Dr Željko Kojadinović — NEUROHIRURGIJA I LEČENJE BOLA
Dr Zeljko Kojadinovic — Pain Treatment & Neurosurgery

Autor: Dr sci. med. Željko Kojadinović, neurohirurg i specijalista za lečenje bola
ONLINE PAIN CONSULTATION
Pain can be: acute (till 3 weeks), subacute (3 weeks to 3 months) and chronic (more than 3 months).
Acute pain is useful only at the beginning of the illness because it indicates that there is a pathological process. Any pain that lasts longer than 3 weeks tends to remain persistent and to become an illness by itself. That’s why it should be treated at the very beginning.
Chronic pain persistent to usual therapy is frequent. 25% of the population need sometimes therapy for chronic pain in their life. It can be cancerous and noncancerous pain. Musculoskeletal and neuropathic pain represents 80% of all chronic pain syndromes
PAIN ANATOMY
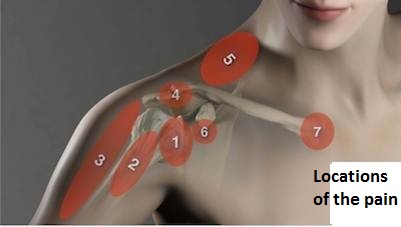
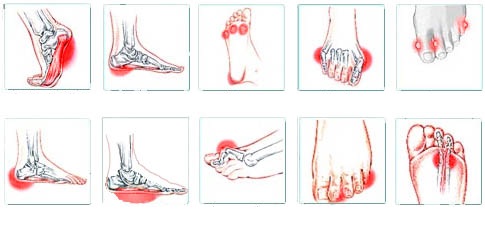
Most of these pain syndromes have similar diagnostic and therapeutic approaches. The following facts can be applied to most pain locations “from head to heel”: headache, Facial pain, Neck pain, Shoulder pain, Arm pain, Back pain, perineal pain, Leg pain, Knee pain, Foot pain, Heel pain, etc.

Essential for the successful treatment of any pain is to identify:
- Which anatomical structure is a source of the pain (pain anatomy)
- What kind of pathologic process is in that structure?
When anatomical sources and pathological processes are identified success in pain treatment (healing or significant reduction) is in 70-90% of the patients. ( We mention that these patients have been suffering from pain for a long time without therapy effect.)
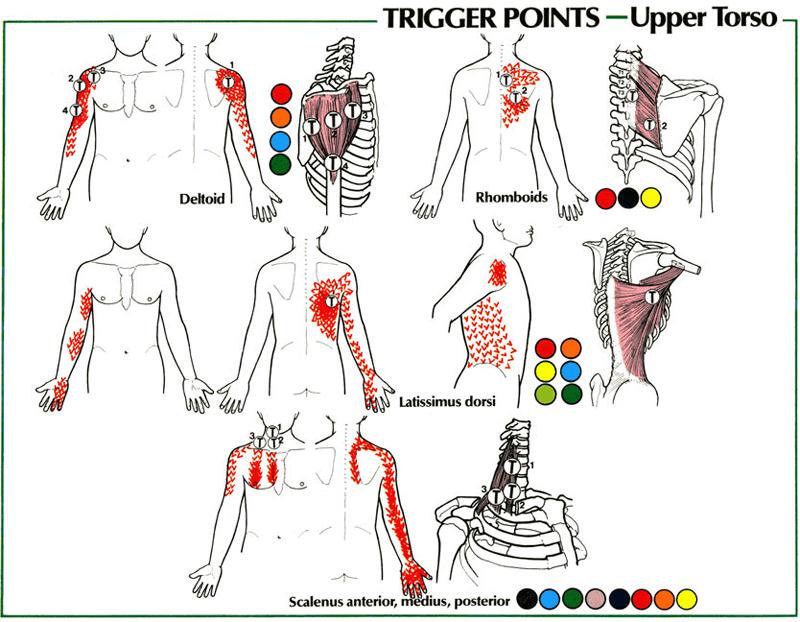
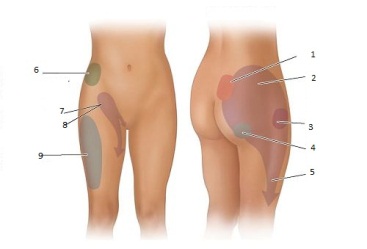
Pain anatomy means that every body region can have 10-20 possible sources of pain such as: muscles, nerves, ligaments, joints, tendons, fascia, bursa, etc.

