoid with symptomatic Tarlov cysts?
There is no single activity rule for all patients with Tarlov cysts, because symptoms and pain generators differ. During painful flares, many patients should avoid prolonged sitting, heavy lifting, repetitive straining, high-impact exercise, aggressive stretching, or movements that clearly reproduce sacral, pelvic, or leg symptoms. Gentle walking, gradual conditioning, pelvic-floor relaxation, and carefully guided core stabilization may be better tolerated, but exercises must be individualized. The goal is not complete inactivity, but avoiding repeated mechanical irritation while maintaining safe mobility. If symptoms worsen with a specific activity, that pattern can also help identify whether the cyst, pelvic mechanics, sacroiliac region, or another structure is contributing to pain.
Can daily activities be affected by symptomatic Tarlov cysts?
Yes, daily activities can be affected when a Tarlov cyst is symptomatic or when it contributes to a broader pain syndrome. Patients may have difficulty sitting for long periods, driving, bending, lifting, walking longer distances, exercising, working at a desk, or tolerating pressure over the sacral and pelvic region. Some may also limit sexual activity or social activities because of pelvic, perineal, or bladder-related symptoms. However, activity limitation does not automatically prove that the cyst is the only cause. Functional assessment helps determine whether symptoms are driven by cyst-related nerve irritation, sacroiliac or pelvic mechanics, muscle spasm, inflammation, sensitization, or combined pain generators.
Can Tarlov cyst pain be assessed through an online consultation?
Yes. A focused online consultation can help assess whether a Tarlov cyst is likely to be symptomatic, contributory, or incidental. Before the consultation, MRI images and reports are reviewed. During the video visit, the doctor asks targeted questions about pain distribution, sitting intolerance, pelvic symptoms, sensory changes, triggers, and previous treatments. Functional self-tests and pressure-point mapping may help identify whether symptoms fit the cyst location or whether another pain generator is more likely. This does not replace emergency care or hands-on examination when needed, but it can provide a structured second opinion, clarify MRI findings, and help guide conservative, image-guided, or surgical decision-making.
Can I get reimbursed by my health insurance for this consultation about Tarlov cyst?
Reimbursement depends on your individual insurance plan and the type of coverage you have. Some patients may be able to submit documentation for reimbursement, especially if their plan includes out-of-network specialist or telehealth benefits. We do not bill insurance companies directly. When a written medical report is provided, it can be accompanied by a detailed invoice containing the clinical information typically required for reimbursement claims. Approval is never guaranteed, so patients should check their insurance policy before assuming reimbursement will be accepted.
Detailed online consultation for Tarlov cyst pain
Schematic explanation of the video consultation for Tarlov cyst pain
Answers to questions about the process and success of video consultations for Tarlov cyst pain
See the page “Possible Reasons for Poor Pain Treatment Effectiveness of Tarlov Cyst Pain” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
Treatment of complex cases of Tarlov cyst pain can be analysed by artificial intelligence (AI)
Video consultation is also known as a virtual visit, video visit, second opinion consultation, online consultation, remote consultation or telehealth appointment.