Pathologic processes in or around these structures can be: inflammation, pressure, strein, overstretch, spasm, and neuropathy.
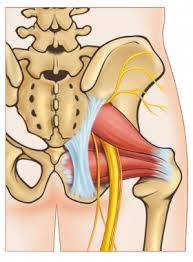
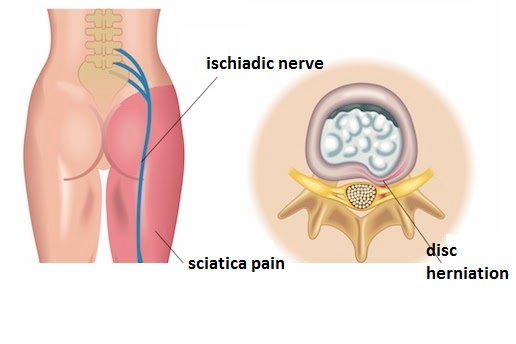
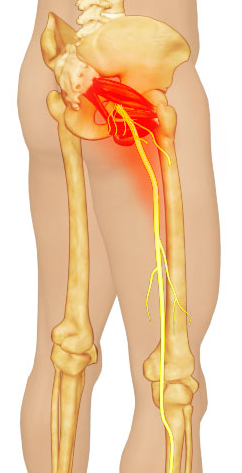
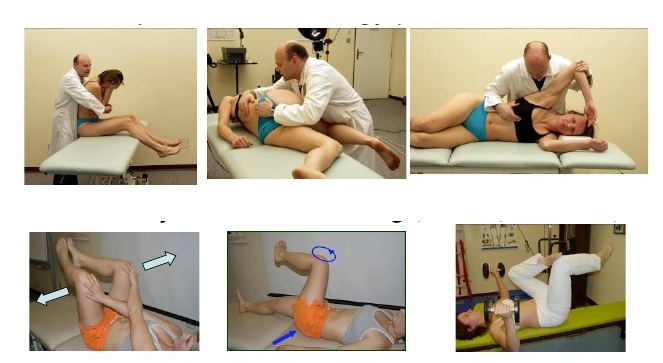
For example: In the picture below the same sciatica can be caused by disc prolapse or by inflammation and spasms of some muscles irritating the sciatic nerve. If this is not known the problem is when nothing is evident on spine CT or MRI. An even bigger problem could be if an asymptomatic discus hernia is visible on images. Then unnecessary surgery could be performed.
Without knowing the real cause of the pain most diagnoses that are not accurate enough are set as final diagnoses. Examples include: sciatica, cervical syndrome, lumbar degenerative pain, spondilopathy, gonarthrosis, rheumatic disease, headache, etc. In these situations usually contributing factors are proclaimed to be the main reasons for the pain like: old age, obesity, bad posture, degenerative changes, psychological overreaction, circle cell anemia, etc. Even if these factors cannot be changed easily it doesn’t mean that in that period patient has to suffer the pain.

PAIN DIAGNOSIS
To determine which anatomical structure is the cause of pain a long conversation with the patient covering all important details. In practice this conversation is too often made without real “listening” to the patient and without entry into important details.

Examination of the patients must include specific examinations. There are a great number of specific tests for different anatomical structures. Without knowing this examinations real cause of the pain and successful treatment cannot be performed.

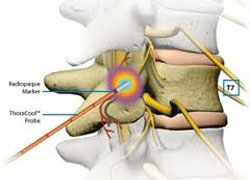
Diagnostic images usually mean: X-Ray, CT (Computer tomography), EMNG, MRI, etc. However one important diagnostic method is usually missing. It is a minimally invasive pain diagnostic intervention. This method is often the only one that can identify the cause of pain. By this, we have avoided performing many unnecessary operations which would be indicated concerning only examination MRI and other images. (For example, many unnecessary disk surgeries are still being performed because this diagnostic method was not done).
PAIN TREATMENT
Pain treatment includes:
- Contemporary medications It is very important to know the type of pathologic process and to cover it with the proper combination of types and dosages of medications. (different types of nociceptive pain, neuropathic pain, psychological component of the pain, etc.). Usually, physicians start with nonsteroid anti-inflammatory drugs (NSAIDs like metamizole, ibuprofen, paracetamol, etc.). Sometimes opioid analgesics are prescribed too early or too long. However, other types of medications and procedures can make opioid usage unnecessary.
- Physiotherapy- is very important but if unsuccessful should not be repeated many times without trying other solutions
- Acupuncture– This method can be valuable, especially in combination with others. All alternative pain treatments are usually not sufficient when intensive pain lasts more than three months resistant to usual medications.
- Chiropractic- the same as acupuncture
- Alternative therapy – the same as acupuncture
- Surgery– mostly done when a mechanical component of pain cannot be treated by any other method. Even if we perform all kinds of surgeries minimally invasive we are always trying and often succeed in treating the pain without them. But when indicated we can perform safely and minimally invasive all kinds of surgeries for pain treatment such as: nerve decompression in the cases of neuralgias (occipital neuralgia, trigeminal neuralgia, carpal tunnel syndrome, cubital syndrome, tarsal syndrome, meralgia, Morton neuroma, etc.); disc surgeries with or without spinal stabilization (lumbar, cervical, etc.) BUT WE STRONGLY RECOMMEND NOT TO DO SURGERY BEFORE TRYING TO SOLVE THE PAIN BY MINIMALLY INVASIVE PAIN TREATMENT INTERVENTIONS IN MOST CASES. FOLLOWING THIS STRATEGY WE SUCCEEDED IN AVOIDING ABOUT 70% OF OPERATIONS THAT WERE INDICATED BY OTHER SURGEONS. If surgical decompression is indicated it must be minimally invasive but sufficient (The next mistake we see in everyday practice is that the doctor decompresses the nerve insufficiently in the endeavor to impress the patient with the small incision).
- Neuromodulation is expensive and reserved for a small percentage of untreatable pain syndromes
MINIMALLY INVASIVE PAIN TREATMENT INTERVENTIONS
- Are not classical blockades. They can only remind them but have much higher precision (e.g. epidural block, facet block, nerve block, trigeminal block, myofascial blockade, articulation injection, application of PRP and stem cells, etc.)
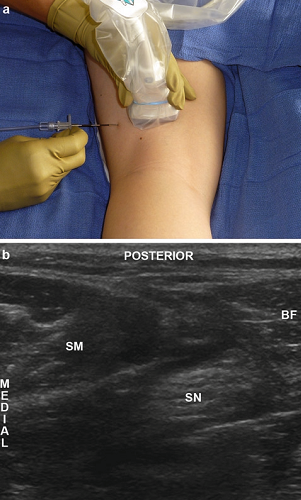
- They are performed with navigation of ultrasound or X-ray fluorography
- Navigation provides accurate application of medications, denervation, hidrodilatation or other interventions
- Most of them can be done ambulatory in local anesthesia and can be done in 30 minutes
- Results are evident immediately
- Mostly 1 to 3 interventions are sufficient
- Good long-lasting results can be achieved in 70-90% of all patients
- They should be performed before most pain surgery procedures to avoid them if possible (e.g. spine disc surgery)




CONCLUSION
-Essential for successful treatment of persistent pain is to identify its real source (PAIN ANATOMY KNOWLEDGE)
-This can be done after detailed conversations with the patients, specific examinations and invasive diagnostic pain procedures
-When classical pain therapy doesn’t help invasive therapeutic pain procedures should be applied
-For the success 1-3(-5,…) procedures are usually needed
-The success rate is in 70-90% of patients suffering from chronic pain resistant to other therapies
We offer you online pain consultation based on telemedicine. Video consultation is also known as a virtual visit, video visit, online consultation, remote consultation or telehealth appointment.
Online pain consultation in detail
Schematic explanation of the video consultation
Answers to questions about the process and success of video consultations
See the page “Possible Reasons for Poor Pain Treatment Effectiveness” for an explanation of why conventional chronic pain treatments often fail—and what we do differently.
By using this service, you agree to our Terms of Use and Privacy Policy (in Serbian – your browser may offer translation).
- TELEMEDICINE – PERSISTENT PAIN (E.G. VARIOUS NEURALGIES) CAN ONLY BE RESOLVED BY AN EXPERT WHO KNOWS THE ANATOMY OF PAIN WELL. PROBABLY YOU DON’T HAVE AN EXPERT LIKE THIS IN YOUR TOWN. TELEMEDICINE ENABLES DIAGNOSIS WITHOUT A CLASSIC EXAMINATION IN THE OFFICE. THAT’S WHY MOST PERSISTENT PAIN IS SOLVED TODAY WITH A VIDEO CONSULTATION WITH AN EXPERT LIKE THIS. ON THE OTHER HAND, MOST PATIENTS IN THE OFFICE ARE EXAMINED BY DOCTORS WHO DO NOT KNOW THE ANATOMY OF PAIN. Affordable and efficient online consultations are possible through this site. We have been using this method of diagnosing and treating pain successfully for 12 years. The consultation is carried out with prior notice to zkoja@yahoo.com. Then send a description of the problem in a few sentences. After announcing, you will receive an email explaining the consultation procedure and determining the time. The GOAL of consultation in the treatment of pain syndrome is to accurately determine the location of the source of pain and which pathological process is occurring in it. This is successfully achieved by reviewing your medical documentation and video interviews. After that, it is possible to prescribe an adequate individual combination of drugs. The goal of this therapy is to resolve the pain within 10 days. After that, it is necessary to control the pain with drugs for a total of 6 weeks in order to achieve a lasting effect, when the drugs are discontinued. This can be achieved in 90% of patients who have chronic persistent pain in any part of the body, which has responded poorly to previous treatment. During all that time, the doctor treating you is available for all your questions. All types of long and persistent pain can be treated in this way, such as headaches, neck pain, facial pain, back pain, herpes zoster neuralgia, intercostal neuralgia, etc.
Start Your Video Consultation
If your pain treatment has failed or you’re unsure what to do next — don’t wait. A detailed video consultation can help identify the exact cause of your pain, even if previous therapies didn’t work.
- ✔ First, send a short message describing your problem
- ✔ You’ll receive a reply if and how we can help — including the consultation cost and a suggested time
- ✔ Only then, you can send your medical documentation
- ✔ The video consultation is followed by a written report and follow-up questions (up to 10 days)
We will inform you about the consultation fee based on the complexity of your case.
There are several reasons why chronic pain treatments fail, and these same mistakes are often repeated in many patients.
👉 Learn more on this page
Additional information
Surgical treatment of chronic pain
Pain treatment – Romanian language
Read more: PAIN TREATMENT in Serbia (Belgrade, Novi Sad) Read more: PAIN TREATMENT in Serbia (Belgrade, Novi Sad)